clinical study protocol preventing cholestasis … · (smoflipid®) with a soybean oil based lipid...
TRANSCRIPT

PreventingCholestasisinPrematureInfantsUsingSMOFLipid®/SMOFLipid®MedicalUniversityofVienna,DepartmentofPediatricsEUDRACTNr2011-005456-33
Date22.8.2013 Version1.3 Page1of38
CLINICALSTUDYPROTOCOL
PREVENTINGCHOLESTASISINPREMATUREINFANTSUSINGSMOFLIPID®
Version1.3/22.8.2013ConfidentialityStatementTheinformationcontainedinthisdocument,especiallyunpublisheddata,isthepropertyofthesponsorofthisstudy.Itisthereforeprovidedtoyouinconfidenceasaninvestigator,potentialinvestigator,orconsultant,forreviewbyyou,yourstaff,andanIndependentEthicsCommitteeorInstitutionalReviewBoard.ItisunderstoodthatthisinformationwillnotbedisclosedtootherswithoutwrittenauthorizationfromtheDepartmentofPediatrics,MedicalUniversityViennaexcepttotheextentnecessarytoobtaininformedconsentfromthosepersonstowhomthestudydrugmaybeadministered.
PreventingCholestasisinPrematureInfantsUsingSMOFLipid®/SMOFLipid®MedicalUniversityofVienna,DepartmentofPediatricsEUDRACTNr2011-005456-33
Date22.8.2013 Version1.3 Page2of38
Testdrug(IMP)andPharmaceuticalCompany
SMOFlipid®FreseniusKabiAG,BadHomburg,Germany
Protocolauthors AndreasRepa,MD
InvestigatorsAndreasRepa,MDNadjaHaiden,MDRenateFuiko,PhD
Documenttype Clinicalstudyprotocol
Studyphase PhaseIV
Documentstatus Version1.2
Date 17.9.2012
Numberofpages 38
PreventingCholestasisinPrematureInfantsUsingSMOFLipid®/SMOFLipid®MedicalUniversityofVienna,DepartmentofPediatricsEUDRACTNr2011-005456-33
Date22.8.2013 Version1.3 Page3of38
1. SPONSOR,INVESTIGATOR,MONITORANDSIGNATURESSponsor/orrepresentative(OEL)(AMG§§2a,31,32) MedicalUniversityofVienna,AustriaO.Univ.Prof.Dr.ArnoldPollak________________ ___________Signature(OEL) DateInvestigator(AMG§§2a,35,36) PDDr.med.univ.NadjaHaiden,DepartmentofPediatrics,MedicalUniversityofVienna,Austria _________________ ___________Signature DateMonitor/orRepresentativeofCRO(AMG§§2a,33,34) KoordinierungszentrumfürKlinischeStudien(PD.Dr.JohannesPleiner)_________________ ___________Signature DateStatistician Mag.IreneSteiner_________________ ___________Signature DateClinicalTrialsCenters:MedicialUniversitiyofVienna,Austria
PreventingCholestasisinPrematureInfantsUsingSMOFLipid®/SMOFLipid®MedicalUniversityofVienna,DepartmentofPediatricsEUDRACTNr2011-005456-33
Date22.8.2013 Version1.3 Page4of38
2. PROTOCOLSYNOPSISTITLE PreventingCholestasisinPrematureInfantsUsingSMOFLipid®OBJECTIVES PrimaryObjective
• To compare a mixed parenteral lipid emulsion containing fish oil(SMOFlipid®)withasoybeanoilbased lipidemulsion (Intralipid®) for itseffectontheoccurrenceofparenteralnutritionassociatedcholestasis inextremelylowbirthweightinfants
SecondaryObjectives• To assess the impact of SMOFLipid® on the long term neurocognitive
developmentofextremelowbirthweightinfantsat12and24monthsofcorrectedage
DESIGN/PHASE Prospective,randomized,double-blind,phaseIVstudy.STUDYPLANNEDDURATION Firstpatient
Firstvisit
1stmonth
LastpatientFirstvisit
36months
LastpatientLastvisit
62months
CENTER(S)/COUNTRY(IES)
Singlecenter,Austria(Medical University Vienna, Austria; Department of Neonatology, PediatricIntensiveCareandNeuropediatrics,UniversityChildren´sHospital,)
PATIENTS/GROUPS 200patientsin2groups100patientspergroupBlockrandomizationratio1:1,stratificationbysexandweight(intwogroups:<750gramvs.≥750gram).Incaseoftwins,randomizationwillbeappliedtothefirstborn;thetwinwillbeassignedtotheothertreatmentgroup.Tripletsorhigherwillbeexcluded.
INCLUSIONCRITERIA • Infants born with a birth weight ≤ 1000 Gram (= extreme low birthweightinfants)
• Admissiontotheneonatalwardinthefirst24hoursoflife• Informed consent obtained and randomized on study drug the first 5
daysoflifeEXCLUSIONCRITERIA • Tripletsorhigher
• Conjugatedbilirubin>1.5mg/dlbeforeinclusiontothestudy• Conditions associated with cholestasis independent of parenteral
nutrition:o Inbornerrorsofmetabolismo ViralInfections(cytomegalyvirus,HIV,HepatitisB,C)o Immunemediatedhemolyticdiesease(e.g.Rhesusincompatibility)o Cysticfibrosiso Primarycholestaticdiseasesoftheliver• ForNeurodevelopmentaloutcomeinfollowupphase:Congenital
neurologicalmalformationsandchromosomalaberrationsSTUDYPERIODS • OperationalPhase:Theoperationalphaseofthestudywilllastforthree
years(months1-39)andstartwiththeinclusionofthefirstpatienttothetrialandwillendwiththelastpatient’sdischargefromhospital.
• Follow Up: The follow up phase will last start with the first includedpatientreachingtheageof12monthscorrectedageandwillendat24monthsofcorrectedgestationalageofthelastincludedpatient(months15-62)
INVESTIGATIONALDRUG SMOFLIPID®:
PreventingCholestasisinPrematureInfantsUsingSMOFLipid®/SMOFLipid®MedicalUniversityofVienna,DepartmentofPediatricsEUDRACTNr2011-005456-33
Date22.8.2013 Version1.3 Page5of38
initialdose:1g/kg/day targetdose:3g/kg/day
COMPARATIVEDRUG/CONTROLCONDITION
INTRALIPID®initialdose:1g/kg/day targetdose:3g/kg/day
CONCOMITANTMEDICATION In case of of cholestasis (i.e. conjugated bilirubin two times > 1.5 mg/dl),ursodeoxycolicacidat20-30mg/kg/dayisthetreatmentofchoice.In case of severe cholestasis (i.e. conjugated bilirubin > 6 mg/dL) andelevationofliverenzymes(3timesovernormal)arescuetherapyusingpurefishoil(Omegaven®)at0.5-1g/kg/daywillbeallowed.
EFFICACYENDPOINT Incidence of parenteral nutrition associated cholestasis (PNAC), defined asconjugatedbilirubin>1.5mg/dlmeasuredontwoconsecutiveoccasionsbybloodsamplingperformedatleastevery10+/-4days.Basedonapresentincidenceof25%usingthecomparativedrugatthestudycenter(unpublisheddata2007-9)anabsolutedifferenceof15%betweenthegroups(25%vs.10%incidence)wasconsideredclinicallysignificant.
TOLERABILITY/SAFETYENDPOINTS
-
PHARMACOKINETIC/PHARMACODYNAMICENDPOINTS
-
QUALITYOFLIFE/PHARMACOECONOMICENDPOINTS
-
STATISTICALMETHODOLOGY PrimaryEndpointPNAC(definitionseeefficacyendpoint)Nullandalternativehypotheses:H0:ThepercentageofPNACingroup1(investigationaldrug)equalsgroup2(comparativedrug)H1:ThepercentageofPNACingroup1(investigationaldrug)doesnotequalgroup2(comparativedrug)SamplesizecalculationAsamplesizeestimationusingaχ2-testindicatedthat200infants(100/group)arerequiredtodetecta15%diference(10%ingroup1vs.25%ingroup2)withapowerof80%andatwo-sidedsignificancelevelof0.05.Theestimateddropoutrateis22%.Therefore,asamplesizeof122patientspergroupisplanned.Forsamplesizeestimation,datawereassumedtobeindependent.StatisticalmethodologyMainanalysisset(s)Aχ2-testwillbeusedforanalysisoftheprimaryoutcomePNAC.Additionally,theeffectoftreatmentandotherrelevantinfluencefactors(i.e.durationofparenteralnutrition,birthweight,necrotizingenterocolitis)ontheprimaryendpointwillbeanalyzedusingalogisticregressionmodelwith

PreventingCholestasisinPrematureInfantsUsingSMOFLipid®/SMOFLipid®MedicalUniversityofVienna,DepartmentofPediatricsEUDRACTNr2011-005456-33
Date22.8.2013 Version1.3 Page6of38
stepwiseselection.Incaseoftwins,theanalysiswillbecarriedout1)asmentionedabove,butonlyincludingthefirstbornand2)bycalculatingageneralizedlinearmodelwithmotherasrandomfactor.OtherendpointsBaileyScalesof InfantDevelopment IIIat12and24months:Differences inthe scores of psychomotor development and neurocognitive development,respectively, between the groups will be analyzed by repeated measuresANOVAs, also accounting for confounder factors (e.g. birth weight, …). Incaseoftwins,theanalysiswillbecarriedout1)asmentionabove,butonlyincludingthefirstbornand2)bycalculatingamixedmodelwithmotherandchildasrandomfactor. Incaseof toomanydropouts,descriptivestatisticswillbecarriedout.ForGrossMotor functionmeasurements at 12 and 24months, descriptivestatisticswillbeconducted.

PreventingCholestasisinPrematureInfantsUsingSMOFLipid®/SMOFLipid®MedicalUniversityofVienna,DepartmentofPediatricsEUDRACTNr2011-005456-33
Date22.8.2013 Version1.3 Page7of38
3. LISTOFABBREVATIONSELBW ExtremeLowBirthWeightICH InternationalConferenceonHarmonizationILE IntravenousLipidEmulsionGCP GoodClinicalPracticeDHA DocosahexaenoicAcidDOH DeclarationofHelsinkiLC-PUFA LongChainPolyunsaturatedFattyAcidsPN ParenteralNutritionPNAC ParenteralNutritionAssociatedCholestasis
PreventingCholestasisinPrematureInfantsUsingSMOFLipid®/SMOFLipid®MedicalUniversityofVienna,DepartmentofPediatricsEUDRACTNr2011-005456-33
Date22.8.2013 Version1.3 Page8of38
4. TABLEOFCONTENTSCLINICALSTUDYPROTOCOL 1PREVENTINGCHOLESTASISINPREMATUREINFANTSUSINGSMOFLIPID® 11. SPONSOR,INVESTIGATOR,MONITORANDSIGNATURES 32. PROTOCOLSYNOPSIS 43. LISTOFABBREVATIONS 74. TABLEOFCONTENTS 8TABLE1.VISITANDASSESSMENTSCHEDULE 105. BACKGROUNDINFORMATION 115.1 BACKGROUND 115.2 STUDYRATIONALE 146. STUDYOBJECTIVES 146.1 PRIMARYOBJECTIVE 146.2 SECONDARYOBJECTIVES 157. STUDYDESIGN 157.1 STUDYPOPULATION 157.1.1 SUBJECTPOPULATION 157.1.2 INCLUSIONCRITERIA 157.1.3 EXCLUSIONCRITERIA 157.1.4 STUDYDURATION 167.1.5 WITHDRAWALANDREPLACEMENTOFSUBJECTS 167.1.6 PREMATURETERMINATIONOFTHESTUDY 178. METHODOLOGY 178.1 STUDYMEDICATION 178.1.1 DOSAGEANDADMINISTRATION 188.1.2 STUDY-DRUGUP-ANDDOWNTITRATION 188.1.3 STUDYDRUGINTERRUPTIONORDISCONTINUATION 188.1.4 STUDYDRUGPREMATUREPERMANENTDISCONTINUATION 188.1.5 STUDY-DRUGDELIVERY&DRUGSTORAGECONDITIONS 198.1.6 STUDYDRUGPACKAGINGANDLABELING 198.1.7 IMPADMINISTRATION&HANDLING 198.1.8 DRUGACCOUNTABILITY 198.1.9 PROCEDURESTOASSESSSUBJECTSCOMPLIANCE 198.1.10 CONCOMITANTMEDICATION 208.2 RANDOMIZATIONANDSTRATIFICATION 208.3 BLINDING 208.3.1 EMERGENCYPROCEDUREFORUNBLINDING 218.3.2 UNBLINDINGATTHEENDOFTHESTUDY. 218.4 BENEFITANDRISKASSESSMENT 218.5 STUDYPROCEDURES 218.5.1 GENERALRULESFORTRIALPROCEDURES 218.5.2 SCREENINGINVESTIGATION 228.5.3 END-OF-STUDY(EOS)EXAMINATION 228.5.4 LABORATORYTESTS 229. SAFETYDEFINITIONSANDREPORTINGREQUIREMENTS 249.1 ADVERSEEVENTS(AES) 24
PreventingCholestasisinPrematureInfantsUsingSMOFLipid®/SMOFLipid®MedicalUniversityofVienna,DepartmentofPediatricsEUDRACTNr2011-005456-33
Date22.8.2013 Version1.3 Page9of38
9.1.1 SUMMARYOFKNOWNANDPOTENTIALRISKSOFTHESTUDYDRUG 249.1.2 DEFINITIONOFADVERSEEVENTS 259.2 SERIOUSADVERSEEVENTS(SAES) 269.2.1 HOSPITALIZATION–PROLONGATIONOFEXISTINGHOSPITALIZATION 269.2.2 SAESRELATEDTOSTUDY-MANDATEDPROCEDURES 279.2.3 SUSPECTEDUNEXPECTEDSERIOUSADVERSEREACTIONS(SUSARS) 279.3 SEVERITYOFADVERSEEVENTS 279.4 RELATIONSHIPTOSTUDYDRUG 289.5 REPORTINGPROCEDURES 299.5.1 REPORTINGPROCEDURESFORSAES 299.5.2 REPORTINGPROCEDURESFORSUSARS 299.5.3 ANNUALSAFETYREPORT 3010. FOLLOW-UP 3010.1 FOLLOW-UPOFSTUDYPARTICIPANTSINCLUDINGFOLLOW-UPOFADVERSEVENTS 3010.2 TREATMENTAFTERENDOFSTUDY 3011. STATISTICALMETHODOLOGYANDANALYSIS 3011.1 ANALYSISSETS 3011.2 SAMPLESIZECONSIDERATIONS 3111.3 RELEVANTPROTOCOLDEVIATIONS 3111.4 STATISTICALANALYSISPLAN 3111.5 MISSING,UNUSEDANDSPURIOUSDATA 3111.6 ENDPOINTSANALYSIS 3211.6.1 PRIMARYENDPOINTANALYSIS 3211.6.2 SECONDARYENDPOINTANALYSIS 3211.6.3 SAFETYANDTOLERABILITYENDPOINTS 3211.6.4 BASELINEPARAMETERSANDCONCOMITANTMEDICATIONS 3211.7 INTERIMANALYSIS 3311.8 SOFTWAREPROGRAM(S) 3312. DOCUMENTATIONANDDATAMANAGEMENT 3312.1 DOCUMENTATIONOFSTUDYRESULTS 3312.1.1 CASEREPORTFORM(CRF) 3312.1.2 DATACOLLECTION 3312.2 SAFEKEEPING 3312.3 QUALITYCONTROLANDQUALITYASSURANCE 3412.3.1 PERIODICMONITORING 3412.3.2 AUDITANDINSPECTIONS 3512.4 REPORTINGANDPUBLICATION 3512.4.1 PUBLICATIONOFSTUDYRESULTS 3513. ETHICALANDLEGALASPECTS 3513.1 INFORMEDCONSENTOFSUBJECTS 3513.2 ACKNOWLEDGEMENT/APPROVALOFTHESTUDY 3513.2.1 CHANGESINTHECONDUCTOFTHESTUDY 3613.3 INSURANCE 3613.4 CONFIDENTIALITY 3613.5 ETHICSANDGOODCLINICALPRACTICE(GCP) 3714. APPENDICES 3715. REFERENCES 37
PreventingCholestasisinPrematureInfantsUsingSMOFLipid®/SMOFLipid®MedicalUniversityofVienna,DepartmentofPediatricsEUDRACTNr2011-005456-33
Date22.8.2013 Version1.3 Page10of38
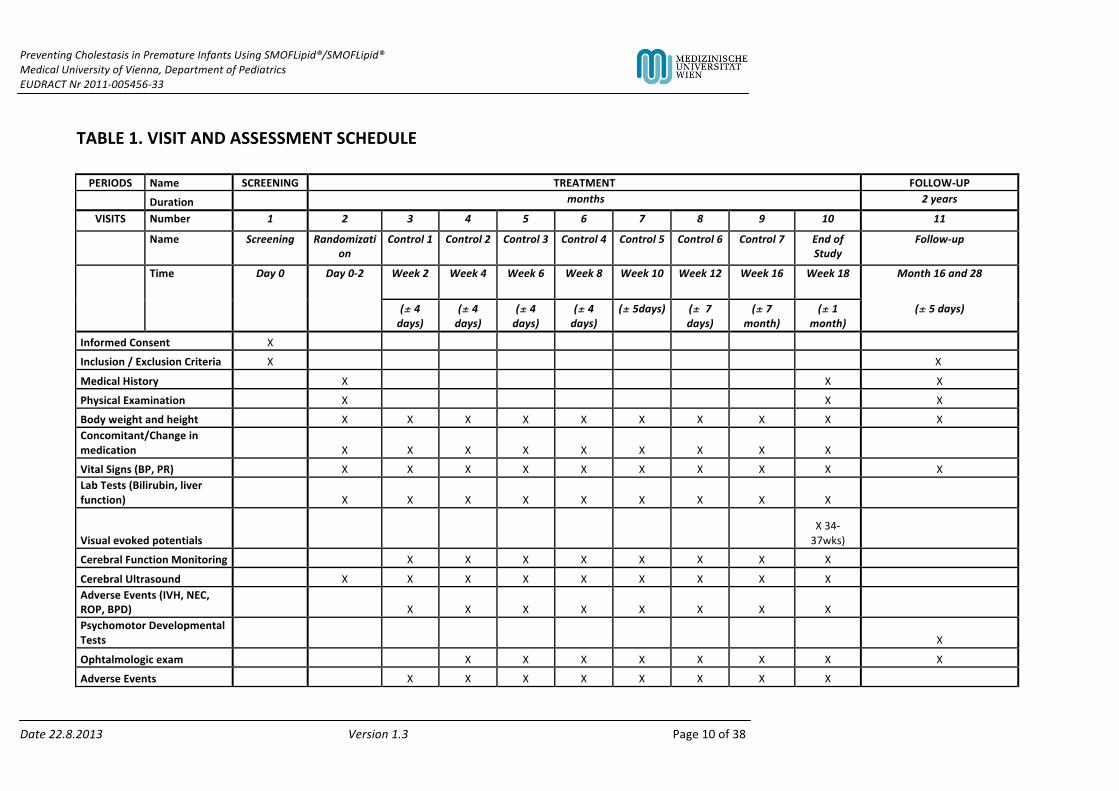
TABLE1.VISITANDASSESSMENTSCHEDULE
PERIODS Name SCREENING TREATMENT FOLLOW-UP
Duration months 2years
VISITS Number 1 2 3 4 5 6 7 8 9 10 11
Name Screening Randomization
Control1 Control2 Control3 Control4 Control5 Control6 Control7 EndofStudy
Follow-up
Time Day0 Day0-2 Week2 Week4 Week6 Week8 Week10 Week12 Week16 Week18 Month16and28
(± 4days)
(± 4days)
(± 4days)
(± 4days)
(± 5days) (± 7days)
(± 7month)
(± 1month)
(± 5days)
InformedConsent X
Inclusion/ExclusionCriteria X X
MedicalHistory X X X
PhysicalExamination X X X
Bodyweightandheight X X X X X X X X X XConcomitant/Changeinmedication X X X X X X X X X
VitalSigns(BP,PR) X X X X X X X X X XLabTests(Bilirubin,liverfunction) X X X X X X X X X
Visualevokedpotentials X34-37wks)
CerebralFunctionMonitoring X X X X X X X X
CerebralUltrasound X X X X X X X X X AdverseEvents(IVH,NEC,ROP,BPD) X X X X X X X X PsychomotorDevelopmentalTests X
Ophtalmologicexam X X X X X X X X
AdverseEvents X X X X X X X X
PreventingCholestasisinPrematureInfantsUsingSMOFLipid®/SMOFLipid®MedicalUniversityofVienna,DepartmentofPediatricsEUDRACTNr2011-005456-33
Date22.8.2013 Version1.3 Page11of38
5. BACKGROUNDINFORMATION
5.1 Background5.1.1Parenteralnutritionassociatedcholestasis(PNAC)
Sincethefirstdescriptionofparenteralnutritionassociatedliverdisease1itiswellestablishedthat
patientsreceivingparenteralnutrition(PN)areatriskfordevelopinghepaticcomplications.In
neonatesandinfants,liverinjuryischaracterizedbyanearlyoccurrenceofintrahepaticcholestasis-
i.e.parenteralnutritionassociatedcholestasis(PNAC)-characterizedbyariseinserumconjugated
bilirubin2.Inseverecaseslivercelldamageandevenprogressiveliverdysfunctionwithanincidence
ofhepaticfailureofupto17%isdescribed3.
5.1.2.Extremelowbirthweightinfants
Preterminfantswithextremelowbirthweight(ELBW)<1000gramareoftendependentonlong
termPNduetointoleranceofenteralfeedings4.Additionallytheyfrequentlyacquirenosocomial
infectionsandareatriskfordevelopingnecrotizingenterocolitis,asevereinflammatorydiseaseof
theintestinewithconsiderablelongtermmorbiditysuchasshortgutsyndrome.Prematurity,long
termPN,nosocomialinfections,necrotizingenterocolitisandshortgutsyndromeareallarerisk
factorsforthedevelopmentofPNAC.ThereforeELBWinfantsareathighrisktodevelopthis
complication2.
5.1.3.ParenterallipidsaspathogenicfactorinPNAC
Besidesfactorsrelatedtoprematurityanditscomplicationsorshortgutsyndrome,PNACis-as
alreadyproposedbythecondition’sname-closelylinkedtoaspectsofPN.Hypercaloricfeedswith
anexcessofglucosecanresultinchroniccholestasis5.Mostimportanthowever,intravenouslipid
emulsions(ILE)seemtobeimplicatedinthedevelopmentofPNAC.Higherparenterallipid
administrationhasbeendocumentedtobecorrelatedwithcholestasisinpediatricpatients6aswell
asverylowbirthweightinfants7.
5.1.4.Soybeanoilbasedintravenouslipidemulsions
Untilnowadays,standardofcareforsupplyinglipidsinPNofpreterminfantsandsickneonatesare
ILEbasedonsoybeanoil(Intralipid®)2.Someofthecomponentsofsoybeanoilarebelievedtobe
implicatedinthepathogenesisofPNAC.Theirhighcontentofω-6polyunsaturatedlongchainfatty

PreventingCholestasisinPrematureInfantsUsingSMOFLipid®/SMOFLipid®MedicalUniversityofVienna,DepartmentofPediatricsEUDRACTNr2011-005456-33
Date22.8.2013 Version1.3 Page12of38
acidsmayexertpro-inflammatoryeffectsandplantsterolsfromsoymayreducebileflowandboth
factorswerelinkedtothedevelopmentofPNAC8.
5.1.5.Fishoilbasedintravenouslipidemulsions
Inrecentyears,ILEscontainingfishoilwereproposedfortreatmentofPNACinpediatricpatients
mainlysufferingfromshortgutsyndrome.Tworesearchgroupsconsecutivelydescribedthe
successfultreatmentofseverePNACinneonatesusingOmegaven®9,10anILEcomposedexclusively
offishoil.Therationalebehindthepositiveeffectsobservedisbuiltontheirhighcontentofω-3
fattyacidswhichactanti-inflammatoryandarethoughttoimprovebileflow11.However,whether
fishoiloronlyreplacementofsoybeanoilbasedILEinPN6causedtheimprovementinthese
patients,cannotbeconcluded.Prospectivetrialsarerequiredtosubstantiatetheevidence8.
5.1.6.PreventingPNACinELBWinfants
InviewoftheirhighrisktodevelopPNAC,ELBWinfantscouldprofitfromaprophylactic
intervention.BasedonthepromisingresultsinthetreatmentofPNAC,ILEsbasedonfishoilseem
attractivecandidates.However,anILEbasedon100%fishoillikeOmegaven®maydelivernot
enoughω-6fattyacidsandthereforecannotbeusedastheexclusiveILEsfornutritionofELBW
infants8.
WithabroaderpanelofILEsavailabletoday,amixtureoffishoilwithsoybeanoil,mediumchain
triglyceridesandoliveoil(SMOFlipid®)hasrecentlyemerged.Aprospectivestudyinatotalof60
preterminfantsshowedthatPNwithSMOFlipid®inducedlowerserumγ-glutamyltransferaselevels
comparedtocontrolsreceivingasoybeanoilbasedILE,suggestingafavourableinfluenceon
cholestasisandliverfunction12.Aprospectiverandomizedtrialin28pediatricpatientsdemonstrated
areductionintotalbilirubinlevelsusingSMOFlipd®comparedtoasoybeanoilbasedILE13.
ImportantlySMOFlipid®isregisteredforPNofpreterminfants,whichmakesadirectcomparisonof
Intralipid®andSMOFlipid®inthesevulnerablepatientsethicallyacceptable14.
5.1.7.Fishoilandneurocognitivedevelopment
LongChainpolyunsaturatedfattyacids(LC-PUFA)arebothstructuralandfunctionallipidsplayingan
importantroleingrowthanddevelopmentofthefetusandthenewborn.Inparticularthe22:6ω3-
LC-PUFAdocosahexaenoicacid(DHA)isdeemedtobecrucialforanormaldevelopmentofthefetal
brain.Inutero,highamountsofDHAcrosstheplacentainthelasttrimester.Afterbirthmother’s
milkisthemostimportantsource15.
Preterminfants–astheirendogenouscapacitytosynthesizeDHAfromprecursorfattyacidsis
limited–dependonexogenoussupply16.Inthiscontext,preterminfantsaccumulateadeficitofup

PreventingCholestasisinPrematureInfantsUsingSMOFLipid®/SMOFLipid®MedicalUniversityofVienna,DepartmentofPediatricsEUDRACTNr2011-005456-33
Date22.8.2013 Version1.3 Page13of38
to44%comparedtoinuteroaccretionrates16.InviewofthedocumentedcorrelationofDHAdeficit
andlowbirthweight16ELBWinfantsareatparticularrisk,astheydependPNforseveralweeksand
DHAisabsentinthetraditionalsoybeanoilbasedILEs.AstheonlysourceofDHAforthepreterm
infantismother’smilkorpretermformuaandnotILEs,theprolongedtimeuntilfullenteralfeedsare
establishedinthesepatientsseemsparticularlycritical.
ThereforeanILElikeSMOFlipid®containgfishoilthatprovidesDHAwouldreducethisdeficitand
maythereforeconferpotentialbenefitsfortheneurocognitivedevelopment.
5.1.8.CurrentStatusofresearchonfishoilandparenteralnutritionassociatedcholestasisin
preterminfants
TherearecurrentlynostudiespublishedonafishoilcontainingILEforprophylaxisofPNAC.
ThereisgrowingsupportiveevidencefortreatmentofestablishedPNACusingILEbasedonfishoilin
pediatricpatientsfromtwoobservationalandoneprospectiveclinicaltrial,buttherearenodata
frompreterminfants.
ThegrowingbeliefinatherapeuticeffectoffishoilcontainingILEsonPNACisbasedonthe
publishedexperienceofcliniciansfromBostonaroundMarkPuder11andTorontoaroundPaulWales9.TheybothdescribedneonateswithsevereshortgutsyndromeandPNACthatdramatically
improvedafterreplacingsomeofthe100%soybeanoilbasedILE“Intralipid®”witha100%fish-oil
basedILE(Omegaven®)(Toronto)orcompletelyswitchingovertoafishoilbasedILE(Boston).The
Bostongroupreportedaresolutionofcholestasisin45-61%(publishedcases:60)10,17.TheToronto
groupreportedarateofresolutionof63%(publishedcases:22)18.Poolingthesecasestogether,a
meanof53.6%(44/82)ofpatientsshowedreversalofcholestasis.Forcomparison,historicalcohorts
ofcomparablepatientswhoreceivedthesoybeanoilbasedIntralipid®forPN,showedresolutionof
cholestasisonlyin5-33%duringthediseasecourse(publishedcases:47)10,17.
TheonlyprospectivetrialusingamixedILEcontaningfishoil(SMOFlipid®)inpediatricpatients
reportedasignificantreductionoftotalbilirubinlevelscomparedwiththesoybeanoilbasedILE
Intralipid®13.
TheonlyprospectivestudyperformedinapopulationofpreterminfantswasperformedbyTomsits
etal12.Inhealthypreterminfants(birthweights1000–2500gramm)theydemonstratedgood
clinicaltoleranceandlowerγ-glutamyltransferaselevelsusingSMOFlipid®comparedtostandard
carewithIntralipid®.Thoughliverfunctionwasonlyasecondaryoutcomeparameterofthestudy
andtheobservationalperiodwastooshorttoassessanyeffectonPNAC,thisfindingsupportsa
prophylacticeffectofSMOFlipid®onliverfunction,underliningtheneedforfurtherinvestigations.
5.1.9.CurrentStatusofresearchonfishoilandneurodevelopmentofpreterminfants
PreventingCholestasisinPrematureInfantsUsingSMOFLipid®/SMOFLipid®MedicalUniversityofVienna,DepartmentofPediatricsEUDRACTNr2011-005456-33
Date22.8.2013 Version1.3 Page14of38
Therearecurrentlynostudiesonlongtermneurodevelopmentofpreterm–inparticularELBW-
infantsafterusingafishoilcontainingILE.
ThereareprospectivetrialsonenteralsupplementationwithLC-PUFAcontainingDHAfromfishoilin
preterminfantsandduringpregnancywithmixedresults15,19.
ClinicalstudiesinpreterminfantsfocusedonenteralsupplementationofLC-PUFAs(includingDHA)
fromfishoilinformulafeedings.Inthiscontext,aCochraneReviewin2008bySimmeret.al19
concludedthatcurrentlythereisnoconvincingevidenceofasustainedimprovementof
neurodevelopmentbyLC-PUFAsupplementation.However,asthemeanbirthweightofpreterm
infantsenrolledinthesestudieswasconsistently>1000gram(1074–1980)theauthorsstressed
thatELBWinfantsshouldbeinvestigated19.Inthiscontext,thereisindirectevidencefromtwo
prospectiverandomizedtrials,thatsupplementationofpregnantwomenwithfishoilconvertsa
beneficialeffectonlaterneurodevelopmentoftheirchildren15.Inlinewiththeevidencefromthese
trials,usinganILEcontainingfishoilforparenteralnutritionofELBWinfantscouldclosethegapuntil
ELBWinfantsarefullynourishedwithmother’smilkorformula(supplementedwithLC-PUFA).A
reductionoftheDHAdeficittheseinfantsnormallyaccumulate16mayconferabenefitto
neurodevelopment.
5.2 StudyrationalePrimaryendpoint:
ELBWinfantsareathighriskfordevelopmentofparenteralnutritionassociatedcholestasis(PNAC).
Thereisgrowingevidenceforapositiveeffectoffishoilbasedintravenouslipidemulsions(ILE)for
thetreatmentofPNAC.PrimaryuseofafishoilcontainingILEforPNmaypreventthedevelopment
ofPNAC.
SecondaryEndpoint:
ELBWinfantsaccumulateadeficitofω3-LC-PUFA(especiallyDHA),whichareimportantfor
neurodevelopment.AnILEcontainingfishoilprovidesthesefattyacidsandwouldreducethedeficit
inELBWinfants,whichmayimprovetheirneurocognitivedevelopment.
6. STUDYOBJECTIVES
6.1 PrimaryObjective

PreventingCholestasisinPrematureInfantsUsingSMOFLipid®/SMOFLipid®MedicalUniversityofVienna,DepartmentofPediatricsEUDRACTNr2011-005456-33
Date22.8.2013 Version1.3 Page15of38
ToinvestigatewhetherELBWinfantstreatedwithtwodifferentILEs(investigationaldrug:
SMOFlipid®,comparativedrug:Intralipid®)differintheoccurrenceofPNAC(conjugatedbilirubin>
1.5mg/dl,measuredontwoconsecutiveoccasions).
6.2 SecondaryObjectives
ToinvestigatewhetherELBWinfantstreatedwithtwodifferentILEs(investigationaldrug:
SMOFlipid®,comparativedrug:Intralipid®)differintheirneurodevelopment(BaileyScalesofInfant
DevelopmentIII)at12and24monthsofcorrectedgestationalage
7. STUDYDESIGN
7.1 Studypopulation
7.1.1 SubjectpopulationPopulation:Extremelowbirthweight(ELBW)infants
Recruitment:About90ELBWinfantsareadmittedtoouruniteachyearinthefirst24hoursoflife.
Weexpecttorecruit90%(81patients/ayear)tothestudy.
DropOuts:Basedonamortalityof22%in2010(KlebermaszK.,unpublisheddata)andaconservative
calculation,weexpect18/81patientstodropout,leaving63patientsayearforanalysisofthe
primaryoutcome.Wedonotexpectanyotherreasonsfordropout.
Lossestofollowup:63patientsareexpectedtobedischargedfromhospitaleachyear.Basedona
followuprateof60%afterdischargein2009(FuikoR,unpublisheddata),weexpectabout38/63
patientstobeavailableforanaylsisofthesecondaryoutcomeeachyear.Intheendweexpectto
lose80/200patientstofollowup.
7.1.2 Inclusioncriteria-Infantswithabirthweight≤1000Gram
-Admissiontotheneonatalwardinthefirst24hoursoflife
-Randomizationontherespectivestudydruginthefirst5daysoflife
7.1.3 Exclusioncriteria
Tripletsorhigher
Conjugatedbilirubin>1.5mg/dlbeforeinclusiontothestudy
Conditionsassociatedwithcholestasisindependentofparenteralnutrition:

PreventingCholestasisinPrematureInfantsUsingSMOFLipid®/SMOFLipid®MedicalUniversityofVienna,DepartmentofPediatricsEUDRACTNr2011-005456-33
Date22.8.2013 Version1.3 Page16of38
-Inbornerrorsofmetabolism
-ViralInfections(cytomegalyvirus,HIV,HepatitisB,C)
-Immunemediatedhemolyticdiesease(e.g.Rhesusincompatibility)
-Diagnosisofcysticfibrosis
-Primarycholestaticdiseasesoftheliver
Atfollowup:
-Congenitalneurologicalmalformationsandpatientswithchromosomalaberrationswillbe
excludedfromfollowupanalysis(exceptscreeningforadverseevents)
7.1.4 Studyduration
Theinterventionalphasestartswithrandomizationonthestudydruginthefirst5daysoflifeand
endswithdiscontinuationofPN,typicallyafter6weeks(mean44days+/-SD34days,personal
data).
Thefollowupphaseendsat24months(2years)ofcorrectedgestationalage.
7.1.5 WithdrawalandreplacementofsubjectsCriteriaforwithdrawalPrematurediscontinuationfromthestudyistobeunderstoodwhenthesubjectdidnotundergoEndofStudy(EOS)examinationand/orallpivotalassessmentsduringthestudy.Subjectsmustbewithdrawnunderthefollowingcircumstances:
• attheirparent´srequestatanytime• iftheinvestigatorfeelsitwouldnotbeinthebestinterestofthesubjecttocontinue• ifthesubjectviolatesconditionslaidoutintheconsentform/informationsheetor
disregardsinstructionsbythestudypersonal• ifthesubjectistransferredtoanotherhospitalbeforeparenteralnutritionisdiscontinued• ifthestudydrugwasnotprovided<80%oftimeasplanedperprotocol• Ifanexclusioncriterionismet,afterinclusiontothestudy(exceptneurologicalmalformation
andchromosomalaberrationwhichonlyleadstowithdrawalfromfollowupanalysisexceptscreeningforadverseevents)
• deathbeforedayoflife28
Inallcases,thereasonwhysubjectsarewithdrawnmustberecordedindetailintheCRFandinthesubject’smedicalrecords.Shouldthestudybediscontinuedprematurely,allstudymaterials(complete,partiallycompletedandemptyCRFs)willberetained.
PreventingCholestasisinPrematureInfantsUsingSMOFLipid®/SMOFLipid®MedicalUniversityofVienna,DepartmentofPediatricsEUDRACTNr2011-005456-33
Date22.8.2013 Version1.3 Page17of38
Follow-upofpatientswithdrawnfromthestudyIncaseofprematurediscontinuationafterstudydrugintake,theinvestigationsscheduledfortheEOSvisitwillbeperformed7+/-4daysafterstudydrugdiscontinuation.Thesubjectswillbeadvisedthatparticipationintheseinvestigationsisvoluntary.Furthermore,theymayrequestthatfromthetimepointofwithdrawalnomoredatawillberecordedandthatallbiologicalsamplescollectedinthecourseofthestudywillbedestroyed.ReplacementpolicyPatientswithdrawnfromthestudy<28days(outcomecannotbecalculated)willbereplacedandthenextfreesubjectnumberwillbeallocated.Dropsoutswillbeincludedinthesamplesize.Ifpatientsarewithdrawnfromthestudyandtheoutcomecanbecalculated,(morethantwobloodsamplestaken),theywillbeconsideredintheintentiontotreatanalysis(seechapter10)
7.1.6 PrematureterminationofthestudyThesponsorhastherighttoclosethisstudyatanytime.TheIECandthecompetentregulatoryauthoritymustbeinformedwithin15daysofearlytermination.Thetrialorsingledosestepswillbeterminatedprematurelyinthefollowingcases:
• Ifadverseeventsoccurwhicharesoseriousthattherisk-benefitratioisnotacceptable.• Ifthenumberofdropoutsissohighthatpropercompletionofthetrialcannotrealisticallybe
expected.
8. METHODOLOGY
8.1 StudymedicationActiveagentandcharacteristics:InvestigationalProductTradenameoftheagent: SMOFlipid200mg/mlEmulsionzurInfusionManufacturer: FreseniusKabiAustriaGmbHDrugsupply: FreseniusKabiAustriaGmbHStorageInstructions: Donotfreeze,donotstore>25°Celsius,protectfromlightRouteofadministration: IntravenousComparatorTradenameoftheagent: Intralipid20%-EmulsionzurInfusionManufacturer: FreseniusKabiAustriaGmbHDrugsupply: FreseniusKabiAustriaGmbHStorageInstructions: Donotfreeze,donotstore>25°Celsius,protectfromlightRouteofadministration: Intravenous
PreventingCholestasisinPrematureInfantsUsingSMOFLipid®/SMOFLipid®MedicalUniversityofVienna,DepartmentofPediatricsEUDRACTNr2011-005456-33
Date22.8.2013 Version1.3 Page18of38
8.1.1 DosageandadministrationInitialdose: 1g/kg/d(=5ml/kg/d)Maintenancedose: 3g/kg/d(=15ml/kg/d)Routeofadministration: IntravenousDuration: Aslongasparenteralnutritionisneeded
8.1.2 Study-drugup-anddowntitrationAccordingtoastepwiseincreaseorreductionofenteralfeedingsaproportionalincreaseorreductionofparenteralnutritionwillperformedincludingareductionofthestudydrug/comparator.Thestudydrug/comparatorwillbefinishedassoonasfullenteralfeedsarereachedandPNisstopped(at140-160ml/kg/doftotalfluidvolumedependingonthefluidneedsoftheinfant).
8.1.3 StudydruginterruptionordiscontinuationTheinvestigatormusttemporarilyinterruptorpermanentlydiscontinuethestudydrugifcontinuedadministrationofthestudydrugisbelievedtobecontrarytothebestinterestsofthepatient.TheinterruptionorprematurediscontinuationofstudydrugmightbetriggeredbyanAE,adiagnosticortherapeuticprocedure,anabnormalassessment(e.g.,laboratoryabnormalities),orforadministrativereasons,inparticularwithdrawalofthepatient’sconsent.Hypertriglceridemia:Thestudydrugwillbeinterruptedfor24hoursattriglyeridelevels>400mg/dlordowntitratedattriglyceridelevelsof251-400mg/dl.Controlmeasurementsoftriglycridelevelswillbeperformedinthenext24-72hourstocontrolforsuccessfulnormalizationoftriglyceridelevelsunderparenteralnutrition.ThereasonforstudydruginterruptionorprematurepermanentdiscontinuationmustbedocumentedintheCRF.
8.1.4 StudydrugprematurepermanentdiscontinuationStudydrugprematurepermanentdiscontinuationduetoanadverseeventIfthereasonforprematurepermanentdiscontinuationofstudytreatmentisanAE,thepatientshouldhavea“PrematureEndofStudy(EOS)”visitwithalltheassessmentsperformedbeforethestudydrugdiscontinuation,wheneverpossible.StudydrugprematurepermanentdiscontinuationduetoanotherreasonthanadverseeventIfthereasonforprematurepermanentdiscontinuationofstudytreatmentisnotanAE,thepatientshouldbewithdrawnfromthestudy(withdrawalofconsent)andhavetheendofstudy(EOS)visitwithalltheassessmentsperformedbeforethestudydrugdiscontinuation,wheneverpossible.
PreventingCholestasisinPrematureInfantsUsingSMOFLipid®/SMOFLipid®MedicalUniversityofVienna,DepartmentofPediatricsEUDRACTNr2011-005456-33
Date22.8.2013 Version1.3 Page19of38
8.1.5 Study-drugdelivery&drugstorageconditionsThestudydrugwillbedeliveredfromthesupplyingcompanytotheinvestigatorsandstoredatroomtemperatureundercontrolledconditions(22°C+/-3°C)inalockedroom.Amin/maxthermometerwillbeusedtocontrolfortemperatureinthestorageroom.Fulldocumentationofdelivery,storageanddispositionwillbemaintained.
8.1.6 StudydrugpackagingandlabelingThestudydrugsaredeliveredinsterileglasscontaninersof100mlbythemanufacturerandwillbere-labelledatthestudysiteasdescribedinsection8.3.Storageisdescribedinsection8.1.5.Forapplicationtostudysubjects,thestudydrugswillbebroughttotheneonatalwardsbyamemberoftheblinidingteam.ForIVapplication,thestudydrugswillbetransferredfromthere-labelledcommercialcontainerstoperfusorsyringesconnectedtoperfuorslinessuitableforIVapplication.Perfusorsyringeswillbelabelled(seesamplelabels1and2below).PreparationforIVapplicationwillbedoneinalaminarairhoodundersterileconditionsbytrainedintensivecarenurses,formingpartoftheblindingteam.SampleLabelNumber1 SampleLabelNumber2
8.1.7 IMPadministration&handlingTheIMPorcomparatormustnotbefrozenorstored>25°C,applicationisperformedinlightprotectedperfusorsyringesandperfusorlines.ApplicationmaybeperformedIVviacentralandperipheralvenouscatheters.TheIMPorcomparatormustnotbemixedwithanyotherdrugbesidesthecommerciallyavailablevitaminsolutions“SoluvitN”and“Vitalipid”(FreseniusKabiAustriaGmbH).
8.1.8 DrugAccountabilityDrugAccountabilitywillberecordedaton-goingbasisonpaperform/sourcedata,DrugdispensinghavetobeenteredintotheCRF.FurthermorethecorrectintakeofIMPoranyvariationsconcerningthatwillberecordedintheCRFateachvisitduringtreatmentperiod
8.1.9 Procedurestoassesssubjectscompliance
PreventingCholestasisinPrematureInfantsUsingSMOFLipid®/SMOFLipid®MedicalUniversityofVienna,DepartmentofPediatricsEUDRACTNr2011-005456-33
Date22.8.2013 Version1.3 Page20of38
WhethertheIMPorcomparatorwhereadministeredcorrectlywillbefollowedfromthedocumentationintheelectronicpatientdocumentarysystemusedattheneonatalICU.
8.1.10 ConcomitantmedicationThewell-beingofthepatienthasthefirstpriority,andmodificationsofconcomitanttreatmentduringthetrialareallowedasnecessary.Theyshouldbedocumentedinthepatient’srecords.Incaseofofcholestasis(i.e.conjugatedbilirubintwotimes>1.5mg/dl),
Ursodeoxycolicacidat20-30mg/kg/dayisthetreatmentofchoice. Omegaven®isallowedasasaddonat1g/kg/d,ifconj.bilirubin>6mg/dl,
8.2 RandomizationandstratificationOnday0,patientsarerandomizedtooneofthetwostudygroupsandthestudymedicationisprovided.Studysubjectswillbeblockrandomized(ratio1:1)andstratifiedaccordingtosexandbirthweight(intwogroups:<750gramvs.≥750gram)usinganonlinerandomizationprogrammeprovidedbytheCenterforMedicalStatistics,Informatics,andIntelligentSystemsoftheMedicalUniversityofVienna.Incaseoftwins,randomizationwillbeappliedtothefirstborn;thetwinwillbeassignedtotheothertreatmentgroup.
8.3 BlindingBlindingofsubjects,investigatorsandoutcomeassessorswillbeperformedasfollows:Firstre-labellingofthestudydrugcontainers(seesamplelabel1and2below)willbeperformedbytwomembersoftheblindingteamnotinvolvedinthecollectionofdata,treatmentofstudysubjectsorpreparationofthestudydrugsforIVapplication.Thestudydrugsarekeptinglasscontainersof100mlandwillbere-labelledwithsamplesasindicated(seesamplelabel1and2below)andstoredasdescribed(section8.1.5).Second,fordeliverytostudysubjectsthestudydrugswillbebroughttothewardsbyamemberoftheblindingteam,wherethepreparationforIVapplicationwillbedoneinalaminarairhoodbyamemberoftheblindingteamasdescribedinsection8.1.7.Asintensivecarenursesinvolvedincaretakingofthepatientsformpartoftheblidingteam,nursingcaregiversarenotblinded.MedicaldoctorsprescribingthedailyamountsoftheIMPremainblinded.SampleLabelNumber1 SampleLabelNumber2:
PreventingCholestasisinPrematureInfantsUsingSMOFLipid®/SMOFLipid®MedicalUniversityofVienna,DepartmentofPediatricsEUDRACTNr2011-005456-33
Date22.8.2013 Version1.3 Page21of38
8.3.1 EmergencyprocedureforunblindingIfunblindingofastudyparticipantisrequiredduetoanemergency,thecodecanbebrokenbytheInvestigator.Codebreakingwillbefullydocumented.
8.3.2 Unblindingattheendofthestudy.Codeswillbebrokenafterdataanalysisoftheprimaryoutcome,thisisafterthelastpatienthasfinishedactivephase.Investigatorsinvolvedinasessmentofdatainthefollowupphase(secondaryoutcomeneurodevelopment)willremainblinded.
8.4 Benefitandriskassessment
8.4.1Benefitforthepatient
Ifthehypothesisiscorrect,participatingpatientsreceivingthestudymedicationwillbenefitfroma
reducedriskofdevelopingliverinjuryduetolongtermparenteralnutrition.Theywillbenefitfroma
improvedlongtermneurodevelopment.
8.4.2Riskforthepatient
Thedrugunderinvestigationfulfilledthecriteriaforregistrationforapplicationinpreterminfants.
Therefore,riskforpatientsreceivingthestudydrugshouldnotbehighercomparedtostandardcare.
Intheworstcaseweexpectthattherewillbenobenefit.
8.5 Studyprocedures
8.5.1 Generalrulesfortrialprocedures
• Allstudymeasureslikebloodsamplingandmeasurements(ultrasoundetc.)havetobedocumentedwithdate(dd:mmm:yyyy).
• Incaseseveralstudyproceduresarescheduledatthesametimepoint,thereisnospecificsequencethatshouldbefollowed.
• Thedatesofallproceduresshouldbeaccordingtotheprotocol.Thetimemarginsmentionedinthestudyflowchartareadmissible.Ifforanyreason,astudyprocedureisnotperformedwithinscheduledmarginsaprotocoldeviationshouldbenoted,andtheprocedureshouldbeperformedassoonaspossibleorasadequate.
• Ifitisnecessaryfororganizationalreasons,itisadmissibletoperformprocedureswhicharescheduledforonevisitattwodifferenttimepoints.Allowedtimemarginsshouldtherebynotbeexceeded.

PreventingCholestasisinPrematureInfantsUsingSMOFLipid®/SMOFLipid®MedicalUniversityofVienna,DepartmentofPediatricsEUDRACTNr2011-005456-33
Date22.8.2013 Version1.3 Page22of38
8.5.2 ScreeninginvestigationAtscreening,thepatient´sdemographicdataandlabresults(seeSection7.1.2and7.1.3Inclusion
andExclusionCriteria)willbeevaluatedforeligibilitytothestudy.
8.5.3 End-of-study(EOS)examinationAtdischargeofthepatientfromhospital,patientsundergotheend-of-studyexaminationthatentails
Weight,crownheellength,headcircumferenceandabasicbloodtest(redandwhitebloodcount,
liverfunctiontests,electrolytes)performedinclinicalroutineinallELBWinfants.
8.5.4 LaboratoryTestsBloodcountsandcompletebloodchemistryisroutinelyperperformedaccordingtothelocal
standardofcareattheunitatleastevery10+/-4daysuntildischargefromhospital.Noadditional
bloodsamplingoranalyseswillbeperformedinstudysubjectsincomparisontostandardofcareof
ELBWinfants.
Alllaboratoryparametersofinterestforthestudyroutinelyperformedare:
denomination Variable timeofmeasurement
Conjugatedbilirubin mg/dL every7-14duntildischarge
ALAT U/L every7-14duntildischarge
ASAT U/L every7-14duntildischarge
γ-glutamyltransferase U/L every7-14duntildischarge
Alkalinephosphatase U/L every7-14duntildischarge
Triglycerides mg/dL every7-14duntildischarge
Additionalparametersusedforthestudy
Alladditionalparametersofinterestaredocumentedorproducedroutinelyduringthepatient’s
admissiontotheunitorfollow-upaccordingtothelocalstandardofcare.Noadditional
interventionswillneedtobeperformed.
denomination Variable timeofmeasurement
Basicdemographicdata
Sex m/f atbirth
Gestationalage days atbirth
Twin yes/no atbirth
Modeofdelivery caesarean/spontaneousatbirth

PreventingCholestasisinPrematureInfantsUsingSMOFLipid®/SMOFLipid®MedicalUniversityofVienna,DepartmentofPediatricsEUDRACTNr2011-005456-33
Date22.8.2013 Version1.3 Page23of38
Prenatalsteroidsforlungmaturation yes/no atbirth
Birthweight gram,ZScore atbirth
Birthcrownheellength cm,ZScore atbirth
Birthheadcircumference cm,ZScore atbirth
Smallforgestationalage yes/no atbirth
Apgarscoresat1,5and10minutes 0-10 atbirth
UmbilicalarterypHatbirth range6.7–7.6 atbirth
Growthandnutritionparameters
Timeonparenteralnutrition days atdischarge
Totalamountofparenterallipids gram atdischarge
Enteralnutritionin1stfirstweekoflife ml/day day0-6
Weightatdischarge gram,ZScore atdischargefromhospital
Crownheellengthatdischarge gram,ZScore atdischargefromhospital
Headcircumferenceatdischarge gram,ZScore atdischargefromhospi
Death>28days yes/no dayoflife28-discharge
(Deathbefore28days=dropout)
Ifdeath dayoflife dayoflife28-discharge
Neonatal(preterm)morbidities
IntraventricularhemorrhageGrad3/4 yes/no atdischarge
Cysticperiventricularleucomalacia yes/no atdischarge
Chroniclungdisease yes/no atdischarge
Receivedsteroidsforchroniclungdisease yes/no atdischarge
Treatmentforpulomanryhypertension yes/no atdischarge
(Sildenafil,iNO)
Cultureprovensepsis yes/no atdischarge
NecrotizingenterocolitisBell´sStage≥IIa yes/no atdischarge
Focalintestinalpeforation yes/no atdischarge
Abdominalsurgery yes/no atdischarge
IbuprofenforPDA yes/no atdischarge
SurgicalligationofPDA yes/no atdischarge
HighestROPGrade 0-5 atdischarge
ROPtreatedwithlaser yes/no atdischarge

PreventingCholestasisinPrematureInfantsUsingSMOFLipid®/SMOFLipid®MedicalUniversityofVienna,DepartmentofPediatricsEUDRACTNr2011-005456-33
Date22.8.2013 Version1.3 Page24of38
ROPtreatedwithantiVEGF yes/no atdischarge
Otherparameters
Lengthofhospitalstay days atdischarge
Ageatdischarge days atdischarge
Otherinvestigations
Cerebralfunctionmonitoring %continouospattern weekly
Visualevokedpotentials N2latencyinmsat34-37wksgestationalage
Assessmentofneurodevelopmentaloutcome
BaileyScalesofInfantDevelopmentIII metric(points) at12and24monthsof
Grossmotordevelopment 0-5points correctedgestationalage.
Opthalmologicexamsatfollowup
Visualfixation yes/no at12and24monthsof
Trackingmovements yes/no correctedgestationalage.
Strabism yes/no
Refractionmeasuredbyskiascopy metric(dioptres)
Binocularvisualization(LangStereotest) pos/neg at24monthsof
correctedgestationalage
9. SAFETYDEFINITIONSANDREPORTINGREQUIREMENTS
9.1 Adverseevents(AEs)
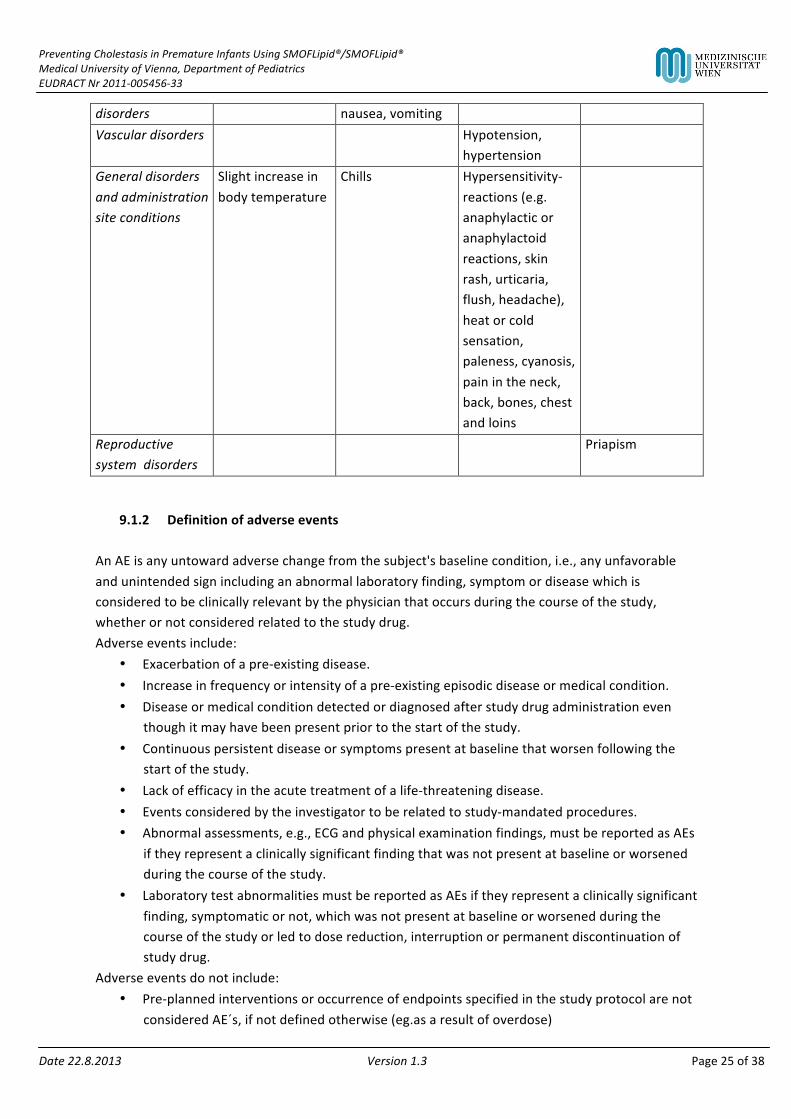
9.1.1 SummaryofknownandpotentialrisksofthestudydrugUndesirableeffectsobservedduringtheadministrationoffatemulsions:
Common(≥1/100to<1/10)
Uncommon(≥1/1000to<1/100)
Rare(≥1/10000to<1/1000)
Veryrare(<1/10000)
Respiratory,thoriacicandmediastinaldisorders
Dyspnoea
Gastrointestinal Lackofappetite,
PreventingCholestasisinPrematureInfantsUsingSMOFLipid®/SMOFLipid®MedicalUniversityofVienna,DepartmentofPediatricsEUDRACTNr2011-005456-33
Date22.8.2013 Version1.3 Page25of38
disorders nausea,vomitingVasculardisorders Hypotension,
hypertension
Generaldisordersandadministrationsiteconditions
Slightincreaseinbodytemperature
Chills Hypersensitivity-reactions(e.g.anaphylacticoranaphylactoidreactions,skinrash,urticaria,flush,headache),heatorcoldsensation,paleness,cyanosis,painintheneck,back,bones,chestandloins
Reproductivesystemdisorders
Priapism
9.1.2 DefinitionofadverseeventsAnAEisanyuntowardadversechangefromthesubject'sbaselinecondition,i.e.,anyunfavorableandunintendedsignincludinganabnormallaboratoryfinding,symptomordiseasewhichisconsideredtobeclinicallyrelevantbythephysicianthatoccursduringthecourseofthestudy,whetherornotconsideredrelatedtothestudydrug.Adverseeventsinclude:
• Exacerbationofapre-existingdisease.• Increaseinfrequencyorintensityofapre-existingepisodicdiseaseormedicalcondition.• Diseaseormedicalconditiondetectedordiagnosedafterstudydrugadministrationeven
thoughitmayhavebeenpresentpriortothestartofthestudy.• Continuouspersistentdiseaseorsymptomspresentatbaselinethatworsenfollowingthe
startofthestudy.• Lackofefficacyintheacutetreatmentofalife-threateningdisease.• Eventsconsideredbytheinvestigatortoberelatedtostudy-mandatedprocedures.• Abnormalassessments,e.g.,ECGandphysicalexaminationfindings,mustbereportedasAEs
iftheyrepresentaclinicallysignificantfindingthatwasnotpresentatbaselineorworsenedduringthecourseofthestudy.
• LaboratorytestabnormalitiesmustbereportedasAEsiftheyrepresentaclinicallysignificantfinding,symptomaticornot,whichwasnotpresentatbaselineorworsenedduringthecourseofthestudyorledtodosereduction,interruptionorpermanentdiscontinuationofstudydrug.
Adverseeventsdonotinclude:• Pre-plannedinterventionsoroccurrenceofendpointsspecifiedinthestudyprotocolarenot
consideredAE´s,ifnotdefinedotherwise(eg.asaresultofoverdose)
PreventingCholestasisinPrematureInfantsUsingSMOFLipid®/SMOFLipid®MedicalUniversityofVienna,DepartmentofPediatricsEUDRACTNr2011-005456-33
Date22.8.2013 Version1.3 Page26of38
• Medicalorsurgicalprocedure,e.g.,surgery,endoscopy,toothextraction,transfusion.However,theeventleadingtotheprocedureisanAE.Ifthiseventisserious,theproceduremustbedescribedintheSAEnarrative.
• Pre-existingdiseaseormedicalconditionthatdoesnotworsen.• Situationsinwhichanadversechangedidnotoccur,e.g.,hospitalizationsforcosmetic
electivesurgeryorforsocialand/orconveniencereasons.• Overdoseofeitherstudydrugorconcomitantmedicationwithoutanysignsorsymptoms.
However,overdosemustbementionedintheStudyDrugLog.
9.2 SeriousAdverseEvents(SAEs)ASeriousAdverseEvent(SAE)isdefinedbytheInternationalConferenceonHarmonization(ICH)guidelinesandWHOGCPguidelinesasanyAEfulfillingatleastoneofthefollowingcriteria:
• Resultsindeaths.• Life-threatening–definedasaneventinwhichthesubjectwas,inthejudgmentofthe
investigator,atriskofdeathatthetimeoftheevent;itdoesnotrefertoaneventthathypotheticallymighthavecauseddeathhaditbeenmoresevere.
• Requiringsubject'shospitalizationorprolongationofexistinghospitalization–inpatienthospitalizationreferstoanyinpatientadmission,regardlessoflengthofstay.
• Resultinginpersistentorsignificantdisabilityorincapacity(i.e.,asubstantialdisruptionofaperson’sabilitytoconductnormallifefunctions).
• Congenitalanomalyorbirthdefect.• Ismedicallysignificantorrequiresinterventiontopreventatleastoneoftheoutcomeslisted
above.Life-threateningreferstoaneventinwhichthesubjectwasatriskofdeathatthetimeoftheevent.Itdoesnotrefertoaneventthathypotheticallymighthavecauseddeathifitweremoresevere.Importantmedicaleventsthatmaynotimmediatelyresultindeath,belife-threatening,orrequirehospitalizationmaybeconsideredasSAEswhen,baseduponappropriatemedicaljudgment,theymayjeopardizethesubjectandmayrequiremedicalorsurgicalinterventiontopreventoneoftheoutcomeslistedinthedefinitionsabove.
9.2.1 Hospitalization–ProlongationofexistinghospitalizationHospitalizationisdefinedasanovernightstayinahospitalunitand/oremergencyroom.Anadditionalovernightstaydefinesaprolongationofexistinghospitalization.HospitalizationascriteriumforSAEclassificationseverylimitedinthisstudy.Inthisstudy,patientsarehospitalizedfromstudystartuntilendoftreatment.Hospitalization–prolongationofexistinghospitalizationshouldbeappliedascriteriumforSAEclassificationonlyincaseofAEsdirectlyleadingtoaprolongationofhospitalization.ThecriteriumshouldnotbeappliedAEsoccurringduringtheroutinehospitalization.ThefollowingisnotconsideredanSAEandshouldbereportedasanAEonly:
• Treatmentonanemergencyoroutsubjectbasisforaneventnotfulfillingthedefinitionofseriousnessgivenaboveandnotresultinginhospitalization.
PreventingCholestasisinPrematureInfantsUsingSMOFLipid®/SMOFLipid®MedicalUniversityofVienna,DepartmentofPediatricsEUDRACTNr2011-005456-33
Date22.8.2013 Version1.3 Page27of38
ThefollowingreasonsforhospitalizationsarenotconsideredAEs,andthereforenotSAEs:• Hospitalizationsforcosmeticelectivesurgery,socialand/orconveniencereasons.• Standardmonitoringofapre-existingdiseaseormedicalconditionthatdidnotworsen,e.g.,
hospitalizationforcoronaryangiographyinasubjectwithstableanginapectoris.• Electivetreatmentofapre-existingdiseaseormedicalconditionthatdidnotworsen,e.g.,
hospitalizationforchemotherapyforcancer,electivehipreplacementforarthritis.
9.2.2 SAEsrelatedtostudy-mandatedproceduresSuchSAEsaredefinedasSAEsthatappeartohaveareasonablepossibilityofcausalrelationship(i.e.,arelationshipcannotberuledout)tostudy-mandatedprocedures(excludingadministrationofstudydrug)suchasdiscontinuationofsubject'sprevioustreatmentduringawashoutperiod,orcomplicationofamandatedinvasiveprocedure(e.g.,bloodsampling,heartcatheterization),orcaraccidentonthewaytothehospitalforastudyvisit,etc.
9.2.3 Suspectedunexpectedseriousadversereactions(SUSARs)SUSARsareallseriousadversereactionswithsuspectcausalrelationshiptothestudydrugthatisunexpected(notpreviouslydescribedintheSmPC-SummaryofProductCharacteristicsorInvestigator’sbrochure)andserious.
9.3 SeverityofadverseeventsTheseverityofclinicalAEsisgradedonathree-pointscale:mild,moderate,severe,andreportedonspecificAEpagesoftheCRF.IftheseverityofanAEworsensduringstudydrugadministration,onlytheworstintensityshouldbereportedontheAEpage.IftheAElessensinintensity,nochangeintheseverityisrequired.IfanAEoccursduringawashoutorplaceborun-inphaseandafterwardsworsensduringthetreatmentphase,anewAEpagemustbefilledinwiththeintensityobservedduringstudydrugadministration.MildEventmaybenoticeabletosubject;doesnotinfluencedailyactivities;theAEresolvesspontaneouslyormayrequireminimaltherapeuticintervention;ModerateEventmaymakesubjectuncomfortable;performanceofdailyactivitiesmaybeinfluenced;interventionmaybeneeded;theAEproducesnosequelae.SevereEventmaycausenoticeablediscomfort;usuallyinterfereswithdailyactivities;subjectmaynotbeabletocontinueinthestudy;theAEproducessequelae,whichrequireprolongedtherapeuticintervention.
PreventingCholestasisinPrematureInfantsUsingSMOFLipid®/SMOFLipid®MedicalUniversityofVienna,DepartmentofPediatricsEUDRACTNr2011-005456-33
Date22.8.2013 Version1.3 Page28of38
Amild,moderateorsevereAEmayormaynotbeserious.Thesetermsareusedtodescribetheintensityofaspecificevent(asinmild,moderate,orseveremyocardialinfarction).However,asevereeventmaybeofrelativelyminormedicalsignificance(suchassevereheadache)andisnotnecessarilyserious.Forexample,nausealastingseveralhoursmayberatedassevere,butmaynotbeclinicallyserious.Feverof39°Cthatisnotconsideredseveremaybecomeseriousifitprolongshospitaldischargebyaday.Seriousnessratherthanseverityservesasaguidefordefiningregulatoryreportingobligations.
9.4 RelationshiptostudydrugForallAEs,theinvestigatorwillassessthecausalrelationshipbetweenthestudydrugandtheAEusinghis/herclinicalexpertiseandjudgmentaccordingtothefollowingalgorithmthatbestfitsthecircumstancesoftheAE:Unrelated
• Mayormaynotfollowareasonabletemporalsequencefromadministrationofthestudyproduct
• Isbiologicallyimplausibleanddoesnotfollowknownresponsepatterntothesuspectstudydrug(ifresponsepatternispreviouslyknown).
• Canbeexplainedbytheknowncharacteristicsofthesubject’sclinicalstateorothermodesoftherapyadministeredtothesubject.
• Unlikely• Mayormaynotfollowareasonabletemporalsequencefromadministrationofthestudy
product• Isbiologicallynotveryplausible• Maybeexplainedbytheknowncharacteristicsofthesubject’sclinicalstateorothermodes
oftherapyadministeredtothesubject.Possiblerelated
• Followsareasonabletemporalsequenceformadministrationofthestudydrug.• Mayfollowaknownresponsepatterntothestudydrug(ifresponsepatternispreviously
known).• Couldnotbereasonablyexplainedbytheknowncharacteristicsofthesubject’sclinicalstate
orothermodesoftherapyadministeredtothesubject,ifapplicable.• Probable• Followsareasonabletemporalsequenceformadministrationofthestudydrug.• Followsaknownresponsepatterntothestudydrug(ifresponsepatternispreviously
known).• othercausesfortheeventareunlikely
Definitelyrelated
• Followsareasonabletemporalsequenceformadministrationofthestudydrug.• Followsaknownresponsepatterntothestudydrug(ifresponsepatternispreviously
known).• Nootherreasonablecauseispresent.
PreventingCholestasisinPrematureInfantsUsingSMOFLipid®/SMOFLipid®MedicalUniversityofVienna,DepartmentofPediatricsEUDRACTNr2011-005456-33
Date22.8.2013 Version1.3 Page29of38
9.5 ReportingproceduresAspecialsectionisdesignatedtoadverseeventsinthecasereportform.Thefollowingdetailsmusttherebybeentered:
• Typeofadverseevent• Start(dateandtime)• End(dateandtime)• Severity(mild,moderate,severe)• Serious(no/yes)• Unexpected(no/yes)• Outcome(resolved,ongoing,ongoing–improved,ongoing–worsening)• Relationtostudydrug(unrelated,possiblyrelated,definitelyrelated)
Adverseeventsaretobedocumentedinthecasereportforminaccordancewiththeabovementionedcriteria.
9.5.1 ReportingproceduresforSAEsIntheeventofserious,theinvestigatorhastouseallsupportivemeasuresforbestpatienttreatment.Awrittenreportisalsotobepreparedandmadeavailabletotheclinicalinvestigatorimmediately.Thefollowingdetailsshouldatleastbeavailable:
• Patientinitialsandnumber• Patient:dateofbirth,sex,ethicalorigin• Thesuspectedinvestigationalmedicalproduct(IMP)• Theadverseeventassessedasserious• Shortdescriptionoftheeventandoutcome
Ifapplicable,theinitialreportshouldbefollowedbytheFollowupreport,indicatingtheoutcomeoftheSAE.
9.5.2 ReportingproceduresforSUSARsItmustberememberedthattheregulatoryauthorities,andincaseofSUSARswhichcouldpossiblyconcernthesafetyofthestudyparticipants,alsotheInstitutionalReviewBoard/IndependentEthicsCommittee(IRB/IEC)aretobeinformed.Suchreportsshallbemadebythestudymanagementandthefollowingdetailsshouldbeatleastavailable:
• Patientinitialsandnumber• Patient:dateofbirth,sex,ethicalorigin• Nameofinvestigatorandinvestigatingsite• Periodofadministration• Thesuspectedinvestigationalmedicalproduct(IMP)• Theadverseeventassessedasseriousandunexpected,andforwhichthereisareasonable
suspectedcausalrelationshiptotheIMP
PreventingCholestasisinPrematureInfantsUsingSMOFLipid®/SMOFLipid®MedicalUniversityofVienna,DepartmentofPediatricsEUDRACTNr2011-005456-33
Date22.8.2013 Version1.3 Page30of38
• Concomitantdiseaseandmedication• Shortdescriptionoftheevent:
• Description• Onsetandifapplicable,end• Therapeuticintervention• Causalrelationship• Hospitalizationofprolongationofhospitalization• Death,life-threatening,persistentorsignificantdisabilityorincapacity
ElectronicreportingshouldbetheexpectedmethodforreportingofSUSARstothecompetentauthority.Inthatcase,theformatandcontentasdefinedbyGuidance(28)shouldbeadheredto.ThelatestversionofMedDRAshouldbeapplied.Lowerlevelterms(LLT)shouldbeused.
9.5.3 AnnualSafetyReportTheAnnualSafetyReportwillbeprovidedbytheprincipalinvestigatoratleastonceayear.ThisreportwillalsobepresentedannuallytotheIndependentEthics(IEC)andtothecompetentauthoritiesbythesponsor.
10. FOLLOW-UP
10.1 Follow-upofstudyparticipantsincludingfollow-upofadverseventsAllstudyparticipantswillbefollowedupto24monthsofcorrectedgestationalagetoassessneurodevelopment,growthparametersandophthalmologicexams(visualdevelopment(accordingtothestandardsofourfollow–upoutpatientclinicforextremelyprematureinfants.SAEsincludingdeathwillbemonitored.Adverseeventswillbefolloweduntiltheyhavebeencompletelyresolvedorstabalizedaccordingtotheinvestigatorsdiscretion.
10.2 TreatmentafterendofstudyThereisnotreatmentaftertheendofthestudy
11. STATISTICALMETHODOLOGYANDANALYSIS
11.1 AnalysissetsTwodifferentanalysissetsaredefined:
PreventingCholestasisinPrematureInfantsUsingSMOFLipid®/SMOFLipid®MedicalUniversityofVienna,DepartmentofPediatricsEUDRACTNr2011-005456-33
Date22.8.2013 Version1.3 Page31of38
(Modified)IntentiontotreatsetThisanalysissetincludesallsubjectswheretheoutcomecanbecalculated(morethantwobloodsamplestaken),eventhoughthesubjectwasnotobservedthefull18weeks.Per-protocolsetThisanalysissetcomprisesallsubjectswhowereobservedthefull18weeks,receivedthestudydrugasplannedanddidnotviolatetheprotocolinawaythatmightaffecttheevaluationoftheeffectofthestudydrugontheprimaryobjective,i.e.,withoutmajorprotocolviolations.
11.2 SamplesizeconsiderationsDatainvestigatingtheincidenceofPNACinourunitshowedanincidenceof25%from2007-9(unpublisheddata).Weconsideredadifferenceof15%betweenthegroups(incidenceofPNAC:25%forIntralipidand10%forSMOFlipid,respectively)asaclinicallyrelevanteffect.Asamplesizeestimationbasedonaχ2-testindicatedthat200infants(100/group)arerequiredtodetectadifferenceof15%betweenthegroupswithapowerof80%andasignificancelevelof0.05.Theestimateddropoutrateis22%.Therefore,asamplesizeof122patientspergroupisplanned.Forsamplesizeestimation,datawereassumedtobeindependent.
11.3 RelevantprotocoldeviationsProtocoldeviationswillhavetobedocumentedandshouldbediscussedwiththeSponsor.Allprotocoldeviationswillbelistedinthestudyreportandreportedtothesponsor.
11.4 StatisticalanalysisplanAstatisticalanalysisplan(SAP)willprovidefulldetailsoftheanalyses,thedatadisplaysandthealgorithmstobeusedfordataderivations.TheSAPfurthermorewillincludedefinitionsofmajorandminorprotocoldeviationsandthelinkofdeviationstotheanalysisset,whichalsowillbecoveredinthefinalstudyreport.Proceduresofreportinganydeviationsfromtheoriginalstatisticalplan(anydeviationsfromtheoriginalstatisticalplanshouldbedescribedandjustifiedintheprotocoland/orinthefinalreport,asappropriate.TheSAPshouldpreferablybeaseparatedocument.Intheprotocolthisdocumentshouldbereferenced.AlternativelytheSAPcouldbefullyincludedinthestudyprotocol.
11.5 Missing,unusedandspuriousdataIflessthantwobloodsamplesofapatientweretaken,theoutcomecannotbecalculatedandtherefore,thispatientwillbeexcludedfromtheanalysis.Theanalysiswillbecarriedoutperprotocol.

PreventingCholestasisinPrematureInfantsUsingSMOFLipid®/SMOFLipid®MedicalUniversityofVienna,DepartmentofPediatricsEUDRACTNr2011-005456-33
Date22.8.2013 Version1.3 Page32of38
Iftheoutcomeofapatientcanbecalculated(morethantwobloodsamplestaken)butthepatientwaswithdrawnfromthestudybeforeweek18,analysiswillbecarriedout1)byintentiontotreatanalysis,withthedurationoftreatmentasadditionalcovariableand2)perprotocol.
11.6 Endpointsanalysis
11.6.1 PrimaryendpointanalysisAχ2-testwillbeusedforanalysisoftheprimaryoutcomePNAC.Additionally,theeffectoftreatmentandotherrelevantinfluencefactors(i.e.durationofparenteralnutrition,birthweight,amountofenteralfeedsinthefirstweekoflife)ontheprimaryendpointwillbeanalyzedusingalogisticregressionmodelwithstepwiseselectionIncaseoftwins,theanalysiswillbecarriedout1)asmentionedabove,butonlyincludingthefirstbornand2)bycalculatingageneralizedlinearmodelwithmotherasrandomfactor.
11.6.2 SecondaryendpointanalysisBaileyScalesofInfantDevelopmentIIIat12and24months:Differencesinthescoresofpsychomotordevelopmentandneurocognitivedevelopment,respectively,betweenthegroupswillbeanalyzedbyrepeatedmeasuresANOVA,alsoaccountingforconfounders(e.g.birthweight,IVHGrade3/4,cysticperiventricularleucomalacia,NEC).Incaseoftwins,theanalysiswillbecarriedout1)asmentionabove,butonlyincludingthefirstbornand2)bycalculatingamixedmodelwithmotherandchildasrandomfactor.Incaseoftoomanydropouts,descriptivestatisticswillbecarriedout.ForGrossMotorfunctionmeasurementsat12and24months,descriptivestatisticswillbeconducted.
11.6.3 SafetyandtolerabilityendpointsHypertriglyceridemia:Peaklevelinmg/dl
11.6.4 BaselineparametersandconcomitantmedicationsThefollowingparameterswillbeinvestigated:Sex(m/f)Ageatbirth(gestationalweeks+days)Twin(yes/no)Modeofdelivery(caesareansection/spontaneousdelivery)Receivedanyprenatalsteroidsforlungmaturation(yes/no).Weight(gram)atbirthLength(cm)atbirthHeadcircumference(cm)atbirthSmallforgestationalage(<10.percentilebirthweight,yes/no)Apgarscoresat1,5and10minutes(0-10)UmbilicalarterypHComcomitantmedicationsandchangesinconcomitantmedicationwillbedocumentedbytheInvestigator.

PreventingCholestasisinPrematureInfantsUsingSMOFLipid®/SMOFLipid®MedicalUniversityofVienna,DepartmentofPediatricsEUDRACTNr2011-005456-33
Date22.8.2013 Version1.3 Page33of38
11.7 InterimanalysisNointerimanalysisplanned.
11.8 Softwareprogram(s)SAS9.2MicrosoftExcel
12. DOCUMENTATIONANDDATAMANAGEMENT
12.1 DocumentationofstudyresultsAsubjectscreeningandenrollmentLogwillbecompletedforalleligibleornon-eligiblesubjectswiththereasonsforexclusion.
12.1.1 Casereportform(CRF)Foreachsubjectenrolled,regardlessofstudydruginitiation,apaperCRFmustbecompletedandsignedbytheinvestigatororadesignatedsub-investigator.Thisalsoappliestothosesubjectswhofailtocompletethestudy.Ifasubjectwithdrawsfromthestudy,thereasonmustbenotedontheCRF.Casereportformsaretobecompletedonanongoingbasis.CRFentriesandcorrectionswillonlybeperformedbystudysitestaff,authorizedbytheinvestigator.Ina“Paper-CRF”allformsshouldbecompletedandmustbelegible.Errorsshouldbecrossedoutbutnotobliterated,thecorrectioninserted,andthechangeinitialedanddatedbytheinvestigator,co-investigatororstudynurse.Theentrieswillbecheckedbytrainedpersonnel(Monitor)andanyerrorsorinconsistencieswillbecheckedimmediately.ThemonitorwillcollectoriginalcompletedandsignedCRFsattheendofthestudy.AcopyofthecompletedandsignedCRFswillremainonsite.CompletedCRFswillbepassedtotheStatisticianforfurtheranalysis.
12.1.2 DataCollectionDatacollectedatallvisitsareenteredintoaninteractiveform.TheCRFswillbesourcedocumentsverifiedfollowingguidelinesestablishedbeforestudyonsetasdetailedintheMonitoringPlan.
12.2 Safekeeping
PreventingCholestasisinPrematureInfantsUsingSMOFLipid®/SMOFLipid®MedicalUniversityofVienna,DepartmentofPediatricsEUDRACTNr2011-005456-33
Date22.8.2013 Version1.3 Page34of38
Theinvestigatorwillmaintainadequateandaccuraterecordstoenabletheconductofthestudytobefullydocumentedandthestudydatatobesubsequentlyverified(accordingtoICH-GCP“essentialdocuments”).Thesedocumentswillbeclassifiedintotwodifferentcategories:investigator'sfile,andsubjectclinicalsourcedocuments.Theinvestigator'sfilewillcontaintheprotocol/amendments,EudraCTforms,CRFs(eCRFprintout),standardoperationprocedures(SOPs),dataclarificationandqueryforms,EC/IRBandHealthAuthorityapprovalwithcorrespondence,informedconsent,drugrecords,staffcurriculumvitaeandauthorizationforms,screeningandenrollmentlogs,andotherappropriatedocuments/correspondenceasperICH/GoodClinicalPractice(GCP)andlocalregulations.Subjectclinicalsourcedocumentsinclude,butarenotlimitedtosubjecthospital/clinicrecords,physician’sandnurse’snotes,appointmentbook,originallaboratoryreports,ECG,X-ray,pathologyandspecialassessmentreports,consultantletters,etc.Thesetwocategoriesofdocumentsmustbekeptonfilebytheinvestigatorforaslongasneededtocomplywithnationalandinternationalregulations(inAustria15yearsafterdiscontinuingclinicaldevelopmentorafterthelastmarketingapproval).Ifsourcedocumentsarenotdurableaslongasneeded(e.g.ECGprintouts)theymustbepreservedasacopy.NostudydocumentshouldbedestroyedwithoutpriorwrittenapprovalfromtheDepartmentof……Whensourcedocumentsarerequiredforthecontinuedcareofthesubject,appropriatecopiesshouldbemadeforstoringoutsideofthesite.
12.3 QualityControlandQualityAssurance
12.3.1 PeriodicMonitoringAccordingtoGCPatleast3monitoringvisitsarescheduled.Aninitiationvisit,oneroutinevisitandacloseoutvisitafterthelastpatienthasfinishedthestudyordatabaselock.ThedesignatedmonitorwillcontactandvisittheinvestigatorregularlyandwillbeallowedtohaveaccesstoallsourcedocumentsneededtoverifytheentriesintheCRFsandotherprotocol-relateddocumentsprovidedthatsubjectconfidentialityismaintainedinagreementwithlocalregulations.Itwillbethemonitor'sresponsibilitytoinspecttheCRFsatregularintervalsaccordingtothemonitoringplanthroughoutthestudy,toverifytheadherencetotheprotocolandthecompleteness,consistencyandaccuracyofthedatabeingenteredonthem.Themonitoringstandardsrequirefullverificationforthepresenceofinformedconsent,adherencetotheinclusion/exclusioncriteria,documentationofSAEsandtherecordingofthemainefficacy,safety,andtolerabilityendpoints.ThemonitorwillbeworkingaccordingtoSOPsandwillprovideamonitoringreportaftereachvisitfortheSponsor.Dependingonthequalityofthedata,additionalmonitoringvisitsmaybenecessaryaccordingtothesponsor’sdiscretion.Theinvestigatorwillresolvediscrepanciesofdata.MonitoringwillbeperformedbyKoordinierungszentrumfürKlinischeStudienonaregularbasisandwillfollowadetailedMonitoringPlan.

PreventingCholestasisinPrematureInfantsUsingSMOFLipid®/SMOFLipid®MedicalUniversityofVienna,DepartmentofPediatricsEUDRACTNr2011-005456-33
Date22.8.2013 Version1.3 Page35of38
12.3.2 AuditandInspectionsUponrequest,theinvestigatorwillmakeallstudy-relatedsourcedataandrecordsavailabletoaqualifiedqualityassuranceauditormandatedbythesponsorortocompetentauthorityinspectors.Themainpurposesofanauditorinspectionaretoconfirmthattherightsandwelfareofthesubjectshavebeenadequatelyprotected,andthatalldatarelevantforassessmentofsafetyandefficacyoftheinvestigationalproducthaveappropriatelybeenreportedtothesponsor.
12.4 ReportingandPublication
12.4.1 PublicationofstudyresultsThefindingsofthisstudywillbepublishedbythesponsor(investigators)inascientificjournalandpresentedatscientificmeetings.Themanuscriptwillbecirculatedtoallco-investigatorsbeforesubmission.Confidentialityofsubjectsinreports/publicationswillbeguaranteed.
13. ETHICALANDLEGALASPECTS
13.1 InformedconsentofsubjectsFollowingcomprehensiveinstructionregardingthenature,significance,impactandrisksofthisclinicaltrial,apatient´scaregiver(motherorfather)mustgivewrittenconsenttoparticipationinthestudy.Duringtheinstructionthetrialparticipantsaretobemadeawareofthefactthattheycanwithdrawtheirconsent–withoutgivingreasons–atanytimewithouttheirfurthermedicalcarebeinginfluencedinanyway.Inadditiontothecomprehensiveinstructionsgiventothetrialparticipantsbytheinvestigator,thetrialparticipantsalsoreceiveawrittenpatientinformationsheetincomprehensiblelanguage,explainingthenatureandpurposeofthestudyanditsprogress.Thepatientsmustagreetothepossibilityofstudy-relateddatabeingpassedontorelevantauthorities.Thepatientsmustbeinformedindetailoftheirobligationsinrelationtothetrialparticipantsinsuranceinordernottojeopardizeinsurancecover.
13.2 Acknowledgement/approvalofthestudyTheinvestigator(oradesignatedCRO)willsubmitthisprotocolandanyrelateddocumentprovidedtothesubject(suchassubjectinformationusedtoobtaininformedconsent)toanEthicsCommittee(EC)orInstitutionalReviewBoard(IRB).Approvalfromthecommitteemustbeobtainedbeforestartingthestudy.TheclinicaltrialshallbeperformedinfullcompliancewiththelegalregulationsaccordingtotheDrugLaw(AMG-Arzneimittelgesetz)oftheRepublicofAustria.

PreventingCholestasisinPrematureInfantsUsingSMOFLipid®/SMOFLipid®MedicalUniversityofVienna,DepartmentofPediatricsEUDRACTNr2011-005456-33
Date22.8.2013 Version1.3 Page36of38
AnapplicationmustalsobesubmittedtotheAustrianCompetentAuthorities(BundesamtfürSicherheitimGesundheitswesen(BASG)representedbytheAgencyforHealthandFoodSafety(AGESPharmMed)andregisteredtotheEuropeanClinicalTrialDatabase(EudraCT)usingtherequiredforms.Thetimelinesfor(silent)approvalsetbynationallawmustbefollowedbeforestartingthestudy.
13.2.1 ChangesintheConductoftheStudy ProtocolamendmentsProposedamendmentsmustbesubmittedtotheappropriateCAandECs.SubstantialamendmentsmaybeimplementedonlyafterCA/ECapprovalhasbeenobtained.AmendmentsthatareintendedtoeliminateanapparentimmediatehazardtosubjectsmaybeimplementedpriortoreceivingCA/ECapproval.However,inthiscase,approvalmustbeobtainedassoonaspossibleafterimplementation.StudyTerminationIfthesponsorortheinvestigatordecidestoterminatethestudybeforeitiscompleted,theywillnotifyeachotherinwritingstatingthereasonsofearlytermination.Interminatingthestudy,thesponsorandtheinvestigatorwillensuretheadequateconsiderationisgiventotheprotectionofthesubjectinterests.Theinvestigator,sponsoror(designatedCROonbehalfofthesponsor)willnotifytherelevantCAandEC.DocumentationwillbefiledintheTrialMasterandInvestigatorFiles.ClinicalStudyReport(CSR)Withinoneyearafterthefinalcompletionofthestudy,afullCSRwillbepreparedbythesponsorandsubmittedtotheECandthecompetentauthority.TheInvestigatorwillbeaskedtoreviewandsignthefinalstudyreport.
13.3 InsuranceDuringtheirparticipationintheclinicaltrialthepatientswillbeinsuredasdefinedbylegalrequirements.Theinvestigatoroftheclinicaltrialwillreceiveacopyoftheinsuranceconditionsofthe'patientsinsurance'.Thesponsorisprovidinginsuranceinordertoindemnify(legalandfinancialcoverage)theinvestigator/centeragainstclaimsarisingfromthestudy,exceptforclaimsthatarisefrommalpracticeand/ornegligence.Thecompensationofthesubjectintheeventofstudy-relatedinjurieswillcomplywiththeapplicableregulations.Detailsontheexistingpatientsinsurancearegiveninthepatientinformationsheet.PatientswillbeinsuredbytheZürich-Versicherung(Nr.07229622-2)accordingtotheAustrianlaw. Pleaseindicateinsurancedetails!
13.4 ConfidentialityTheinformationcontainedinthisdocument,especiallyunpublisheddata,isthepropertyofthesponsor.Itisthereforeprovidedtoyouinconfidenceasaninvestigator,potentialinvestigator,or
PreventingCholestasisinPrematureInfantsUsingSMOFLipid®/SMOFLipid®MedicalUniversityofVienna,DepartmentofPediatricsEUDRACTNr2011-005456-33
Date22.8.2013 Version1.3 Page37of38
consultant,forreviewbyyou,yourstaff,andanEthicsCommitteeorInstitutionalReviewBoard.Itisunderstoodthatthisinformationwillnotbedisclosedtootherswithoutwrittenauthorizationfromthesponsor.
13.5 EthicsandGoodClinicalPractice(GCP)Theinvestigatorwillensurethatthisstudyisconductedinfullconformancewiththeprinciplesofthe"DeclarationofHelsinki"(asamendedatthe56thWMAGeneralAssembly,Tokyo,Japan,2008)andwiththelawsandregulationsofthecountryinwhichtheclinicalresearchisconducted.Theinvestigatoroftheclinicaltrialshallguaranteethatonlyappropriatelytrainedpersonnelwillbeinvolvedinthestudy.AllstudiesmustfollowtheICHGCPGuidelines(June1996)and,ifapplicable,theCodeofFederalRegulations(USA).InothercountriesinwhichGCPGuidelinesexist,theinvestigatorswillstrictlyensureadherencetothestatedprovisions.ThereforethisstudyfollowstheEUDirectiveembeddedintheAustriandrugact.
14. APPENDICESAppendix1.InformedConsentForm(Version1.0;Date8.11.11)Appendix2.Summaryofproductcharacteristics
15. REFERENCES1. Peden,V.H.,Witzleben,C.L.&Skelton,M.A.Totalparenteralnutrition.TheJournalof
pediatrics78,180-181(1971).2. Lloyd,D.A.&Gabe,S.M.Managingliverdysfunctioninparenteralnutrition.TheProceedings
oftheNutritionSociety66,530-538(2007).3. Sondheimer,J.M.,Asturias,E.&Cadnapaphornchai,M.Infectionandcholestasisinneonates
withintestinalresectionandlong-termparenteralnutrition.Journalofpediatricgastroenterologyandnutrition27,131-137(1998).
4. Commare,C.E.&Tappenden,K.A.Developmentoftheinfantintestine:implicationsfornutritionsupport.NutrClinPract22,159-173(2007).
5. Messing,B.,Colombel,J.F.,Heresbach,D.,Chazouilleres,O.&Galian,A.Chroniccholestasisandmacronutrientexcessinpatientstreatedwithprolongedparenteralnutrition.Nutrition(Burbank,LosAngelesCounty,Calif8,30-36(1992).
6. Colomb,V.,etal.Roleoflipidemulsionsincholestasisassociatedwithlong-termparenteralnutritioninchildren.Jpen24,345-350(2000).
7. Shin,J.I.,Namgung,R.,Park,M.S.&Lee,C.Couldlipidinfusionbeariskforparenteralnutrition-associatedcholestasisinlowbirthweightneonates?Europeanjournalofpediatrics167,197-202(2008).
8. Koletzko,B.&Goulet,O.Fishoilcontainingintravenouslipidemulsionsinparenteralnutrition-associatedcholestaticliverdisease.Currentopinioninclinicalnutritionandmetaboliccare13,321-326(2010).
9. Diamond,I.R.,Sterescu,A.,Pencharz,P.B.,Kim,J.H.&Wales,P.W.Changingtheparadigm:omegavenforthetreatmentofliverfailureinpediatricshortbowelsyndrome.Journalofpediatricgastroenterologyandnutrition48,209-215(2009).
PreventingCholestasisinPrematureInfantsUsingSMOFLipid®/SMOFLipid®MedicalUniversityofVienna,DepartmentofPediatricsEUDRACTNr2011-005456-33
Date22.8.2013 Version1.3 Page38of38
10. Gura,K.M.,etal.Safetyandefficacyofafish-oil-basedfatemulsioninthetreatmentofparenteralnutrition-associatedliverdisease.Pediatrics121,e678-686(2008).
11. deMeijer,V.E.,Gura,K.M.,Le,H.D.,Meisel,J.A.&Puder,M.Fishoil-basedlipidemulsionspreventandreverseparenteralnutrition-associatedliverdisease:theBostonexperience.Jpen33,541-547(2009).
12. Tomsits,E.,etal.Safetyandefficacyofalipidemulsioncontainingamixtureofsoybeanoil,medium-chaintriglycerides,oliveoil,andfishoil:arandomised,double-blindclinicaltrialinprematureinfantsrequiringparenteralnutrition.Journalofpediatricgastroenterologyandnutrition51,514-521(2010).
13. Goulet,O.,etal.Anewintravenousfatemulsioncontainingsoybeanoil,medium-chaintriglycerides,oliveoil,andfishoil:asingle-center,double-blindrandomizedstudyonefficacyandsafetyinpediatricpatientsreceivinghomeparenteralnutrition.Jpen34,485-495(2010).
14. Baer,G.R.&Nelson,R.M.Ethicalchallengesinneonatalresearch:Summaryreportoftheethicsgroupofthenewborndrugdevelopmentinitiative.Clinicaltherapeutics28,1399-1407(2006).
15. Belkind-Gerson,J.,Carreon-Rodriguez,A.,Contreras-Ochoa,C.O.,Estrada-Mondaca,S.&Parra-Cabrera,M.S.Fattyacidsandneurodevelopment.Journalofpediatricgastroenterologyandnutrition47Suppl1,S7-9(2008).
16. Lapillonne,A.&Jensen,C.L.ReevaluationoftheDHArequirementfortheprematureinfant.Prostaglandins,leukotrienes,andessentialfattyacids81,143-150(2009).
17. Puder,M.,etal.Parenteralfishoilimprovesoutcomesinpatientswithparenteralnutrition-associatedliverinjury.Annalsofsurgery250,395-402(2009).
18. Diamond,I.R.CombinationTherapywithOmegavenandIntralipidinChildrenwithintestinalfailureandAdvancedParenteralNutritionAssociatedLiverdisease(PNALD).inXIInternationalSmallBowelTransplantSymposium(Bologna,2009).
19. Simmer,K.,Schulzke,S.M.&Patole,S.Longchainpolyunsaturatedfattyacidsupplementationinpreterminfants.Cochranedatabaseofsystematicreviews(Online),CD000375(2008).
20. Bines,J.ParenteralNutrition-AssociatedLiverDiseaseinWalker'spediatricgastrointestinaldisease:physiology,diagnosis,managementVol.1;614(People´sMedicalPublishingHouse,Shelton,2008).