closure of gastrojejunostomy for the relief of post-vagotomy symptoms
TRANSCRIPT

Br. J. Surg. Vol. 65 (1978) 161-163
Closure of gastrojejunostomy for the relief of post-vagotomy symptoms R O G E R G R E E N , A N N E S P E N C E R A N D T E R E N C E K E N N E D Y *
SUMMARY When dumping, diarrhoea or bile vomiting follows vagotomy and gastrojejunostomy, simple closure of the stoma, without alternative drainage, has been performed in 19 patients. Thirteen patients, 5 with truncal, 7 with selective and I with proximal gastric vagotomy, have been followed up for 1-6 years. Five were completely relieved of symptoms, 7 improved and there was only I complete failure. Bile vomiting was more often relieoed than dumping or diarrhoea. The procedure is safe and significant gastric retention does not occur provided that at least one year is allowed to elapse after the primary operation.
ALTHOUGH in some centres proximal gastric vagotomy without drainage has become the standard operation for chronic duodenal ulcer (Johnston and Wilkinson, 1970; Amdrup et al., 1974), the procedure has not yet been universally accepted, and reports of relatively high recurrence rates appear to justify caution (Kronborg and Madson, 1975; Jensen and Amdrup, 1977). It is likely that many patients will continue to be treated by vagotomy and drainage and that the sequelae, other than recurrent ulceration, will cause difficulties of management in a significant number of cases.
Diarrhoea, dumping and bile vomiting may all be associated with vagotomy and drainage, although the incidence varies with the type of operation performed. Selective vagotomy has been shown to be followed by fewer cases of troublesome diarrhoea (Frohn et al., 1968; Kennedy et al., 1973a), but possibly to be associated with a higher incidence of dumping than truncal vagotomy (Sawyers et al., 1968). Gastro- jejunostomy was associated with a higher incidence of bile vomiting than pyloroplasty in patients having truncal vagotomy in Glasgow (MacKenzie et al., 1977). In our experience, the overall incidence of bile vomiting after either pyloroplasty or gastrojejuno- stomy has been 9 per cent (Kennedy et al., 1973b). Although a small number of patients develop trouble- some symptoms after vagotomy and drainage, those that have a gastrojejunostomy are at an advantage in that the stoma can easily be closed. Ordinarily, closure is followed by pyloroplasty as an alternative drainage procedure. Closure of the gastrojejunostomy without any alternative drainage-ven after truncal vagotomy -has been used by the present authors in cases where there is no pyloric or duodenal stenosis and where at least one year has elapsed after the primary operation. The purpose of this paper is to present the mid-term results in a small group of patients.
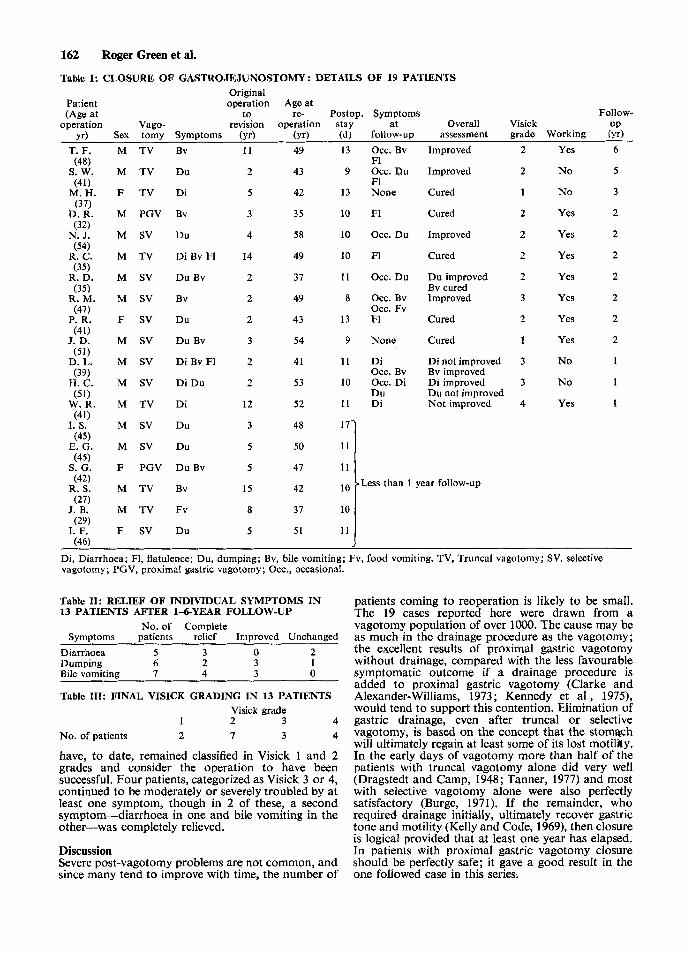
Patients and methods Nineteen patients, all of whom had previously undergone vagotomy and gastrojejunostomy for duodenal ulcer (18) or gastric ulcer (I) , were reoperated on between 1970 and 1977. Seven of these had truncal, 10 selective and 2 proximal gastric vagotomies. The main indication for closure of the gastro- jejunostomy was diarrhoea in 2 cases, dumping in 6, bile vomiting in 4 and a combination of these symptoms in 6 cases. Patients were investigated by radiology and endoscopy to
exclude the presence of recurrent ulcer, gallbladder disease or pyloroduodenal obstruction. Other causes of diarrhoea were, as far as possible, excluded. Operation was performed only after at least one year had elapsed and vigorous medical measures had been tried. The interval from primary operation to revision varied from 2 to 15 years (mean 5 years).
A laparotomy was performed through the previous scar and adhesions were divided in the regions of the duodenum and the gastrojejunostomy so that these areas could be carefully inspected for evidence of recurrent ulceration. The gastro- jejunostomy was then taken down and direct visual exclusion of jejunal ulcer was made. The pylorus was inspected and the presence of an adequate lumen confirmed, often by inserting a finger through the opening in the stomach and through the pylorus-at the same time excluding the presence of active duodenal ulceration. The jejunum and stomach were closed separately in two layers with chromic catgut. A nasogastric tube was routinely left in the stomach for about 48 h post- operatively in case early gastric retention should develop.
At clinical assessment each patient was allotted a Visick grading. Grade 1 patients were absolutely symptom-free and grade 2 patients had only minor, but not troublesome, symptoms. Grades 3 and 4 were qualified or absolute failures.
Results There were no deaths among the 19 patients and all made satisfactory progress in the postoperative period ; none showed early evidence of gastric stasis and all were able to take a normal diet at the time of discharge from hospital, 8-17 days after operation. There were no significant postoperative complications. Thirteen of the 19 patients, 1 with proximal gastric vagotomy, have been followed for a minimum of 12 and a maximum of 72 months (mean 26 months); the remaining 6, having not yet qualified for 12-month follow-up, have not been included in the assessment. No patient has required reoperation for gastric retention.
Details of all the cases are shown in Table I. Five patients were completely relieved of their symptoms, a further 7 were improved and only 1 patient, with diarrhoea, failed to gain any relief. Of the 5 patients with multiple symptoms, 2 were completely relieved but 3 gained relief of one symptom only. Looking at the symptoms individually, 3 of 5 patients with diarrhoea obtained complete relief, as did 2 of 6 dumpers and 4 of 7 bile vomiters (Table ZI). Con- siderable improvement was achieved in 3 of the remaining dumpers and in all the remaining cases with bile vomiting. The results are reflected in the Visick grading (Table H I ) . There were 7 patients in grade 2 who complained of a mild degree of flatulence after closure of the gastrojejunostomy, compared with only 2 with this symptom before reoperation. It was not considered disabling by any of the patients and in only one patient was there any other symptomatic or clinical evidence of gastric stasis. This man complained of occasional food vomiting, though he remains at work as a postman. Over 70 per cent of the patients
* Royal Victoria Hospital, Belfast. Present address of R. Green: Surgical Unit, The London Hospital, London El. Correspondence to : T. Kennedy.
162 Roger Green et al.
Table I: CLOSURE OF GASTROJEJUNOSTOMY: DETAILS O F 19 PATIENTS Original
Patient operation Age at (Age at to re- Postop. Symptoms Follow-
operation Vago- revision operation stay at Overall Visick U P yr) Sex tomy Symptoms (yr) (yr) (d) follow-up assessment grade Working (yr)
T. F.
s. w. (41)
M. H. (37)
D. R. (32)
N. J. (54)
R. c. (35)
R. D. (35)
R. M. (47)
P. R. (41)
J. D. ( 5 1 )
D. L. (39)
H. C. (51)
W. R. (41)
I. s. (45)
E. G. (45)
S. G. (42)
R. S.
J. B.
I. F. f46)
(48)
(27)
(29)
M TV Bv
M TV Du
F TV Di
M PGV Bv
M SV Du
M TV DiBvF1
M SV DuBv
M SV Bv
F SV Du
M SV DuBv
M SV DiBvF1
M SV DiDu
M TV Di
M SV Du
M SV Du
F PGV DuBv
M T V Bv
M TV Fv
F SV Du
11
2
5
3
4
14
2
2
2
3
2
2
12
3
5
5
15
8
5
49
43
42
35
58
49
37
49
43
54
41
53
52
48
50
47
42
37
5 1
13
9
13
10
10
10
11
a
13
9
I 1
10
11
11
Occ. Bv F1 occ. a u FI None
F1
Occ. Du
F1
Occ. Du
Occ. Bv Occ. Fv F1
None
Di Occ. Bv Occ. Di Du Di
Improved
Improved
Cured
Cured
Improved
Cured
Du improved Bv cured Improved
Cured
Cured
Di not improved Bv improved Di improved Du not improved Not improved
111 Less than 1 year follow-up
11
~
2
2
1
2
2
2
2
3
2
1
3
3
4
Yes
No
No
Yes
Yes
Yes
Yes
Yes
Yes
Yes
NO
No
Yes
6
5
3
2
2
2
2
2
2
2
1
1
1
Di, Diarrhoea; F1, flatulence; Du, dumping; Bv, bile vomiting; Fv, food vomiting. TV, Truncal vagotomy; SV, selective vagotomy; PGV, proximal gastric vagotomy; Occ., occasional.
Table 11: RELIEF OF INDIVIDUAL SYMPTOMS IN 13 PATIENTS AFTER 1-6-YEAR FOLLOW-UP
No. of Complete Symptoms patients relief Improved Unchanged
Diarrhoea 5 3 0 2 Dumping 6 2 3 1 Bile vomiting 7 4 3 0
Table 111: FINAL VISICK GRADING IN 13 PATIENTS Visick grade
1 2 3 4 No. of patients 2 7 3 4
have, to date, remained classified in Visick 1 and 2 grades and consider the operation to have been successful. Four patients, categorized as Visick 3 or 4, continued to be moderately or severely troubled by at least one symptom, though in 2 of these, a second symptom-diarrhoea in one and bile vomiting in the other-was completely relieved.
Discussion Severe post-vagotomy problems are not common, and since many tend to improve with time, the number of
patients coming to reoperation is likely to be small. The 19 cases reported here were drawn from a vagotomy population of over 1OOO. The cause may be as much in the drainage procedure as the vagotomy; the excellent results of proximal gastric vagotomy without drainage, compared with the less favourable symptomatic outcome if a drainage procedure is added to proximal gastric vagotomy (Clarke and Alexander-Williams, 1973; Kennedy et al , 1975), would tend to support this contention. Elimination of gastric drainage, even after truncal or selective vagotomy, is based on the concept that the stomach will ultimately regain at least some of its lost motility. In the early days of vagotomy more than half of the patients with truncal vagotomy alone did very well (Dragstedt and Camp, 1948; Tanner, 1977) and most with selective vagotomy alone were also perfectly satisfactory (Burge, 1971). If the remainder, who required drainage initially, ultimately recover gastric tone and motility (Kelly and Code, 1969), then closure is logical provided that at least one year has elapsed. In patients with proximal gastric vagotomy closure should be perfectly safe; it gave a good result in the one followed case in this series.
Closure of gastrojejunostomy 163
BURGE H. (1971) Selective vagotomy without drainage. Br. Med.
CHRISTIANSEN P. M. (1977) Reconstruction of the pylorus. (Personal communication.)
Reconstruction of the pylorus for post-vagotomy diar- rhoea and dumping. Br. J. Surg. 61, 519-520.
CLARKE R. J. and ALEXANDER-WILLIAMS J. (1973) The effect of preserving antral innervation and of a pyloroplasty on gastric emptying after vagotomy in man. Gut 14, 300-307.
CRAFT I. L. and VENABLES c. w. (1968) Antiperistaltic segment of jejunum for persistent diarrhoea following vagotomy. Ann. Surg. 167,282-286.
DRAGSTEDT L. R . and CAMP E. H. (1948) Follow-up of vagotomy in treatment of peptic ulcer. Gasfroenterof. 2, 460-465.
FROHN M., DESAI s. and BURGE H. (1968) Bilateral selective vagotomy in the prevention of post-vagotomy diarrhoea. Br. Med. J. 1, 481-483.
HERRINGTON J. L.jun. and SAWYERS J. L. (1972) A new operation for the dumping syndrome and post-vagotomy diarrhoea. Ann. Surg. 175, 790-799.
JENSEN H. E. and AMDRUP E. (1977) Five years after parietal cell vagotomy. Chir. Gastroenterol. 2, 59-62.
JOHNSON A. G. (1975) Cholecystectomy and gallstone dyspepsia. Ann. R. CON. Surg. Engl. 56, 69-80.
vagotomy without a drainage procedure in the treatment of duodenal ulcer. Br. J. Surg. 57, 289-296.
KELLY K. A. and CODE c. F. (1969) The effect of transthoracic vagotomy on canine gastric electrical activity. Gasrro- enterol. 57, 51-58.
KENNEDY T., CONNELL A. M., LOVE A. H. G. et al. (1973a) Selective or truncal vagotomy? Five-year results of a double-blind, randomized, controlled trial. Br. J. Surg. 60, 944-948.
KENNEDY T., JOHNSTON G. w., LOVE A. H. G. et al. (1973b) PyloroplAsty versus gastrojejunostomy. Results of a double-blind cofitrolled trial. Br. J. Surg. 60, 949-953.
Proximal gastric vagotomy. Interim results of a randomized controlled trial. Br. Med. J. 2, 301-303.
KRONBORG 0. and MADSON P. (1975) A controlled, randomized trial of highly selective vagotomy versus selective vago- tomy and pyloroplasty in the treatment of duodenal ulcer.
MACKENZIE I. , KENNEDY F., MACKAY c. et al. (1977) A pro- spective controlled trial of tuncal vagotomy and drainage for chronic duodenal ulcer. Br. J. Surg. 64, 292.
RODGERS H. w (1977) Pyloroplasty reconstruction. (Personal communication.)
SAWYWS J. L. and HERRINGTON I. L. (1971) Antiperistaltic jejunal segments for control of the dumping syndrome and post-vagotomy diarrhoea. Surgery 69, 263-267.
SAWYERS J. L., SCOTT H. w., EDWARDS w. H. et al. (1968) Comparative studies of the clinical effects of truncal and selettive gastric vagotomy. Am. J. Surg. 115, 165-172.
TANNER N. c. (1976) Personal observations and experiences in the diagnosis and management of ulcer disease and disabilities that follow peptic ulcer operations. Surg. Clin. North Am. 56, 1349-1363.
TANNER N. c. (1977) Vagotomy without drainage: closure of gastrojejunostomy. (Personal communication.)
Paper accepted 7.9.1977.
J. 1, 172-173.
CHRISTIANSEN P. M., HANjEN 0. H. and PEDERSON T. (1974)
JOHNSTON D . and WILKINSON A. R. (1970) Highly Selective
KENNEDY T., JOHNSTON 0. W . , MACRAE K. D . et al. (1975)
Gut 16, 268-271.
Successful reconstruction of the pylorus for the relief of dumping and diarrhoea after vagotomy has been described (Christiansen et al., 1974). There was no evidence of gastric retention in a long f61Iow-up (Christiansen, 1977). This has been confirmed by the unpublished experience of Rodgers (1977) with 4 cases of pyloroplasty reconstruction. Tanner (1976, 1977) has had success with both pyloric reconstruction and closure of gastrojejunostomy after vagotomy.
In those patients with severe and persistent post- vagotomy symptoms following gastrojejunostomy, closure of the stoma will allow the pylorus to reassume its role in the regulation of gastric emptying, and also its important anti-reflux function (Johnson, 1975), thus protecting the gastric mucosa from the adverse effects of regurgitated bile.
In our experience with 19 cases, the operation has proved simple and safe to perform and there have been no problems of gastric retention in the early postoperative period, nor any difficulty experienced by the patient in returning to a normal diet.
One patient has subsequently complained of vomiting food and, although the original problem of bile reflux is greatly improved, he now has some delay in gastric emptying. Although a mild degree of flatulence has persisted in 7 patients, this has not been associated with any other clinical or radiological evidence of gastric retention, and we do not believe that this will prove to be a significant problem provided that pyloroduodenal narrowing has been excluded.
The results of operation are most encouraging when performed for bile vomiting; of the patients followed for more than one year, the majority obtained complete relief and the remainder were improved. For diarrhoea and dumping the results were less consistent, although the majority were improved. These results suggest that either rapid gastric emptying is not the only aetiological factor in the causation of diarrhoea and dumping, or that closure of the gastrojejunostomy alone is insufficient to control gastric incontinence after vagotomy and that in these patients a jejunal interposition to control dumping (Sawyers and Herrington, 1971) or a reversal to control diarrhoea (Craft and Venables, 1968) or both (Herrington and Sawyers, 1972) may be required. The pattern of gastric emptying after gastrojejunostomy closure requires further study; it is unlikely to be absolutely normal.
In the management of post-vagotomy dysfunction, when patient and surgeon are often reluctant to embark on major revision procedures, closure of the gastrojejunostomy has been shown to be a simple and safe procedure, with relief of symptoms in the majority of patients.
References AMDRUP E., IENSEN H. E., JOHNSTON D. et al. (1974) Clinical
results of parietal cell vagotomy (highly selective vago- tomy) two to four years after operation. Ann. Surg. 180, 279-284.