cns depressants. classification ethyl alcohol general anaesthetics opioid analgesics sedative...
TRANSCRIPT
CNS DEPRESSANTS
CLASSIFICATION
ETHYL ALCOHOLGENERAL ANAESTHETICSOPIOID ANALGESICSSEDATIVE HYPNOTICS
ALCOHOL
• INEBRIANT POISONS PRODUCE INTOXICATION• THAT IS Light headednessConfusionDisorientation Drowsiness
• In most case there is recovery after prolonged sleep, with some after-effects(hangover)
• Consisting ofHeadache Irritability LethargyNauseaAbdominal discomfort

Alcohol-Ethyl alcohol
• Transparent • Colorless• Volatile liquid• Spirituous odor• Burning taste

• Absolute alcohol contains 99.95%
• Rectified spirit -90%
• Denatured alcoholAlcohol95%Wood naphtha 5%
Ethanol
• sugar +yeast=ethanol by fermentation process• Process stops when 15% alcohol is formed as
yeast is destroyed
Alcoholic beverages
• Are mixture of alcohol+water+small amount of congeners which are produced in fermentation
• Flavour is due to congeners Propyl alcoholOctyl alcoholGlycerineAldehydes
Dimethyl and diethyl esters Acids from acetic to linoleic,ketones,trimethyl
amine,allyl mercaptan etc.Total content of congeners rarely exceeds half
%
• Odour may persist in tissues for several hours after all alcohol is metabolised
Proof spirit-is one which at 10.5 degree celisus weighs exactly 12/13 part of equal measure of distilled water
Under proof –weaker spiritsOver proof – stronger spirits
• Proof is defined as twice the % of alcohol content of the drink
• Expressed in units • 1 unit=8g of alcohol
Alcohol content in beverages
• Vodka:60 to 65%
• Rum,liquors:50 to 60%
• Whisky.gin,brandy:40 to 45%
• port,sherry:20%
• Wine ,champagne:10 to 15%
• Beers:4 to 8%
Vodka:60 to 65%
Rum,liquors:50 to 60%
Brandy40 to 45% of alcohol
Beers:4 to 8%

Whisky.gin,brandy:40 to 45%
Safe limit of drinking to avoid liver damage
• Men=210g/per week• Women=140g/per week

Arrack
• It is a liquor distilled from palm,rice,sugar or jaggery,etc.
• 40 to 50% of alcohol • For kick-is mixed with chloral hydrate and
potassium bromide.

Absorption
Requires no digestion prior to absorption
Mouth & oesophagus-small amount absorbed
Stomach & small intestine- immediately
20% 80%
• 10 to 20% is prevent absorption by consumption of food with alcohol.
• Warm alcoholic drinks- absorbed fast as they dilated the gastric capillaries.
• Achloryhydria or chronic gastritis have slower absorption rates.
• 10 to 20% conc of alcohol absorbed rapid

• Dil.alcohol- empty stomach -30 to 60mins -60%
• 90% in 60 to 90 mins• Whisky and beer – in blood in just 2 to 3 mins
after few sips• Max.conc in blood reached within 45 to 90
mins• Majority in 1 hour

• Carbonated drinks hastens absorption as the bubbles greatly increases the surface area carrying alcohol.
• Food delays its absorption
• Fats and protein delay more nearly for hours
• Mixed meal depress max.conc in blood alcohol by half hour
• Lower and higher concentration absorbed quickly
• Beer takes longer absorption time than stronger drinks .
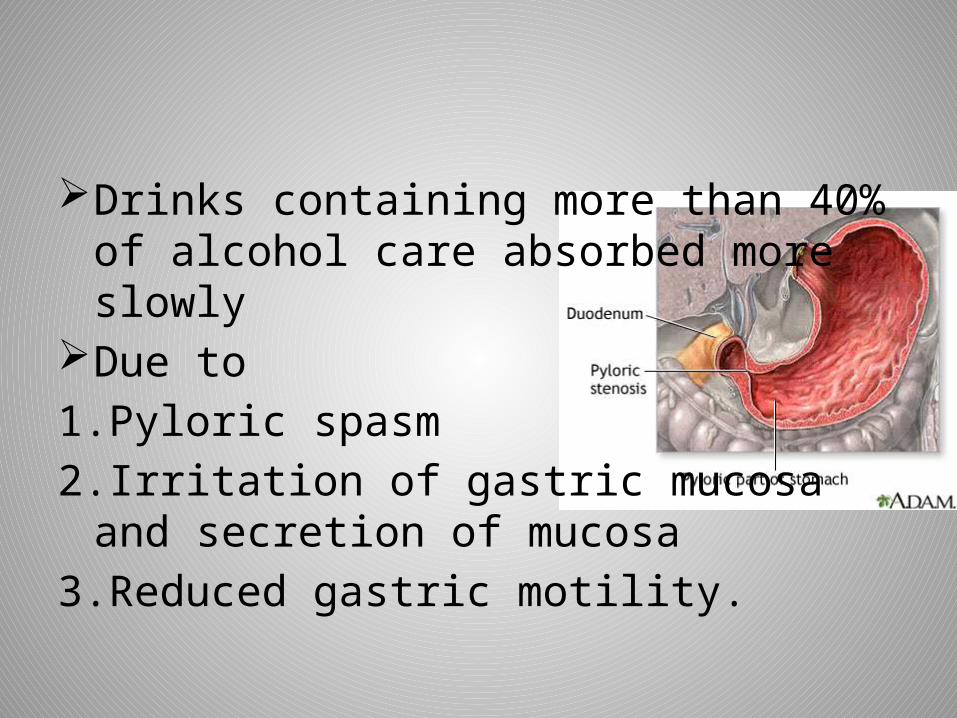
Drinks containing more than 40% of alcohol care absorbed more slowly
Due to 1.Pyloric spasm2.Irritation of gastric mucosa and secretion of
mucosa3.Reduced gastric motility.
• Habituated drinkers absorb alcohol more rapidly than abstainers,probably due to more rapid emptying time of the stomach and thus the rate of absorption .
• Drugs like benzine and atropine may slow the rate of absorption of alcohol by retarding the emptying time of stomach.
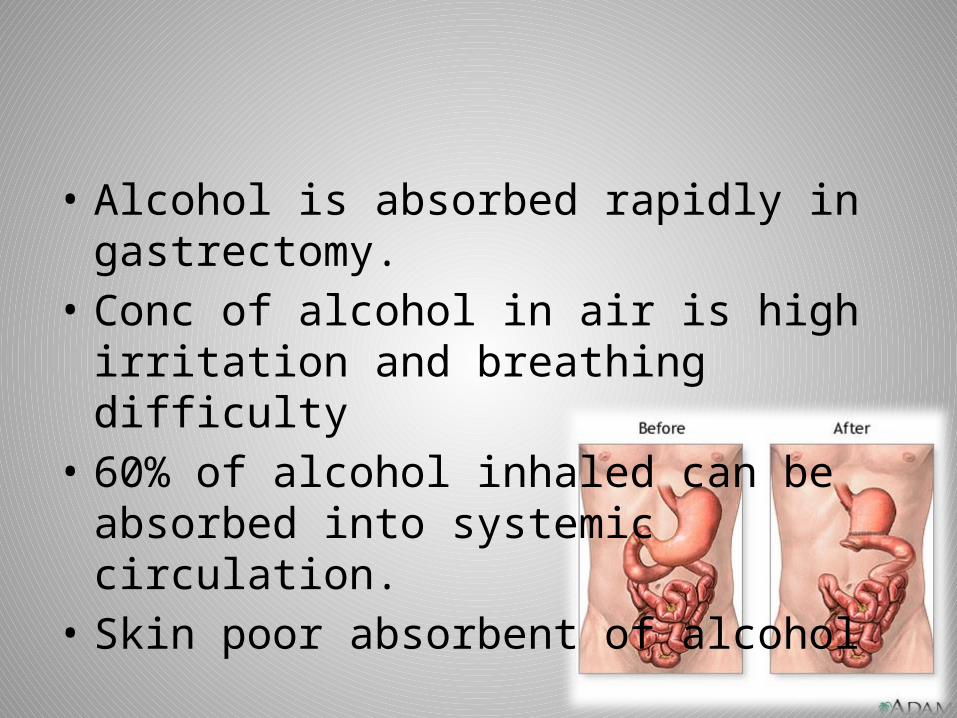
• Alcohol is absorbed rapidly in gastrectomy.• Conc of alcohol in air is high irritation and
breathing difficulty• 60% of alcohol inhaled can be absorbed into
systemic circulation.• Skin poor absorbent of alcohol
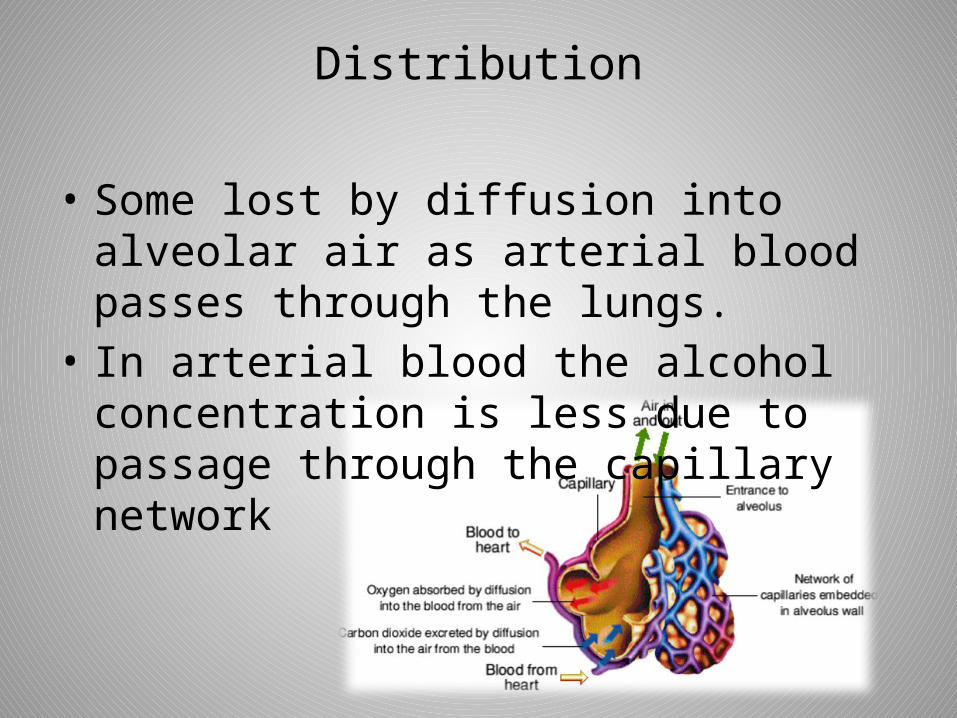
Distribution
• Some lost by diffusion into alveolar air as arterial blood passes through the lungs.
• In arterial blood the alcohol concentration is less due to passage through the capillary network
• Adipose tissue –ethanol is insoulble in fat.
• Red cells contains less alcohol then plasma.
• Plasma level of alcohol is high
• Serum level of alcohol is high
• A given intake of alcohol will prouce high level of alcohol in obese people then lean of same weight due to the aqueous compartment is smaller
• Ethanol passes through blood brain barrier and baths neuron via the cerebral extracelluar fluid.
• In females the con is higher due to small aqueous compartment

Excretion
• 5% ingested alcohol excreted via breath
• 5% in urine• Negligible amount are
excreted in the sweat,saliva,milk ,tears and faeces.
• Odour is due to excretion via skin glands.
Metabolism
90% of alcohol absorbed in oxidised in liver 10% is excreted
liver
• Acetate is oxidised into co2 and water in krebs cycle
• Diabetic who is ketogenic will produce fat from alcohol , because he cannot use the sugar.
• Enzymes can be increased by regulary use of alcoholic beverages and alcohol decrease may be doubled

OXIDATION
• Alcohol is not stored in tissues• Disappears from blood fairly uniform rate of
about 10 to 15ml per hour• This is equivalent of about 15mg 100ml• Larger doses are lost faster.• Chronic alcoholics are able to metabolise
alcohol faster -40 to 50 mg/100ml /hr
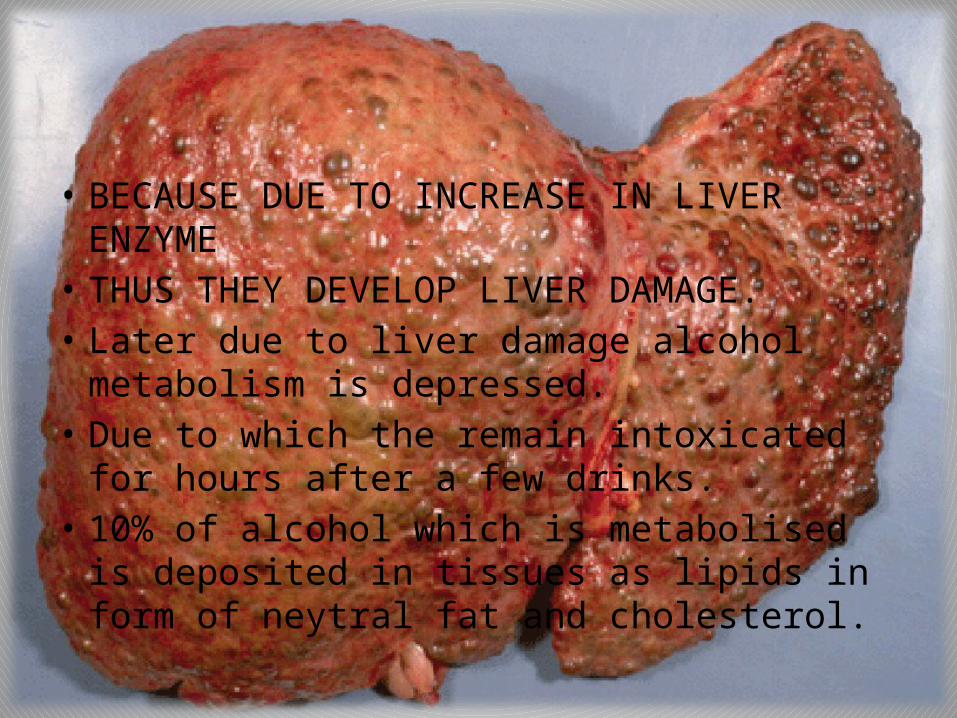
• BECAUSE DUE TO INCREASE IN LIVER ENZYME• THUS THEY DEVELOP LIVER DAMAGE.• Later due to liver damage alcohol metabolism is
depressed.• Due to which the remain intoxicated for hours
after a few drinks.• 10% of alcohol which is metabolised is
deposited in tissues as lipids in form of neytral fat and cholesterol.
ACTION
• Traces of ethyl alcohol are found in all persons.
• Endogenous alcohol Normal metabolismBacterial activity in git
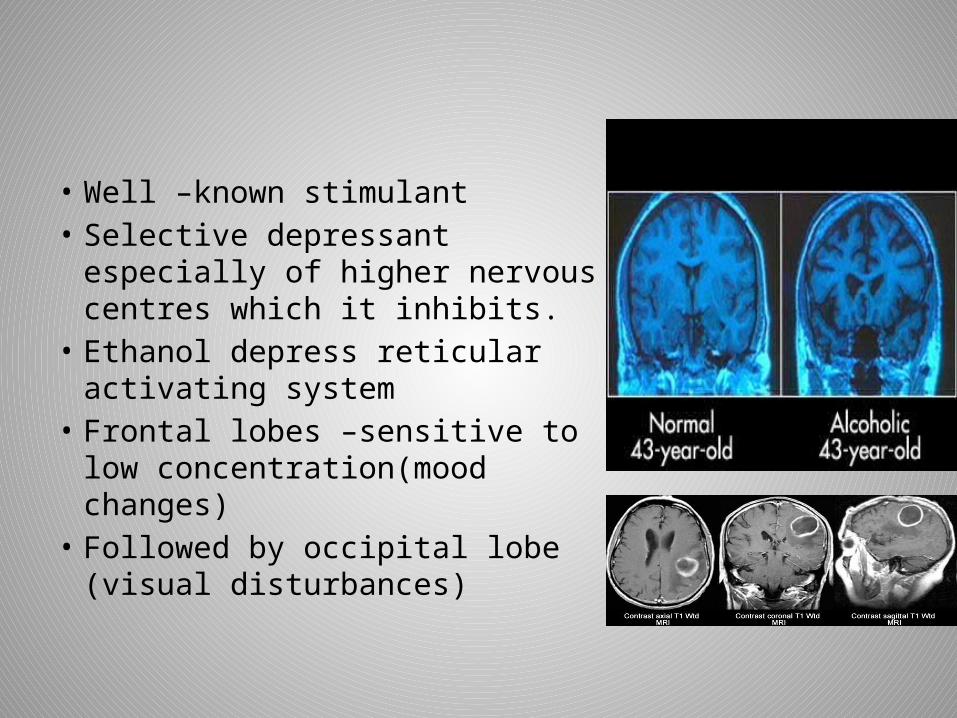
• Well –known stimulant• Selective depressant especially of
higher nervous centres which it inhibits.
• Ethanol depress reticular activating system
• Frontal lobes –sensitive to low concentration(mood changes)
• Followed by occipital lobe (visual disturbances)

• Cerebellum – loss of coordination
• Lower concentration-depression of more specialised and sensitive cells of cerebral cortex(centres regulating conduct,judgement,self criticism)
• Increasing concentration –depresses more brain function.
• Finally vital centres in mid brain and medulla are depressed – death from cardio –respiratory failure.

• Causes generalised vasodialation ,especially in skin.
• Not true aphrodisiac• Hynotic and diaphorectic• Creates sensation of
warmth ,but increases heat loss• Low concentration –heart rate
increased• More than 300mg % -
bradycardia
• Moderate –stimulates appetite as it promotes salivation and secretion of gastric juice
• Stronger beverages the reverse action
• Little brandy –carminative action
• Diuresis occurs secondary to inhibition of ADH
Release from posterior pituitary.
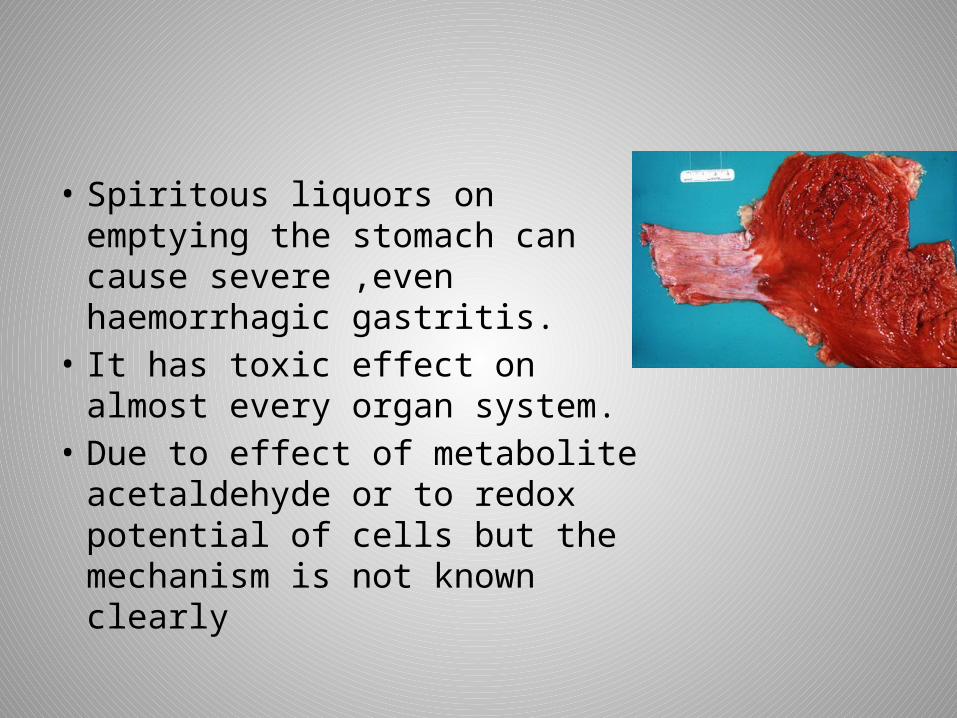
• Spiritous liquors on emptying the stomach can cause severe ,even haemorrhagic gastritis.
• It has toxic effect on almost every organ system.
• Due to effect of metabolite acetaldehyde or to redox potential of cells but the mechanism is not known clearly
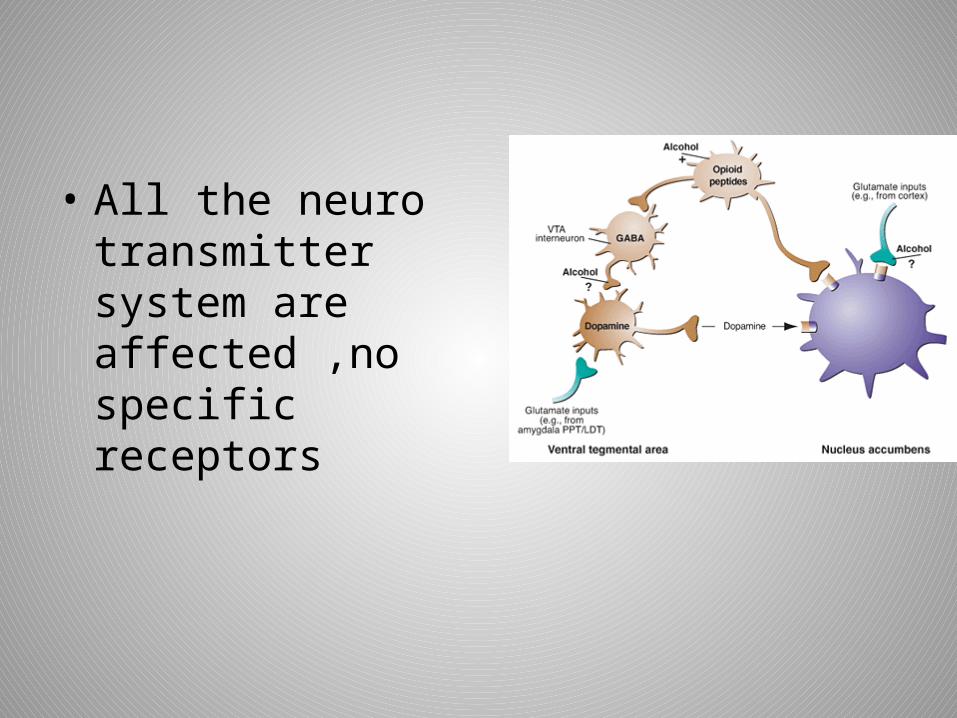
• All the neuro transmitter system are affected ,no specific receptors
• It has synergistic effect with other sedative-hypnotic agents.
• 15 to 30g /day consumption increases the concentration of hdl and decreases ldl.
• It has favourable effects on haemostatic factors such plasma fibrinogen ,fibrinolytic activity and platelet adhesiveness.

• MIXING OF DRINKS-greater intoxicationThan the amount consumed. Due to presence or formation of substances
which affect the rate of emptying of stomach,with more rapid absorption of alcohol.

• Roman saying “IN VINO VERITAS” which means “IN WINE THERE IS TRUTH”
• The real personality of individual often will be revealed when he is intoxicated.
Cause of deathDirect depressive effects upon brain stem
mediated via the respiratory centreAspiration of vomitDeath due to acute overdoses not commonChronic effects of alcohol are common.
3 phases
• There are three phases of intoxicationStage of excitementStage of incoordinationStage of coma
Stage of excitement
First a feeling of wellbeing and certain slight excitation.
Actions ,speech and emotions are less controlled due to lowering of inhibition normally exercised by higher centre of the brain
Increased confidence and lack of self control constant feature of alcoholic poisoning.

• Mental concentration is poor and judgement impaired.
• Attention is impaired• Recall memory is often disturbed
• Disclose secrets.• Good manners are forgotten• The neat and orderly are careless in their
dress• Blood alcohol concentration of 30mg%
impairment of cognitive function,motor coordination and sensory perception occur
• 50 mg % - slurring of speech,unsteadiness,drowsiness,impaired
reasoning and memory ,reduced perception and decreased concentration occur.
• Alcohol reduces visual in conc as low as 20mg% in abstainers
• 20 to 30mg% in moderate drinkers• 40 to 70 mg %in heavy drinkers
• Affects the judgement and motor control when BAC of 25 to 50mg%
• Strong light is needed for distinguish objects• Dimly lighted object may not be distinguished• It alters time and space preception.• Pupils are dilated
• Between 50 to 100 mg% -loss of inhibition ,loquaciousness and laughter occurs.
• Slurred speech ,unsteadiness and nausea are between 100 to 150mg%.
• When jerking movements is in the direction of gaze and independent of position of the head- it is known as alcohol gaze nystagmus and appears at blood level of 40 to 100mg%
• Emotions are affected• It increases the desire for sex but it impairs
the performance at 50 to 150mg% of blood alcohol
Stage of incoordination
• At 150 to 250mg/100ml the sense of perception and skilled movements are affected.
• Loss of control over the higher centres causes alteration in conduct .
• Carefree,cheerful,ill tempered ,irritable,excitable,quarrelsome,sleeply .
• Clumsiness and incoordination of movements which are skilled ones
• Alteration in speech• Nausea and vomiting • Breath smells of alcohol• Face – flused,pulse –rapid• Sense of touch,taste,smell and hearing are diminished.• Temperature – subnormal• Heart rate increased
Stage of coma
• Motor and sensory cells are deeply affected• Speech –thick and slurring , coordination is
markedly affected• Giddy,stagger and possibly fall• Person passes into state of coma with
stertorous breathing.• Pulse is rapid and temperature subnormal.

• Pupils are contracted but stimulation of the person e,g by pincing or slapping ,cause them to dilate with slow return Mc EWAN SIGN.
With recovery –coma lightens into deep sleepRecovery -8 to 10hrsWake up –with depression,nausea ,abdominal
discomfort,irritability,lethargy and severe headache.
Munich beer heart
In which cardiac dilation and hypertrophy is seen due to excessive and prolonged beer drinking.
MICTURITION SYNCOPE A condition which occurs usually after heavy
beer drinking .when the person rises from bed in the middle of night to pass urine ,he loses consciousness during the act of urination,probably due to sudden upright posture
• If coma continues more than 5hrs condition is going to worse
• Death –due to asphyxia,respiratory paralysis ,may occur in shock.
• Mostly death occurs not due to high blood level but after it have damaged the vital organs.
• Acute intoxication death –BAC of less than 400mg%
• In person with chronic diseases Arteriosclerotic heart Pulmonary emphysemaChronic lung diseasesHypoxia severe condition
• Prolonged coma leads to hypoxic brain damage and death with BAC low.
• As the alcohol might be oxdised and excreted.
• Fatal dose -150 to 250ml of absolute alcohol/one hr
• Fatal period -12 to 24hr• Tolerance to alcohol it is aquired and may be lost by those ‘out of
practice’
Consent of examination
• Consent of the detained person for medical examination is necessary.
• If the person is unconscious or not fit for consent ,the doctor called by police should not disclose to police any information he has obtained during examintion but should wait to get the consent of the patient when he regains consciousness,or in fit condition to be asked
TREATMENT
Evacuation of stomach and gastric lavage with an alkaline solution
Patient must be kept warm Congestion of the brain –ice berg should be
applied to head.One litre of normal saline with
10%glucose,100mg thiamine and 15 units of insulin are useful.
If coma deepens ,nerve stimulants such as caffeine and strychnine should be used and artificial respiration,if there is difficulty in breathing .
Inhalation of oxygen is of great useHaemodialysis or peritoneal dialysis is very
useful.
POSTMORTEM APPEARANCES
• On opening the cavities of the body ,alcoholic odour is frequently noted
• Acute inflammation of stomach with a coating of mucus is commonly found.
• The brain ,liver and lungs are congested and the smell of alcohol in the viscera may be noted.
• Blood-fluid and dark• Oedema and congestion of brain • Meninges and cloudy swelling of
parenchymatous organs are seen
CHRONIC POISONING
• Alcohol addicts withdrawal symptoms,if they do
• Results in impaired social or occupational functioning
• Chronic alcoholics are those who have reached a state of more or less irreversible somatic or brain changes caused by alcohol.
Patient suffers from
• Nausea• Vomiting• Anorexia• Diarrhoea• Jaundice• Tremors of tongue and hands• Insomnia• Loss of memory• Impaired power of judgement• Hypoproteinaemia• General anasarca Symptoms of peripheral neuritis and dementia occur in last stage Suddenly they die from coma
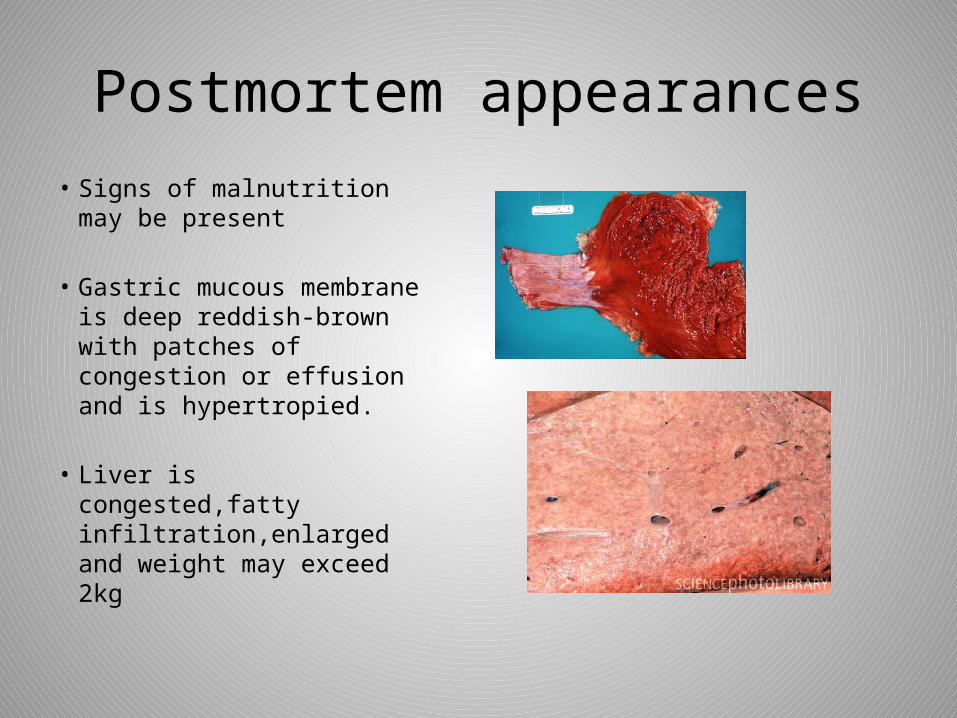
Postmortem appearances• Signs of malnutrition may
be present
• Gastric mucous membrane is deep reddish-brown with patches of congestion or effusion and is hypertropied.
• Liver is congested,fatty infiltration,enlarged and weight may exceed 2kg
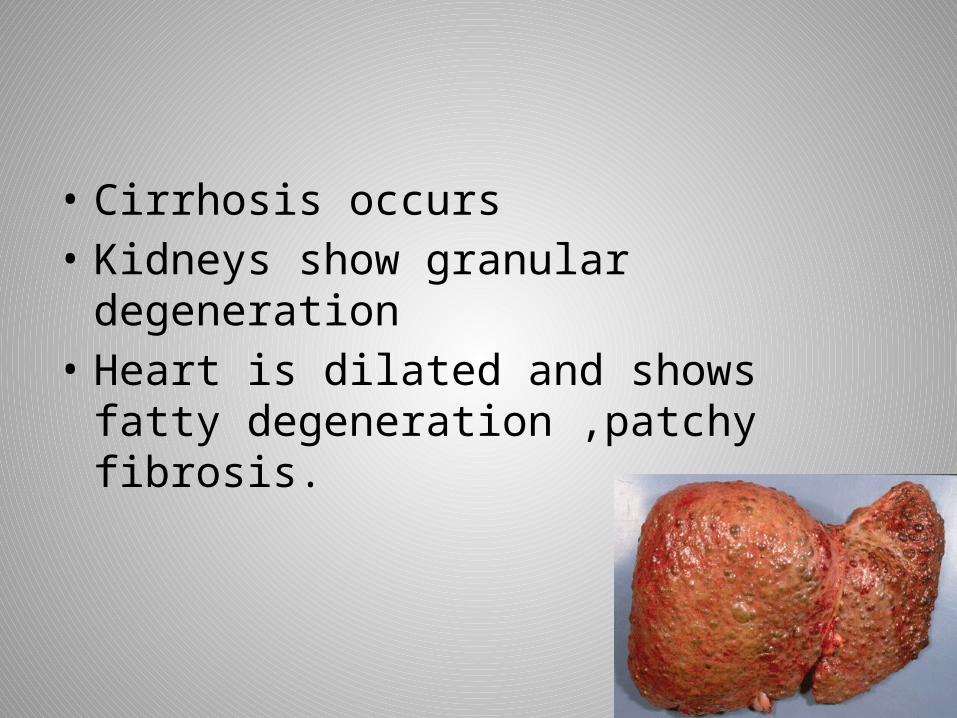
• Cirrhosis occurs • Kidneys show granular degeneration • Heart is dilated and shows fatty
degeneration ,patchy fibrosis.
Treatment
• Disulfiram-single dose daily 250mgIt is reduced gradually untill 0.125 to 0.25g is
reached which should be continued untill the patient has been conditioned to accept adequate follow-up therapy.
Antabuse inhibits the biotransformation of ethanol beyond the acetaldehyde stage.
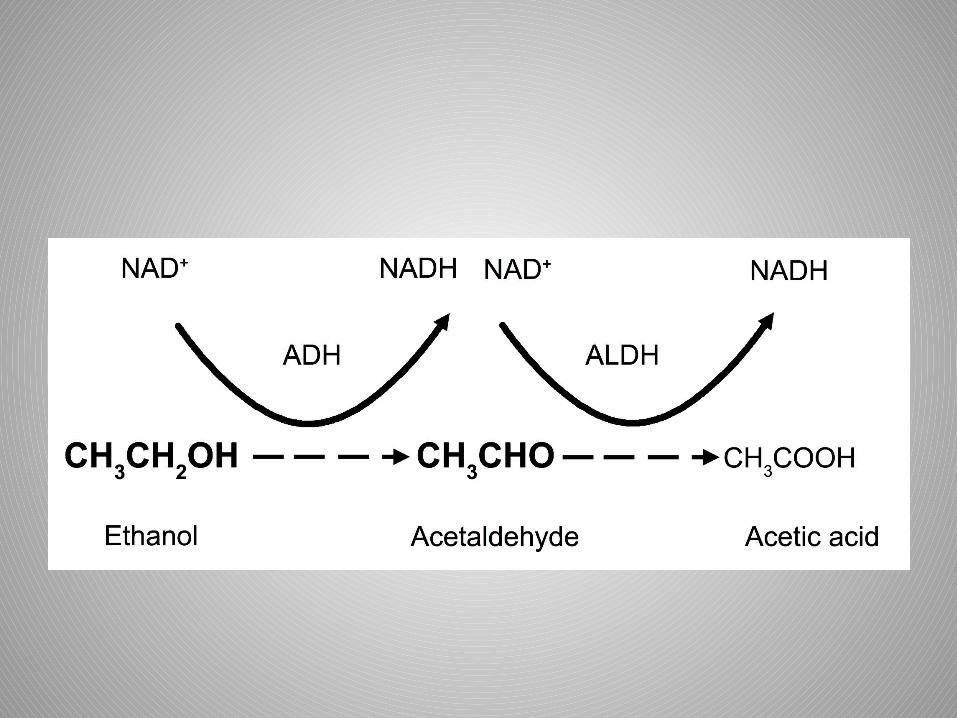
• Ethyl alcohol is metabolised by the liver as two step process
Antabuse partially blocks reaction 2,leading to acculumation of acetaldehyde in blood and tissues and causes unpleasant symptoms
Flushing ,palpitation,anxiety,sweating,headache,abdominal cramps,nausea and vomiting due to which the patient dislikes alcohol.
Citrated calcium carbimide 50mg.tablet once a day can be used with less side effects.
Chlorpromazine 25 to 50mg every 4 to 6 hours is also useful
Clonidine 60 to 180mg/hr i.vchlormethiazole
Conditioned reflex treatment
It consists of giving alcoholic beverages to the patient in surroundings that affect his visual and olfactory senses.
With a backdrop of bottles of various alcoholic beverages the patient is given various types of liquor ,togather with drugs that will cause immediate and acute nausea and vomiting .
• After 5 to 8 daily treatments,symptoms are brought on simply by sight of a bottle and the patient begins mentally to associate his painful sickness with alcohol.
• Hypnosis and psychotherapy also useful
Alcoholics anonymous
• International organisation which has branches throughout india.
• The addicts who are desirous to give up alcohol narrate their bad experiences to other alcoholics through group meetings,letters,press and other media.
• The organisation functions on self-supporting basis through contribution from the membranes.
Drunkenness
• Drunkenness is a condition produced in a person who has taken alcohol in a quantity sufficient to cause him to lose control of faculties to such an extent ,that he is unable to execute safely ,in the occupation in which he was engaged at particular time
Clinical diagnosis
• Same amount-different person-different effects-same circumstances.
• Mentally unstable ,epileptics and those who have suffered cerebral trauma show excessive reaction for small amounts.
Model scheme of medical examination
• The scheme of examination of an alleged alcoholic has been suggested by special committee of british medical association “THE DRINKING DRIVER”1965
Medical examiner’s record should note the DATEand TIME at beginning and at the end of the examination.
• (1) Exclusion of Injuries and Pathological States:• The following conditions which simulate alcoholic intoxication
should be excluded :• (a)Severe head injuries,• (b) Metabolic disorders, e.g.hypoglycemia,diabetic pre-coma,
uremia,hyperthyroidism.• (c) Neurological conditions,e.g. disseminated sclerosis,intracranial
tumors,Parkinson's disease, epilepsy, acute aural vertigo,• (d) Drugs: Insulin, barbiturates, antihistamines,morphine, atropine,
hyoscine..Drugs capable of producing sedation or depression of the nervous system (antihistaminic, tranquillizers), will simulate or enhance the effects of alcohol,
• (e) Certain preexisting psychological disorders, e.g. hypomania,general paresis,
• (f) High fever,• (g) Exposure to CO.

(2) History: Enquire whether he suffers
from any disease or disability and whether he is under medical treatment.
(3) General Behavior:(a) General manners and behavior,(b) State of dress: Presence
of slobber on mouth or clothing; presence, character and color of any vomit, soiling of clothes by excretions,
(c) Speech: Note the type, e.g.is it thick, slurred or over-precise? Slight blurring of certain consonants is one of the earliest signs of in coordination of the muscles of the tongue and lips. Certain test phrases may be used to bring out thisdifficulty in speech, such as 'British Constitution', West Register Street,Truly Rural',etc.A sober person will say that he is not good at such phrases; the semi-intoxicated person will often insist on getting them correctly,
(d) Self-control.: Note whether he is able to control himself in response to the demands made on him by the examiner.
(4) Memory and Mental Alertness:The memory of the person for recent events, and his appreciation of time can be judged by asking suitable questions about his movements during the preceding few hours, and the details of his accident if any. A few very simple sums of addition or subtraction may be asked.
(5)Handwriting:The examinees should be asked to copy a few lines from a newspaper or book. A note should be made of:(a) The time taken,(b) Repetition or omission of words,letters, or lines,(c) Ability to read his own writing. Both the original and the copy should be retained. The examinees should be asked to sign his name.The signature can be compared with that on his driving license if any.
(6) Pulse:The resting pulse should be taken at the beginning and at the end of the examination.The pulse is rapid and is usually full and bounding. A slight increase in B.P. may occur, often in the systolic level.
(7) Temperature:The surface temperature is usually raised.
(8) Skin:Note whether skin is dry, moist,flushed or pale.Skin is warm, dry and flushed in drunkenness.
(9) Mouth:(a) Record the general state of mouth, teeth and tongue, noting whether the tongue is dry, furred or bitten,(b) The smell of the breath should be recorded
(10) Eyes:(a) General appearance :(1) Whether the lids are swollen or red, and whether the conjunctiva are congested.(2) The color of the eyes, and abnormalities.(b) Visual acuity: Any gross defect should be noted.(c) Intrinsic muscles:(1) Pupils: Equal or unequal, dilated or contracted or abnormal in any way(usually dilated in early stages, but may becontracted in later stages or coma).(2) Reaction to light : Note whether the action is brisk, slow or absent. They may become unequal, equalizing againin response to light, and dilate again slowly even if the light continues to be directed into the eyes.
(d) Extrinsic muscles:(1) Convergence: Test the degree of
ability to follow a finger in all normal directions and to converge the eyes normallyon a near object.
(2) Strabismus : Note whether it is present.
(3) Nystagmus : The presence of fine lateral nystagmus may indicate alcoholic intoxication. Nystagmus may be produced by fatigue, emotion or postural hypotension.
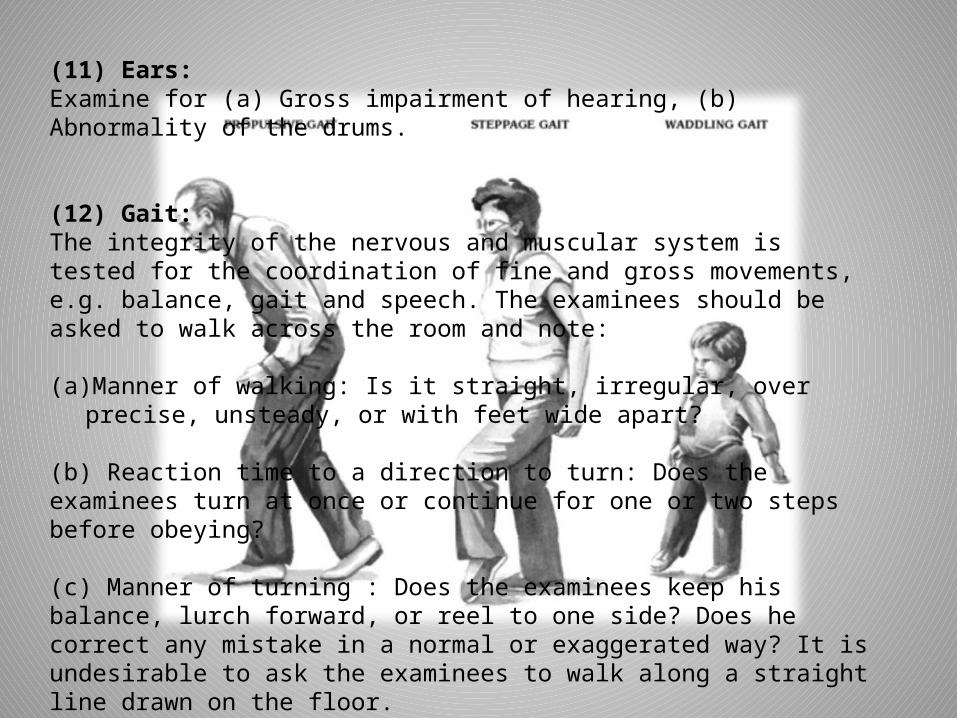
(11) Ears:Examine for (a) Gross impairment of hearing, (b) Abnormality of the drums.
(12) Gait:The integrity of the nervous and muscular system is tested for the coordination of fine and gross movements, e.g. balance, gait and speech. The examinees should be asked to walk across the room and note:
(a) Manner of walking: Is it straight, irregular, over precise, unsteady, or with feet wide apart?
(b) Reaction time to a direction to turn: Does the examinees turn at once or continue for one or two steps before obeying?
(c) Manner of turning : Does the examinees keep his balance, lurch forward, or reel to one side? Does he correct any mistake in a normal or exaggerated way? It is undesirable to ask the examinees to walk along a straight line drawn on the floor.
(13)Stance :Note whether the examinees can stand with his eyes closed and heels together without swaying.
(14) Muscular Coordination :Ask the examinees to perform the following tests:(a) Placing finger to nose,
(b) Placing finger to finger,
(c) Picking up medium-sized objects from the floor,
(d) Lighting a cigarette with a match,
(e) Unbuttoning and rebuttoning coat.
(f) Lifting two objects, such as tumblers from the table, and replacing them side by side on the table.
The examiner should not ask the examinees to perform any act which he could not perform easily himself. He should also appreciate the difficulty involved for some people in apparently simple movements, such as picking up small objects from the floor. A chronic alcoholic when sober may not be able to perform tests for coordination as well as when he has actually consumed alcohol.
(15) Reflexes :Knee and ankle reflexes should be tested which are delayed or sluggish.Plantar reflex may be extensor or flexor.
(16)Pulmonary, Cardiovascular and Alimentary Systems:The heart, lungs and abdomen should be examined, and the blood pressure taken to establish the presence or absence of disease.
(17) Tests:Some of the following objective tests are useful; flicker fusion test, measurements of tremor during standing, oscillations during forced imbalance, pupillary reflex time, speed of spinal reflexes, presence of random ocular movements with closed eye, nerve conduction speed, complex reaction time, delayed auditory feedback, positional nystagmus, glare recovery test, color difference threshold, etc.
(18) Laboratory Investigations:The degree of intoxication can be estimated by the concentration of alcohol in the blood, urine, breath, or saliva. In fatal accidents with partial body destruction, muscle or the fluid in the eye can be analyzed. Vitreous humour and urine are protected from putrefactive processes for a longer period of time and do not contain much glucose. Blood is the most suitable and the most direct evidence of the concentration of alcohol in the brain.
The disadvantages are: (1) it may be difficult to collect from an uncooperative person, (2) consent of the person is necessary, (3) substances like acetone, ether, paraldehyde, etc. when present in the blood are estimated as alcohol.
URINE : Urine has about 25% more water than an equal volume of blood, •so its concentration of alcohol would be about 25% higher than in blood collected at the same time.• As the urine is secreted, its water will have essentially the same alcohol concentration as the water of the blood passing through the kidney. •If the bladder contains urine before drinking began, urine secreted during or after the period will be diluted with the alcohol-free urine.• If the bladder was empty when drinking began, urine secreted after some time will reflect the blood concentration of alcohol at that time. In order to compare the urine and blood, a ratio of 1.3:1.0 is usually accepted when urine and blood are in equilibrium.
Analysis of two urine samples are required. The first sample should be taken as soon as possible following the incident, the bladder being completely emptied. The second sample should be taken 25 to 30 minutes later. The concentration of alcohol in the second specimen reflects the blood alcohol level during the inter-specimen interval. The difference in the alcohol concentrations in the two samples indicates whether the subject was in the absorptive phase, at its peak, or, in the elimination phase. Multiplication of alcohol concentration in the second urine specimen by 0.75 (based on a bio urine alcohol ratio of 1:1.35) gives an approximate value of the blood alcohol level, during the time that this specimen was being secreted.
The disadvantages of urine examination are: (1) A time lag before equilibrium between blood and urine is reached; the maximum concentration is reached about twenty to twenty-five minutes later than in blood.
(2) The urine alcohol concentration at any given time after the maximum concentration in blood has been reached will be higher by twenty to thirty percent than in the blood, because the specimen of urine examined will have been secreted from the blood at some earlier period.
(3) Alcohol may pass through the lining of the bladder in either direction both in life and after death, depending on the relative concentration of alcohol in blood and urine.

Collection of Blood:Spirit must not be used for cleaning the skin, and the syringe must be free from any trace of alcohol. The skin is cleaned with a solution of 1:1000 mercuric chloride or washed with soap and water. Blood samples should be preserved by the addition of hundred mg. of sodium fluoride for ten ml., followed by thorough shaking. This prevents loss of alcohol by glycolysis and bacterial action. Such samples will maintain alcohol concentration for several weeks ,even at room temperature. Hundred mg. of phenyl mercuric nitrate or sodium azide can also be used, as a preservative for 10 ml of blood or urine.
PrecautionsScrew capped glass bottle of universal size is used
Container should be tightly clamped
Sealed to prevent loss of alcohol by evaporation and labelled with name and date ,time of taking the specimens
Rubber stopper should be avoided ,because they may contaminate the sample with oxidisable substances.
It must be refrigerated if not sent to lab but not froze it
Which will cause cells to lyse
When blood is kept in a refrigerator ,formation of oxidisible substances is not significant.
Analysis is best made within a week
Serum or plasma alcohol concentration is 12 to 20% higher than that of whole blood.
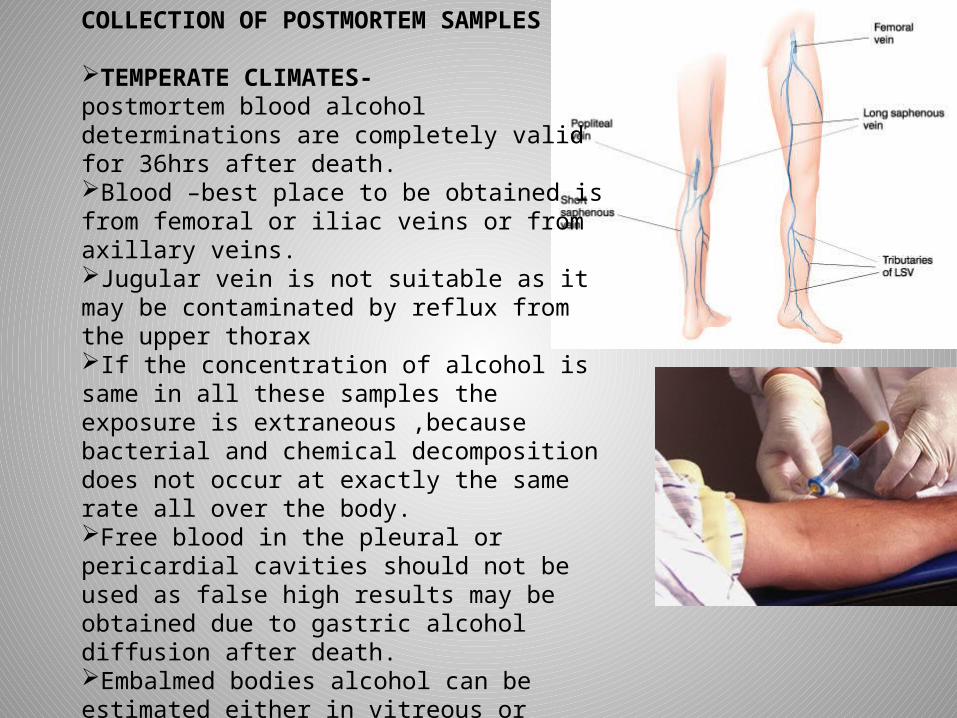
COLLECTION OF POSTMORTEM SAMPLES
TEMPERATE CLIMATES-postmortem blood alcohol determinations are completely valid for 36hrs after death.Blood –best place to be obtained is from femoral or iliac veins or from axillary veins.Jugular vein is not suitable as it may be contaminated by reflux from the upper thoraxIf the concentration of alcohol is same in all these samples the exposure is extraneous ,because bacterial and chemical decomposition does not occur at exactly the same rate all over the body.Free blood in the pleural or pericardial cavities should not be used as false high results may be obtained due to gastric alcohol diffusion after death.Embalmed bodies alcohol can be estimated either in vitreous or muscle.Erroneous result can be obtained due to haemolysis ,clot formation ,postmortem diffusion from other body fluids and tissues ,not properly preserved sample ,and putrefactionFalse blood alcohol levels in excess of 0.1 mg% may be produced if autopsy blood samples are stored at room temperature for more than a week
Widmark formula for bloodSize,sex,type of alcohol consumed . formulaA=PRCA-WEIGHT OF ALCOHOL IN g in the bodyP- is the body weight in kgC-is the concentration of alcohol in blood in mg per kgR- is a constant0.6-men 0.5 –women
For urine analysisA=3/4 PRQQ-ALCOHOL CONCENTRATION IN mg per kg
Methods used for determining blood alcoholBasic principal: reduction of potassium bichromate by test substance1.Kozelka and hine test is a macro-method.2.Cavett test is a micro-method.Many procedures are there but gas chromatography in a specificity can be ascertained
Test:in a test tube place one ml of unknown solution +one ml of acetic acid+one drop of sulphuric acid and heat gently for one minute .=strong fruity odour is positive.
BREATH : breath analysis machine operte on the principle that alcohol absorbs radiation in the infrared light absorbed by a vapour is proportional to the concentration of the alcohol in that vapour.•60 to 100 ml of breath is received into dry ballon and analysed by drunkotester, drunkometer, intoximeter, alcometer, alcotest or breathalyser•The end portion of prolonged forced expiration gives correct results .•The concentration of alcohol in deep lung air is dependant on conc in arterial blood.•2100 to 2300ml of alveolar air contains the same amount of alcohol as one ml of blood.
Factors that can upset the breath testSternuous hyperventilation Violent physical exercise Emesis Regurgitation of stomach contentsEructation or belching and drinking of liquor within few minutes of the time of the performance of the test .False value is obtained in these conditions
Saliva-mouth should be thoroughly washed with water and about 5ml of saliva collected in test tube containing 10mg of sodium fluoride
Vitreous- at equilibrium for every unit of alcohol in blood ,there are 1.2 units of alcohol in vitreous ,as it has a high water content .
During the absorptive phase of alcohol ,vitreous alcohol levels are lower than the blood.
Vitreous alcohol lags behind blood alcohol by 1 to 2 hours
It does not change after death due to putrefaction. Henry ‘s law when volatile chemical is dissolved in a liquid and is brought to equilibrium with air ,there is a fixed ratio between the concentration of volatile compound in air and its concentration in the liquid and the ratio is constant at given temperature.Temperature is 37⁰c that is exhaled air temperature
Diagnosis-
Extreme cases –no problem
Marginal cases – problem
usual Signs of drunkenness
Strong odourLoss of selfcontrolUnsteady gaitVacant lookCongested eyesDilated pupilsDry lipsIn creased pulse rateUnsteady and thick voice Talks at random Lack of perception of passage of time.
DETERMINATION OF BLOOD ALCOHOL HELPS: the concentration of alcohol circulating in the bodyThis can be attempted only after equilibrium between the blood and tissues has been attained which helps the court in testing reliabity of statement of accusedTo assits in conforming Enable to accept clinical diagnosisHelps to judge the non medical witness
Medical terminology
• Under the influence means that due to drinking alcohol,a person has lost his clearness of mind and self control.
• Loss of judgement• 140mg%- intoxicated to the point where they
cannot deal with unusual ,emergency or noncustomary problems
• Below 10mg:sober• 20 to 70mg%:drinking• 80 to 100mg%:under the influence• 150 to 300mg%:drunk or intoxicated• 400mg% and above :coma and death

Under the influence• Symptoms Flushed face Dilated and sluggish pupils Euphoria Loss of restraint Thickness of speech Carelessness and
recklessness Incoordination Stagger on sudden
Drunk Flushed face Dilated and inactive pupils Rapid movement of eyes Unstable mood Loss of restraint Clouding of intellect Thickness of speech Incoordination Staggering gait with reeling and
lurching when asked to make sudden turns
Very drunk
Mental confusion Gross incoordination Slurred speech Staggering Reeling gait Tendency to lurch and fall Vomiting
Coma Rapid pulse Subnormal temperature stertorous breathing Contracted pupils
Hazards of alcohol• Child abuse,domestic violence,suicide• Personal risk Death Pneumonia Vomit Choking Lowers resistances effect on hypoxia May fall down Head injury Drowned Electrical shock Poisoned Accidents Saturaday night paralysis

Alcoholic palimpsests or blackout
• Loss of memory of a period during a drinking spell or in some cases ,inability to recall what happened over period of days.
• The person may cause a criminal act and may not remember it when they recover

Alcohol and traffic accidents
• Driving ability 1/α conc of alcohol in blood
• Increases reaction time• Increases false confidence• Impairs concentration• Dulls judgement• Degrades muscular
coordination• Decreases visual and
auditory acuity

• Below 50%- no risk in driving• At 50%- control of
speed ,sensorimotor coordination ,braking is impaired.
• Boldness increases and impulses also
• At60%-risk of accident is higher• As mg% increases risk also
increases
In india the limit of bac
• 30mg%-first offence Rs.2000 or 6 months imprisonment or both
• Second or subsequent offence-Rs3000 or imprisonment up to 2 years or both
Alcohol withdrawl
• Symptoms appear 12 to 48hrs after reduction in alcohol intake
• Tremors of hands,tongue and eyelids • Nausea and vomiting• Malaise and weakness• Hypertension• Tachycardia,sweating• Anxiety,depressed mood ,irritability• Transient hallucinations and illusions• Headache and insomnia• Delirium tremens
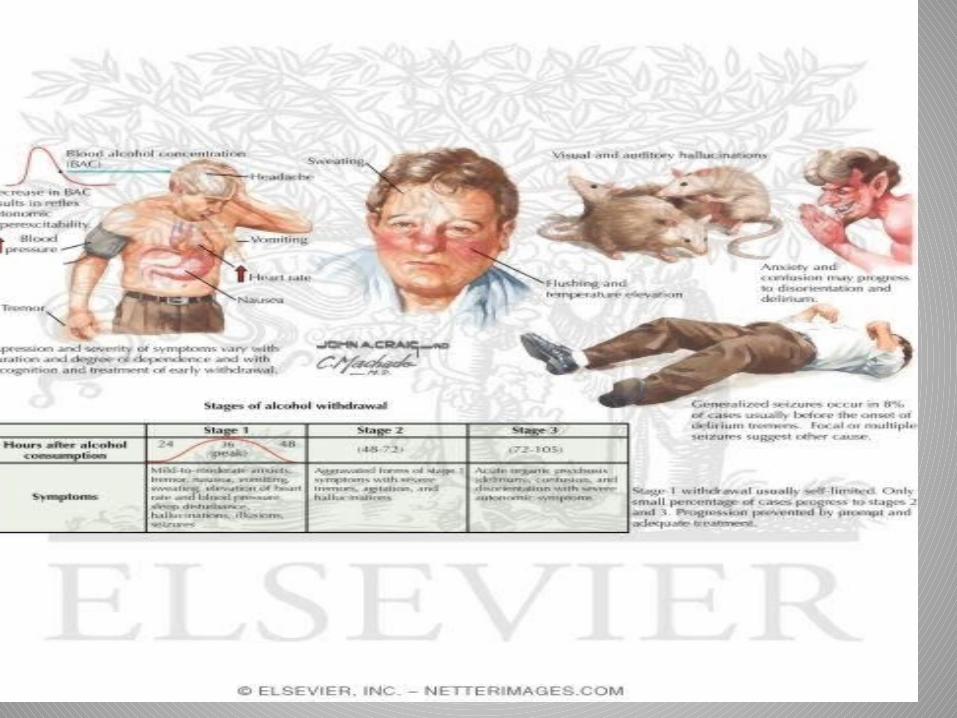
Treatment
• 20 mg of CHLORDIAZEPOXIDE or 100mg of diazepam are given 4times a day
PATHOLOGY1.DELIRIUM TREMENS –72 to 96 hrs after the last drinkTEMPORARY EXCESSSUDDEN WITHDRAWLSHOCK AFTER INJURY ,FRACTUREACUTE INFECTION-
PNEUMONIA,INFLUENZA,ERYSIPELAS
Alcoholic polyneuritisWeaknessPain in extremitiesWrist and foot dropUnsteady gaitLoss of deep reflexes and tenderness of
muscles of arm and leg
• Alcoholic paranoiaFixed delusions no hallucinationsDeeply suspicious of the motives and action of
their family members
• Acute alcoholic hallucinosisPersistent hallucination develop within 48hr
after cessationHallucination by be visual or audioContent will be unpleasant and disturbingLasts for several weeks and months

• Alcoholic epilepsy Seizures occur a day or more after termination
of drinking sessionSometimes during drinking itself it may occur
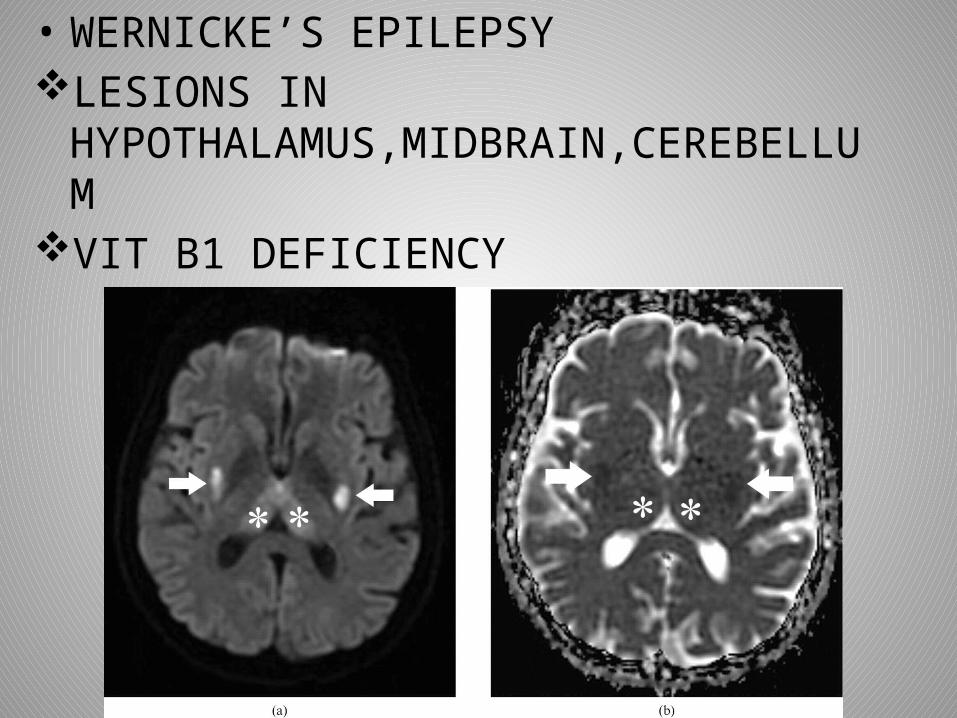
• WERNICKE’S EPILEPSYLESIONS IN
HYPOTHALAMUS,MIDBRAIN,CEREBELLUMVIT B1 DEFICIENCY
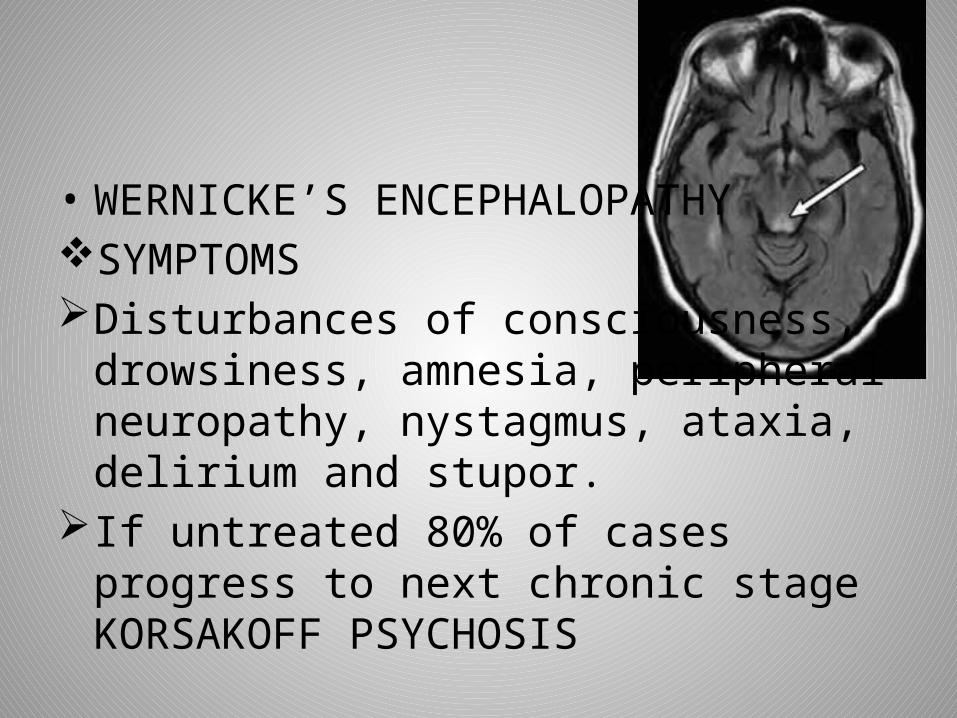
• WERNICKE’S ENCEPHALOPATHY SYMPTOMSDisturbances of consciousness, drowsiness,
amnesia, peripheral neuropathy, nystagmus, ataxia, delirium and stupor.
If untreated 80% of cases progress to next chronic stage KORSAKOFF PSYCHOSIS
KORSAKOFF PSYCHOSISIMPAIRMENT OF anterogade and retrograde
memoryDisorientation in timeInability to learn new information and
confabulation
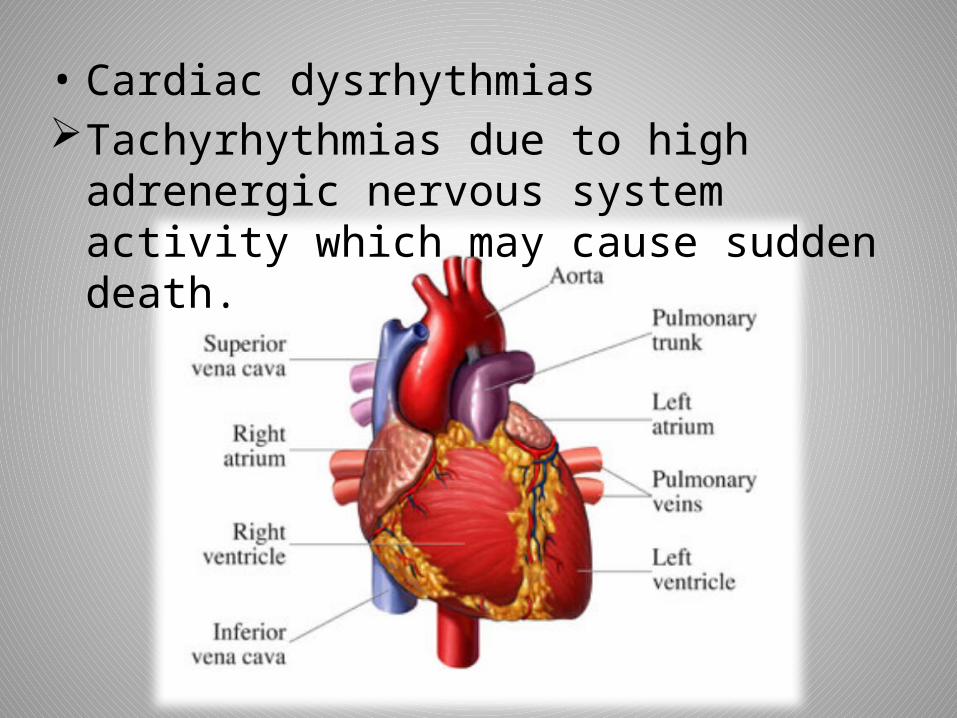
• Cardiac dysrhythmias Tachyrhythmias due to high adrenergic
nervous system activity which may cause sudden death.
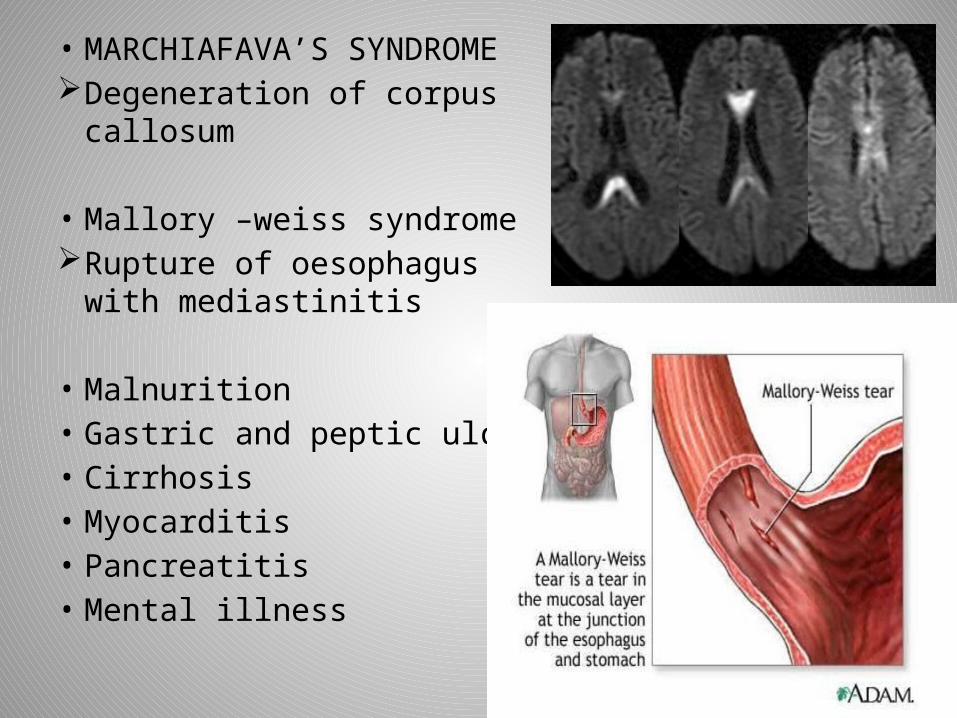
• MARCHIAFAVA’S SYNDROME Degeneration of corpus callosum
• Mallory –weiss syndrome Rupture of oesophagus with
mediastinitis
• Malnurition• Gastric and peptic ulcer• Cirrhosis• Myocarditis• Pancreatitis• Mental illness
Alcoholic and Criminal behaviour
• it is not due to infulence but due to the repression of inhibitory influences that prevents in sober person to commited a crime
• due excitement and stimulation of the brain at high peak
• suppressed feelings of aggression and hostility are released,the drinker goes into the state of artificial display of bravery
• suicides and homicides• slows the reaction of the victim• not able to protect himself• causes dilation small injury may lead
congestion of blood vessels dur to prolonged bleeding
• CHRONIC LIVER DISEASES –IMPAIRS CLOTTING• DIE FROM INHALATION OF VOMIT OR BLOOD
DUE TO INJURY• SECTION 510 IPC-MISCONDUCT IN PUBLIC-
IMPRISONMENT FOR 24HRS
ALCOHOL AND SUDDEN DEATH
• EFFECT ON MYOCARDIUM AND PRODUCES ARRHYTHMIAS
• Cardiopulmonary arrest- intoxicated –struggle-dies.no anatomical causes for death
• Catecholamines+alcohol=cardiac arrhythmia=death• “Cardiopulmonary arrest contributed by alcohol
during violent struggle”• Intoxicated person beaten in face=death –cns
depression and diffuse axonal injury from beating
Alcohol after death
• Diffuses through the stomach wall into pleural fluid,pericardinal fluid,blood and tissues
• Higher level means it was the level during living• Trauma – subdural clots and blood level of
concentration will be same in case of fatal injury• Severe internal injury –gastric contents may collect in
thoracic cavity so diffusion possibity is high • No loss occurs by evapouration• Putrefaction-alcohol level is destroyed .analysis of brain
gives best results.
• Endogenous alcohol due to bacterial activity occurs by fermentation of carbohydrates and proteins .e.coil.
• Longer interval after death .higher temperture α more production of alcohol
• 0.2% -putrefaction alcohol• 0.2% above –alcohol consumption• Blood,organs but not in urine and vitreous
humour it is not due to putrefaction.