community-based rehabilitation in moshupa village, botswana
TRANSCRIPT
d i s a b i l i t y a n d r e h a b i l i t a t i o n , 1999; v o l . 21, n o s . 10± 11, 515± 521
Community-based rehabilitation in Moshupavillage, Botswana
LENA A. NORDHOLM ‹ * andBIRGITTA LUNDGREN-LINDQUIST Œ
‹ Go$ teborg University, Department of Rehabilitation, Box 111, SE40530 Go$ teborg, Sweden
ΠLa Trobe University, School of Occupational Therapy, Bundoora, Victoria 3083, Australia
Summary
This article presents a summary of ® ndings from the`Moshupa Community Based Rehabilitation (CBR) project’ ,which to date have been the subject of three studies: one initialsurvey of disabled people and two follow-up studies. Of the 132disabled people who were identi® ed in the survey, all but threecould be accounted for in the ® rst follow-up. Seventy-sevenwere interviewed about independence of activities of dailyliving, school} jobs and quality of life. A high percentage ofelderly (17% were 65 and over) were alive, and most hadmaintained high levels of ADL skills. Twenty per cent of theadult disabled were working, 10 out of 14 school-aged childrenwere enrolled in schools, and life satisfaction was high. Thesecond follow-up study indicated that personnel, althoughacknowledging the bene® ts of the programme, pointed toseveral remaining problems such as lack of rehabilitationeducation for the personnel. The results are discussed withreference to the CBR programme’s aims, and implicationsdrawn for industrialized countries.
Introduction
In this article we will describe the Botswana
Community-Based Rehabilitation (CBR) project, which
was initiated in 1990 and ® rst described by Lundgren-
Lindquist and Nordholm 1993." A follow-up study on
the impact of CBR was next carried in 1993# and a
second follow-up of a selected group of clients and the
rehabilitation workers and volunteers in 1995.$ Details
of the second follow-up have not previously been
published.
b a c k g r o u n d
In 1976 the member countries of WHO adopted an
approach to rehabilitation called community-based re-
* Author for correspondence.
habilitation.% Rehabilitation is de® ned as `a process
aimed at enabling persons with disabilities to reach and
maintain their optimal physical, sensory, intellectual,
psychiatric and} or social functional levels, thus pro-
viding them with tools to change their lives towards a
higher level of independence’ .& In CBR the emphasis
traditionally placed on an institutional approach has
been shifted to a community-oriented approach. This
approach has been described by Helander as `a strategy
for enhancing the quality of life of disabled people by
improving service delivery, by providing more equitable
opportunities and by promoting and protecting their
human rights. It calls for the full and coordinated
involvement of all levels of society : community ; in-
termediate and national’ .’
At the community level CBR is seen as a component of
community development. It involves mobilization of
local resources, such as the family. The community
should support the families who carry out rehabilitation
at home. It should also provide opportunities for
education, and functional and vocational training, and
ensure that disabled members are not deprived of their
human rights. Self-actualization, self-determination,
social integration and empowerment are key concepts. A
community committee should be set up to provide local
management. ’
At the intermediate level the government should
provide professional support services. The personnel
should train and supervise the community personnel,
provide services and managerial support, and liaise with
referral services. ’
At the national level CBR seeks the involvement of the
government in planning, implementing coordinating,
and evaluating the CBR system. This should be done in
cooperation with communities, the intermediate-level
and the non-governmental sector, including
organizations of disabled people. ’
Disability and Rehabilitation ISSN 0963± 8288 print} ISSN 1464± 5165 online # 1999 Taylor & Francis Ltdhttp:} } www.tandf.co.uk} JNLS } ids.htm
http:} } www.taylorandfrancis.com} JNLS } ids.htm
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
McM
aste
r U
nive
rsity
on
10/2
8/14
For
pers
onal
use
onl
y.
L. A. Nordholm and B. Lundgren-Lindquist
CBR may be the best answer for a majority of disabled
people, but it is of greatest importance that a person with
a disability is carefully assessed and given full equal
opportunities for development of his } her full talents. `If
a blind boy is capable of becoming a professor there is
absolutely no reason why he should be encouraged to
take up dairy farming, operating a small shop in a village
or do similar occupations.’ ( Therefore, according to
Advani,( it is necessary to `develop delivery programmes
that are balanced, realistic and are tailored to the needs
not just of the majority but also of a minority which is
talented and capable of making a valuable contribution
to the enrichment of our social, economic and cultural
life’ .
CBR programmes have been initiated in many of the
developing countries. However, not all of these are
sustained over a period of time. In countries where a
large proportion of the people live in poverty, govern-
mental priorities may not emphasize the needs of disabled
people. Along with the establishment of CBR pro-
grammes, the need for evaluation has been recognized
and the importance of continuous follow-up
emphasized. ) Several successful evaluation studies have
been carried out, such as Finnstam et al.,* Rottier et al." ! ,
Mariga and McConkey " " and Lagerkvist. " # These studies
suggest that CBR is a feasible and e� cient way of
providing guidance and assistance to the disabled.
p u r p o s e
The major purposes for the three studies carried out
on the Botswana project were :
(1) to identify and describe disabled people in
Moshupa village, in the context of establishing a
CBR programme initially;
(2) to follow up the disabled people in order to study
the impact of the CBR programme at a later date ;
(3) to assess the perceptions of rehabilitation workers
in Moshupa village as to the strengths and
weaknesses of the programme.
b o t s w a n a Ð t h e c o u n t r y a n d i t s p o p u l a t i o n
Botswana lies at the centre of the southern African
plateau. Approximately 84% of the land surface is
covered with sand, which supports a low savanna
vegetation. The population was about 1.3 million in early
1992. There are many diŒerent tribal groups and many
languages and dialects spoken. The most common
language is Setswana, but the o� cial language in English.
The household is the basic unit in each village. One or
more rondavels Ð circular, thatch-roofed clay houses Ð
situated within a compound, surrounded by a fence or
low wall, accommodate the household. The huts are
mainly used as bedrooms. All activities such as cooking,
other household work, repair of utensils or production of
utility products take place outside the huts. All of these
activities are usually performed by the women when they
are not busy in the ® elds, stamping corn, or carrying
water from a distant pipe.
The village Moshupa was chosen as study area. This
village, situated in the south district of Botswana, close
to the desert, has a population of about 11000, and is
fairly typical of a large village in Botswana. It is
governed by a chief and 15 headmen. People have more
than one homestead, such as a cattlepost, a shelter on
their agricultural land and a home in the village. This
pattern of settlement is typical for the country, but
makes it hard to locate people. Health services are
provided by three small health posts. There is no doctor
in the village.
Method
s u r v e y m e t h o d
The ® rst study of the Botswana project was carried out
in 1990 and is described in more detail in Lundgren-
Lindquist and Nordholm. " The initial phase of the
project involved educating and motivating the com-
munity leaders to obtain their support for the project. In
order to identify disabled persons, a door-to-door survey
was conducted. The personnel participating in the survey
were given education about CBR and instructions about
the survey form to be used. The standardized questions
used in the survey included:
(1) Family history (e.g. Were the parents related?
How many children in the family? Birth order of
the disabled person).
(2) Pregnancy and delivery.
(3) History of disability (e.g. At what age was the
disability discovered? What was the perceived
cause of the disability?)
(4) Type of disability.
(5) Type of treatment Ð if any.
(6) Education.
(7) Activities of daily living.
As a result of the survey, 151 disabled persons were
identi® ed. However, su� ciently completed survey forms
were available for 132 individuals, who thus comprised
the study population. Rehabilitation interventions were
proposed for all those concerned, which included
surgery, medical treatment, blind} deaf school referrals,
orthoses, prostheses and technical aids.
516
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
McM
aste
r U
nive
rsity
on
10/2
8/14
For
pers
onal
use
onl
y.
CBR in Moshupa village, Botswana
m e t h o d o f t h e f i r s t f o l l o w - u p s t u d y
In 1993 (3 years after the establishment of the CBR
programme) a follow-up of the 132 disabled persons was
conducted. # When a client had been located, a re-
habilitation assistant conducted the interview in
Swetsana under the guidance of a senior researcher. Each
interview lasted between 30 and 60 minutes. The disabled
person was interviewed whenever possible. In some cases
(for example very young children or persons who were
unable to communicate) a family member, relative or
caregiver answered for the disabled person. The interview
questions included family structure, treatment, activities
of daily living, use of aids, working} schooling, per-
ception of whether life was better} worse } the same as 3
years earlier, quality of life.#
m e t h o d o f t h e s e c o n d f o l l o w - u p s t u d y
Two years later again (in 1995), a second follow-up
study was carried out.$ A small selected sample of 20
clients were interviewed, but the major emphasis in this
study was on the rehabilitation personnel, in order to
ascertain their perceptions of strengths and weaknesses
of the CBR programme in Moshupa. Two persons of the
CBR team and 15 Red Cross volunteers were interviewed
with standardized open-ended questions using an in-
terpreter, who was a member of the Red Cross team.
The questions included CBR training, use of the CBR
manual, visits to disabled persons, perceived strengths
and weaknesses of the CBR programme, suggestions for
improving the CBR programme.
Results
d e s c r i p t i o n o f t h e s t u d y p o p u l a t i o n
Age and sex
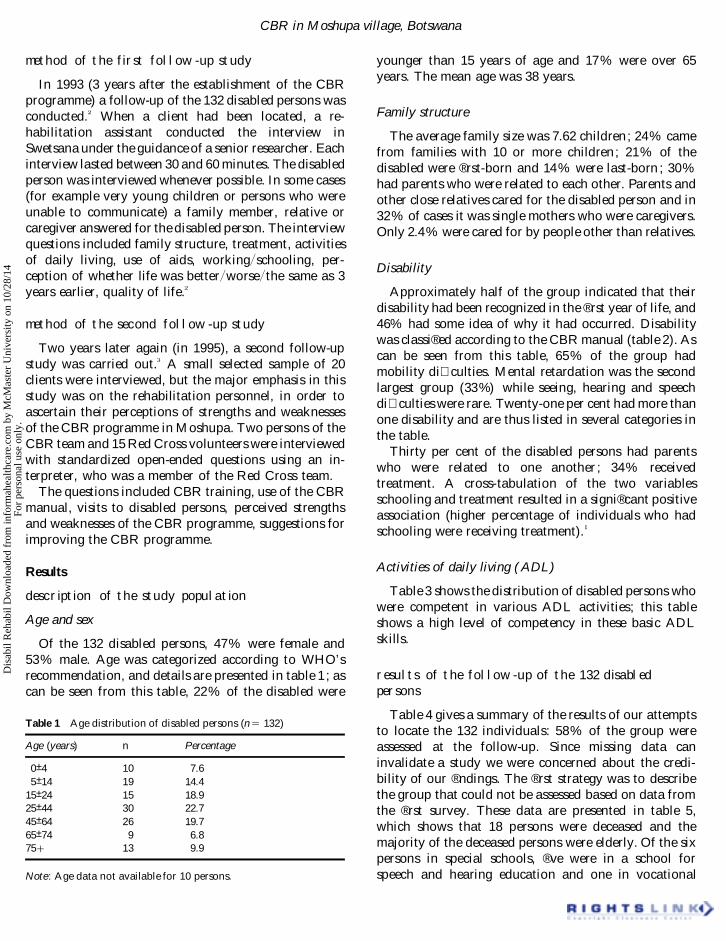
Of the 132 disabled persons, 47% were female and
53% male. Age was categorized according to WHO’ s
recommendation, and details are presented in table 1 ; as
can be seen from this table, 22% of the disabled were
Table 1 Age distribution of disabled persons (n 5 132)
Age (years) n Percentage
0± 4 10 7.65± 14 19 14.4
15± 24 15 18.925± 44 30 22.745± 64 26 19.765± 74 9 6.8751 13 9.9
Note: Age data not available for 10 persons.
younger than 15 years of age and 17% were over 65
years. The mean age was 38 years.
Family structure
The average family size was 7.62 children; 24% came
from families with 10 or more children; 21% of the
disabled were ® rst-born and 14% were last-born ; 30%
had parents who were related to each other. Parents and
other close relatives cared for the disabled person and in
32% of cases it was single mothers who were caregivers.
Only 2.4% were cared for by people other than relatives.
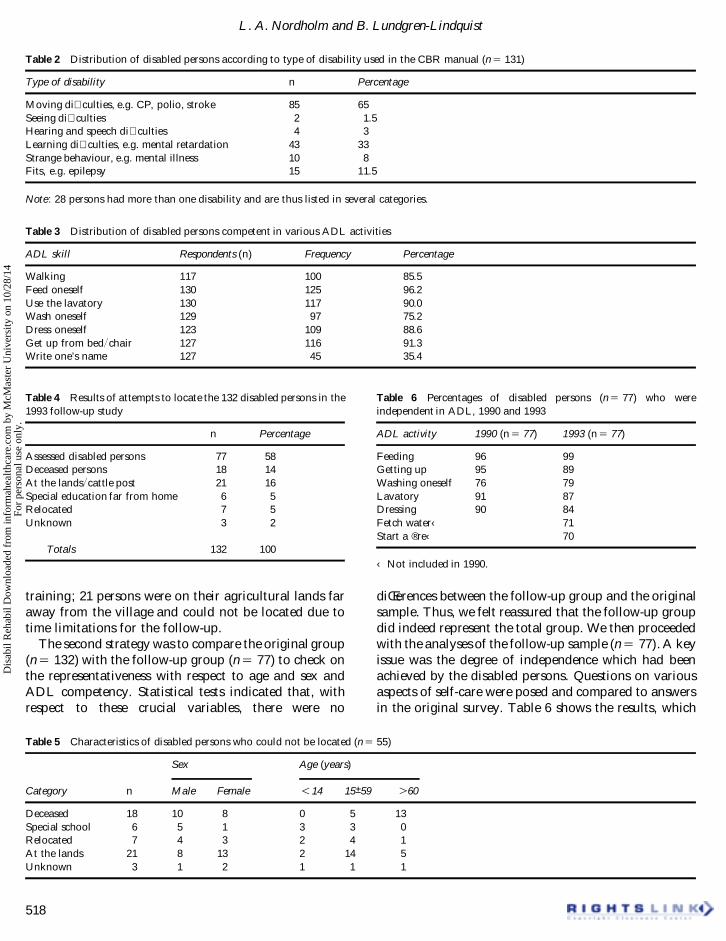
Disability
Approximately half of the group indicated that their
disability had been recognized in the ® rst year of life, and
46% had some idea of why it had occurred. Disability
was classi® ed according to the CBR manual (table 2). As
can be seen from this table, 65% of the group had
mobility di� culties. Mental retardation was the second
largest group (33%) while seeing, hearing and speech
di� culties were rare. Twenty-one per cent had more than
one disability and are thus listed in several categories in
the table.
Thirty per cent of the disabled persons had parents
who were related to one another; 34% received
treatment. A cross-tabulation of the two variables
schooling and treatment resulted in a signi® cant positive
association (higher percentage of individuals who had
schooling were receiving treatment). "
Activities of daily living (ADL)
Table 3 shows the distribution of disabled persons who
were competent in various ADL activities; this table
shows a high level of competency in these basic ADL
skills.
r e s u l t s o f t h e f o l l o w - u p o f t h e 132 d i s a b l e d
p e r s o n s
Table 4 gives a summary of the results of our attempts
to locate the 132 individuals: 58% of the group were
assessed at the follow-up. Since missing data can
invalidate a study we were concerned about the credi-
bility of our ® ndings. The ® rst strategy was to describe
the group that could not be assessed based on data from
the ® rst survey. These data are presented in table 5,
which shows that 18 persons were deceased and the
majority of the deceased persons were elderly. Of the six
persons in special schools, ® ve were in a school for
speech and hearing education and one in vocational
517
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
McM
aste
r U
nive
rsity
on
10/2
8/14
For
pers
onal
use
onl
y.
L. A. Nordholm and B. Lundgren-Lindquist
Table 2 Distribution of disabled persons according to type of disability used in the CBR manual (n 5 131)
Type of disability n Percentage
Moving di� culties, e.g. CP, polio, stroke 85 65
Seeing di� culties 2 1.5Hearing and speech di� culties 4 3
Learning di� culties, e.g. mental retardation 43 33
Strange behaviour, e.g. mental illness 10 8
Fits, e.g. epilepsy 15 11.5
Note: 28 persons had more than one disability and are thus listed in several categories.
Table 3 Distribution of disabled persons competent in various ADL activities
ADL skill Respondents (n) Frequency Percentage
Walking 117 100 85.5Feed oneself 130 125 96.2Use the lavatory 130 117 90.0Wash oneself 129 97 75.2Dress oneself 123 109 88.6Get up from bed} chair 127 116 91.3Write one’s name 127 45 35.4
Table 4 Results of attempts to locate the 132 disabled persons in the
1993 follow-up study
n Percentage
Assessed disabled persons 77 58
Deceased persons 18 14
At the lands} cattle post 21 16
Special education far from home 6 5
Relocated 7 5
Unknown 3 2
Totals 132 100
training; 21 persons were on their agricultural lands far
away from the village and could not be located due to
time limitations for the follow-up.
The second strategy was to compare the original group
(n 5 132) with the follow-up group (n 5 77) to check on
the representativeness with respect to age and sex and
ADL competency. Statistical tests indicated that, with
respect to these crucial variables, there were no
Table 5 Characteristics of disabled persons who could not be located (n 5 55)
Sex Age (years)
Category n Male Female ! 14 15± 59 " 60
Deceased 18 10 8 0 5 13
Special school 6 5 1 3 3 0
Relocated 7 4 3 2 4 1
At the lands 21 8 13 2 14 5
Unknown 3 1 2 1 1 1
Table 6 Percentages of disabled persons (n 5 77) who were
independent in ADL, 1990 and 1993
ADL activity 1990 (n 5 77) 1993 (n 5 77)
Feeding 96 99
Getting up 95 89
Washing oneself 76 79
Lavatory 91 87
Dressing 90 84
Fetch water‹ 71
Start a ® re‹ 70
‹ Not included in 1990.
diŒerences between the follow-up group and the original
sample. Thus, we felt reassured that the follow-up group
did indeed represent the total group. We then proceeded
with the analyses of the follow-up sample (n 5 77). A key
issue was the degree of independence which had been
achieved by the disabled persons. Questions on various
aspects of self-care were posed and compared to answers
in the original survey. Table 6 shows the results, which
518
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
McM
aste
r U
nive
rsity
on
10/2
8/14
For
pers
onal
use
onl
y.
CBR in Moshupa village, Botswana
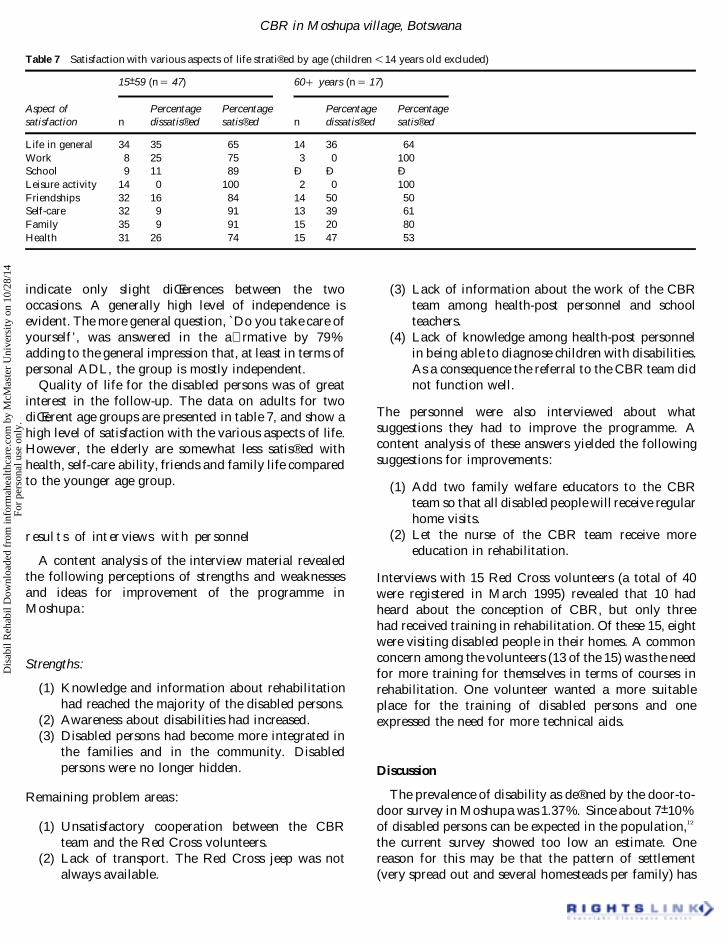
Table 7 Satisfaction with various aspects of life strati® ed by age (children ! 14 years old excluded)
15± 59 (n 5 47) 60 1 years (n 5 17)
Aspect of
satisfaction n
Percentage
dissatis® ed
Percentage
satis® ed n
Percentage
dissatis® ed
Percentage
satis® ed
Life in general 34 35 65 14 36 64
Work 8 25 75 3 0 100
School 9 11 89 Ð Ð Ð
Leisure activity 14 0 100 2 0 100
Friendships 32 16 84 14 50 50
Self-care 32 9 91 13 39 61
Family 35 9 91 15 20 80
Health 31 26 74 15 47 53
indicate only slight diŒerences between the two
occasions. A generally high level of independence is
evident. The more general question, `Do you take care of
yourself ’ , was answered in the a� rmative by 79%
adding to the general impression that, at least in terms of
personal ADL, the group is mostly independent.
Quality of life for the disabled persons was of great
interest in the follow-up. The data on adults for two
diŒerent age groups are presented in table 7, and show a
high level of satisfaction with the various aspects of life.
However, the elderly are somewhat less satis® ed with
health, self-care ability, friends and family life compared
to the younger age group.
r e s u l t s o f i n t e r v i e w s w i t h p e r s o n n e l
A content analysis of the interview material revealed
the following perceptions of strengths and weaknesses
and ideas for improvement of the programme in
Moshupa:
Strengths:
(1) Knowledge and information about rehabilitation
had reached the majority of the disabled persons.
(2) Awareness about disabilities had increased.
(3) Disabled persons had become more integrated in
the families and in the community. Disabled
persons were no longer hidden.
Remaining problem areas :
(1) Unsatisfactory cooperation between the CBR
team and the Red Cross volunteers.
(2) Lack of transport. The Red Cross jeep was not
always available.
(3) Lack of information about the work of the CBR
team among health-post personnel and school
teachers.
(4) Lack of knowledge among health-post personnel
in being able to diagnose children with disabilities.
As a consequence the referral to the CBR team did
not function well.
The personnel were also interviewed about what
suggestions they had to improve the programme. A
content analysis of these answers yielded the following
suggestions for improvements :
(1) Add two family welfare educators to the CBR
team so that all disabled people will receive regular
home visits.
(2) Let the nurse of the CBR team receive more
education in rehabilitation.
Interviews with 15 Red Cross volunteers (a total of 40
were registered in March 1995) revealed that 10 had
heard about the conception of CBR, but only three
had received training in rehabilitation. Of these 15, eight
were visiting disabled people in their homes. A common
concern among the volunteers (13 of the 15) was the need
for more training for themselves in terms of courses in
rehabilitation. One volunteer wanted a more suitable
place for the training of disabled persons and one
expressed the need for more technical aids.
Discussion
The prevalence of disability as de® ned by the door-to-
door survey in Moshupa was 1.37%. Since about 7± 10%
of disabled persons can be expected in the population," #
the current survey showed too low an estimate. One
reason for this may be that the pattern of settlement
(very spread out and several homesteads per family) has
519
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
McM
aste
r U
nive
rsity
on
10/2
8/14
For
pers
onal
use
onl
y.

L. A. Nordholm and B. Lundgren-Lindquist
contributed to the di� culty in identifying the disabled.
Another reason may be the greater ease with which a
mildly retarded individual is integrated in a rural
community.
Since children are overrepresented in the age dis-
tribution of developing countries (approximately 50%),
the ® nding that only 22% of the disabled were children
is surprising. Similarly surprising is the large proportion
of elderly disabled (10% were 75 years old or above).
The large average family size was expected and is
comparable with previous studies. * In countries where
birth control is not practised, and where children provide
valuable work on the land, and support for the parents
in their old age, women have many children. In this
society the mother is the centre of the family, since in
many cases the father is working away from home.
Women do most work on the land and in the family.
Women may choose not to marry, so as to keep the right
to their own property, wages, etc. ; women predominated
as caregivers, and single mothers were the largest group.
To be cared for in one’ s own home by a loving family
which can provide support and guidance has been
recognized as a major advantage of the CBR pro-
gramme. " $
The follow-up study produced several encouraging
results. First, many of the old disabled people were still
alive; 17% were 65 years or older. Given the generally
lower level of life expectancy for disabled persons, " % this
® nding was surprising. However, it must be noted that
the elderly people in our sample had not been born
disabled, but were suŒering from age-related functional
loss, e.g. loss of sight, hearing or mobility, and were thus
more similar to a `normal ’ old-age population.
Both at the time of the initial survey and at the follow-
up, the disabled persons had great competency in ADL
skills. There was no noticeable change between these two
occasions, but possibly the CBR programme has con-
tributed to the maintenance of competencies. In the
follow-up study two instrumental ADL activities were
added (fetching water and starting a ® re). In a rural
community these are important tasks of independent
living, which 70% of the group did manage. Many
clients lived in three-generation households and the
average number of the family group was seven persons.
This probably implies that the disabled person who
cannot manage ADL would receive help from family
members. By contrast, in industrialized countries many
persons live alone (36%) and face the threat of isolation
and loneliness." &
The CBR programme for children had promoted
integration into normal schools for physically disabled
children and referrals to special schools for those with
hearing and seeing disabilities. The follow-up study
showed that these recommendations had been followed
to a large extent. These result corroborate several
previous studies which have emphasized the bene® ts of
CBR to children. " # , " ’
The CBR programme for adults had attempted to ® nd
jobs for the adult disabled. Several other studies have
examined the proportion of disabled people in work as a
measure of CBR." # We found that 20% were working
despite di� culties about ® nding jobs in a rural area such
as Moshupa. Examples of employment were farming,
cattle, work in small shops or in the only petrol station.
Quality of life was a major concern in this study. With
a dichotomized (satis® ed vs dissatis® ed) scale we com-
pared older people (60 and over) with younger persons
(15± 59). Although the groups expressed similar levels of
satisfaction with life in general, older people were less
satis® ed with the aspects of friends, self-care, and health.
These results are understandable since dissatisfaction
with life among elderly people is often correlated with
disease, loneliness, widowhood, or ® nancial di� culties." (
The ® nding that older people were less satis® ed than
younger ones was further supported by answers to the
question : `How is your life today compared to three
years ago? ’ While a majority (60%) of younger persons
judged it better, and only 16% judged it worse, 80% of
the older people found it worse and only 7% better. This
® nding is probably correlated to opportunities for work
and involvement in community life, in which younger
people are likely to be engaged.
Comparisons between men and women yielded only
one signi® cant result. A greater proportion of males were
satis® ed with friends. This may re¯ ect a cultural pattern
in rural South Africa where women do most of the work
on ® elds and around the home and men can often be seen
sitting around with other men. " )
Most of the data in the present project are quantitative
except for the interviews with personnel. Although there
are obvious di� culties with carrying out interviews with
the help of interpreters, the need for qualitative data of
good quality is obvious. This point was made by
Finken¯ ugel et al.," * who emphasized the need for
process-oriented data and development of qualitative
research in CBR.
When evaluating the CBR programme in Botswana it
is obvious that it has indeed been a component of
community development in the spirit of the WHO
approach. The programme has many volunteers who,
despite insu� cient training, still try to ful® l the goals of
CBR to the best of their ability. Most volunteers
expressed the need for more training in CBR, thus
substantiating the view elaborated by Hale and Wallner# !
520
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
McM
aste
r U
nive
rsity
on
10/2
8/14
For
pers
onal
use
onl
y.

CBR in Moshupa village, Botswana
that CBR workers need to be trained in greater numbers
to provide acceptable standards of service. Clients cannot
be left without some continued support such as home
visits. If rehabilitation workers do not provide such
services for at least some minimum of time after the
initiation of the CBR programme, the programme is not
likely to survive. The Rehabilitation Committee also has
an important function. In Moshupa village a Rehabili-
tation Committee has been formed, which works for self-
determination and social integration of disabled people.
The committee has organized fund-raising and social
events in the village.
While the government at the national level has
recognized its responsibility for the disabled in the
National Development Plan, there are as yet insu� cient
support structures at the intermediate level. Support
personnel such as physiotherapists and occupational
therapists are needed to advise, train and supervise
rehabilitation personnel. The role of physiotherapists in
this context has been discussed by Kay et al.# " They point
out that physiotherapists are currently under-utilized,
and suggest that physiotherapists achieve an elevated
and more independent role in areas of management,
assessment and treatment. This proposed role within the
medical domain should include out-reach and edu-
cational programmes at the local level. A similar role
would be equally appropriate to other categories of
rehabilitation workers such as occupational therapists.
Finally, we would like to suggest that CBR has
important implications not only for developing
countries, but also for the rest of the world. Many
industrialized countries are experiencing great strain on
® nancial resources for health care, and governments are
cutting back funds. This, in association with an ageing
population and the increasing demands on health care
for the aged, may give impetus to establishment of more
CBR programmes in the near future.
References
1 Lundgren-Lindquist B, Nordholm LA. Community-based rehabili-tation ± a survey of disabled in a village in Botswana. Disability andRehabilitation 1993; 15 : 83± 89.
2 Lundgren-Lindquist B, Nordholm LA. The impact of community-based rehabilitation as perceived by disabled people in a village inBotswana. Disability and Rehabilitation 1996; 18 : 329± 334.
3 Utter BW, Al Helo HY. Community-based rehabilitation inMoshupa, Botswana Ð a follow-up study. Go$ teborg College ofHealth Sciences, Go$ teborg, Sweden, 1995 (unpublished manu-script).
4 World Programme of Action Concerning Disabled Persons. UnitedNations Document A } 37} 51. New York: United Nations, 1983.
5 United Nations. Standard rules on the equalizationof opportunitiesfor disabled persons. Vienna: United Nations, 1992 AHWG}SRDP} 3 } 4.
6 Helander E. Prejudice and Dignity: An Introduction to Community-Based Rehabilitation. New York: UN Development Programme,1993.
7 Advani L. Is community based rehabilitation the answer for everydisabled person? Indian Journal of Disability and Rehabilitation1993; 7 : 71± 73.
8 Jo$ nsson T. OMAR in Rehabilitation. A Guide on Operations,Monitoring, and Analysis of Results. New York: UNOP, 1994.
9 Finnstam J, Grimby G, Nelson G, Rashio S. Evaluation ofcommunity-based rehabilitation in Punjab, Pakistan. I : Use of theWHO manual, training disabled people in the community.International Disability Studies 1988; 10 : 54± 58.
10 Rottier MJN, Broer RW, Vermeer A, Finken¯ ugel HJM. A studyof follow up of clients in community-based rehabilitation projectsin Zimbabwe: the functioning of rehabilitation technicians, localsupervisors and caregivers. Journal of RehabilitationSciences 1993;6 : 35± 41.
11 Mariga L, McConkey R. Home-based learning programmes formentally handicapped people in rural areas of Zimbabwe. Inter-national Journal of Rehabilitation Research 1987; 10 : 175± 183.
12 Lagerkvist B. Rehabilitation in practice: community-based re-habilitation outcome for the disabled in the Philippines andZimbabwe. Disability and Rehabilitation 1992; 14 : 44± 50.
13 Freeman EA. Community-based rehabilitationof the person with asevere brain injury. Brain Injury 1997; 11 : 143± 153.
14 Haber LD, Dowd JE. A Human DevelopmentAgenda for Disability:statistical considerations. New York: United Nations. StatisticalDivision, 1994.
15 Perspektiv pa/ va$ lfa$ rden 1987. Levnadsfo$ ha/ llanden nr 53.Stockholm: Statistiska Centralbyra/ n, 1987.
16 O’Toole B. Development and evaluation of a community-basedrehabilitation programme for pre-school disabled children inGuyana. Georgetown, Guyana: University of Guyana, 1989.
17 Grimby A, Wiklund I. Health-related quality of life in old age. Astudy among 76-year-old Swedish urban citizens. ScandinavianJournal of Social Medicine, 1994; 22 : 7± 14.
18 Concha ME, Lerenco T. The prevalence of disability in a rural areaof South Africa-Gazankulu. Paper presented at the EuropeanCongress of Occupational Therapy, Portugal, 1988.
19 Finken¯ ugel HJM, Van Maanen V, Schut W, Vermeer A, Jelsma J,Moyo A. Appreciation of community-based rehabilitationby care-givers of children with a disability. Disability and Rehabilitation1996; 18 : 255± 260.
20 Hale LA, Wallner PJ. The challenge of service provision in SouthAfrica for patients with hemiplegia. Physiotherapy 1996; 82 :156± 158.
21 Kay E, Kilonzo C, Harris MJ. Improving rehabilitation services indeveloping nations: the proposed role of physiotherapists. Physio-therapy 1994; 80 : 77± 82.
521
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
McM
aste
r U
nive
rsity
on
10/2
8/14
For
pers
onal
use
onl
y.