comorbidity of auditory processing, language, and reading ......comorbidity of auditory processing,...
TRANSCRIPT

Comorbidity of Auditory Processing,Language, and Reading Disorders
Purpose: The authors assessed comorbidity of auditory processing disorder (APD),language impairment ( LI), and reading disorder (RD) in school-age children.Method: Children (N = 68) with suspected APD and nonverbal IQ standard scores of80 or more were assessed using auditory, language, reading, attention, and memorymeasures. Auditory processing tests included the Frequency Pattern Test (FPT; F. E.Musiek, 1994; D. Noffsinger, R. H. Wilson, & F. E. Musiek, 1994); the DichoticDigit Test Version 2 (DDT; F. E. Musiek, 1983); the RandomGap Detection Test (R.W.Keith, 2000); the 500-Hz tone Masking Level Difference (V. Aithal, A. Yonovitz, &S. Aithal, 2006); and a monaural low-redundancy speech test (compressed andreverberant words; A. Boothroyd & S. Nittrouer, 1988). The Clinical Evaluation ofLanguage Fundamentals, Fourth Edition (E. Semel, E. Wiig, &W. Secord, 2003) wasused to assess language abilities (including auditory memory). Reading accuracy andfluency and phonological awareness abilities were assessed using the WheldallAssessment of Reading Passages (A. Madelaine & K. Wheldall, 2002) and theQueensland University Inventory of Literacy (B. Dodd, A. Holm, M. Orelemans, &M. McCormick, 1996). Attention was measured using the Integrated Visual andAuditory Continuous Performance Test (J. A. Sandford & A. Turner, 1995).Results:Of the children, 72% had APD on the basis of these test results. Most of thesechildren (25%) had difficulty with the FPT bilaterally. A further 22% had difficulty withthe FPT bilaterally and had right ear deficits for the DDT. About half of the children(47%) had problems in all 3 areas (APD, LI, and RD); these children had the poorestFPT scores. More had APD–RD, or APD–LI, than APD, RD, or LI alone. There weremodest correlations between FPT scores and attention and memory, and between DDTscores and memory.Conclusions: LI and RD commonly co-occur with APD. Attention and memory arelinked to performance on some auditory processing tasks but only explain a smallamount of the variance in scores. Comprehensive assessment across a range of areasis required to characterize the difficulties experienced by children with APD.
KEY WORDS: auditory processing disorder, language processing disorder,reading disorder, Children’s Auditory Processing Performance Scale (CHAPPS),attention, memory
S ome school-age children appear to have hearing difficulties, despitehaving normal hearing sensitivity. Teachers and parents describethem as children who are distracted by background sounds, do not
follow multiple instructions, take longer to comprehend simple auditorydirections, occasionally misconstrue what is being said, or appear to have“selective” hearing (Benson, Seaton, & Johnson, 1997). Anecdotally, itappears that these children could be diagnosed as having an auditoryprocessing disorder (APD), a language impairment (LI), or attentiondeficits, depending on which professional first assesses the child.
APD has been defined by the American Speech-Language-HearingAssociation (ASHA)TaskForce onCentral Auditory ProcessingConsensus
Mridula SharmaSuzanne C. Purdy
Macquarie University, Sydney, Australia, andUniversity of Auckland, New Zealand
Andrea S. KellyUniversity of Auckland
Journal of Speech, Language, and Hearing Research • Vol. 52 • 706–722 • June 2009 • D American Speech-Language-Hearing Association1092-4388/09/5203-0706
706

Development (1996) as problems in one or more of thefollowing auditory behaviors: sound localization and lat-eralization, auditory discrimination, auditory patternrecognition, temporal aspects of audition, and auditoryperformance decrements with competing acoustic signalsand degraded acoustic signals. Because of the complexityof auditory processing and the heterogeneity of APD, theASHA Task Force on Central Auditory Processing Con-sensus Development (1996) recommended that clinicaltests for APD include temporal processing, localizationand lateralization, perception of low-redundancy mon-aural speech, dichotic listening, and binaural interaction.
The technical report of the ASHAWorking Group onAuditoryProcessingDisorders (2005) suggests thatAPDcan coexist with other disorders, such as LI and learningdisability. LI has been defined as significantly poor lan-guage (receptive or expressive) when intelligence andhearing sensitivity are within normal limits, and thereare no other physical or emotional difficulties (Bishop,1992). Definitions of LI vary; however, they are typicallybased on a discrepancy between receptive and/or expres-sive language andnonverbal IQ,whennonverbal IQ scoresare within the normal range (Bishop, Bishop, et al., 1999;Kamhi, 1998; Weismer et al., 2000). Although there isevidence that LI can coexist with APD (e.g., Benasich,Thomas, & Leppanen, 2002;McArthur&Bishop, 2004a,2004b; Tallal & Stark, 1981; Wible, Nicol, & Kraus, 2005),this has been questioned by some authors (e.g., Bishop,Carlyton, Deeks, & Bishop, 1999; Helzer, Champlin, &Gillam, 1996; Rosen, 1999). The Bishop et al. (1999)and Rosen (1999) studies found no difficulty on auditorytasks in children with specific LI.
Similarly disparate results have been found forchildren with reading disorder (RD). Children with RDhave problems with written language in the presence ofaverage nonverbal intelligence and having received ad-equate instruction to acquire written and spoken lan-guage (McArthur & Bishop, 2001). A number of studieshave found that some children with RD have audi-tory processing deficits (Ahissar, Protopapas, Reid, &Merzenich, 2000; Amitay, Ahissar, & Nelken, 2002;Heiervang, Stevenson, & Hugdahl, 2002; Rosen &Manganari, 2001; Sharma et al., 2006), whereas othershave questioned whether children with RD have audi-tory difficulties (McAnally&Stein, 1996; Schulte-Körne,Deimel, Bartling, & Remschmidt, 1998). The literatureis rife with research investigating causes of RD. Muchof this work has focused on the link between temporalauditory processing and RD (for a review, see Ramuset al., 2003). These studies have used a range of tasks,such as backward masking, gap detection, and auditorypitch discrimination (Rosen, 2003). Ramus et al. (2003)concluded that a percentage of children with RD do havedifficulties on auditory processing tasks. Only a fewstudies in the reading literature (Bishop, Carlyton, et al.,
1999; King, Lombardino, Crandell, & Leonard, 2003;Watson & Miller, 1993) have used a range of auditoryprocessing measures to assess children with reading orlanguage problems (McArthur&Bishop, 2001). Of thesestudies, only King et al. (2003) used tests recommendedfor APD diagnosis by the ASHATask Force on CentralAuditory Processing Consensus Development (1996).
The current study investigated the reading and lan-guage status of school-age children diagnosed with APDon the basis of the results of a range of APD assessmentsto determine (a) whether children with a clinical diag-nosis of APD have coexisting reading and/or languagedisorder and (b) whether different types of auditoryprocessing difficulties are associated with reading and/orlanguage disorders.
Reading and language disorders have been reportedas simultaneously present in some children (Anderson,Brown, & Tallal, 1993; Bishop, 2001; Snowling, Bishop,& Stothard, 2000). However, at least some children withLI demonstrate age-appropriate reading abilities (Bishop& Adams, 1990; Catts, 1993). Richard (2007, p. 400) re-ferred to an “auditory processing continuum” whereby(central) auditory, phonemic, and language processingare regarded as the primary differential aspects, withAPD occurring in isolation or in combination with otherdisorders. Phonemic awareness is the ability to isolateandmanipulate subsyllabic sounds, and it is regarded asa component of phonological awareness (Scholes, 1998).
People with auditory, language processing, and/orRDs are heterogeneous (Aram & Nation, 1980; Bellis,2007, p. 127; Ramus et al., 2003; Reed & Baker, 2005,p. 85), and there is some existing evidence for comorbidity(King et al., 2003;M.M.Walker, Shinn, Cranford,Givens,& Holbert, 2002). Few studies have conducted compre-hensive evaluations of awide range of auditory, language,and reading skills in the same group of children, andhence the overlap between deficits in these areas is notclear. The aim of the current study was to determine thepercentage of children with APD who have coexistinglanguageand/orRD, and to characterize thenature of theauditory processing difficulties in childrenwith languageand/or reading difficulties. The link between auditoryprocessing, sustained attention, and short-term auditorymemory was also investigated.
MethodParticipants
Sixty-eight children 7–12 years of age participated.Children had either (a) APD suspected by teachers and/or parents or (b) a diagnosis of APD by an audiologist,a speech-language therapist, or an educational psycholo-gist. Childrenwho agreed to participatewere screened to
Sharma et al.: Comorbidity of APD, LI, and RD 707

ensure that (a) they hadType-A tympanograms, (b) theirnonverbal intelligence scorewas 80 or higher on the Testof Nonverbal Intelligence (TONI-3; Brown, Sherbenou,& Johnsen, 1997), and (c) their pure-tone hearing thresh-olds were 15 dB HL or better.
Participants included 44 boys (65%) and 24 girls(35%). Average age was 9.8 and 9.7 years for boys andgirls, respectively (SD = 1.6; range = 7.0, 12.8). In gen-eral, none of the children had any formal prior diag-noses other than APD (n = 9; 13%) and, in some cases,RD (n = 20; 29%). A small number of children had otherdiagnoses, such as dyspraxia (n = 3; 4%), Asperger ’ssyndrome (n = 2; 3%), attention-deficit/hyperactivitydisorder–attention deficit disorder (n = 4; 6%), or tin-nitus (n = 1; 1%). Parents of some children reportedspeech and language concerns; however, none of thechildren had a formal diagnosis of speech or LI.
Ten children (15%) who participated because of pa-rental concern had no formal diagnosis. At the time oftheir participation in the study, none of the childrenwere undergoing any treatment for language or readingdifficulties, and none were using any form of classroomamplification or personal frequency modulated devices.Nearly half of the children participating in the study hada prior history of multiple middle ear infections (49%),and at least 43% had another familymember—such as aparent, sibling, or first cousin—who had a diagnosis ofAsperger’s syndrome, autism, APD, attention-deficit/hyperactivity disorder–attention deficit disorder, orreading/learning disorder.
Handedness was informally measured by offering apen/pencil and asking the children to write their nameon a piece of paper. The childrenwere also askedwhetherthey always or sometimes used the same hand for alltasks, such as sports. Seven children (10%) were classedas having mixed handedness, as they used differenthands and feet for different tasks. Ten children were lefthanded (15%).
ProcedurePeripheral hearing was tested using pure-tone,
speech, and immittance audiometry, as well as transientclick-evoked otoacoustic emissions (OAEs). All partici-pants had (a) pure-tone thresholds of 15 dBHL or betterat octave frequencies ranging from 250 Hz to 8000 Hz,(b) Type-A tympanograms (Jerger, 1970), (c) ipsilateral1000-Hz acoustic reflex thresholds less than 100 dB HL(Silman & Gelfand, 1981), (d) left and right ear CVCphoneme scores of 90% or better for speech presented inquiet (Boothroyd&Nittrouer, 1988), and (e) OAE strengthwithin the normal range on the basis of the pass/refercriteria in the transient evoked OAE protocols of theScout Sport System (Bio-Logic Systems Corporation,
Mundelein, IL) thatwere adopted fromHall (2000). If allmeasures of peripheral hearing were normal, partici-pants proceeded to the psycho-educational, language,hearing, and auditory processing test battery (see de-scription of tests in Table 1). The tasks were under-taken in four sessions, each approximately 2 hr in length.Session durationwas reducedwhen the child’s attentionandmotivationwere problematic. A few children requiredan additional 1–2 test sessions.
Case HistoryParents completed a case history providing details
of birth history, early speech and language milestones,as well as language and reading progress to the time ofparticipation in the study. Parents also completed theChildren’s Auditory Processing Performance Scale(CHAPPS) questionnaire developed by Smoski, Brunt,and Tannahill (1998). The CHAPPS has 36 items con-cerning listening behavior in a variety of listening con-ditions and functions. Children are rated on a 7-pointscale ranging from –5 (cannot function at all) to 1 (lessdifficulty than peers) on items relating auditorymemory/sequencing and attention and listening to speech innoise, in quiet, in ideal conditions, and with multiple in-puts. CHAPPS questionnaire results were comparedwith findings for the APD test battery; however, thediagnosis of APD was not based on CHAPPS scores.
Auditory Processing Test BatteryFive behavioral tests were used to test a range of au-
ditory processes: (a) Dichotic Digit Test Version 2 (DDT-2;Musiek, 1983), (b) Frequency Pattern Test (FPT;Musiek,1994; Noffsinger, Wilson, & Musiek, 1994), (c) RandomGap Detection Test (RGDT; Keith, 2000), (d) compressed(45%) and reverberant (0.3-s) CVC words (Boothroyd &Nittrouer, 1988), and (e) 500-Hz toneMasking Level Dif-ference (MLD; Aithal, Yonovitz, & Aithal, 2006). Pure-tone audiometry andbehavioral auditory processing testswere administered using a Grason-Stadler (Milford,NH) clinical audiometer and TDH-39 earphones (Tucker-Davis Technologies, Alachua, FL). Test materials werepresented at 60 dBHL using a CD player (BassXPander,P882). For FPTandmonaural low-redundancy tests, stim-uli to right and left ears were presented separately, withstarting ear randomized. For DDTs and RGDTs, rightand left ears were tested simultaneously. The FPT andDDT scores were considered to be a “pass” if the scoreswere within 2SDs of themean for the normative sample(for norms, see Kelly, 2007). For the RGDT, a gap de-tection threshold of 20 ms or lower was regarded as apass (Keith, 2000). Compressedand reverberant speechscores were comparedwith locally developed norms (Kelly,
708 Journal of Speech, Language, and Hearing Research • Vol. 52 • 706–722 • June 2009
2007), and scores more than 2 SDs on two tests or 3 SDsbelow the mean for one test were regarded as abnormal(ASHA Working Group on Auditory Processing Disor-ders, 2005).
The MLD is the difference in threshold of the signal(in dB) for the case inwhich the signal and the noise havethe same phase and level relationships at the two ears,and the case in which the interaural phase and/or levelrelationships of the signal and noise are different. TheMLD is ameasure of the improvement in detectability ofa signal that normally occurs under binaural listeningconditions. For theMLD task, an 11-dBor greater 500-Hzthreshold difference between the SPN0 (tone presentedto the two ears in opposite phase, noise presented in thesame phase) and S0N0 (tone and noise presented to the
two ears in the same phase) conditions was regarded asnormal (Aithal et al., 2006). Diagnosis of APDwas basedon FPT, DDT, RGDT, MLD, and/or compressed and re-verberant speech scores.
Cognition and LanguageThe TONI-3 measures the child’s reasoning ability
with minimum language influence (Brown et al., 1997).It is a norm-referenced measure of cognitive ability thatassesses intelligence aptitude, abstract thinking, andproblem solving for individuals 6–89 years of age. Foreach item, the child selected one of six options to com-plete the pattern. In the current study, the lower cutofffor nonverbal intelligence scores of 80 was selected on
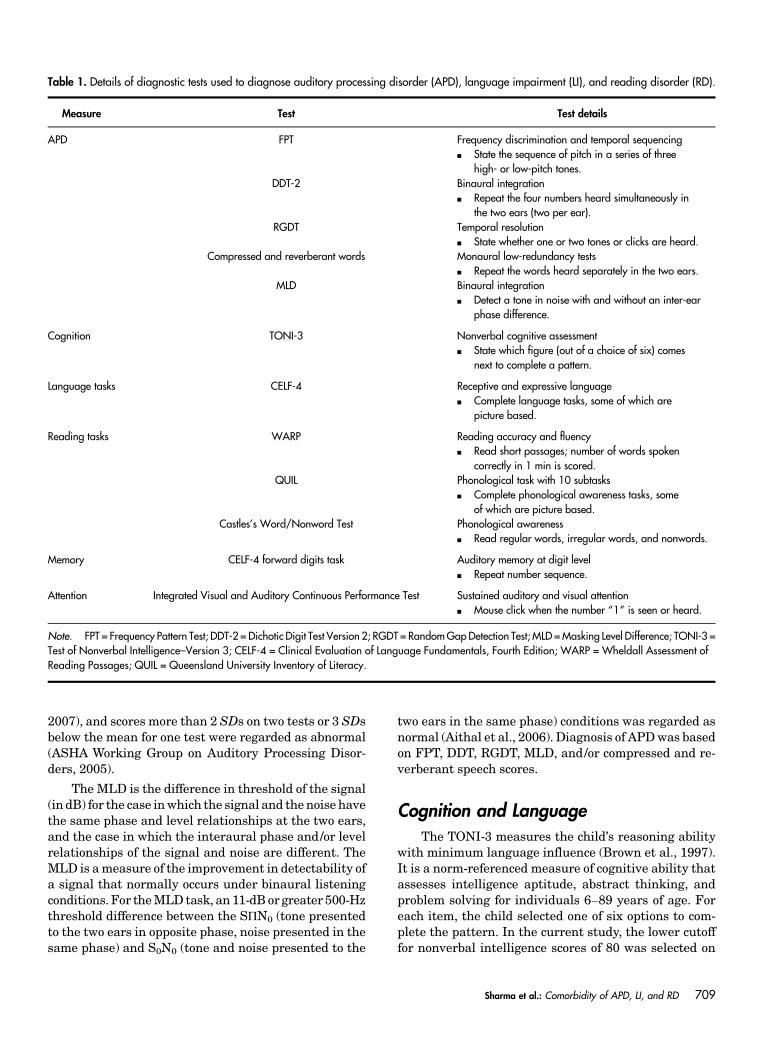
Table 1. Details of diagnostic tests used to diagnose auditory processing disorder (APD), language impairment (LI), and reading disorder (RD).
Measure Test Test details
APD FPT Frequency discrimination and temporal sequencingh State the sequence of pitch in a series of three
high- or low-pitch tones.DDT-2 Binaural integration
h Repeat the four numbers heard simultaneously inthe two ears (two per ear).
RGDT Temporal resolutionh State whether one or two tones or clicks are heard.
Compressed and reverberant words Monaural low-redundancy testsh Repeat the words heard separately in the two ears.
MLD Binaural integrationh Detect a tone in noise with and without an inter-ear
phase difference.
Cognition TONI-3 Nonverbal cognitive assessmenth State which figure (out of a choice of six) comes
next to complete a pattern.
Language tasks CELF-4 Receptive and expressive languageh Complete language tasks, some of which are
picture based.
Reading tasks WARP Reading accuracy and fluencyh Read short passages; number of words spoken
correctly in 1 min is scored.QUIL Phonological task with 10 subtasks
h Complete phonological awareness tasks, someof which are picture based.
Castles’s Word/Nonword Test Phonological awarenessh Read regular words, irregular words, and nonwords.
Memory CELF-4 forward digits task Auditory memory at digit levelh Repeat number sequence.
Attention Integrated Visual and Auditory Continuous Performance Test Sustained auditory and visual attentionh Mouse click when the number “1” is seen or heard.
Note. FPT = Frequency Pattern Test; DDT-2 = Dichotic Digit Test Version 2; RGDT = RandomGapDetection Test; MLD =Masking Level Difference; TONI-3 =Test of Nonverbal Intelligence–Version 3; CELF-4 = Clinical Evaluation of Language Fundamentals, Fourth Edition; WARP = Wheldall Assessment ofReading Passages; QUIL = Queensland University Inventory of Literacy.
Sharma et al.: Comorbidity of APD, LI, and RD 709

the basis of Fey, Long, and Cleave’s (1994) finding thatgains in grammatical skills made by children with thescores of 70–84 were comparable with those meeting anonverbal IQ criterion of 85 and above.
The Clinical Evaluation of Language Fundamen-tals, Fourth Edition (CELF-4; Semel, Wiig, & Secord,2003) was used to assess children’s receptive and ex-pressive language scores. The receptive language scoreis a cumulative score from subtests such asConcepts andFollowing Directions, and Receptive Word Classes (se-mantic relationships). The expressive language score isthe cumulative score from subtests such as FormulatingSentences, Recalling Sentences, and Expressive WordClasses.
Reading and Phonological TasksChildren were tested using (a) the Wheldall Assess-
ment of ReadingPassages (WARP;Madelaine&Wheldall,2002), which measures reading fluency and accuracy, and(b) theCastles’sWord/NonwordTest (Castles&Coltheart,1993), which measures reading accuracy for regular/irregular words and nonwords. WARP and Word/Nonword Test norms were adopted from Madelaineand Wheldall (2002) and Edwards and Hogben (1999),respectively.
The Queensland University Inventory of Literacy(QUIL; Dodd, Holm, Orelemans, & McCormick, 1996) isa phonological awareness assessment that has been stan-dardized on Australian schoolchildren 2–7 years of age.The QUIL has the following 10 subtasks: (a) reading ofnonwords, (b) spelling of nonwords (e.g., lont, sheve, etc.),(c) segmentation of syllables (to determine the number ofsyllables in a given word), (d) identification of syllables,(e) visual rhyming, (f ) auditory rhyming (judgment ofpairs of words, such as “shell” and “bell” or “bout” and“bait”), (g) spoonerisms (swapping the first sound froma pair of words and making new words, such as “felt”and “make” swapped to “melt” and “fake”), (h) pho-neme detection (identifying the odd word out, whichmay be different because of first /second or third sound),(i) phoneme segmentation, and ( j) phoneme manip-ulation (identify and remove a sound from the givenword and then say the word; e.g., “frog” without “r” is“fog”).
Auditory MemoryAuditory memory was measured using the CELF-4
forward digits task. The task requires the child to recallnumbers in correct serial order after hearing the num-bers. The numbers are spoken slowly in a monotonevoice, and the child is asked to repeat them in the exactorder. The length of the series keeps increasing until thechild can no longer repeat the series in the correct order.
Sustained Attention: Auditory and VisualChildren were tested on the Integrated Visual and
Auditory Continuous Performance Test (Sandford &Turner, 1995), which assesses the children’s performanceon a combined visual and auditory task. The test was pre-sented on a laptop computer, and the childwas instructedto click the mouse whenever the number 1 was seen orheard and to ignore the number 2. Numbers 1 and 2were seen andheard in pseudorandomorder. Therewere500 trials, and the task took about 15 min to complete.Feedback was provided only during practice trials.
ResultsAPD
On the basis of the clinical test battery and thecriterion of APD scores falling 2 SDs below the mean ontwo tests, or 3 SDs below the mean on any one test(ASHA Working Group on Auditory Processing Disor-ders, 2005), 49 children (72%) were diagnosed as havingAPD. CHAPPS questionnaires were completed by 65parents. Smoski et al. (1998) suggested that CHAPPSratings less than –11 indicate that a child is “at risk” foran auditory processing problem, on the basis of summedratings across the 36 items in the questionnaire. On av-erage, CHAPPS scores were –10.4 (SD = 5.4; range =–21.3, 2.3), and only 43% of the children (n = 29) whoseparents had completed the questionnaire met thecriterion of scores less than –11, indicating that theirchild may be at risk of APD. Twenty-five children (37%)were identified with APD by both the questionnaire andthe test battery. Twenty-two children with APD did nothave CHAPPS scores less than –11 and, hence, wouldhave beenmissed if diagnosiswas based on the CHAPPS.Four children were identified as being at risk for APD onthebasis of theCHAPPSbut passed theAPD test battery.Of these children, 3 had RD and/or LI but did not meetcriteria for APD. These findings do not support the use ofthe CHAPPS as a screening or diagnostic tool for APDbecause many children with APD were not identified onthe basis of their CHAPPS scores, and some were incor-rectly identified. The CHAPPS questionnairemay still bea valuable component of the case history, however, forchildren with suspected APD because it highlights areasof difficulty in the classroom and, hence, could be used toguide intervention in combinationwith other test findings.
None of the children showed significant difficultieson the compressed and reverberant speech task; however,the scores for this test indicate that it was quite an easytask. Average scores for right and left ears were 88.8%(SD = 7.1; range = 66%, 100%) and 88.3% (SD = 6.6;range = 62%, 100%), respectively. Although none of thechildren were below the norm on this task, a repeated
710 Journal of Speech, Language, and Hearing Research • Vol. 52 • 706–722 • June 2009
measures analysis of variance—with test ear and noisecondition asmain effects and age as a covariate—showeda significant decline in phoneme scores, F(1, 66) = 14.4,p < .001, for the distorted speech condition comparedwith the nondistorted speech condition. As expected,speech scores were also affected by participant age,F(1, 66) = 4.1, p = .047.
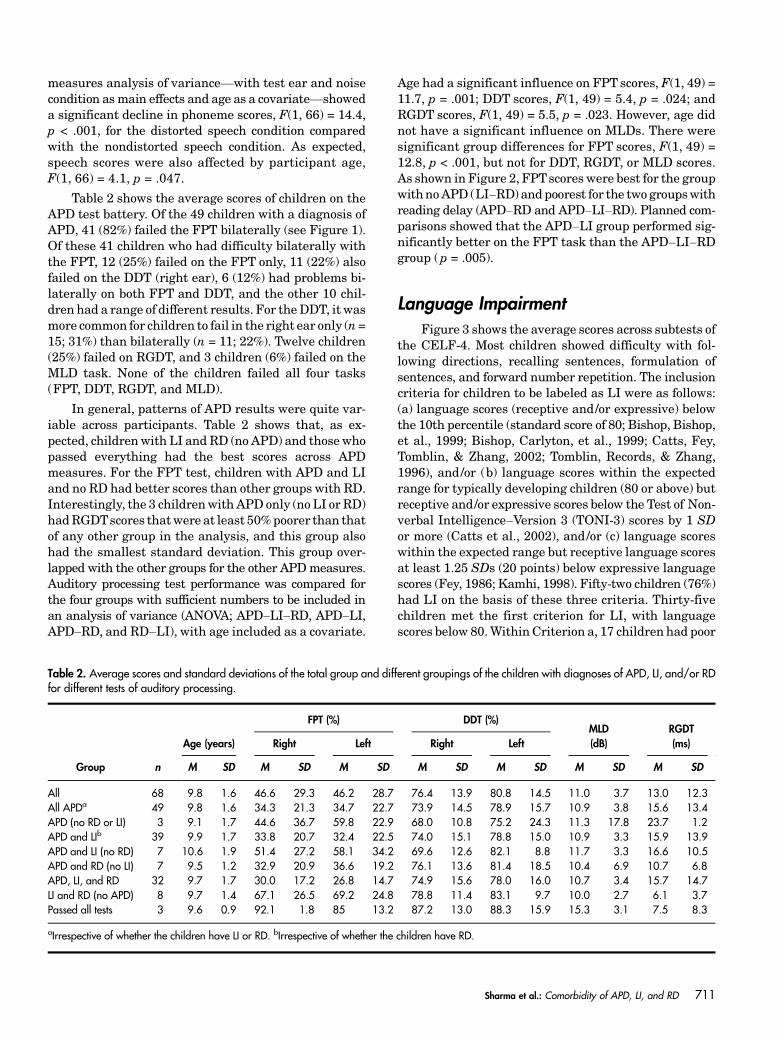
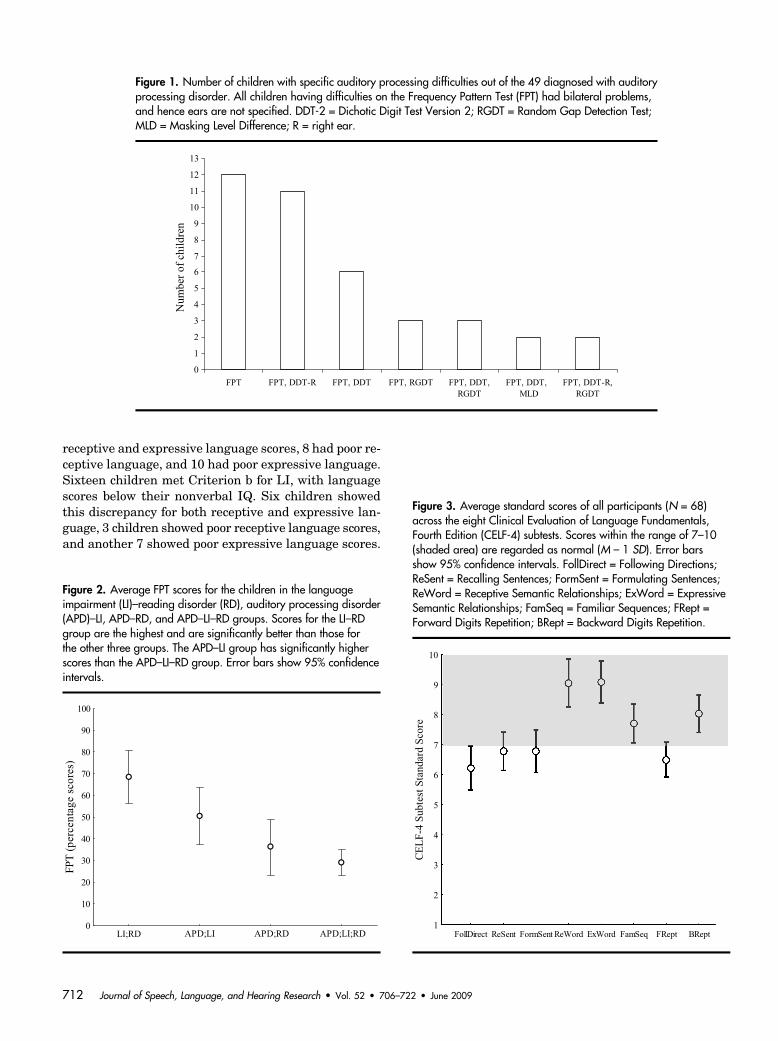
Table 2 shows the average scores of children on theAPD test battery. Of the 49 children with a diagnosis ofAPD, 41 (82%) failed the FPT bilaterally (see Figure 1).Of these 41 children who had difficulty bilaterally withthe FPT, 12 (25%) failed on the FPT only, 11 (22%) alsofailed on the DDT (right ear), 6 (12%) had problems bi-laterally on both FPT and DDT, and the other 10 chil-dren had a range of different results. For theDDT, it wasmore common for children to fail in the right ear only (n=15; 31%) than bilaterally (n = 11; 22%). Twelve children(25%) failed on RGDT, and 3 children (6%) failed on theMLD task. None of the children failed all four tasks(FPT, DDT, RGDT, and MLD).
In general, patterns of APD results were quite var-iable across participants. Table 2 shows that, as ex-pected, childrenwith LI and RD (no APD) and those whopassed everything had the best scores across APDmeasures. For the FPT test, children with APD and LIand no RD had better scores than other groups with RD.Interestingly, the 3 childrenwith APD only (no LI or RD)hadRGDTscores thatwere at least 50%poorer than thatof any other group in the analysis, and this group alsohad the smallest standard deviation. This group over-lapped with the other groups for the other APDmeasures.Auditory processing test performance was compared forthe four groups with sufficient numbers to be included inan analysis of variance (ANOVA; APD–LI–RD, APD–LI,APD–RD, and RD–LI), with age included as a covariate.
Age had a significant influence on FPT scores, F(1, 49) =11.7, p = .001; DDT scores, F(1, 49) = 5.4, p = .024; andRGDT scores, F(1, 49) = 5.5, p = .023. However, age didnot have a significant influence on MLDs. There weresignificant group differences for FPT scores, F(1, 49) =12.8, p < .001, but not for DDT, RGDT, or MLD scores.As shown in Figure 2, FPTscores were best for the groupwithnoAPD (LI–RD) andpoorest for the two groupswithreading delay (APD–RD and APD–LI–RD). Planned com-parisons showed that the APD–LI group performed sig-nificantly better on the FPT task than the APD–LI–RDgroup (p = .005).
Language ImpairmentFigure 3 shows the average scores across subtests of
the CELF-4. Most children showed difficulty with fol-lowing directions, recalling sentences, formulation ofsentences, and forward number repetition. The inclusioncriteria for children to be labeled as LI were as follows:(a) language scores (receptive and/or expressive) belowthe 10th percentile (standard score of 80; Bishop, Bishop,et al., 1999; Bishop, Carlyton, et al., 1999; Catts, Fey,Tomblin, & Zhang, 2002; Tomblin, Records, & Zhang,1996), and/or (b) language scores within the expectedrange for typically developing children (80 or above) butreceptive and/or expressive scores below the Test of Non-verbal Intelligence–Version 3 (TONI-3) scores by 1 SDor more (Catts et al., 2002), and/or (c) language scoreswithin the expected range but receptive language scoresat least 1.25 SDs (20 points) below expressive languagescores (Fey, 1986; Kamhi, 1998). Fifty-two children (76%)had LI on the basis of these three criteria. Thirty-fivechildren met the first criterion for LI, with languagescores below 80.Within Criterion a, 17 children had poor
Table 2. Average scores and standard deviations of the total group and different groupings of the children with diagnoses of APD, LI, and/or RDfor different tests of auditory processing.
Group n
Age (years)
FPT (%) DDT (%)MLD(dB)
RGDT(ms)Right Left Right Left
M SD M SD M SD M SD M SD M SD M SD
All 68 9.8 1.6 46.6 29.3 46.2 28.7 76.4 13.9 80.8 14.5 11.0 3.7 13.0 12.3All APDa 49 9.8 1.6 34.3 21.3 34.7 22.7 73.9 14.5 78.9 15.7 10.9 3.8 15.6 13.4APD (no RD or LI) 3 9.1 1.7 44.6 36.7 59.8 22.9 68.0 10.8 75.2 24.3 11.3 17.8 23.7 1.2APD and LIb 39 9.9 1.7 33.8 20.7 32.4 22.5 74.0 15.1 78.8 15.0 10.9 3.3 15.9 13.9APD and LI (no RD) 7 10.6 1.9 51.4 27.2 58.1 34.2 69.6 12.6 82.1 8.8 11.7 3.3 16.6 10.5APD and RD (no LI) 7 9.5 1.2 32.9 20.9 36.6 19.2 76.1 13.6 81.4 18.5 10.4 6.9 10.7 6.8APD, LI, and RD 32 9.7 1.7 30.0 17.2 26.8 14.7 74.9 15.6 78.0 16.0 10.7 3.4 15.7 14.7LI and RD (no APD) 8 9.7 1.4 67.1 26.5 69.2 24.8 78.8 11.4 83.1 9.7 10.0 2.7 6.1 3.7Passed all tests 3 9.6 0.9 92.1 1.8 85 13.2 87.2 13.0 88.3 15.9 15.3 3.1 7.5 8.3
aIrrespective of whether the children have LI or RD. bIrrespective of whether the children have RD.
Sharma et al.: Comorbidity of APD, LI, and RD 711
receptive and expressive language scores, 8 had poor re-ceptive language, and 10 had poor expressive language.Sixteen children met Criterion b for LI, with languagescores below their nonverbal IQ. Six children showedthis discrepancy for both receptive and expressive lan-guage, 3 children showed poor receptive language scores,and another 7 showed poor expressive language scores.
Figure 1. Number of children with specific auditory processing difficulties out of the 49 diagnosed with auditoryprocessing disorder. All children having difficulties on the Frequency Pattern Test (FPT) had bilateral problems,and hence ears are not specified. DDT-2 = Dichotic Digit Test Version 2; RGDT = Random Gap Detection Test;MLD = Masking Level Difference; R = right ear.
Figure 2. Average FPT scores for the children in the languageimpairment (LI)–reading disorder (RD), auditory processing disorder(APD)–LI, APD–RD, and APD–LI–RD groups. Scores for the LI–RDgroup are the highest and are significantly better than those forthe other three groups. The APD–LI group has significantly higherscores than the APD–LI–RD group. Error bars show 95% confidenceintervals.
Figure 3. Average standard scores of all participants (N = 68)across the eight Clinical Evaluation of Language Fundamentals,Fourth Edition (CELF-4) subtests. Scores within the range of 7–10(shaded area) are regarded as normal (M – 1 SD). Error barsshow 95% confidence intervals. FollDirect = Following Directions;ReSent = Recalling Sentences; FormSent = Formulating Sentences;ReWord = Receptive Semantic Relationships; ExWord = ExpressiveSemantic Relationships; FamSeq = Familiar Sequences; FRept =Forward Digits Repetition; BRept = Backward Digits Repetition.
712 Journal of Speech, Language, and Hearing Research • Vol. 52 • 706–722 • June 2009
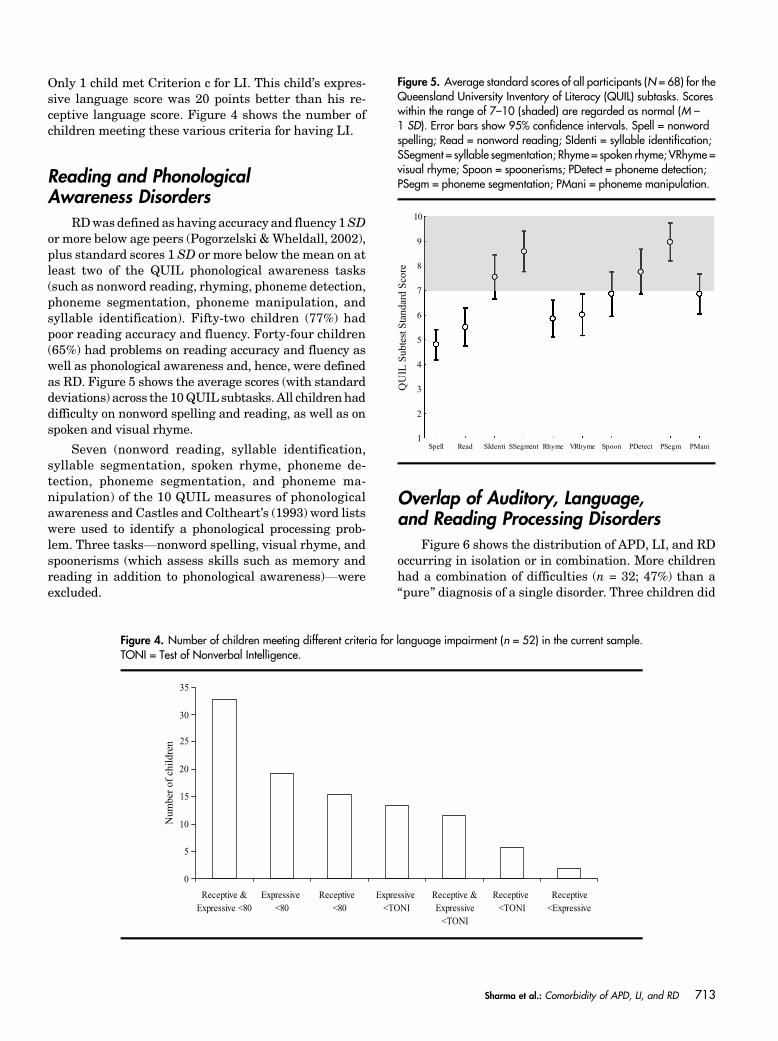
Only 1 child met Criterion c for LI. This child’s expres-sive language score was 20 points better than his re-ceptive language score. Figure 4 shows the number ofchildren meeting these various criteria for having LI.
Reading and PhonologicalAwareness Disorders
RDwas defined as having accuracy and fluency 1SDor more below age peers (Pogorzelski &Wheldall, 2002),plus standard scores 1 SD or more below the mean on atleast two of the QUIL phonological awareness tasks(such as nonword reading, rhyming, phoneme detection,phoneme segmentation, phoneme manipulation, andsyllable identification). Fifty-two children (77%) hadpoor reading accuracy and fluency. Forty-four children(65%) had problems on reading accuracy and fluency aswell as phonological awareness and, hence, were definedas RD. Figure 5 shows the average scores (with standarddeviations) across the 10QUIL subtasks. All childrenhaddifficulty on nonword spelling and reading, as well as onspoken and visual rhyme.
Seven (nonword reading, syllable identification,syllable segmentation, spoken rhyme, phoneme de-tection, phoneme segmentation, and phoneme ma-nipulation) of the 10 QUIL measures of phonologicalawareness and Castles and Coltheart’s (1993) word listswere used to identify a phonological processing prob-lem. Three tasks—nonword spelling, visual rhyme, andspoonerisms (which assess skills such as memory andreading in addition to phonological awareness)—wereexcluded.
Overlap of Auditory, Language,and Reading Processing Disorders
Figure 6 shows the distribution of APD, LI, and RDoccurring in isolation or in combination. More childrenhad a combination of difficulties (n = 32; 47%) than a“pure” diagnosis of a single disorder. Three children did
Figure 4. Number of children meeting different criteria for language impairment (n = 52) in the current sample.TONI = Test of Nonverbal Intelligence.
Figure 5. Average standard scores of all participants (N = 68) for theQueensland University Inventory of Literacy (QUIL) subtasks. Scoreswithin the range of 7–10 (shaded) are regarded as normal (M –1 SD). Error bars show 95% confidence intervals. Spell = nonwordspelling; Read = nonword reading; SIdenti = syllable identification;SSegment = syllable segmentation; Rhyme = spoken rhyme; VRhyme =visual rhyme; Spoon = spoonerisms; PDetect = phoneme detection;PSegm = phoneme segmentation; PMani = phoneme manipulation.
Sharma et al.: Comorbidity of APD, LI, and RD 713
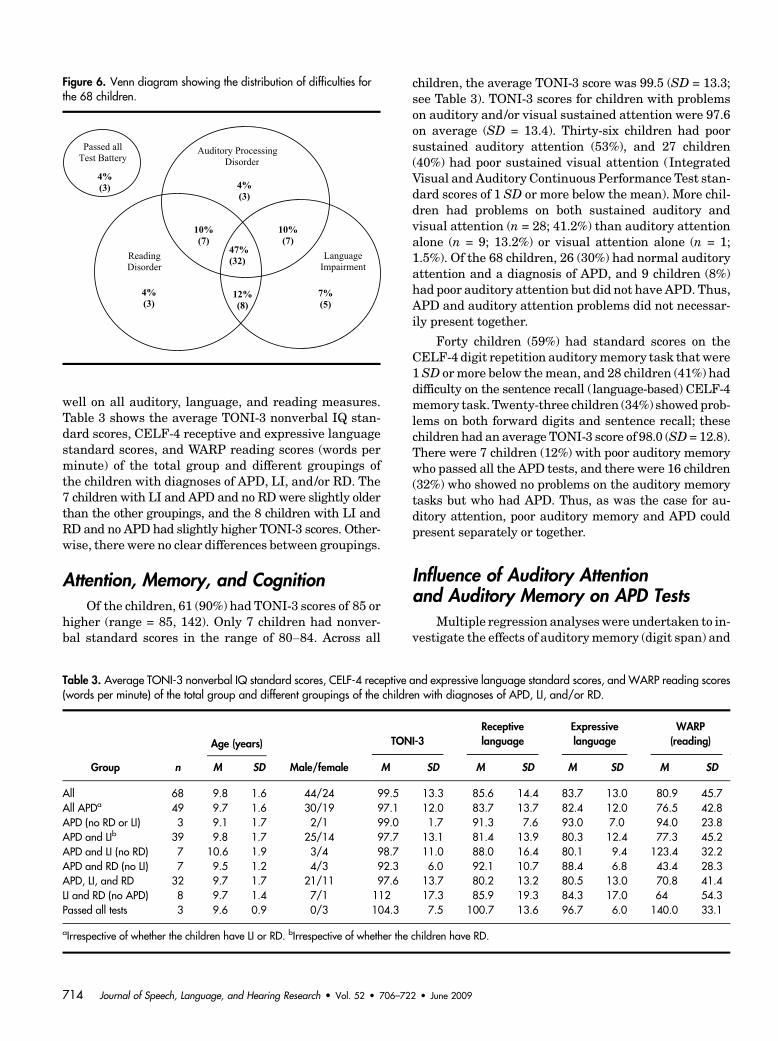
well on all auditory, language, and reading measures.Table 3 shows the average TONI-3 nonverbal IQ stan-dard scores, CELF-4 receptive and expressive languagestandard scores, and WARP reading scores (words perminute) of the total group and different groupings ofthe children with diagnoses of APD, LI, and/or RD. The7 children with LI and APD and no RDwere slightly olderthan the other groupings, and the 8 children with LI andRD and no APD had slightly higher TONI-3 scores. Other-wise, there were no clear differences between groupings.
Attention, Memory, and CognitionOf the children, 61 (90%) had TONI-3 scores of 85 or
higher (range = 85, 142). Only 7 children had nonver-bal standard scores in the range of 80–84. Across all
children, the average TONI-3 score was 99.5 (SD = 13.3;see Table 3). TONI-3 scores for children with problemson auditory and/or visual sustained attention were 97.6on average (SD = 13.4). Thirty-six children had poorsustained auditory attention (53%), and 27 children(40%) had poor sustained visual attention (IntegratedVisual and Auditory Continuous Performance Test stan-dard scores of 1 SD or more below the mean). More chil-dren had problems on both sustained auditory andvisual attention (n = 28; 41.2%) than auditory attentionalone (n = 9; 13.2%) or visual attention alone (n = 1;1.5%). Of the 68 children, 26 (30%) had normal auditoryattention and a diagnosis of APD, and 9 children (8%)had poor auditory attention but did not have APD. Thus,APD and auditory attention problems did not necessar-ily present together.
Forty children (59%) had standard scores on theCELF-4 digit repetition auditorymemory task thatwere1SD ormore below themean, and 28 children (41%) haddifficulty on the sentence recall (language-based) CELF-4memory task. Twenty-three children (34%) showed prob-lems on both forward digits and sentence recall; thesechildren had an average TONI-3 score of 98.0 (SD = 12.8).There were 7 children (12%) with poor auditory memorywho passed all the APD tests, and there were 16 children(32%) who showed no problems on the auditory memorytasks but who had APD. Thus, as was the case for au-ditory attention, poor auditory memory and APD couldpresent separately or together.
Influence of Auditory Attentionand Auditory Memory on APD Tests
Multiple regression analyseswere undertaken to in-vestigate the effects of auditorymemory (digit span) and
Table 3. Average TONI-3 nonverbal IQ standard scores, CELF-4 receptive and expressive language standard scores, and WARP reading scores(words per minute) of the total group and different groupings of the children with diagnoses of APD, LI, and/or RD.
Group n
Age (years)
Male/female
TONI-3Receptivelanguage
Expressivelanguage
WARP(reading)
M SD M SD M SD M SD M SD
All 68 9.8 1.6 44/24 99.5 13.3 85.6 14.4 83.7 13.0 80.9 45.7All APDa 49 9.7 1.6 30/19 97.1 12.0 83.7 13.7 82.4 12.0 76.5 42.8APD (no RD or LI) 3 9.1 1.7 2/1 99.0 1.7 91.3 7.6 93.0 7.0 94.0 23.8APD and LIb 39 9.8 1.7 25/14 97.7 13.1 81.4 13.9 80.3 12.4 77.3 45.2APD and LI (no RD) 7 10.6 1.9 3/4 98.7 11.0 88.0 16.4 80.1 9.4 123.4 32.2APD and RD (no LI) 7 9.5 1.2 4/3 92.3 6.0 92.1 10.7 88.4 6.8 43.4 28.3APD, LI, and RD 32 9.7 1.7 21/11 97.6 13.7 80.2 13.2 80.5 13.0 70.8 41.4LI and RD (no APD) 8 9.7 1.4 7/1 112 17.3 85.9 19.3 84.3 17.0 64 54.3Passed all tests 3 9.6 0.9 0/3 104.3 7.5 100.7 13.6 96.7 6.0 140.0 33.1
aIrrespective of whether the children have LI or RD. bIrrespective of whether the children have RD.
Figure 6. Venn diagram showing the distribution of difficulties forthe 68 children.
714 Journal of Speech, Language, and Hearing Research • Vol. 52 • 706–722 • June 2009
sustained auditory attention on APD results for four ofthe APD assessments (FPT, DDT, RGDT, and MLD). Asthere were no significant effects of test ear on FPT andDDT, scores for the two ears were averaged. Age, au-ditory memory, and auditory attention explained 21.6%of the variance in FPT scores. Partial correlations withFPT scores were .32 and .30 for auditory memory andauditory attention, respectively. Age, auditory memory,and auditory attention explained 28.5% of the variancein DDT scores. Partial correlations showed significantlinks between DDTscores and age (r = .34), and betweenDDT scores and auditory attention (r = .44). Attentionand memory had no significant effect on RGDT or MLDscores.
DiscussionDiagnosis of APD, LI, and RD
Unfortunately, there are no widely recognized “goldstandards” for identifying APD, RD, and LI; therefore,the extent of comorbidity of these conditions will dependon the specific diagnostic tests used to assess thesedifferent areas of difficulty as well as test sensitivity andspecificity. Only two of the APD tests used in the currentstudy, FPT and DDT, are extremely well-establishedmeasures of auditory processing with good sensitivityand specificity (Musiek & Chermak, 1994).
As noted earlier, there is considerable variation inthe criteria used to diagnose RD and LI; consequently,the overlap between APD, RD, and LI groups is likely tovary between studies. Many definitions of LI requirenonverbal IQ scores within the normal range; however,the criterion for nonverbal intelligence standard scoresvaries from 75 to 85 across studies (Kamhi, 1998). Starkand Tallal (1981) recommended using a representativeset of language tasks to diagnose LI, rather than usingone task (Plante, 1998). Despite these variations in de-finitions between studies, the overlap in APD, LI, andRD is consistent with Bishop, Bishop, et al. (1999) andRamus et al. (2003).
Bishop, Bishop, et al. (1999) compared auditoryprocessing abilities (on the basis of Tallal and Stark ’s,1981, auditory repetition task) in children with andwithout LI. All the children had nonverbal intelligencescores of 80 or above; however, the children with LI hada 15-point discrepancy between their receptive languageand nonverbal intelligence scores. The auditory pro-cessing findings were equivalent between groups. In thecurrent study, children with APD with and without LIhad similar mean scores on FPT, DDT, MLD, and RGDTmeasures of auditory processing (see Table 2). Thus,children with similar profiles of auditory processingdifficulties may or may not have LI; therefore, it is notpossible to predict the presence of LI in children with
APD on the basis of the APD tests used in the currentstudy. This is consistent with the recommendations ofthe ASHA Task Force on Central Auditory ProcessingConsensus Development (1996) and the ASHAWorkingGroup on Auditory Processing Disorders (2005) thatchildrenwith suspected APDhave both audiological andspeech-language assessments.
Thirteen childrenwithLI hadnoAPDon the basis ofthe measures used in the current study. The 39 childrenwith both LI and APD (with and without RD) all haddifficulty with auditory processing tasks that requiredtemporal processing (FPT, RGDT, and/or MLD). Thereis evidence that temporal processing performancevery early in life predicts later language performance(Benasich et al., 2006; Benasich & Tallal, 2002; Guttormet al., 2005), and there is considerable support for theview that temporal processing disorders are causallylinked to LI and RD (see review by Tallal, 2004). At firstglance, the finding that not all childrenwith LI had APDin the current study appears to contradict this view;however, this ignores the potential long-lasting impactof APD early in life on language and reading develop-ment, even if APDgoes on to resolve. An older child couldhave LI and/or RD but no concurrent APD, even whenthere is an auditory basis to the LI/RD, if the APD hasresolved as a result of maturation, the learning and/orhome environment, and so forth. This highlights one ofthe main limitations of cross-sectional studies. Longitudi-nal studies that begin early in life are needed to be able todraw conclusions about causality as well as comorbidity.
There is objective evidence from a longitudinal studyof 109 typically developing children for a link betweenearly auditory processing and later reading ability (Espy,Molfese, Molfese, & Modglin, 2004). Espy et al. (2004)measured auditory evoked potentials (AEPs) to speechand nonspeech sounds and found that the rate of mat-uration of AEP amplitudes from 1 to 4 years and from 4 to8 years was predictive of word-level reading at 8 years.Sharmaetal. (2006) found significant differences inAEPsbetween school-age children who had never experiencedreading difficulties versus children with a history ofreading difficulties who had reading scores withinthe normal range at the time of testing (“compensated”readers). Thus, even though reading performance wasnormal, there was electrophysiological evidence for dif-ferent underlying auditory processing in children withprevious reading difficulties. It is also possible that thechildren with LI and no evidence of APD in the currentstudy might have electrophysiological evidence of alteredauditory processing. Thus, longitudinal studies using bothelectrophysiological and behavioral measures of auditoryprocessing, language, and reading would help our under-standing of the causal links between these conditions.
Pogorzelski and Wheldall (2002) defined readingaccuracy and fluency as poor when scores were more
Sharma et al.: Comorbidity of APD, LI, and RD 715
than 1 SD below the mean for typically developing agepeers. The same criterion was used to define a problemon phonological awareness tasks. There were 10 QUILsubtasks, all of which produced a wide range of per-formance. The subtasks producing the highest aver-age scores were phoneme segmentation and syllablesegmentation. Performance was poorest overall for non-word reading and spoken rhyme. For 5 of the QUILtasks—nonword reading, syllable segmentation, sylla-ble identification, phoneme detection, and rhyming—only 16 children passed. Previous studies have used someof these tasks to identify a phonological awareness deficit.For example, Heath and Hogben (2000) measured pho-neme detection; Leitao, Hogben, and Fletcher (1997)measured phoneme segmentation and nonword reading;and Rack, Snowling, and Olson (1992) measured non-word reading. Unfortunately, there is no clear consensusin the literature regarding which phonological aware-ness tasks are most reliable and valid.
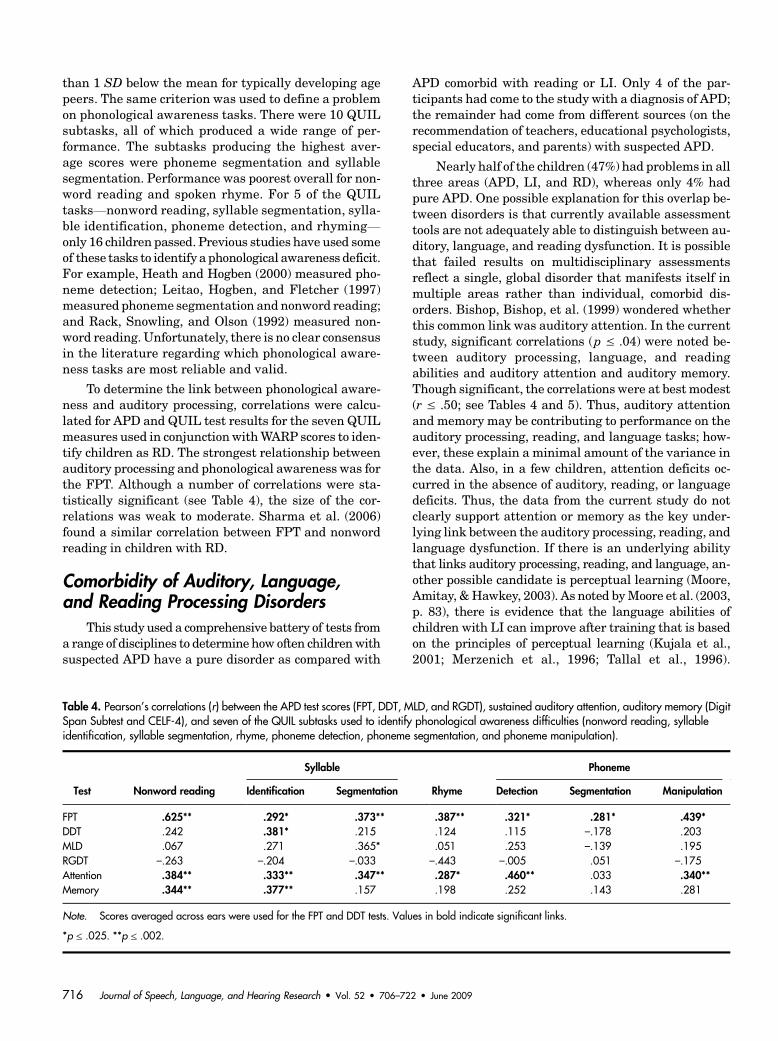
To determine the link between phonological aware-ness and auditory processing, correlations were calcu-lated for APD and QUIL test results for the seven QUILmeasures used in conjunctionwithWARP scores to iden-tify children as RD. The strongest relationship betweenauditory processing and phonological awareness was forthe FPT. Although a number of correlations were sta-tistically significant (see Table 4), the size of the cor-relations was weak to moderate. Sharma et al. (2006)found a similar correlation between FPT and nonwordreading in children with RD.
Comorbidity of Auditory, Language,and Reading Processing Disorders
This study used a comprehensive battery of tests froma range of disciplines to determine how often childrenwithsuspected APD have a pure disorder as compared with
APD comorbid with reading or LI. Only 4 of the par-ticipants had come to the study with a diagnosis of APD;the remainder had come from different sources (on therecommendation of teachers, educational psychologists,special educators, and parents) with suspected APD.
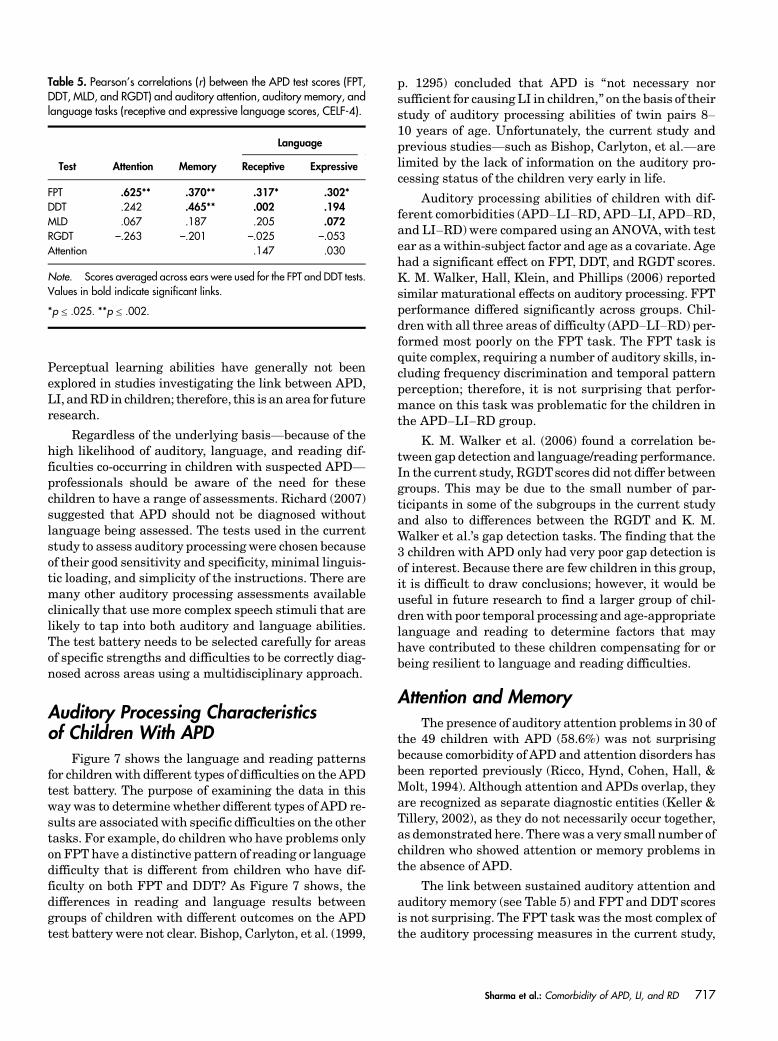
Nearly half of the children (47%) had problems in allthree areas (APD, LI, and RD), whereas only 4% hadpure APD. One possible explanation for this overlap be-tween disorders is that currently available assessmenttools are not adequately able to distinguish between au-ditory, language, and reading dysfunction. It is possiblethat failed results on multidisciplinary assessmentsreflect a single, global disorder that manifests itself inmultiple areas rather than individual, comorbid dis-orders. Bishop, Bishop, et al. (1999) wondered whetherthis common link was auditory attention. In the currentstudy, significant correlations (p ≤ .04) were noted be-tween auditory processing, language, and readingabilities and auditory attention and auditory memory.Though significant, the correlations were at best modest(r ≤ .50; see Tables 4 and 5). Thus, auditory attentionand memory may be contributing to performance on theauditory processing, reading, and language tasks; how-ever, these explain a minimal amount of the variance inthe data. Also, in a few children, attention deficits oc-curred in the absence of auditory, reading, or languagedeficits. Thus, the data from the current study do notclearly support attention or memory as the key under-lying link between the auditory processing, reading, andlanguage dysfunction. If there is an underlying abilitythat links auditory processing, reading, and language, an-other possible candidate is perceptual learning (Moore,Amitay, &Hawkey, 2003). As noted byMoore et al. (2003,p. 83), there is evidence that the language abilities ofchildren with LI can improve after training that is basedon the principles of perceptual learning (Kujala et al.,2001; Merzenich et al., 1996; Tallal et al., 1996).
Table 4. Pearson’s correlations (r) between the APD test scores (FPT, DDT, MLD, and RGDT), sustained auditory attention, auditory memory (DigitSpan Subtest and CELF-4), and seven of the QUIL subtasks used to identify phonological awareness difficulties (nonword reading, syllableidentification, syllable segmentation, rhyme, phoneme detection, phoneme segmentation, and phoneme manipulation).
Test Nonword reading
Syllable
Rhyme
Phoneme
Identification Segmentation Detection Segmentation Manipulation
FPT .625** .292* .373** .387** .321* .281* .439*DDT .242 .381* .215 .124 .115 –.178 .203MLD .067 .271 .365* .051 .253 –.139 .195RGDT –.263 –.204 –.033 –.443 –.005 .051 –.175Attention .384** .333** .347** .287* .460** .033 .340**Memory .344** .377** .157 .198 .252 .143 .281
Note. Scores averaged across ears were used for the FPT and DDT tests. Values in bold indicate significant links.
*p ≤ .025. **p ≤ .002.
716 Journal of Speech, Language, and Hearing Research • Vol. 52 • 706–722 • June 2009
Perceptual learning abilities have generally not beenexplored in studies investigating the link between APD,LI, andRD in children; therefore, this is anarea for futureresearch.
Regardless of the underlying basis—because of thehigh likelihood of auditory, language, and reading dif-ficulties co-occurring in children with suspected APD—professionals should be aware of the need for thesechildren to have a range of assessments. Richard (2007)suggested that APD should not be diagnosed withoutlanguage being assessed. The tests used in the currentstudy to assess auditory processingwere chosen becauseof their good sensitivity and specificity, minimal linguis-tic loading, and simplicity of the instructions. There aremany other auditory processing assessments availableclinically that use more complex speech stimuli that arelikely to tap into both auditory and language abilities.The test battery needs to be selected carefully for areasof specific strengths and difficulties to be correctly diag-nosed across areas using a multidisciplinary approach.
Auditory Processing Characteristicsof Children With APD
Figure 7 shows the language and reading patternsfor children with different types of difficulties on the APDtest battery. The purpose of examining the data in thisway was to determine whether different types of APD re-sults are associated with specific difficulties on the othertasks. For example, do children who have problems onlyon FPT have a distinctive pattern of reading or languagedifficulty that is different from children who have dif-ficulty on both FPT and DDT? As Figure 7 shows, thedifferences in reading and language results betweengroups of children with different outcomes on the APDtest battery were not clear. Bishop, Carlyton, et al. (1999,
p. 1295) concluded that APD is “not necessary norsufficient for causingLI in children,” on the basis of theirstudy of auditory processing abilities of twin pairs 8–10 years of age. Unfortunately, the current study andprevious studies—such as Bishop, Carlyton, et al.—arelimited by the lack of information on the auditory pro-cessing status of the children very early in life.
Auditory processing abilities of children with dif-ferent comorbidities (APD–LI–RD, APD–LI, APD–RD,and LI–RD) were compared using an ANOVA, with testear as a within-subject factor and age as a covariate. Agehad a significant effect on FPT, DDT, and RGDT scores.K. M. Walker, Hall, Klein, and Phillips (2006) reportedsimilar maturational effects on auditory processing. FPTperformance differed significantly across groups. Chil-dren with all three areas of difficulty (APD–LI–RD) per-formed most poorly on the FPT task. The FPT task isquite complex, requiring a number of auditory skills, in-cluding frequency discrimination and temporal patternperception; therefore, it is not surprising that perfor-mance on this task was problematic for the children inthe APD–LI–RD group.
K. M. Walker et al. (2006) found a correlation be-tween gap detection and language/reading performance.In the current study, RGDTscores did not differ betweengroups. This may be due to the small number of par-ticipants in some of the subgroups in the current studyand also to differences between the RGDT and K. M.Walker et al.’s gap detection tasks. The finding that the3 children with APD only had very poor gap detection isof interest. Because there are few children in this group,it is difficult to draw conclusions; however, it would beuseful in future research to find a larger group of chil-drenwith poor temporal processing and age-appropriatelanguage and reading to determine factors that mayhave contributed to these children compensating for orbeing resilient to language and reading difficulties.
Attention and MemoryThe presence of auditory attention problems in 30 of
the 49 children with APD (58.6%) was not surprisingbecause comorbidity of APD and attention disorders hasbeen reported previously (Ricco, Hynd, Cohen, Hall, &Molt, 1994). Although attention and APDs overlap, theyare recognized as separate diagnostic entities (Keller &Tillery, 2002), as they do not necessarily occur together,as demonstrated here. Therewas a very small number ofchildren who showed attention or memory problems inthe absence of APD.
The link between sustained auditory attention andauditory memory (see Table 5) and FPTand DDT scoresis not surprising. The FPT task was the most complex ofthe auditory processing measures in the current study,
Table 5. Pearson’s correlations (r) between the APD test scores (FPT,DDT, MLD, and RGDT) and auditory attention, auditory memory, andlanguage tasks (receptive and expressive language scores, CELF-4).
Test Attention Memory
Language
Receptive Expressive
FPT .625** .370** .317* .302*DDT .242 .465** .002 .194MLD .067 .187 .205 .072RGDT –.263 –.201 –.025 –.053Attention .147 .030
Note. Scores averaged across ears were used for the FPT and DDT tests.Values in bold indicate significant links.
*p ≤ .025. **p ≤ .002.
Sharma et al.: Comorbidity of APD, LI, and RD 717
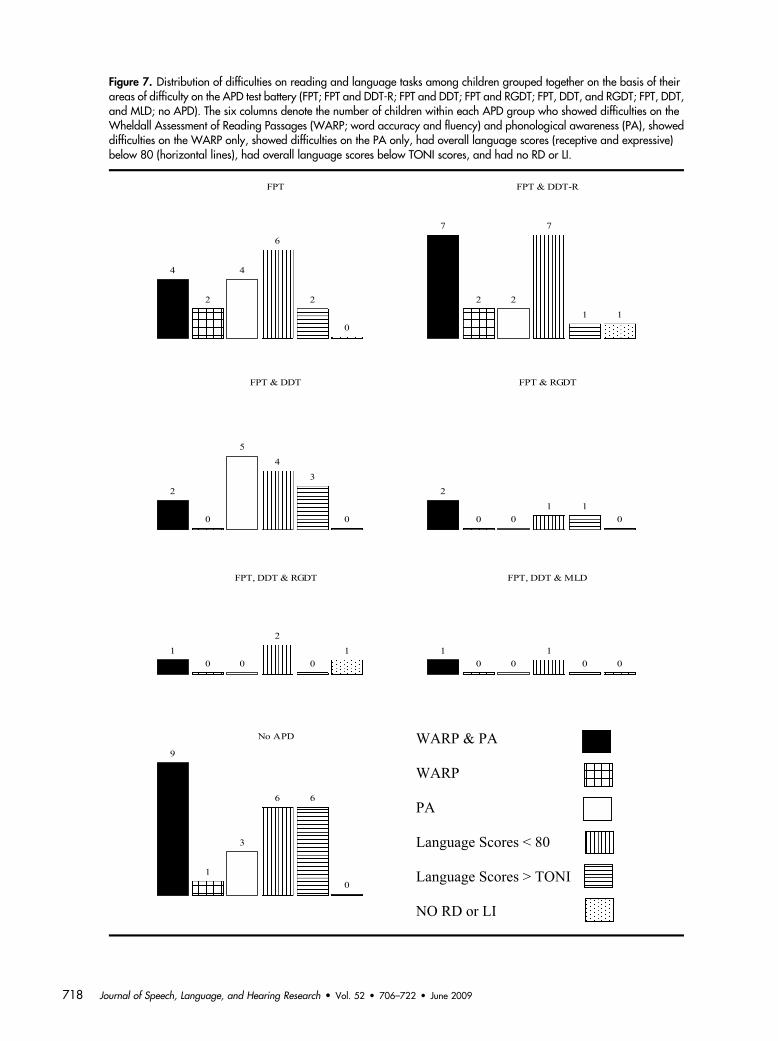
Figure 7. Distribution of difficulties on reading and language tasks among children grouped together on the basis of theirareas of difficulty on the APD test battery (FPT; FPT and DDT-R; FPT and DDT; FPT and RGDT; FPT, DDT, and RGDT; FPT, DDT,and MLD; no APD). The six columns denote the number of children within each APD group who showed difficulties on theWheldall Assessment of Reading Passages (WARP; word accuracy and fluency) and phonological awareness (PA), showeddifficulties on the WARP only, showed difficulties on the PA only, had overall language scores (receptive and expressive)below 80 (horizontal lines), had overall language scores below TONI scores, and had no RD or LI.
718 Journal of Speech, Language, and Hearing Research • Vol. 52 • 706–722 • June 2009

requiring children to attend to instructions, discrimi-nate tones of different frequencies, and remember andlabel an auditory sequence. Scores on theDDT taskwerenot correlated with memory but were correlated withsustained attention. Care was taken to ensure childrenwere performing optimally, with session times short-ened if necessary. Ideally, assessment sessions should beshort with adequate practice to make sure that the childhas understood the task and reinforcement to ensurethat the child remains on task (Silman, Silverman, &Emmer, 2000). This flexibility is possible in a researchsetting but may not always be possible clinically. Un-fortunately, if auditory attention is extremely poor, aninaccurate diagnosis of APD could occur (Sutcliffe,Bishop, Houghton, & Taylor, 2006). Motivation is an-other important consideration. Chermak (2005) sug-gested that if performance is poor for all APD tasks, thenthe audiologist should suspect global deficits, such aspoor attention, memory, language, or motivation.
Another question of interest in the current studywas whether children with lower nonverbal intelligencescores have the most coexisting problems. Table 2 pre-sents the average TONI-3 scores for the differentgroupings of the children, showing considerable overlapin the scores. An ANOVA—with age as a continuouspredictor—comparing the TONI-3 scores of the chil-dren with APD, LI, and RD (n = 32) versus childrenwith fewer difficulties (n = 36) showed no significantdifference, F(1, 63) = 0.4, p = .538. Therefore, childrenwith lower cognitive scores did not necessarily havemoreproblems across tasks.
ConclusionsMore than half of the participating children showed
comorbidity of APD, LI, and RD. Scores for two of theAPD tasks were linked to auditory attention (FPT) and/or memory (FPT and DDT); however, only weak cor-relations were obtained, indicating that these abilitiesonly had a minor effect on scores. There were only mod-est correlations between auditory attention, auditorymemory, reading, and language performance. Childrenin the APD–LI–RD group had the poorest FPT scores.Children presented with a number of different combina-tions of difficulties, however, highlighting the importanceof assessing language, reading, attention, andmemory inaddition to auditory processing. There is consensus thatinterventions for children with APD should be customizedand deficit focused (ASHA Working Group on AuditoryProcessing Disorders, 2005). To achieve this, audiologistsneed to carefully consider the choice of assessments andensure that childrenare performing optimally; in addition,they need to ensure that they work collaboratively withrelated professionals, such as speech-language patholo-gists and educational psychologists.
ReferencesAhissar, M., Protopapas, A., Reid,M., &Merzenich, M.M.(2000). Auditory processing parallels reading abilities inadults. Proceedings of National American Society, 97,6832–6837.
Aithal, V., Yonovitz, A., & Aithal, S. (2006). Tonal maskinglevel differences in Aboriginal children: Implications forbinaural interaction, auditory processing disorders andeducation. Australian and New Zealand Journal of Audiol-ogy, 28, 31–40.
American Speech-Language-Hearing AssociationTaskforce on Central Auditory Processing ConsensusDevelopment. (1996). Central auditory processing: Cur-rent status of research and implications for clinical practice.American Journal of Audiology, 5, 41–54.
American Speech-Language-Hearing AssociationWorking Group on Auditory Processing Disorders.(2005). Central auditory processing. Available from www.asha.org/members/deskref-journals/deskref /default.
Amitay, S., Ahissar, M., & Nelken, I. (2002). Auditoryprocessing deficits in reading disabled adults. Journal ofAssociated Research Otolaryngology, 3, 302–320.
Anderson, K. C., Brown, C. P., & Tallal, P. (1993). Dev-elopmental language disorders: Evidence for a basic proces-sing deficit.Current Opinion inNeurology andNeurosurgery,6, 98–106.
Aram, D. M., & Nation, J. (1980). Preschool language dis-orders and subsequent language and academic difficulties.Journal of Communication Disorders, 13, 159–179.
Bellis, T. J. (2007). Historical foundation and the nature of(central) auditory processing disorder. In Handbook of(central) auditory processing disorder: Auditory neuroscienceand diagnosis (Vol. 1, pp. 119–136). Oxfordshire, England:Plural Publishing.
Benasich, A. A., Choudhury, N., Friedman, J. T., RealpeBonilla, T., Chojnowska, C., & Gou, Z. (2006). Infants asa prelinguistic model for language learning impairments:Predicting from event-related potentials to behavior.Neuropsychologia, 44, 396–411.
Benasich, A. A., & Tallal, P. (2002). Infant discrimination ofrapid auditory cues predicts later language impairment.Behavioural Brain Research, 136, 31–49.
Benasich, A. A., Thomas, J. J., & Leppanen, P. H. T.(2002). The importance of rapid auditory processing abil-ities to early language development: Evidence of con-verging methodologies. Developmental Psychobiology, 40,278–292.
Benson, P. V., Seaton, J. B., & Johnson, C. D. (1997).Educational audiology handbook. San Diego, CA: Singular.
Bishop, D. V. M. (1992). The underlying nature of specificlanguage impairment. Journal of Child Psychology andPsychiatry, 33, 3–66.
Bishop, D. V. M. (2001). Genetic influences on languageimpairment and literacy problems in children: Same ordifferent? Journal of Child Psychology and Psychiatry, 42,189–198.
Bishop, D. V. M., & Adams, C. (1990). A prospective studyof the relationship between specific language impairment,phonological disorders, and reading retardation. Journal ofChild Psychology and Psychiatry, 21, 1027–1050.
Sharma et al.: Comorbidity of APD, LI, and RD 719
Bishop, D. V. M., Bishop, S. J., Bright, P., James, C.,Delaney, T., & Tallal, P. (1999). Different origin of au-ditory and phonological awareness problems in childrenwith language impairment: Evidence from a twin study.Journal of Speech, Language, and Hearing Research, 42,155–168.
Bishop, D. V. M., Carlyton, R. P., Deeks, J. M., & Bishop,S. J. (1999). Auditory temporal processing impairment:Neither necessary nor sufficient for causing languageimpairment in children. Journal of Speech, Language,and Hearing Research, 42, 1295–1310.
Boothroyd, A., & Nittrouer, S. (1988). Mathematicaltreatment of context effects in phoneme and word recog-nition. The Journal of the Acoustical Society of America,84, 101–114.
Brown, L., Sherbenou, R., & Johnsen, S. (1997). Test ofNonverbal Intelligence. Austin, TX: Pro-Ed.
Castles, A., & Coltheart, M. (1993). Varieties of develop-mental dyslexia. Cognition, 47, 149–180.
Catts, H. W. (1993). The relationship between speech lan-guage impairments and reading disabilities. Journal ofSpeech and Hearing Research, 36, 948–958.
Catts, H. W., Fey, M. E., Tomblin, J. B., & Zhang, X. (2002).A longitudinal investigation of reading outcomes in childrenwith language impairments. Journal of Speech, Language,and Hearing Research, 45, 1142–1157.
Chermak, G. D. (2005). Differential diagnosis of (C) APD orADHD. Available from www.eastbaylda.org/newsletter/may13/2005.
Dodd, B., Holm, A., Orelemans, M., & McCormick, M.(1996). QUIL: Queensland University Inventory of Literacy.Brisbane, Australia: The University of Queensland.
Edwards, V. T., & Hogben, J. H. (1999). New norms forcomparing children’s lexical and nonlexical reading: Afurther look at subtyping dyslexia. Australian Journal ofPsychology, 51, 37–49.
Espy, K. A., Molfese, D. L., Molfese, V. J., &Modglin, A. M.(2004). Development of auditory event-related potentialsin young children and relations to word-level readingabilities at age 8 years. Annals of Dyslexia, 54, 9–38.
Fey, M. (1986). Language intervention with young children.Boston: Allyn & Bacon.
Fey, M. E., Long, S. H., & Cleave, P. L. (1994). A recon-sideration of IQ criteria in the definition of specific languageimpairment. In R. V. Watkins & M. L. Rice (Eds.), Specificlanguage impairments in children (pp. 161–178). Baltimore:Brookes.
Guttorm, T. K., Leppanen, P. H. T., Poikkeus, A.-M.,Eklund, K. M., Lyytinen, P., & Lyytinen, H. (2005). Brainevent-related potentials (ERPs) measured at birth predictlater language development in children with and withoutfamilial risk for dyslexia. Cortex, 41, 291–303.
Hall, J. W. (2000). Handbook of otoacoustic emissions. SanDiego, CA: Singular.
Heath, S. M., & Hogben, J. H. (2000). Auditory temporalprocessing, phonological awareness and oral languageability in pre-readers: Can we identify children at risk forreading disability more accurately? Australian Educationaland Developmental Psychologist, 17, 32–62.
Heiervang, E., Stevenson, J., & Hugdahl, K. (2002). Au-ditory processing in dyslexia. Journal of Child Psychologyand Psychiatry, 43, 931–938.
Helzer, J. R., Champlin, C. A., & Gillam, R. B. (1996).Auditory temporal resolution in specifically language-impaired and age matched children. Perceptual and MotorSkills, 83, 1171–1181.
Jerger, J. F. (1970). Clinical experience with impedanceaudiometry. Archives of Otolaryngology, 92, 311–324.
Kamhi, A. G. (1998). Trying to make sense of developmentallanguage disorders.Language, Speech, andHearing Servicesin Schools, 29, 35–44.
Keith, R. W. (2000).RandomGap Detection Test. San Antonio,TX: Auditec.
Keller, W. D., & Tillery, K. L. (2002). Reliable differentialdiagnosis and effective management of auditory processingand attention deficit hyperactivity disorders. Seminars ofHearing, 23, 337–348.
Kelly, A. S. (2007). Normative data for behavioural testsof auditory processing for New Zealand school childrenaged 7-12 years. Australian and New Zealand Journal ofAudiology, 29, 60–64.
King, W. M., Lombardino, L. J., Crandell, C. C., &Leonard, C. M. (2003). Comorbid auditory processingdisorder in developmental dyslexia. Ear and Hearing, 24,448–456.
Kujala, T., Karma, K., Ceponiene, R., Belitz, S., Turkkila,P., Tervaniemi, M., & Naatanen, R. (2001). Plastic neuralchanges and reading improvement caused by audiovisualtraining in reading-impaired children. Proceedings of theNational Academy of Sciences, USA, 98, 10509–10514.
Leitao, S., Hogben, J., & Fletcher, J. (1997). Phonologicalprocessing skills in speech and language impaired children.European Journal of Disorders of Communication, 32, 2,91–113.
Madelaine, A., & Wheldall, K. (2002). Further progresstowards a standardized curriculum-based measure of read-ing: Calibrating a new passage reading test against the NewSouth Wales Basic Skills Test. Educational Psychology, 22,461–471.
McAnally, K. I., & Stein, J. F. (1996). Auditory temporalcoding in dyslexia. Proceedings of the Royal Society, B:Biological Sciences, 263, 961–965.
McArthur, G. M., & Bishop, D. V. M. (2001). Auditory per-ceptual processing in people with reading and oral languageimpairments: Current issues and recommendations. Dys-lexia, 7, 150–170.
McArthur, G. M., & Bishop, D. V. M. (2004a). Frequencydiscrimination deficits in people with specific languageimpairment: Reliability, validity, and linguistics correlates.Journal of Speech, Language, and Hearing Research, 47,527–541.
McArthur, G. M., & Bishop, D. V. M. (2004b). Which peoplewith specific language impairment have auditory processingdeficits? Cognitive Neuropsychology, 21, 79–94.
Merzenich,M.M., Jenkins,W.M., Johnston, P., Schreiner,C., Miller, S. L., & Tallal, P. (1996, January 5). Temporalprocessing deficits of language-learning impaired childrenameliorated by training. Science, 271, 77–81.
720 Journal of Speech, Language, and Hearing Research • Vol. 52 • 706–722 • June 2009
Moore, D. R., Amitay, S., & Hawkey, D. J. C. (2003). Audi-tory perceptual learning. Learning & Memory, 10, 83–85.
Musiek, F. E. (1983). Assessment of central auditory dys-function: The Dichotic Digits Test revisited. Ear andHearing, 4, 79–83.
Musiek, F. E. (1994). Frequency (pitch) and duration patterntests. Journal of the American Academy of Audiology, 5,265–268.
Musiek, F. E., & Chermak, G. D. (1994). Three commonlyasked questions about central auditory processing dis-orders: Assessment. American Journal of Audiology, 3,23–27.
Noffsinger, D., Wilson, R. H., & Musiek, F. E. (1994).Department of Veterans Affairs compact disc recordingfor auditory perceptual assessment: Background and intro-duction. Journal of the American Academy of Audiology, 5,231–235.
Plante, E. (1998). Criteria for SLI: The Stark and Tallallegacy and beyond. Journal of Speech, Language, andHearing Research, 41, 951–957.
Pogorzelski, S., & Wheldall, K. (2002). Do differences inphonological processing performance predict gains madeby older low-progress readers following intensive literacyintervention? Educational Psychology, 22, 413–427.
Rack, J. P., Snowling, M. J., & Olson, R. K. (1992). Thenonword reading deficit in developmental dyslexia: Areview. Reading Research Quarterly, 27, 28–53.
Ramus, F., Rosen, S., Dakin, S. C., Day, B. L., Castellote,J. M., White, S., & Frith, U. (2003). Theories of develop-mental dyslexia: Insights from multiple case study ofdyslexic adults. Brain, 126, 841–865.
Reed, V. A., & Baker, E. (2005). Toddlers and preschoolerswith specific language impairment. In V. A. Reed (Ed.), Anintroduction to children with language disorders (3rd ed.;pp. 75–131). Upper Saddle River, NJ: Pearson Education.
Ricco, C. A., Hynd, G. W., Cohen, M. J., Hall, J., & Molt, L.(1994). Comorbidity of central auditory processing disorderand attention-deficit hyperactivity disorder. Journal of theAmerican Academy of Child and Adolescent Psychiatry, 33,849–857.
Richard, G. J. (2007). Cognitive-communication and lan-guage factors associated with (central) auditory processingdisorder: A speech-language pathology perspective. In F. E.Musiek & G. D. Chermak (Eds.), Handbook of (central)auditory processing disorder: Auditory neuroscience anddiagnosis (Vol. 1, pp. 397–415). Oxfordshire, England:Plural Publishing.
Rosen, S. (1999). A problem with auditory processing?Current Biology, 9, R698–R700.
Rosen, S. (2003). Auditory processing in dyslexia and spe-cific language impairment: Is there a deficit? What is itsnature? Does it explain anything? Journal of Phonetics, 31,509–527.
Rosen, S., & Manganari, E. (2001). Is there a relationshipbetween speech and nonspeech auditory processing in chil-dren with dyslexia? Journal of Speech, Language, andHearing Research, 44, 720–736.
Sandford, J. A., & Turner, A. (1995). Integrated Visualand Auditory Continuous Performance Test. RetrievedApril 5, 2007, from www.addwarehouse.com/shopsitesc/
store/html/integrated-visual-and-auditory-continuous-performance-test.
Scholes, R. J. (1998). The case against phonemic awareness.Journal of Research in Reading, 21, 177–188.
Schulte-Körne, G., Deimel, W., Bartling, J., & Remschmidt,H. (1998). Auditory processing and dyslexia: Evidence for aspecific speech processing deficit. NeuroReport, 9, 337–340.
Semel, E., Wiig, E., & Secord, W. (2003). Clinical Evaluationof Language Fundamentals, Fourth Edition (CELF-4).San Antonio, TX: The Psychological Corporation.
Sharma,M., Purdy, S.C.,Newall,P.,Wheldall,K., Beaman,R., & Dillon, H. (2006). Electrophysiological and behav-ioural evidence of auditory processing disorders in chil-dren with reading disorders. Clinical Neurophysiology, 117,1130–1144.
Silman, S., & Gelfand, S. A. (1981). The relationship be-tween magnitude of hearing loss and acoustic reflex thresh-old levels. Journal of Speech and Hearing Disorders, 46,312–316.
Silman, S., Silverman, C. A., & Emmer, M. B. (2000).Central auditory processing disorders and reduced motiva-tion: Three case studies. Journal of the American Academyof Audiology, 11, 57–63.
Smoski, W. J., Brunt, M. A., & Tannahill, J. C. (1998).Children’s Auditory Performance Scale. Tampa, FL: Educa-tional Audiology Association.
Snowling, M., Bishop, D. V. M., & Stothard, S. E. (2000). Ispreschool language impairment a risk factor for dyslexia inadolescence? Journal of Child Psychology and Psychiatry &Allied Disciplines, 41, 587–600.
Stark, R. E., & Tallal, P. (1981). Selection of children withspecific language deficits. Journal of Speech and HearingDisorders, 46, 114–122.
Sutcliffe, P., Bishop, D. V. M., Houghton, S., & Taylor, M.(2006). Effect of attentional state on frequency discrimina-tion: A comparison of children with ADHD on and offmedication. Journal of Speech, Language, and HearingResearch, 49, 1072–1084.
Tallal, P. (2004). Improving language and literacy is a matterof time. Nature Reviews Neuroscience, 5, 721–728.
Tallal, P., & Stark, R. E. (1981). Speech acoustic-cue discrim-ination abilities of normally developing and language-impaired children. The Journal of the Acoustical Societyof America, 69, 568–574.
Tallal, P., Steve, L., Miller, S. L., Bedi, G., Byma, G., Wang,X., et al. (1996, January 5). Language comprehension inlanguage-learning impaired children improved with acous-tically modified speech. Science, 271, 81–84.
Tomblin, J. B., Records, N., & Zhang, X. (1996). A sys-tem for the diagnosis of specific language impairment inkindergarten children. Journal of Speech and HearingResearch, 39, 1284–1294.
Walker, K. M., Hall, S. E., Klein, R. M., & Phillips, D. P.(2006). Development of perceptual correlates of readingperformance. Brain Research, 1124, 126–141.
Walker, M. M., Shinn, J., Cranford, J. L., Givens, G., &Holbert, D. (2002). Auditory temporal processing perfor-mance of young adults with reading disorders. Journal ofSpeech, Language, and Hearing Research, 45, 598–605.
Sharma et al.: Comorbidity of APD, LI, and RD 721

Watson, B. U., & Miller, T. K. (1993). Auditory perception,phonological processing, and reading ability/disability.Journal of Speech and Hearing Research, 36, 850–863.
Weismer, S. E., Tomblin, J. B., Zhang, X., Buckwalter, P.,Chynoweth, J. G., & Jones, M. (2000). Nonword repetitionperformance in school-age children with and without lan-guage impairment. Journal of Speech, Language, andHearing Research, 43, 865–878.
Wible, B., Nicol, T., & Kraus, N. (2005). Correlation betweenbrainstem and cortical auditory processes in normal andlanguage-impaired children. Brain, 128, 417–423.
Received September 26, 2007
Revision received April 27, 2008
Accepted October 5, 2008
DOI: 10.1044/1092-4388(2008/07-0226)
Contact author: Mridula Sharma, Macquarie University–Linguistics, Building C5, Room 513, Macquarie University,Sydney, New South Wales 2106, Australia.E-mail: [email protected].
722 Journal of Speech, Language, and Hearing Research • Vol. 52 • 706–722 • June 2009