cns excitatory and inhibitory amino acids
DESCRIPTION
הרצאה 28- 6.8.2008- SETRANSCRIPT
Neurotransmitters in the Central Nervous System
Simone Engelender

.
Neuronal communication

Fast synaptic transmission
Interval between action potential at the nerve terminal and postsypatic response: 500 s Opening of Ca2+ channels (calcium microdomains ≥100 M) Neurotransmitter secretion and start of postsynapse response

Neurotransmitter criteriaclassical definition
a) Synthesis of neurotransmitters (enzymes, prohormones)b) Vesicular storage (vesicle types, transporters)c) Release of neurotransmitters (exocytosis)d) Receptor activation (ionotropic and metabotropic)e) Inactivation (degradation, uptake)

Synaptic vesicles and SNARE

Drugs that can alter synaptic transmission
vesamicol bafilomycin
-conotoxinCo2+, Mn2+
hemicholinium-3

Known neurotransmitters Biogenic amines (classical
neurotransmitters)catecholamines (dopamine, norepinephrine and epinephrine)serotonin (5-HT)histamine
Acetylcholine Purinergic transmitters
(ATP, UTP, adenosine) Amino acid transmitters
Glutamate (aspartate)GABA, glycine
Peptide neurotransmitters Opioid peptides (endorphins, dynorphins, enkephalins), Neuropeptide Y, Neurotensin Cholecystokinin, Somatostatin, Tachykinins (substance P, neurokinin), Oxytocin, Vasopressin, etc
Unconventional transmitters (nitric oxide, carbon monoxide)

Types of receptors
Ionotropic receptors
The receptor itself incorporates an ionophore (ion channel), the gating of which is allosterically regulated by agonist binding to the receptor.
Metabotropic receptors
The receptor signals via intracellular intermediates to cause a change in ion channel gating, cell excitability, metabolic state or gene expression.

Structure of ionotropic receptors
-Ionotropic receptors are composed of subunits with four transmembrane domains and are assembled as tetramers or pentamers.
-TM2 form the main lining of the pore
-Neurotransmitter binding induces rapid conformational changes that promote the increase in the diameter of the pore.
-Cation or anion selectivity is obtained through the coordination of specific negatively or positively charged amino acids at strategic locations in the receptor pore.

Structure of metabotropic receptors
-Metabotropic receptors are G-protein coupled receptors, which are composed of a single subunit with seven transmembrane domains. Binding site for neurotransmitter lies within the core of the circular structure formed by the transmembrane segments.
-Third internal loop can have different sizes, depending on the type of metabotropic receptor.
-Third internal loop seems to be important for G-protein coupling and activation. Conformational changes upon transmitter binding exposes third internal loop.
-Can have different types of coupled G-proteins. A single receptor can activate multiple G-proteins molecules “collision coupling”. Most common effector enzymes: Adenylate cyclase (cAMP), Phospholipase C (diacyl-glycerol (DAG) + inositol trisphosphate (IP3 Ca2+).
-cAMP, cGMP, DAG, Ca 2+ can activate protein kinases but can also modulate ion channels. G proteins can also couple directly to ion channels.
-Receptor desensitization occur by covalent modifications, such as phosphorylation (fast), or by physical removal (sequestration/downregulation; slow).

Neurotransmitter receptorsIonotropic receptors
Metabotropic receptors

CNS acting drugs
• Opioid analgesics• Psychotomimetics, stimulants, alcohol and other drugs of
abuse• Drugs used in psychiatry:
– Antidepressants– Antipsychotics (neuroleptics)– Anxiolytics, hypnotic-sedatives
• General anesthetics• Anticonvulsants (antiepileptics)• Drugs for Parkinson’s and Alzheimer’s diseases

Amino acid neurotransmitters Derived from intermediary glucose metabolism and also glutamineExcitatory – glutamate, aspartateInhibitory – GABA, glycine

Cartoon of glutamatergic neuron
Two precursors for glutamate synthesis
glutamine ketoglutarate
transaminase glutaminase (phosphate-
activated)
glutamate
-Major excitatory transmitter in the brain-Almost ubiquitously present in the CNS-Mostly projection neurons (e.g. pyramidal cells of cerebral cortex)
(GABA-T)

Glutamate receptorsnon-NMDA (AMPA/KA) receptors
-Mediate most fast synaptic excitation
-Not very Ca2+ permeable
NMDA receptors
-Ca2+ permeable
-Critical for long term-potentiation (LTP)
Metabotropic (mGluR) receptors
-G-protein coupled receptor
-IP3 formation and intracellular Ca2+ signaling, and inhibition of adenylate cyclase
-Pre- and postsynaptic
-mGluR1, mGluR5 (Gq PLC)
-mGluR2, mGluR3, mGluR4, mGluR6,GluR7, mGluR8 (Gi AC)
-mGluR1: long-term synaptic plasticity (LTP, LTD)

1 .NMDA (N-methyl-D-aspartate*) receptors
2 .KA (kainate*) receptors
3 .AMPA (-amino-3-hydroxy-5-methylisoxazoleproprionic acid*) receptors
*preferred agonist
NMDA receptor KA receptors AMPA receptors
Ionotropic G lutam ate Receptors
Ionotropic Glutamate Receptors

Ionotropic glutamate receptors
-Non-NMDA receptors: Pentameric (GluR1-GluR4), GluR2 alone produce little current (relatively impermeable to Ca2+)
-NMDA receptors: obligatory NR1 subunit with multiple NR2(A-D) subunits
-NMDA receptors: well modulated channel. Important for development, learning and also neuronal damage
glycine and d-serine are co-agonists. L-aspartate can also activate NMDA channel
Mg2+ provides a voltage-dependent block
PCP and MK-801 block its ion channel
AP-5 is an antagonist of glutamate-binding site
Ion (Ca2+) channel

Long term potentiation (LTP)

Properties of Glutamate Receptors

NMDA and Schizophrenia: PCP (Phencyclidine)
-Developed in the 1950s as an intravenous anesthetic. Postoperative symptoms included dysphoria, confusion, delirium, and psychosis.
-Popular names: Angel dust, Ozone, Wack and Rocket fuel
-It is a "dissociative drug”: it distorts perceptions of sight, sound and produces feelings of detachment (dissociation) from the environment and self.
-PCP is addictive
-High doses can cause symptoms that mimic schizophrenia, such as delusionsשווא) paranoia, disordered thinking, a sensation of ,הזיות)) hallucinations ,(מחשבות distance from one's environment, and catatonia.
-Abuse of PCP for long periods can cause memory loss, difficulties with speech and thinking, depression, and weight loss. PCP has sedative effects, and interactions with other central nervous system depressants, such as alcohol and benzodiazepines, can lead to coma.

NMDA and Schizophrenia: glycine and d-Serine
- NMDARs require the binding of co-agonists (glycine or d-serine) for efficient opening of the ion channel.
- d-Serine was found to co-agonize the NMDA receptor with even greater potency than glycine.
- Removal of d-serine can block NMDA-mediated excitatory neurotransmission and toxicity.
- d-serine is produced by serine racemase in glial cells and neurons, and is enriched in the same areas as NMDA receptors.
- The use of d-serine and glycine as adjuvant therapy (together with clozapine) or monotherapy for schizophrenic patients is under investigation.

NMDA and general anesthetics: ketamine• Binds to the same PCP site. Also bind to opioid receptors.
• Patients reach rapid hypnotic state, analgesia, unresponsiveness and amnesia but can open their eyes, have involuntary movements and spontaneous respiration (Cataleptic state: Dissociative anesthesia).
• May have nystagmus with pupillary dilation, salivation and/or lacrimation, spontaneous limb movement with increased muscle tone
• Increase of cerebral blood flow and intracranial pressure (contraindicated in patients with increased intracranial pressure and cerebral ischemia).
• Can cause increase in blood pressure
• Potent bronchodilator (indicated for patients with bronchospasm)
• Important side effect: hallucinations, vivid dreams, delusions…

NMDA and Alzheimer’s disease: Memantine
Common adverse drug reactions (≥1% of patients) include: confusion, dizziness, drowsiness, headache, insomnia, agitation, and/or hallucinations. Less common adverse effects include: vomiting, anxiety, hypertonia, cystitis, and increased libido.
Memantine is a low-affinity non-competitive antagonist of NMDA receptors. The low affinity and rapid off-rate kinetics of memantine at the level of the NMDA receptor preserves the physiological function of the receptor that can still be activated by high concentrations of glutamate following depolarization.

Cartoon of GABAergic neuron
- Major inhibitory transmitter in the brain- Glutamic acid decarboxylase (GAD 65/67) is the critical biosynthetic enzyme for GABA.- GAD is not present in glutamatergic neurons. GABA and glutamate NT pools never colocalize.- Major postsynaptic GABA receptor is GABAA. - Release is regulated by GABAB metabotropic autoreceptors at the terminals- Inactivation by GABA transporters (same family as NET, DAT, SERT, GLYT): neuron and glia- Metabolized by GABA-T (back to Krebs Cycle – so called GABA shunt)- GABA neurons are prominent in the cortex where they are local circuit interneurons. Can also be
long-axoned GABA projection neurons (e.g. striatum to substantia nigra).
glutaminase (phosphate-
activated)
transaminase (GABA-T)
Two pathways for GABA synthesis
glutamine ketoglutarate
glutamate
GABA
glutamic acid decarboxylase
(GAD65/67)

GABA receptors
GABAA receptors- Major inhibitory receptor in the brain
- Ionotropic
- Multiple subunits providing numerous combinatorial possibilities- Well modulated channel -many drugs can interact with this channel:
-Barbiturates
- Benzodiapines (regulates and potentiate GABA binding) Used in Status Epilepticus
-Ethanol
-Neuroactive steroids (metabolites of progesterone, coticosterone and testosterone potentiate GABA currents), anesthetics
-Picrotoxin (convulsant-prevent ion flow)
-Bicucullin (convulsant-decrease binding of GABA)
-Metabotropic, dimeric receptorCan be pre- and postsynaptic
Coupled to adenylate cyclase, inhibitory
Agonist: Baclofen (muscle relaxant): spinal cord injury, cerebral palsy, etc.
Benzodiazepine
Channel poreChloride
Picrotoxin
GABA
Barbiturates
Steroids
Cl-
GABAB receptors

GABA receptors
• GABA-A: inhibitory
ionotropic ↑ chloride conductance
• GABA-B inhibitory (presynaptic)
metabotropic ↓ Ca++ conductance
inhibitory (post-synaptic)
↑ K+ conductance

GABAA Receptor
GABA binding site
Cl-
channel
1
1
2
2
2

GABA receptorsagonists and antagonists
Agonists Antagonists
• GABA-A Muscimol Bicuculline, (binds to GABA site) Picrotoxin
BDZ: Flumazenil
• GABA-B Baclofen Saclofen
Amanita muscaria contains muscimol (alkaloid)- cause hallucinations

BDZ X Barbiturates• Barbiturates produce their effects by increasing the length of time the
chloride GABAA ion channel remains open.
• The benzodiazepines increase the opening frequency of the GABAA chloride ion channel.
• The more extensive opening of the chloride ion channel seems to be one of the reasons for the increased toxicity of barbiturates compared to benzodiazepines in overdose.

GABAA and benzodiazepines• Unlike barbiturates, BDZ increase GABA binding
• Sedation rather general anesthesia, decreased anxiety, muscle relaxation, coronary vasodilation, anterograde amnesia /hypnosis
• Effective anticonvulsivants and used in status epilepticus (Diazepam)
• Used for anxiolysis, sedation and amnesia prior to anesthesia or small procedure that does not require anesthesia.
• Midazolam (Hypnotic) used for small procedures since it has a short half-life and it can be administered iv and by infusions
• Decrease blood pressure and respiratory drive (can result in apnea in children, patients with decreased hepatic function, alchool abuse…)
• Competitive antagonist: Flumazenil
• Also used in alcohol withdrawal syndrome: Prevent seizures and delirium

GABAA and benzodiazepines
• Drowsiness • Dizziness • Upset stomach • Blurred Vision • Headache • Confusion • Depression • Impaired coordination • Changes in heart rate • Trembling• Weakness • Dreaming or nightmares • Chest pain• Vision changes • Jaundice• Amnesia, cognitive decline• Paradoxical reactions: mania, anger, impulsivity, violent outbursts
Side effects

GABAA and barbiturates• Binds to site different from GABA and also BDZ. Enhance the effects of GABA and can
produce profound CNS depression (pentobarbital, thiopental)
• Also block the AMPA receptor, which can explain the strong CNS-depressant effects of these agents
• Sedation and anesthesia. They are also effective as anxiolytics, hypnotic and as anticonvulsants.
• Certain barbiturates have anticonvulsant activity (Phenobarbital, mephobarbital)
• More sedation than BDZ, may have euphoriant effects (specially among geriatric patients)
• In patients with pain, restlessness, excitement, delirium and increase of pain may occur
• Interaction with ethanol can increase CNS depression
• Tolerance, addition, overdose
• Thiopental is an ultra-short acting barbiturate used as a "truth serum". The drug decrease inhibitions, making people more likely to be caught off guard when questioned.

GABAA and barbiturates
- Physical and psychic dependence
- Intoxication include: Respiratory depression, lowered blood pressure, fatigue, fever, unusual
excitement, irritability, dizziness, poor concentration, sedation, confusion, impaired coordination (Ataxia), nystagmus, impaired judgment, addiction, and respiratory arrest, which may lead to death.

GABAA and ethanol
• Bicuculline and Flumazenil reduce ethanol consumption in rodents.
• Injection of agonist muscimol in the limbic system can substitute ethanol in rodents.

GABAA and ethanol
• Death from ethyl alcohol consumption is possible when blood alcohol level reaches 0.4%. A blood level of 0.5% or more is commonly fatal. Levels of even less than 0.1% can cause intoxication, with unconsciousness often occurring at 0.3–0.4%
GABAA and ethanol
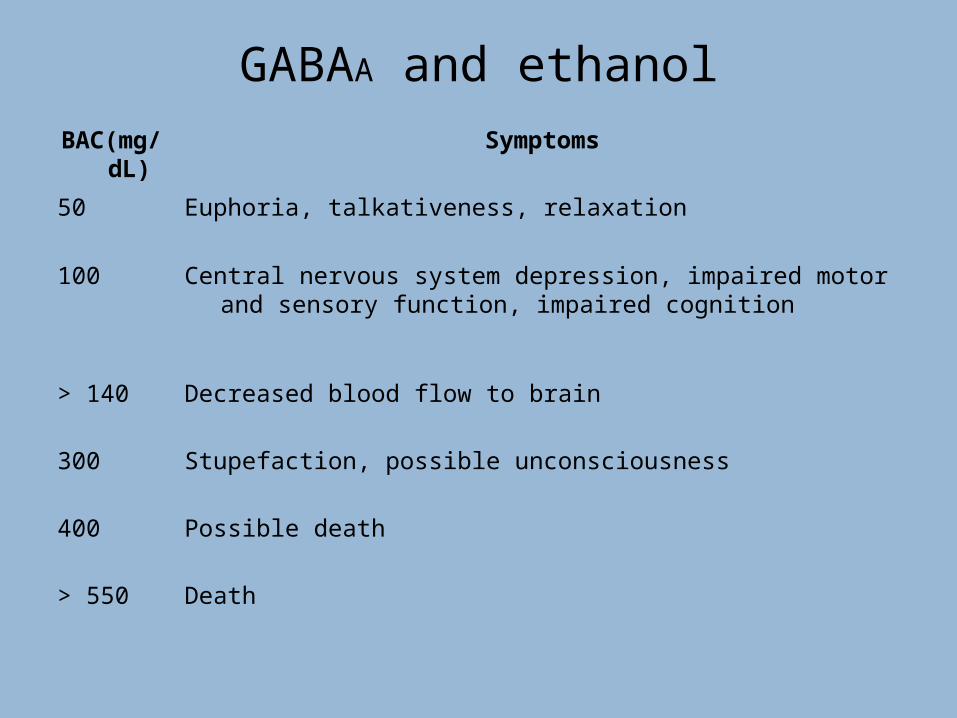
BAC(mg/dL)
Symptoms
50 Euphoria, talkativeness, relaxation
100 Central nervous system depression, impaired motor and sensory function, impaired cognition
> 140 Decreased blood flow to brain
300 Stupefaction, possible unconsciousness
400 Possible death
> 550 Death

GABAA and general anesthetics
• GABAA is sensitive to inhaled gases, such as halotane.
• Also to intravenous agents: barbiturates, propofol, etc.
• They decrease the closure of ion channel of GABAA receptor.
• Probably GABAA receptor has a specific site for binding anesthetics since mutations in the receptor can eliminate their effects.

GABAA and Antiepileptic drugs
Alter GABA release and uptake ?
Gabapentin
(Neuropathic and herpetic pain)
GABA reuptake inhibitorTiagabine
GABA-Transaminase inhibitor
Vigabatrin
GABA-Transaminase inhibitor (+/-)
Valproate
dizziness, fatigue, drowsiness, gastrointestinal upsets, ataxia, tremor
fatigue, drowsiness, weight gain, behavioral and mood changes, depression, agitation, confusion, psychosis (rare), visual defects (after long term use)
gastrointestinal upsets, alopecia, peripheral edema, weight gain, hepatotoxicity, teratogenicity
dizziness, fatigue, confusion, depression, confusion, ataxia, tremor, gastrointestinal upsets, psychosis (rare), skin rash

GABAA and Antiepileptic drugsSeizure Type Drug
Simple and complex
partial
Lamotrigine (Lamictal), Oxcarbazepine (Trileptal), Gabapentin (Neurontin), Topiramate (Topamax)
Phenytoin (Dilantin), Carbamezapine (Tegretol), Valproate
Secondarily generalized tonic-clonic
Same as “Simple and complex Partial”
Absence Ethosuximide, Lamotrigine, Valproate
Myoclonic Lamotrigine, Valproate, Clonazepam
Atonic Lamotrigine, Valproate, Felbamate
Tonic-clonic Same as “Simple and complex Partial”

Glycine neurotransmission
- Major inhibitory neurotransmitter in spinal cord and brainstem
- Actions terminated by uptake (GLYTs) by neurons and glia
-Glycine receptors are ionotropic (similar to GABAA receptors): permeable to Cl-
- Receptors blocked by strychnine
and subunits. subunit is widespread and may have additional functions besides its association with glycine receptors.
- Glycine also binds to NMDA-R (co-agonist)

Glycine receptors
Action: inhibitory, ↑ chloride conductance
Agonists taurine, -alanine
Antagonist strychnine