collagenous colitis: a cause of chronic diarrhea diagnosed only by biopsy of normal appearing...
TRANSCRIPT

Rectum 1980;23:567-9.10. Geboes K, Broeckaert L, Vantrappen G. Varices of the colon: "
diagnosis by colonoscopy. Gastrointest Endosc 1975;22:43-5.11. Pickens CA, Tedesco FJ. Colonic varices-unusual cause of
rectal bleeding. Am J GastroenteroI1980;73:73-4.12. Izsak EM, Finley JM. Colonic varices. Three case reports and
review of the literature. Am J Gastroenterol 1980;73:131-6.13. Van der Jagt EJ. Varices of the colon. Diagn Imaging
1983;52:230-5.
Collagenous colitis: a cause of chronicdiarrhea diagnosed only by biopsy ofnormal appearing colonic mucosa
William B. Salt II, MDPedro P. L1aneza, MD
In 1976, Lindstrom1 described an abnormal subepithelial deposition of collagen in the colonic mucosaof a patient with chronic diarrhea. This collagenouscolitis now appears to be a distinct clinical and pathologic entity. Since the original report, more than 20cases have been described to date.1-19 Our objective isto alert the endoscopist to this colonic cause of chronicwatery diarrhea, since it is usually necessary to biopsycolonic mucosa in order to diagnose collagenous colitis. The mucosa in this disorder is often of normalappearance at colonoscopy. We describe a case ofcollagenous colitis in which the colonic mucosa wastypically normal at colonoscopy and mucosal biopsywas essential in establishing the diagnosis.
CASE REPORT
A 70-year-old white woman was referred with an 18month history of diarrhea of gradual onset. Her premorbidbowel habit had been one formed stool daily. The diarrheahad progressed to the point that she was having an averageof 8 to 10 watery bowel movements daily. The frequency ofdaily stools ranged from as few as three to as many as 15.She had never noted blood, pus, or mucus in the stools. Thecondition was relatively painless, although she did note somemild and intermittent lower abdominal cramping relievedwith defecation. She denied any consistent weight loss, fever,or loss of appetite. She had mild hypertension and had takenDyazide(' for 5 years, although the temporary discontinuation of the drug had not relieved the diarrhea. She took noother drugs regularly.
Her physical examination was entirely normal, with noevidence of thyroid dysfunction, protein-calorie malnutrition, or vitamin or nutrient deficiency.
The initial laboratory studies included a normal completeblood count and white blood cell differential, multichemistry
From the Department of Internal Medicine, Mount Carmel MedicalCenter, and Department of Medicine, Ohio State University, Columbus, Ohio. Reprint requests: William B. Salt II, Department ofInternal Medicine, Mount Carmel Medical Center, 793 West StateStreet, Columbus, Ohio 43222.
VOLUME 32, NO.6, 1986
14. Federle M, Clark RA. Mesenteric varices: a source of mesosystemic shunts and gastrointestinal hemorrhage. GastrointestRadioI1979;4:331-7.
15. Patel KR, Wu TK, Powers SR Jr. Varices of the colon as acause of gastrointestinal hemorrhage: report of a case andreview of the literature. Dis Colon Rectum 1979;22:321-3.
16. Sauerbruch T, Weinzierl M, Dietrich HP, Antes G, EisenbergJ, Paumgartner G. Sclerotherapy of a bleeding duodenal varix.Endoscopy 1982;14:187-9.
profile, and thyroid function. A previous consultant hadobtained the following studies, all of which were normal:three stools for ova and parasites, four separate stool determinations for occult blood, bacterial stool culture, stool forphenolphthalein, fecal leukocytes, duodenal aspirate for ova,parasites, and quantitative bacterial culture, proctosigmoidoscopy, and barium enema. She had failed to respond totherapeutic trials with cholestyramine, metronidazole, bulking agents, loperamide hydrochloride, and doxepin.
Evaluation included a normal upper gastrointestinal series with small bowel follow through and D-xylose absorption test. A quantitative 72-hour stool collection yieldedfecal fat of 3.1 g/24 hours and weight of 420 g/24 hours.Colonoscopy including terminal ileoscopy was performed,and the mucosa was grossly normal without discernablemacroscopic abnormality. Random biopsies throughout theentire colon all confirmed the diagnosis of collagenous colitis(Fig. 1 and 2). Biopsies of the terminal ileum were normal.
DISCUSSION
The patient described in this report demonstratesmany of the characteristics of the previously publishedcases of "collagenous colitis."1-19 Most of these caseswere women in their forties and fifties (range, 23 to89 years of age). The predominant clinical manifestation of this entity is chronic watery diarrhea in theabsence of both steatorrhea and blood or pus in thestool. Other symptoms described include abdominalpain, distension, and nausea.
The light microscopic appearance of collagenouscolitis is characterized by a collagenous band measuring 10 to 60 fl in thickness deposited immediatelybeneath the colonic epithelium (Figs. 1 and 2). Thethickness of this abnormal collagen band is evidenton light microscopy. This collagen band stains eosinophilic with hematoxylin and eosin and green withMasson's trichrome. Amyloidosis can mimic this entity; however, it can be differentiated with ultrastructural studies and Congo red staining.4
, 5 Ultrastructural studies of collagenous colitis have demonstratedthe abnormal amount of subepithelial collagen fibersof normal periodicity and their tendency to be arranged around small capillaries.6
The etiology and pathogenesis of collagenous colitisis obscure. Bogomoletz et al.2 and Van den Oord etal.3 studied normal control subjects and patients with
421
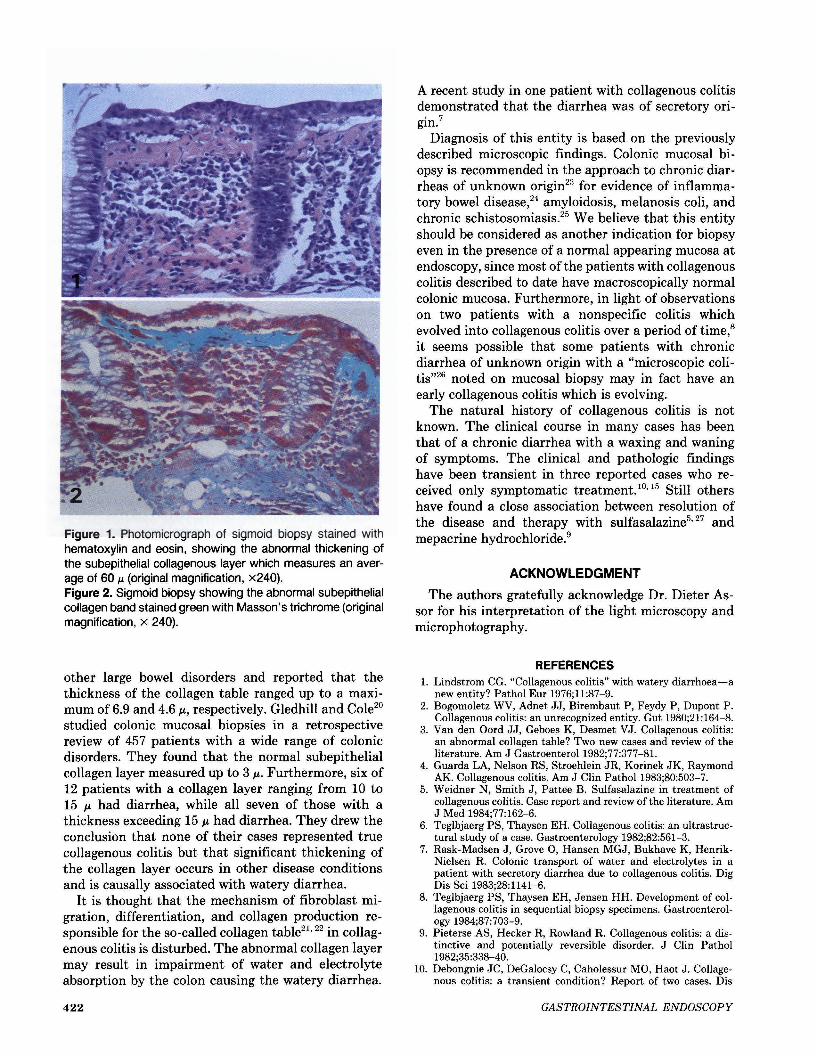
Figure 1. Photomicrograph of sigmoid biopsy stained withhematoxylin and eosin, showing the abnormal thickening ofthe subepithelial collagenous layer which measures an average of 60 f.L (original magnification, x240).Figure 2. Sigmoid biopsy showing the abnormal subepithelialcollagen band stained green with Masson's trichrome (originalmagnification, x 240).
other large bowel disorders and reported that thethickness of the collagen table ranged up to a maximum of 6.9 and 4.6 J.L, respectively. Gledhill and Cole20
studied colonic mucosal biopsies in a retrospectivereview of 457 patients with a wide range of colonicdisorders. They found that the normal subepithelialcollagen layer measured up to 3 J.L. Furthermore, six of12 patients with a collagen layer ranging from 10 to15 J.L had diarrhea, while all seven of those with athickness exceeding 15 J.L had diarrhea. They drew theconclusion that none of their cases represented truecollagenous colitis but that significant thickening ofthe collagen layer occurs in other disease conditionsand is causally associated with watery diarrhea.
It is thought that the mechanism of fibroblast migration, differentiation, and collagen production responsible for the so-called collagen table21,22 in collagenous colitis is disturbed. The abnormal collagen layermay result in impairment of water and electrolyteabsorption by the colon causing the watery diarrhea.
422
A recent study in one patient with collagenous colitisdemonstrated that the diarrhea was of secretory origin.7
Diagnosis of this entity is based on the previouslydescribed microscopic findings. Colonic mucosal biopsy is recommended in the approach to chronic diarrheas of unknown origin23 for evidence of inflammatory bowel disease,24 amyloidosis, melanosis coli, andchronic schistosomiasis.25 We believe that this entityshould be considered as another indication for biopsyeven in the presence of a normal appearing mucosa atendoscopy, since most ofthe patients with collagenouscolitis described to date have macroscopically normalcolonic mucosa. Furthermore, in light of observationson two patients with a nonspecific colitis whichevolved into collagenous colitis over a period of time,8it seems possible that some patients with chronicdiarrhea of unknown origin with a "microscopic colitis,,26 noted on mucosal biopsy may in fact have anearly collagenous colitis which is evolving.
The natural history of collagenous colitis is notknown. The clinical course in many cases has beenthat of a chronic diarrhea with a waxing and waningof symptoms. The clinical and pathologic findingshave been transient in three reported cases who received only symptomatic treatment.10,15 Still othershave found a close association between resolution ofthe disease and therapy with sulfasalazine5,27 andmepacrine hydrochloride.9
ACKNOWLEDGMENT
The authors gratefully acknowledge Dr. Dieter Assor for his interpretation of the light microscopy andmicrophotography.
REFERENCES1. Lindstrom CG. "Collagenous colitis" with watery diarrhoea-a
new entity? Pathol Eur 1976;11:87-9.2. Bogomoletz WV, Adnet JJ, Birembaut P, Feydy P, Dupont P.
Collagenous colitis: an unrecognized entity. Gut 1980;21:164-8.3. Van den Oord JJ, Geboes K, Desmet VJ. Collagenous colitis:
an abnormal collagen table? Two new cases and review of theliterature. Am J Gastroenterol 1982;77:377-81.
4. Guarda LA, Nelson RS, Stroehlein JR, Korinek JK, RaymondAK. Collagenous colitis. Am J Clin PathoI1983;80:503-7.
5. Weidner N, Smith J, Pattee B. Sulfasalazine in treatment ofcollagenous colitis. Case report and review of the literature. AmJ Med 1984;77:162-6.
6. Teglbjaerg PS, Thaysen EH. Collagenous colitis: an ultrastructural study of a case. Gastroenterology 1982;82:561-3.
7. Rask-Madsen J, Grove 0, Hansen MGJ, Bukhave K, HenrikNielsen R. Colonic transport of water and electrolytes in apatient with secretory diarrhea due to collagenous colitis. DigDis Sci 1983;28:1141-6.
8. Teglbjaerg PS, Thaysen EH, Jensen HH. Development of collagenous colitis in sequential biopsy specimens. Gastroenterology 1984;87:703-9.
9. Pieterse AS, Hecker R, Rowland R. Collagenous colitis: a distinctive and potentially reversible disorder. J Clin Pathol1982;35:338-40.
10. Debongnie JC, DeGalocsy C, Caholessur MO, Haot J. Collagenous colitis: a transient condition? Report of two cases. Dis
GASTROINTESTINAL ENDOSCOPY

Colon Rectum 1984;27:672-6.11. Colina F, Munoz-Yague MT, Solis-Herruzo JA, Vazquez G,
Perez-Barrios A. Collagenous colitis: the clinical and morphological features. Postgrad Med J 1982;58:390-5.
12. Yeshaya C, Novis B, Bernheim J, Leichtmann G, Samara M,Griffel B. Collagenous colitis. Report of a case. Dis ColonRectum 1984;27:111-3.
13. Bogomoletz WV, Potet F, Capron JP, Triplet C, de la Lande P,Sayegh R. Collagenous colitis (abstract). Gut 1983;24:A500,F60.
14. Erlendsson J, Fenger C, Meinicke J. Arthritis and collagenouscolitis. Scand J Rheumatol 1983;12:93-5.
15. Eaves ER, McIntyre RLE, Wallis PL, Korman MG. Collagenous colitis: a recently recognized reversible clinicopathologicalentity. Aust NZ J Med 1983;13:630-2.
16. Grouls V, Vogel J, Sorger M. Collagenous colitis. Endoscopy1982;14:31-3.
17. Nielsen VT, Vetner M, Harslof E. Collagenous colitis. Histopathology 1980;4:83-6.
18. Fausa 0, Foerster A. Collagenous colitis (abstract). Scand JGastroenteroI1983;18(suppI86):15.
19. Bamford MJ, Matz JA, Armstrong JA, Harris AR. Collagenouscolitis: a case report and review of the literature. Pathology1982;14:481-4.
20. Gledhill A, Cole FM. Significance of basement membrane thickening in the human colon. Gut 1984;25:1085-8.
VOLUME 32, NO.6, 1986
21. Pascal RR, Kaye GI, Lane N. Colonic pericryptal fibroblastsheath: replication, migration, and cytodifferentiation of a mesenchymal cell system in adult tissue. I. Autoradiographic studiesof normal rabbit colon. Gastroenterology 1968;54:835-51.
22. Kaye GI, Lane N, Pascal RR. Colonic pericryptal fibroblastsheath: replication, migration, and cytodifferentiation of a mesenchymal cell system in adult tissue. II. Fine structural aspectsof normal rabbit and human colon. Gastroenterology1968;54:852-65.
23. Read NW, Krejs GJ, Read MG, Santa Ana CA, Morawski SG,Fordtran JS. Chronic diarrhea of unknown origin. Gastroenterology 1980;78:264-71.
24. Surawicz CM, Meisel JL, Ylvisaker T, Saunders DR, RubinCEo Rectal biopsy in the diagnosis of Crohn's disease: value ofmultiple biopsies and serial sectioning. Gastroenterology1981;81:66-71.
25. Krejs GJ, Fordtran JS. Diarrhea. In: Sleisenger MH, FordtranJS, eds. Gastrointestinal disease. Philadelphia: WB Saunders,1983:257-80.
26. Kingham JGC, Levison DA, Ball JA, Dawson AM. Microscopiccolitis-a cause of chronic watery diarrhoea. Br Med J1982;285:1601-4.
27. Farah DA, Mills PR, Lee FD, McLay A, Russell RI. Collagenouscolitis: possible response to sulfasalazine and local steroid therapy. Gastroenterology 1985;88:792-7.
423