comparison of direct versus indirect laryngoscopy for ... vs indirect... · comparison of direct...
TRANSCRIPT

A P R O G R E S S U P D A T E
B R I A N S A V I N O
COMPARISON OF DIRECT VERSUS INDIRECT LARYNGOSCOPY FOR INTUBATION IN THE
PREHOSPITAL SETTING: A SYSTEMATIC REVIEW AND META-ANALYSIS

BACKGROUND
• Laryngoscopy as
practiced today was
developed in the 1940s.
• Classically the Macintosh
and Miller blades are
used to intubate,
especially in the acute-
care settings (ED, ICU)

INDIRECT LARYNGOSCOPY
• National Overall Success of Direct: 85%
• Indirect video devices introduced in early 2000s and rapidly gained acceptance in ED settings.
• Hospital studies show improved first-pass success rates and time to successful intubation, especially among novice intubators.
Brown, C. A., 3rd, A. E. Bair, D. J. Pallin, R. M. Walls, and Near Iii Investigators. "Techniques, Success, and
Adverse Events of Emergency Department Adult Intubations." Ann Emerg Med 65, no. 4 (Apr 2015): 363-70 e1.

DIRECT VS INDIRECT LARYNGOSCOPY
Direct
Indirect

INDIRECT DEVICE EXAMPLES
• Macintosh Reusable
Blades and Handles
• Glidescope Ranger
• AirTraq
• King Vision LT

PREHOSPITAL INTUBATION
• Studies show paramedics outcomes are worse than
physicians.
• Can we apply hospital success with novice
intubators to the prehospital setting?
• Is there evidence for benefit for indirect
laryngoscopy in the prehospital setting when
compared to direct?

WHY LOOK INTO THIS?
• Prehospital treatment isn’t always the same as in-
hospital treatment.
• EMS systems vary – what’s good for one isn’t
necessarily good for all.
• Cost/Benefit: These Indirect devices cost money
and require training!

RESEARCH QUESTION
• For definitive airway management in the
prehospital setting, does indirect laryngoscopy lead
to better overall intubation success and first-pass
success than direct laryngoscopy?
• PICO
• P – patients requiring intubation in the prehospital setting
• I – Indirect Laryngoscopy
• C – Direct Laryngoscopy
• O – Overall Success, First-pass success

WHAT RESEARCH EXISTS?
• We can do: A Systematic Review and Meta-analysis

DEFINITIONS
• Direct Laryngoscopy: Insertion of the endotracheal tube by a method of directly visualizing the vocal cords. • Examples: Macinotosh blade, Miller Blade.
• Indirect Laryngoscopy: Insertion of the endotracheal tube by a method of indirectly visualizing the vocal cord, either using a video camera or optics (mirrors). • Examples: (GlideScope, Airtraq, King Vision LT)

SYSTEMATIC REVIEW
• Inclusion Criteria: • Prehospital Setting
• Human Studies
• Exclusion Criteria: • No comparison to direct laryngoscopy
• Case Reports and Case Series studies
• Studies restricted to pediatrics
• Studies comparing indirect laryngoscopy to rescue airway devices (supraglottic airways, oral airways, bag-valve mask)
• In-hospital settings (ED, OR, ICU etc.)
• Non-human studies, manikin studies
• Cadaver Studies

SYSTEMATIC REVIEW
• Outcomes: • Overall Success
• First Pass Success
• Search Terms: • EMS, Emergency Medical Services, Prehospital, Pre-hospital,
Paramedic, Air Medical, Helicopter, Out-of-Hospital/Out of Hospital AND • Video laryngoscopy
• Video Intubation • Indirect Laryngoscopy • Indirect Intubation • Glidescope • Airtraq
• Vividtrac • CMAC, C-MAC • King Vision

OUTCOME DEFINITIONS
• Overall Success Rate: Proportion of patients
successfully intubated with the intended device
• First-Pass Success Rate: Proportion of patients
successfully intubated with the intended device on
the first attempt.

WHY THE PROXY MEASURES OF OUTCOME?
• Traditionally, EMS and Hospital systems do not share data. This is starting to change, but still very difficult to follow up on patients.
• Developing a proxy measure of outcome versus longitudinal follow-up is more cost-effective, especially for regular QI activities.
• Acute-care in-hospital studies show the most predictive variable for poor outcomes is the number of intubation attempts: • 1 attempt: 14% adverse event rate
• 2 attempts or more: 47% adverse event rate


SYSTEMATIC REVIEW – STUDY CHARACTERISTICS
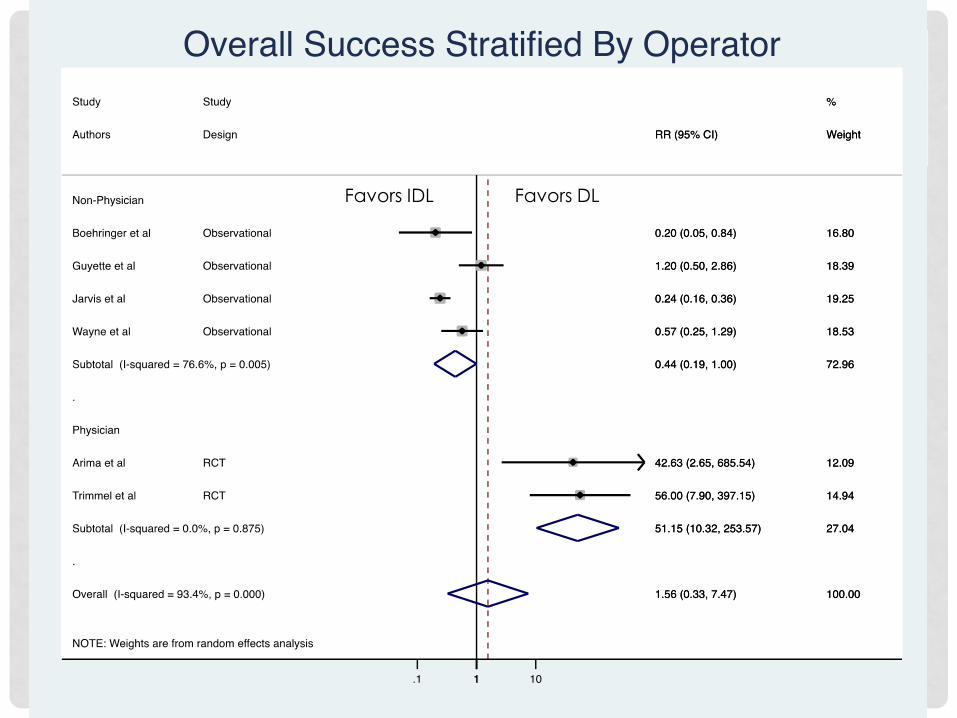
META-ANALYSIS OVERALL SUCCESS WITH IDL VS DL
Favors DL Favors IDL Favors DL Favors IDL

META-ANALYSIS OVERALL SUCCESS WITH IDL VS DL

OBSERVATIONS
• Significant heterogeneity when physician/non-
physicians grouped together, but not when
separated.
• Physicians (experienced operators) do better with
DL for overall success while non-physicians
(inexperienced operators) do better with IDL.
• RCTs show better results with DL than observational
studies (although RCTs both used physicians).

META-ANALYSIS FIRST-PASS SUCCESS WITH IDL VS DL

META-ANALYSIS FIRST-PASS SUCCESS WITH IDL VS DL

OBSERVATIONS
• Only one study used physicians, only study is an
RCT.
• Again, non-physicians seem to perform better with
IDL than DL.
• Still some significant heterogeneity.

SO WHAT SHOULD WE DO?
• There is not currently evidence to support or discourage the use of indirect laryngoscopy in the prehospital setting. Studies are heterogeneous.
• Medical directors and EMS/Public Health agencies interested in
deploying these devices should consider looking at studies that mirror their systems (i.e. helicopter, physician-based etc, experience)
• Training is crucial. Many studies suggested the reason for their results had to do with inadequate training.
• Non-studied benefits: Recording intubations for QI/Training, more unified training, ease/quickness of learning skill
• Non-studied harms: Device failure, cost, loss of skills
• MORE STUDIES ARE NEEDED HERE!

REFERENCES
1. Diggs LA, Yusuf JE, De Leo G. An update on out-of-hospital airway management practices in the United States. Resuscitation 2014;85(7): 885-92.
2. Bernhard M, Becker TK, Gries A, et al. The First Shot Is Often the Best Shot: First-Pass Intubation Success in Emergency Airway Management. Anesth Analg 2015;121(5):1389-93.
3. Sakles JC, Chiu S, Mosier J, et al. The importance of first pass success when performing orotracheal intubation in the emergency department. Acad Emerg Med 2013;20(1):71-8.
4. Macintosh RR. A New Laryngoscope. The Lancet 1943;241(6233):205.
5. Miller RA. The development of the laryngoscope. Anaesthesist 1972;21(3):145-7.
6. Brown CA, 3rd, Bair AE, Pallin DJ, et al. Techniques, success, and adverse events of emergency department adult intubations. Ann Emerg Med 2015;65(4):363-70 e1.
7. De Jong A, Molinari N, Conseil M, et al. Video laryngoscopy versus direct laryngoscopy for orotracheal intubation in the intensive care unit: a systematic review and meta-analysis. Intensive Care Med 2014;40(5):629-39.
8. Griesdale DE, Liu D, McKinney J, et al. Glidescope(R) video-laryngoscopy versus direct laryngoscopy for endotracheal intubation: a systematic review and meta-analysis. Can J Anaesth 2012;59(1):41-52.
9. Selde W, English K, Heffelfinger M, et al. Successful airtraq use in an air medical transport system. Air medical journal 2014;33(6):331-4.
10. Boedeker BH, Berg BW, Bernhagen M, et al. Endotracheal intubation comparing a prototype storz CMAC and a GlideScope videolaryngoscope in a medical transport helicopter - A pilot study. Presented at Studies in Health Technology and Informatics2009.
11. Burnett AM, Frascone RJ, Wewerka SS, et al. Comparison of success rates between two video laryngoscope systems used in a prehospital clinical trial. Prehosp Emerg Care 2014;18(2):231-8.
12. Bernhard M, Mohr S, Weigand MA, et al. Developing the skill of endotracheal intubation: implication for emergency medicine. Acta Anaesthesiol Scand 2012;56(2):164-71.
13. Arima T, Nagata O, Miura T, et al. Comparative analysis of airway scope and Macintosh laryngoscope for intubation primarily for cardiac arrest in prehospital setting. The American journal of emergency medicine 2013;32(1):40-3.
14. Jarvis JL, McClure SF, Johns D. EMS Intubation Improves with King Vision Video Laryngoscopy. Prehosp Emerg Care 2015;19(4):482-9.
15. Wayne MA, McDonnell M. Comparison of traditional versus video laryngoscopy in out-of-hospital tracheal intubation. Prehospital Emergency Care 2010;14(2):278-82.
16. Boehringer B, Choate M, Hurwitz S, et al. Impact of Video Laryngoscopy on Advanced Airway Management by Critical Care Transport Paramedics and Nurses Using the CMAC Pocket Monitor. BioMed Research International 2015;2015.
17. Guyette FX, Farrell K, Carlson JN, et al. Comparison of video laryngoscopy and direct laryngoscopy in a critical care transport service. Prehospital Emergency Care 2013;17(2):149-54.
18. Trimmel H, Kreutziger J, Fertsak G, et al. Use of the Airtraq laryngoscope for emergency intubation in the prehospital setting: A randomized control trial. Critical Care Medicine 2011;39(3):489-93.
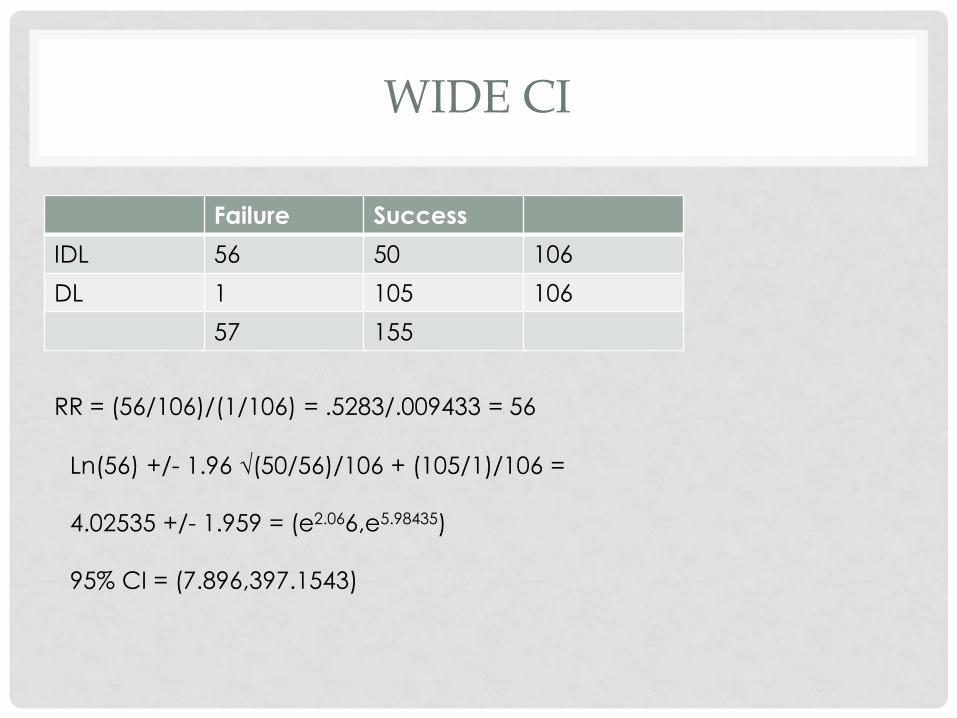
WIDE CI
Failure Success
IDL 56 50 106
DL 1 105 106
57 155
RR = (56/106)/(1/106) = .5283/.009433 = 56
Ln(56) +/- 1.96 √(50/56)/106 + (105/1)/106 =
4.02535 +/- 1.959 = (e2.066,e5.98435)
95% CI = (7.896,397.1543)