cognitive disorders - lippincott williams &...
TRANSCRIPT

C H A P T E R
31
key termsagnosiaaphasiaapraxiacognitive mental disordersconfabulationdeliriumdementiasundowning
learning objectivesOn completion of this chapter, you should be able to accomplish the following:
1. Define the term cognitive mental disorder.
2. Discuss the incidence and significance of cognitive disorders.
3. Identify clinical features or behaviors associated with cognitive disorders.
4. Compare possible etiologies of various cognitive disorders, especiallyAlzheimer’s disease.
5. Explain the continuum of care and interdisciplinary treatment/management for clients and families dealing with cognitive disorders.
6. Discuss common interventions for cognitive disorders.
7. Apply the steps of the nursing process to care for clients with cognitive disorders.
Cognitive DisordersAnita Amelia Thompson Heisterman

in a few days to weeks. In contrast, results fromprimary brain pathology that usually is irreversible, chronic,and progressive. Prognosis with dementia depends on whethera cause can be identified and reversed. For example, promptoxygen treatment for dementia stemming from hypoxia canprevent further damage. A comparison of the characteristicsof delirium versus dementia is shown in TABLE 31.1.
With most cognitive disorders, the brain is temporarilyor permanently compromised. Usual consequences includedisturbed perceptions, delusions, paranoia, and aggressiveand disruptive behaviors. Clients may sense that their think-ing is impaired and become frustrated, anxious, frightened,and distraught. High emotion may compound an alreadydisordered state.
Most cognitive disturbances belong to one of the follow-ing categories:
• Primary brain disease• Response of the brain to systemic (eg, metabolic, cardio-
vascular) disturbance• Unique reaction of brain tissue to an exogenous substance• Residual effects of or withdrawal from an exogenous sub-
stance (APA, 2000)
Many illnesses and medications can impair cognition.Any physical illness may present initially with neurologic
dementiaare characterized by adisruption of or deficit in cognitive function, which
encompasses orientation, attention, memory, vocabulary, cal-culation ability, and abstract thinking (see Chap. 10). Specificcategories delineated by the American Psychiatric Associa-tion (APA, 2000) include the following:
1. Delirium, dementia, and amnestic and other cognitivedisorders
2. Mental disorders resulting from a general medical condition (see Chap. 39)
3. Substance-related disorders (see Chap. 30)
This chapter focuses on delirium and dementia. Amnestic dis-orders are covered briefly, in line with their classification inthe Diagnostic and Statistical Manual of Mental Disorders,4th ed., text revision (DSM-IV-TR).
ETIOLOGIC AND DIAGNOSTICCHALLENGES OF COGNITIVEDISORDERS
usually results from an acute disruption in thehomeostasis of the brain. Once the cause of disruption is elim-inated or subsides, related cognitive deficits generally resolve
Delirium
ognitive mental disorders
652 Psychiatric DisorderssixU N I T
C
table
31.1 Delirium Versus Dementia
Characteristic Delirium Dementia
Gradual and insidious developmentLong, with progressive deterioration
Stable progression of symptomatology
Short-term and long-term memoryimpairments, with eventual complete lossProgressively decreases
Difficulty recalling the correct word; latermay lose languageOften absent but can progress to para-noia, delusions, hallucinations, and illusionsNot affected
May develop day-night reverse in laterstagesNot affected initially, late in illness, rest-lessness with pacingDepression/anxiety when insight intocondition is present; late in pathology,anger with outbursts
Rapid developmentBrief duration of 1 month or less, depend-ing on causeDiurnal alterations, more nocturnalexacerbationsDisorganized and impaired
Markedly decreased, especially to environ-mental cuesRambling, pressured, irrelevant
Environment unclear, progressing to illusions,hallucinations, and delusions
Cloudiness that fluctuates; inattentivenessto hyperalert with distractibilityDay–night reversal, insomnia, vivid dreamsand nightmaresSluggish to hyperactive; change of rangeunpredictableAnxious with changes in sleep; fearful ifexperiencing hallucinations; weeping;yelling
OnsetDuration
Course
Thinking and short-termmemoryOrientation
Language
Perceptual disturbance
Level of consciousness
Sleep
Psychomotor actions
Emotional status

Older adults are at significant risk for delirium, particu-larly those with pre-existing cognitive impairment and post-operative clients. With aging, the neurologic system becomesmore vulnerable to insults caused by underlying systemic con-ditions. Indeed, delirium often predicts or accompanies phys-ical illness in older adults (Cole, 2004). This population alsois at risk because of the number of medications (over-the-counter and prescription) many of them use (FIGURE 31.1).Medications, particularly those that exert effects on the CNS,are frequent causes of delirium (Gurwitz et al., 2003).
Any disturbance in any organ or system can disruptoverall metabolism and neurotransmission, leading to cog-nitive decline. Infections and fluid and electrolyte imbal-ances are common examples. Not surprisingly, medicationsare the primary exogenous offenders, especially in olderadults. Often, an interplay of several factors leads to delir-ium (Foreman et al., 2003).
Signs and Symptoms/Diagnostic CriteriaClinical pictures of delirium vary. Nevertheless, the threesalient features that comprise the main diagnostic criteria are(1) disordered cognition, (2) attention deficit, and (3) disturbedconsciousness (DSM-IV-TR BOX 31.1).
In delirium, cognition becomes disorganized. Clientsappear confused and cannot reason, handle complex tasks,or problem-solve. Associated speech may be pressured, ram-bling, bizarre, incoherent, or nearly absent. Impaired orienta-tion and spatial ability may cause clients to confuse realitywith imagery and dreams. Suspiciousness and persecutorydelusions are common (Sadock & Sadock, 2007).
Clients may experience disturbed perceptions. Halluci-nations usually are graphic and can induce anxiety vergingon panic. Agitated clients can become combative to eludeperceived threats. Mood alterations can lead to great lability,from irritability and dysphoria to euphoria (Sadock & Sadock,2007).
Memory, particularly short-term, becomes impaired.Another feature is an inability to focus or shift attention. Clientsmay have trouble attending to environmental stimuli. Atten-tion problems usually are more pronounced at night. Clientsmay be disoriented to time, place, and person (Sadock &Sadock, 2007). In severe cases, they mistake the unfamiliar forthe familiar. For example, they may identify and subsequentlycall healthcare providers by the names of siblings, spouses,or children.
Additional features of delirium include reduced conscious-ness, disrupted sleep–wake cycles, and abnormal psycho-motor behaviors. Clients may fluctuate between alertness andsomnolence. They may be drowsy during the day and nap spo-radically at night, becoming extremely agitated on awakening
symptoms, behavioral manifestations, or both. Thus, cognitivedisorders may be difficult to diagnose and involve multiplevisits to several practitioners, extensive laboratory and diag-nostic tests, and many examinations over an extended period.Such intensive care usually is necessary to establish what iscausing or contributing to the cognitive decline so that health-care providers can initiate appropriate treatment or manage-ment. Failure to treat a reversible condition may cause furtherdamage, functional decline, or death.
Another complication is that multiple factors may under-lie the clinical presentation of a cognitive disorder. For exam-ple, the same client may have Alzheimer’s disease (dementia)and acute intoxication from overmedication (delirium). Ora client with the chronic problem of vascular dementia mayexperience delirium while hospitalized with pneumonia.Dementia itself is a risk factor for delirium. Thus, connectingthe correct etiology and symptoms can challenge the mostcapable clinicians. As a practice standard, any change fromthe client’s baseline functioning is a clue to investigate causesbeyond the primary diagnosis.
DELIRIUMDelirium is characterized by rapid onset of cognitive dys-function and disrupted consciousness. It also is referred toas intensive care unit psychosis, acute brain syndrome, acuteconfusion, and acute toxic psychosis.
Incidence and PrevalenceGrowing rates of delirium mirror the increasing older adultpopulation and are expected to continue to rise. Delirium is themost common psychiatric syndrome in general hospitals,occurring in as many as 50% of elderly inpatients. It is associ-ated with significantly increased morbidity and mortality bothduring and after hospitalization (Balas et al., 2007; McAvayet al., 2006; Rigney, 2006). Approximately 30% to 40% ofclients older than 65 years experience delirium while hospi-talized for a medical condition; another 10% to 15% havedelirium on admission (Sadock & Sadock, 2007). The preva-lence of repeated episodes of acute confusion in nursinghomes for those older than 75 years is 60%; more than 80% ofclients with terminal illnesses experience delirium-relatedcognitive impairment (Sadock & Sadock, 2007).
Delirium related to surgery is common among all agegroups. Estimates are that 30% of clients in surgical intensivecare units, 40% to 50% of clients recovering from hip surgery,and more than 50% of postcardiotomy clients experiencedelirium (Sadock & Sadock, 2007).
EtiologyAny process, disorder, or agent that disrupts integrity of thecentral nervous system (CNS) and diffusely impairs its cellu-lar functioning can induce delirium (BOX 31.1). Researchershave postulated numerous risk factors: aging, postoperativestatus, metabolic disorders, drug withdrawal, and toxicitysecondary to drugs or other exogenous substances.
Cognitive Disorders 65331C H A P T E R
✔C h e c k p o i n t Q u e s t i o n s1. How does delirium differ from dementia?2. What is a frequent cause of delirium in older adults?

(Sadock & Sadock, 2007). Psychomotor activity may rangefrom hypoalert and hypoactive (typical of metabolic dysfunc-tion) to hyperalert and hyperactive (common with drug with-drawal), to any combination. Hypoalert, hypoactive clientsshow minimal activity, appear stuporous, and are slow torespond. Others may mistakenly perceive them to have depres-sion, missing the signs of delirium (Fick et al., 2007). Hyper-alert, hyperactive clients are animated to the point of agitationand frequently have loud and pressured speech. They mayremove intravenous (IV) lines and other tubes, “pick” at the airor sheets, or try (often successfully) to climb over side railsor the ends of beds. In addition, they often exhibit the classic,autonomic responses of dilated pupils, elevated pulse, and di-aphoresis. See CASE VIGNETTE 31.1.
Implications and PrognosisDelirium indicates an underlying medical problem and shouldbe considered an urgent condition. Prognosis for recovery isgood if the cause is recognized and managed promptly. Withearly identification and treatment, delirium usually lasts 3 to5 days but may continue (rarely) for as long as 3 weeks. Fail-ure to reverse the underlying cause may result in irreversiblebrain damage or death.
654 Psychiatric DisorderssixU N I T
box
31.1 Specific Causes of Delirium
Primary Brain Disease• Head injury: concussion, contusion, hemorrhage, vascular
obstruction• Tumors
Systemic Diseases Secondarily Disrupting Brain Homeostasis• Acid-base imbalance• Cancer• Cerebrovascular accident• Dehydration• Endocrine disorders: diabetes (hypoglycemia), hypothyroidism,
or hyperthyroidism• Epilepsy• Fever from any cause• Hypokalemia• Hypoperfusion of the brain: myocardial infarction, dysrhyth-
mia, congestive heart failure, vascular hypotension• Hypoproteinemia• Hypotension with cerebral ischemia• Hypothermia or hyperthermia• Hypoxia producing chronic obstructive pulmonary disease,
anemia, gastrointestinal bleeding• Infections: bacteremia, septicemia, urinary tract infection,
upper respiratory infection• Malnutrition• Organ failure: hepatic, renal, pulmonary• Postoperative state• Sodium depletion• Trauma: burns, hip fracture
• Uremia• Vitamin deficiencies
Withdrawal of Exogenous Substances of Abuse• Alcohol• Barbiturates• Sedative-hypnotics• Tranquilizers
Brain Toxic Exogenous Substances• Anticholinergic drugs• Antidepressants: amitriptyline, doxepin• Antidiarrheal agents: diphenoxylate• Antidysrhythmic drugs: lidocaine, amiodarone, propranolol,
digitalis• Antihistamines• Antihypertensives: methyldopa• Antimicrobials• Antiparkinsonian agents• Antipsychotics: chlorpromazine, thioridazine• Cimetadine• Corticosteroids• Digitalis glycosides• Diuretics• Narcotic analgesics: meperidine, pentazocine• Neuroleptics• Nonsteroidal anti-inflammatory agents: indomethacin• Over-the-counter cold and cough medications• Psychiatric medications: diazepam, flurazepam, tricyclic
antidepressants, benzodiazepines• Xanthines: caffeine, theophylline
figure 31.1 Older adults and other clients who use multiplemedications are at risk for experiencing delirium. The confu-sion can develop as a side effect, an adverse reaction, aninteraction among drugs or with foods or other substances,or as an idiosyncratic response.

Cognitive Disorders 65531C H A P T E R
Delirium Due to a General Medical Condition
• The client has disturbed consciousness (reduced environ-mental awareness) and decreased capacity to focus, sustain, or shift attention.
• Cognition changes (eg, memory deficit, disorientation, language disturbance) or perceptual disturbances are notbetter explained by a pre-existing, established, or evolvingdementia.
• The change or disturbance develops quickly (usually hoursto days) and tends to fluctuate.
• Evidence from the history, physical examination, or lab-oratory tests supports that the disturbance is caused by a general medical condition.
Substance-withdrawal Delirium
• Consciousness is disturbed; ability to focus, sustain, orshift attention is reduced.
• Cognition changes or perceptual disturbances are not betterexplained by a pre-existing, established, or evolving dementia.
• The disturbance develops quickly (usually hours to days)and tends to fluctuate.
• Evidence from the history, physical examination, or labora-tory tests supports that symptoms developed during orshortly after a withdrawal syndrome.
Substance-intoxication Delirium
• Consciousness is disturbed, and ability to focus, sustain,or shift attention is reduced.
D S M - I V - T R B O X 3 1 . 1
Delirium• Cognition changes or perceptual disturbances are not
better explained by a pre-existing, established, or evolvingdementia.
• The disturbance develops quickly (usually hours to days)and tends to fluctuate.
• Evidence from the history, physical examination, or labora-tory tests supports either (1) symptoms developed duringsubstance intoxication or (2) medication use is related tothe disturbance.
Delirium Due to Multiple Etiologies
• Consciousness is disturbed, and ability to focus, sustain,or shift attention is reduced.
• Cognition changes or perceptual disturbances are not better explained by a pre-existing, established, or evolvingdementia.
• The disturbance develops quickly (usually hours to days)and tends to fluctuate.
• Evidence from the history, physical examination, or labora-tory tests supports more than one etiology (eg, a medicalcondition and substance intoxication).
Delirium Not Otherwise Specified
The client’s delirium does not meet criteria for any specifictype of delirium. For example, clinical presentation is sus-pected to result from a medical condition or substance, butevidence to establish a specific etiology is insufficient.
Adapted with permission from the American Psychiatric Association (APA). (2000). Diagnostic and statistical manual of mental disorders (4th ed., text rev.). Washington, DC: Author.
Case Vignette 31.1
The physician orders computed tomography (CT) scan-ning to rule out a possible brain injury sustained in the initialfall. He also orders chest radiography and a urine culture.Results of the CT scan and chest radiography are normal;however, the urine culture reveals a urinary tract infection.The physician prescribes antibiotics to treat it and haloperidol,as needed, for the agitation.
Reflection and Critical Thinking
• What risk factors did Meredith have for experiencing delirium?• How is Meredith’s experience consistent with the etiology
and clinical features of delirium? Could anything havebeen done to prevent this episode?
M eredith, 75 years old and frail, is admit-ted to the hospital with a hip fracture. She undergoessurgery on a general unit to repair the hip. Postoperatively,she initially appears alert and oriented, although she is in pain. She is receiving intravenous fluids and has anindwelling urinary catheter, both of which are to be discontinued in the morning.
The evening of the first postoperative day, Meredithtells the nurse that bugs are on the walls and that shewants to leave “this place.” Upon further questioning,Meredith becomes mildly agitated and tells the nurse to“get out!” The nurse notifies the physician of the change inMeredith’s mental status.

Clear and concise explanations for interventions also helpto allay anxiety and promote orientation. Empathetic expres-sions of concern can ease clients’ and relatives’ fears. Theyalso help to address the delirious symptoms of impaired mem-ory and emotional problems. It is better to express empathyand choose interventions that allay anxiety than to be con-frontational and, for instance, dispute possible delusions.
Team members must keep families informed and includedin treatment plans. Relatives need to understand the biologicbasis for the behavior that they witness in their loved ones.Helping them to understand the difference between deliriumand dementia can be reassuring. Staff also should encouragerelatives to join in efforts to reorient clients.
Interdisciplinary Goals and TreatmentInterdisciplinary goals are to identify clients at risk for delir-ium, recognize early signs, and quickly institute measures tocorrect underlying causes. In addition to early diagnosis andprompt treatment, therapeutic goals include managing acuteconfusion to maximize cognitive function, avoid injury, andprevent further decline.
Medical InterventionsMedical interventions focus on the underlying cause and thusvary. In cases of hypoperfusion or cerebral hypoxia, supple-mental oxygen may significantly improve delirious symptoms.Similarly, withdrawing medications or giving antibiotics forinfections may lead to improvement.
Environmental InterventionsTeam members must avoid use of physical and chemicalrestraints as much as possible. When these measures areabsolutely necessary, they require utmost caution. The impe-tus for chemical or physical restraint clearly must be to pro-tect clients from harm. Indeed, any type of restraint is a riskfactor for, and may compound, delirium.
The team structures the environment to ensure safetyas well as to maximize cognitive abilities and psychologicalcomfort for clients. A fine balance exists between overstim-ulation and understimulation. Tailoring the environment toenhance the client’s cognitive capability is essential. Provid-ing a private room is beneficial, so that staff can minimizenoxious and confusing environmental stimuli and maximizethe services of supportive family or staff who can continuallyremain with clients. However, the healthcare team cannotcompletely extinguish stimuli. Doing so may cause clients towithdraw and focus internally. Television often inundatesclients with confusing sensory input, whereas soft music pro-vides appropriate stimulation. Adequate lighting during theday and evening promotes realistic environmental percep-tions. Clients should use any sensory aids (eg, glasses, hear-ing aids) that they normally require.
Client safety during episodes of delirium must not becompromised. Staff must be alerted if clients are at risk forwandering or leaving the premises. The propensity of clientswith delirium to pull tubes, climb over side rails, or fall mayrequire staff to institute one-on-one observation or encouragerelatives to stay with clients at all times (FIGURE 31.2). Con-sistency from staff in terms of assignments and unhurried,daily routines is helpful, as are continuous visits by loved ones.Encouraging relatives to bring familiar objects from home(eg, personal effects, photographs) can increase the comfortlevel of clients with their current environment.
Cognitive and Psychosocial InterventionsStaff members can try to direct activity and cognitive focus byreorienting clients to the environment with calendars, clocks,and seasonal decorations. Ongoing interactions with clients areimportant. Therapeutic communication about the day’s activi-ties, repetition of explanations for the hospitalization, and re-assurance that any hallucinations and delusions are part of thetransient condition of delirium are helpful to clients.
656 Psychiatric DisorderssixU N I T
figure 31.2 Clients with delirium may require one-on-oneobservation from a healthcare provider or relative to main-tain their safety and prevent falls, aggressive behavior, orother negative consequences.
✔C h e c k p o i n t Q u e s t i o n s3. What are the components of cognition?4. For approximately how long does delirium typically
last?
A P P L Y I N G T H E N U R S I N G P R O C E S SA P P L Y I N G T H E N U R S I N G P R O C E S S
Delirium
● A S S E S S M E N TEarly assessment of acute confusion is essential nursing carefor all hospitalized clients, particularly older adults. Nurses arein an ideal position to detect delirium. Prompt recognitionand subsequent identification and treatment of underlying

● N U R S I N G D I A G N O S I SNursing diagnoses common to clients with delirium includethe following (NANDA-I, 2007):
Acute Confusion related to delirium of known orunknown etiologyRisk for Injury related to confusion and cognitive deficitsBathing/Hygiene, Toileting, Feeding, and Dressing/Grooming Self-Care Deficit related to cognitive impairmentDeficient Knowledge of family related to client diagno-sis, progression, and prognosis
● O U T C O M E I D E N T I F I C A T I O N A N D P L A N N I N G
Planning is a collaborative effort of the entire treatment teamin conjunction with family and clients (as able). Nurses mustdeliberately design the plan of care to meet each client’sunique needs. General goals of care for clients with delirium,linked to the Nursing Outcomes Classification (NOC), are asfollows (Moorhead et al., 2008):
Risk Control: The client will remain physically safe.Self-Care: Activities of Daily Living: The client’s basicneeds will be met until self-care ability resumes.Cognitive Orientation: The client will return to baselinecognitive functioning.
causes can prevent deleterious effects, as well as the pro-gression and ramifications of acute confusion.
All clients should undergo a baseline neurologic exami-nation at the onset of care for any illness. Clients atincreased risk for delirium (eg, older adults, those with headinjury) should have mental status examinations (MSEs) rou-tinely throughout treatment (see Chap. 10). Nurses shouldevaluate for delirium in clients who show subtle or overtchanges from baseline in mental status, orientation, or levelof consciousness.
Use of systematic assessment and screening tools canenhance detection and management. The Delirium Observa-tion Screening Scale (DOS) is a useful 25-item tool basedon DSM-IV-TR criteria (Schuurmans et al., 2003). The Regis-tered Nurses Association of Ontario (RNAO, 2003) has rec-ommended the widely used Confusion Assessment Method(CAM) in its practice guidelines. The CAM focuses on (1) acuteonset and fluctuating course of the condition, (2) inattention,(3) disorganized thinking, and (4) altered level of conscious-ness. Both the DOS and the CAM are specific to delirium.The Folstein Mini-Mental State Examination (MMSE) is excel-lent for evaluating cognitive function; however, it does notdifferentiate delirium from dementia. It includes questionsthat test orientation, attention span, recall, and ability toexecute simple instructions. The MMSE also can be used in conjunction with the DOS or CAM to test the client’simprovement or deterioration (ASSESSMENT TOOL 31.1). Oncedelirium is diagnosed and as treatment progresses, ongoingassessment of mental status is necessary to monitor theclient’s recovery.
In addition to experiencing cognitive changes, disorientedclients are likely to be anxious and emotionally distraught.Nurses assess for any changes in anxiety level. If anxietyescalates to overt agitation, clients can become dangerous toself and others. Carefully assessing anxiety and watching forsigns of agitation (eg, increased motor activity, labile mood,combativeness) can alert staff to the need for interventionsthat increase psychological comfort and decrease the poten-tial for danger.
Nurses also monitor the client’s ability to perform dailyself-care. Confused clients may be too distracted to eat ordrink adequately; they may be inattentive to hygiene. On-going assessment of functional ability is necessary for theircomfort and physical well-being.
Cognitive Disorders 65731C H A P T E R
?T h i n k A b o u t I t 3 1 . 1James Serby brings his 75-year-old wife, Helen, to theclinic. She has a history of Parkinson’s disease anddiabetes. Mr. Serby states that his wife hasn’t seemedherself for the last few days. She is lethargic duringthe day and sometimes seems confused. He states herblood glucose levels have been elevated and that shefrequently has been incontinent of urine. The nurseevaluates Mrs. Serby’s mental status. The client is notsure of the day or year and has trouble with short-termmemory. Is the client experiencing delirium or demen-tia? Provide support for your conclusion. Explain whatMrs. Serby’s priority need is and why.
• What is the year?• What is today’s date?• In what city (town) are we?• Spell “globe” backward.
A S S E S S M E N T T O O L 3 1 . 1
Sample Mini-Mental Status Examination Questions• Repeat the following statement:
“A rolling stone gathers no moss.”• Write a sentence of your own choice. (Nurse evaluates
whether sentence has a subject, predicate [verb], and object.)
Questions adapted from Folstein, M. E., Folstein, S. E., & McHugh, P. R. (1975). Mini-Mental State: A practical method for grading the cognitive state of patients for the clinician. Journal of PsychiatricResearch, 12(189), 189–198. Used with permission.

may be disoriented, they often recognize and are reassuredby the presence of supportive relatives. Staff and familyshould reinforce the predictability of routines by tellingclients what they are doing, what to expect, the time of day,and other relevant data as they proceed with activities. Consistency is stabilizing for these clients.
Directed activity may be helpful. Agitated clients maybenefit from psychomotor tasks that distract them from anxi-ety. Bags with familiar items to “pack” and “unpack,” Velcroto fasten and unfasten, and zippers to open and close pro-vide sensory stimulation at a level adjusted to the client’scompromised function. However, because inability to focusand attend to tasks is a hallmark of delirium, not all clientscan or should participate in such activity.
Nurses approach clients calmly and empathetically, call-ing them by name and introducing themselves to facilitateattention and correct interpretation. They also are carefulnot to approach clients from behind, which allows minimaltime to make adjustments. So that clients do not becomefrustrated, nurses avoid frequently quizzing them about ori-entation or posing questions that require decision making orabstract thinking. Instead, family and staff communicate insimple, direct sentences and focus on what is meaningfulto clients.
Because clouded consciousness waxes and wanes,nurses never should assume that clients do not need or willnot understand explanations. Recognizing their fears is help-ful. Nurses may respond to fear with “It must be difficult tobe so frightened, but I want you to know that I will not gofar and I will do what needs to be done to keep you safe.”Nurses must accept the sometimes bizarre behavior ofclients with delirium and not demean or correct them foractions that they cannot control (CHALLENGING BEHAVIORS 31.1).
Occasionally, clients become so agitated that they needmedication. Staff members must seriously consider thisoption when a client’s behavior threatens the safety of self,family, or staff. Haloperidol (Haldol), a neuroleptic giveneither orally or by injection, is most commonly used forsymptoms of delirium. It has minimal anticholinergic effectsand does not cause the serious cardiovascular and respiratoryside effects found with some other classes of antipsychotics.Extrapyramidal side effects are possible (Lacasse et al., 2006).Haloperidol is inexpensive and can be given orally in concen-trated form at 1 to 2 mg every 2 to 4 hours. Older adultsshould receive 0.25 to 0.5 mg every 4 hours.
Atypical antipsychotics, including quetiapine (Seroquel),risperidone (Risperdal), olanzapine (Zyprexa), aripiprazole(Abilify), and ziprasidone (Geodon), occasionally are used to treat agitation related to cognitive disorders. Olanzapine,risperidone, and ziprasidone are available as intramuscularinjections. Although considered first-line treatments for agita-tion related to dementia, they have not yet been adequatelyand systematically studied to support short-term use overhaloperidol for acute agitation in delirium (Alexopoulos et al.,2004). In fact, all antipsychotics, including Haldol, havewarnings from the U.S. Food and Drug Administration (FDA)regarding potential cardiac events in older adults from pro-
● I M P L E M E N T A T I O NCommon Nursing Interventions Classification (NIC) labelsrelated to management of delirium include, but are not limited to, Anxiety Reduction, Delirium Management, Environmental Management: Safety, Fall Prevention,Reality Orientation and Self-Care Assistance (Bulecheket al., 2008).
Managing Symptoms of DeliriumPrimary nursing interventions for delirium involve addressingthe underlying cause and preventing further decline. Safety,hydration, nutrition, comfort, and pain management are coreelements of care (Foreman et al., 2003). Simple physicaland psychological comfort measures such as warmth, com-panionship, fluid provision, and reassurance are elemental(FIGURE 31.3).
Pain, too many stimuli, abrupt changes in routine, poorsleep, and insensitivity from others easily can worsen confu-sion and agitation. Nurses perform many activities to help pro-mote a therapeutic milieu for those with acute confusion. Infact, environmental management is one of the most influentialinterventions for this condition. Confused clients are calmerwhen nurses eliminate stimuli that invite misinterpretation,such as abstract pictures or excessive noise. Conversely, cuessuch as clocks, recognizable photos, and calendars helprestore orientation to time and place. One caveat is to avoidan understimulating environment, which also can be detri-mental. The key is to remove difficult-to-interpret cues andreplace them with simple, easy-to-recognize ones.
Confused clients also benefit from consistent routinesimplemented by familiar staff or family. Even though clients
658 Psychiatric DisorderssixU N I T
figure 31.3 Addressing comfort, pain management, andother basic human needs is a core nursing intervention forclients with delirium.

option, nurses should identify the reason for use and findalternatives, such as providing the presence of loved ones,consistent caregivers, and attention to sleep, nutrition, toilet-ing, and pain (O’Connell & Mion, 2003; Park et al., 2005).Because foreseeing all potential environmental dangers isimpossible, nurses frequently check on these clients. Attimes, even this level of care is insufficient. Nurses may askrelatives to stay with loved ones, especially at night or duringmore agitated periods.
Assisting With Personal CareThe distractibility and cognitive disorganization of clientswith delirium may seriously hamper their ability to maintainADLs. Potential consequences include poor nutrition andhydration, discomfort from wet clothing, skin breakdown,and immobility. Nurses must support the efforts of clientsto carry out whatever activities of daily living (ADLs) theycan, as well as assume responsibility for those necessaryactivities that clients cannot manage. Establishing a routineto carry out activities also is helpful to confused clients. Thisroutine should include regular toileting, offering fluids andfood, and providing an opportunity for passive or activeexercise (FIGURE 31.4).
Providing Client and Family EducationClients who realize that their thinking is disordered may befrightened. Nurses must explain the nature of delirium.Clients and families need to realize that associated confusionand abnormal behavior have a biologic basis and are tran-sient. Explaining the process, progress, and prognosis ofdelirium should alleviate some anxiety and apprehension.The team must continually update family as to the state ofthe underlying problem and the progress being made toresolve it. Relatives need to become partners with the teamin planning care and implementing some interventions, suchas reorientation.
longation of the Q-T interval. Expert consensus guidelinesrecommend tapering use of antipsychotics over 1 weekonce delirium has been stabilized (Alexopoulos et al., 2004).
For clients with hepatic dysfunction, lorazepam (Ativan)orally, intramuscularly, or intravenously may be used indoses from 0.5 to 2 mg. Lorazepam can affect respiratoryand cardiac function; thus, nurses must monitor clients tak-ing it. In some instances, lorazepam increases agitation andmust be discontinued. Its use is most appropriate duringalcohol withdrawal and for short-term treatment of anxiety(Alexopoulos et al., 2005).
Providing a Safe EnvironmentBecause clients with clouded cognition are likely to misinter-pret environmental clues, they are vulnerable to harm. Manyalso behave unsafely, such as pulling out tubes or wanderingfrom units. Making the environment safe helps prevent harmthat might result from confusion. Nurses place personal andfamiliar items (eg, call light, water pitcher, eyeglasses) closeat hand so that clients are not injured while attempting to getthem. Clients with delirium have sustained significant injuriesby wandering into traffic, falling down stairs, or getting lost.Alerting staff and family to the possibility that clients mayescape or wander and arranging for continuous observationif necessary helps prevent accidents.
Many clients with delirium, especially older adults, areinjured climbing over raised bed rails. Beds should remain inthe lowest position with rails down unless policy demandsotherwise. Regular toileting may help prevent clients fromattempting to get out of bed alone. Lighting needs to bebright enough so clients can see accurately. This is especiallyimportant at night and significant for older adults who needbrighter light to see at all.
Nurses should not use restraints. Physical limitationmay cause clients to become agitated and fearful, whichincreases stress and risk for injury. If restraints are the only
Cognitive Disorders 65931C H A P T E R
Strategy: The client needs immediate action to remain safeand to determine the etiology of her delirium. The multi-disciplinary team assesses all biopsychosocial elements pos-sible and institutes measures to reverse the acute confusion.The nurse assesses for pain.
Nurse Action/Communication: Assign someone to staywith the client. Do not use restraints. Move her away fromsome of the stimulation of the ED if possible. Explain proce-dures clearly and concisely and offer reassurance. You mightsay, “I imagine you are feeling quite afraid right now. Youare in the emergency department of the hospital. We willkeep you safe.”
Challenging Behaviors 31.1The Client Who Has Acute Confusion
Situation: Your assigned client has just arrived in the emer-gency department (ED). She is an 81-year-old woman whois emaciated, dirty, disheveled, and odiferous. She is yelling“Help me. Help me.” At other times, she is difficult to arouse.She picks at her clothing and is attempting to get off thestretcher.
Your Potential Feelings: Anxiety, concern, repugnance
What Is Going On? The client is delirious from an unknownetiology. She cannot focus her attention, and her conscious-ness waxes and wanes. The top three culprits that cause delir-ium are medications, infections, and metabolic disturbances.
Incidence and PrevalenceThe U.S. National Institute of Neurological Disorders (NationalInstitute of Neurological Disorders and Stroke [NINDS], 2007)reports that at least 6.8 million people have chronic cognitiveimpairment related to dementia; in some communities 50% ofthose 85 years or older have dementia. Given that those olderthan 85 years are the fastest-growing segment of older adultsand that the large cohort born after World War II is now enter-ing its seventh decade, incidence and prevalence of demen-tia are likely to increase. See HEALTHY PEOPLE 2010 31.1 fornational objectives related to dementia and other cognitivedisorders.
Signs and Symptoms/Diagnostic CriteriaThe clinical presentations of disorders within the subcategoryof dementia do not differ significantly. All are characterizedby ongoing multiple cognitive deficits, memory impairmentsevere enough to compromise social or occupational func-tion, and decline from previous functioning (APA, 2000). Thedistinctiveness of the disorders arises from their differing ori-gins (DSM-IV-TR BOX 31.2).
● E V A L U A T I O NAs stated previously, signs and symptoms of delirium mayfluctuate each day. A perspective on how well clients arerecovering may evolve over several days. Because clientshave varying baseline cognitive function, nurses evaluateeach person’s progress according to previous level. Indica-tors of resolving confusion include the following:
Improved score on the chosen assessment scale (CAM,DOS, or MMSE)Improved ability to communicateIncreased ability to focus attentionIncreased ability to make decisionsReduced delusional behaviorImproved ability to care for selfDecreased anxiety and agitation
DEMENTIADementia is the term used for a syndrome characterized byseveral cognitive deficits that result from a general medicalcondition, use of a substance, or multiple biologic etiologies.Although there are several types, all forms of dementia affectmemory and cognition.
660 Psychiatric DisorderssixU N I T
figure 31.4 The nurse is performing passive range-of-motionexercises for a hospitalized client with episodic delirium topreserve overall health.
✔C h e c k p o i n t Q u e s t i o n s5. What medication is used most commonly to treat
the symptoms of delirium?6. Why should restraints be avoided as much as
possible in clients with delirium?
1-1. Increase the proportion of persons with health insurance.
1-4. Increase the proportion of persons who have a specificsource of ongoing care.
1-6. Reduce the proportion of families that experience diffi-culties or delays in obtaining healthcare or do not receiveneeded care for one or more family members.
1-15. Increase the proportion of persons with long-term careneeds who have access to the continuum of long-term careservices.
17-3. Increase the proportion of primary care providers,pharmacists, and other healthcare professionals who routinely review with their patients aged 65 years andolder and patients with chronic illnesses or disabilities all new prescribed and over-the-counter medicines.
18-6. Increase the number of persons seen in primaryhealthcare who receive mental health screening andassessment.
18-9. Increase the proportion of adults with mental disorderswho receive treatment.
18-14. Increase the number of states, territories, and theDistrict of Columbia with an operational mental health planthat addresses mental health crisis interventions, ongoingscreening, and treatment services for elderly persons.
H E A L T H Y P E O P L E 2 0 1 0 3 1 . 1
Objectives Related to Cognitive Disorders
From U.S. Department of Health and Human Services (USDHHS).(2007). Healthy People 2010. Retrieved July 18, 2007, fromhttp://www.healthypeople.gov.

Impaired ReasoningDementia affects reasoning. Clients no longer seem able torespond to everyday problems at work or home. Ultimately,their thought processes degenerate so much that they showsignificant deficits in abstract thinking. They cannot cogni-tively adapt to new situations. This impairment severely lim-its their competence to adjust to the dynamics of life (APA,2000). For example, if the bathroom at home floods, a clientwith dementia may be in a quandary about how to respond.Clients also may begin to exhibit uncharacteristic disregardfor social conduct. For example, they may disrobe in public,exhibit inappropriate sexual behavior, suddenly use profan-ity, and strike out at others when frustrated. Families find suchchanges alarming and distressing.
Compromised Spatial Ability and OrientationBecause their ability to process sensory information dimin-ishes, clients gradually begin to experience confusion, which
Impaired LearningMemory impairment significantly affects the relationships andwork of clients with dementia. It encompasses the ability tolearn and retain new material (short-term memory) as well asto recall previously learned information (long-term memory)(APA, 2000). Clients become repetitive and have difficultyremembering recent conversations, events, and appointments.They continually lose things. They may attempt to compen-sate for these lapses.
Compromised Ability for Complex TasksThe chronic and degenerative nature of dementia causes sig-nificant deficiencies. Well-preserved social skills and attemptsto conceal impairments often obscure clients’ mental deterio-ration and mislead clinicians (Geldmacher, 2007). Familymembers often first recognize cognitive problems when lovedones have difficulties with routine activities: meal planning,managing checkbooks, driving, and using the telephone.
Cognitive Disorders 66131C H A P T E R
Dementia of the Alzheimer’s Type
• Client has multiple cognitive deficits manifested by both:1. Impaired memory (either for new or previously learned
information)2. One (or more) of the following: aphasia, apraxia, agnosia,
disturbed executive functioning• Cognitive deficits significantly impair social or occupational
functioning and represent a significant decline from previ-ous levels.
• The course is characterized by gradual onset and continu-ing cognitive decline.
• The cognitive deficits are not from other CNS conditionsthat cause progressive deficits in memory and cognition,systemic conditions known to cause dementia, or substance-induced conditions.
• The deficits do not occur exclusively during delirium.• The disturbance is not better explained by another Axis I
disorder (eg, schizophrenia).
Vascular Dementia
• The client develops multiple cognitive deficits manifestedby both:1. Impaired memory (for either new or previously learned
information)2. One (or more) of the following: aphasia, apraxia, agnosia,
disturbed executive functioning• Cognitive deficits significantly impair social or occupational
functioning and represent a significant decline from previ-ous levels.
D S M - I V - T R B O X 3 1 . 2
Dementia• Focal neurologic signs and symptoms (eg, exaggerated
deep tendon reflexes, extensor plantar response, pseudo-bulbar palsy, gait abnormalities, extremity weakness) orlaboratory evidence indicate cerebrovascular disease (eg, multiple infarctions involving cortex and underlyingwhite matter) judged to be etiologically related to the disturbance.
• Deficits do not occur exclusively during delirium.
Dementia Due to Medical Conditions
• Client develops multiple cognitive deficits manifested by both:1. Impaired memory (for either new or previously learned
information)2. One (or more) of the following: aphasia, apraxia, agnosia,
disturbed executive functioning• The cognitive deficits significantly impair social or occupa-
tional functioning and represent a significant decline fromprevious levels.
• Evidence from the history, physical examination, or lab-oratory tests indicates that the disturbance is caused by a medical condition other than Alzheimer’s disease or vas-cular dementia (eg, HIV infection, Parkinson’s disease,Huntington’s chorea, Pick’s disease, Creutzfeldt-Jakob disease).
• The deficits do not occur exclusively during delirium.
Adapted with permission from the American Psychiatric Association (APA). (2000). Diagnostic and statistical manual of mental disorders (4th ed., text rev.). Washington, DC: Author.

pumpkin). In addition, they may have difficulty followingconversations.
Behavioral ProblemsBehavior refers to individual responses to continual internaland external changes and to the brain’s physiologic sound-ness. When something interferes with or interrupts brainintegrity, maladaptive behavior often follows. This behavioris not to be confused with that of delirium, even though aber-rant behavior is a hallmark of both conditions.
No key behavioral characteristic occurs in every clientwith dementia, but most changes become more pronouncedafter sunset (a phenomenon known as ). Clientsmay become more irritable and suspicious and misinterpretvisual or auditory cues. Because of their diffuse cognitiveimpairment, they may experience illusions and hallucinations(see Chap. 29). Family members may report that loved oneshave developed poor hygiene and become defensive or apa-thetic. Clients may find that they cannot perform motor tasks(eg, brushing the teeth, combing the hair) despite intact motorfunction, a condition known as (APA, 2000).apraxia
sundowning
Types of DementiaTABLE 31.2 compares the characteristics of the most commonforms of dementia. Alzheimer’s disease is discussed in the mostdetail below because of its frequency and growing emergenceas a national health problem.
Alzheimer’s DiseaseAlzheimer’s disease (AD) is the most prevalent form ofdementia. Approximately 4.5 million Americans have it, anumber that has more than doubled since 1980 (Hebert et al.,2003). Incidence and prevalence directly correlate withincreased age. The illness occurs in 10% of people 65 yearsor older and rises to nearly 50% of those 85 years or older. Asthe population continues to grow and age, the number ofpeople with AD will likely reach 11 to 16 million by 2050(Hebert et al., 2003).
The incidence of AD is higher in women than in men,which may be because women outlive men. According to theNational Institute on Aging (NIA, 2007), approximately 10%of cases are familial and result from mutations on chromo-somes 1, 14, and 21. Familial AD (FAD) always has an onsetbefore 65 years.
ETIOLOGICAL FACTORS. Hallmark pathologic featuresof AD are neurofibrillary tangles and beta-amyloid plaques
affects attentiveness to the environment. As consciousnessdecreases, clients cannot concentrate, their attention spanprogressively declines, and they become distractible. Theyalso may become disoriented. Eventually, they can no longerrecognize or identify familiar objects (eg, parts of a tele-phone), a condition called . When sensory input fallsbelow certain minimum requirements and when the brain isaffected structurally so that it no longer perceives and inter-prets stimuli adequately, orientation decreases.
Disorientation and problems with spatial ability can makedriving a point of contention. Relatives often recognize thataffected clients are no longer safe drivers. Clients who con-tinue driving may do so aimlessly for hours, unable to find theirway home. Nevertheless, they usually have little insight intothis declining ability.
Clients with dementia seem unable to organize itemsaround the house. They get lost and cannot find their wayaround their neighborhood or home. They do not know wherethey are, how they came to be there, why they are there, orhow they fit into the milieu. One man with early-stage demen-tia described his experience as having lost his “internal roadmap.” Getting lost in a familiar place is often the incident rel-atives identify as the onset of dementia in loved ones.
Language DeficitsFrequently, clients with dementia have difficulty findingthe words they want to use ( ) in conversation (FIG-URE 31.5). This problem can result in a frustrating processof “charades,” relying on others to guess the forgotten word(eg, referring to Thanksgiving as the time of the turkey or
aphasia
agnosia
662 Psychiatric DisorderssixU N I T
figure 31.5 Aphasia, or difficulty finding words and language,is a hallmark finding with dementia. It can be one of the mostfrustrating and challenging symptoms for clients.
✔C h e c k p o i n t Q u e s t i o n s7. What term denotes the loss of the ability to recognize
familiar objects?8. When do most behaviors become more pronounced
in clients with dementia?

that destroys ACh) have shown efficacy in slowing AD (Birkset al., 2000; Birks & Harvey, 2006). Thus, neuronal destruc-tion and resulting disruption of ACh transmission are involvedin the elusive etiology of AD.
Extensive research continues to unravel the mysteriousetiology of AD. Multiple and diverse studies are investigatingthe role of genetics, inflammation, oxidative stress, vascular
in the brain on postmortem examination (UNDERSTANDING
BIOLOGIC FOUNDATIONS 31.1). In fact, AD is definitivelydiagnosed according to these findings. The disease results inneuronal death and disrupted neurotransmission. Especiallyaffected is acetylcholine (ACh), a critically important neuro-transmitter for memory and cognition. Clinical studies withacetylcholinesterase inhibitors (drugs that inhibit the enzyme
Cognitive Disorders 66331C H A P T E R
table
31.2 Comparative Assessment for Cognitive Disorders
Level ofCognition Consciousness Memory Appearance Emotions
Clouding late indisease; short-term memoryloss initially pro-gressing to bothshort-term andlong-term loss
Not affected
Choreiformmovements
Suspended intimeRecall limits to2–3 minExtensive memory lossDoes not handlenew situationswell
Initially depres-sion and anxietyabout recognizedregression,progressing to loss or severedampening ofemotionsSubtle loss of interest in workInability to rec-ognize familymembersDramatic personal-ity changesSocially inappropri-ate behaviorFlippant beyondreasonableproprietyMood swings fromapathy to aggres-sive behaviorInappropriatebehaviorDespair aboutchanges takingplaceSuicidaltendenciesDecreased interestin jobCommunicationimpaired related tomemory gapsConfabulation
Depression orpseudo-depression
Progressive lossof groominghabits as a resultof forgotten socialbehaviors anddecreasing coor-dination requiredto dress
Very poorhygiene
Disheveled
Unsteady gaitfrom peripheralneuropathies
Deterioration of hygienic standards
Alzheimer’sdisease
Pick’s disease
Huntington’schorea
Wernicke-Korsakoffsyndrome
Vasculardementia
Insidious onsetcharacterized ini-tially by “mistakesin judgment,”progressing to inability tocomprehend,agraphia, apha-sia, and finally tounresponsiveness
Lack of insightinto diseaseprocess
Increasingly aproblem aspathologyprogresses butwithout aphasia,agnosia, or apraxia
AlertCannot learn newor recall previ-ously learnedmaterial
Proceeds in astepwise pro-gression as mini-strokes occur
Global intellec-tual impairment
Intellect intact
Insight into thepsychologicaldegenerativechanges
Cannot learnnew informa-tion because ofan inability toretain facts
Not affected

664 Psychiatric DisorderssixU N I T
U N D E R S T A N D I N G B I O L O G I C F O U N D A T I O N S 3 1 . 1
Neurologic Alterations in Alzheimer’s Disease
Neurofibrillary tangles. The microscopicstudy image shows normal neurons versus thecharacteristic tangles of AD.
Cortical atrophy. Compare the normal brainon the left with the brain ravaged by AD onthe right.
Brain scans. Dark bluish purple areas signifyareas of lost brain activity. Compare the multi-colored normal brain scan on the left with thevast bluish regions found in the client with ADon the right.
Neurofibrillarytangle
Normal neurons
NORMAL AD
NORMAL AD

drome (defect in chromosome 21); those with FAD havemutations on chromosomes 1, 14, and 21. Even those withnonfamilial or sporadic AD seem at increased risk if theycarry the apolipoprotein E (apoE) gene on chromosome 19.This gene has three forms, and having an apoE4 gene fromboth parents seems to increase risk (NIA, 2007). Searchingfor clues to the formation of beta-amyloid plaques, investiga-tors also are looking at other chromosomes.
Oxidative Stress. Oxidative stress is cellular damage causedby oxygen-free radicals. Some researchers believe that agingresults from oxidative stress. They are attempting to deter-mine if free radicals contribute to the tangles and plaques thatlead to neuron death in AD. Results have been inconclusive;it is unclear whether oxidative stress precedes or results fromthe plaques and tangles (NIA, 2007). Although it has yet tobe replicated, one study demonstrated some benefit of vita-min E, an antioxidant, in slowing the progression of AD (Tabetet al., 2000). Two animal studies found that antioxidants com-bined with behavioral enrichment enhanced cognition in dogs(Milgram et al., 2004, 2005). The practice guidelines of theQuality Standards Subcommittee of the American Academyof Neurology support the use of up to 1,000 IUs of vitamin Etwice a day (Doody et al., 2001). Many clinicians empiricallyprescribe 400 to 800 units of vitamin E with cholinesteraseinhibitors to people diagnosed with dementia.
Immunology. Some studies showing abnormally high anti-body titers in clients with AD raised the possibility of animmunologic etiology. Researchers thought that immuniza-tion could prevent beta-amyloid plaques, leading to a vaccinefor AD. However, clinical trials were discontinued because ofsubsequent inflammation in the brains of some participants.Research continues with the discovery that passive immu-nization removed beta-amyloid from the brains of immunizedmice (NIA, 2007). Similar investigations into the tau proteinsthat make up neurofibrillary tangles have revealed that amodified piece of tau given as a vaccine to mice helped elim-inate tau from the brain (NIA, 2007). Investigators have foundthat specific forms of tau and beta amyloid must be present tocreate conditions leading to AD. Beta amyloid seems to trig-ger various changes that lead to tau alterations, causing anatmosphere that creates tangles that contribute to neuron death(NIMDS, 2007).
Hormones. Researchers have explored hormones, specificallyestrogen, and nerve growth factors. Although initial animalstudies suggested that hormone replacement therapy in post-menopausal women protected against cognitive decline, laterevidence found that women taking combined estrogen andprogestin were at significantly increased risk for dementia(Schumaker et al., 2003). Investigation into nerve growth fac-tors (proteins that regulate neuronal maturation, survival, andrepair) led to the development of memantine (Galantamine),a drug that is beneficial for cognition and function in moder-ate to severe AD (McShane et al., 2006).
Inflammation. Vascular disease and AD share risk factors,so investigators continue to study the relationship between
changes, metabolism, beta-amyloid and tau proteins, lifestylesand education levels, hormones, and growth factors. The eti-ology of AD may be a combination of genetic vulnerabilityand exposure to environmental and psychosocial stressors.Research supported by the NIA has focused not only on eti-ology, but also on risk and protective factors and efforts toslow disease progression.
Ultimately, researchers may find that interacting etiolo-gies are responsible for AD. Certainly, the course of the illnessvaries widely. A person may have biologic markers for AD butshow no symptoms and function well (Snowdon, 2003). AD isconsidered to be clinically heterogeneous; that is, symptoma-tology varies during its average 8- to 10-year course. Variousgroups have attempted to stage the progressive functionaldecline of AD (BOX 31.2). Doing so helps clients, family mem-bers, and healthcare providers to plan for the extensive man-agement necessary for those with the illness.
Genetics. Researchers continue to investigate genetics in AD.The incidence of AD has been associated with Down syn-
Cognitive Disorders 66531C H A P T E R
box
31.2 Stages of Alzheimer’s Disease
Mild
The client:• Frequently repeats himself or herself• Regularly misplaces articles• Cannot recall familiar words to use in conversation• Withdraws from formerly enjoyed activities• Is aware of and frustrated with own “forgetfulness”Changes are not readily apparent to others and often aredenied or excused by family.
Moderate
The client:• Has decreased ability to carry out ADLs and IADLs• Encounters difficulty finding way around neighborhood
and home• Is disoriented to time and place• Shows disruptive behaviors (wandering, pacing)• Has hallucinations and delusions• Cannot perform complex motor activities• Shows problems with visual perception (and thus is
susceptible to accidents)• Needs supervision frequently• Displays temperament fluctuations, from composed and
tranquil to screaming and argumentativeDeterioration is apparent to friends and family.
Severe
The client:• Has lost capacity for self-care and use of language• Has only minimal long-term memory• Must have 24-hour, 7-day-a-week care

ing blood viscosity, modifying neurotransmitters, and reducingthe density of oxygen-free radicals (see Chap. 17). Its efficacyin improving memory is inconclusive and requires furtherresearch (Birks & Grimley-Evans, 2007).
Vascular DementiaThe second most common form of dementia is vasculardementia. Although its overall incidence is considerably lessthan that of AD, some researchers allege that it is the mostcommon dementia in men and in those older than 85 years.Risk factors for vascular dementia parallel those for stroke:hypertension, smoking, hyperlipidemia, atrial fibrillation, anddiabetes. Computed tomography scanning and magnetic res-onance imaging (MRI) often verify the brain disease in thisparticular dementia. On examination clients may have carotidbruits, funduscopic abnormalities, or enlarged heart cham-bers (Sadock & Sadock, 2007).
In vascular dementia, cognitive deficits arise from mul-tiple infarcts in the cortex and white matter of the brain fol-lowing hemorrhage or stroke. Clients experience a faster onsetwith vascular dementia than with AD, and a stepwise or fluc-tuating progression, rather than a steady and gradual deteriora-tion. They show focal neurologic signs. Specific symptomsdepend on the affected brain sectors and the extent of dam-age. Frequently, accompanying neurologic evidence of cerebro-vascular disease includes paresis (limb paralysis) or headaches.Clients with vascular dementia also experience impaired mem-ory, aphasia, apraxia, agnosia, and difficulties with executivefunctioning. Mixed dementias (both vascular and AD) arecommon (NINDS, 2007).
Lewy Body DiseaseLewy body disease is sometimes mistaken for AD because ofclinical similarity but is associated with earlier and moreprominent visual hallucinations, parkinsonian features, anddisturbed behaviors. The exact incidence is unknown becauseonly four population studies have been conducted, but theestimated prevalence of Lewy body disease is 22% of alldementias (Rahknone et al., 2003). On autopsy, Lewy inclu-sion bodies in the cerebral cortex confirm diagnosis. A dis-tinguishing characteristic is significant adverse reactions toantipsychotic drugs (NINDS, 2007).
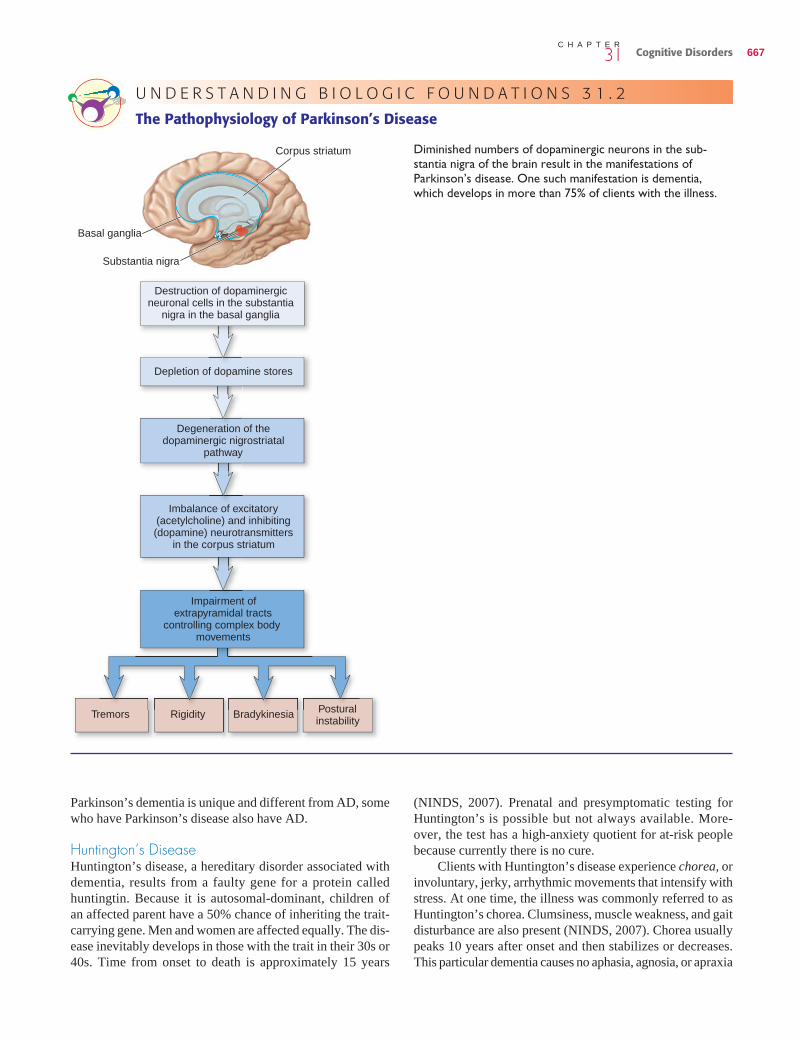
Parkinson’s DiseaseParkinson’s disease progresses slowly and has no knowncure. This neurodegenerative illness affects 1 million Amer-icans. Although its predominant feature is immobility, cog-nitive decline runs concurrently in more than 30% of clients(NINDS, 2007). Decreasing brain cells in the substantia nigraresult in depletion of dopamine (UNDERSTANDING BIOLOGIC
FOUNDATIONS 31.2). Clients exhibit involuntary muscle move-ments at rest, overall slowness, and rigidity. Most often, theyhave postural instability and disturbed gait. Intellectual deficitsvary, but their progression is insidious. Unlike other types,Parkinson’s dementia does not impair language capabilities.It does impair memory retrieval and executive function. While
neuron death from stroke and from AD (NIA, 2007; NINDS,2007). Studies by the NIA (2007) found that the inflamma-tory response following stroke led to rapid formation of beta-amyloid. With a possible relationship between inflammationand AD, some researchers believe that anti-inflammatorymedications (eg, ibuprofen, aspirin) may help prevent AD.Although studies have not clearly supported this notion (Tabet& Feldman, 2003) and guidelines do not support nonsteroidalanti-inflammatory drugs (NSAIDs) as treatment (Doody et al.,2001), some clinicians empirically prescribe them for clientswith AD and no evidence of vascular dementia. Researchersare studying other medications used for cardiovascular treat-ment as preventive drugs against AD (NINDS, 2007). Reportsfrom the longitudinal Honolulu Asia Aging Study indicateincreased formation of plaques and tangles in the brains ofthose with high cholesterol levels. Reducing cholesterol levelswith statins has been shown to prevent pathogenesis associ-ated with AD (Scott & Laake, 2001).
PREVENTIVE FACTORS. Research has not been limitedto biologic etiologies. Incidence of AD is higher among peopleliving in industrialized areas and from lower socioeconomicgroups (NIA, 2007). Many factors could account for these find-ings, including environmental toxins, diet, lifestyle, and stress.Several large epidemiological studies and research initiatives(Abbott et al., 2004; Larson et al., 2006; Podewils et al., 2005;Weuve et al., 2004) have shown a lower incidence of cogni-tive decline in people who regularly exercise. Researchers alsoare investigating the roles of leisure, education, and cognitivestimulation. Frequent participation in cognitively stimulat-ing activities may be associated with decreased incidence ofAD (Snowdon, 2003) (FIGURE 31.6). Similarly, a high level ofeducation may be a protective factor. Although education maystimulate neuronal connections, the finding also could resultfrom the degree of exposure to risk factors associated withsocioeconomic status. The herb ginkgo biloba has manypromising properties, including increasing blood supply, reduc-
666 Psychiatric DisorderssixU N I T
figure 31.6 Ongoing participation in cognitively stimulatingactivities may be protective against the development of AD.
(NINDS, 2007). Prenatal and presymptomatic testing forHuntington’s is possible but not always available. More-over, the test has a high-anxiety quotient for at-risk peoplebecause currently there is no cure.
Clients with Huntington’s disease experience chorea, orinvoluntary, jerky, arrhythmic movements that intensify withstress. At one time, the illness was commonly referred to asHuntington’s chorea. Clumsiness, muscle weakness, and gaitdisturbance are also present (NINDS, 2007). Chorea usuallypeaks 10 years after onset and then stabilizes or decreases.This particular dementia causes no aphasia, agnosia, or apraxia
Parkinson’s dementia is unique and different from AD, somewho have Parkinson’s disease also have AD.
Huntington’s DiseaseHuntington’s disease, a hereditary disorder associated withdementia, results from a faulty gene for a protein calledhuntingtin. Because it is autosomal-dominant, children of an affected parent have a 50% chance of inheriting the trait-carrying gene. Men and women are affected equally. The dis-ease inevitably develops in those with the trait in their 30s or40s. Time from onset to death is approximately 15 years
Cognitive Disorders 66731C H A P T E R
Diminished numbers of dopaminergic neurons in the sub-stantia nigra of the brain result in the manifestations of Parkinson’s disease. One such manifestation is dementia,which develops in more than 75% of clients with the illness.
Destruction of dopaminergic neuronal cells in the substantia
nigra in the basal ganglia
Depletion of dopamine stores
Degeneration of the dopaminergic nigrostriatal
pathway
Imbalance of excitatory (acetylcholine) and inhibiting (dopamine) neurotransmitters
in the corpus striatum
Impairment of extrapyramidal tracts
controlling complex body movements
Tremors Rigidity Bradykinesia Postural instability
Basal ganglia
Substantia nigra
Corpus striatum
U N D E R S T A N D I N G B I O L O G I C F O U N D A T I O N S 3 1 . 2
The Pathophysiology of Parkinson’s Disease

a prion (NINDS, 2007). Symptoms ensue after age 60 years.Although 5% to 10% of U.S. cases are thought to be genetic,the disease is thought to spread through contact with contami-nated human brain tissue or from improperly sterilized neuro-surgical tools. Ingestion of certain neurologic parts of cowsinfected with a prion similar to the one causing Creutzfeldt-Jakob disease has been the source of contamination inBritish and U.S. outbreaks. This type is a variant of theclassic Creutzfeldt-Jakob disease and is more common inadults younger than 60 years. Both forms are termed “spongi-form” because of the spongy appearance of the cerebral andcerebellar cortex (NINDS, 2007). In older adults, the dis-ease may be misdiagnosed as AD, but symptoms are ini-tially more suggestive of a psychiatric illness other thandementia (NINDS, 2007).
Clients with Creutzfeldt-Jakob disease pass through threedistinct stages. Initially, mental abnormalities progress to arapidly deteriorating dementia. Then, jerking, seizure-likeactivity appears, with ataxia, dysarthria, and other cerebellarsigns. Extrapyramidal signs, sensory disruption, and seizuresare other manifestations during the middle phase. Coma marksthe final phase, with clients dying of infections and respira-tory problems (NINDS, 2007).
Implications and PrognosisPrognosis for people with dementia is poor. Currently, nocures are available; however, certain interventions appear todelay or slow progression of some forms and symptoms.
Interdisciplinary Goals and ManagementClients and families truly need participation from an entirehealthcare team for a comprehensive management regimen.Overall goals for clients with dementia include physical care,a safe environment, behavior management, and psychosocialsupport and education of clients and caregivers. See EVIDENCE-BASED PRACTICE SPOTLIGHT 31.1.
Clients with dementia benefit from as early a diagnosis aspossible to promote interventions that slow illness progres-sion. Early diagnosis also gives relatives time to adjust andrearrange their lives as they increasingly assume the caregiverrole. The healthcare team interacts most intensively withclients during early stages, when clients are still aware of andthus most frustrated and depressed about cognitive losses. Asthe disease becomes more incapacitating, healthcare providersexpand their involvement with relatives, often forming close-knit partnerships. These alliances promote the physical healthand safety of clients and support the whole family.
As they lose cognitive abilities, clients develop moreextensive and demanding needs. Families need teaching fromphysicians and nurses on how to care for loved ones who canno longer independently handle ADLs. Relatives (most oftenspouses or daughters) usually assume the role of primary care-giver. In doing so, they take on an exhausting and constantjob for people who show decreasing appreciation and, withtime, no longer even recognize them. This is not only physi-cally but also emotionally stressing. Healthcare providers
but does result in memory deficits, slowed thinking, problemswith attention, and deficient judgment. Cognitive symptomsoften begin as mild emotional manifestations (eg, irritability)and progress to anxiety and depression (NINDS, 2007). Asthe frontal lobe deteriorates, clients become labile, impulsive,easily frustrated, irritable, hostile, and aggressive. The illnessbecomes increasingly relentless, and clients often exhibitmood or intermittent explosive disorders.
Human Immunodeficiency Virus DementiaHuman immunodeficiency virus (HIV) dementia is seen morefrequently in a younger population than are the other dementiasbecause HIV is more prevalent in younger people. Althoughdementia occurs in as many as 75% of those with HIV, othercauses such as infections, tumors, and adverse drug reactionsneed consideration (Sadock & Sadock, 2007). MRI of the brainoften reveals some type of pathologic change, and clients usu-ally manifest other symptoms accompanying HIV. Cliniciansshould be alert for mild cognitive decline or neurologic symp-toms such as headaches, vision changes, and neuropathies thatmight signal CNS involvement in clients with AIDS (Sadock& Sadock, 2007).
Those with HIV dementia show memory loss, poor judg-ment, and decreased executive function. At times, motormovements are delayed. Progression of HIV dementia differsfrom other forms with a predictably steady mental deteriora-tion. Some clients with HIV dementia have daily episodesof memory loss and confusion alternating with mental clar-ity. Problems also can stabilize for months to years beforedownward progression ensues. Antiretroviral drugs used totreat HIV/AIDS can delay onset and reduce symptoms(NINDS, 2007).
Pick’s DiseasePick’s disease accounts for approximately 5% of progressivedementias. Onset is at 40 to 60 years of age; studies show thatPick’s occurs slightly more often in men, usually those withan affected first-degree relative (Sadock & Sadock, 2007).Although the cause is unknown, researchers suspect a geneticcomponent. Pick’s disease is another degenerative dementiawhose clinical picture so resembles AD that in several instancesdifferentiation happens only on autopsy. General microscopicfindings include atrophy of the frontotemporal regions of thebrain, in contrast to the more parietal-temporal distribution ofAD (Sadock & Sadock, 2007). Investigators do not clearlyunderstand why this atrophy occurs, but they believe it toexplain aberrant behaviors seen with Pick’s disease. In begin-ning stages, people with Pick’s disease have less disorientationand memory loss than do those with AD and more personalitychanges, including loss of social constraints (resulting in fre-quent social and behavioral problems).
Creutzfeldt-Jakob DiseaseWith a global incidence of approximately one new case per1 million people per year, this rare, rapidly progressive, andultimately fatal disease results from a protein-like agent called
668 Psychiatric DisorderssixU N I T

Although the cause of this problem remains unknown, ithappens early in the disease. Compelling evidence shows thatdrugs that inhibit ACh destruction or increase cholinergicactivity can slow deterioration of memory and function. Sys-tematic reviews of two such drugs, rivastigmine and donepezil,support their efficacy for treatment of AD and dementiarelated to Parkinson’s disease (Birks et al., 2000; Maidmantet al., 2006).
Cholinesterase inhibitors increase availability of ACh byinterfering with the enzyme that breaks it down. These cen-trally acting drugs help elevate the level of ACh by decreasingthe binding sites of acetylcholinesterase, which lengthens thepotential for cholinergic activity. These drugs are effective aslong as some cells still produce ACh (Sunderland et al., 2004).Thus, they are most efficacious for mild to moderate AD. Eventhen, their effects on cognition are modest, with only smallimprovements and possible slowing of deterioration. However,clinical evidence suggests that cholinesterase inhibitors havesignificant benefits by improving function for clients anddecreasing burden for caregivers (Geldmacher, 2007).
Tacrine (Cognex) was the first centrally acting, noncom-petitive acetylcholinesterase inhibitor to be created. The liverrapidly absorbs and metabolizes tacrine, making it vulnerableto toxicity and requiring ongoing monitoring of liver function,
must be resources to family for innovative care tactics, refer-rals to community offerings for respite and home healthcare,information about support groups, and group or personal coun-seling. Such support helps family to care for loved ones anddelays or permanently avoids the institutionalization of clients.
Medical and Supportive InterventionsFamily caregivers need to know how to meet the physicalneeds of loved ones as self-care capabilities diminish. Somefamilies need minimal information and guidance; othersrequire more tangible assistance (eg, home health aides).
Changing the environment often can assuage behavioralproblems as dementia progresses. Sometimes, however,behavioral problems are best managed pharmacologically.Behaviors that warrant medication include extreme agitation,depression, and disinhibition. Clients with dementia takingany medications require careful monitoring because the drugsactually can cause or compound behavioral problems. Some-times, merely lowering a dosage, discontinuing the medica-tion, or substituting another drug resolves issues.
Psychopharmacologic InterventionsOne finding in AD is diminished cholinergic neurotransmis-sion, resulting in too little ACh in the cholinergic system.
Cognitive Disorders 66931C H A P T E R
E V I D E N C E - B A S E D P R A C T I C E S P O T L I G H T 3 1 . 1
Nonpharmacologic Treatment of Dementia-Related AgitationOverview of Effective Treatment: Interventions based onunderstanding the meaning of behavior and a comprehen-sive biopsychosocial assessment allow nurses to modify theenvironment and adapt nursing care to client needs. Majorpractice recommendations support assessing patterns ofagitated behaviors, avoiding triggers for these behaviors,implementing general communication techniques, and usingspecific interventions, including sensory enhancement/relaxation, social contact, behavior therapy, structuredactivities, and environmental modifications. These havebeen found to decrease agitation and reduce the need forphysical and chemical restraints. The strongest evidencebased on randomized controlled studies supports the useof individualized music that stimulates remote memory and sensation.
What Has Not Been Shown Effective: Restraints havenot been shown effective in preventing injury or reducingdementia-related agitation. In fact, increased agitation andinjury have been associated with restraint use. The currentstandard of care is restraint free, requiring both institutionalpolicies and individualized care of cognitively impaired clients.Although antipsychotic medications are effective for short-term management of agitation, they are not without risk.
Implications for Practice: Physical and chemical restraintsare associated with increased risk to people with cognitiveimpairment. Comprehensive assessment and individualizedcare along with environmental modifications are evidence-based nursing interventions that can significantly improve thecare and reduce agitated behaviors in people with dementia.
References
Agency for Healthcare Research and Quality (AHRQ). (2007). Efficacy and comparative effectiveness of off-label use of atypical antipsychotics.A summary for clinicians and policymakers, AHRQ publication no. 07-EHCoo3-2. Available at: www.effectivehealthcare.ahrq.gov
Gerdner, L. (2007). Individualized music for elders with dementia. Iowa City, IA: University of Iowa Gerontological Nursing InterventionsResearch Center, Research Dissemination Core.
McGonigal-Kenney, M. L., & Schutte, D. L. (2004). Non-pharmacologic management of agitated behaviors in persons with Alzheimer diseaseand other chronic dementing conditions. Iowa City, IA: University of Iowa Gerontological Nursing Interventions Research Center,Research Dissemination Core.
Park, M., Hsiao-Chen Tang, J., & Ledford, L. (2005). Changing the practice of physical restraint use in acute care. Iowa City, IA: University ofIowa Gerontological Nursing Interventions Research Center, Research Dissemination Core.
Thiru-Chelvam, B. (2004). Bathing persons with dementia. Iowa City, IA: University of Iowa Gerontological Nursing Interventions ResearchCenter, Research Dissemination Core.

reduction in caregiver psychological distress, as well asimproved caregiver knowledge and client mood (Brodaty et al.,2003). These data are vital because enhanced caregiver copingand self-care may help delay or prevent institutionalizationof clients with dementia, as well as caregiver morbidity. SeeEVIDENCE-BASED PRACTICE SPOTLIGHT 31.2.
especially the level of alanine aminotransferase (ALT), everyweek for the first 18 weeks of use of tacrine. Because of thepotential for liver toxicity, tacrine is no longer used. Rivas-tigmine (Exelon), galantamine (Reminyl), and donepezil(Aricept) are more widely used cholinesterase inhibitors.Rivastigmine now has an FDA warning because of cardiaccomplications noted in two large clinical trials. The most com-mon drug is donepezil. In some people, donepezil delays theprogression of dementia for 6 to 12 months. It has a longerduration than tacrine, does not require monitoring of liverfunction, and is administered only once a day at bedtime.Clients usually start with 5 mg/day, increasing to 10 mg/dayafter 4 to 6 weeks. Higher doses may not help all clients, anddonepezil has an increased risk of cholinergic side effects(nausea, diarrhea, insomnia). Donepezil can cause irregularheartbeats in clients with heart conditions (Sunderland et al.,2004). See Chapter 16 as well.
Memantine has shown promise in improving symptomsin people with mild to moderate dementia. It is particularlyuseful for vascular dementia and in combination with cho-linesterase inhibitors. It has shown a detectable effect on cog-nitive function and functional decline measured at 6 monthsin people with moderate to severe AD (McShane et al., 2006).Twenty milligrams a day seems to prevent neurodegenerativechanges (Sunderland et al., 2004). Other drugs thought to havesome neuroprotective promise (discussed earlier) for peoplewith early signs or family history of AD are anti-inflammatorymedications such as ibuprofen; statins (for lipid control);antioxidants, particularly vitamin E; and ginkgo biloba.
Psychosocial InterventionsBecause of dementia’s grim prognosis, clients and familyneed support from the interdisciplinary team to endure theshock of its initial diagnosis. They also need guidance for thefuture. In early stages, clients may need emotional support todeal with their cognitive losses. Caregivers need progressivehelp from professionals to deal with their own exhaustion,depression, and frustration. Family needs to participate in careplanning and receive education about available assistancewith the physical care they render.
Psychoeducational approaches have been shown to en-hance caregivers’ coping (Hepburn et al., 2003). Althoughperceived caregiver burden may not change significantly,psychosocial interventions are associated with significant
670 Psychiatric DisorderssixU N I T
?T h i n k A b o u t I t 3 1 . 2A client with AD was initially prescribed tacrine.However, his physician has discontinued use of tacrinebecause of possible liver problems and has ordereddonepezil. Develop a teaching plan for the client’sfamily about donepezil, including the differencesbetween it and tacrine.
✔C h e c k p o i n t Q u e s t i o n s9. What is the hallmark pathologic feature of AD?
10. What is the second most common form of dementia?
11. What hereditary disease is associated with dementia?12. Which class of drugs has been proven to be
moderately successful in slowing the cognitivedecline of dementia?
A P P L Y I N G T H E N U R S I N G P R O C E S SA P P L Y I N G T H E N U R S I N G P R O C E S S
Dementia
● A S S E S S M E N TThe first step in determining nursing approaches to manage-ment is assessment. Clients require screening for any under-lying, treatable physical problems that accentuate or areco-morbid with dementia. Any condition in BOX 31.3 canconfound diagnosis. All potentially reversible and treatablecauses must be ruled out before a diagnosis is made. Doingso necessitates extensive history taking, thorough physicalassessment (including neurologic and mental status exami-nations), and diagnostic testing (ASSESSMENT TOOL 31.2). If screening procedures reveal treatable illnesses, actionshould be initiated to resolve them. Treating underlying illnesses expedites recovery from any delirium, improvesoverall health and delays further decline, and eliminatessymptoms that can obscure dementia and thus preventtimely diagnosis. Once clients have been evaluated andtreated for underlying medical conditions, nurses can proceed with assessment of cognitive functioning.
BehaviorNurses assess various components of behavior and func-tion (ASSESSMENT TOOL 31.3). A functional assessment with ascreening tool that measures not only physical ADLs but alsoinstrumental ADLs (IADLs) can be useful for determining thelevel of impairment and degree of assistance needed. Anexample is the Functional Assessment Questionnaire (FAQ).
Assessment of the client’s ability to perform ADLs isone of the most important parameters in the detection ofdementia. Clients may have minimal to no insight aboutwhen decline in cognition and function or behavioral changesbegan. Family must be involved in supplying information
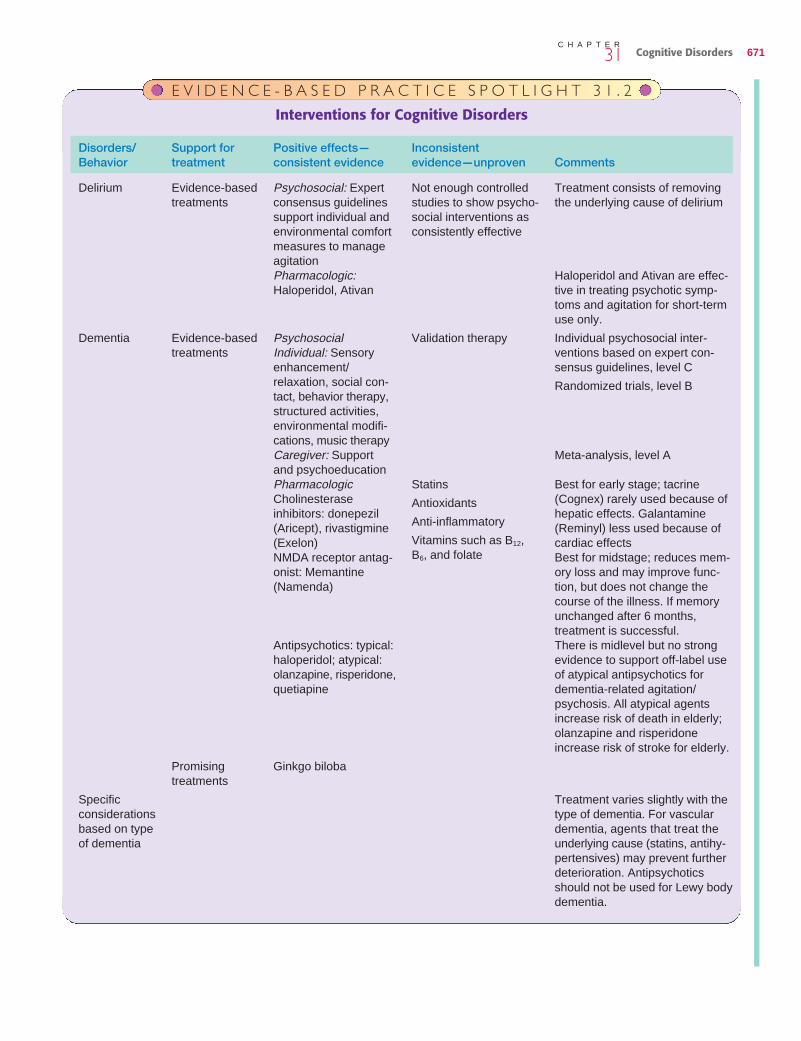
Cognitive Disorders 67131C H A P T E R
E V I D E N C E - B A S E D P R A C T I C E S P O T L I G H T 3 1 . 2
Interventions for Cognitive Disorders
Evidence-basedtreatments
Evidence-based treatments
Promising treatments
Psychosocial: Expertconsensus guidelinessupport individual andenvironmental comfortmeasures to manageagitationPharmacologic:Haloperidol, Ativan
PsychosocialIndividual: Sensoryenhancement/relaxation, social con-tact, behavior therapy,structured activities,environmental modifi-cations, music therapyCaregiver: Supportand psychoeducationPharmacologicCholinesteraseinhibitors: donepezil(Aricept), rivastigmine(Exelon)NMDA receptor antag-onist: Memantine(Namenda)
Antipsychotics: typical:haloperidol; atypical:olanzapine, risperidone,quetiapine
Ginkgo biloba
Not enough controlledstudies to show psycho-social interventions asconsistently effective
Validation therapy
Statins
Antioxidants
Anti-inflammatory
Vitamins such as B12,B6, and folate
Treatment consists of removingthe underlying cause of delirium
Haloperidol and Ativan are effec-tive in treating psychotic symp-toms and agitation for short-termuse only.
Individual psychosocial inter-ventions based on expert con-sensus guidelines, level C
Randomized trials, level B
Meta-analysis, level A
Best for early stage; tacrine(Cognex) rarely used because ofhepatic effects. Galantamine(Reminyl) less used because ofcardiac effectsBest for midstage; reduces mem-ory loss and may improve func-tion, but does not change thecourse of the illness. If memoryunchanged after 6 months, treatment is successful.There is midlevel but no strongevidence to support off-label useof atypical antipsychotics fordementia-related agitation/psychosis. All atypical agentsincrease risk of death in elderly;olanzapine and risperidoneincrease risk of stroke for elderly.
Treatment varies slightly with thetype of dementia. For vasculardementia, agents that treat theunderlying cause (statins, antihy-pertensives) may prevent furtherdeterioration. Antipsychoticsshould not be used for Lewy bodydementia.
Disorders/ Support for Positive effects— InconsistentBehavior treatment consistent evidence evidence—unproven Comments
Delirium
Dementia
Specific considerations based on type of dementia

Family members may provide invaluable associated data.They can contribute information about unusual behavior andrelate any episodes of hallucinations (eg, a client verbalizedfears and concerns about seeing bugs that no one else saw).
OrientationNurses must ask such questions about orientation to person,place, time, and date skillfully so as not to insult clients’ intel-ligence. They phrase questions conversationally or informclients that some basic questions are part of the examina-tion. Nurses also should ask family members if clientsbecome more restless, agitated, or confused in the evening(sundowning).
MemoryIncidents evoking remote memory usually are easy to elicitfrom clients, but more recent events may prove problematic.Nurses can assess recent memory by evaluating responsesof clients to questions involving events of the previous hour,day, or week. Use of the MMSE, described previously, canprovide ongoing objective data about short-term memory.
FamilyFamily members, as indicated previously, are vital resourcesfor historical data. They often can provide much informationconcerning a client’s ability to carry out ADLs and IADLs.Interactions between family and client during the interviewalso can reveal the condition of the client’s social skills andfamily dynamics.
Nurses must assess family members, especially care-givers, for signs of stress or burnout. Although this issuemight not be pertinent during early stages of dementia, itbecomes paramount as clients progressively degenerate anddemands for physical care mount. It also becomes a factoras the role of “caregiver” increasingly becomes dominant,while the roles of spouse, companion, confidante, and loverfade. Loss of these roles can result in loneliness and depres-sion. Early detection of caregiver and family stress may helpprevent elder abuse and neglect, preserve family relation-ships, and prevent caregiver morbidity.
EducationNurses must determine the needs of clients and family forinformation and instruction about the illness, its manage-ment, and support. Caregivers can provide better assistancewhen they know what to expect as the disease progressesand how to address common problems. Burnout, guilt, andfrustration may be ameliorated when family membersunderstand the commonality of and how to handle theirfeelings. Use of psychoeducational approaches has beendemonstrated effective in enhancing family coping andreducing caregiver depression and anger (Coon et al.,2003; Hepburn et al., 2003).
● N U R S I N G D I A G N O S E SThere are as many nursing diagnoses for clients with demen-tia as there are possible symptoms. Although nursing diag-
because they may be more reliable sources. Nurses ques-tion clients and family in a nonjudgmental, nonthreateningway and recognize that denial is common. Clients may try tocover up gaps in memory, and family may rationalize disrup-tive behavior as “quirks.”
Mental StatusSeveral tools to assess mental status are available (ASSESS-MENT TOOL 31.4). An example is the Short, Portable MentalStatus Questionnaire (SPMSQ) developed by Pfeiffer. TheMMSE remains the gold standard for assessment of mem-ory. Its excellent reliability and validity make it widely used invarious clinical settings, including primary care. Scores below23 indicate a need for further evaluation in high school grad-uates; scores below 26 should prompt further investigationin those with higher education levels. Although the MMSEdoes not assess abstract thinking, nurses can assess it byasking clients to interpret a proverb such as “a rolling stonegathers no moss.” Failure to adequately explain such a say-ing may indicate problems with abstract reasoning, concen-tration, or executive functioning. However, nurses need toconsider first whether clients would be familiar with a partic-ular proverb based on age and culture.
Another useful and simple clinical tool is the Clock DrawTest, first developed by Shuman in 1986. Nurses ask clientsto draw a clock, put numbers on it, and put the hands at aspecified time (FIGURE 31.7). This simple test of executivefunctioning, visuospatial skills, and general organization canmeasure cognition over time (Levenson et al., 2005).
Perceptual ProblemsNurses may discover perceptual problems by observingbehavior and exploring odd or unusual comments of clients.
672 Psychiatric DisorderssixU N I T
box
31.3 Differential Diagnosis for Dementia
• Drug withdrawal (benzodiazepines, alcohol, opioids,cocaine)
• Endocrine disturbance (thyroid disorder, Cushing’s syndrome, Addison’s disease)
• Heavy metal toxicity (lead, mercury, arsenic)• Infections (HIV/AIDS, neurosyphilis, viral hepatitis,
systemic)• Bowel impactions• Metabolic disruption (fluid and electrolyte imbalances,
hepatic encephalopathy, uremia, porphyria, hypoxia,hypotension, chronic obstructive pulmonary disease)
• Neoplastic• Neurologic disease (Parkinson’s disease)• Nutritional (deficiencies in vitamin B12, folate, or thiamine;
malnutrition)• Pain• Seizures• Sensory deficits or overload• Trauma

Risk for Injury related to cognitive and psychomotor impair-ments reducing ability to adapt to changing environmentCaregiver Role Strain related to the ongoing and mount-ing needs of the client as evidenced by expressions ofsadness, guilt, despair, and stress
noses must reflect the uniqueness of each client, a plan ofcare might include the following (NANDA-I, 2007):
Chronic Confusion related to cerebral degenerationSelf-Care Deficit related to cognitive and motor impairments
Cognitive Disorders 67331C H A P T E R
A S S E S S M E N T T O O L 3 1 . 2
Screening Tests for Dementia
Compiled from Sadock, B. J., & Sadock, V. A. (2007). Kaplan & Sadock’s synopsis of psychiatry (10th ed.). Philadelphia, PA: Lippincott Williams & Wilkins; and from Gauthier, S. (2007). Clinical diagnosis and management of Alheizmer’s Disease (3rd ed.). Boca Raton. Abingdon Oxon Taylor Francis.
Test
1. White blood cell count with differential2. Complete blood count with differential; hemoglobin (Hb)3. Erythrocyte sedimentation rate (ESR)4. Urine examination and toxicology test
a. Sugar and acetoneb. Leukocytesc. Barbiturates and other toxic substancesd. Albumine. Porphyria screenf. Heavy metals (lead, mercury, manganese, aluminum,
arsenic); can be done as serum test as well5. Serum tests
a. Blood urea nitrogenb. Creatininec. Glucosed. Triiodothyronine (T3), thyroxine (T4)e. Electrolytes
f. Mg+, Br+
g. Copperh. Serum folate level, ferritin, iron
i. Vitamin B12
j. Aspartate aminotransferase (AST)k. Bilirubinl. Venereal Disease Research Laboratory (VDRL) or
rapid plasma reagin (RPR)m. Drug levels—specific search for evidence of drugsn. Human immunodeficiency virus (HIV)o. Lactate dehydrogenase (LDH)
p. Parathyroid hormone6. Routine radiographs
a. Chestb. Skull
7. Electroencephalogram (EEG)8. Computed tomography (CT) scan9. Magnetic resonance imaging (MRI)
10. Spinal tap—cerebrospinal fluid (CSF)11. Ultrasound—carotid or Doppler12. Single-photon emission computed tomography (SPECT)
Clinical importance
1. Infection2. Anemia and hematocrit (Hct)3. Infection or vasculitis4. Urine examination and toxicology test
a. Diabetesb. Infectionc. Toxicityd. Renal failuree. Renal failuref. Heavy metal intoxication
a. Renal failureb. Renal failurec. Diabetes, hypoglycemiad. Thyroid diseasee. Evaluation for imbalance, including NA+, K+, Ca2+,
Cl−, PO4; parathyroid-induced changes in calcium,phosphate
f. Bromides still are present in some common drugsand overuse may inadvertently lead to toxicity
g. Wilson’s diseaseh. Nutritional problems, thiamin deficiency, iron
deficiencyi. Dementia, delirium, malnutritionj. Increased in hepatic disease
k. Increased in hepatic diseasel. Syphilis
m. Barbiturate, ethanol (ETOH), other drug overdosen. Present in AIDS dementiao. Elevated in myocardial infarction, hepatic disease,
and central nervous system damagep. Associated with variety of cognitive disorders
6. Routine radiographsa. Infection, heart failureb. Evidence of increased intracranial pressure, fractures
7. Ictal phenomena8. Brain tumor, subdural hematoma, infection, hemorrhage9. More sensitive for detection of vascular changes than CT
10. Infection, hemorrhage11. Detect vascular dementia12. Highlights brain activity, helps in differential diagnosis of
dementias

674 Psychiatric DisorderssixU N I T
Subjective Data
Behavioral Changes (Often Asked of the Family)
Is there a change in behavior? If so,a. How does the present behavior differ from former
behavior?b. When was this change in behavior first recognized?
Emotional Changes
• Are any of the following present: depression, anxiety, para-noia, agitation, grandiosity, confabulation?
• Does the client have insight into the fact that “things arenot right?”
• Is the client complaining of many physical ailments forwhich there are no bases?
• Are certain previous personality traits becoming predominantor exaggerated?
Social Changes
• Is the client exhibiting embarrassingly loud and jocularbehavior?
• Is there sexual acting-out beyond the bounds of propriety?• Has the client shown signs of short temper, irritability, or
aggressiveness?• Is there an increasing inability to make social judgments?
Intellectual Behavior
• Has the ability to remember recent events decreased?• Has the ability to problem-solve decreased? (This might be
especially apparent in the work or job area.)• Do new environments or even old environments result in
the client’s disorientation?• Is it difficult for the client to carry out complex motor skills?
Do his or her efforts result in many errors?• Are any of the following language problems present:
• Has the client’s language changed?• Does the client’s language ramble and wander from the
point of the conversation?• Is the point of the conversation never clearly stated?• Is there difficulty comprehending complex material?• Does the client have trouble remembering names of
people and objects?• Does the client have difficulty writing?
Functional Capacity
• Are there any changes in the client’s ability to performactivities of daily living (ADLs)?
• Is there difficulty transferring or ambulating?• Is there difficulty bathing, dressing, or grooming?• Is there difficulty eating or toileting?• Are there any changes in the client’s ability to perform
instrumental ADLs (IADLs)?
A S S E S S M E N T T O O L 3 1 . 3
Questionnaire for Dementia• Is the client able to make a grocery list, shop for food, and
handle money?• Is the client able to use the telephone?• Can the client prepare a meal and complete housekeeping
tasks?
Objective Data
Level of Consciousness
Is the client confused, sleepy, withdrawn, adynamic, apathetic?
Appearance
Is there decreased personal hygiene?
Attention
• Does the client have decreased ability to repeat digits afterthe interviewer?
• Do other stimuli in the environment easily distract the clientfrom the interviewer?
• Does the client focus on only one of the stimuli in the envi-ronment, and is he or she unable to turn attention from theone stimulus?
Language
• Outflow of words decreases.• Patterns of repetitive, tangential, or concrete speech
appear.• Writing skills decrease more rapidly than the spoken word.
Memory
Test the client’s ability to remember four unrelated wordsand recent events. (Confabulation and anger often will beused by the client to move the interviewer away from ques-tions related to memory.)
Constructional Ability
The client is instructed to copy a series of line drawings; theclient often is unable to do this, or the ability to do sodeclines dramatically over time.
Cortical Function
• The client’s ability to perform arithmetic is faulty andreveals many errors.
• Proverb interpretation—Usually, the client gives only aconcrete interpretation of the proverb.
• Similarities—The client often denies similarities betweentwo objects and instead gives a concrete answer. Forexample, when asked, “What is the similarity between atiger and a cat?,” the client may reply, “One is small andone is large. There is no similarity.”

Caregiver Well-Being: The caregivers will take measuresto ensure adequate respite and find ongoing avenues forsupport.Family Coping: The client’s caregivers and family will havepsychosocial support and resources for respite care.
● I M P L E M E N T A T I O NInterventions for clients with dementia and their familiesare numerous and range the entire holistic spectrum. Some common NIC labels include, but are not limited to,Caregiver Support, Coping Enhancement, DementiaManagement, Environmental Management, RealityOrientation, Respite Care, and Support Group(Bulechek et al., 2008).
CASE IN POINT 31.1 describes nursing care for a client andfamily facing Alzheimer’s disease.
Managing the Client’s HealthEssential nursing actions are facilitating optimal function-ing and preventing further decline by promoting physical
Interrupted Family Processes related to degenerativecerebral changes in a family member
● O U T C O M E I D E N T I F I C A T I O N A N D P L A N N I N G
Planning care for clients with dementia is most effectivewhen family, clients, and team members collaborate todetermine the most realistic goals. Those involved alsoshould include measures that encourage family cohesive-ness and stability. The family needs to decide what responsi-bilities different members can assume and what respiteinterventions they can initiate to prevent exhaustion. Majorgoals for the care of clients with dementia, organized accord-ing to NOC, are as follows (Moorhead et al., 2008):
Health Maintenance: The client’s physical needs will be met.Cognitive Orientation: The client’s environment will besafe and protected.Distorted Thought Control: The client will have infrequentepisodes of agitation.
Cognitive Disorders 67531C H A P T E R
A B C D
figure 31.7 A useful and simple test of mentalstatus is the Clock Draw Test. The example in Awould be rated as excellent, whereas B would begood, C would be fair, and D would be poor.
(text continues on page 681)
A S S E S S M E N T T O O L 3 1 . 4
Testing for Cognitive Deficits
Focus of test Name of test What is measured Analysis potential
Intelligence, verbalperformance
Memory
Language skills
Conceptualization
Visuospatial skills
Attention
Wechsler Adult IntelligenceScale—Revised (WAIS-R)
Wechsler MemoryScale–Revised California VerbalLearning Test
Boston Diagnostic AphasiaExamination
WAIS-R Similarities Subtest
Benton Visual Retention TestBlock Design subtest of theWAIS-R
Digit Span Subtest of the WAIS-R
Crystallized and fluid intelligence
Aphasia subtest—word-findingability (common in dementia)
Abstract versus concrete thinking
Notes if client can pay attentionand use memory
Alzheimer’sSensitive in early dementiaIf single finding, may indicateamnestic disorder
Alzheimer’sSingle finding may indicate focaldeficit
Alzheimer’s
Single finding may indicatedelirium disorder, focal frontallesion
Zarit, S. H., & Zarit, J. M. (2007). Mental disorders in older adults: Fundamentals of assessment andtreatment. New York, NY: Guilford Press.

676 Psychiatric DisorderssixU N I T
Key Ass e s sment F indings
• Impaired memory; forgetfulness• Disturbed executive function
(inability to find way home fromgrocery store)
• Cognitive deficits• Decreased involvement in social
activities (bridge games)• Below normal score on Mini-MSE• New diagnosis—Dementia of
Alzheimer’s type: late onset• Therapy with donepezil (Aricept)
B etty, 76 years old, lives with her daughter and son-in law. Shemoved in with them 11 years ago, following the death of her husband. Bettyhas many friends and has stayed active. Her daughter Audrey and son-in lawLinc have accompanied Betty to a doctor’s appointment.
Audrey reports to the nurse that she is concerned about her mother’sbehavior. “I’m not surprised that she forgot my birthday last week becauseshe’s having difficulty recalling when she’ll celebrate hers! Lately she’s for-gotten other things, like bingo games. She’s also been avoiding her weeklybridge game with friends, telling me she’s too tired or doesn’t feel like it.”Audrey reports that Betty, normally an early riser and fastidious, has beenstaying in bed late and spending days in her pajamas. “I asked her aboutthis, thinking she wasn’t feeling well. She told me angrily, ‘Why can’t I enjoymy old age? Why should I be busy every minute?’ ” Audrey relates that a fewmonths ago, Betty got lost coming back from a grocery trip. After meander-ing over several back roads, it became clear that she was lost, and she calledLinc for help. Upon questioning by the nurse, Betty states that she justwanted to go for a drive.
Betty undergoes physical, neurologic, mental status, and functional eval-uations, a battery of laboratory tests, and a computed tomography scan. Sheuses some words inappropriately and scores 22 on the Mini-MSE. No othersignificant findings appear. The physician gives a diagnosis of Dementia ofAlzheimer’s Type: Late Onset, Uncomplicated. Because the disease is in anearly stage, she prescribes donepezil (Aricept).
The nurse is discussing with the family the prognosis and needs forfuture care. Betty is very upset. Initially, she denies her problem but thencries and admits that she has been concerned about her mental functioning.Discussion centers on the need for support and that eventually Audrey andLinc may need help for Betty to remain at home. All agree that Betty shouldremain as active as possible and continue bridge and cognitively stimulatingactivities.
Nursing Diagnosis: Anticipatory Grieving related torecent diagnosis of dementia as evidenced by changes incurrent status, initial denial of problems, and reaction todiagnosis
NOC: Grief Resolution: The client will verbalize feelingsabout diagnosis and potential decline in functional ability.
NOC: Psychosocial Adjustment: Life Change: The familywill set realistic goals, maintain productivity, and use effec-tive coping strategies.
NIC: Grief Work Facilitation• Assist the client to identify and express fears and feelings.
Help her deal with her initial reaction. Listen carefully andempathetically. Communicate acceptance. Include signifi-cant others (FIGURE A). Encouraging the client to expressfeelings and listening empathetically help her release sad-ness and fear. They also help her to feel that others care.
• Instruct the family about the phases of grieving; supportthe client’s progression through them. Loss of cognitivefunction is one of the most frightening changes a personcan face. The family needs time to process their feelings.
(continued on page 677)
Case in Point 31.1Betty’s Story
FIGURE A. The nurse encourages the client and family to share feelings aboutthe diagnosis of AD and gives acceptance and support.

Cognitive Disorders 67731C H A P T E R
• Help the client identify existing coping strategies and con-sider new ones. Examples include living in the present,meditating, praying, and practicing deep breathing orrelaxation. Establishing a plan for stress managementcan help the client during times of fear and anxiety.Stress-reduction techniques also may increase feelingsof well-being.
NIC: Anticipatory Guidance• Assist the family to identify available resources. Doing so
reveals additional support. Options allow the family tofind solutions for problems, which enhances feelings ofcontrol.
• Rehearse techniques needed to cope with upcomingcrises as appropriate. Practicing techniques facilitatestheir use when needed.
Nursing Diagnosis: Risk for Injury related to cognitiveimpairment as evidenced by progressive changes in mem-ory and executive function
NOC: Personal Safety Behavior: The client will remainfree from injury.
NOC: Safe Home Environment: The family will adjust thehome as necessary to ensure it is in optimal condition tomaintain safe and independent living for the client.
NIC: Environmental Management: Safety• Identify danger areas and safety hazards in the home.
Instruct the family to make garages and basementsunavailable to the client because dangerous items oftenare stored there. Teach them to lock medications, poi-sons, cleaning agents, and other toxic fluids in securecontainers or rooms. Ensure that doors leading outsideare locked or have alarms installed. Instruct the family tosecure windows and any doors on the upper floors of thehome. Decreasing cognitive skills increase the client’s riskfor injury. Keeping certain areas off-limits and the rest ofthe house safe and secure optimizes the client’s freedomat home while protecting her.
• Modify the environment to minimize hazards and risks.Plug electrical outlets and remove electrical items that
pose hazards. Move the thermostat on the hot waterheater to its lowest setting. Remove all electrical appli-ances from counters and control knobs from the stoveand oven. Making the home safer should give the familysome peace of mind about the client’s safety. Monitoringthe home is the best intervention for maintaining safety.Interventions will help prevent accidental bums or fires.
• Recommend appropriate protective and adaptive devices(FIGURE B). Protective devices limit mobility or access toharm; adaptive devices increase environmental safety.
• Provide emergency phone numbers; have the family keep them readily available. Quick access is crucial during a crisis.
Nursing Diagnosis: Chronic Confusion related toAlzheimer’s disease as evidenced by memory impairment,forgetfulness, and client’s statements about changes inmental functioning
NOC: Cognition: The client will exhibit adequate mentalfunctioning with assistance.
NIC: Dementia Management• Control environmental stimulation. Help establish a calm-
ing atmosphere. Encourage the family to remove house-hold clutter and to provide adequate lighting withoutglare. Create predictability and simplify choices. Assist thefamily to establish a daily routine for grooming, meals,and activities; teach them to ask relatives and friends tovisit, but to do so one or two at a time. Controlled stim-ulation will help the client feel secure at home. Simplechoices and tasks that she can complete successfully pre-vent frustration and loss of self-esteem. Nonglare lightingis less disruptive and helps decrease perceptual difficul-
Case in Point 31.1 (continued)
Betty’s Story
9/13/08: The client begins to verbalize feelings associatedwith her condition. The family discusses the reality of the situ-ation and unresolved conflicts. They plan to share the newsand ask for support from a few relatives and close friends.They also plan to seek solace from a spiritual advisor and tocontinue recreational and other enjoyable activities for aslong as possible.
B. Morita, RN
FIGURE B. The family installs guard rails along the client’s bed to protectagainst falling or wandering at night. They place a commode in her bedroomas well so that she does not have to leave her room during sleep (and riskinjury) if she develops the urge for elimination.
(continued on page 678)

678 Psychiatric DisorderssixU N I T
ties. Limiting visitors allows the client to continue socializ-ing but in a controlled way.
• Introduce self when initiating contacts with the client;address her distinctly by name. Speak slowly in a clear,low, warm, and respectful tone of voice. These measuresprevent startling the client. Using her name helps reorienther as needed.
• Use distraction, not confrontation, to manage behavioralproblems. Confrontation increases the client’s frustrationand stress.
• Provide space for the client to pace or wander safely; pro-vide finger foods if the client cannot sit and eat. Providingspace minimizes the risk of injury; finger foods can helppromote adequate nutrition.
• Encourage one-to-one and group activities geared to theclient’s cognitive abilities and interests. When giving direc-tions, do so one at a time. Limiting choices and activitiesminimizes overstimulation, which can increase anxiety.Individual simple directions prevent the client frombecoming overwhelmed.
• Use symbols to locate areas or important items. Symbols maybe easier for the client to comprehend than the written word.
NIC: Cognitive Stimulation• Orient the client to person, place, and time. Provide envi-
ronmental memory cues. Cut out pictures from magazinesand place them on cabinets and drawers to illustrate con-tents. Provide a large-print calendar in a conspicuous spotand record all appointments there (FIGURE C). Encouragethe client to review the calendar daily. Reinforce andrepeat information. Environmental cues will help jog theclient’s memory and keep her as independent as possiblefor as long as possible. Repetition promotes awareness.
Nursing Diagnosis: Decisional Conflict related to uncertainty about future health and resources
NOC: Decision Making: The family will verbalize appropri-ate plans for the future.
NOC: Participation in Healthcare Decisions: The familywill identify available support for achieving outcomes.
NIC: Decision-making Support• Establish communication; facilitate articulation for goals
of care. Communication is important for the therapeuticrelationship; knowledge of goals facilitates an individual-ized plan of care.
• Provide information as requested. Describe options avail-able for care, including full-time nursing at home, adultday care centers, nursing homes, and other long-termfacilities (FIGURE D). Help the family explore the advantagesor disadvantages of each option. Supply all informationas requested but avoid portraying a hopeless prognosis.Respect the client’s right to receive or not receive infor-mation. Family members need information so they canplan for the future. The current plan of caregiving by the
Case in Point 31.1 (continued)
Betty’s Story
10/7/08: The family participates in a thorough home evalu-ation and demonstrates substantially adequate lighting andhandrails, use of personal alarm system, accessible assistivedevices, and furniture arrangement to reduce risks. No injuriesor problems have occurred since the initial visit. They also haveposted emergency numbers and a hotline in key locations. Theclient is maintaining adequate cognitive function with assis-tance. She demonstrates only mild compromise in attentive-ness, concentration, and cognitive orientation. She canidentify self, place, and time and respond to cues.
B. Morita, RN
FIGURE C. The nurse works with the family to establish a calendar that listsall of the month’s events so that they can be more organized while integrat-ing the client’s situation into their lifestyle. The month and year are displayedin large letters and numbers to reinforce time orientation for the client.
FIGURE D. The nurse discusses various options for short-term and long-termcare with the family.
(continued on page 679)

Cognitive Disorders 67931C H A P T E R
daughter and son-in-law alone will not be feasible if theclient needs more than their resources allow. The clientstill may be in denial; the healthcare team needs torespect her right to not receive information.
• Help the client clarify values and make important deci-sions while cognitive function is high. Encourage her toprovide advance directives. Facilitating decisions nowhelps ensure that others can carry out the client’s wishesif she cannot make necessary legal decisions.
Nursing Diagnosis: Interrupted Family Processesrelated to changes in client’s health status as evidenced byprogressive cognitive changes and changes in usual roles
NOC: Family Coping: The family will demonstrate positivecoping measures to deal with changes.
NIC: Family Process Maintenance• Identify effects of role changes on family processes. Pro-
mote family cohesion. Help family members, includingthe client, identify their feelings about role and health sta-tus changes. Help them resolve any guilt feelings. Identifyeffective coping mechanisms; encourage their use as fam-ily adjusts to changes. Discuss strategies for normalizingfamily life. Open communication about the effects of ADwill help family members. The client may feel guilt aboutnot being able to help more or becoming a “burden” onthe family; caregivers may have resentment aboutincreased responsibilities.
• Minimize disruptions by facilitating family routines and rituals. Encouraging normal activities reduces feel-ings of guilt or anxiety related to the client’s currentcondition.
• Discuss existing social support mechanisms; assist thefamily to use them. Help them resolve any conflicts; sug-gest attending an Alzheimer’s support group. Identifyhome care needs and how these might be incorporatedinto the family lifestyle (FIGURES E and F). Helping thefamily resolve feelings and identify appropriate copingbehaviors will decrease stress. Support groups are atremendous resource for sharing feelings and gaininginsight and help. Incorporating home care needs mini-mizes disruptions.
Nursing Diagnosis: Risk for Caregiver Role Strainrelated to increasing requirements for care as evidenced byprogressive nature of disorder
NOC: Caregiver Stressors: The caregiver will identify needfor assistance in caring for her mother.
NOC: Caregiver Emotional Health and Caregiver Physi-cal Health: The daughter will obtain essential respite andsupport to maintain her own functioning while caring forher mother.• Determine the caregiver’s level of knowledge and accep-
tance of role. Provide practical support. Explore her re-action and help her identify stressors, tasks, or behaviors
Case in Point 31.1 (continued)
Betty’s Story
FIGURES E and F. The family arranges for ongoing visits from a home health aide, who provides assistance withmeals and housecleaning. Such help is often necessary to account for the extra demands that the client’s illnessplaces on the entire family.
(continued on page 680)

680 Psychiatric DisorderssixU N I T
that are most frustrating or anxiety producing. Help herdevelop a plan for managing them. Provide support forher decisions. Give information about the disease andlocal support groups. Helping the caregiver becomeaware of her feelings, strengths, the progressive nature ofAD, and available supports will empower her to managethe increasing demands of caregiving while protectingher emotional state. Thinking through and planningahead will help her manage responsibilities.
• Teach techniques to improve the security of the client.Techniques for client security reduce the risk of injury tothe client and caregiver.
• Explore with the caregiver how she is coping; teach stressmanagement techniques and healthcare maintenancestrategies to sustain her physical and mental health.Determining coping and providing instruction aboutstress management and healthcare maintenance strate-gies enhance her ability to provide the necessary care.
• Give encouragement to the caregiver during setbacks forthe client. Setbacks can promote guilt, frustration, andanxiety. Encouragement helps preserve the caregiver’sself-esteem.
NIC: Emotional Support• Provide emotional support. Make supportive or empa-
thetic statements. Emotional support helps to reduce feelings of anxiety in stressful situations.
• Encourage the caregiver to get adequate rest and tomaintain her own physical, emotional, and spiritualhealth. Help her recognize that caregiving is stressful.Encourage her to express feelings of anxiety, anger, orsadness. Encourage her not to feel ashamed or guilty ifshe experiences impatience, frustration, sadness, oranger. Deep breathing, meditation, and visualization, aswell as physical exercise and adequate rest, can help thecaregiver manage feelings of anxiety and stress. Findingsources for personal comfort and happiness will help hermaintain an identity separate from her caregiving role.She then can come to understand that these emotionsare natural when caring for someone who may beunhappy, ungrateful, or difficult.
NIC: Respite Care• Monitor the caregiver’s endurance. Establish a plan for
respite care. Encourage her to set realistic limits on whatand how much she can do. Counsel her to avoid becom-ing isolated and to accept help from others. The caregivercannot perform total full-time care alone.
• Coordinate volunteers for in-home services. Arrange forsubstitute caregivers. Identify community resources forrespite care or other family members or friends who canregularly relieve the caregiver for a few hours at a time(FIGURE G). Respite is essential to prevent burnout, whichis common among full-time caregivers, especially thosewho are socially isolated or have no relief from their duties.
Case in Point 31.1 (continued)
Betty’s Story
12/16/08: The family has established plans that assist themto manage their new reality. They involve a cousin and anephew to provide respite care 2 days a week. They arrange fora nursing home health aide to visit once a week to assist withvarious tasks and for Betty to attend an adult day care facil-ity once a week. They continue to enjoy normal family rou-tines and attend support meetings. The daughter reports mildcompromise in life satisfaction and sense of control. She verbalizes no feelings of resentment and says that she can currently balance her caregiving responsibilities.
B. Morita, RN
E P I L O G U ENine months have passed since Betty was first diagnosed with AD. Since then, Audrey and Linc have been providingcare with support from family, friends, the local Alzheimer’s association, and health services. However, in the pastmonth, Betty’s condition has deteriorated. She has become increasingly confused, with mood fluctuations, and cannotdress or wash herself. She also has become incontinent of urine, mostly at night. Audrey reports, “She tried to maketea yesterday and left the stove on. Sometimes, she doesn’t recognize me.” Two days ago, Betty got out of bed duringthe night, fell, and fractured her hip. She was admitted to the local hospital for treatment. Linc says, “My wife is soexhausted. Her mother needs so much care. I don’t think Audrey can handle this anymore. We’re meeting with a socialworker to make a decision about moving Mom to a nursing home.”
FIGURE G. The client attends a day program once a week so that her daugh-ter has an outlet for respite care.

Encouraging Appropriate BehaviorsClients with dementia often cannot change their behavior.Therefore, the most successful nursing intervention may beto change what clients experience. Restructuring the environ-ment to make it less formidable is especially helpful. Pharma-cologic intervention may be necessary to manage behaviorthat is harmful to clients, their family, or the healthcare team.
Modifying the EnvironmentClients with dementia face multiple dangers resulting fromimpaired cognitive abilities. Safety concerns include falls, poi-soning, wandering and getting lost, and injury to self or othersfrom dangerous objects. Starting fires and getting burned alsoare fairly common. All these situations are worsened by theclient’s inability to respond quickly to emergencies. Environ-mental modification can be the key to managing behaviorand keeping clients safe. Pathologic changes in the braindecrease the ability of clients to interpret the environmentaccurately. Many clients overreact, especially when multiplecues bombard them. Decreasing noise, choices, pain, andoverstimulating interactions can help clients maintain stable,appropriate behaviors. Simply controlling environmental lightmay decrease hallucinations or illusions. Instituting routinesand simplifying choices help easily confused clients.
Times when personal care is being given, such as bathing,seem especially to agitate clients with dementia. There oftenis a way to modify the environment to provide positiveexperiences for clients. Sometimes, changing the site of thebath or giving a bed bath instead of a shower or tub bath inthe bathroom of the home or the institution is helpful (FIG-URE 31.8). Adapting bath time to the client’s usual schedule,rather than the institutional routines, may be helpful (Thiru-Chelvam, 2004).
The goals of care for people with dementia are toenhance function and prevent further decline. Preservation
health, environmental stability, and emotional well-being.Because exogenous substances can initiate or exacerbateaberrant behavior, nurses must be sensitive to the responseof clients to prescribed medications. In addition to knowingthe side effects and toxic reactions of specific drugs thatclients receive, nurses also must be alert to possible druginteractions.
Nurses assess for any symptoms of physical illness.Prompt recognition and appropriate intervention may stopan episodic illness from becoming co-morbid, or a co-morbidillness from accelerating mental dysfunction. Nurses pay particular attention to nutrition and hydration, as well as tobowel and bladder elimination. Clients with dementia mayresist or neglect eating, and poor hydration usually accompa-nies poor diet. Nurses offer foods and fluids throughout theday. Giving food in small portions or offering finger foodsmay increase the likelihood of eating.
Constipation or impaction from insufficient bulk or watercan have serious consequences if not treated promptly. Clientsmay be unable to articulate feelings of fullness; caregiversshould keep a record of bowel movements to monitor regular-ity. Insufficient fluids can lead to urinary stasis and urinary tractinfections. Monitoring fluid intake so that clients receive at least2,000 mL/day (unless contraindicated by renal or cardiacdisease) helps prevent infection and maintain health.
Enhancing Sensory CapabilitiesFor clients with trouble interpreting the environment, sen-sory aids, such as eyeglasses and hearing aids, can beinstrumental in helping them feel more in control. Nursescan provide reading material in large type, if necessary,and speak to clients directly and carefully to further maxi-mize ability to process sensory input. Caregivers also needto be aware that sensory disturbances are not limited tosight and hearing but also may involve perception of painand temperature. Thus, caregivers must take precautionswith hot liquids and bath water to avoid burning clients.Diminished or altered pain perception further emphasizesthe need for surveillance by staff of the client’s physicalcondition.
Meeting the Client’s Physical NeedsThe ability of clients to care for themselves decreases as theseverity of dementia increases. The healthcare team andfamily need to reevaluate continually the client’s capacityfor self-care. Caregivers can help by enhancing the environ-ment to facilitate the limited ability of clients to performADLs and IADLs and by fulfilling unmet needs themselves.Sometimes, clients display aberrant behavior because ofunmet needs. An underlying medical problem may beundetected, or clients may be in pain. As ability to commu-nicate decreases, caregivers and healthcare staff need toobserve clients carefully to try to discern the meaningbehind their actions. Something as basic as discomfortfrom constipation can drive problem behavior, which maysubside after a basic need has been met.
Cognitive Disorders 68131C H A P T E R
figure 31.8 Bathing and hygiene can be activities duringwhich clients with dementia become particularly agitated,fearful, or confused. Care providers should take measuresto preserve safety and comfort, such as ensuring the client’swarmth and performing a sitting shower bath to minimizesymptoms.

occupations, and lifestyles, the more individualized care canbe. Developing creative and flexible interventions and provid-ing safe alternatives to potentially harmful behaviors is a keyto less disruptive behavior. To help guide care, evidence-basedpractice guidelines for nonpharmacologic management of agi-tated behaviors are available at [email protected] (McGonigal-Kenney & Schutte, 2004).
Those caring for clients with cognitive disorders canmonitor their interactions with them. Usually, caregiverswith a calm demeanor have more success handling orinteracting with clients manifesting problems. An attentive,gentle approach is especially helpful when personal care isrequired. In fact, Werezak and Morgan’s (2003) investiga-tions led them to suggest that the psychosocial environ-ment is the most important element of care for peoplewith dementia.
At times, there may seem to be no way to resolve theemotional frustration, agitation, or outbursts of clients who
of function requires nurses to encourage clients to performtheir own ADLs, rather than to do these tasks for them.Cueing and prompting are two strategies designed to pre-serve functioning. For example, a nurse might put toothpasteon a toothbrush and hand it to the client as a cue to brushthe teeth. The nurse may lay out clothing in the order inwhich the client should put it on. Prompting involves verbalstep-by-step directions, but only as much direction as clientsneed. Such interventions provide assessment data as well.
Enhancing environmental cues may be beneficial forclients. Clocks and calendars strategically placed may helpkeep clients oriented. Reality orientation, sensitively applied,can be beneficial, but care must be taken to avoid frustrat-ing clients and causing more problems. Although validationtherapy has not been found consistently useful for thosewith cognitive impairment (Neal & Briggs, 2003), validatingand attending to the feeling behind the content of communi-cation is a vital component of psychiatric nursing care.
Management of disruptive behaviors exhibited by clients,such as wandering, attempting to leave, entering others’rooms, and hoarding items, can challenge nurses as well as family caregivers. At times, efforts to intervene in suchbehaviors seem only to result in further agitation and evenaggression (CHALLENGING BEHAVIORS 31.2). Formal researchinto nonpharmacologic interventions has been hindered bythe need for a common language and a systematic approach(Cohen-Mansfield, 2003). Although such investigations arenow being conducted to determine which interventions areconsistently most helpful, empirical evidence suggests a multi-modal, individualized approach to be most effective (Werner,2003). All behavior has meaning and should be viewed asan attempt by clients to communicate a need. Therefore,attempting to discern and respond to the need expressed byclients may help calm them. For example, if a client is wander-ing, the nurse should walk with her (FIGURE 31.9). If a client istaking clothing from another person’s room, the nurse shouldattempt to distract him by giving him laundry to sort and fold.The more nurses know about their clients’ former routines,
682 Psychiatric DisorderssixU N I T
her or a family member. She may think you are an intruderor are attempting to harm her.
Strategy: Step back, literally and figuratively, and determinewhat the client is attempting to communicate through herbehavior. Formulate a response based on your assessment.
Nurse Action/Communication: You might say, “I have somelaundry I need to put away. Can you come help me sort andfold it?” Walk with her to her room and provide her withsome towels to fold.
Challenging Behaviors 31.2The Client Who Is Disruptive
Situation: Your assigned client is an 81-year-old womanwith Alzheimer’s disease. She has been wandering in andout of other client rooms, taking their clothing and belong-ings. When you attempt to redirect her, she yells “Get out of my way. I am trying to do my work” and takes a swing at you.
Your Potential Feelings: Fear, frustration, surprise
What Is Going On? The client cannot perceive reality andmay believe she is home and that the clothing belongs to
figure 31.9 Some nursing homes and long-term care facili-ties have outdoor areas where nurses, visitors, and health-care personnel can walk with clients who have dementiaand are pacing or wandering.

Performing Pharmacologic InterventionsCholinesterase inhibitors are moderately successful at slow-ing the cognitive decline of dementia (Birks et al., 2000;Birks & Harvey, 2006). Healthcare teams must determinewhich medication is best for each client and educate family
are angry with their environment and those in it. Caregiversmight find it beneficial to redirect or distract clients. They cando so by asking to see personal items, such as photographs,and then talking about illustrated family members and lifeevents (THERAPEUTIC COMMUNICATION 31.1).
Cognitive Disorders 68331C H A P T E R
I N E F F E C T I V E D I A L O G U E E F F E C T I V E D I A L O G U E
ROY: It’s too early to eat, Annie. You eat at 11:30, just afterceramics.
ANNIE: (Walks with Roy out of the day room) When will I eat? Do I eat soon?
ROY: (Looks at watch and shakes his head) You don’t eatuntil later. I have to go into the sunroom to work on theplants.
ANNIE: (Follows Roy to the sunroom) When will I eat?
ROY: (Sighs and continues to water the plants) Annie, are you hungry?
ANNIE: NO! I’m not hungry! Why do you ask that?
ROY: (Notices Annie’s behavior is beginning to escalateand feels puzzled as to why she is getting upset) Annie, goback to the other room and look at your memory book.(Points to Annie’s pocketbook) It’s in your purse. I’ll walkyou there. (Walks Annie to the day room, sits her at a tableand tells another nurse to keep an eye on Annie)
ANNIE: (Sits at the table, looking confused and sad)
ROY: It’s too early to eat, Annie. Lunch is at 11:30, just afterceramics.
ANNIE: (Walks with Roy out of the day room) When will I eat?Do I eat soon?
ROY: (Stops, looks directly at Annie, and smiles) Annie, youeat at lunch time, 1 hour from now. Let’s go into the sun-room. You can help me water the plants. (Remains patientwith Annie, sensing that she is trying to express somethingother than her words)
ANNIE: (Helps Roy bring plants to the sink in the sunroom)When did you say I will eat?
ROY: (Stops watering the plants, looks at Annie, andsmiles) Annie, are you hungry? (Uses positive and “cueing”nonverbal behavior)
ANNIE: NO! I’m not hungry! Why do you ask that? (Gets louder)
ROY: (Realizes Annie’s behavior is beginning to escalate)Annie, I remember seeing a picture of you in your garden.Would you show me that picture again? I think it’s in yourmemory book in your purse. (Points to Annie’s pocketbook)Would you show me the picture of you in your garden?
ANNIE: (Looks at her purse and then rummages through it and pulls out a little photo book) You want to see my pictures?
ROY: Yes, Let’s go sit on the sofa and look at them. (Goesover and sits down, patting the cushion for Annie to sit.Annie comes over and begins thumbing through the book,telling Roy about the pictures.)
R e f l e c t i o n a n d C r i t i c a l T h i n k i n g• What types of communication did Annie exhibit in both scenarios? Assess the reason for Annie’s repetitive speech.
Why might she be more hungry, tired, or insecure this morning?• What nonverbal cues did Roy give in the first scenario? How did these differ from his actions in the second
scenario? What were the results of the differences?• What methods of communication did Roy use in the second scenario that ultimately were more effective than
those he used in the first?
Therapeutic Communication 31.1A Client with Dementia
A nnie Tepsin, a 64-year-old woman with dementia, comes to the day care center threetimes a week. Today, Annie’s husband tells Roy Smith, the nurse, that Annie was awake most of theprevious night. After her husband leaves, Annie begins to follow Roy in and out of the day room,activity room, kitchen, and sunroom. Around 10:30 am, she asks Roy, “Are we going to eat soon?”

reveals that interventions are no longer effective or feasible,the healthcare team and family (and clients, if possible)need to devise different interventions. Indicators of an effec-tive care plan include the following:
The client’s physical needs are met.The client is well nourished and well hydrated.The client does not sustain injuries.Episodes of wandering or agitation are infrequent andmanaged successfully.The caregiver reports satisfaction with his or her quality of life and has social supports and respite care options in place.
AMNESTIC DISORDERSAmnestic disorders include conditions with short-term mem-ory loss as the hallmark. Memory deterioration is so great thatit prevents clients from functioning at previous levels ofsocial and occupational performance and seriously detersthem from learning new information. They typically cannotrecollect events as recent as 2 minutes earlier; they may havedifficulty recalling events or knowledge that they formerlyknew. Acuity of remote memory recall varies, and clientsbecome adept at confabulation to hide deficits.
Brain damage leaves clients disoriented to time and placeto some degree but not to personhood (APA, 2000). Theyhave a superficiality of emotions that precludes deep ties withothers. They frequently adopt a blandness of affect. Progres-sion of symptomatology depends on the underlying etiologyand its severity.
Classifications of amnestic disorders are listed in DSM-IV-TR BOX 31.3. Like dementia, the symptomatologies sharecommonalities; etiologies are the differentiating factors.
Wernicke’s syndrome and Korsakoff syndrome co-occurso frequently that they present a classic picture and thus oftenare combined and referred to as Wernicke-Korsakoff syn-drome. By itself, Wernicke’s produces ataxia, confusion, andparalysis of some ocular motor muscles. Both syndromesresult from compulsive ingestion of alcohol that supersedesnutritional intake (see Chap. 30). Indeed, this syndrome usu-ally is found in 40- to 70-year-old clients with alcoholism anda history of steady and progressive alcohol intake. In time,they develop a vitamin B1 (thiamin) deficiency that directlyinterferes with glucose production (the brain’s main nutrient),resulting in symptomatology (Sadock & Sadock, 2007). Clientshave great difficulty with recent memory, specifically learningnew information. Because they cannot recall recent events,they fill in memory gaps with fabricated or imagined data( ). This is truly a case of anterograde amne-sia. Clients have no awareness of their memory defect, nor dothey care.
The prognosis for people experiencing amnestic disordersvaries greatly. As with other cognitive disorders, etiology deter-mines duration and severity. With Wernicke-Korsakoff syn-drome, administration of thiamin can help alleviate someataxia. Generally, however, memory impairment remains.
confabulation
members about dosages, schedules, and possible sideeffects. Team members also must take responsibility forassessing the client’s response and any possible side effects.
Preserving the Family UnitFamily members must be prepared for the personal toll thattheir new role as caregivers may take. Nurses can provideinformation concerning creative ways to care for loved ones,including providing counseling and information about respitecare. Day care for clients is one possibility that allows relativesto rest from their extensive caregiving activities and allowsthem to continue with their own daily routines and responsi-bilities (FIGURE 31.10). Through day care, a spouse or childmay be able to retain a job and income and have the energyto care for the client during evening and weekend hours.Some communities have overnight respite care to give thecaregiver welcomed “down time.”
Family support groups and individual family counselingmay help some families experiencing stress or having difficultycoping. As previously noted, one of the most effective inter-ventions is to educate family members about the necessaryskills of caregiving. Nurses empower families when they workwith relatives to increase their problem-solving skills. Showingfamily members that they have options and linking them tocommunity-based services are tremendous contributions.
Although many families wish to keep their loved ones athome as long as possible, all must recognize that long-termcare is an option. Only the family can make this decision, butprofessional care providers should tactfully raise this issueoccasionally.
● E V A L U A T I O NOutcomes for clients may focus less on improving cognitionand more on maintaining current functioning for as long aspossible and on successful adaptations by clients and familyto the ongoing decline. When evaluation of the plan of care
684 Psychiatric DisorderssixU N I T
figure 31.10 Adult day care centers can provide respite out-lets for family members who have to work or need a reprievefrom the ongoing work involved in preserving the healthand safety of clients with dementia. They also may providea socialization outlet, particularly for clients with mild tomoderate problems.

dying and death, and emotional responses of family membersstruggling with their own fears and guilt challenge the phys-ical stamina and mental acumen of the most dedicated andexperienced nurses.
To preserve “self,” nurses overcome with responsibilitiesmay begin to burn out. Some nurses may begin to approachclient care with a “policy-only” mentality and sequester them-selves emotionally from situations or interactions. They maypersonally develop problems with substances and health andmay engage in frequent absenteeism, tardiness, and turnover.
Nurses who find themselves burning out must recognizethe signs of this stress reaction and take steps to intervenebefore becoming locked into a pattern. Those who noticesigns of burnout should seek help from healthcare profession-als and their supervisors.
NURSE’S SELF-CARENurses working with clients who have dementia may experi-ence challenging feelings that arise from knowing there is, asyet, no cure for the ongoing cerebral degeneration. Thosewho work with clients who have dementia deliver highlystressful care. In nursing homes especially, staff membersface arduous work environments with intense labor and clientdemands. Debilitating illnesses, the psychological overlay of
Cognitive Disorders 68531C H A P T E R
Amnestic Disorder Due to a General MedicalCondition (Specify)
• Memory is impaired as manifested by impaired ability tolearn new information or inability to recall previouslylearned information.
• The memory disturbance significantly impairs social oroccupational functioning and represents a significantdecline from previous functioning.
• The memory disturbance does not occur exclusively duringdelirium or dementia.
• Evidence from the history, physical examination, or labora-tory tests supports that the disturbance is directly causedby a medical condition (including physical trauma).
SpecifyTransient is if memory impairment lasts for 1 month or less.Chronic is if it lasts for more than 1 month.
D S M - I V - T R B O X 3 1 . 3
Amnestic DisordersSubstance-Induced Persisting Amnestic Disorder
• Memory is impaired as manifested by impaired ability to learnnew information or recall previously learned information.
• The memory disturbance significantly impairs social oroccupational functioning and represents a significantdecline from previous functioning.
• The memory disturbance does not occur exclusively duringdelirium or dementia and persists beyond the usual durationof substance intoxication or withdrawal.
• Evidence from the history, physical examination, or labora-tory tests supports that the memory disturbance is etiologi-cally related to the persisting effects of substance use.
Adapted with permission from the American Psychiatric Association (APA). (2000). Diagnostic and statistical manual of mental disorders (4th ed., text rev.). Washington, DC: Author.
✔C h e c k p o i n t Q u e s t i o n s13. What is the hallmark of amnestic disorders?14. What is confabulation?
Chapter Summary
• Cognitive disorders appear throughout the general population. They are especially prominent among older adults.
• Possible etiologies of cognitive disorders include primarybrain disease, systemic disturbances, influences of exo-genous substances, and withdrawal and residual effects ofexogenous substances.
• Aberrant behaviors associated with cognitive disordersmay include deficits in the sensorium, attention span,orientation, perception, and memory.
• Symptoms of cognitive disorders may be approached interms of acute onset and chronic progression.
• Gathering and analyzing assessment data for a client with acognitive disorder requires participation of family membersor friends who have been in close contact with the client.
reviewing and applying your knowledgereviewing and applying your knowledge

4. The nurse questions the wife of a client with dementia toassess if she is at risk for depression or anxiety related toher caregiving activities. Which of the following state-ments or questions would be most useful in elicitinginformation?
a. “You must feel overwhelmed by your caregivingresponsibilities. Tell me about it.”
b. “Why don’t you tell me about what your usual day is like?”
c. “Do you feel stressed by your caregiving responsibilities?”
d. “Do you wish you had more help with your husband?”
5. A client with early-stage Alzheimer’s disease is startedon donepezil. The nurse is evaluating the caregiver’sunderstanding of the medication and determines that thecaregiver has understood the instructions when shemakes which of the following statements?
a. “My husband will only need to take this medicationonce a day.”
b. “This medicine will not affect his stomach and can betaken between meals.”
c. “This medication will prevent my husband’s memoryproblems from worsening.”
d. “This medication may cause urinary retention. I’llmonitor his intake and output.”
Critical Thinking Questions
1. Reread CASE VIGNETTE 31.1 and CASE IN POINT 31.1.Compare how the memory of each client is affected.What are the differences and similarities in behavior?
2. Compare and contrast the prognoses for both clients.
3. What nursing interventions would be appropriate foreach client?
4. Would you work with the families differently? How and why?
• Continuum of care involves the collaborative efforts of theentire interdisciplinary healthcare team.
• Goal-setting for the client with an organic disorderfocuses on eliminating the organic etiology, preventingacceleration of symptoms, and preserving dignity. Pre-serving optimal levels of functioning and preventing further decline are key goals.
• Specific nursing interventions strive to maintain theclient’s optimal physical health, structure the environ-ment, promote socialization and independent functioning,and preserve the family unit.
Study Questions
1. Delirium develops in a 78-year-old man recovering fromemergency hip surgery. He seems to be hallucinating andis mildly confused. Which of the following would thenurse do first?
a. Loosely apply a vest restraint.
b. Obtain an order for haloperidol.
c. Arrange for an unlicensed assistant to sit with the client.
d. Move the client to a room close to the nurse’s station.
2. An 82-year-old woman with no history of neurologicdysfunction is admitted to the hospital with a possiblebowel obstruction. She has been vomiting for severaldays. In addition to managing her medical care, nursesare monitoring the client for signs of delirium. Which ofthe following assessment findings would suggest thatdelirium may be developing in the client?
a. The client removes her IV line and tries to climb overthe side rails to get out of bed.
b. The client has trouble finding the right word whenspeaking.
c. The client requests pain medication frequently.
d. The client is not sleeping well at night.
3. A 70-year-old woman with dementia, Alzheimer’s typelives at home with her husband, who is her full-timecaregiver. The nurse is teaching the husband about inter-ventions to prevent injury. Which of the following suggestions would be most appropriate?
a. Put childproof caps on bottles containing cleaning fluids.
b. Put cleaning fluids on a high shelf.
c. Lock cleaning fluids in a cabinet in the kitchen.
d. Store cleaning fluids in plain bottles in the garage.
686 Psychiatric DisorderssixU N I T

Hepburn, K. W., Lewis, M., & Sherman, C. W. (2003). The savvy care-giver program: Developing and testing a transportable dementiafamily caregiver training program. Gerontologist, 43(6), 908–915.
Lacasse, H., Perreault, M. M., & Williamson, D. R. (2006). System-atic review of antipsychotics for the treatment of hospital-associated delirium in medically or surgically ill patients. Annalsof Pharmacotherapy, 40(11), 1966–1973.
Larson, E. B., Wang, L., Bowen, J. D., McCormick, W. C., Teri, L.,Crane, P., & Kukull, W. (2006). Exercise is associated withreduced risk for incident dementia among persons 65 years of ageand older. Annals of Internal Medicine, 144(2), 73–81.
Levenson, J. L., Collins, J., & Puram, D. (2005). Images in psycho-somatic medicine: The Clock-Drawing Test. Psychosomatics, 46,77–78.
Maidmant, I., Fox, C., & Boustani, M. (2006). Cholinesterase inhibitorsfor Parkinson’s disease dementia. Cochrane Database of System-atic Reviews, Jan 25;(1):CD004747.
McAvay, G., Van Ness, P. H., Bogardus, S. T., Zhang, Y., Leslie,D. L., Leo-Summers, L. S., et al. (2006). Older adults dischargedfrom the hospital with delirium: 1-year outcomes. Journal of theAmerican Geriatrics Society, 54(8), 1245–1250.
McGonigal-Kenney, M. L., & Schutte, D. L. (2004). Non-pharmacologicmanagement of agitated behaviors in persons with Alzheimer disease and other chronic dementing conditions. Iowa City, IA:University of Iowa Gerontological Nursing Interventions ResearchCenter, Research Dissemination Core.
McShane, R., Arreosa Sastre, A., & Minakaran, N. (2006). Meman-tine for dementia. Cochrane Database of Systematic Reviews, Apr19;(2):CD003154.
Milgram, N. W., Head, E., Zicker, S. C., Ikeda-Douglas, C., Murphey,H., Muggenburg, B. A., et al. (2004). Long-term treatment withantioxidants and a program of behavioral enrichment reduces age-dependent impairment in discrimination and reversal learning inbeagle dogs. Experimental Gerontology, 39(5), 753–765.
Milgram, N. W., Head, E., Zicker, S. C., Ikeda-Douglas, C., Murphey, H., Muggenburg, B. A., et al. (2005). Learning ability in aged beagledogs is preserved by behavioral enrichment and dietary fortification:A two year longitudinal study. Neurology of Aging, 26(1), 77–90.
Moorhead, S., Johnson, M., Maas, M. L., & Swanson, E. (2008).Nursing outcomes classification (NOC) (4th ed.). St. Louis, MO:Mosby.
NANDA-I. (2007). Nursing diagnoses: Definitions and classification(2007–2008). Philadelphia: Author.
National Institute on Aging (NIA). (2007). Alzheimer’s Disease Edu-cation and Referral Center. Progress report on AD 2005–2006.Retrieved October 13, 2007, from www.nia.nih.gov/Alzheimers.
National Institute of Neurological Disorders and Stroke (NINDS).(2007). The dementias: Hope through research. Retrieved October 17, 2007, from www.ninds.nih.gov.
Neal, M., & Briggs, M. (2003). Validation therapy for dementia.Cochrane Database of Systematic Reviews, (3):CD001394.
O’Connell, A. M., & Mion, L. C. (2003). Use of physical restraints in theacute care setting. In M. D. Mezey, T. Fulmer, & I. Abraham (Eds.),Geriatric nursing protocols for best practice (2nd ed., pp. 116–140).New York, NY: Springer.
Park, M., Hsiao-Chen Tang, J., & Ledford, L. (2005). Changing thepractice of physical restraint use in acute care. Iowa City: Universityof Iowa Gerontological Nursing Interventions Research Center,Research Translation and Dissemination Core.
Podewils, L. J., Guallar, E., Kuller, K. H., Fried, L. P., Lopez, O. L.,Carlson, M., et al. (2005). Physical activity, APOE, genotype anddementia like findings from the Cardiovascular Health CognitionStudy. American Journal of Epidemiology, 161(7), 639–651.
Rahknone, T., Eloniemi-Sulkava, U., Rissanen, S., Vafanen, A.,Viramo, P., & Sulkava, R. (2003). Dementia with Lewy bodiesaccording to the consensus criteria in a general population aged
referencesAbbott, R. D., White, R., Ross, G. W., Masaki, K. H., Curb, J. D., &
Petrovich, H. (2004). Walking and dementia in physically capableelderly men. Journal of the American Medical Association, 292(12),1447–1453.
Alexopoulos, G. S., Streim, J., Carpenter, D., & Docherty, J. P.;Expert Consensus Panel for Using Antipsychotic Drugs in OlderPatients. (2004). Using antipsychotic agents in older patients.Journal of Clinical Psychiatry, 65(Suppl. 2), 5–99; discussion100–102; quiz 103–104.
American Psychiatric Association. (2000). Diagnostic and statisticalmanual of mental disorders (4th ed., text rev.). Washington, DC:Author.
Balas, M. C., Deutschman, C. S., Sullivan-Marx, E. M., Strumpf,N. E., Alston, R. P., & Richmond, T. S. (2007). Delirium in olderpatients in surgical intensive care units. Journal of NursingScholarship, 39(2), 147–154.
Birks, J. S., & Grimley-Evans, J. (2007). Ginkgo biloba for cognitiveimpairment and dementia. Cochrane Database of SystematicReviews, Apr 18;(2):CD003120.
Birks, J. S., Grimley-Evans, J., Iakovidou, V., & Tsolaki, M. (2000).Rivastigmine for Alzheimer’s disease. Cochrane Database ofSystematic Reviews, (4):CD001191.
Birks, J. S., & Harvey, R. (2006). Donepezil for dementia due toAlzheimer’s disease. (Cochrane Review). Cochrane Database of Systematic Reviews, Jan 25;(1):CD001190.
Brodaty, H., Green, A., & Koschera, A. (2003). Meta-analysis ofpsychosocial interventions for caregivers of people with dementia.Journal of the American Geriatrics Society, 51(5), 657–664.
Bulechek, G. M., Butcher, H. K., & McCloskey Dochterman, J. (2008).Nursing interventions classification (NIC) (5th ed.). St. Louis, MO:Mosby.
Cohen-Mansfield, J. (2003). Non-pharmacologic interventions forpsychotic symptoms in dementia. Journal of Geriatric Psychiatryand Neurology, 16(4), 219–224.
Cole, M. G. (2004). Delirium in elderly patients. American Journal ofGeriatric Psychiatry, 12, 7–21.
Coon, D. W., Thompson, L., Steffan, A., Sorocco, K., & Gallagher-Thompson, D. (2003). Anger and depression management: Psycho-education skill training interventions for women caregivers of arelative with dementia. Gerontologist, 43(5), 678–689.
Doody, R. S., Stevens, J. C., Beck, C., Dubinsky, R. M., Kaye, J. A.,Gwyther, L., et al. (2001). Practice parameter: Management ofdementia (an evidence-based review). Report of the Quality Stan-dards Subcommittee of the American Academy of Neurology.Neurology, 56(9), 1154–1166.
Fick, D. M., Hodo, K. M., Lawrence, F., & Inouye, S. K. (2007). Rec-ognizing delirium superimposed on dementia: Assessing nurses’knowledge using case vignettes. Journal of Gerontological Nursing,33(2), 40–47; 48–49.
Foreman, M. D., Mion, L. C., Trygstad, L., & Fletcher, K. (2003).Delirium: Strategies for assessing and treating. In M. D. Mezey, T.Fulmer, & I. Abraham (Eds.), Geriatric nursing protocols for bestpractice (2nd ed., pp. 116–140). New York, NY: Springer.
Geldmacher, D. (2007). Treatment guidelines for Alzheimer’s disease:Redefining perceptions in primary care. Primary Care Companionto Journal of Clinical Psychiatry, 9, 2.
Gurwitz, J. H., Field, T. S., Harrold, L. R., Rothschild, J., Debellis, K.,Seger, A. C., et al. (2003). Incidence and preventability of adversedrug events among older persons in the ambulatory setting. Jour-nal of the American Medical Association, 289(9), 1107–1116.
Hebert, L. E., Scherr, P. A., Bienias, J. L., Bennett, D. A., & Evans,D. A. (2003). Alzheimer disease in the U.S. population: Preva-lence estimates using the 2000 census. Archives of Neurology,60(8), 1119–1122.
Cognitive Disorders 68731C H A P T E R

Tabet, N., Birks, J., & Grimley-Evans, J. (2000). Vitamin E forAlzheimer’s disease. Cochrane Database of Systematic Reviews,(4):CD002854.
Tabet, N., & Feldman, H. (2003). Ibuprofen for Alzheimer’s disease.Cochrane Database of Systematic Reviews, (2):CD004031.
Thiru-Chelvam, B. (2004). Bathing persons with dementia. Iowa City,IA: University of Iowa Gerontological Nursing InterventionsResearch Center, Research Dissemination Core.
Werezak, L. J., & Morgan, D. G. (2003). Creating a therapeuticpsychosocial environment in dementia care: A preliminary frame-work. Journal of Gerontological Nursing, 29(12), 18–25.
Werner, P. (2003). Nursing care adaptations, behavioral inter-ventions, environmental changes and sensory enhancement: Conceptual, process and outcome issues. In D. P. Hay, D. T.Klein, L. K. Hay, G. T. Grossberg, & J. S. Kennedy (Eds.), Agitation in patients with dementia: A practical guide to diag-nosis and management (pp. 91–102). Washington, DC: AmericanPsychiatric Publishing.
Weuve, J., Kung, J. H., Manson, J., Bretcher, M. M., Ware, J. H., &Goldstein, F. (2004). Physical activity, including walking and cog-nitive function in older women. Journal of the American MedicalAssociation, 292(12), 1454–1461.
web resourcesAlzheimer’s Association: www.alz.orgAlzheimer’s Disease Education and Referral (ADEAR) Center:
http://alzheimer’s.orgChildren of Aging Parents (CAPs): www.aoa.dhhs.gov/coa/dir/77.htmlEldercare Locator: www.aoa.dhhs.gov/elderpage/locator.html
75 years or older. Journal of Neurology, Neurosurgery and Psychi-atry, 74(5), 720.
Registered Nurses Association of Ontario (RNAO). (2003). Screeningfor delirium, dementia and depression in older adults. Toronto,Ontario, Canada: Author.
Rigney, T. S. (2006). Delirium in the hospitalized elder and recom-mendations for practice. Geriatric Nursing, 27(3), 151–157.
Sadock, B. J., & Sadock, V. A. (2007). Delirium, dementia, andamnesic and other cognitive disorders and mental disorders due to a general medical condition. In B. J. Sadock & V. A. Sadock(Eds.), Kaplan and Sadock’s synopsis of psychiatry: Behavioralsciences/clinical psychiatry (10th ed., pp. 319–349). Philadelphia,PA: Lippincott Williams & Wilkins.
Schumaker, S. A., Legault, C., Rapp, S. R., Thal, L., Wallace, R. B.,Ockene, J. K., et al. (2003). Estrogen plus progestin and the inci-dence of dementia and mild cognitive impairment in post-menopausal women: The Women’s Health Initiative MemoryStudy: A randomized controlled trial. Journal of the AmericanMedical Association, 289(20), 256–262.
Schuurmans, M. J., Shortridge-Baggett, L. M., & Duursma, S. A.(2003). The Delirium Observation Screening Scale: A screeninginstrument for delirium. Research and Theory for Nursing Prac-tice, 17(1), 31–50.
Scott, H. D., & Laake, K. (2001). Statins for the prevention ofAlzheimer’s disease. Cochrane Database of Systematic Reviews,(4):CD003160.
Snowdon, D. A. (2003). Healthy aging and dementia: Findings fromthe Nun Study. Annals of Internal Medicine, 139(5 Pt 2), 450–454.
Sunderland, T., Mirza, N., & Linker, G. (2004). Cognitive enhancers.In A. F. Schatzberg & C. B. Nemeroff (Eds.), Textbook of psy-chopharmacology (3rd ed., pp. 639–650). Washington, DC: Amer-ican Psychiatric Publishing.
688 Psychiatric DisorderssixU N I T