communicating in ageing societies
TRANSCRIPT
“Communicating in Ageing Societies: Diversity and Dementia Looking to 2050”
Authors
Hamish Robertson, Postgraduate Student, FoM, UNSWAssociate Professor Tuly Rosenfeld MBBS, FRACP, FoM, UNSW
Dr Joanne Travaglia, PhD, Senior Lecturer, FoM, UNSW

Introduction
• Changing global conditions, ageing and vulnerability
• Implications of population ageing for communication theory and practice
• Issues associated with the clinical aspects of ageing societies
• Social and societal changes have communication consequences – diversity matters
• Issues associated with globalisation, immigration and emigration

Disasters and Extreme Weather EventsNew Zealand, Japan, Thailand (etc) in 2001 Alone
Source: Sydney Morning Herald 19th November 2011
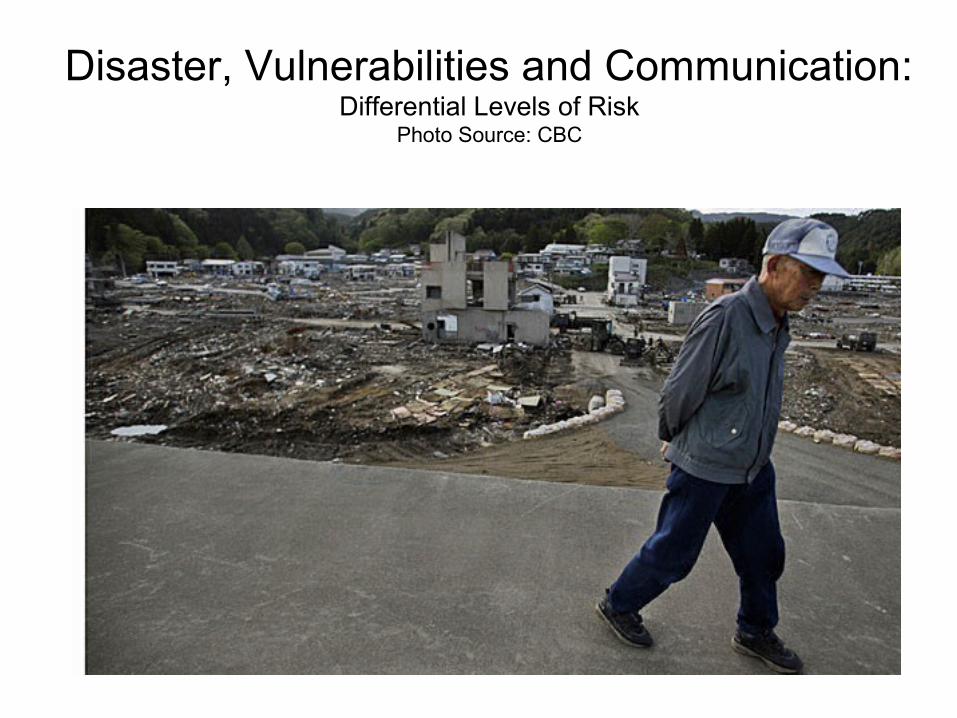
Disaster, Vulnerabilities and Communication:Differential Levels of Risk
Photo Source: CBC
Future Issues for the Asia-Pacific Region
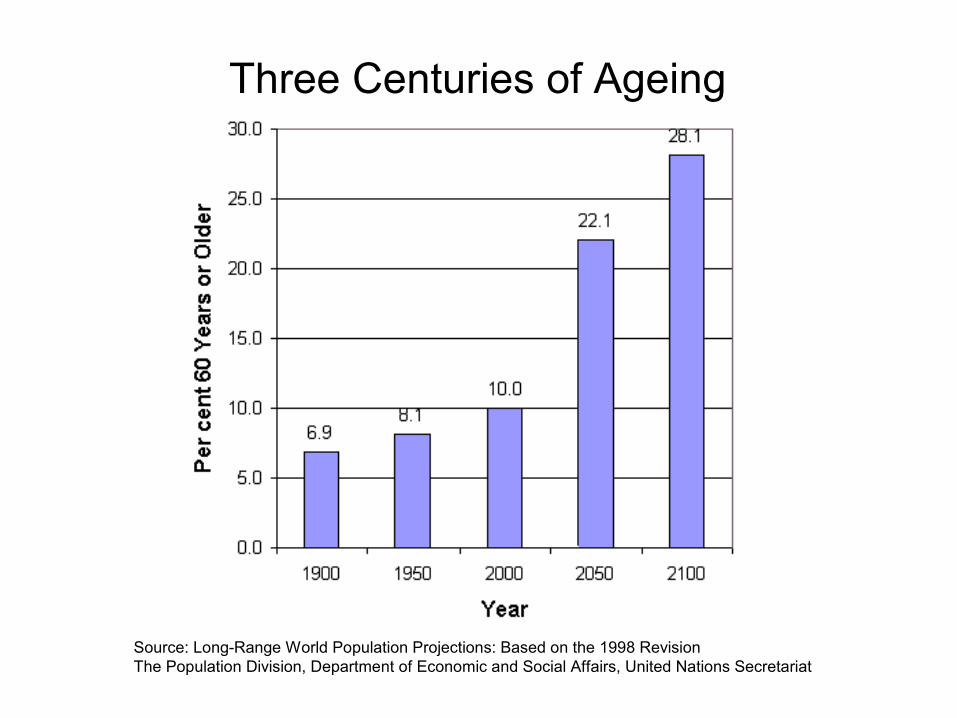
Three Centuries of Ageing% Aged 60+
Source: Long-Range World Population Projections: Based on the 1998 RevisionThe Population Division, Department of Economic and Social Affairs, United Nations Secretariat

Global Population AgeingSource: Why Population Aging Matters: A Global Perspective, USA, 2007

Population Ageing in Australia
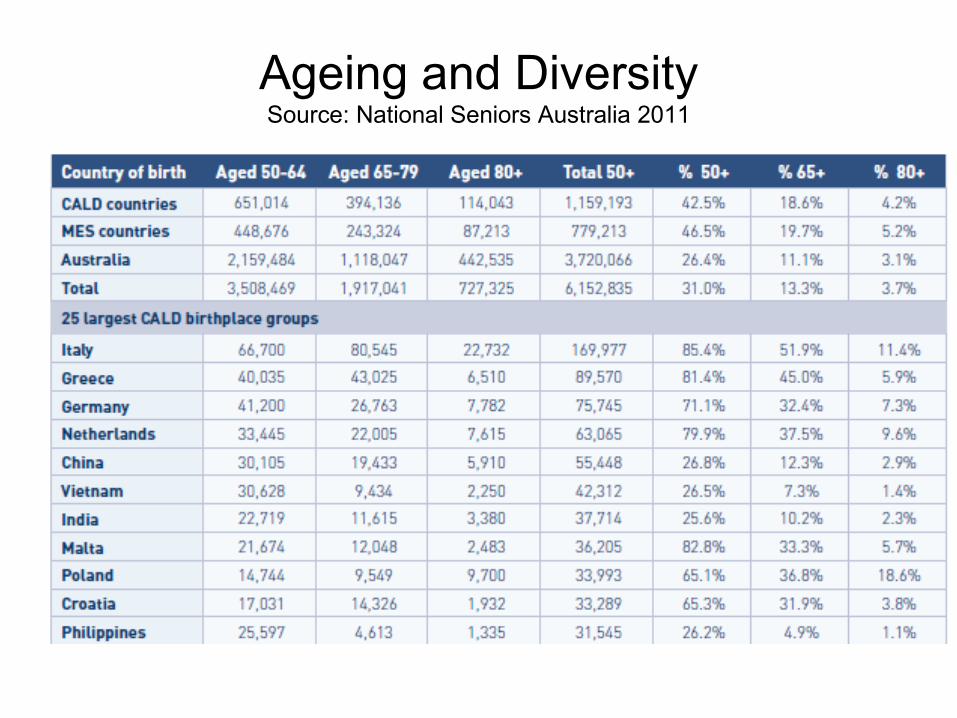
Ageing and DiversitySource: National Seniors Australia 2011

First World Epidemiologic TransitionsImmediate causes of death
18th-19th century 20th century 21st century
Infectious Diseases
Typhoid, CholeraDiarrhoeasSmall Pox & TB
Mortality - high in Infants/Children
Fertility - high
Systemic Diseases
Heart, Vascular, Stroke, Diabetes Lung diseases
Mortality – high in mid-life - then delay
Fertility – falling
Brain Diseases *
Dementias; PDCognitive disordersGait disorders
Mortality delayed to Old Age
Fertility - low
*G.A. Broe and H. Creasey - New Epidemiological Transition – 1997, 2003

Human Life Expectancy
• 2.5 yrs on average for every decade of the 20th century – Vaupel et al
• Upper limits to LE, if so what?, or LE plasticity (neural plasticity now well known)
• Centenarian studies eg. Okinawa, Sardinia
• Emergence of supercentenarians aged 110+?
• Health and social policy challenged to catch up to a century-long trend!
Epidemiology of Ageing
• Older people are more likely to have a complex set of co-morbidities esp. chronic conditions
• Neurodegenerative diseases rise in prevalence and incidence with ageing esp. the ‘old old’
• Disability status of older people is usually more complex• Diagnosis of older peoples’ conditions in systems that
focus younger to mid-life health issues is problematic• Life expectancies are still rising but systems are proving
slow to adapt• Many health professions focus on their preferred patient
types rather than emergent types e.g. child and maternal versus geriatrics

Clinical Aspects: Examples• Visual impairments including macular degeneration• Hearing impairments including Deafness/deaf/deaf-blind/HoH/
tinnitus • Cognitive, memory and behavioural problems associated with
neurodegenerative disorders/diseases• Dementia spectrum including MCI and AD – 50:50 chance of
diagnosis in primary care (Draper et al, 2011)• Movement disorders including PD and gait ataxias• TIA/Stroke – aphasia etc• Persistent pain – eg. post-operative and post event, headache,
neuralgia, severe/persistent dental infections etc• Delirium in hospital – eg. staph infection and consent• Polypharmacy – multiple drugs and their interactions in frail older
people• Disability status, cause and consequences for daily life
The whole issue of ethical communication in healthcare settings is very poorly addressed and will grow in scope and complexity as the population ages.

Communication and Satisfaction with Health Providers
Source: Patient Experience Survey, ABS (2011)
• Levels of satisfaction also differed by age. Of persons aged 75 years and over that visited an ED in the previous 12 months for their own health, 93% felt that ED doctors and specialists always or often spent enough time with them, compared with 73% of those aged 25-34.
• When it came to whether hospital doctors and specialists always or often listened carefully, persons from areas of most disadvantage reported lower rates of satisfaction (87%) than those from areas of least disadvantage (92%)


Diversity, Ageing and Communication
• Varied and changing social structures eg. families, marriages, households, immigration, emigration, sexuality etc
• Diversity is the human social norm but generally vilified by the modern state and its entities eg. language, culture, ethnicity and religion in health, education and justice
• Migration experiences e.g. educational, economic, displaced, refugee, climate change?!
• Language and literacy issues eg. spoken, written, contextual, experiential, accents!
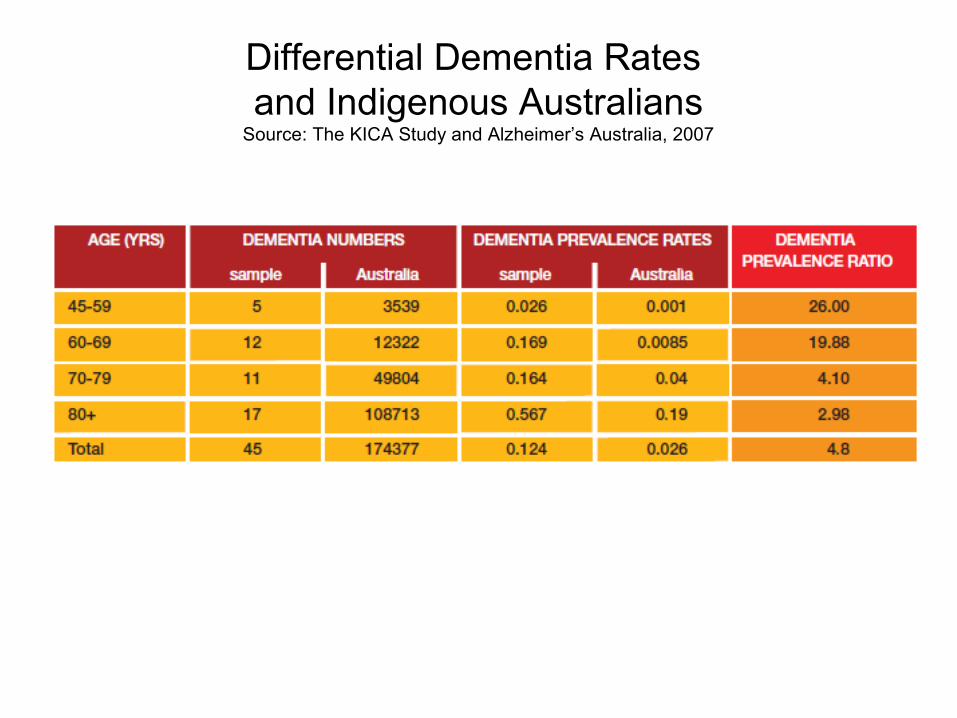
Differential Dementia Rates and Indigenous Australians
Source: The KICA Study and Alzheimer’s Australia, 2007

Social Aspects• Social changes have important implications for
communications theory and practice – old norms easily superseded and institutions usually shaped around these, not emerging norms (lag effects)
• Diversity has major implications for care in ageing societies eg. disability groups, gay and lesbian issues, ethnic and linguistic minorities, refugee groups, isolated individuals, religious minorities => bioethics
• Capacity of monolingual systems to adapt to diversity of needs eg. health care systems, education etc
• Contextual factors eg. individual, educational, financial, social supports etc
• The persistence of racialised thought and language as independent knowledge in situations requiring knowledge about diversity, migration, communication and ageing
Societal Aspects
• Broader social, economic, environmental and climatic changes – vulnerabilities are man-made
• Globalisation of population and population movements, skills, labour, educational and even health markets
• Globalisation of media including linguistic minority media in many countries eg. cable, TV, newspapers, radio and internet in Australia – transnational consumption
• Changes in knowledge production and underlying assumptions about the world ie. epistemic shifts (epistemic modesty needed)

Conclusion
• Ethical issues are substantial, persistent, growing and poorly addressed – delirium scenario typical, TB, consent, patient safety etc
• Health professionals need to be educated in diversity not just about diversity (practice over concepts over ideology)
• Communication professionals need to address the ideology-practice divide and broaden/contribute to these issues
• Theory and knowledge base need to expand in the face of these major and inevitable changes