color stability of white mineral trioxide aggregate in ... · in contact with hypochlorite solution...
TRANSCRIPT

Color Stability of White Mineral Trioxide Aggregatein Contact with Hypochlorite SolutionJosette Camilleri, PhD
AbstractIntroduction: One of the uses of white mineral trioxideaggregate (MTA) is as an apical barrier in immatureteeth. Although this treatment has been reported tohave high success rates, a number of cases of discolor-ation have been noted. The aim of this research was toinvestigate the color stability of white MTA in contactwith various solutions used in endodontics. Methods:The change in color of white MTA after immersion inwater, sodium hypochlorite, or hydrogen peroxide wasassessed by viewing the color change on digital photo-graphs and also by using a spectrophotometer. WhiteMTA, white Portland cement, and bismuth oxide wereassessed. The changes in the material after immersionin the different solutions were assessed by x-ray diffrac-tion analysis and Fourier transform infrared spectros-copy. Results: Immersion of white MTA and bismuthoxide in sodium hypochlorite resulted in the formationof a dark brown discoloration. This change was notobserved in Portland cement. X-ray diffraction analysisand Fourier transform infrared analysis displayed thereduction of sodium hypochlorite in contact with bis-muth oxide and MTA to sodium chloride. Conclusions:Contact of white MTA and other bismuth-containingmaterials with sodium hypochlorite solution should beavoided. (J Endod 2014;40:436–440)
Key WordsBismuth oxide, characterization, color stability, dentalmaterial, radiopacifier, root-end filling materials
Mineral trioxide aggregate (MTA) is composed of a mixture of Portland cement andbismuth oxide (1). MTA was introduced for use as a root-end filling material and
for repair of root perforations. However, it is currently used for a variety of applicationsincluding pulp capping, apexification procedures, as a dressing over pulpotomies, andmany other endodontic procedures (2). Initially only gray MTA was available; however,because of potential discoloration effect of gray MTA, white MTA has been introducedinto endodontic treatment for the same purposes. No difference was observed in theoutcome of treatment (3) and biocompatibility (4) of the different variants of MTA.White MTA (MTA Branco; Angelus, Londrina, Brazil) has been used to seal root perfo-rations where the gray version (MTA Angelus) had been reported to cause discolorationof the marginal gingiva (5).
Tooth discoloration has been reported with the use of both gray and white MTA(MTA Angelus). In fact, both types of MTA induced significant decreases in L*, a*,and b* values (Commission Internationale de l’!eclairage), with the color change beinggreater with grayMTA. GrayMTA led to clinically perceptible crown discoloration after 1month, whereas the total color change caused by white MTA exceeded the perceptiblethreshold for the human eye after 3 months. This suggests that the application of grayMTA in the aesthetic zone should be avoided, whereas white MTA should be used withcaution when filling pulp chambers with the materials (6). Crown discoloration hasbeen reported when MTA was used as a dressing for molar pulpotomies instead ofcalcium hydroxide (7), as an apical barrier after initial calcium hydroxide therapy(MTA Angelus) (8), for apexification procedures of replanted teeth (ProRoot MTA)(9), for treatment of fractured teeth (10), for treatment of root resorption (MTAAngelus) (11), and for revascularization of immature necrotic permanent teeth (12).
Attempts at removal of MTA from the root canal revealed a change in color of theMTA (13). After the removal of MTA from the tooth where it was placed as a dressing, asignificant color change was observed in the tooth crown, which was further improvedwith internal bleaching (14). Application of dentin bonding agent before placement ofMTA may prevent tooth discoloration (15).
The recommendations by clinicians to date have been to use MTA cautiously in theaesthetic zone. The aim of this researchwas to investigate the color stability of whiteMTAin contact with various solutions used in endodontics.
Materials and MethodsMaterials used in this study included Portland cement (PC) (CEM 1, 52.5 N;
LaFarge Cement, Birmingham, UK), ProRoot MTA (Dentsply Tulsa Dental, JohnsonCity, TN; lot number 09001920), and bismuth oxide (Sigma Aldrich, St Louis, MO).The cements were mixed at a liquid-to-powder ratio of 0.30.
The cements were cured for 24 hours at 37!C and 100% humidity, after which thecements and bismuth oxide powder were immersed in different solutions for 24 hours:
1. Water2. Sodium hypochlorite solution (Milton; Laboratoire Rivadis, Louzy, France)3. Hydrogen peroxide (Bells Sons & Co Ltd, Southport, UK)
The cements and bismuth oxide powder were then dried and tested.
Assessment of Color StabilityCylindrical specimens 10 mm in diameter and 2 mm high were prepared for MTA
and Portland cement by curing in the molds for 24 hours at 100% humidity and 37!C.
From the Department of Restorative Dentistry, Faculty ofDental Surgery, University of Malta, Msida, MSD, Malta.
Address requests for reprints to Prof Josette Camilleri,Department of Restorative Dentistry, Faculty of Dental Surgery,University of Malta, Medical School, Mater Dei Hospital, Msida,MSD 2090,Malta. E-mail address: [email protected]/$ - see front matter
Copyright ª 2014 American Association of Endodontists.http://dx.doi.org/10.1016/j.joen.2013.09.040
Basic Research—Technology
436 Camilleri JOE — Volume 40, Number 3, March 2014
The color of the specimens was assessed by using a spectrophotometer(Minolta CM-50Bi; Minolta Co Ltd, Osaka, Japan). The CommissionInternationale de l’!eclairage system was used to calculate the difference
in color. The value of the luminance (L) and the coordinates of thechromatic component (a and b) were measured before and afterimmersion in different solutions. Color photographs of the specimens
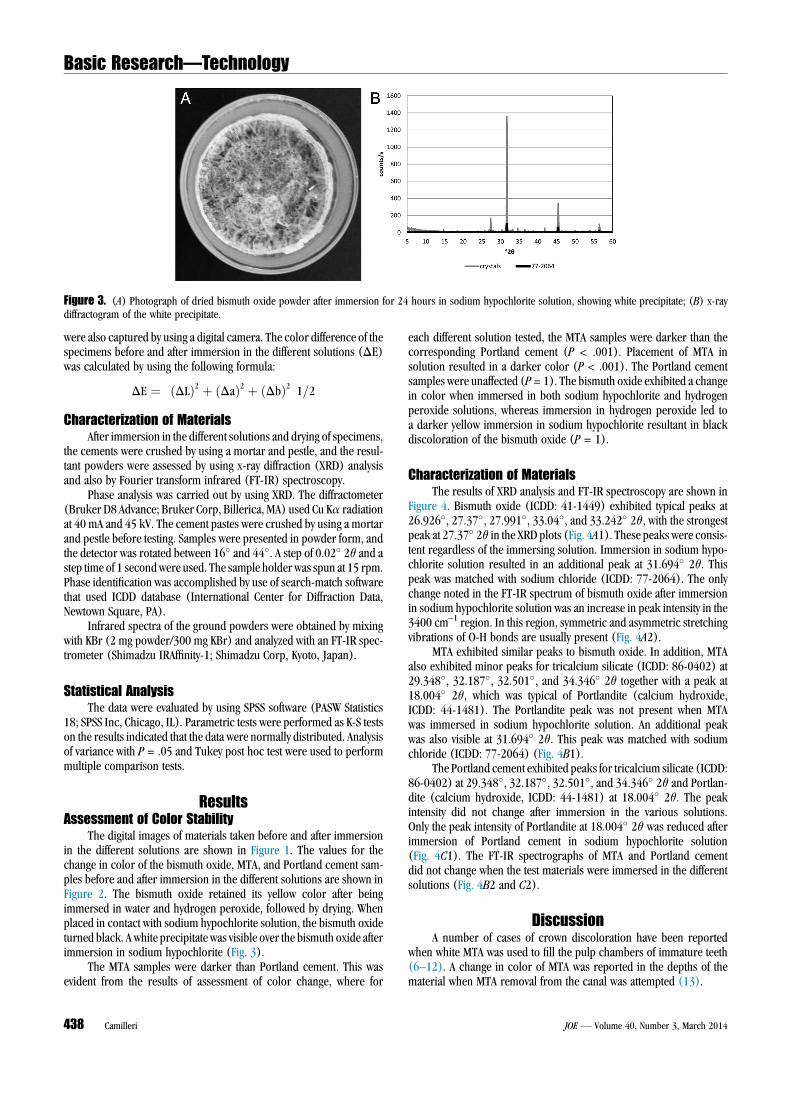
Figure 2. Color change recorded by spectrophotometer for the different test materials after immersion in different solutions.
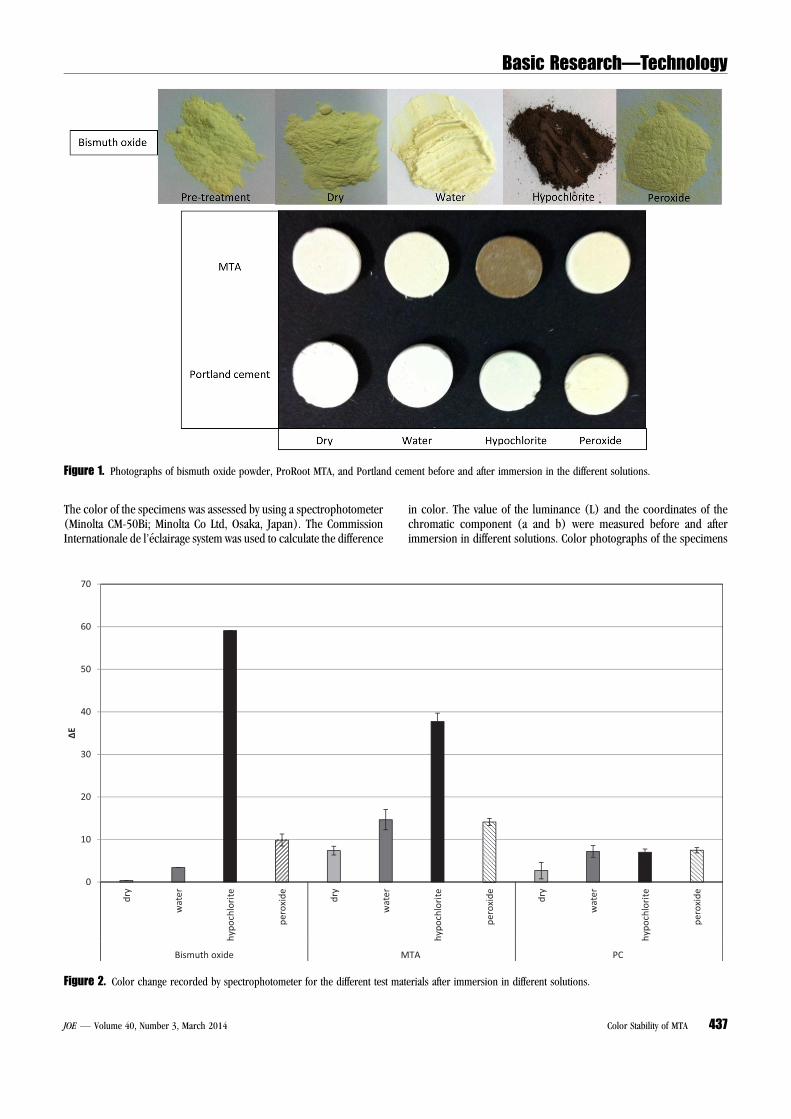
Figure 1. Photographs of bismuth oxide powder, ProRoot MTA, and Portland cement before and after immersion in the different solutions.
Basic Research—Technology
JOE — Volume 40, Number 3, March 2014 Color Stability of MTA 437
were also captured by using a digital camera. The color difference of thespecimens before and after immersion in the different solutions (DE)was calculated by using the following formula:
DE "!#DL$2 % #Da$2 % #Db$2
"1=2
Characterization of MaterialsAfter immersion in the different solutions and drying of specimens,
the cements were crushed by using a mortar and pestle, and the resul-tant powders were assessed by using x-ray diffraction (XRD) analysisand also by Fourier transform infrared (FT-IR) spectroscopy.
Phase analysis was carried out by using XRD. The diffractometer(Bruker D8 Advance; Bruker Corp, Billerica, MA) used Cu Ka radiationat 40 mA and 45 kV. The cement pastes were crushed by using a mortarand pestle before testing. Samples were presented in powder form, andthe detector was rotated between 16! and 44!. A step of 0.02! 2q and astep time of 1 secondwere used. The sample holder was spun at 15 rpm.Phase identification was accomplished by use of search-match softwarethat used ICDD database (International Center for Diffraction Data,Newtown Square, PA).
Infrared spectra of the ground powders were obtained by mixingwith KBr (2 mg powder/300 mg KBr) and analyzed with an FT-IR spec-trometer (Shimadzu IRAffinity-1; Shimadzu Corp, Kyoto, Japan).
Statistical AnalysisThe data were evaluated by using SPSS software (PASW Statistics
18; SPSS Inc, Chicago, IL). Parametric tests were performed as K-S testson the results indicated that the data were normally distributed. Analysisof variance with P = .05 and Tukey post hoc test were used to performmultiple comparison tests.
ResultsAssessment of Color Stability
The digital images of materials taken before and after immersionin the different solutions are shown in Figure 1. The values for thechange in color of the bismuth oxide, MTA, and Portland cement sam-ples before and after immersion in the different solutions are shown inFigure 2. The bismuth oxide retained its yellow color after beingimmersed in water and hydrogen peroxide, followed by drying. Whenplaced in contact with sodium hypochlorite solution, the bismuth oxideturned black. A white precipitate was visible over the bismuth oxide afterimmersion in sodium hypochlorite (Fig. 3).
The MTA samples were darker than Portland cement. This wasevident from the results of assessment of color change, where for
each different solution tested, the MTA samples were darker than thecorresponding Portland cement (P < .001). Placement of MTA insolution resulted in a darker color (P < .001). The Portland cementsamples were unaffected (P= 1). The bismuth oxide exhibited a changein color when immersed in both sodium hypochlorite and hydrogenperoxide solutions, whereas immersion in hydrogen peroxide led toa darker yellow immersion in sodium hypochlorite resultant in blackdiscoloration of the bismuth oxide (P = 1).
Characterization of MaterialsThe results of XRD analysis and FT-IR spectroscopy are shown in
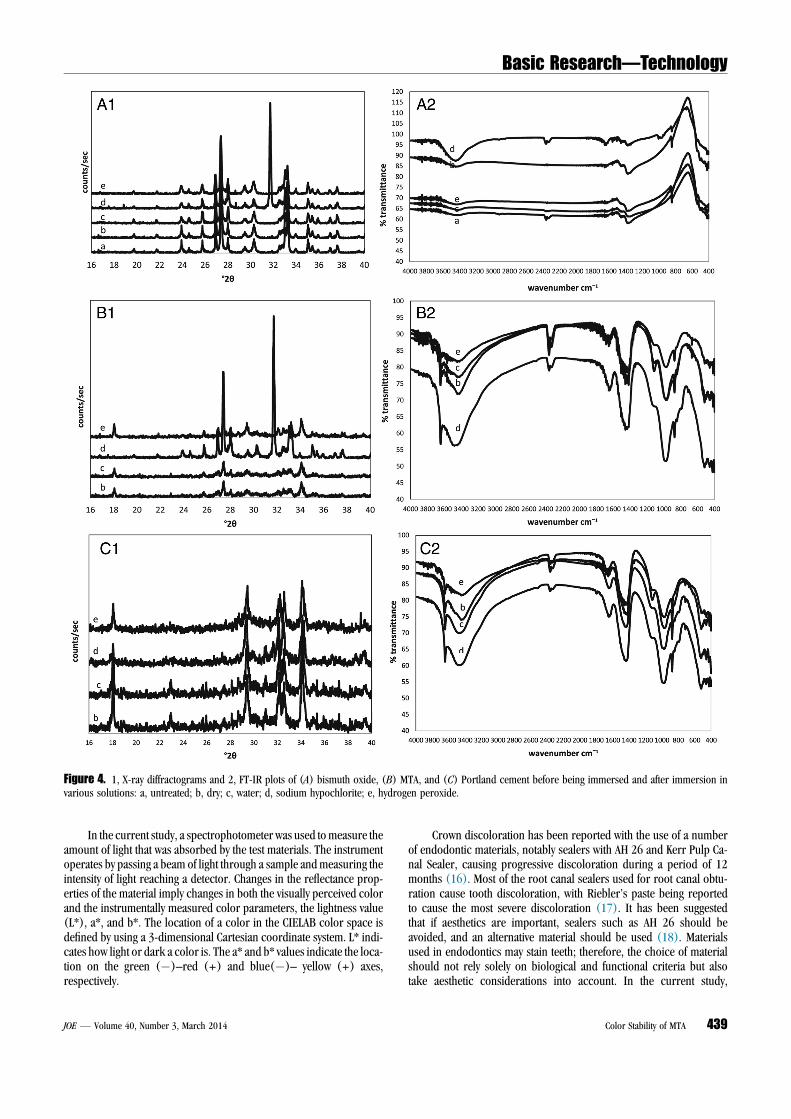
Figure 4. Bismuth oxide (ICDD: 41-1449) exhibited typical peaks at26.926!, 27.37!, 27.991!, 33.04!, and 33.242! 2q, with the strongestpeak at 27.37! 2q in the XRD plots (Fig. 4A1). These peaks were consis-tent regardless of the immersing solution. Immersion in sodium hypo-chlorite solution resulted in an additional peak at 31.694! 2q. Thispeak was matched with sodium chloride (ICDD: 77-2064). The onlychange noted in the FT-IR spectrum of bismuth oxide after immersionin sodium hypochlorite solution was an increase in peak intensity in the3400 cm–1 region. In this region, symmetric and asymmetric stretchingvibrations of O-H bonds are usually present (Fig. 4A2).
MTA exhibited similar peaks to bismuth oxide. In addition, MTAalso exhibited minor peaks for tricalcium silicate (ICDD: 86-0402) at29.348!, 32.187!, 32.501!, and 34.346! 2q together with a peak at18.004! 2q, which was typical of Portlandite (calcium hydroxide,ICDD: 44-1481). The Portlandite peak was not present when MTAwas immersed in sodium hypochlorite solution. An additional peakwas also visible at 31.694! 2q. This peak was matched with sodiumchloride (ICDD: 77-2064) (Fig. 4B1).
The Portland cement exhibited peaks for tricalcium silicate (ICDD:86-0402) at 29.348!, 32.187!, 32.501!, and 34.346! 2q and Portlan-dite (calcium hydroxide, ICDD: 44-1481) at 18.004! 2q. The peakintensity did not change after immersion in the various solutions.Only the peak intensity of Portlandite at 18.004! 2q was reduced afterimmersion of Portland cement in sodium hypochlorite solution(Fig. 4C1). The FT-IR spectrographs of MTA and Portland cementdid not change when the test materials were immersed in the differentsolutions (Fig. 4B2 and C2).
DiscussionA number of cases of crown discoloration have been reported
when white MTA was used to fill the pulp chambers of immature teeth(6–12). A change in color of MTA was reported in the depths of thematerial when MTA removal from the canal was attempted (13).
Figure 3. (A) Photograph of dried bismuth oxide powder after immersion for 24 hours in sodium hypochlorite solution, showing white precipitate; (B) x-raydiffractogram of the white precipitate.
Basic Research—Technology
438 Camilleri JOE — Volume 40, Number 3, March 2014
In the current study, a spectrophotometer was used tomeasure theamount of light that was absorbed by the test materials. The instrumentoperates by passing a beam of light through a sample andmeasuring theintensity of light reaching a detector. Changes in the reflectance prop-erties of the material imply changes in both the visually perceived colorand the instrumentally measured color parameters, the lightness value(L*), a*, and b*. The location of a color in the CIELAB color space isdefined by using a 3-dimensional Cartesian coordinate system. L* indi-cates how light or dark a color is. The a* and b* values indicate the loca-tion on the green (&)–red (+) and blue(&)– yellow (+) axes,respectively.
Crown discoloration has been reported with the use of a numberof endodontic materials, notably sealers with AH 26 and Kerr Pulp Ca-nal Sealer, causing progressive discoloration during a period of 12months (16). Most of the root canal sealers used for root canal obtu-ration cause tooth discoloration, with Riebler’s paste being reportedto cause the most severe discoloration (17). It has been suggestedthat if aesthetics are important, sealers such as AH 26 should beavoided, and an alternative material should be used (18). Materialsused in endodontics may stain teeth; therefore, the choice of materialshould not rely solely on biological and functional criteria but alsotake aesthetic considerations into account. In the current study,
Figure 4. 1, X-ray diffractograms and 2, FT-IR plots of (A) bismuth oxide, (B) MTA, and (C) Portland cement before being immersed and after immersion invarious solutions: a, untreated; b, dry; c, water; d, sodium hypochlorite; e, hydrogen peroxide.
Basic Research—Technology
JOE — Volume 40, Number 3, March 2014 Color Stability of MTA 439

MTA and Portland cement did not exhibit the same changes whenexposed to different solutions. This is in contrast to a previous studyreporting no statistically significant difference between Portlandcement and MTA that were placed in contact with bovine dentin for12 months (19). Blood contamination was shown to exacerbate thechange in color (19, 20). In both studies (19, 20) all the toothspecimens were washed with sodium hypochlorite solution beforeobturation with the different test materials.
The current study evaluated the effect that routine solutions used inendodontics have on whiteMTA. The hydrogen peroxide did not seem toaffect the test materials. An investigation of the effect of bleaching agentson the microstructure of MTA exhibited deterioration in the MTA sur-face after exposure to hydrogen peroxide. The elemental distributionwas affected, with a decrease in calcium and an increase in siliconshown (21). No discoloration of MTA was demonstrated in the currentstudy; however, the effect on MTA microstructure of contact with solu-tions used routinely in endodontics should be investigated. The sodiumhypochlorite solution that is used in every endodontic case being treatedcaused a change in color in both white MTA and bismuth oxide, whichforms part of MTA. Contact of bismuth-containing substances withsodium hypochlorite led to a dark brown, nearly black discoloration.The sodium hypochlorite solution was reduced to sodium chloride.This was evident from the white precipitate formed on the bismuthoxide. XRD analysis of this precipitate showed definite peaks for sodiumchloride. Thus, a reaction is occurring, with the sodium hypochloritelosing oxygen.
The bismuth oxide did not exhibit any evident chemicalchanges as observed in the FT-IR and XRD analysis. The changein color could indicate a change from oxide to bismuth metal,which is black in color. Bismuth gives similar peaks to bismuth ox-ide in XRD analysis. Other methods are thus suggested to verify thechange from bismuth oxide to bismuth. If the oxide is converted toa metal, oxygen is lost to the environment. Thus in both reactions,oxygen gas is liberated in a confined space within the tooth. Theclinical implications of this chemical reaction should be investigated.Another hypothesis put forward to explain the change in colorwould be the further oxidation of bismuth oxide that can causedestabilization of the oxide, with reaction of carbon dioxide inthe air leading to the formation of bismuth carbonate. Bismuth car-bonate is light sensitive (22). A recent investigation in the color sta-bility of white MTA showed distinctive light sensitivity of the whiteMTA in oxygen-free environments (23). In addition, it was reportedthat the combination of light and anaerobic conditions (similar tothose in clinical situations) results in differences in color of ProRootWMTA, Angelus WMTA, and Portland cement with bismuth oxideduring a period of 5 days. Only Biodentine and Portland cementdemonstrated color stability (24). From the current study and therecent investigations on color stability of various tricalcium silicatecement–based materials, it is very clear that the bismuth oxide isbeing affected by light and oxygen, thus producing a black precip-itate. Additional investigations on the exact mechanism leading tothese changes are necessary.
ConclusionsContact of white MTA and other bismuth-containing compounds
with sodium hypochlorite should be avoided because this leads toreaction of the bismuth oxide and formation of dark brown precipitate,which can discolor the tooth.
AcknowledgmentsThe author thanks the University of Malta Research Grant
committee for funding; Diagnostic Science Laboratory, HeritageMalta for access to equipment; Mr L. Spiteri of Diagnostic ScienceLaboratory, Heritage Malta, Mr J. Spiteri of the Department of Chem-istry, Faculty of Science, and Ing J. Camilleri of the Metallurgy andMaterials Science Laboratory, Faculty of Engineering, University ofMalta for their technical expertise; and Dr Heather Pitt Ford for dis-cussing this clinical problem.
The author denies any conflicts of interest related to this study.
References1. Torabinejad M, White DJ. Tooth filling material and use. United States patent num-
ber 5,769,638; 1995.2. Torabinejad M, Chivian N. Clinical applications of mineral trioxide aggregate.
J Endod 1999;25:197–205.3. Parirokh M, Asgary S, Eghbal MJ, et al. A comparative study of white and grey min-
eral trioxide aggregate as pulp capping agents in dog’s teeth. Dent Traumatol 2005;21:150–4.
4. Camilleri J, Montesin FE, Papaioannou S, et al. Biocompatibility of two commercialforms of mineral trioxide aggregate. Int Endod J 2004;37:699–704.
5. Bortoluzzi EA, Ara!ujo GS, Guerreiro Tanomaru JM, Tanomaru-Filho M. Marginalgingiva discoloration by gray MTA: a case report. J Endod 2007;33:325–7.
6. Ioannidis K, Mistakidis I, Beltes P, Karagiannis V. Spectrophotometric analysis ofcoronal discoloration induced by grey and white MTA. Int Endod J 2013;46:137–44.
7. Liu H, Zhou Q, Qin M. Mineral trioxide aggregate versus calcium hydroxide forpulpotomy in primary molars. Chin J Dent Res 2011;14:121–5.
8. Moore A, Howley MF, O’Connell AC. Treatment of open apex teeth using two types ofwhite mineral trioxide aggregate after initial dressing with calcium hydroxide in chil-dren. Dent Traumatol 2011;27:166–73.
9. Jacobovitz M, de Pontes Lima RK. The use of calcium hydroxide and mineral trioxideaggregate on apexification of a replanted tooth: a case report. Dent Traumatol 2009;25:e32–6.
10. Erdem AP, Ozdas DO, Dincol E, et al. Case series: root healing with MTA afterhorizontal fracture. Eur Arch Paediatr Dent 2009;10:110–3.
11. Jacobovitz M, de Lima RK. Treatment of inflammatory internal root resorption withmineral trioxide aggregate: a case report. Int Endod J 2008;41:905–12.
12. Dabbagh B, Alvaro E, Vu DD, et al. Clinical complications in the revascularization ofimmature necrotic permanent teeth. Pediatr Dent 2012;34:414–7.
13. Boutsioukis C, Noula G, Lambrianidis T. Ex vivo study of the efficiency of two tech-niques for the removal of mineral trioxide aggregate used as a root canal fillingmaterial. J Endod 2008;34:1239–42.
14. Belobrov I, Parashos P. Treatment of tooth discoloration after the use of white min-eral trioxide aggregate. J Endod 2011;37:1017–20.
15. Akbari M, Rouhani A, Samiee S, Jafarzadeh H. Effect of dentin bonding agent on theprevention of tooth discoloration produced by mineral trioxide aggregate. Int J Dent2012;2012:563203.
16. Parsons JR, Walton RE, Ricks-Williamson L. In vitro longitudinal assessment ofcoronal discoloration from endodontic sealers. J Endod 2001;27:699–702.
17. van der Burgt TP, Mullaney TP, Plasschaert AJ. Tooth discoloration induced by end-odontic sealers. Oral Surg Oral Med Oral Pathol 1986;61:84–9.
18. Thomson AD, Athanassiadis B, Kahler B, Walsh L. Tooth discoloration: stainingeffects of various sealers and medicaments. Aus Endod J 2012;38:2–9.
19. Lenherr P, Allgayer N, Weiger R, et al. Tooth discoloration induced by endodonticmaterials: a laboratory study. Int Endod J 2012;45:942–9.
20. Felman D, Parashos P. Coronal tooth discoloration and white mineral trioxideaggregate. J Endod 2013;39:484–7.
21. Tsujimoto M, Ookubo A, Wada Y, et al. Surface changes of mineral trioxide aggre-gate after the application of bleaching agents: electron microscopy and an energy-dispersive X-ray microanalysis. J Endod 2011;37:231–4.
22. Bismuth subcarbonate. Available at: http://en.wikipedia.org/wiki/Bismuth_subcarbonate. Accessed March 10, 2013.
23. Vall!es M, Mercad!e M, Duran-Sindreu F, et al. Color stability of white mineral trioxideaggregate. Clin Oral Investig 2013;17:1155–9.
24. Vall!es M, Mercad!e M, Duran-Sindreu F, et al. Influence of light and oxygen on thecolor stability of five calcium silicate–based materials. J Endod 2013;39:525–8.
Basic Research—Technology
440 Camilleri JOE — Volume 40, Number 3, March 2014