colorectal cancer - university...
TRANSCRIPT

Colorectal cancer
Chapelle, J Clin Oncol, 2010

Asit Paul, MD, PhD
11/24/15
Early-Stage Colorectal cancer:
Microsatellite instability, multi-gene assay & emerging molecular strategy

Mr. X:
A 50 yo asymptomatic male, Mr X, underwent staging
colonoscopy. Colonoscopy showed a 3 cm-mass in the
sigmoid colon. Staging scans showed no adenopathy or
distant metastases. CEA was 2.0 ng/mL (normal <3 ng/mL).
Patient underwent sigmoid colonic resection. Pathology
showed moderately differentiated adenocarcinoma,
invading upto muscularis propria (pT2). 20 lymph nodes
were retrieved and negative for metastasis.
What is the next step to do?
1. Observation
2. Adjuvant chemotherapy
3. Testing for MMR protein
4. Testing for RAS and BRAF status

Mr. Y:
A 45 yo M presented with 3 episodes of FBPR within a month.
Colonoscopy with EUS showed a 4-cm ulcerating-mass
obstructing the sigmoid colon, but no enlarged LN. Staging scans
showed no adenopathy or distant metastases. CEA was 4.2 ng/mL
(normal <3 ng/mL). Patient underwent R hemicolectomy with
diverting colostomy. Pathology showed a mucinous
adenocarcinoma with involvement of serosa (pT4). 27 lymph
nodes were retrieved and negative for metastasis.
What is the next step to do?
1. Observation
2. Adjuvant chemotherapy
3. Testing for MMR-protein
4. Multi-gene expression analysis

Current standard of care for
non-metastatic CRC
• Stage I (T1/T2, Node negative): • Surgery alone
• Stage II (T3/T4, Node-negative): • Surgery -> ??
• Stage III (any N, Node positive)• : Surgery + adjuvant chemotherapy

Adjuvant chemotherapy is
stage II CRC could be
beneficial, but the absolute
benefit is small (5.4% high-
risk, 3.6% low risk, over 5
years)
Lancet, 2007, 370:2020-29

Adjuvant Chemotherapy
Guidelines for stage II CRC
• pT4
• Tumor perforation
• Obstructing tumor
• Inadequate node sampling (<12
nodes)
High-risk
stage II Colon
cancer

Beyond the traditional measures
of risk stratification….
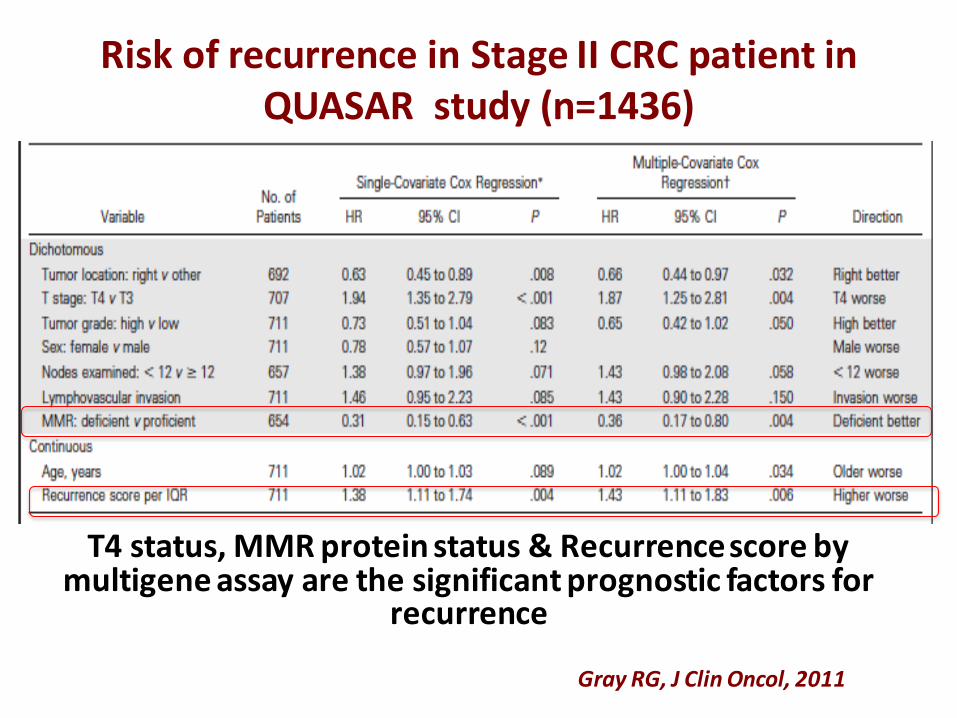
Risk of recurrence in Stage II CRC patient in QUASAR study (n=1436)
Gray RG, J Clin Oncol, 2011
T4 status, MMR protein status & Recurrence score by multigene assay are the significant prognostic factors for
recurrence

• Basics
• Testing strategy
• Clinical relevance
MMR & MSI

CRC carcinogenesis pathways
Villar & Gruber, Nat Rev Oncol, 2010

Microsatellites
Microsatellites are short (1-7 bp) repetitive
nucleotide sequences scattered throughout
human genome.
There are estimated 500,000 microsatellites in
human genome. Most common MS in human
genome is a dinucloide-repeats of A & C
Length of microsatellites varies from person-
to-person, but have a set length for an
individual person (‘DNA finger print’).

• Microsatellites are prone to replication error
• Erroneous replication process leads to increase or
decrease in number of repeats in MS known as
microsatellite instability (MSI)
Microsatellite Instability (MSI)
Gruber, J Nat Cancer Inst, 2003

In most cases, MSI may not have any
consequences. If MSI occurs in an important
gene, it leads to disease. MSI was first
described in XP.
MSI in an oncogene or tumor suppressor gene
increases the risk of cancer. Lynch syndrome is
the classic example of MSI as a result of germ-
line mutation of MMR gene
Consequence of MSI

Mismatched Repair Proteins (MMR)
• MMR proteins are responsible for
surveillance & correction of replication-
errors
• MMR proteins are products of 4 genes:
MLH1, MSH2, MSH6, PMS2
• Deficiency of MMR protein (MMR-d), due to
mutation of MMR gene (germ line or
sporadic), leads to replication error & MSI

Testing of MMR/MSI
• IHC of tumor tissue for MMR protein expressions
• MSI testing of tumor tissue
A panel of microsatellite
markers, is compared in
tumor tissue and normal
tissue. Core panel of
five markers are
generally used: BAT25,
BAT26, D2S123, D5S346,
and D17S250
Chapelle, J Clin Oncol, 2010
• DNA-based testing, PCR, gene-sequencing analysis
(blood or tumor tissue)

MMR Proteins
• MMR proteins make heterodimers
• MLH1 & MSH2 are the dominant partner of their pair
• MSH6 & PMS2 proteins are unstable in absence of their dominant partners

IHC patterns
of MMR
protein
expression
Richman, Int J of Oncol, 2015

Mr. Z:
A 51 yo M underwent staging colonoscopy. Colonoscopy
showed a non-obstructing 3 cm-mass in the ascending
colon. Staging scans showed no adenopathy or distant
metastases. CEA was 3.0 ng/mL. Patient underwent colonic
resection & anastomosis. Pathology showed mucinous
adenocarcinoma, invading through muscularis propria to
adjacent pericolonic tissue (pT3). 27 lymph nodes were
retrieved and negative for metastasis.
What is the next step to do?
1. Observation
2. Adjuvant chemotherapy
3. Testing for MMR proteins
4. Testing for RAS and BRAF status

Who should get testing for MMR/MSI
Testing for MMR protein and/or MSI should be done for all patients with newly-diagnosed colorectal cancer
ASCO, ESMO & ACG guidelines, 2014
Patients who are diagnosed with colorectal cancer <70 years, stage II tumors, or who meet the Bethesda Criteria
NCCN, 2015

Infiltrating Mucinous differentiation
Poorly differentiated
with medullary
growth pattern
Crohn-like lymphocytic
reaction
Phenotype of d-MMR/ MSI
Early age of onset, R sided tumors,
synchronus or metachronus tumors, high-grade/low-stage

Mr. ZMr. Z with pT3pN0M0 (stage II) colon cancer. His tumor resected tumor was tested for MMR-protein expression by IHC. Staining showed absence of MLH1 & PMS2-proteins, staining for MSH2 & MSH6 are positive.
What to do next?
1. Observation2. Adjuvant chemotherapy3. MSI-testing of tumor tissue4. Testing for BRAF mutation
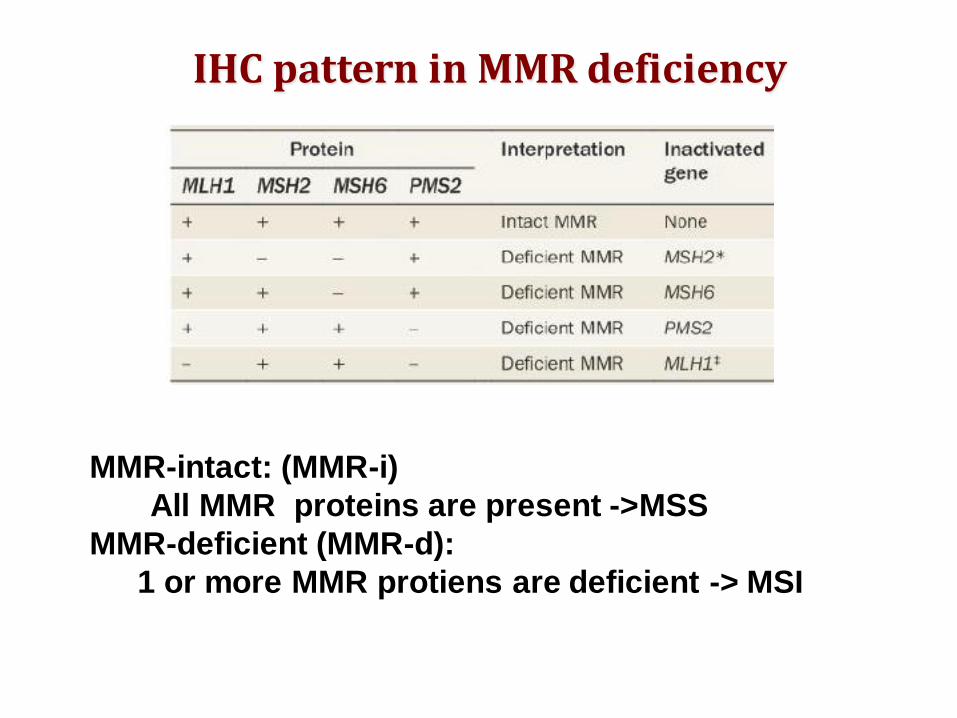
IHC pattern in MMR deficiency
MMR-intact: (MMR-i)
All MMR proteins are present ->MSS
MMR-deficient (MMR-d):
1 or more MMR protiens are deficient -> MSI

• 15% of CRCs are MMR-d (MSI)
• More commonly, MMR-d is
sporadic & is due to
hypermethylation of MLH1
gene promoter. Sporadic
tumors often carry the BRAF
V600E somatic mutation.
• Others have germ line
mutation of MMR gene
(MLH1,MSH2, MSH6, PMS2) i.e
Lynch syndrome
• In case of MLH1-loss by IHC,
BRAF testing should be done
prior to testing for Lynch
Syndrome

Majority of MMR deficiency are
sporadic, not Lynch Syndrome
• Loss of MLH1: Check BRAF mutation first. If wt,
genetic testing for LS
• Loss of MSH2, MSH6, PMS2: genetic testing for LS

Prognostic value ofMMR/MSI status in CRC

Gryffe, NEJM, 2000
• N=607, 50 y or younger
• 17% patients have MSI
• MSI has independent survival
advantage over other risk factors
• MSI tumors tend to metastasize
to LNs less

Patients with stage II & III CRC & MSI-status
have better prognosis
n outcome HR CI Data type
Dienstmann R, J Clin Oncol. 2015

MSI as a predictor of response to 5FU based chemotherapy
Villar & Gruber, Nat Rev Oncol, 2010

Mr. Z
Mr. Z with pT3pN0M0 (stage II) colon cancer. Patient’s resected
tumor was tested for MMR-protein expression by IHC.
Staining showed absence of MLH1 & PMS2-proteins,
staining for MSH2 & MSH6 are positive. BRAF mutation
testing of the tumor was done, which came out to be
mutated for BRAF 600E
Based on the molecular markers, who has the best & worst prognosis
1. MMR-i (MSS), BRAF wt, R sided tumor
2. MMR-i (MSS), BRAF V600 E mutated, L sided tumor
3. MMR-d (MSI), BRAF wt, R sided tumor
4. MMR-d (MSI), BRAF V600E mutated, R sided tumor

MSS- All site MSS- Left side MSS- Right side
Popovici, BMC cancer, 2013
In stage II-III colorectal cancer, BRAF mutation was confirmed a marker of
poor survival only in subpopulations involving microsatellite stable and
left-sided tumors (n=1423, PET-ACC3 cohort). KRAS status had no
prognostic value.
Prognostic value of BRAF V600E mutation

• BRAF V600E is considered poor prognostic factor in CRC
• Interpretation of BRAF V600E mutation should always be done
in the context of MSI status in early CRC
• The prognostic effect of MSI in early CRC overrides poor
prognosis determined by BRAF
• Worst prognosis is seen in patient with MMR-i (MSS) & L sided
tumorDienstmann R, J Clin Oncol. 2015

Mr. Q
A 51 yo M underwent staging colonoscopy. Colonoscopy showed
a non-obstructing 3 cm-mass in the sigmoid colon. Staging scans
showed no adenopathy or distant metastases. CEA was 3.0 ng/mL.
Patient underwent sigmoid colonic resection. Pathology showed
mucinous adenocarcinoma, invading through muscularis propria
to adjacent pericolonic tissue (pT3). 27 lymph nodes were
retrieved and negative for metastasis. IHC showed expression of
all 4 MMR proteins (MMR-i). 27 lymph nodes were retrieved and
negative for metastasis.
What is the next step to do?
1. Observation
2. Adjuvant chemotherapy
3. Molecular/genetic testing for MSI-status
4. Multi-gene assay

Multigene assay in CRC
Dienstmann R, J Clin Oncol. 2015


Risk of recurrence in Stage II CRC patient who were treated with edrecolomab or observation in CALGB
9851 study (n=162)
Venook, J Clin Oncol. 2013
Recurrence score
&
5 year risk of of recurrence

Incorporating RS & MMR-status in
decision making of stage II CRC
• T4 tumor: – High risk, independent of RS & MMR status
– Gene expression analysis in not needed
– Patient should receive adjuvant treatment
• T3 Tumor, MMR-deficient (MSI)– Good outcome, adjuvant chemotherapy is not
indicated
• T3 Tumor, MMR-intact (MSS)– Standard risk patient
– Multigene assay can identify high risk patient

• IHC of MMR proteins is recommended for all new
patients with CRC
• MLH1 loss by IHC can be associated with germ-line
mutation or sporadic mutation.
• Loss of MLH1 should have BRAF testing to rule out
sporadic mutation
• Loss of MLH2, MSH2, PMS2 are due to germ line
mutation.
• Germ line mutation of MMR-gene is the hall-mark of
Lynch Syndrome.
• Patients with MMR-d/ MSI have better prognosis
• Patients with BRAF V600E mutation has poor
prognosis, when combined with MSS state

Adjuvant chemotherapy in stage II CRC
Dienstmann R, J Clin Oncol. 2015

Adjuvant chemotherapy
• Stage III (node-positive), CRC patients are at high risk &
should receive adjuvant chemotherapy.
• In Stage II standard risk patients, MMR status & Multigene
assay should be taken into consideration in deciding
chemotherapy
• MMR-d (MSI) has good prognosis without adjuvant
treatment in stage II CRC.
• Stage II, MMR-i(MSS) can be risk stratified using
multigene assay
• To date, none of the multi-gene assay are predictive of
treatment benefit & should always be used in conjunction
with MMR status & clinico-pathologic variables

Emerging Molecular Strategy in
CRC

Herzig & Vassiliki, J Surg Onc, 2015

Hereditary Colorectal Neoplasms
• The Genetics of Colorectal Cancer
– Jasperson K & Burt RW, Surg Oncol Clin N Am,
2015: 24:683–703
• ACG clinical guideline
– Syngal et al, Am J Gastroenterol, 2015; 110: 223-
262
• Genetic/familial high risk assessment, NCCN
• GeneReviews@ NCBI

Hereditary CRC
• 5-6% of all CRCs are associated with
germ-line mutations, causing
hereditary predisposition
• Lynch syndrome is the most common,
accounting for 2-3% of all CRCs
• FAP patients account for <1% of CRCs
• Other hereditary CRCs are very rare

Jasperson, Sur Clin NA, 2015

Jasperson, Sur Clin NA, 2015
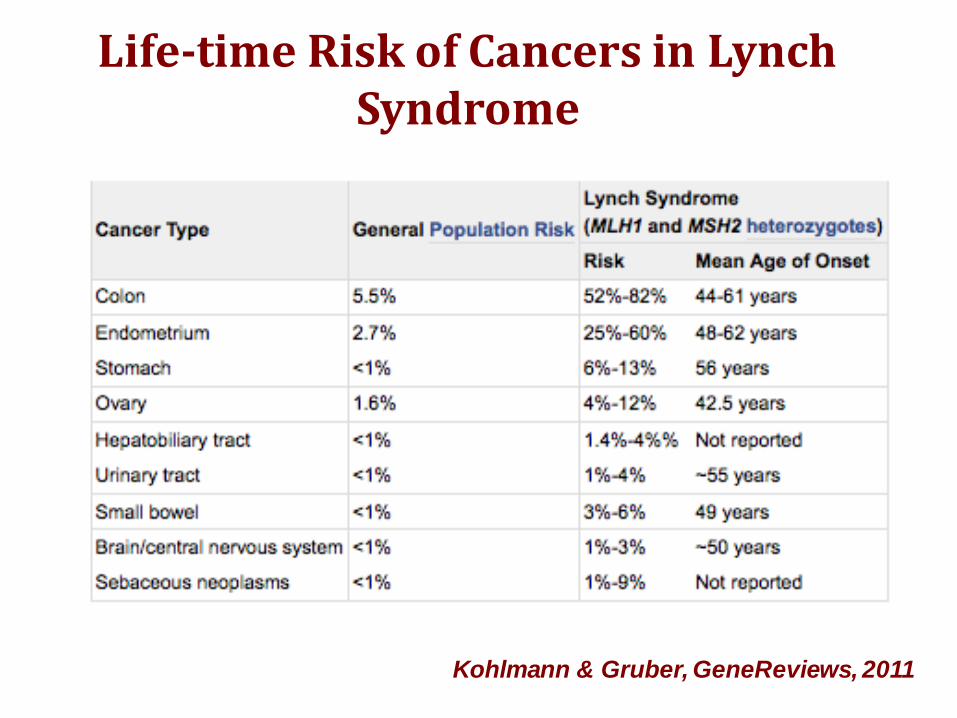
Life-time Risk of Cancers in Lynch Syndrome
Kohlmann & Gruber, GeneReviews, 2011

Kastrinos, JAMA, 2009
• 6342 individuals from 147 families• 31 families (21%) had at least 1
pancreas CA

Indications of MSI testing to rule out Lynch
Syndrome

Jasperson, Sur Clin NA, 2015

Questions?