combined spinal epidural anesthesia emelita a. umali, md, fpba
TRANSCRIPT

Combined Spinal Epidural AnesthesiaEMELITA A. UMALI, MD, FPBA

Benefits:•Rapid onset of action (spinal anesthesia action)•Good block and good muscle relaxation (spinal anesthesia)•Spread of anesthesia is optimized, anesthesia can be prolonged (epidural)•Post-operative analgesia can be achieved (via epidural anesthesia)
Indications for the CSE technique
1. Obstetrics * (cesarean section, labor analgesia)
2. Gynecologic surgery
3. Orthopedic surgery
4. Urologic surgery
5. Major vascular surgery
6. Pediatric surgery
7. Ambulatory surgery
Various options for CSE technique1. Double needle (needle- through- needle) -
single interspace*
2. Double catheter ( catheters in epidural and subarachnoid spaces)
3. Double needle- separate interspaces
4. Double needle (needle- beside- needle) - single interspace
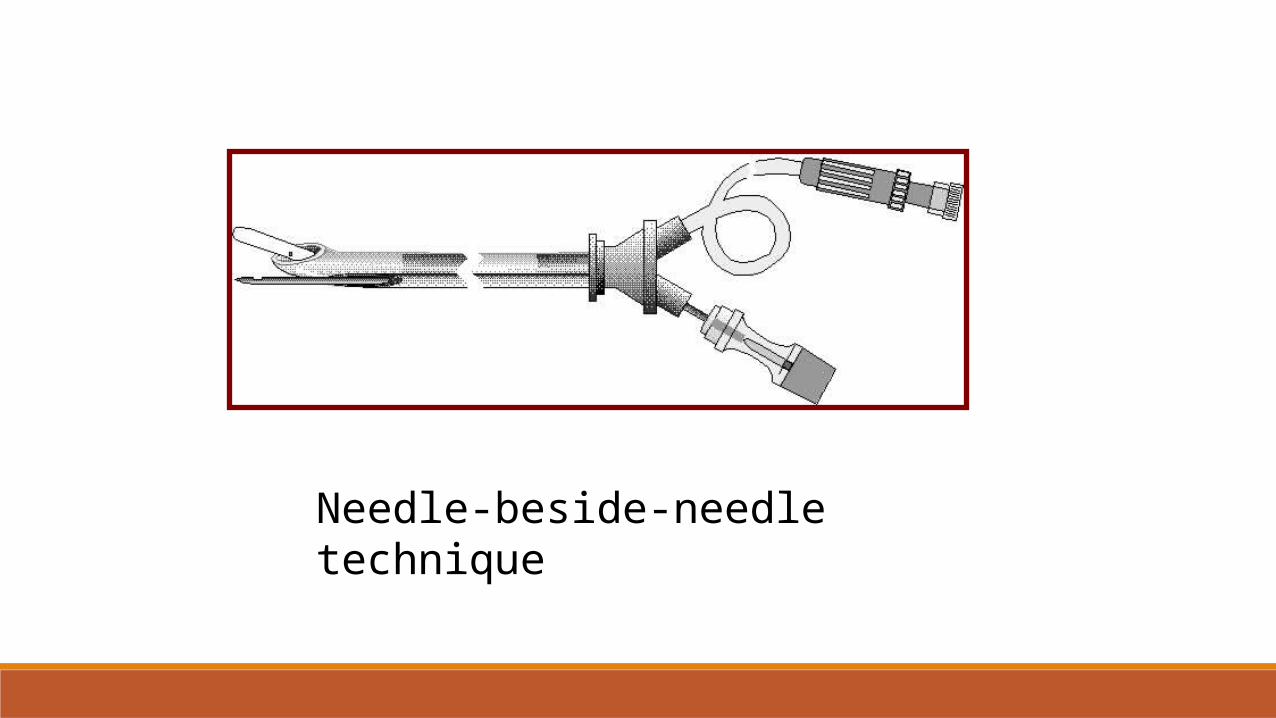
Needle-beside-needle technique

Needle-through-needle technique
“Painting both sides of the fence”

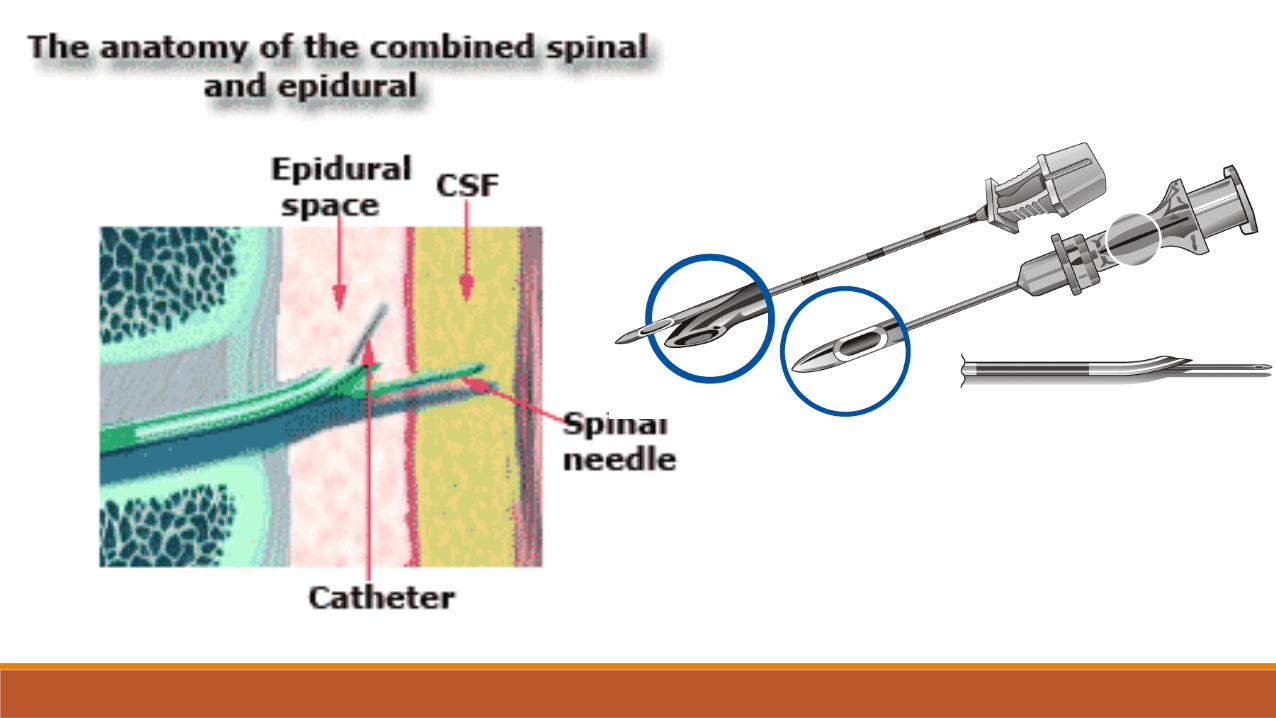
CSE technique (needle –through-needle)
With the patient in a lateral decubitus position or sitting position, an epidural needle is inserted at the desired intervertebral space below L2 .

Epidural space identified in the same manner using the loss of resistance to air technique
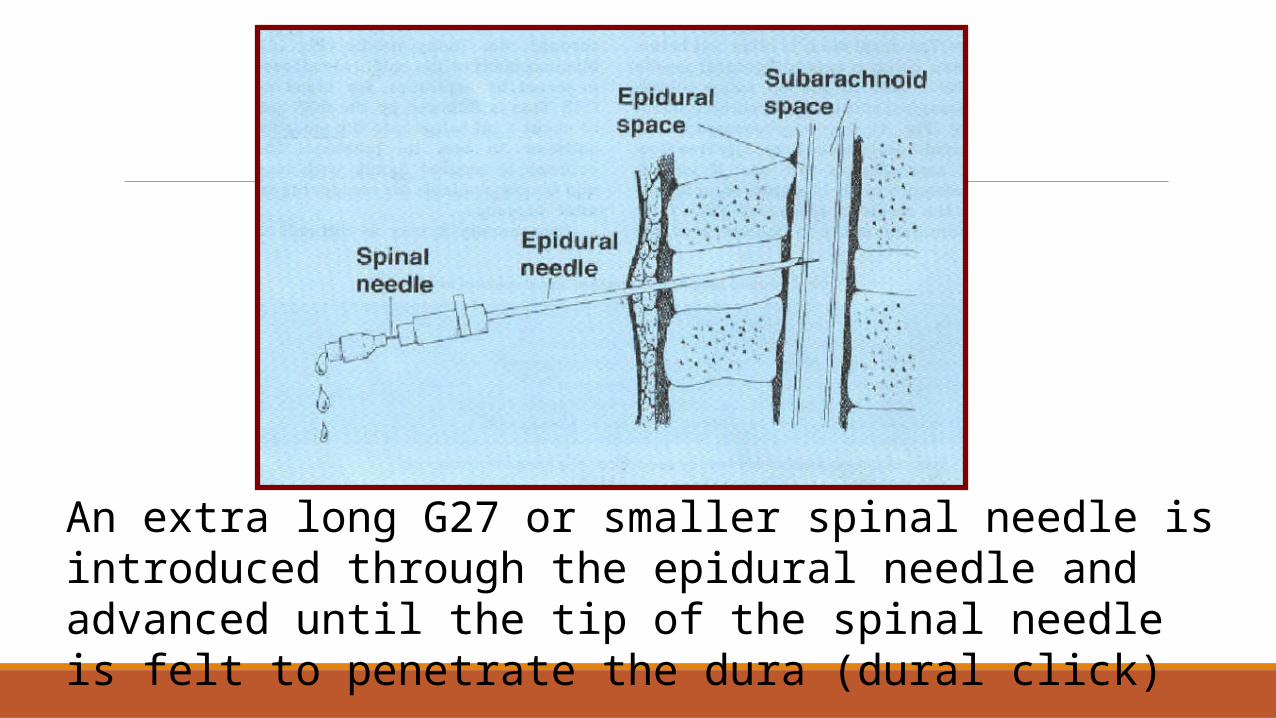
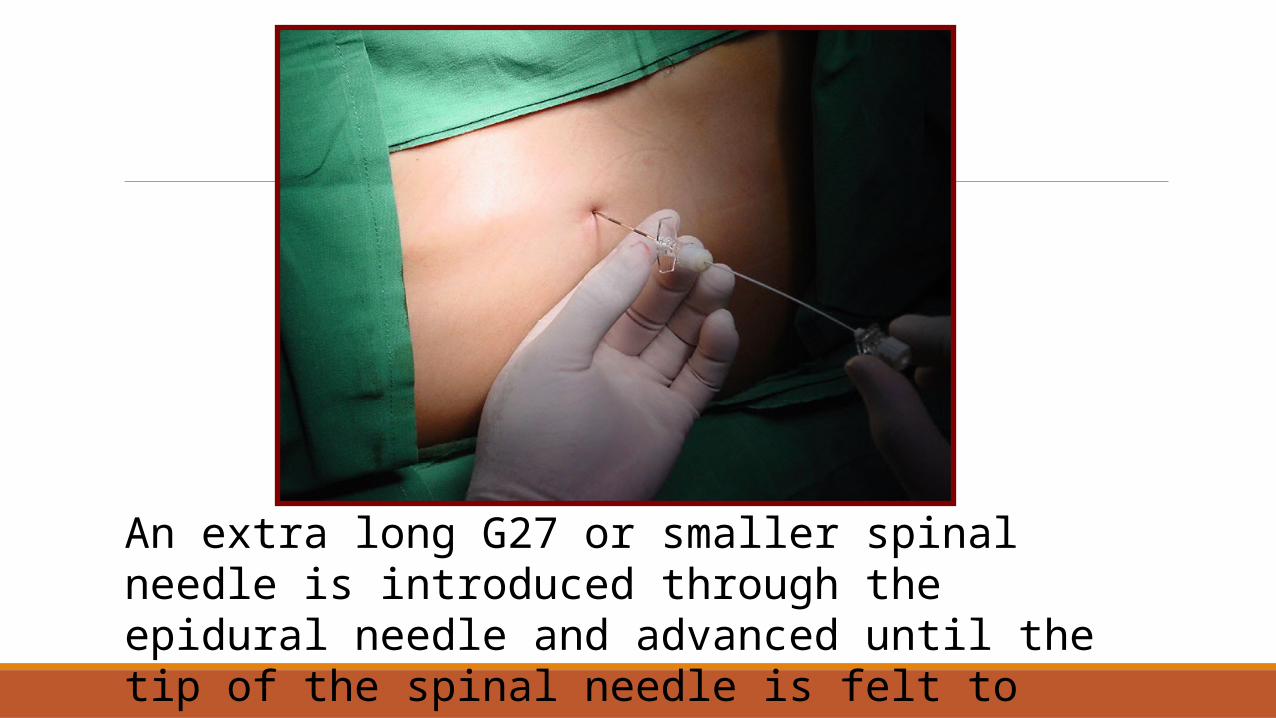
An extra long G27 or smaller spinal needle is introduced through the epidural needle and advanced until the tip of the spinal needle is felt to penetrate the dura (dural click)
An extra long G27 or smaller spinal needle is introduced through the epidural needle and advanced until the tip of the spinal needle is felt to penetrate the dura (dural click)
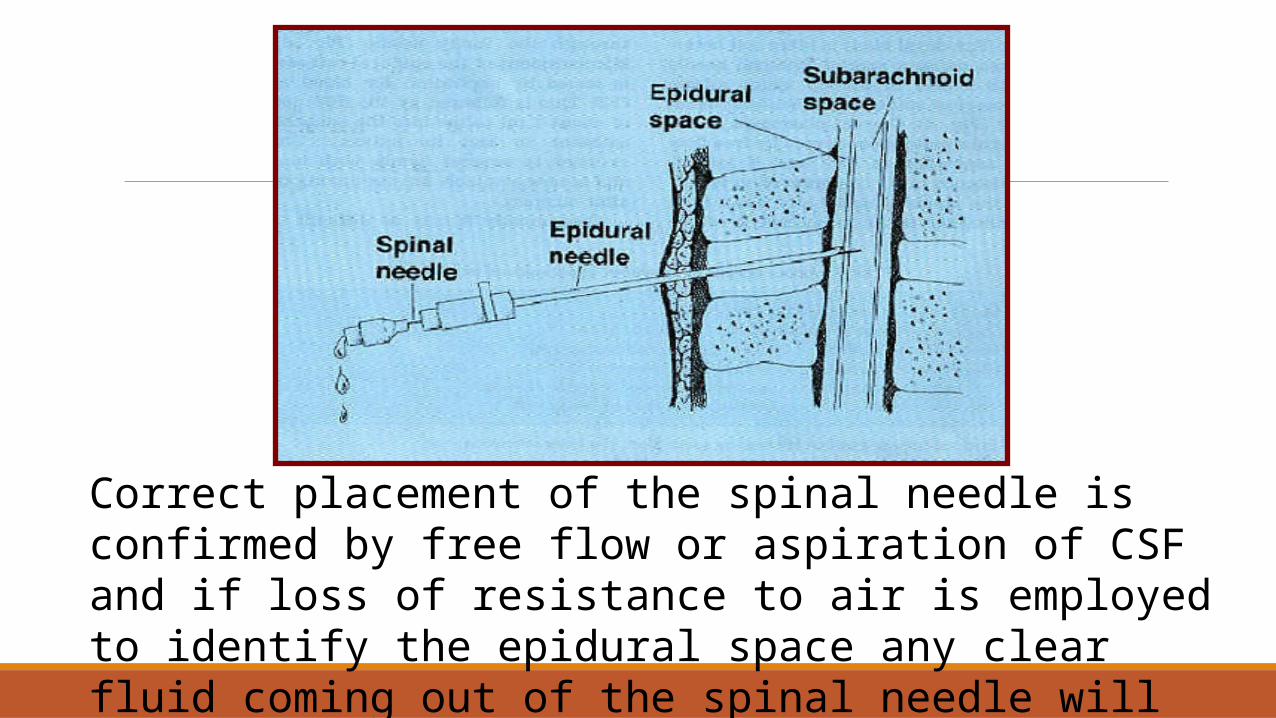
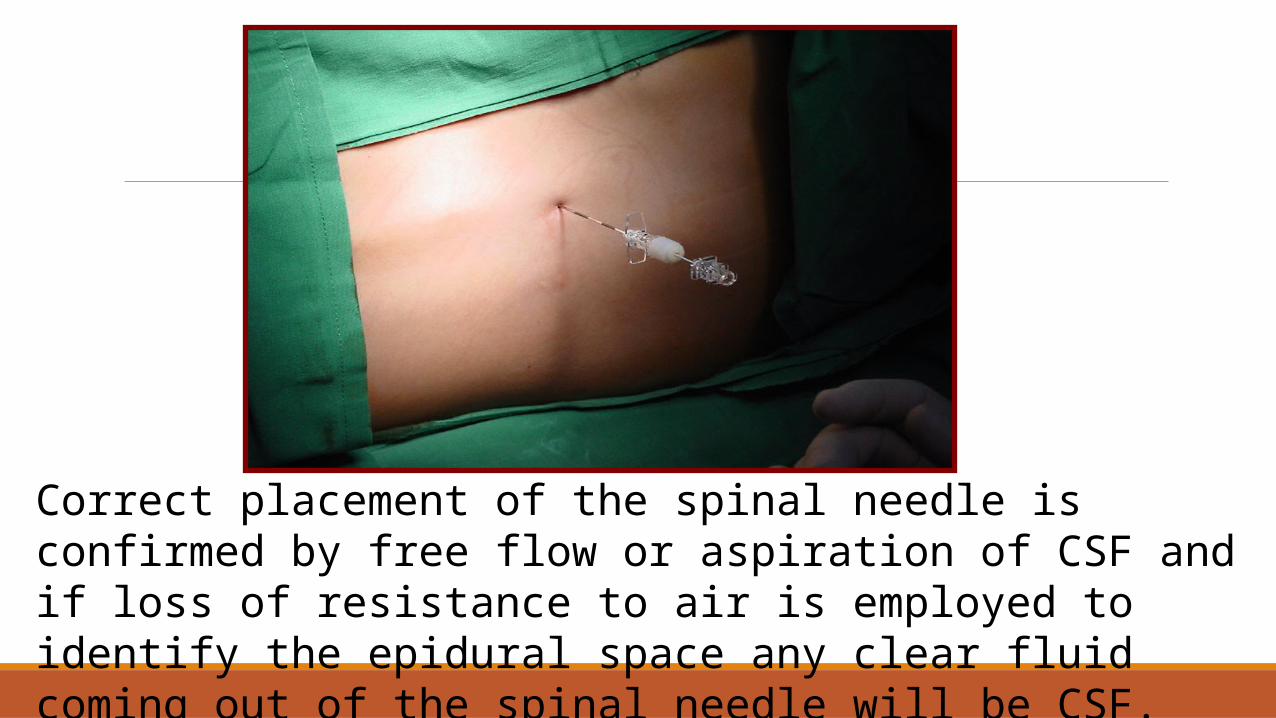
Correct placement of the spinal needle is confirmed by free flow or aspiration of CSF and if loss of resistance to air is employed to identify the epidural space any clear fluid coming out of the spinal needle will be CSF.
Correct placement of the spinal needle is confirmed by free flow or aspiration of CSF and if loss of resistance to air is employed to identify the epidural space any clear fluid coming out of the spinal needle will be CSF.

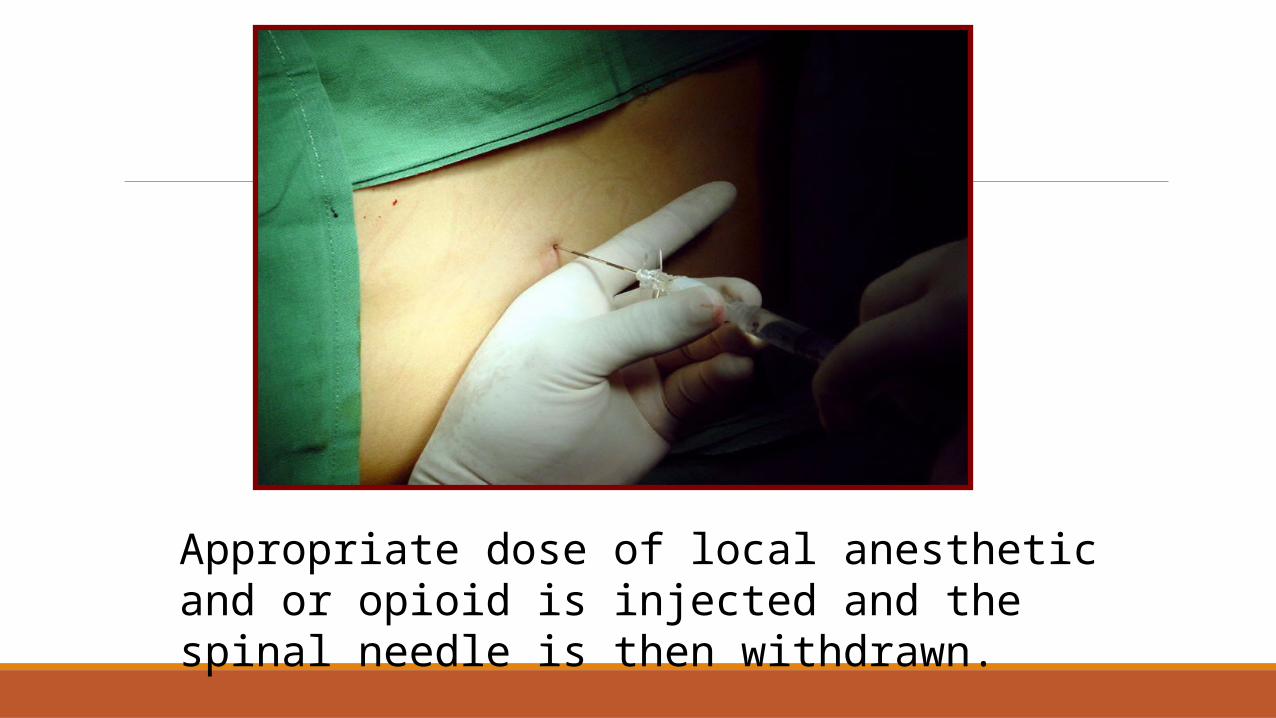
Appropriate dose of local anesthetic and or opioid is injected and the spinal needle is then withdrawn.
Appropriate dose of local anesthetic and or opioid is injected and the spinal needle is then withdrawn.

After withdrawing the spinal needle, a catheter is introduced about 4-5 cm into the epidural space through the tuohy needle. Misplacement of the epidural catheter is tested by aspiration for blood or CSF.

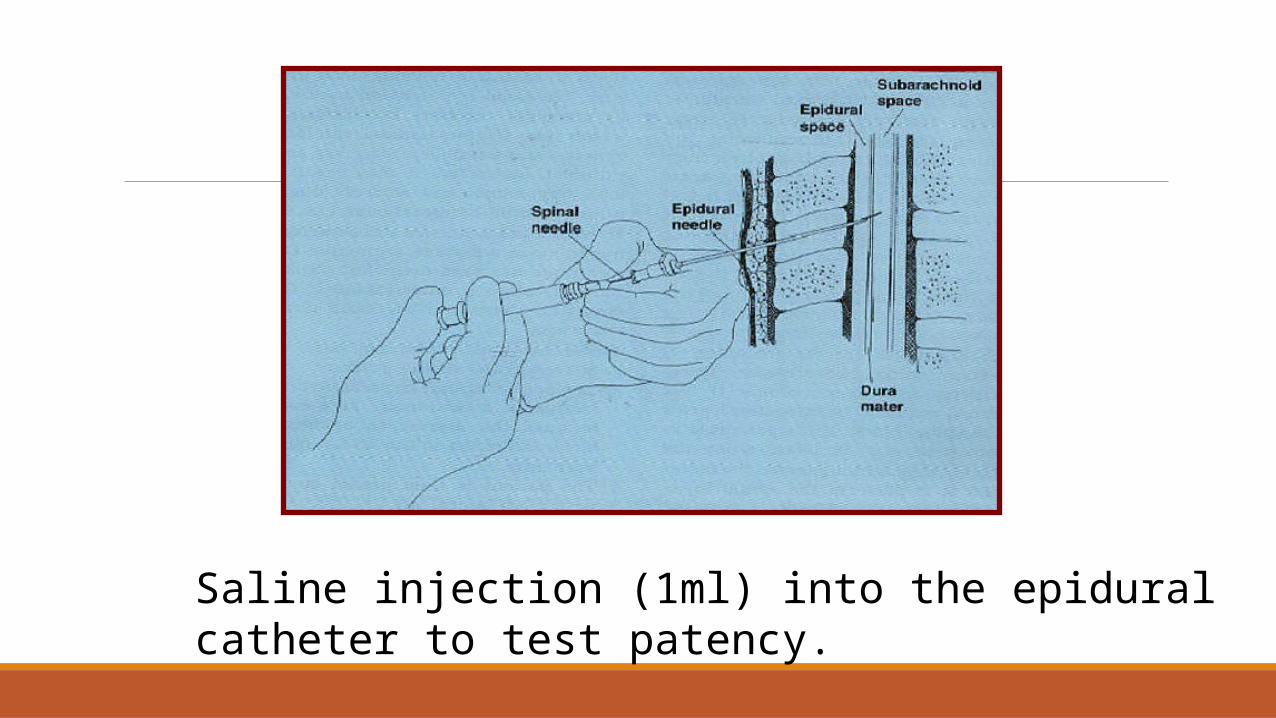
Saline injection (1ml) into the epidural catheter to test patency.


The catheter is secured firmly with tape and is now available for use during labor and delivery.

Things to remember:1. aspiration test
2. incremental loading
Thank you!