‘cognitive biases plus,’ healthcare organizations, quality of evidence, and person- centered...
TRANSCRIPT

‘Cognitive biases plus,’ healthcare organizations, quality of evidence, and
person-centered care*Dr. Shashi Seshia** et al.
Healthcare Evidence
**Dept. of Pediatrics, University of Saskatchewan, Canada * Title shortened to key words, here and in the companion poster
Introduction
• In their BMJ June 2014 essay, “EBM: a movement in crisis?,” Greenhalgh et al wrote in passing: “EBM has not addressed the problem it was meant to resolve: evidence biases and the hidden hand of vested interests, which have become subtler and harder to detect.”
• We have explored these issues in a recent two part review, and feel privileged to brainstorm our thoughts with you at this meeting.

Hypothesis (JECP 2014;20:734-58)
EBM paradigm
Organizations that influence healthcare evidence & delivery
Point of Care: Individual & Population
Cognitive biases plus

Methods etc.
• Qualitative review. • Detailed in JECP 2014;20:734-58.• References (200 or so) from diverse
disciplines, including behavioral economics.• Note: Handout (with some definitions, and a
table of cognitive biases plus), and PDFs of an earlier review ‘pre-circulated.’
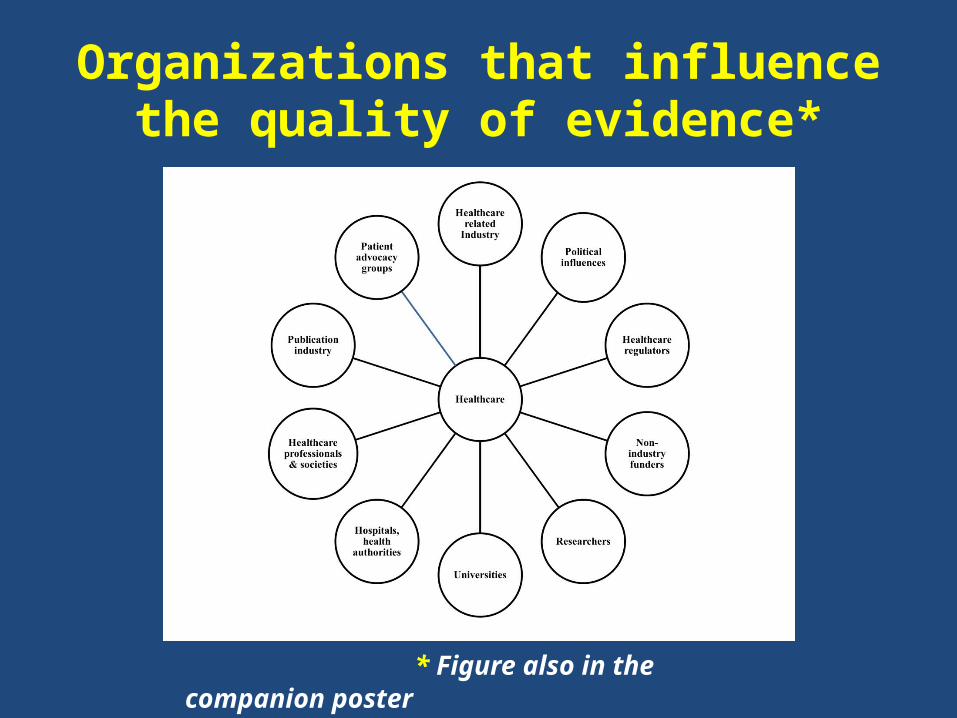
Organizations that influence the quality of evidence*
* Figure also in the companion poster

Cognitive biases plus• Variable combination of
CoIs (financial, non-financial-intellectual etc), cognitive biases, fallacies & ethical violations.
• Hard wired primarily at the unconscious level (limbic system: “reptilian brain”).
• Influenced by emotion etc.• None of us is immune.

Financial and non-financial CoIs, often co-occur: red flags for self-serving bias and bad decisions (Campbell et al 2009 etc)

Two other important biases that contribute to flawed evidence
Authority*(Hubris)
Herd (lemming**) Effect
*Authority: individual,organization, high impact publication **http://www.google.ca/imgres?imgurl=http://3.bp.blogspot.com/-
foW99izIOiY/T_weZUNIaoI/AAAAAAAAF-8/8iU2niB-UI4/s1600/Lemmings...
Cartoon:CMadden

A third: Scientific inbreeding, often associated with publication biases
(Ioannidis)
http://www.google.ca/imgres?imgurl=http://super-trainer.com/wp-content/uploads/2011/06/herd_of_sheep_311px1.gif&imgrefurl=http://super-trainer.com/building-a-

The ‘Cognitive biases plus’ cascade and evidence*
* Figure also in the companion poster

Organizations that influence the quality of evidence*
* Figure also in the companion poster

We must be aware & beware: Faulty evidence is well camouflaged!
• Cognitive biases plus, including methodological & statistical skulduggery & persuasive but fallacious discourses typically from authority, difficult to detect.“

Our hypothesis is plausible but…limitations
• Review is qualitative.• Our own ‘cognitive biases plus.’• Evidence circumstantial.• We have not proven ‘cause and effect’ (Sir
Austin Bradford Hill’s concept of “Causation or Association?”).
Conclusions
• To achieve “real EBM”: recognize and address cognitive biases plus, especially CoIs, that have blighted the landscape of evidence; to cure: must uproot the causes.
• Above all, reclaim integrity, a quality Sir Austin considered essential for the practice of Medicine.

They are discussing EBM
Beetle Bailey Cartoon: creator ‘Mort’ Walker

Acknowledgements
• Children’s Foundation of Saskatchewan.
• Journal of Evaluation in Clinical Practice 2014; 20: 734-58 (Talk, handout, poster based on this two part review; figures from the review). Saskatoon, Saskatchewan

Suggestions
• Recognize the role of cognitive biases plus in compromising healthcare evidence and delivery.
• Involve experts in ethics, law and social behavioral research to help formulate remedial action.
• Abolish incentives that spawn self-serving bias; punishment for breaches should be severe.
• Universities must value integrity, dedication to patient care and teaching at least as much as they do research.

Suggestions (2)
• Discard the impact factor (DeAngelis): a tarnished and misleading standard.
• Groupthink in organizations can only be minimized by obtaining and incorporating independent opinions (Kahneman 2011).
• Use of social media for messaging integrity and code of honor.
• Our responsibility is global &• Action must be: Collective.

Publication Industry (including pre-appraised evidence): A major gatekeeper of information
• Smith: Medical journals marketing arms of industry.• Angell: Cannot rely on medical literature for reliable
information.• DeAngelis: Impact factor is manipulative…abolish!• Hirst & Altman; Macleod et al: Much published
research misleading/biased, even harmful.• Financial CoI; other cognitive biases plus (editors etc).• Promoted an infallible view of EBM?• Culpability of publication industry an important factor
in the dissemination of flawed evidence.