coma and brain stem death
TRANSCRIPT

Coma
Coma and brain stem deathDavid Bates
AbstractComa is a medical emergency; after resuscitation the cause must be
defined and a prognosis provided. The situation is monitored using the
Glasgow Coma Scale and appropriate biochemical, neurophysiological
and imaging tests are performed. In this article an algorithm for the ex-
amination and assessment of the patient in coma is provided. Common
syndromes are identified and the process of investigation is explained.
Those factors which help determine prognosis are described and the
terminal conditions of brain stem death and persistent vegetative state
are defined.
Keywords brain stem death; clinical signs; coma; prognosis; vegeta-
tive state
Coma is seen most commonly in three clinical situations: • following head injury • after an overdose of sedating drugs • non-traumatic coma, most commonly caused by anoxia, is-
chaemia, infection or metabolic derangement.Assessment of patients in coma is a medical emergency; the
aims are to identify and, when possible, correct the pathological cause, to protect the brain from irreversible damage and to iden-tify patients for whom the prognosis is hopeless and in whom institution and persistence of resuscitative measures is inappro-priate and will only prolong the anguish of relatives and carers.1 It is important that doctors assessing patients in coma develop systems to enable recognition of changes in consciousness, to identify the likely diagnosis, and to define appropriate investiga-tive and therapeutic manoeuvres.
Definitions (Figure 1)
Normal consciousnessConsciousness is a state of awareness of self and environment in an individual provided with adequate stimuli. Normal conscious-ness is exhibited by patients who are fully responsive to stimuli and show appropriate behaviour and speech. Patients who are
David Bates MA FRCP is Professor of Clinical Neurology at the Royal
Victoria Infirmary, Newcastle upon Tyne, UK. He qualified at Cambridge
University and Middlesex Hospital, London, and trained in neurology
at the Mayo Clinic, Rochester, Minnesota, USA. His research interests
include coma and multiple sclerosis. Competing interests: none
declared.
mEDICINE 36:11 60
asleep can be roused from this state and are then able to perform normally.
Normal consciousness depends on integration of activity in both the ascending reticular activating substance (ARAS) of the brain stem and the neuronal connections between areas of the cerebral cortex.2 The ARAS extends throughout the brain stem from the spinal cord to the subthalamus; it determines arousal, which is shown by the phenomenon of awakening with eye opening, motor responses and the possibility of verbal commu-nication. The content of consciousness (the combination of psy-chological responses to feeling, emotions and mental activity) is mediated by the cerebral cortex. Damage to the brain stem affecting the ARAS, or significant bilateral damage to areas of the cerebral hemispheres, results in disturbance of normal con-sciousness (Figure 2).
ConfusionClouding of consciousness characterized by an impaired capac-ity to think, understand and respond to and remember stimuli is termed ‘confusion’. Patients are usually disoriented and exhibit reduced attention, inability to express thoughts, drowsiness and defects in memory. It is important to distinguish confusion from dysphasia, amnesia, acute psychosis, the retardation of severe depression and dementia. Confusion is most commonly seen as a result of toxic or metabolic abnormalities, particularly in the elderly.3
DeliriumDelirium is characterized by motor restlessness, hallucination, disorientation and sometimes delusion. Patients are often fright-ened and irritable. Delirium is commonly seen in patients with toxic or metabolic disorders, and can be mimicked by degenera-tive brain disease, acute psychosis and hypomania. Delirium can be regarded as a more profound state of confusion and should alert the doctor to impending coma.
StuporPatients in stupor appear to be asleep with little or no spon-taneous activity, responding only to vigorous stimulation then returning to somnolence. It may be difficult to distinguish stu-por from catatonic schizophrenia or severe retarded depression, but in stupor caused by organic disease an electroencephalogram (EEG) is always abnormal.
ComaComa is a state of unrousable unconsciousness without any psy-chologically understandable response to external stimuli or inner need. Patients may appear to be asleep, but are incapable of responding normally to external stimuli other than by eye open-ing, flexion or extension of the muscles in the limbs, or occa-sional grunting or groaning in response to pain.
Vegetative stateVegetative state is a condition of unawareness of self and envi-ronment in which patients breathe spontaneously, have a stable circulation and exhibit cycles of eye opening and eye closure that may simulate sleep and waking. Other terms used to describe this state include ‘coma vigile’, ‘apallic syndrome’, ‘cerebral death’, ‘neocortical death’ and ‘total dementia’. Vegetative state
1 © 2008 Elsevier Ltd. all rights reserved.

Coma
Normal consciousness Vegetative state
Locked-in syndrome Brain stem death
Cortex
Ascending reticular activating substance
Destruction of cortex and hemispheres
Intact ascending reticular activating substance
Intact ascending reticular activating substance
Damage to ventral pons
Intact cortex
Irremediable damage to brain stem
Figure 1
may be seen transiently in recovery from coma or may persist to death. It is usually seen in those with diffuse bilateral cerebral hemisphere disturbance with an intact brain stem, although it can occur following damage to the most rostral part of the brain stem. Vegetative state is most commonly seen after head injury or as a result of hypoxic–ischaemic damage following cardiac arrest.
Causes of coma
Focal brain stem lesions
Diffuse cortical pathology
Mass lesions
Uncal herniation causing IIIrd nerve palsy
Diencephalicherniation
Figure 2
mEDICINE 36:11 60
Because the individual appears to be awake but is unaware, vegetative state often causes distress to carers and relatives. If it persists for more than 6 months following coma without head injury, or for more than 12 months following head injury, the prognosis is very poor and a return to sentience is unlikely. With adequate nursing and support, patients in a continuing vegeta-tive state may enter a permanent vegetative state, which can continue for years and lead to major problems for relatives and carers. Avoidance of permanent vegetative state is one of the most important reasons for attempting to define prognosis early in coma.
Locked-in syndromeDamage to the ventral portion of the pons, below the level of the third nerve nuclei, results in locked-in syndrome, a rare con-dition in which there is total paralysis of the limbs and lower cranial nerves but consciousness is intact.4 Patients can open, elevate and depress their eyes but cannot move them horizon-tally, and have no other voluntary movement or speech. The diagnosis is made when the doctor recognizes that the patient can open his or her eyes voluntarily and close them in response to commands, and can therefore respond to verbal and sensory stimuli by blinking. The most common cause is infarction of the ventral pons, usually in hypertensive individuals. Locked-in syndrome is also seen in patients with pontine tumours or multiple sclerosis, in central pontine myelinolysis following profound hyponatraemia, and after head injury. The prognosis is poor, although some patients recover, usually with residual spasticity.
Psychogenic unresponsivenessThe term ‘pseudocoma’ (psychogenic unresponsiveness) is used in patients who appear to be unconscious and in coma, but are not. The simplest means of identifying pseudocoma is oculo-vestibular testing (see below), which reveals nystagmus and indicates that the patient has an intact brain stem and cortex.
2 © 2008 Elsevier Ltd. all rights reserved.

Coma
Assessment and management of coma
ResuscitationEstablishing adequate airway and circulation takes precedence over assessment of patients in coma. The decision on whether or not endotracheal intubation, assisted respiration and oxygen are required depends on the assessment of the airway, breath-ing and the PO2 measured by oximetry or sampling. This should be followed by establishment of intravenous access, at which time blood must be withdrawn for estimation of glucose and other metabolites, and to enable later estimation of drug levels. Patients in coma should receive thiamine, glucose and also nal-oxone if there is the possibility of opiate poisoning. Vasopressor agents and blood volume expansion may be required. Trauma should always be considered and, when likely, the neck should be immobilized. Evidence of injuries to other parts of the body must not be overlooked, particularly in the casualty department, where head injury, knife or gunshot wounds, flail chest and ruptured abdominal viscera should be excluded.
HistoryOnce the patient is stabilized, it is important to establish the history. This may be self-evident in those already in hospital in whom coma is the expected outcome in a diagnosed disease. When coma occurs unexpectedly in hospital, however, and in all patients admitted to the emergency unit, those who witnessed the onset of the coma or who accompanied the patient to hospital must be questioned. Admitting officers commonly fail to take an adequate history from the ambulance personnel or police who delivered the patient to hospital. Details of medical and therapeu-tic history, possible exposure to toxins and possibility of trauma must be emphasized.
It is usually possible to identify the cause from the history alone. Difficulties arise when the patient is found unconscious, or when an elderly patient is discovered at home days or weeks after a documented head injury. The most common complicat-ing factor in the assessment of unconscious patients is exposure to drugs or toxins (e.g. alcohol), particularly in those who have also suffered head trauma. The investigation and assessment of a patient found at home with empty tablet bottles and a ‘suicide note’ should clearly be different from that of a patient seen to collapse suddenly in a public place.
General examinationTemperature, pulse, blood pressure, respiration and examina-tion of the skin, cardiovascular system, chest and abdomen often yield important clues to the cause of loss of consciousness. • Fever is not diagnostic, but usually indicates systemic in-fection, meningitis, encephalitis or abscess; the presence of seizures increases the likelihood of these conditions. It is axi-omatic that any suspicion of meningitis should lead to use of antibiotics. Hypothermia is most commonly seen following ex-posure to low environmental temperatures, intoxication with alcohol or barbiturates, peripheral circulatory failure or pro-found myxoedema. • Tachyarrhythmia, bradyarrhythmia or evidence of valvular heart disease or peripheral emboli suggests a possible cardiogenic cause. Bruits over the carotid vessels suggest cerebrovascular disease, splinter haemorrhages endocarditis or collagen vascular disease.
mEDICINE 36:11 6
• Hypotension suggests possible shock, myocardial infarction or septicaemia, and Addison’s disease should be considered. Hypertension is a less helpful clinical sign because it may re-sult from a cerebral insult or indicate hypertensive encephalo-pathy. • It is important to assess respiration before providing respira-tory support. Slow, shallow breathing suggests drug intoxication, deep and rapid respiration suggests pneumonia or metabolic aci-dosis, periodic respiration suggests a cardiological or brain stem lesion, and rapid shallow respiration may indicate a brain stem lesion. • The odour of an unconscious patient’s breath may indicate al-cohol, ketones (diabetes) or the fetor of hepatic or renal failure. • Clubbing of the fingers suggests a respiratory or gastrointestinal abnormality. • Evidence of tracheal deviation, fluid in the chest or collapse of the lung suggests a respiratory cause. • In the abdomen, organ enlargement might indicate portal hypertension, polycystic kidneys and an associated subarachnoid haemorrhage, or abnormality in the blood-forming organs. • The general colour of the skin and mucous membranes may reveal anaemia, jaundice, cyanosis or the pink discoloration of carbon monoxide poisoning. Purpura suggests a bleeding dia-thesis; bruising around the head indicates trauma or a base-of-skull fracture. A rash may indicate an infective or inflammatory disease. Hyperpigmentation raises the possibility of Addison’s disease. Evidence of puncture wounds may identify individuals with diabetes or recreational drug users.
Involuntary movements should be noted, particularly focal jerking, which might indicate seizure activity or the presence of multi-focal myoclonus, usually indicative of diffuse anoxic injury.
Neurological examinationNeurological examination of an unconscious patient requires observation and assessment of reflex responses. Position, pos-ture and any spontaneous movements should be noted. The skull and spine should be examined, and neck stiffness and Kernig’s sign sought to identify meningeal irritation. Ophthalmoscopy identifies papilloedema, fundal haemorrhages, emboli and sub-hyaloid haemorrhage, indicating the presence of subarachnoid blood. Remember, the absence of papilloedema does not neces-sarily mean the intracranial pressure is not raised, but the pres-ence of spontaneous venous pulsation in the venules close to the disc is a useful sign to exclude it. The ears and fauces should also be examined.5
The most important aspects of the neurological examination are defining conscious level, eliciting brain stem responses and determining the presence of lateralizing clinical signs.
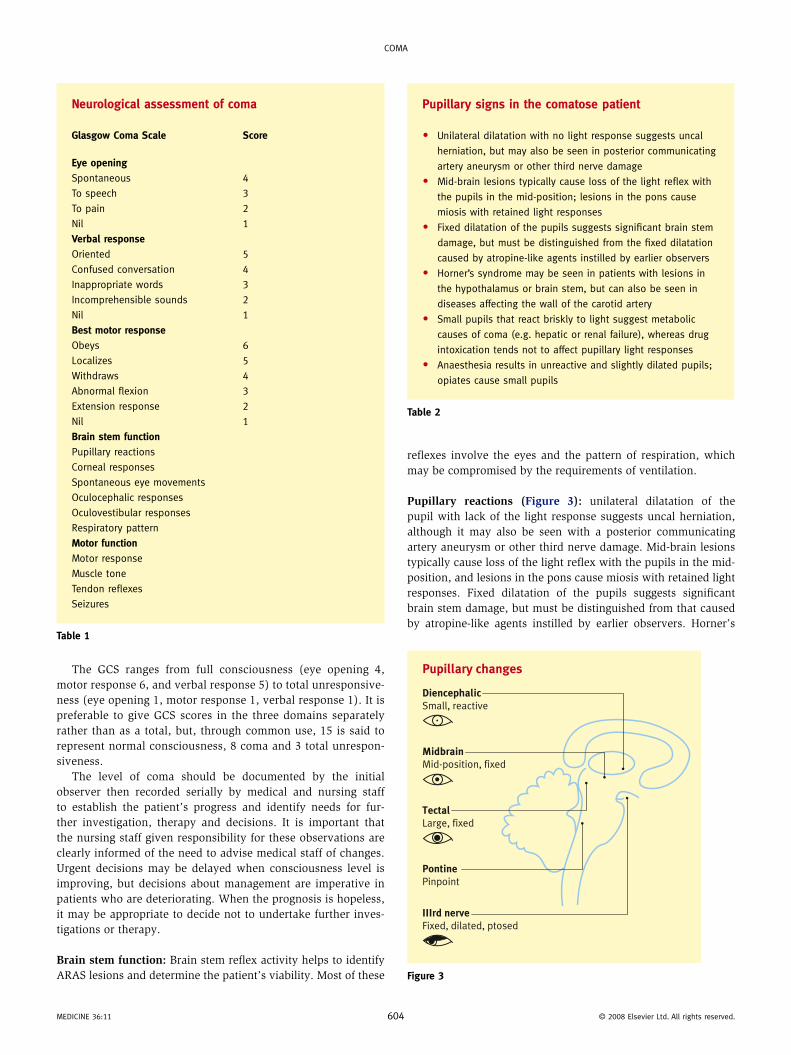
Conscious level: the most useful scale is the Glasgow Coma Scale (GCS),6 which measures patients’ response to graded stim-uli in terms of eye opening, motor response and verbal response (Tables 1 and 2). Patients are stimulated verbally by shouting their name, possibly using a nickname. Response to pain is assessed using supraorbital pressure as a central stimulus and nail-bed pressure as a peripheral stimulus; all four limbs are observed and the best response is recorded as the motor score. Any asymmetry should be noted and may be important in defin-ing lateralization.
03 © 2008 Elsevier Ltd. all rights reserved.
Coma
The GCS ranges from full consciousness (eye opening 4, motor response 6, and verbal response 5) to total unresponsive-ness (eye opening 1, motor response 1, verbal response 1). It is preferable to give GCS scores in the three domains separately rather than as a total, but, through common use, 15 is said to represent normal consciousness, 8 coma and 3 total unrespon-siveness.
The level of coma should be documented by the initial observer then recorded serially by medical and nursing staff to establish the patient’s progress and identify needs for fur-ther investigation, therapy and decisions. It is important that the nursing staff given responsibility for these observations are clearly informed of the need to advise medical staff of changes. Urgent decisions may be delayed when consciousness level is improving, but decisions about management are imperative in patients who are deteriorating. When the prognosis is hopeless, it may be appropriate to decide not to undertake further inves-tigations or therapy.
Brain stem function: Brain stem reflex activity helps to identify ARAS lesions and determine the patient’s viability. Most of these
Neurological assessment of coma
Glasgow Coma Scale Score
Eye openingSpontaneous 4
To speech 3
To pain 2
Nil 1
Verbal responseoriented 5
Confused conversation 4
Inappropriate words 3
Incomprehensible sounds 2
Nil 1
Best motor responseobeys 6
Localizes 5
Withdraws 4
abnormal flexion 3
Extension response 2
Nil 1
Brain stem functionPupillary reactions
Corneal responses
Spontaneous eye movements
oculocephalic responses
oculovestibular responses
Respiratory pattern
Motor functionmotor response
muscle tone
Tendon reflexes
Seizures
Table 1
mEDICINE 36:11 60
reflexes involve the eyes and the pattern of respiration, which may be compromised by the requirements of ventilation.
Pupillary reactions (Figure 3): unilateral dilatation of the pupil with lack of the light response suggests uncal herniation, although it may also be seen with a posterior communicating artery aneurysm or other third nerve damage. Mid-brain lesions typically cause loss of the light reflex with the pupils in the mid-position, and lesions in the pons cause miosis with retained light responses. Fixed dilatation of the pupils suggests significant brain stem damage, but must be distinguished from that caused by atropine-like agents instilled by earlier observers. Horner’s
Pupillary signs in the comatose patient
• Unilateral dilatation with no light response suggests uncal
herniation, but may also be seen in posterior communicating
artery aneurysm or other third nerve damage
• mid-brain lesions typically cause loss of the light reflex with
the pupils in the mid-position; lesions in the pons cause
miosis with retained light responses
• Fixed dilatation of the pupils suggests significant brain stem
damage, but must be distinguished from the fixed dilatation
caused by atropine-like agents instilled by earlier observers
• Horner’s syndrome may be seen in patients with lesions in
the hypothalamus or brain stem, but can also be seen in
diseases affecting the wall of the carotid artery
• Small pupils that react briskly to light suggest metabolic
causes of coma (e.g. hepatic or renal failure), whereas drug
intoxication tends not to affect pupillary light responses
• anaesthesia results in unreactive and slightly dilated pupils;
opiates cause small pupils
Table 2
Pupillary changes
MidbrainMid-position, fixed
TectalLarge, fixed
IIIrd nerveFixed, dilated, ptosed
PontinePinpoint
DiencephalicSmall, reactive
Figure 3
4 © 2008 Elsevier Ltd. all rights reserved.
Coma
syndrome may be seen in patients with lesions in the hypothala-mus or brain stem, or diseases affecting the wall of the carotid artery. Small pupils that react briskly to light raise the possibility of metabolic causes of coma (e.g. hepatic or renal failure). Drug intoxication tends not to affect pupillary light responses. Anaes-thesia results in unreactive and slightly dilated pupils; opiates cause small pupils.
Corneal reflex is usually retained until coma is very deep. When absent in a patient who otherwise appears to be in light coma, the cause may be drug intoxication. Loss of corneal reflex in the absence of drug overdose is a poor prognostic indicator, provided that the patient is not wearing contact lenses.
Spontaneous eye movements: note the resting position of the eyes and any spontaneous eye movements. Conjugate deviation of the eyes suggests a focal hemispheric or brain stem lesion; depression of the eyes may be seen following damage to the mid-brain at the level of the tectum and occasionally in metabolic coma. Skew deviation of the eyes suggests a lesion at the pon-tomedullary junction, and dysconjugate eyes suggest damage to the oculomotor or abducens nerve in the brain stem or pathways. However, a minor degree of divergence is normal in unconscious patients.
Patients in light coma often exhibit roving eye movements simi-lar to those seen in sleep; these may be conjugate or dysconjugate and imply an active brain stem. They cannot be mimicked, and their presence excludes psychogenic unresponsiveness, in which eye movements, if visualized through blepharospasm, are more likely to be jerky. Repetitive, conjugate, horizontal ocular devia-tion (‘ping-pong gaze’) is an indicator of a lesion in the brain stem. Retractory nystagmus, in which the eyes jerk backwards in the orbits, usually indicates a mid-brain lesion. Intermittent down-wards jerking of the eyes (ocular bobbing) is seen in patients with lesions in the low pons. Spontaneous nystagmus is seldom seen in coma because the quick phase of nystagmus depends on an inter-action between the oculovestibular system and the cerebral cortex and disappears when cortical influences are reduced.
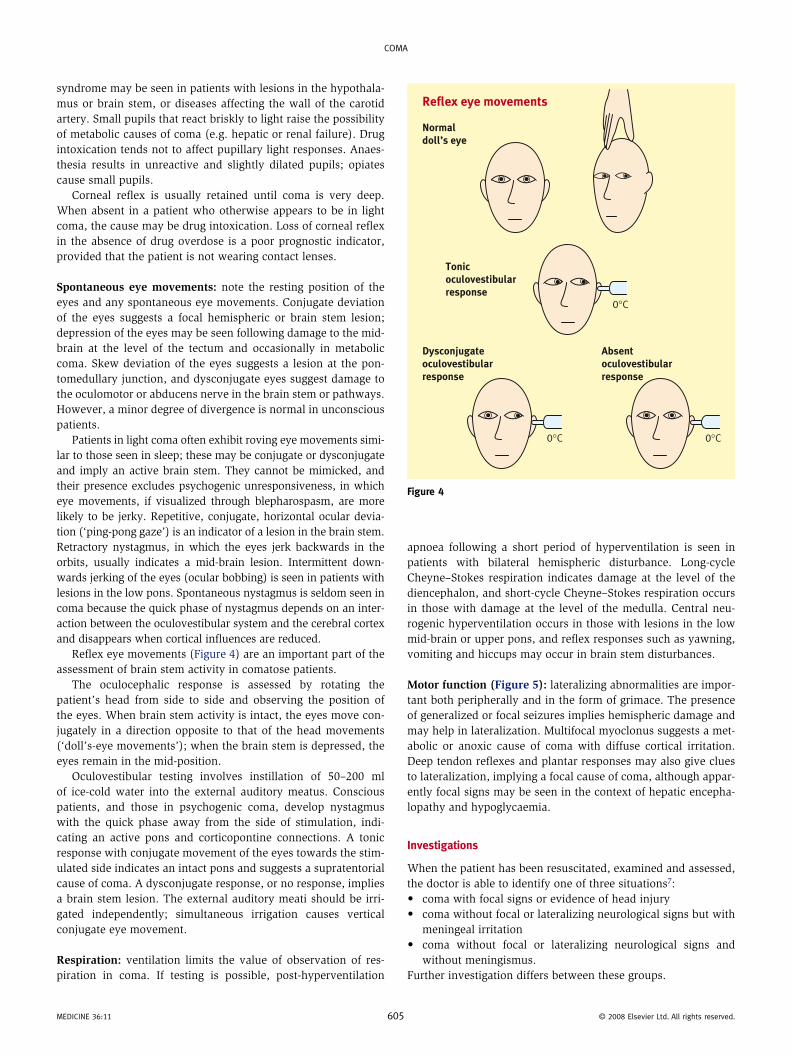
Reflex eye movements (Figure 4) are an important part of the assessment of brain stem activity in comatose patients.
The oculocephalic response is assessed by rotating the patient’s head from side to side and observing the position of the eyes. When brain stem activity is intact, the eyes move con-jugately in a direction opposite to that of the head movements (‘doll’s-eye movements’); when the brain stem is depressed, the eyes remain in the mid-position.
Oculovestibular testing involves instillation of 50–200 ml of ice-cold water into the external auditory meatus. Conscious patients, and those in psychogenic coma, develop nystagmus with the quick phase away from the side of stimulation, indi-cating an active pons and corticopontine connections. A tonic response with conjugate movement of the eyes towards the stim-ulated side indicates an intact pons and suggests a supratentorial cause of coma. A dysconjugate response, or no response, implies a brain stem lesion. The external auditory meati should be irri-gated independently; simultaneous irrigation causes vertical conjugate eye movement.
Respiration: ventilation limits the value of observation of res-piration in coma. If testing is possible, post-hyperventilation
mEDICINE 36:11 60
apnoea following a short period of hyperventilation is seen in patients with bilateral hemispheric disturbance. Long-cycle Cheyne–Stokes respiration indicates damage at the level of the diencephalon, and short-cycle Cheyne–Stokes respiration occurs in those with damage at the level of the medulla. Central neu-rogenic hyperventilation occurs in those with lesions in the low mid-brain or upper pons, and reflex responses such as yawning, vomiting and hiccups may occur in brain stem disturbances.
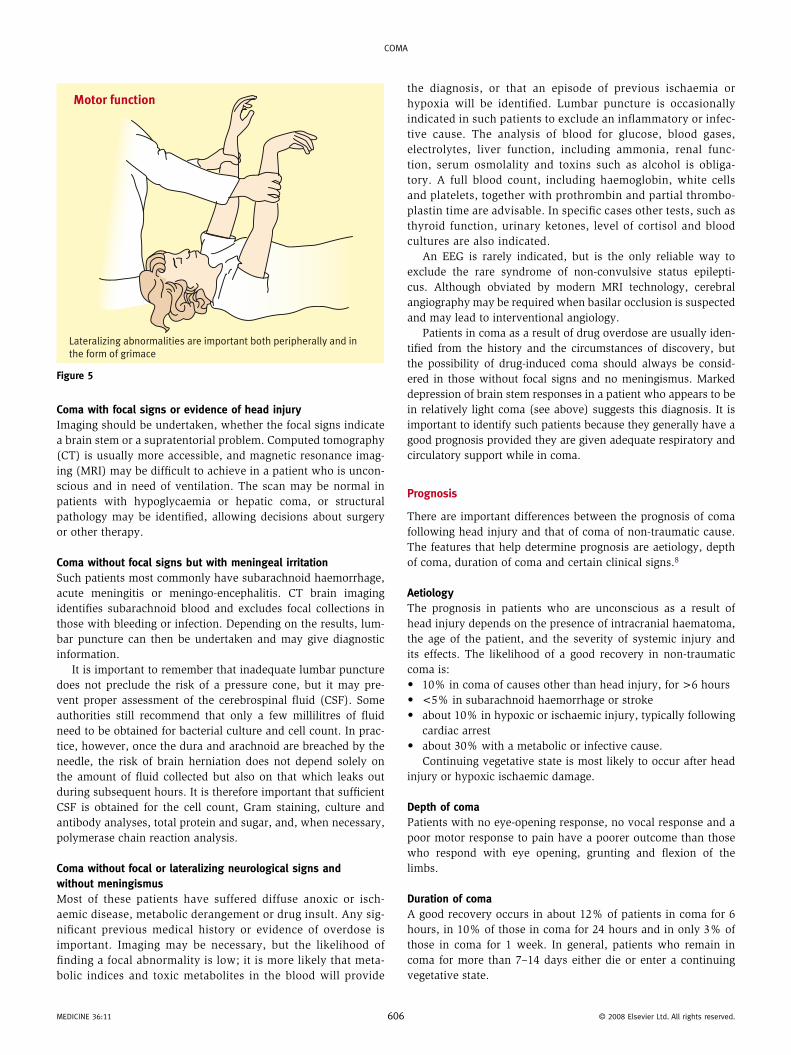
Motor function (Figure 5): lateralizing abnormalities are impor-tant both peripherally and in the form of grimace. The presence of generalized or focal seizures implies hemispheric damage and may help in lateralization. Multifocal myoclonus suggests a met-abolic or anoxic cause of coma with diffuse cortical irritation. Deep tendon reflexes and plantar responses may also give clues to lateralization, implying a focal cause of coma, although appar-ently focal signs may be seen in the context of hepatic encepha-lopathy and hypoglycaemia.
Investigations
When the patient has been resuscitated, examined and assessed, the doctor is able to identify one of three situations7: • coma with focal signs or evidence of head injury • coma without focal or lateralizing neurological signs but with
meningeal irritation • coma without focal or lateralizing neurological signs and
without meningismus.Further investigation differs between these groups.
Reflex eye movements
Normal doll’s eye
Tonic oculovestibular response
Dysconjugate oculovestibular response
Absent oculovestibular response
0°C
0°C 0°C
Figure 4
5 © 2008 Elsevier Ltd. all rights reserved.
Coma
Coma with focal signs or evidence of head injuryImaging should be undertaken, whether the focal signs indicate a brain stem or a supratentorial problem. Computed tomography (CT) is usually more accessible, and magnetic resonance imag-ing (MRI) may be difficult to achieve in a patient who is uncon-scious and in need of ventilation. The scan may be normal in patients with hypoglycaemia or hepatic coma, or structural pathology may be identified, allowing decisions about surgery or other therapy.
Coma without focal signs but with meningeal irritationSuch patients most commonly have subarachnoid haemorrhage, acute meningitis or meningo-encephalitis. CT brain imaging identifies subarachnoid blood and excludes focal collections in those with bleeding or infection. Depending on the results, lum-bar puncture can then be undertaken and may give diagnostic information.
It is important to remember that inadequate lumbar puncture does not preclude the risk of a pressure cone, but it may pre-vent proper assessment of the cerebrospinal fluid (CSF). Some authorities still recommend that only a few millilitres of fluid need to be obtained for bacterial culture and cell count. In prac-tice, however, once the dura and arachnoid are breached by the needle, the risk of brain herniation does not depend solely on the amount of fluid collected but also on that which leaks out during subsequent hours. It is therefore important that sufficient CSF is obtained for the cell count, Gram staining, culture and antibody analyses, total protein and sugar, and, when necessary, polymerase chain reaction analysis.
Coma without focal or lateralizing neurological signs and without meningismusMost of these patients have suffered diffuse anoxic or isch-aemic disease, metabolic derangement or drug insult. Any sig-nificant previous medical history or evidence of overdose is important. Imaging may be necessary, but the likelihood of finding a focal abnormality is low; it is more likely that meta-bolic indices and toxic metabolites in the blood will provide
Motor function
Lateralizing abnormalities are important both peripherally and in the form of grimace
Figure 5
mEDICINE 36:11 60
the diagnosis, or that an episode of previous ischaemia or hypoxia will be identified. Lumbar puncture is occasionally indicated in such patients to exclude an inflammatory or infec-tive cause. The analysis of blood for glucose, blood gases, electrolytes, liver function, including ammonia, renal func-tion, serum osmolality and toxins such as alcohol is obliga-tory. A full blood count, including haemoglobin, white cells and platelets, together with prothrombin and partial thrombo-plastin time are advisable. In specific cases other tests, such as thyroid function, urinary ketones, level of cortisol and blood cultures are also indicated.
An EEG is rarely indicated, but is the only reliable way to exclude the rare syndrome of non-convulsive status epilepti-cus. Although obviated by modern MRI technology, cerebral angiography may be required when basilar occlusion is suspected and may lead to interventional angiology.
Patients in coma as a result of drug overdose are usually iden-tified from the history and the circumstances of discovery, but the possibility of drug-induced coma should always be consid-ered in those without focal signs and no meningismus. Marked depression of brain stem responses in a patient who appears to be in relatively light coma (see above) suggests this diagnosis. It is important to identify such patients because they generally have a good prognosis provided they are given adequate respiratory and circulatory support while in coma.
Prognosis
There are important differences between the prognosis of coma following head injury and that of coma of non-traumatic cause. The features that help determine prognosis are aetiology, depth of coma, duration of coma and certain clinical signs.8
AetiologyThe prognosis in patients who are unconscious as a result of head injury depends on the presence of intracranial haematoma, the age of the patient, and the severity of systemic injury and its effects. The likelihood of a good recovery in non-traumatic coma is: • 10% in coma of causes other than head injury, for >6 hours • <5% in subarachnoid haemorrhage or stroke • about 10% in hypoxic or ischaemic injury, typically following
cardiac arrest • about 30% with a metabolic or infective cause.
Continuing vegetative state is most likely to occur after head injury or hypoxic ischaemic damage.
Depth of comaPatients with no eye-opening response, no vocal response and a poor motor response to pain have a poorer outcome than those who respond with eye opening, grunting and flexion of the limbs.
Duration of comaA good recovery occurs in about 12% of patients in coma for 6 hours, in 10% of those in coma for 24 hours and in only 3% of those in coma for 1 week. In general, patients who remain in coma for more than 7–14 days either die or enter a continuing vegetative state.
6 © 2008 Elsevier Ltd. all rights reserved.

Coma
Clinical signsBrain stem reflexes are the most important clinical signs in defin-ing the prognosis; absence of corneal or pupillary reflexes or ocu-lovestibular responses at 24 hours, in the absence of sedative drugs, is almost incompatible with recovery to independence, whatever the cause of the coma. Development of nystagmus on oculovestibular testing or the vocalization of any recogniz-able word within 48 hours indicates a 50% likelihood of a good recovery.
No single clinical sign is statistically significant as an indicator of prognosis in individual patients, but a combination of clini-cal signs (e.g. absence of oculovestibular responses and corneal responses with extension of the limbs in response to pain) iden-tifies, by 24 hours, a cohort of patients in whom, within 95% confidence limits, the likelihood of making any useful recovery to sentience is less than 3%. Conversely, in patients who exhibit intact pupillary and corneal responses and movements of local-ization by 24 hours, the likelihood of achieving independence is 40%.9
Although clinical signs are the mainstay of assessment and monitoring of the patient in coma there is increasing evidence that biochemical values and neurophysiological tests may have a role to play.10 Somatosensory evoked potential recording nor-mally reveals an N-20 wave (N20 SSEP) which, if bilaterally absent, predicates a poor outcome. Biochemically the measure-ment of neurone-specific enolase (NSE) in peripheral blood at levels greater than 33 μg/litre is also predictive of a bad outcome. It is suggested that the combination of these two parameters pro-vides a higher positive likelihood ratio and a lower false positive rate than the commonly used clinical signs of absence of pupil-lary and corneal responses in predicting a poor outcome.
There are presently still reservations in accepting the signifi-cance and value of these parameters but there is logic in continu-ing to search for biological parameters and to attempt to justify those already identified in large studies of prognosis. It is evi-dent that a reproducible and validated biological marker would improve decision making in the early management of the patient in coma and might avoid the prolongation of an insentient life.
Continuing care of comatose patients
Once the cause of coma has been identified, therapy adminis-tered and the reversibility of the lesion defined, long-term care should be considered. When the prognosis is hopeless, the patient should probably not be exposed to the rigours of intensive care medicine, but should continue to receive basic care in a routine hospital ward. Patients with a potential for recovery should be cared for in an intensive care unit, where respiration, skin, cir-culation, and bladder and bowel function should be protected, any seizures controlled and conscious level monitored. There is no evidence that specific stimulation is likely to affect the rate of recovery. Correction of metabolic or surgical abnormalities is obligatory, but techniques such as hyperventilation and empiri-cal corticosteroid therapy are generally of no value and do not improve the prognosis.
Prolonged survival of patients in coma usually indicates devel-opment of a vegetative state. This must be distinguished from states of severe disability or ‘minimal responsiveness’, in which patients are aware but so paralysed that they cannot respond
mEDICINE 36:11 60
easily. Differentiation of these conditions requires sufficient time for observation and assessment of responses, and involves nurs-ing staff, carers and relatives. When patients are shown to have some level of cognition or sentience, it is obligatory that their care is maintained, unless an advance directive was formally made by the patient before the onset of coma.
There is continuing debate about the potential for recovery of patients in a vegetative state. In patients who have suffered non-traumatic injuries such as anoxia or ischaemia, the progno-sis is poor after the first few weeks and almost negligible after 6 months. There are reports of improvement after many months in patients in a vegetative state following head trauma, but these anecdotal cases are difficult to validate – it is possible that the patients were not truly vegetative but in a state of profound dis-ability, retaining cognition.
The use of sophisticated imaging with positron emission tomography and functional MRI may ultimately provide a method whereby patients in a minimally conscious state can be clearly defined from those in a true vegetative state. The techniques now available are still being validated by research and at present, and for some time to come, the true assessment of sentience and of consciousness will remain clinical.11
Many patients in a persisting vegetative state have received artificial ventilation at some time during their initial coma or resuscitation, but are not dependent on it. These patients depend on their carers only for a supply of liquid and nutrients, and for prevention of intercurrent infection. Management of such patients depends on circumstances, other aspects of the diagno-sis and a consideration of the prognosis. Recent advice from the UK Royal Colleges of Physicians on the diagnosis and manage-ment of permanent vegetative state, and the involvement of the courts in decisions to withdraw artificial hydration and nutrition, should be observed.
Brain stem death
In 1976 and 1979, the UK Conference of Medical Royal Colleges and their Faculties produced memoranda on which the identifi-cation of brain stem death is based. A recent report from a work-ing party of the Conference has suggested that death may be defined as ‘the irreversible loss of the capacity for consciousness, combined with the irreversible loss of the capacity to breathe’. Thus, the more correct term ‘brain stem death’ should replace the previous term ‘brain death’. There are three prerequisites for brain stem death: • There should be no doubt that the patient’s condition is caused by irremediable brain damage of known aetiology. • The patient should be deeply comatose, and the effects of de-pressant drugs, primary hypothermia, and potentially reversible metabolic and endocrine disturbances as the cause of continua-tion of coma must be excluded. It is recognized that metabolic and endocrine disturbances (e.g. hyponatraemia and diabetes insipidus) are a likely accompaniment of brain stem death, but these are an effect rather than the cause of that condition and do not preclude the diagnosis. • The patient is being maintained on a ventilator because spon-taneous respiration has become inadequate or has ceased.When these prerequisites are fulfilled, the patient should be examined to ensure that all brain stem reflexes are absent. It
7 © 2008 Elsevier Ltd. all rights reserved.
Coma
is customary to repeat these tests to ensure that there is no observer error; it is recommended that two assessors undertake the examination individually. • The pupils are fixed in diameter and do not respond to sharp changes in the intensity of instant light. • There is no corneal reflex. • The vestibulo-ocular reflexes are absent. • No motor responses within the cranial nerve distribution can be elicited by adequate stimulation of any somatic area. • There is no gag reflex or reflex response to bronchial stimulation by a suction catheter passed down the trachea. • No respiratory movements occur when the patient is dis-connected from the mechanical ventilator for sufficiently long to ensure that arterial carbon dioxide tension rises above the threshold for stimulation of respiration.
When these criteria are fulfilled, additional information from imaging or EEG is unnecessary and unhelpful. Brain stem death can be diagnosed, family and carers informed, and ventilatory support disconnected. ◆
REFERENCES
1 Bates D. Defining prognosis in medical coma. J Neurol Neurosurg
Psychiatry 1991; 54: 569–71.
2 moruzzi G, magoun HW. Brain stem reticular formation and
activation of the EEG. Electroencephalogr Clinl Neurophysiol 1949;
1: 455–73.
3 mRC Brain Injuries Committee. a glossary of psychological terms
commonly used in cases of head injury. mRC War memorandum 4.
London: HmSo, 1941.
mEDICINE 36:11 60
4 metenberg o, mumenthaler m, Karbowski K. Quadriparesis and
nuclear oculomotor palsy with total bilateral ptosis mimicking
coma. a mesencephalic ‘locked-in syndrome’. Arch Neurol 1997; 36:
708–10.
5 Bates D. The management of medical coma. J Neurol Neurosurg
Psychiatry 1993; 56: 589–98.
6 Teasdale G, Jennett WB. assessment of coma and impaired
consciousness: a practical scale. Lancet 1974; ii: 81–84.
7 Fisher Cm. The neurological examination of the comatose patient.
Acta Neurol Scand 1969; 43: 1–56.
8 Plum F, Posner JB, Saper CB, Nicholas DS. Diagnosis of stupor and
coma. oxford: oxford University Press, 2007.
9 Levy DE. Predicting outcome from hypoxic-ischaemic coma. J Am
Med Assoc 1985; 253: 1420–26.
10 Zanbergen EJG. Prediction of poor outcome within the first three
days of post-anoxic coma. Neurology 2006; 66: 62–68.
11 Pickard JD. Functional imaging, electrophysiology and mechanical
intervention. Neuropsychol Rehab 2006; 15: 272–306.
Practice points
• Resuscitation takes precedence over diagnosis
• always remember to measure blood glucose
• History of the onset of coma and the circumstances is very
important
• Brain stem death cannot be diagnosed without a known
diagnosis
8 © 2008 Elsevier Ltd. all rights reserved.