common complications in obstetric anesthesia– and how to avoid them. tom archer, md, mba ucsd...
TRANSCRIPT
Common Complications in Obstetric Anesthesia–
and How to Avoid Them.
Tom Archer, MD, MBAUCSD Anesthesia Resident Lecture Series
January 23, 2013
My definition of “common”
• A complication you will see at least once in a career in which you do some OB anesthesia.
• If you do OB anesthesia regularly, you will see most of the following complications many, many times.
Common OB Anesthesia Complications
• Difficulty placing spinal or epidural, causing patient distress.
• “Sketchy-dural” (poor epidural)
• Post-dural puncture headache (PDPH)
• Hypotension after neuraxial block
Common OB Anesthesia Complications
• High spinal or epidural respiratory failure +/- hypotension
• Low spinal or epidural anesthesia failure
• Intraoperative pain (incomplete block)
• Can’t intubate (and can’t ventilate?) under GA.
Common OB Anesthesia Complications
• Fetal bradycardia after CSE or epidural
• Post-delivery lower extremity neuropathy

I am not going to discuss:
• Local anesthetic or contaminant toxicity to nerves (rare in modern practice).
• Direct needle trauma to nerve roots or spinal cord (rare).
• Epidural abscess or hematoma (rare).
• Aspiration
Difficulty placing spinal or epidural, with patient distress.
Difficulty placing spinal or epidural, with patient distress.
• We have all been there, many times. At least I have.
• 20-60 minutes of effort.• Patient is in tears. You are sweating.• You have called for help. They couldn’t do it
either.• Is this inevitable, or is there a way to reduce
the frequency of such events?
Making epidural placement easier for patient and doctor
• “Management of expectations”: “5-10% of the time the epidural does not work properly. We will do our best…” Don’t promise perfection!
• Achieve patient rapport and cooperation.• Demonstrate posture.• Reinforce positioning– patients straighten up
over time when in pain. • IV fentanyl makes a big difference.
Making epidural placement easier for patient and doctor
• If you anticipate difficult placement (e.g. an obese patient) consider IV fentanyl and ultrasound before you start.
• Don’t wait until patient is in tears to give fentanyl and to use ultrasound.
Can ultrasound make neuraxial block easier?
• Many practitioners say it is an unnecessary waste of time. I disagree, at least in selected cases.
• Ultrasound can help identify:– MIDLINE (true location of spinous processes)– DEPTH TO LIGAMENTUM FLAVUM– SPINAL ROTATION, IF PRESENT
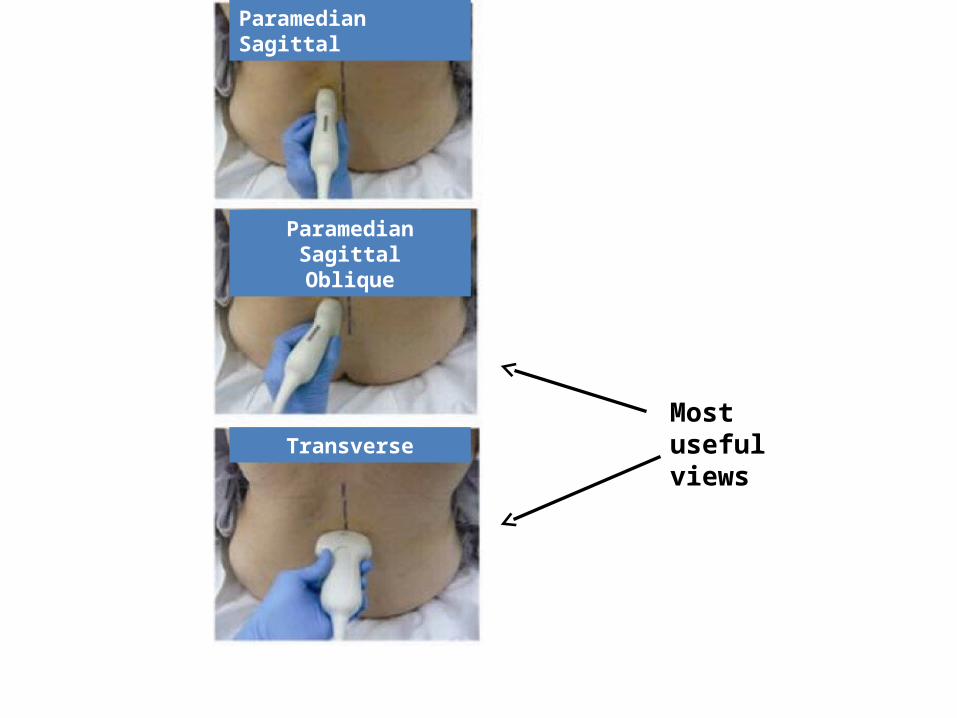
Paramedian Sagittal
Paramedian SagittalOblique
Transverse
Most useful views
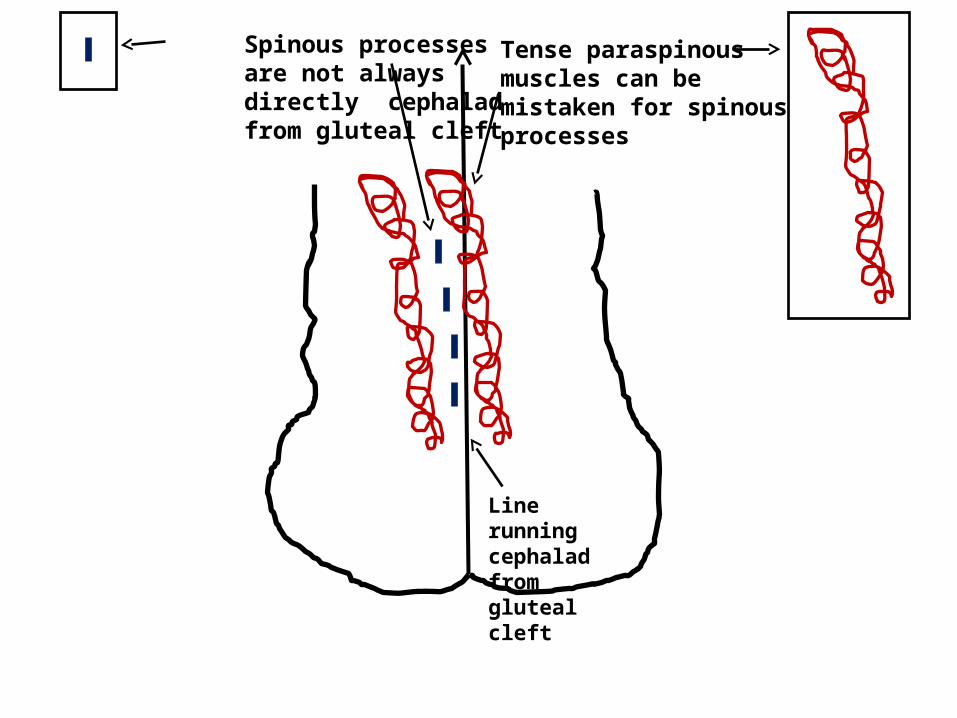
Spinous processes are not always directly cephalad from gluteal cleft
Tense paraspinous muscles can be mistaken for spinous processes
Line running cephalad from gluteal cleft
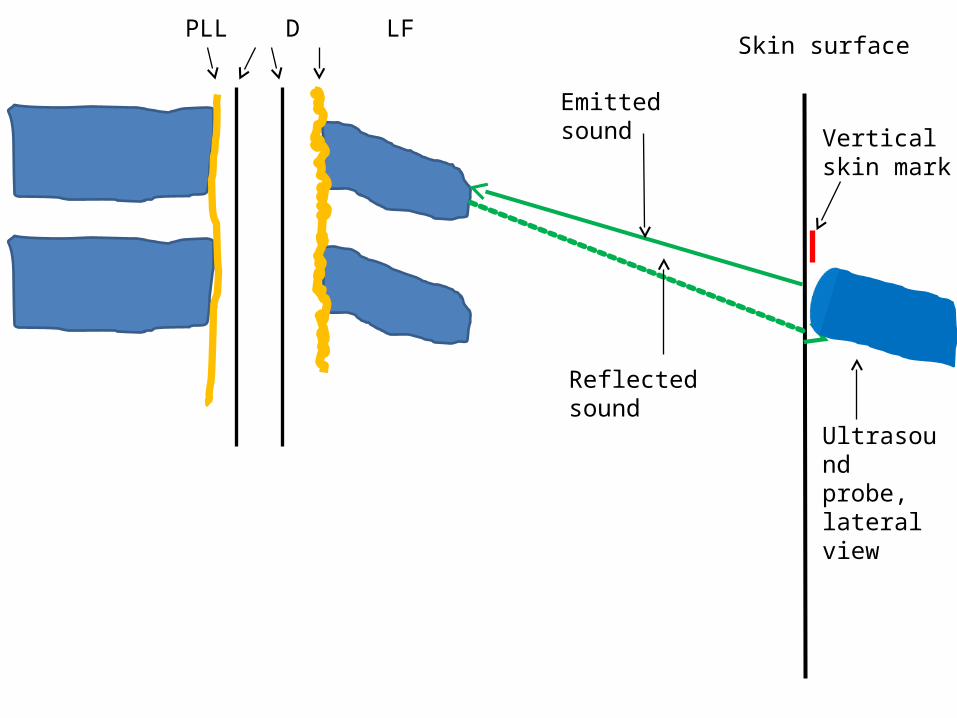
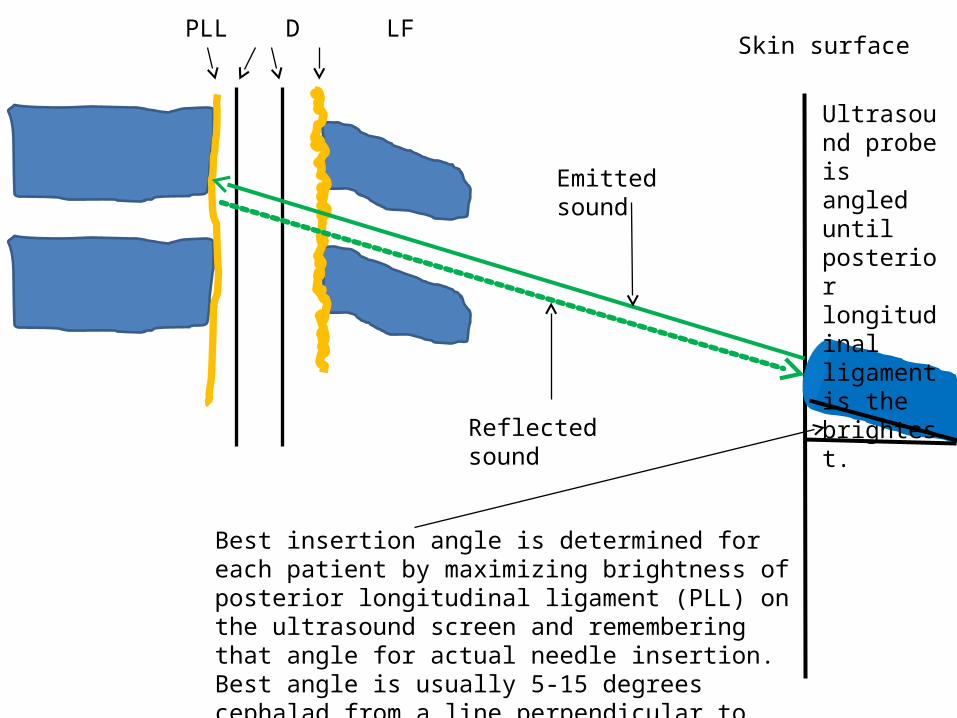
PLL D LFSkin surface
Emitted sound
Reflected sound
Ultrasound probe, lateral view
Vertical skin mark
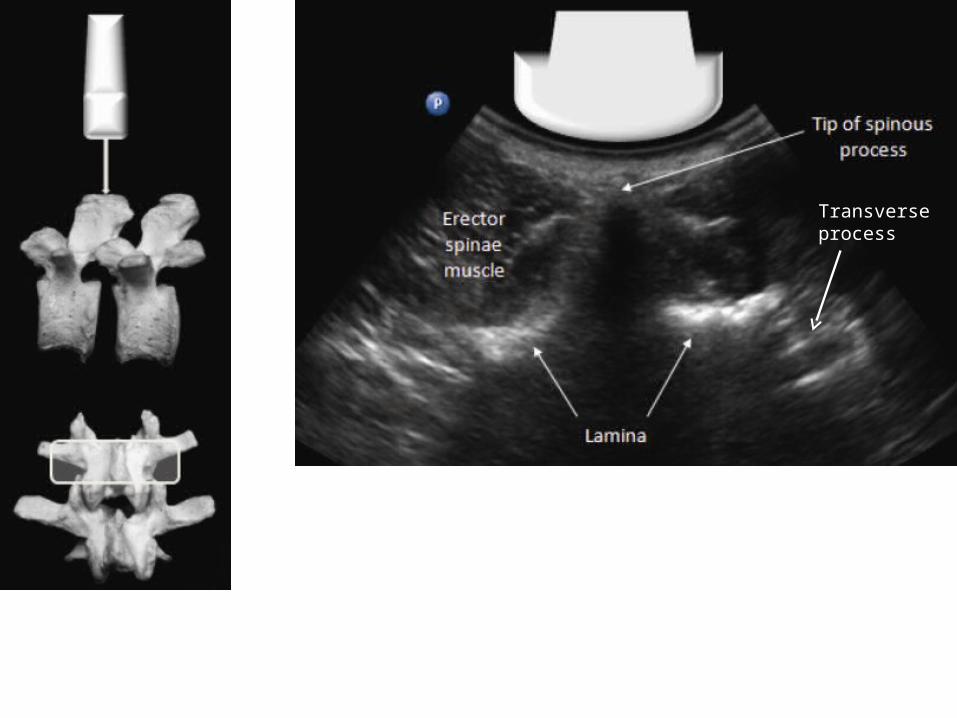
Transverse process
PLL D LFSkin surface
Emitted sound
Reflected sound
Best insertion angle is determined for each patient by maximizing brightness of posterior longitudinal ligament (PLL) on the ultrasound screen and remembering that angle for actual needle insertion. Best angle is usually 5-15 degrees cephalad from a line perpendicular to the skin.
Ultrasound probe is angled until posterior longitudinal ligament is the brightest.
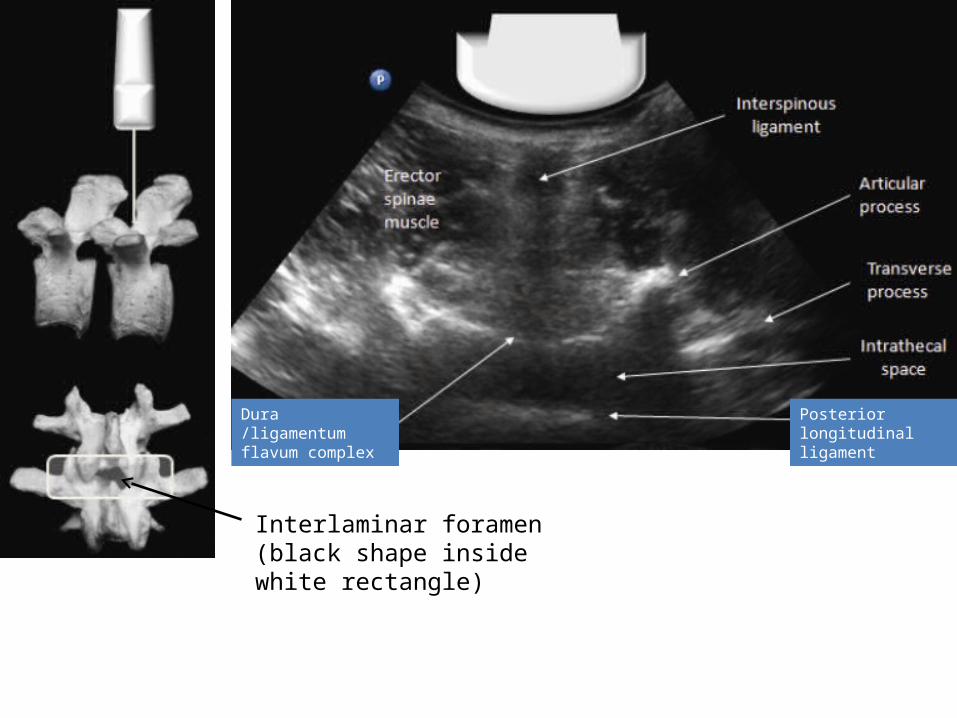
Dura /ligamentum flavum complex
Posterior longitudinal ligament
Interlaminar foramen (black shape inside white rectangle)
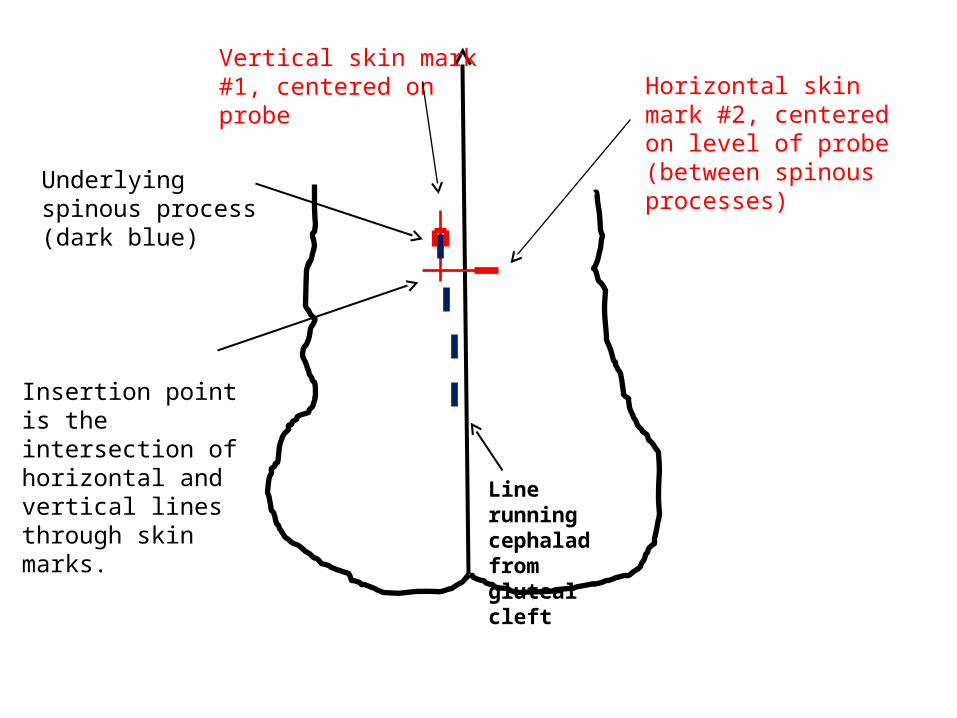
Vertical skin mark #1, centered on probe
Underlying spinous process (dark blue)
Line running cephalad from gluteal cleft
Horizontal skin mark #2, centered on level of probe (between spinous processes)
Insertion point is the intersection of horizontal and vertical lines through skin marks.
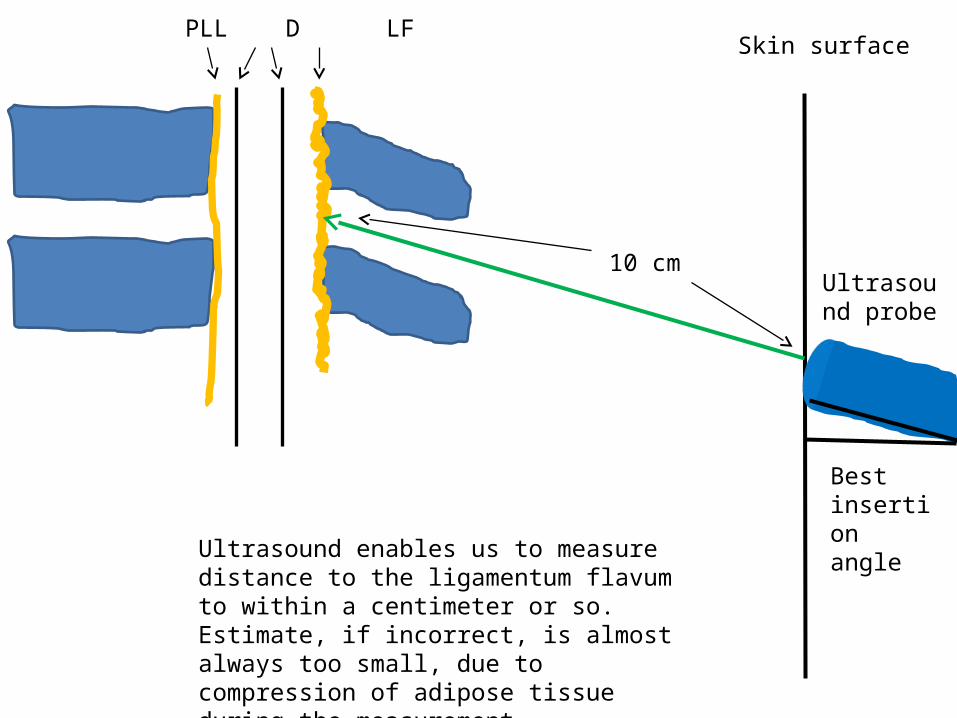
PLL D LFSkin surface
10 cmUltrasound probe
Best insertion angle
Ultrasound enables us to measure distance to the ligamentum flavum to within a centimeter or so. Estimate, if incorrect, is almost always too small, due to compression of adipose tissue during the measurement.
“Sketchy-dural” (poor epidural)
“Sketchy-dural”
• They happen, no matter how good you are.
• “Management of expectations.” Don’t promise the patient a perfect epidural.
• That said, here is my advice to minimize impact of sketchy-durals on our care…
“Sketchy-dural”
• Be honest with yourself. Many sketchy-durals are simply not in the right place.
• Check what is really going on, with ice– systemic fentanyl can mask a non-epidural.
• Have a low threshold for replacement.
“Sketchy-dural”
• A disadvantage of IV fentanyl is that the analgesia it provides can mask a poor epidural.
• Ask the patient how her legs feel. The answer should be “numb” or “tingly”. “Fine” is NOT a good answer– it means there is no block!
• Epidurals requiring more than one MD bolus have a higher failure rate for CS.
“Sketchy-dural”• What exactly is the problem? Talk with and examine
the patient.
• Just doesn’t work at all? replace
• One sided? bolus with less-affected side down. Next step pull back one cm. Next step replace
• “Hot spot” but otherwise OK? Position side with “hot spot” downwards and bolus with stronger local anesthetic + epinephrine + fentanyl.
“Sketchy-dural”
• Think about other causes of “abnormal” pain fetal head pressing on nerves, uterine rupture, placental abruption, “intradural placement.”
• There should be no pain (or much sensation at all) with an epidural injection.
• Discomfort in the back during epidural injections suggests intramuscular or subcutaneous injection.
“Sketchy-dural”
• Consider ultrasound the second time (or the first time!) to confirm:
– MIDLINE (true location of spinous processes)
– DEPTH to ligamentum flavum
– ROTATION of the spinal column
“Sketchy-dural” goes to CS.
• Can you do a spinal on top of a “sketchy-dural”?
• Yes, but do it carefully and understand that high spinal may occur.
• CSE with low intrathecal dose, or titrated epidural are options.
Post dural puncture headache(“Spinal headache”)
Post dural puncture headache(PDPH)
• Third most common cause of lawsuit in OB anesthesia.
• Can be disabling and distressing, particularly for a mother trying to take care of a newborn and a household.
Post dural puncture headache(PDPH)
• Third most common cause of lawsuit in OB anesthesia.
• Can be disabling and distressing, particularly for a mother trying to take care of a newborn and a household.

PDPH
• Midline frontal and/or occipital. Not lateralized!
• May extend into neck (stiff neck)
• Worse with upright posture (usually immediate onset, may be delayed 20 minutes)
• Relief with flat posture (usually immediate).
PDPH
• May be associated with diplopia (abducens palsy) and muffled hearing or tinnitus.
• May be associated with N+V.
But is it really PDPH?
• The key question: Could it be something else?
• If you Rx PDPH and it is something else you incur two problems: unnecessary treatment risk AND missed Dx.
• It could be: lactation HA, migraine, subdural hematoma, brain tumor, AVM, cortical vein thrombosis, dural sinus thrombosis, etc.
Yes, it is PDPH
• Conservative therapy vs. Blood patch?• Conservative therapy: NSAIDs, other oral
analgesics, caffeine, fluids, salty foods.• Epidural blood patch (EBP): 10-30 mL of
patient’s blood injected into epidural space.• EBP complications: back pain, leg paresthesias
(common), epidural abscess or adhesive arachnoiditis (rare).
In favor of EBP
• Severe disability, >24 hours of Sx.
• Patient confined to bed– unable to function
• Associated signs + Sx of decreased ICP (abducens palsy, hearing changes, N+V)
In favor of conservative therapy
• Uncertain Dx.
• Patient uncomfortable but able to function.
• If they are sitting up in bed, or walking, when I enter the room, I am hesitant to do a blood patch.
PDPH etiology• Traditional theory: loss of CSF leads to brain “settling
down” in skull, with resultant traction on dura and nerves
• Vasodilation theory: loss of CSF leads to translocation of CSF to lumbar area with upright posture. Volume in skull must remain constant, hence vasodilation + HA.
• Therapeutic efficacy of caffeine and vasoconstrictors supports vasodilation theory
Hypotension after labor epidural
Hypotension after labor epidural
• Occurs VERY commonly. 30-40% of the time?
• Consider low dose prophylactic phenylephrine or ephedrine after block placement.
Hypotension after labor epidural
• 95% of fetal distress after epidural is due to hypotension.
• The other 5% may be “uterine hypertonus” due to rapid pain relief (discussed later).
• Both things might be happening.
• When there is fetal distress palpate uterus!
Hypotension after labor epidural
• Routine therapy for hypotension (in absence of uterine hyperstimulation) is:
Position change (Left or right side down).Fluid bolusVasopressorsOxygen, if there is fetal bradycardia.
Hypotension with labor epidural
• Treat hypotension early, treat often.
• Prevention with low-dose vasopressor has very little downside.
• Is there a role for non-invasive cardiac output measurement in labor to detect occult IVC obstruction?
Physiology of post-block hypotension

http://health.usf.edu/nocms/medicine/anatomylab/modules/pelvic_autonomic_module/pelvic_page02.html
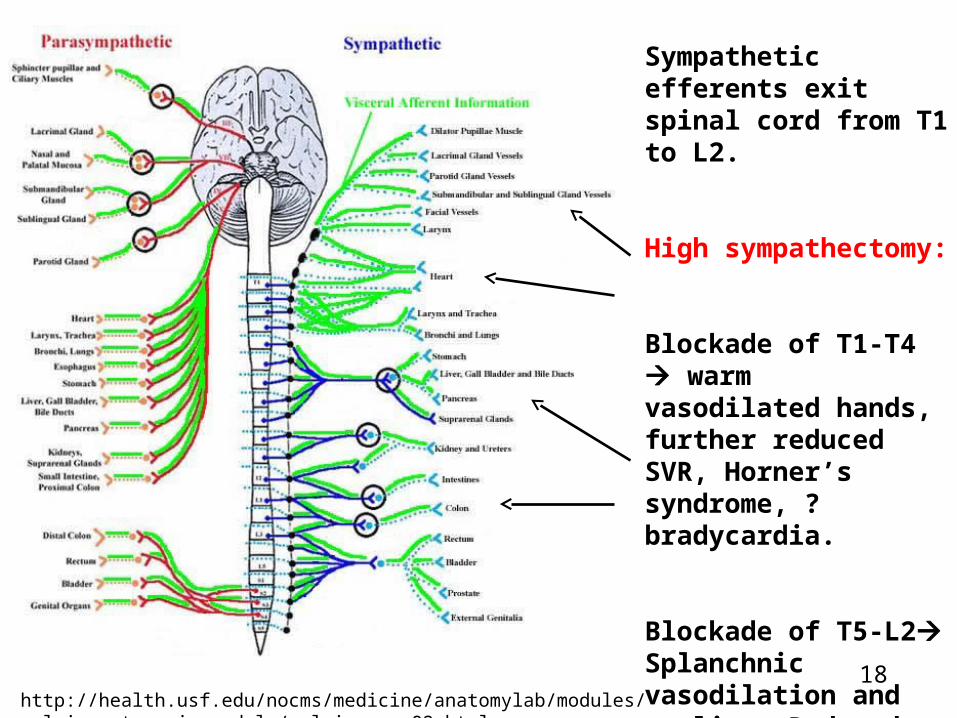
Sympathetic efferents exit spinal cord from T1 to L2.
Low sympathectomy:
Blockade of T5-L2Splanchnic vasodilation and pooling. Reduced venous return (CO), especially with IVC obstruction. Reduced SVR.17
http://health.usf.edu/nocms/medicine/anatomylab/modules/pelvic_autonomic_module/pelvic_page02.html
Sympathetic efferents exit spinal cord from T1 to L2.
High sympathectomy:
Blockade of T1-T4 warm vasodilated hands, further reduced SVR, Horner’s syndrome, ? bradycardia.
Blockade of T5-L2Splanchnic vasodilation and pooling. Reduced venous return (CO), especially with IVC obstruction. Reduced SVR.18
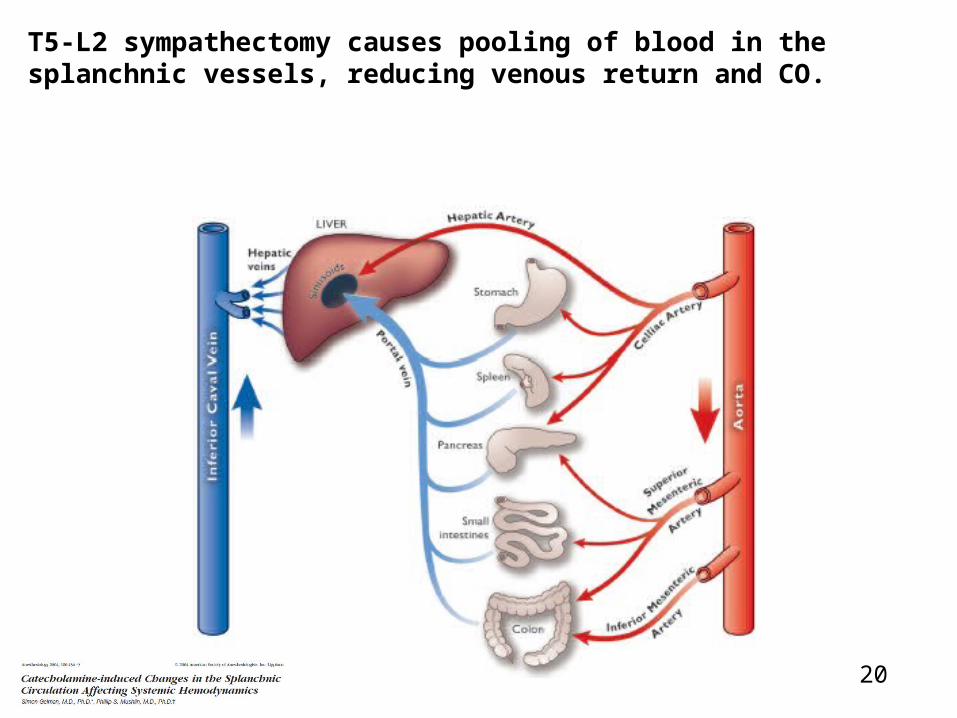
T5-L2 sympathectomy causes pooling of blood in the splanchnic vessels, reducing venous return and CO.
20
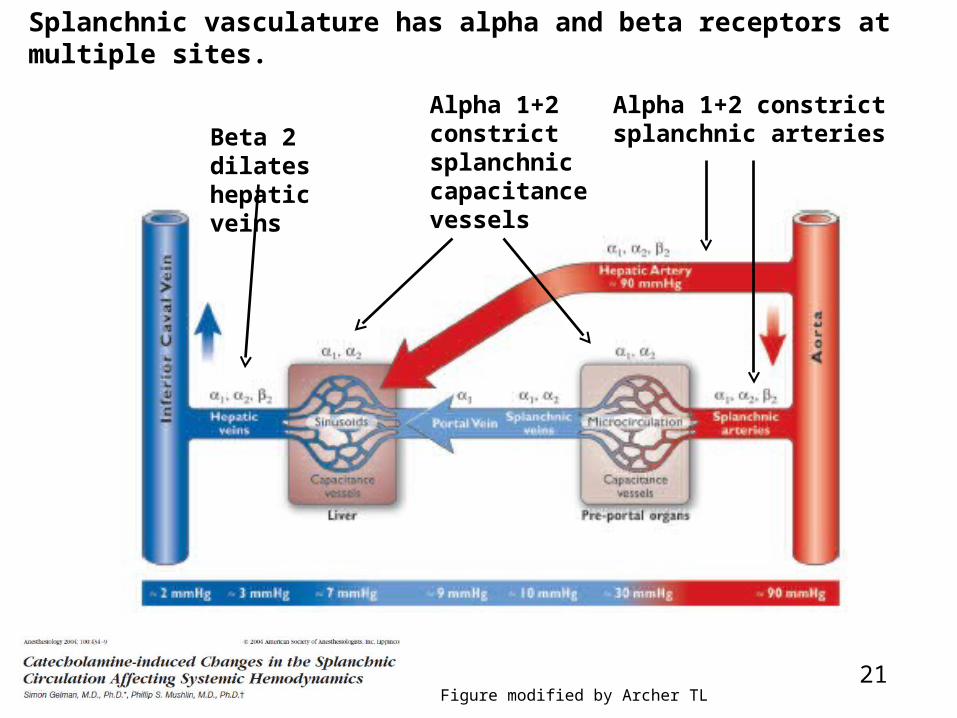
Splanchnic vasculature has alpha and beta receptors at multiple sites.
Beta 2 dilates hepatic veins
Alpha 1+2 constrict splanchnic capacitance vessels
Alpha 1+2 constrict splanchnic arteries
Figure modified by Archer TL21
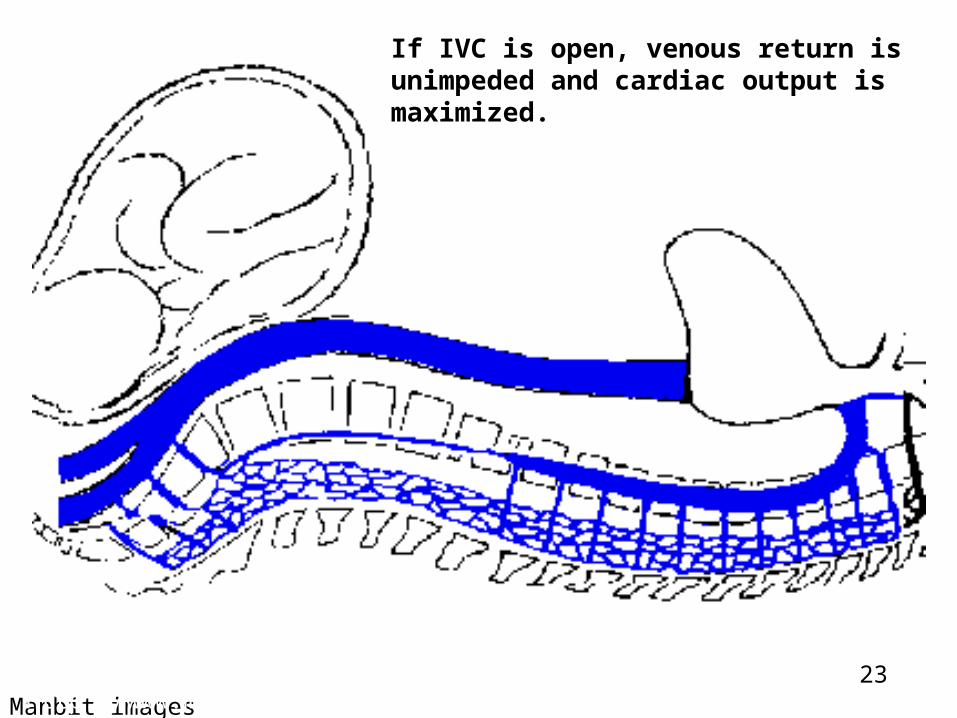
Decreased venous return and cardiac output due to sympathectomy is exacerbated by obstruction of IVC.
22
Manbit imageshttp://www.manbit.com/OA/f28-1.htm
If IVC is open, venous return is unimpeded and cardiac output is maximized.
23
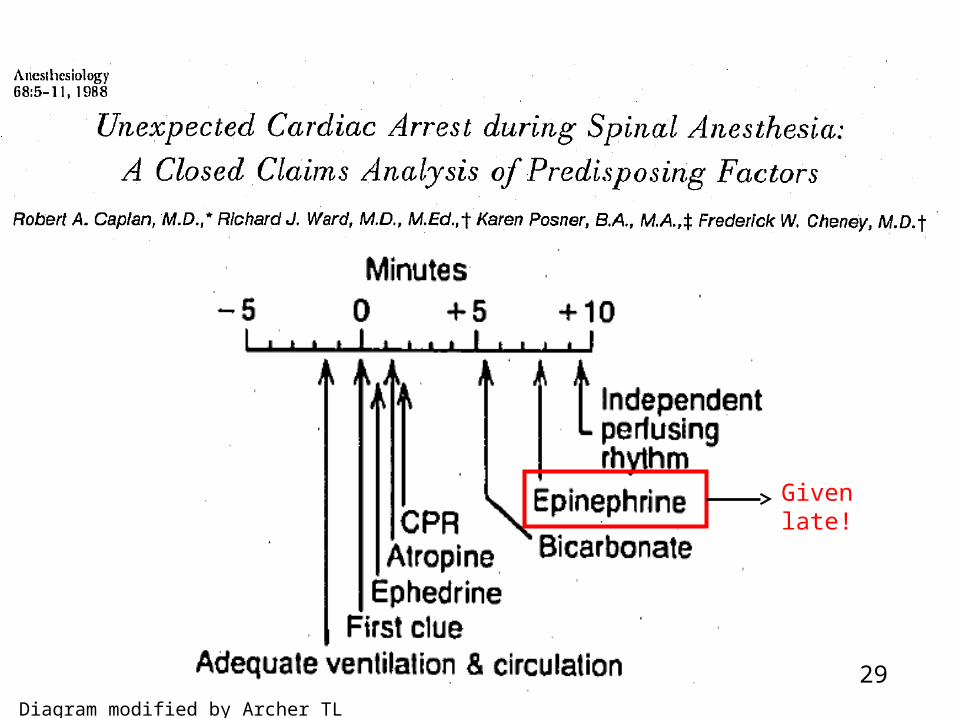
Given late!
Diagram modified by Archer TL
29
Avoid cardiac arrest after neuraxial block
• Talk with patient during test dose. “Heart pounding, legs numb or weak?” Have Ambu bag and pressors immediately available.
• Allow 2-3 minutes for test dose to be positive. Consider dosing epidural fentanyl 100 mcgm after test dose since it will augment block but not “burn any bridges.”
• Stay with patient 15-30 minutes after initiation of block to r/o hypotension, hyperstimulation or excess block. Do charting. Start infusion. Make sure nurse will stay with patient after you leave. 30
Cardiac arrest in labor room– do the CS in the labor room!
• “Four minute rule”– start CS within 4 minutes of arrest. Deliver baby within 5 minutes to avoid neonatal brain damage.
• “Our findings imply that perimortem cesarean delivery during actual arrest would require more than 5 minutes and should be performed in the labor room rather than relocating to the operating room.”
Obstet Gynecol. 2011 Nov;118(5):1090-4.Labor room setting compared with the operating room for simulated perimortem cesarean delivery: a randomized controlled trial.Lipman S, Daniels K, Cohen SE, Carvalho B.
33
High spinal (or epidural)
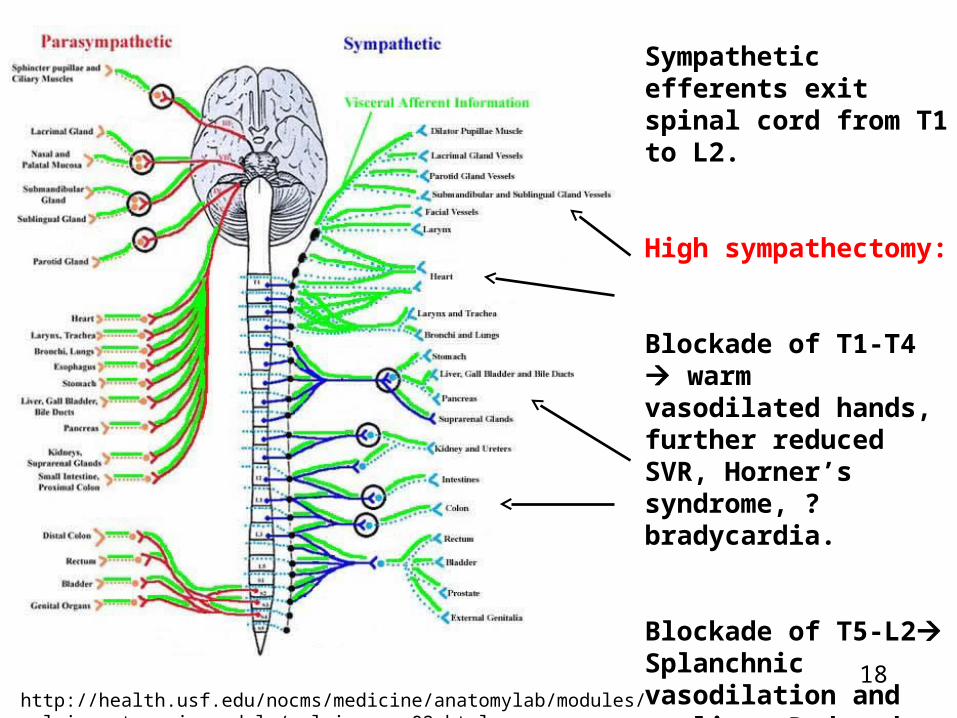
http://health.usf.edu/nocms/medicine/anatomylab/modules/pelvic_autonomic_module/pelvic_page02.html
Sympathetic efferents exit spinal cord from T1 to L2.
High sympathectomy:
Blockade of T1-T4 warm vasodilated hands, further reduced SVR, Horner’s syndrome, ? bradycardia.
Blockade of T5-L2Splanchnic vasodilation and pooling. Reduced venous return (CO), especially with IVC obstruction. Reduced SVR.18
High or Total Spinal
• A circulatory as well as respiratory emergency.
• You will have to assist or control ventilation.
• You must recognize situation immediately and act rapidly and with confidence so that patient does not panic (too much).
High or Total Spinal
• Say three things:
– “You’re going to be OK.”
– “This happens sometimes when the spinal goes too high.”
– “I’m going to help you breathe.”
High or Total Spinal
• Do this:
• Unwrap circle system tubing and mask and close down pop-off valve.
• Put mask on face and assist ventilation. Explain what you are doing. Patient is panicking.
•

High or Total Spinal
• Do this:
• Feel for a pulse and if weak (or just empirically) give ephedrine 10-25 mg. Atropine for bradycardia.
• Check BP, but all that really matters is ventilation and a good pulse.
High or Total Spinal
• Should you intubate?
• It depends, but ventilation trumps intubation.
• Ventilation even trumps aspiration.
• My rule of thumb: LOC, total apnea intubate. But stabilize BP and oxygenation first, even before intubation!
Low spinal
Low spinal
• Hyperbaric (bupivacaine) solution will “pool” in the dural sac below the sacral promontory if patient is allowed to sit for too long after the intrathecal injection.
• Trendelenburg position often used “to move level up”– but no proof it really works.
Low spinal
• Cough often used “to move level up”-- but no proof it really works.
• T’burg + flexion of thighs on the abdomen– straightens lumbar curve and raises intra-abdominal pressure.
• I believe this works.
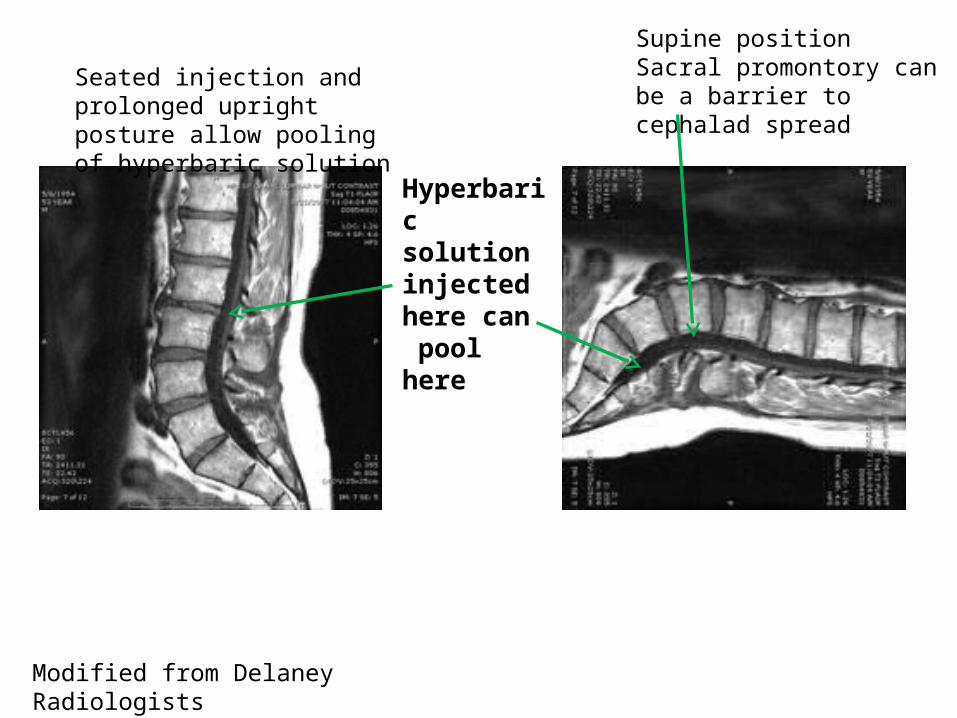
Hyperbaric solution injected here can pool here
Seated injection and prolonged upright posture allow poolingof hyperbaric solution
Modified from Delaney Radiologists
Supine positionSacral promontory can be a barrier to cephalad spread
Avoiding a low spinal• Have patient lie down rapidly after intrathecal
injection. Have her position herself on the OR table. Trendelenberg? Cough?
• Flexion of thighs on the abdomen to flatten lumbar curve and to increase intra-abdominal pressure.
Image from Boba, Inc.
Repeat the spinal?
• Bupivacaine takes 15-20 minutes for full effect, so don’t rush it.
• Beware of high or total spinal if you repeat the injection.
• How’s the airway?
• Epidural may be better.

Fetal bradycardia after neuraxial analgesia
Fetal bradycardia after neuraxial analgesia
• Classic scenario for hypertonic uterus is: Patient has oxytocin augmentation of labor and severe pain. CSE with lipid soluble narcotic is given rapid pain relief. Fetal bradycardia occurs 10-30 minutes after the block. Loss of beta stimulus?
• May or may not be accompanied by hypotension, but hypertonic uterus is a separate phenomenon, requiring uterine relaxation. Correction of BP is not enough!
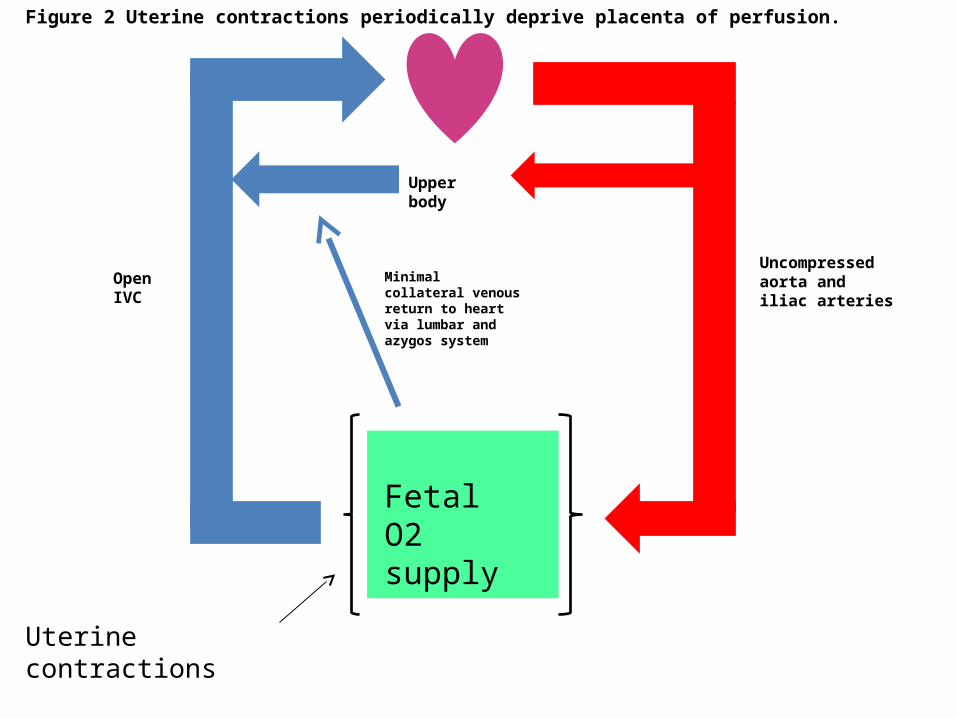
Minimal collateral venous return to heart via lumbar and azygos system
Open IVC
Uncompressed aorta and iliac arteries
Figure 2 Uterine contractions periodically deprive placenta of perfusion.
Upper body
Uterine contractions
Fetal O2 supply
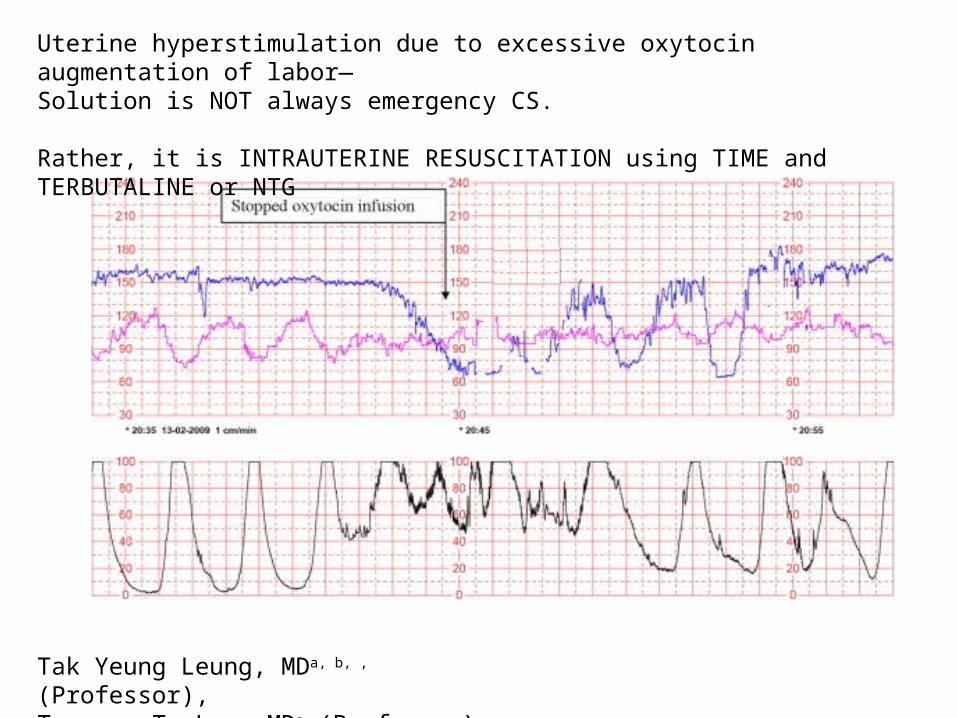
Tak Yeung Leung, MDa, b, , (Professor), Terence T. Lao, MDa (Professor)
Uterine hyperstimulation due to excessive oxytocin augmentation of labor—Solution is NOT always emergency CS.
Rather, it is INTRAUTERINE RESUSCITATION using TIME and TERBUTALINE or NTG
Detecting uterine hyperstimulation
• Key “maneuver” is to think of the possibility and to evaluate uterine tone by palpation or IUPC during fetal bradycardia.
• Recognition of uterine hyperstimulation and reversal with terbutaline SC or NTG SL or IV can avoid an unnecessary CS!
Intraoperative pain during CS
Intraoperative pain during CS• “Management of expectations”– don’t
promise a pain-free experience. • Discuss intraoperative pain management
options ahead of time. What will patient tolerate?
• Mild discomfort fentanyl + local infiltration?
Intraoperative pain during CS
• More discomfort Fentanyl, midazolam + ketamine (low dose and maintain responsivenss). Keep your suction at the ready.
• Severe discomfort RSI/ GA.
Choice of neuraxial technique when airway is bad.
• Consider avoiding CSE if airway is bad: epidural may fail, leaving patient with surgery underway and disappearing block.
• If airway is bad, straight epidural or continuous spinal anesthesia may be a better choice than CSE, since you know it works from the outset, before surgery starts.
Can’t intubate under GA
Can’t intubate under GA
• A few comments only:
• 1) Pregnancy involves weight gain and airway edema.
• 2) Pre-eclampsia and pushing make 1) worse.
• 3) Nose bleeds easily in pregnancy.
Can’t intubate under GA
• 4) Position every patient assuming you will have to intubate her (e.g. ramp, Glidescope, etc, available if need foreseen).
• 5) Avoid CSE if airway is unfavorable for intubation. The reason is: epidural part of CSE may fail when you try to activate it.
• 6) Continuous epidural or spinal is better if airway is bad. That way you know anesthesia will work as long as you need it, before surgery starts.
Management of “can’t intubate” situation
• Elective procedure awaken patient and secure airway by other means (e.g. AFOI).
• Emergency procedure LMA?, careful ventilation, good paralysis (avoids coughing and retching).
Post-delivery lower extremity neuropathy
Post-delivery lower extremity neuropathy
• “Post-delivery” does not = “Due to anesthesia”
• Vast majority of post-delivery neuropathies are due to nerve stretch, pressure, compression or ischemia– not due to needle damage or local anesthetic toxicity.
• “Obstetric palsy”– from fetal head, forceps or positioning. Often seen without anesthesia.
Post-delivery lower extremity neuropathy
• So, relax when you see these patients!
• You probably did not (directly) cause it-- and it will almost certainly resolve over time.
• On the other hand– listen well, be sympathetic and get proper consultation and therapy.
• Do not be dismissive of the problem!
Post-delivery lower extremity neuropathy
• Take a good history and do a good physical.
• Rule out signs and symptoms of meningitis, spinal hematoma or infection.
• Do not hesitate to get Neurology consultation.
• Stay in touch with the patient.
Obstetric palsy
• From nerve compression within the pelvis, by fetal head, forceps or retractors.
• Often blamed on neuraxial anesthesia.
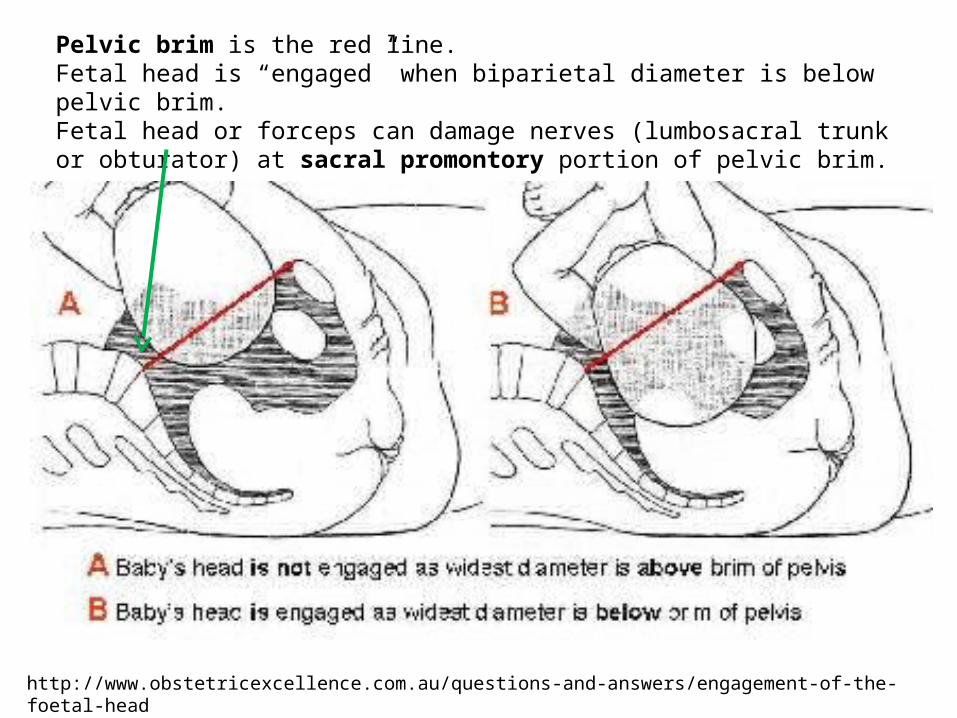
Pelvic brim is the red line.Fetal head is “engaged” when biparietal diameter is below pelvic brim.Fetal head or forceps can damage nerves (lumbosacral trunk or obturator) at sacral promontory portion of pelvic brim.
http://www.obstetricexcellence.com.au/questions-and-answers/engagement-of-the-foetal-head
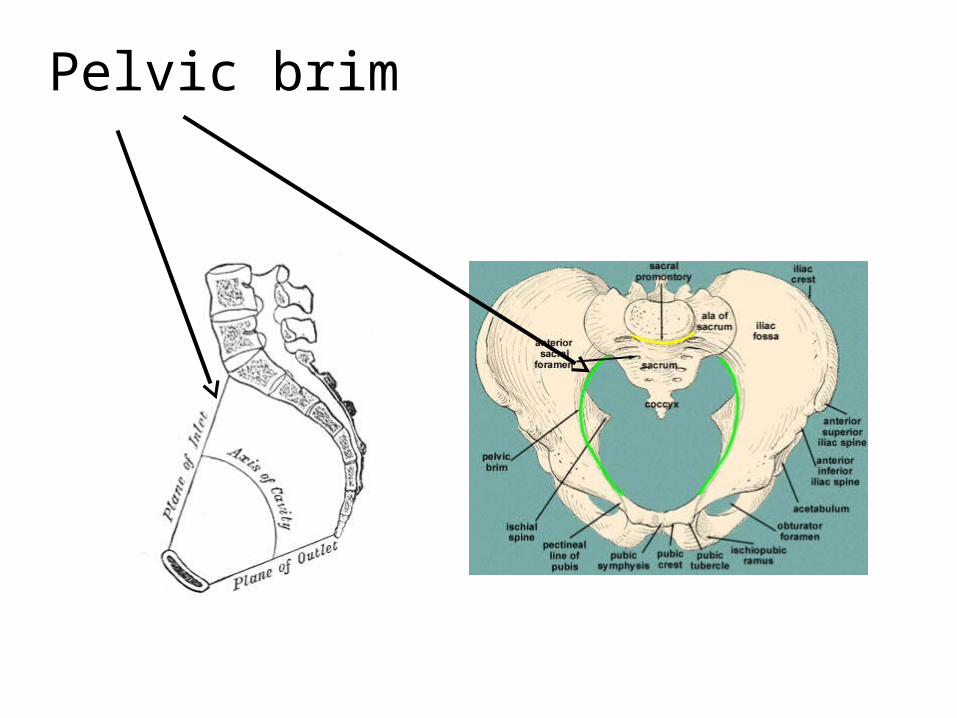
Pelvic brim
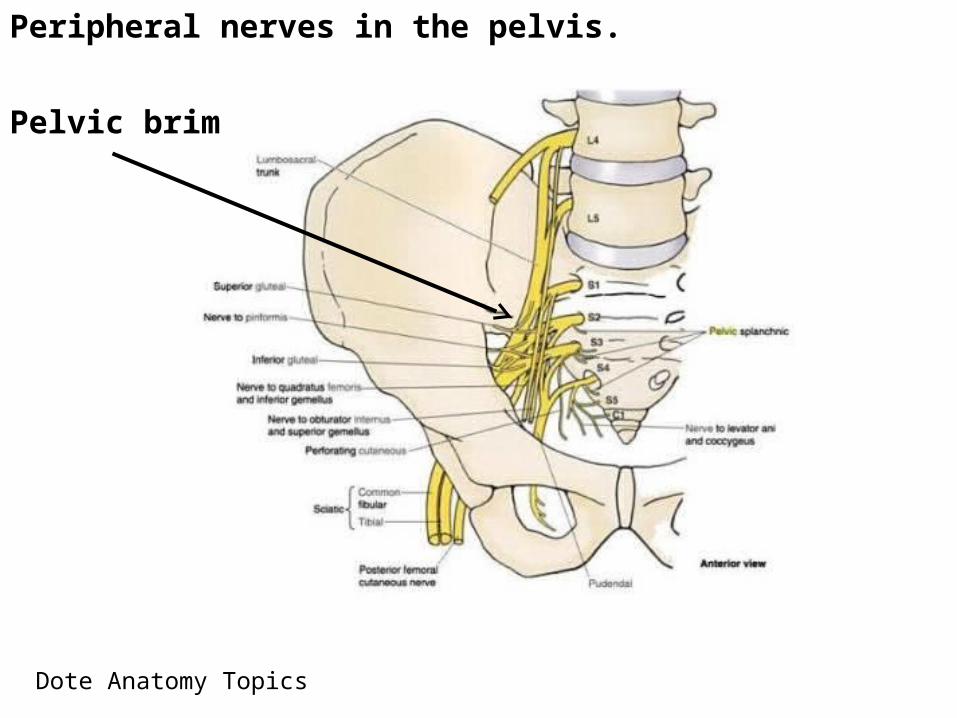
Peripheral nerves in the pelvis.
Pelvic brim
Dote Anatomy Topics
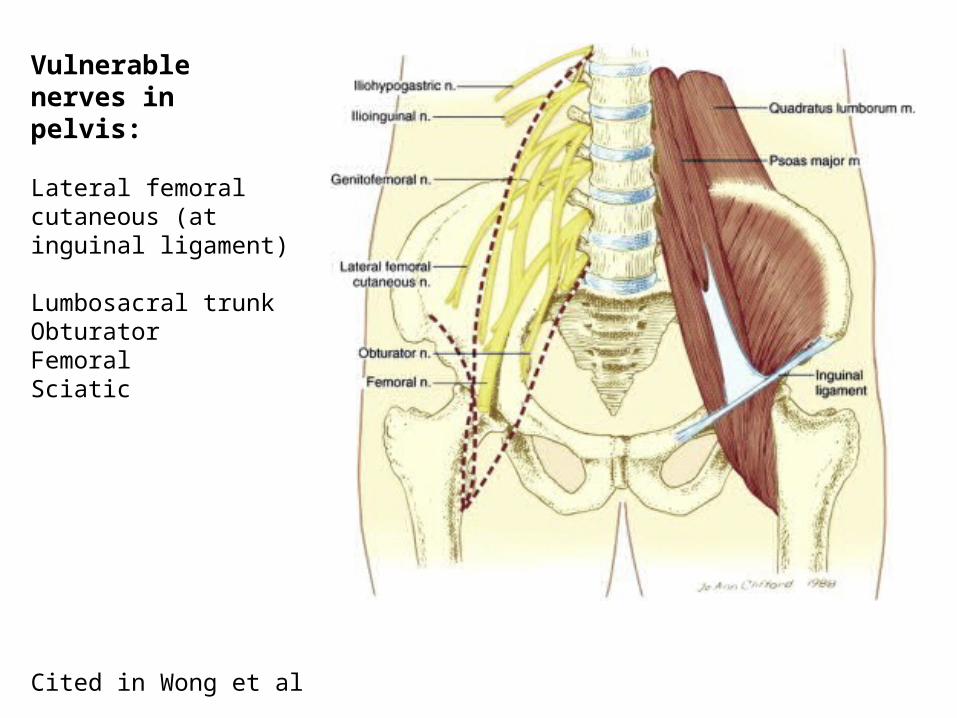
Cited in Wong et al
Vulnerable nerves in pelvis:
Lateral femoral cutaneous (at inguinal ligament)
Lumbosacral trunkObturatorFemoralSciatic
Safeguards to Minimize Peripheral Nerve Compression
• Be watchful for patient positioning that contributes to nerve compression…
• Avoid prolonged use of the lithotomy position; regularly reduce hip flexion and abduction.
• Avoid prolonged positioning that may cause compression of the sciatic or peroneal nerve.
F. Reynolds in Chestnut
Safeguards to Minimize Peripheral Nerve Compression
• Place the hip wedge under the bony pelvis rather than the buttock.
• Use low-dose local anesthetic/opioid combinations during labor to minimize numbness and allow maximum mobility.
• Encourage the parturient to change position regularly.
F. Reynolds in Chestnut

Peripheral Neuropathy Syndromesin Obstetrics
• “Meralgia Paresthetica”– lateral femoral cutaneous nerve (pure sensory)– numbness of lateral thigh. Common in pregnancy.
• Femoral nerve damage from prolonged hip flexion weak quadriceps. Can’t straighten leg and climb stairs.
Peripheral Neuropathy Syndromesin Obstetrics
• Foot drop– Impaired foot dorsiflexion due to:– Common peroneal nerve at fibula (leg holders)– Lumbosacral trunk at pelvic brim (fetal head)
• Impaired dorsi- and plantar-flexion of foot and numbness below knee: Sciatic nerve damage. Pressure on buttock during long CS? Diabetic patient?
• Impaired adduction of thigh and inner thigh numbness– obturator palsy at pelvic brim
The End
Extra slides

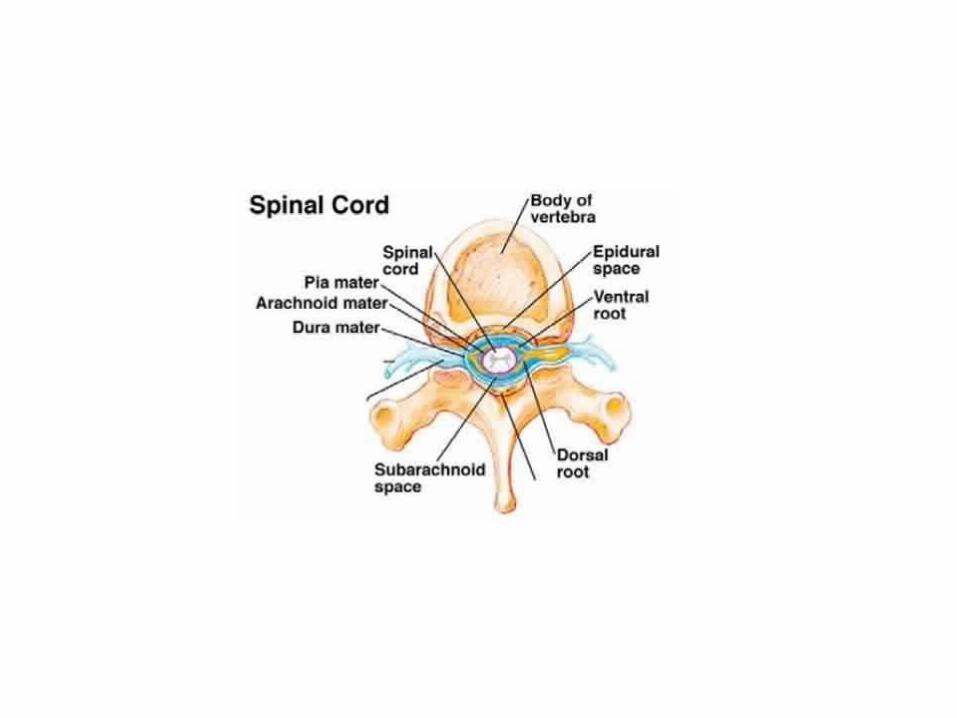
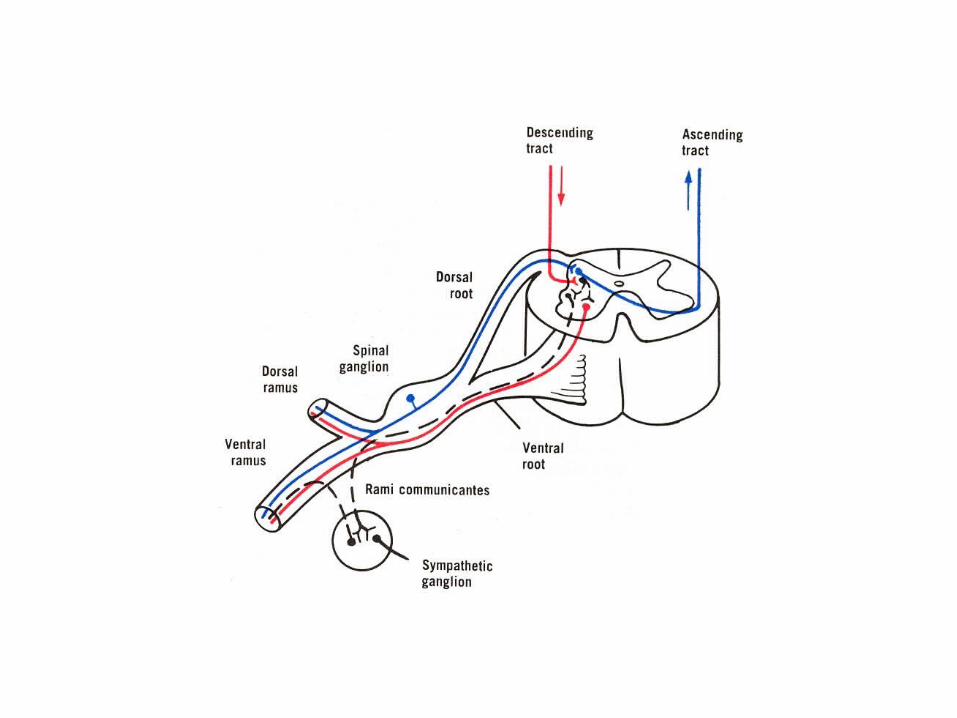
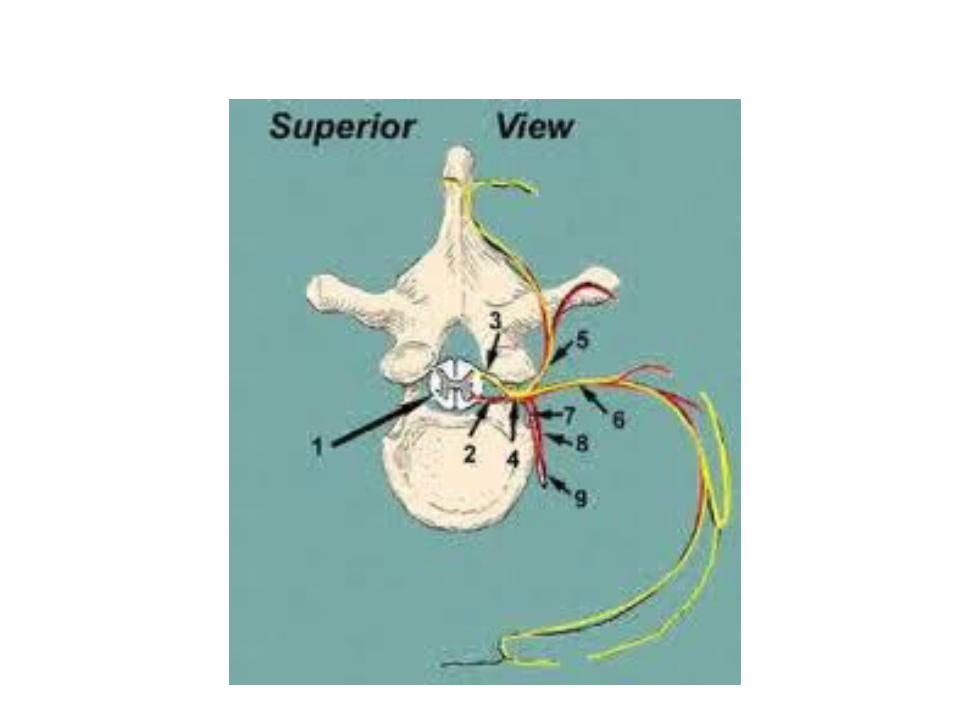
Spinal nerve “roots” are within the spinal canal. Dorsal root ganglion is at intervertebral foramen.