concurrent use of alcohol interactive medications and
TRANSCRIPT

RESEARCH ARTICLE Open Access
Concurrent use of alcohol interactivemedications and alcohol in older adults:a systematic review of prevalence andassociated adverse outcomesAlice E. Holton1*, Paul Gallagher1, Tom Fahey2 and Gráinne Cousins1
Abstract
Background: Older adults are susceptible to adverse effects from the concurrent use of medications and alcohol.The aim of this study was to systematically review the prevalence of concurrent use of alcohol and alcohol-interactive (AI)medicines in older adults and associated adverse outcomes.
Methods: A systematic search was performed using MEDLINE (PubMed), Embase, Scopus and Web of Science (January1990 to June 2016), and hand searching references of retrieved articles. Observational studies reporting on the concurrentuse of alcohol and AI medicines in the same or overlapping recall periods in older adults were included. Twoindependent reviewers verified that studies met the inclusion criteria, critically appraised included studies andextracted relevant data. A narrative synthesis is provided.
Results: Twenty studies, all cross-sectional, were included. Nine studies classified a wide range of medicines as AI usingdifferent medication compendia, thus resulting in heterogeneity across studies. Three studies investigated any medicationuse and eight focused on psychotropic medications. Based on the quality assessment of included studies, the mostreliable estimate of concurrent use in older adults ranges between 21 and 35%. The most reliable estimate of concurrentuse of psychotropic medications and alcohol ranges between 7.4 and 7.75%. No study examined longitudinal associationswith adverse outcomes. Three cross-sectional studies reported on falls with mixed findings, while one study reported onthe association between moderate alcohol consumption and adverse drug reactions at hospital admission.
Conclusions: While there appears to be a high propensity for alcohol-medication interactions in older adults, there is alack of consensus regarding what constitutes an AI medication. An explicit list of AI medications needs to be derived andvalidated prospectively to quantify the magnitude of risk posed by the concurrent use of alcohol for adverse outcomes inolder adults. This will allow for risk stratification of older adults at the point of prescribing, and prioritise alcohol screeningand brief alcohol interventions in high-risk groups.
Keywords: Alcohol, Drug interaction, Alcohol interactive, Older adult, Psychotropic medicines, Adverse outcomes
* Correspondence: [email protected] of Pharmacy, Royal College of Surgeons in Ireland (RCSI), Dublin 2,IrelandFull list of author information is available at the end of the article
© The Author(s). 2017 Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, andreproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link tothe Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver(http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
Holton et al. BMC Geriatrics (2017) 17:148 DOI 10.1186/s12877-017-0532-2

BackgroundBy 2050, older adults aged ≥60 years are expected to ac-count for 34% of the population in Europe [1]. While al-cohol consumption changes over the life-course, with adecline in consumption in older age, recent evidencefrom nine UK based prospective cohort studies, haveshown that drinking occasions tend to become more fre-quent among older adults [2]. There is also evidence of acohort effect, with successive birth cohorts reporting anincrease in alcohol consumption across all age-groups,including among older adults [3].Even at relatively low levels of alcohol consumption,
older adults can be vulnerable to harm, with physio-logical changes exacerbating these harms [4, 5]. Further-more, older adults experience a disproportionate burdenof alcohol related-harm; in England between 2009 and2010, adults aged ≥65 years accounted for approximately44% (461,400) of alcohol-related hospital admissions yetcomprised of only 17% of the population [6, 7]. Alcohol-related deaths were also highest among those aged 55 to74 years [4].Furthermore, the use of multiple medicines is increas-
ing in older adults [8–11]. A recent Irish study reportedan increase in polypharmacy from 17.8 to 60.4% betweenthe years 1997–2012 in older adults aged ≥65 years [11].Certain medications have the potential to interact withalcohol; these medications are referred to as alcoholinteractive (AI) medications [12]. They may interact withalcohol by altering the metabolism (pharmacokinetic) oreffects (pharmacodynamic) of alcohol and/or the medi-cation [12]. Certain interactions may occur with any al-cohol consumption, whereas other interactions mayfollow a dose response, with the risk or severity of aninteraction increasing with increasing levels of alcohol[13]. AI medications, when combined with alcohol, in-crease the risk of medical complications such ashypoglycaemia, hypotension, sedation, gastrointestinalbleeds and liver damage, in older adults [5, 12]. For ex-ample, older adults are vulnerable to the sedating effectsof alcohol and when combined with central nervous sys-tem (CNS) agents, such as psychotropic medications,older adults have an increased risk of sedation anddrowsiness [5]. Psychotropic medicines include antide-pressants, sedatives/hypnotics, stimulants and neurolep-tics, all of which act on the CNS and are commonlyprescribed to older adults [14]. Similarly, concurrent useof alcohol with cardiovascular agents, such as vasodila-tory agents, increases the risk of hypotension in olderadults [5], with concurrent use with non-steroidal anti-inflammatory drugs (NSAIDs) increasing the risk ofgastrointestinal bleeds [12].While a recent systematic review has assessed the
prevalence of concurrent alcohol use and prescriptionsedative-hypnotic medicines in middle-aged and older
adults, [15] there have been no systematic reviews onthe prevalence of concurrent use of alcohol and alcoholinteractive medications beyond psychotropic medica-tions and associated adverse outcomes in older adults.An older review did investigate the potential risk ofcombining alcohol with medications in older adultshowever the focus of the review was on the pharmacol-ogy and mechanism of action involved in alcohol-medication interactions and potential clinical implica-tions of these interactions [5]. Therefore this study aimsto systematically review the prevalence of concurrentuse of alcohol and alcohol interactive medications inolder adults and associated adverse outcomes.
MethodsThis systematic review was performed according to Pre-ferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines [16].
Search strategyA comprehensive systematic search was performed usingMEDLINE (PubMed), Embase, Scopus and Web of Sci-ence. A combination of the following keywords and MeSHterms were used: “ethanol”, “alcohol”, “drug interactions”,“drug alcohol interaction” and “aged”. This search wassupplemented by a search in Google Scholar and by handsearching references of retrieved articles. The search wasrestricted to English language articles and articles pub-lished since January 1990 to June 2016.
Study selection and data extractionStudies were included if they met the following eligibilitycriteria: Observational studies reporting on the concur-rent use of alcohol and alcohol interactive (AI) medi-cines in the same or overlapping recall periods in olderadults. Studies also had to report on the quantity or fre-quency of alcohol consumption. We excluded studieswhich exclusively sampled patients with specific ill-nesses, or those seeking treatment for alcohol use disor-ders (AUD) or illicit drug use.Title and abstracts of identified studies were reviewed
by one reviewer (AH) to determine potential eligibility.Full text articles were then reviewed by two reviewers(AH/GC) for those studies considered eligible from title/abstract, or when it was unclear whether a study met theinclusion criteria. The following data were extracted bytwo reviewers (AH/GC): year of publication, country,study sample, study design, measurement and definitionof alcohol interactive (AI) medications, measurement ofalcohol consumption, prevalence of alcohol use and AImedication use and prevalence of concurrent alcoholand AI medication use. Adverse outcomes associatedwith concurrent use of alcohol and AI medications werealso extracted if reported. Any uncertainty in relation to
Holton et al. BMC Geriatrics (2017) 17:148 Page 2 of 16

study eligibility and data extraction was resolved throughdiscussion between two reviewers (GC/AH).
Critical appraisalThe risk of bias was evaluated, by two reviewers (AH/GC), using an adapted form of the Newcastle Ottawa co-hort scale (NOS) [17]. This amended NOS scale allowedfor the evaluation of cross-sectional studies, focussingon the risk of selection bias and information bias, specif-ically misclassification bias of both exposures (alcoholand AI medications) and the outcome (concurrent useof alcohol and AI medications) across included studies.
ResultsOf the 546 citations identified from this search strategy,108 full text articles were assessed for eligibility, with 20studies meeting the inclusion criteria [14, 18–36] (Fig. 1).
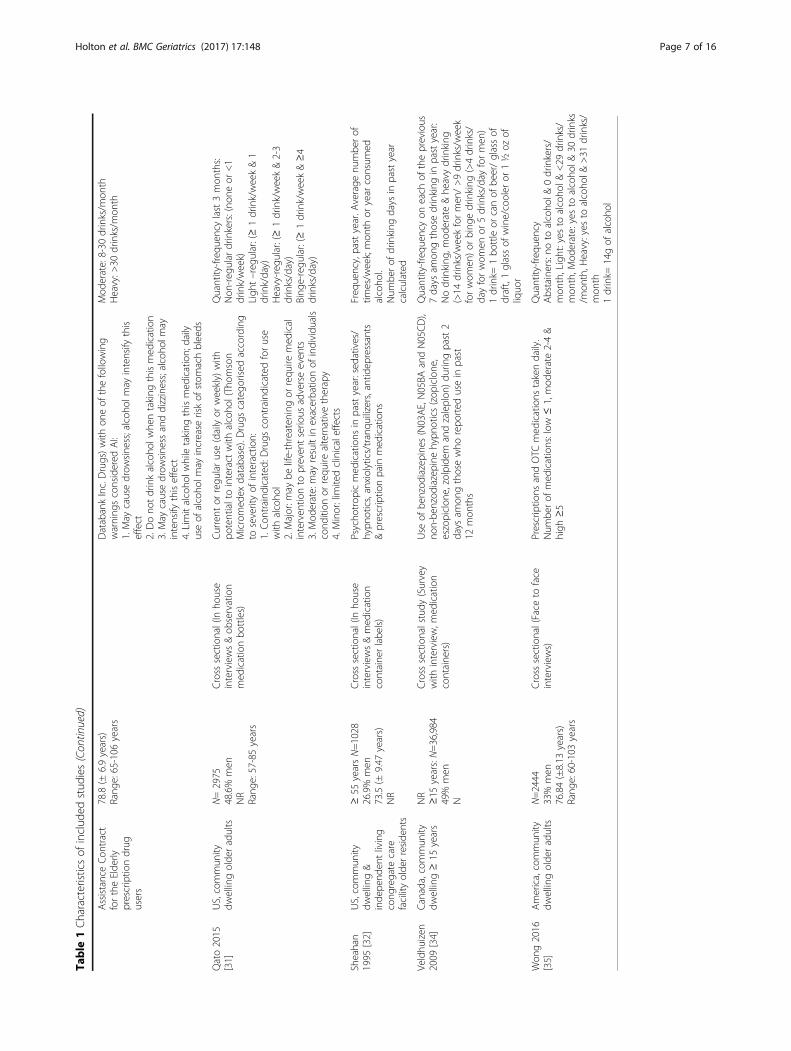
Study characteristicsTen of the included studies were conducted in Europe[14, 19, 21–23, 25, 27–29, 36], eight in North America[18, 20, 24, 30–32, 34, 35] and two in Australia [26, 33].(Table 1) All studies were cross-sectional [14, 18–36].Study settings varied across studies with; community-dwelling [14, 19, 21–27, 31, 34–36], both communitydwelling or living independently in care facilities [32],general populations [20, 28, 33], hospital setting [29], re-tirement communities [18] and participants signed up toa pharmaceutical assistance contract for the elderly [30]reported.Sample sizes varied from 311 to 83,321 participants
[18, 30] . Men and women were included in all studies,with the exception of one Australian study which only in-cluded men [26]. Nine studies reported on a wide range ofprescription and/or over the counter (OTC) medicines withpotential to interact with alcohol [18–21, 24, 27, 29–31] .Three studies investigated any medication use during therecall period [23, 33, 35], and a further eight focused onpsychotropic medications [14, 22, 25, 26, 28, 32, 34, 36]. Ofthe eight studies focusing on psychotropic medications, fiveinvestigated psychotropic medications alone [22, 25, 26, 34,36] and three studies also included analgesics [14, 28, 32].Of the nine studies focusing on a wide range of AI med-
ications, all studies classified central nervous system(CNS) agents as AI medications (Table 1). Consistent withthose studies investigating psychotropic medications[14, 22, 25, 26, 28, 32, 34, 36], the following drugclasses were classified as AI medications, sedatives/hypnotics [18–21, 24, 27, 30, 31], antidepressants[18–21, 27, 30, 31], opioids/narcotics [18–21, 27, 30,31], anticonvulsants [19–21, 24, 27, 30, 31] and anti-psychotics [19–21, 27, 29, 30]. After CNS agents, car-diovascular medicines (CVS) were the most commonAI medicines [18–21, 24, 27, 29–31], followed by
antidiabetic drugs [18, 20, 21, 24, 27, 29–31], warfarin[18–21, 24, 27, 30, 31], gastrointestinal agents [18–21,24, 30, 31], non-steroidal anti-inflammatory drugs(NSAIDs) [18–21, 29–31], antibiotics/anti-infectives [21,24, 27, 29–31] and anti-histamines [19–21, 30].
Quality assessmentThe methodological quality of the included studies is de-tailed in Table 2. The external validity was high in 4studies, as they reported on random population samplesof community dwelling older adults aged ≥60 or≥65 years [21, 24, 27] or in the case of Breslow et al., arandom population sample with oversampling of olderadults aged ≥60 years [20]. Ten studies were consideredto have moderate external validity; five studies sampledrandom community dwelling older adults but with agerestrictions which may have introduced selection bias[14, 19, 25, 26, 31] such as including adults aged be-tween 53 and 75 years [25] or only including adults≥75 years [19]. A further five studies reported on ran-dom population samples of community dwelling adultswith subgroup analysis of older adults, however they didnot report oversampling of older adults [22, 23, 28, 33, 34].The six remaining studies were considered to have poorexternal validity, as the risk of selection bias is consideredto be high [18, 29, 30, 32, 35, 36]. For example, Pringle etal. recruited enrollees in the Pennsylvania pharmaceuticalassistance contract for the elderly, which may not be repre-sentative of all older adults as the members are older(mean age 78.8 years) and more likely to be female andwhite with multiple chronic conditions [30].Internal validity was assessed by evaluating the potential
risk of misclassification bias for both exposure and out-come across studies. Ten studies were considered to have alow risk of misclassifying exposure to medications whichhave the potential to interact with alcohol, as they usedprescription claims data or in house inventories where theyrecorded details from the labels of medication containersor prescriptions and provided references supporting the in-clusion of medicines as potentially alcohol interactive(Table 2) [14, 20, 21, 25, 26, 28, 30–32, 34]. The potentialfor misclassification bias was considered high in theremaining studies as they relied on self-report for medica-tion exposure [18, 22, 23, 27, 29, 33, 35, 36] and/or did notprovide references supporting the inclusion of medicinesas potentially alcohol interactive [19, 23, 24, 29, 33, 35].While all studies relied on self-reported alcohol con-
sumption, thus introducing potential biases in recall andreporting, 11 studies were considered to have a lowerrisk of bias as they reported on both quantity and fre-quency of alcohol consumption within a specified recallperiod, ranging from 1 week to 12 months (Table 2)[14, 18–23, 25, 26, 31, 34]. The risk of misclassificationbias, specifically underestimating exposure to alcohol, was
Holton et al. BMC Geriatrics (2017) 17:148 Page 3 of 16

considered to be higher in the remaining studies as theyused quantity or frequency measures alone [24, 32, 35],did not specify the recall period [24, 27, 30, 35], restrictedmeasurements to wine consumption [29, 36] and used avery narrow recall period “last working day or last week-end” [28]. Ascertainment of exposure to alcohol was un-clear in one study [33].In relation to outcome assessment, no study directly
measured the concurrent use of alcohol and AI medica-tions, rather all studies inferred concurrent use. Althoughpossible for all studies, the risk of misclassifying the out-come of concurrent use was considered lowest in thosestudies identified as having a low risk of misclassifying
exposure, who used the same recall period for both expo-sures or inferred concurrent use based on alcohol con-sumption within a specific recall period, ranging between1 week and 12 months, and current or regular medicationuse (Table 2) [14, 20, 21, 25, 26, 31, 34].
Summary of findingsAs noted in Table 1, all estimates relate to studies fromNorth America, Europe and Australia.
Alcohol consumptionThe prevalence of alcohol consumption ranged between57 and 63% in studies reporting on nationally representative
Fig. 1 Flow diagram of studies included in this review
Holton et al. BMC Geriatrics (2017) 17:148 Page 4 of 16

Table
1Characteristicsof
includ
edstud
ies
Reference
Setting
Participants:N
,sex,m
ean
age(±sd),rang
eStud
yde
sign
(surveymod
e)Measuremen
t&D
efinition
:
AIM
edication(s)
Alcoh
olCon
sumptionQuantity/Frequ
ency;
thresholds
applied
Adams1995
[18]
UnitedStates
(US),
retirem
entcommun
ityreside
nts
N=311
23%
men
83(±
6years)
NR
Cross
sectional(Mailedself-
repo
rted
survey)
Regu
laror
occasion
aluseof
“highrisk”
med
sin
last
6mon
ths:NSA
IDS,aspirin
,sed
atives,narcotics,
antid
epressants,anti-h
ypertensives,antacids,H2
blockers,w
arfarin
&med
sforcong
estivehe
artfailure,
gout
ordiabetes.Referen
cesource
notrepo
rted
Khavariq
uestionn
aire:q
uantity
–fre
quen
cy,last6mon
ths,Non
e,1–6drinks/w
eekor
≥7drinks/w
eek
1drink=12
oz.ofbe
er,5
oz.ofwine,
3oz.offortified
wineor
1.5oz.of
hard
liquo
r.
Aira
2005
[19]
Finland,
commun
itydw
ellingolde
radults
N=521
27%
men
81(±
4.4years)
Rang
e:75–95.7years
Cross
sectional(Nurse
interview;
prescriptio
ns&containe
rs)
Current
useof
med
ications
having
potential
interactions
with
alcoho
l:Acetaminop
hen
(Paracetam
ol),anticon
vulsants,antidep
ressants,TCAs,
antih
istamines,b
enzodiazep
ines,H
2receptor
antago
nists,ne
urolep
tics,nitrates,N
SAIDs,op
iates&
warfarin
.Referen
cesource
notrepo
rted
Beverage
specificqu
antity-fre
quen
cy,
last12
mon
ths:Non
e,1–7un
its/w
eek,
>7un
its/w
eek
1unit=11-12gof
alcoho
l
Breslow
2015
[20]
US,ge
neralp
opulation
≥20
years
≥65
years
N=7183
≥20
yearsN=26,657
51%
men
NR
Cross
sectional(Interviewsin-
home,med
icationcontaine
rs)
Use
ofAIp
rescrip
tionmed
ication,pastmon
th;
iden
tifiedusing(i)
Drugs.com
,(ii)Carem
ark.com,(iii)
Health
line.com,(iv)DailyMed
databases&(v)
references
from
3pu
blications
[12,43,44]
includ
ing:
cardiovascular
agen
ts,C
NSagen
ts,coagu
latio
nmod
ifiers,GI,metabolic,p
sychothe
rape
utic&
respiratory
agen
ts
Quantity
–fre
quen
cyin
last12
mon
ths:
Non
e,forwom
enof
allage
s&men
>65
years:mod
erateconsum
ption:>0–7drinks/
week&he
avierdrinkers(>
7drinks/w
eek).
Formen
20–64yearsmod
erate:>0–14
drinks/w
eek&he
avier>14drinks/w
eek
Cou
sins
2013
[21]
Ireland
,com
mun
itydw
ellingolde
radults
≥60
years
N=3815
46.6%
males
69.7(±7.3years)
Rang
e:60–99years
Cross
sectional(Nurse
led
interviewsin-hom
e;med
ications
review
ed&self-completed
questio
nnaire)
Current
orregu
laruseof
med
ications
with
potential
tointeract
with
alcoho
lide
ntified
usingStockley’s
DrugInteractions,BritishNationalFormularyand
Irish
Med
icines
Form
ulary:cardiovascular
agen
ts,
CNSagen
ts,antihistamines,b
lood
agen
ts,
antid
iabe
ticagen
ts,anti-infectives,G
Idrugs,
immun
omod
ulators&musclerelaxants
Quantity-freq
uency,past6mon
ths:Non
e,Ligh
t/mod
erate(≤
4drinks/day
or10
drinks
/week)andhe
avydrinkers(>4drinks/day
or10
drinks/week)
1drink=10
gof
alcoho
l
DelRio
1996
[23]
Spain,commun
itydw
ellingadults
≥16
years
≥66
yearsN=3003
≥16
years
N=21,084
48%
men
NR
Cross
sectional(survey
with
interview)
Med
icationuse,past2weeks.N
oreferencesource
repo
rted
Beverage
specificqu
antity-fre
quen
cy,p
ast
2weeks
DelRio
2002
[22]
Spain,commun
itydw
ellingadults
≥16
years
≥66
years=1025
≥16
yearsN=6396
48%
men
NR
Cross
sectional(survey
with
interview)
Benzod
iazepine
use,past2weeks
Beverage
specificqu
antity-fre
quen
cypast2
weeks:Low
(men
:≤21
units/w
eek,wom
en:
≤14
units/w
eek),m
oderate(m
en:22–50
units/w
eek,wom
en:15–35
units/w
eek)&
high
consum
ption(m
en:>
50un
its/w
eek&
wom
en:>
35un
its/w
eek)
1un
it=10
gof
alcoho
l
Du2008
[14]
Germany,commun
itydw
ellingolde
radults
N=1605
45.2%
men
NR
Rang
e:60–79years
Cross
sectional(survey
&interview;p
rescrip
tions
ororiginalcontaine
rs)
Any
psycho
trop
icmed
icationusein
past7days:A
TCne
rvou
ssystem
drug
scode
dN00.(Exclud
eddrug
scode
dN02Baspirin
¶cetamol,excep
tfor
N02BA
71)O
piatecode
ines
used
asantitussiveswere
Beverage
specificqu
antity-fre
quen
cy,p
ast
12mon
ths:Prob
lem
use(riskydrinking
):daily
consum
ption≥10
gforwom
en&≥
20gformen
Holton et al. BMC Geriatrics (2017) 17:148 Page 5 of 16

Table
1Characteristicsof
includ
edstud
ies(Con
tinued)
merge
dwith
N02A&op
iatesforGIcon
ditio
ns(A07D)wereno
trecorded
Forster
1993
[24]
US,commun
itydw
ellingolde
radults
N=667
39.9%
men
74.1(±6.6years)
NR
Cross
sectional(survey
&
interview;m
edicationcontaine
rs)
Prescriptio
nor
OTC
med
ications
curren
tlyor
past
mon
th:A
Idrugs
defined
bystud
yclinicalteam
:OTC
painkillers,anti-h
ypertensives,d
iuretics,OTC
cold
prep
arations,arthritismed
ications,heartmed
ications,
antib
iotics,mindalterin
gmed
ications,che
stpain
med
ications,p
ainmed
ications,d
iabe
tesmed
ications,
ulcermed
ications,sleep
ingpills,O
TCnasalsprays,
steroids,b
lood
agen
ts,insulin,seizure
med
ications
&OTC
asthmamed
ication
Freq
uency:ne
ver,rarely,som
etim
es&
regu
larly
Ilomaki
2008
[25]
Finland,
commun
itydw
ellingolde
radults
N=1,774
48.1%
men
63years(NR)
Rang
e:53-73years
Cross
sectional(mailedsurvey
&interview;p
rescrip
tions
brou
ght
ifanyprob
lems)
Regu
laruseof
psycho
trop
icdrug
sat
timeof
interview:antipsychotics,anxiolytics,hypn
otics,
sedatives,antidep
ressants&combinatio
ns
Beverage
specificqu
antity-fre
quen
cypast
12mon
ths:fre
quen
t≥2tim
es/w
eek,bing
e(m
en≥5un
its/occasion:wom
en≥4un
its/
occasion
)&he
avydrinking
(men
:>14
units
/week:wom
en>7un
its/w
eek
1un
it=12
gof
alcoho
l
Ilomaki
2013
[26]
Australia,com
mun
itydw
ellingolde
rmen
≥70
yearsN=1,705
100%
men
NR
NR
Cross
sectional(Interview:
med
ications
brou
ght)
Antidep
ressants(includ
ingSSRIS,TC
As,MAOIsand
othe
rs)&
SADs(includ
ingbe
nzod
iazepine
sand
benzod
iazepine
-like
hypn
otics)
Beverage
specificqu
antity-fre
quen
cypast
12mon
ths:daily
(7days/w
eek),b
inge
(≥5
drinks
atleaston
ce/m
onth),he
avy(>2
drinks/day)&prob
lem
drinkers(CAGEscore
≥2).N
ondrinkers:former
orne
verdrinkers
1drink=
10gof
alcoho
l
Immon
en2012
[27]
Finland,
commun
itydw
ellingolde
radults
≥65
yearsN=1,395
35.5%
men
78.7years(NR)
NR
Cross
sectional(mailedsurvey)
Current
prescribed
med
ications:Swed
ish,Finn
ish
InteractionX-referencing(SFINX)
interaction
database
iden
tifiedsign
ificant
drug
-alcoh
olinteractions:m
etronidazole,tinidazole,disulfiram,
griseo
fulvin,p
razosin,metform
in&tacrolim
us.C
NS
agen
ts,hypog
lycaem
icsandwarfarin
Beverage
specificqu
antity-fre
quen
cy:A
trisk
(>7drinks/week,or
≥5drinks
onatypical
drinking
dayor
≥3drinks
severaltim
es/
week),m
oderatedrinkers(atleast1drink/
mon
thbu
t<7drinks/w
eek)&minim
al/non
-users(<1drink/mon
th)
1drink=12
gof
alcoho
l
John
2007
[28]
Germany,ge
neral
popu
latio
n≥20
years
NR
≥20
yearsN=4290
49%
men
NR
Rang
e:20-79years
Cross
sectional;(Interview;
containe
ror
participant
provided
inform
ationon
curren
tmed
ications)
Use
ofsedative,hypn
oticsor
anxiolytics(SHA)
med
icines
includ
ing:
barbitu
rates(&
derivatives),
benzod
iazepine
s(&
derivatives),carbam
ates,
pipe
ridined
ione
derivatives,hypno
ticsor
anxiolytics
&combinatio
nsof
sedatives
andhypn
otics.SO
grou
p:includ
edSH
Aandop
ioid,p
ast7days
Quantity
ofbe
verage
specificalcoho
lconsum
edon
lastworking
dayandlast
weekend
:Riskdrinking
(men
:>30
g/day&
wom
en>20g/day)
Lagn
aoui
2001
[36]
France,com
mun
itydw
ellingolde
radults
≥65
yearsN=3767
41.7%
men
NR
NR
Cross
sectional;(Interview
atho
me;adho
cqu
estio
nnaire;
visualinspectio
n)
Benzod
iazepine
use
Quantity:D
ailywineconsum
ptiondivide
dinto:I)no
neii)mod
erateup
to0.25
lday
-1
&iii)he
avy>0.25
lday
-1(ld
ay−1 =
litres
consum
eddaily)
Ond
er2002
[29]
Italy,hospital
admission
sam
ong
olde
radults
N=22,778
45%
men
70.3(±
16years)
NR
Cross
sectional(qu
estio
nnaire
atadmission
s)Med
ications
takenpriorto
admission
,during
hospitalstay&prescribed
atdischarge:drug
sclassifiedaccordingto
riskof
causingadversedrug
reactio
nsusingNaranjo
algo
rithm
Quantity
ofdaily
consum
ptionpriorto
hospital
admission
:(daily
wineun
its).Non
-drin
kers&
mod
eratedrinkerson
ly,heavy
alcoho
lusers
wereexclud
ed
Pringle2005
[30]
US,Penn
sylvania
Pharmaceutical
N=83,321
19%
men
Cross
sectional(survey
&prescriptio
nclaimsdata)
Filledprescriptio
ns,p
ast45
days:d
rugs
with
potentialfor
alcoho
linteractio
ns(using
First
Current
quantity-fre
quen
cy:
Ligh
t:1-7drinks/m
onth
Holton et al. BMC Geriatrics (2017) 17:148 Page 6 of 16
Table
1Characteristicsof
includ
edstud
ies(Con
tinued)
AssistanceCon
tract
fortheElde
rlyprescriptio
ndrug
users
78.8(±
6.9years)
Rang
e:65-106
years
DatabankInc.Drugs)with
oneof
thefollowing
warning
sconsidered
AI:
1.May
causedrow
sine
ss;alcoh
olmay
intensify
this
effect
2.Dono
tdrinkalcoho
lwhe
ntaking
thismed
ication
3.May
causedrow
sine
ssanddizziness;alcoho
lmay
intensify
thiseffect
4.Limitalcoho
lwhiletaking
thismed
ication;daily
useof
alcoho
lmay
increase
riskof
stom
achbleeds
Mod
erate:8-30
drinks/m
onth
Heavy:>
30drinks/m
onth
Qato2015
[31]
US,commun
itydw
ellingolde
radults
N=2975
48.6%
men
NR
Rang
e:57-85years
Cross
sectional(In
house
interviews&ob
servation
med
icationbo
ttles)
Current
orregu
laruse(dailyor
weekly)with
potentialtointeract
with
alcoho
l(Thom
son
Micromed
exdatabase).Drugs
catego
rised
according
toseverityof
interaction:
1.Con
traind
icated
:Drugs
contraindicatedforuse
with
alcoho
l2.Major:m
aybe
life-threaten
ingor
requ
iremed
ical
interven
tionto
preven
tserio
usadverseeven
ts3.Mod
erate:may
resultin
exacerbatio
nof
individu
als
cond
ition
orrequ
irealternativetherapy
4.Minor:lim
itedclinicaleffects
Quantity-freq
uencylast3mon
ths:
Non
-reg
ular
drinkers:(no
neor
<1
drink/week)
Ligh
t–reg
ular:(≥1drink/week&1
drink/day)
Heavy-reg
ular:(≥1drink/week&2-3
drinks/day)
Bing
e-regu
lar:(≥
1drink/week&≥4
drinks/day)
Sheahan
1995
[32]
US,commun
itydw
elling&
inde
pend
entliving
cong
regate
care
facilityolde
rreside
nts
≥55
yearsN=1028
26.9%
men
73.5(±
9.47
years)
NR
Cross
sectional(In
house
interviews&med
ication
containe
rlabe
ls)
Psycho
trop
icmed
ications
inpastyear:sed
atives/
hypn
otics,anxiolytics/tranqu
ilizers,antidep
ressants
&prescriptio
npain
med
ications
Freq
uency,pastyear.A
verage
numbe
rof
times/w
eek;mon
thor
year
consum
edalcoho
l.Num
berof
drinking
days
inpastyear
calculated
Veldhu
izen
2009
[34]
Canada,commun
itydw
elling≥15
years
NR
≥15
years:N=36,984
49%
men
N
Cross
sectionalstudy
(Survey
with
interview,m
edication
containe
rs)
Use
ofbe
nzod
iazepine
s(N03AE,N05BA
andN05CD
),no
n-be
nzod
iazepine
hypn
otics(zop
iclone
,eszopiclon
e,zolpidem
andzaleplon
)du
ringpast2
days
amon
gthosewho
repo
rted
usein
past
12mon
ths
Quantity-freq
uencyon
each
oftheprevious
7days
amon
gthosedrinking
inpastyear:
Nodrinking
,mod
erate&he
avydrinking
(>14
drinks/w
eekformen
/>9drinks/w
eek
forwom
en)o
rbing
edrinking
(>4drinks/
dayforwom
enor
5drinks/day
formen
)1drink=
1bo
ttleor
canof
beer/glassof
draft,1glassof
wine/cooler
or1½
ozof
liquo
r
Won
g2016
[35]
America,commun
itydw
ellingolde
radults
N=2444
33%
men
76.84(±8.13
years)
Rang
e:60-103
years
Cross
sectional(Face
toface
interviews)
Prescriptio
nsandOTC
med
ications
takendaily.
Num
berof
med
ications:low
≤1,mod
erate2-4&
high
≥5
Quantity-freq
uency
Abstainers:no
toalcoho
l&0drinkers/
mon
th,Light:yes
toalcoho
l&<29
drinks/
mon
th,M
oderate:yesto
alcoho
l&30
drinks
/mon
th,H
eavy:yes
toalcoho
l&>31
drinks/
mon
th1drink=
14gof
alcoho
l
Holton et al. BMC Geriatrics (2017) 17:148 Page 7 of 16

samples of community dwelling older adults (Table 3)[21, 24, 27]. Prevalence estimates of alcohol consump-tion were generally lower in studies sampling restrictedage-groups, for example estimates ranged between 33.7and 44% for studies restricted to older adults aged>70 years [26] and >75 years [19]. Similarly, prevalence es-timates of alcohol consumption were generally lower inthose studies considered to have a high risk of selectionbias [18, 29, 30, 32, 35]. For example, 20% of older adultsregistered on the Pennsylvania pharmaceutical assistancecontract for the elderly reported alcohol consumption[30]. All studies reporting on gender differences identifieda higher prevalence of alcohol consumption in men[19–21, 25, 29, 31, 36].
Alcohol interactive (AI) medicinesExposure to alcohol interactive medications varied acrossstudies; nationally representative studies of communitydwelling older adults using objective measures of AI ex-posure estimate exposure at between 72 and 79% amongthe total study samples (Table 3) [20, 21]. Studies with ob-jective measures of exposure to psychotropic medicationsin community dwelling older adults reported prevalenceestimates of between 11.5–20% among the total studysamples [14, 25, 26]. In contrast to alcohol consumption,
use of psychotropic medications was significantly higherin women than men [14, 22, 25, 28, 32].
Concurrent use of alcohol and AI medications amongolder adultsEleven studies reported on the concurrent use of alcoholand alcohol interactive medications among the total studysamples (Table 3) [14, 18–20, 23, 24, 31–33, 35, 36]. Eightof the 11 studies reported on alcohol consumption and awide range of medicines with potential to interactwith alcohol, with the prevalence of concurrent useranging between 18 and 39% among the total studysamples [18–20, 23, 24, 31, 33, 35]. Only two of thesestudies were considered to have a low risk of mis-classification bias for concurrent use [20, 31] . Bre-slow et al. estimated the prevalence of concurrent useamong older adults at 35% [20]. Concurrent use washighest for cardiovascular agents (28%) followed bymetabolic agents (17%), CNS agents (10%) and coagu-lation modifiers (10%). Approximately 7.75% of allolder adults were identified as concurrent users of al-cohol and psychotropic medications [20]. Qato et al.reported a prevalence estimate of 21%, with potentialalcohol-medication interactions in older adults agedbetween 57 and 84 years being significantly more
Table 2 Results of the critical appraisal of included studies
Study Representativenessof sample
Ascertainment ofalcohol consumption
Ascertainment ofAI medications(classified)
Ascertainment ofAI medications(measured)
Assessment ofthe outcome(concurrent use)
Study total:
a) Cross Sectional Studies Outcome of Interest Concurrent use of alcohol and medications:
Adams et al. 1995 [18] ++ + +++
Aira et al. 2005 [19] + ++ ++ +++++
Breslow et al. 2015 [20] ++ ++ ++ ++ ++ ++++++++++
Cousins et al. 2014 [21] ++ ++ ++ ++ ++ ++++++++++
Del Rio et al. 1996 [23] + ++ +++
Del Rio et al. 2002 [22] + ++ ++ +++++
Du et al. 2008 [14] + ++ ++ ++ ++ +++++++++
Forster et al. 1995 [24] ++ + ++ +++++
Ilomaki et al. 2008 [25] + ++ ++ ++ ++ +++++++++
Ilomaki et al. 2013 [26] + ++ ++ ++ ++ +++++++++
Immonen et al. 2012 [27] ++ + ++ +++++
John et al. 2007 [28] + + ++ ++ ++++++
Lagnaoui et al. 2001 [36] ++ ++
Onder et al. 2002 [29] + +
Pringle et al. 2005 [30] + ++ ++ +++++
Sheahan et al. 1995 [32] + ++ ++ +++++
Qato et al. 2015 [31] + ++ ++ ++ ++ +++++++++
Swift et al. 2007 [33] + +
Veldhuizen et al. 2009 [34] + ++ ++ ++ ++ +++++++++
Wong et al. 2016 [35]
Holton et al. BMC Geriatrics (2017) 17:148 Page 8 of 16

Table
3Summaryof
results;p
revalenceof
alcoho
lcon
sumption,
alcoho
linteractivemed
icationuseandconcurrent
useam
ongolde
radults
Stud
yPrevalen
ceof
alcoho
lconsum
ptionin
olde
radults(gen
der);
Heavy/Problem
drinking
(gen
der)
Prevalen
ceof
alcoho
linteractivemed
icationuse:
Con
curren
tuserepo
rted
amon
g:Totalsam
pleof
olde
radults
Con
curren
tuserepo
rted
amon
g:AIm
edicationusers
Con
curren
tuserepo
rted
amon
g:Current
drinkers
Stud
iesrepo
rtingon
awiderang
eof
alcoho
linteractive(AI)med
icines
(n=13
stud
ies)
Adams
1995
[18]
47%
drankalcoho
linprevious
6mon
ths
Heavy
(>7drinks/w
eek):8%
80%
used
oneor
moreof
thefollowingin
thelast6
mon
ths:NSA
IDS,aspirin
,sedatives,narcotics,
antid
epressants,anti-
hype
rten
sives,antacids,H
2
blockers,w
arfarin
&med
sforcong
estivehe
artfailure,
gout
ordiabetes
38%
repo
rted
concurrent
useof
alcoho
land
AI
med
ications,6%
repo
rted
concurrent
heavyalcoho
lconsum
ptionandAI
med
ications
Overalldrinkers:80%
used
anAIm
edication(50%
used
anti-
hype
rten
sives,27%
used
aspirin
,20%
used
NSA
IDs,18%
used
chroniche
artfailure
drug
s,11%
used
sedatives;5%
used
narcotics,
5%used
warfarin
,4%
used
diabeticdrug
s,3%
used
antid
epressants,3%
used
drug
sforgo
ut)
Heavy
drinkers:80%
used
anAI
med
ication(48%
used
anti-
hype
rten
sives,28%
used
aspirin
,16%
used
NSA
IDs,16%
used
chroniche
artfailure
drug
s,4%
used
sedatives,4%
used
narcotics,
4%used
warfarin
,8%
used
diabetic
drug
s,12%
used
antid
epressants,
4%used
drug
sforgo
ut)
Aira
2005
[19]
44%
drankalcoho
linprevious
12mon
ths(66%
ofmen
&37%
ofwom
en)
Heavy
(>7un
its/w
eek):7%
ofmen
&0%
ofwom
en
90%
used
oneor
moreof
thefollowingregu
larly
oras
need
ed:acetaminop
hen,
anticon
vulsants,antidep
ressants,
antih
istamines,b
enzodiazep
ines,
histam
ineH2receptor
agon
ist,
neurolep
tics,nitrates,N
SAIDs,
opiatesor
warfarin
39%
repo
rted
concurrent
useof
alcoho
land
AI
med
ications,1.9%
repo
rted
concurrent
heavyalcoho
lconsum
ptionandAI
med
ications.C
oncurren
talcoho
land
specificAI
med
ications:7.5%
acetam
inop
hen,0.19%
anticon
vulsants,5.16%
antid
epressants,0.76%
antih
istamines,11%
benzod
iazepine
s,1.15%
histam
ineH2receptor
agon
ist,2.29%
neurolep
tics,
23%
nitrates,29%
NSA
IDs,
3.8%
opiates&3.6%
warfarin
OverallAIm
edication
users:44%
drankalcoho
l(36%
acetam
inop
hen
users,17%
anticon
vulsants
users,40%
antid
epressants
users,21%
antih
istamines
users,38%
benzod
iazepine
users,43%
histam
ineH2
receptor
agon
istusers,
25%
neurolep
ticusers,
43%
nitrateusers,46%
NSA
IDusers,38%
opiate
users&40%
warfarin
users)
Overalldrinkers:88%
used
AI
med
ications
Breslow
2015
[20]
47%
drankalcoho
linprevious
12mon
ths(55%
ofmen
&39.7%
ofwom
en)
78.6%
used
oneor
moreof
the
following:
cardiovascular
agen
ts,
CNSagen
ts,coagu
latio
nmod
ifiers,GIage
nts,metabolic
agen
ts,p
sychothe
rape
utic
agen
ts,respiratory
agen
ts
35%
repo
rted
concurrent
useof
alcoho
land
AI
med
ications.C
oncurren
talcoho
land
specificAI
med
ications:28%
cardiovascular
agen
ts,10%
OverallAIm
edication
users:45%
drankalcoho
l(44%
cardiovascular
agen
tsusers,40%
CNS
agen
tusers(34%
anticon
vulsants,40%
Overalldrinkers:77.8%
took
AI
med
ications
(61.3%
used
cardiovascular
agen
ts,
22%
used
CNSagen
t(3.9%
used
anticon
vulsants,4.6%
used
anxiolytic/sed
ative/hypn
otic,4.8%
Holton et al. BMC Geriatrics (2017) 17:148 Page 9 of 16

Table
3Summaryof
results;p
revalenceof
alcoho
lcon
sumption,
alcoho
linteractivemed
icationuseandconcurrent
useam
ongolde
radults(Con
tinued)
CNSagen
ts(1.8%
anticon
vulsants,2%
anxiolytic/sed
ative/hypn
otic,
2%narcotics,2.2%
NSA
IDs),
3%coagulationmod
ifiers,
2.2%
GIage
nts,16.9%
metabolicagen
ts,3.9%
psycho
therapeutic
agen
ts(3.8%
antid
epressants),2.1%
respiratory
agen
ts
anxiolytic/sed
ative/
hypn
otic,43%
NSA
ID),
44%
coagulationmod
ifier
users,43%
GIage
ntusers,
43%
metabolicagen
tusers,
41%
psycho
therapeutic
agen
tusers(42%
antid
epressants),48%
respiratory
agen
tusers)
used
NSA
ID),6%
used
coagulation
mod
ifier,4.7%
used
GIage
ntusers,
36.5%
used
metabolicagen
t,9.6%
used
psycho
therapeutic
agen
t(9.2%
used
antid
epressants),4.6%
used
respiratory
agen
t)
Cou
sins
2013
[21]
62.8%
drankalcoho
lpreviou
s6mon
ths(72%
ofmen
&59%
ofwom
en)
Heavy
(>4drinks/day
or>10
drinks/w
eek):20%
(32%
ofmen
&11%
ofwom
en)
CAGE:8%
(12.2%
ofmen
&4%
ofwom
en)
72%
took
oneor
moreof
the
following:
cardiovascular
agen
ts,
CNSagen
ts,antihistamines,
Bloo
d,antid
iabe
ticagen
ts,anti-
infectives,G
Iage
nts,
immun
omod
ulatorsor
muscle
relaxants
OverallAIm
edication
usersconcurrent
useof
alcoho
l:60%
drankalcoho
l(60%
cardiovascular
agen
tusers,53.5%
CNSagen
tusers(59%
ofNSA
IDusers,
54%
hypn
oticusers,44%
anxiolyticusers,52.9%
antid
epressantusers),
66.9%
antih
istamineusers,
58.5%
bloo
dmed
ication
users,54%
antid
iabe
ticagen
tusers,47%
anti-
infectiveusers,50%
GI
agen
tusers,51%
immun
omod
ulator
users
&80.3%
musclerelaxant
users)
AIm
edicationusers
concurrent
heavyalcoho
lconsum
ption:25%
antih
istamineusers,20%
cardiovascular
agen
tusers,
20%
bloo
d(anti-coagu
lant
oranti-platelet)users,20%
anti-diabeticagen
tusers,
16%
CNSagen
tusers(13%
usersof
anti-ep
ileptic
agen
ts;13%
antip
sychotic
agen
ts;13%
hypn
oticusers
&18%
antid
epressantusers)
DelRio
1996
[23]
App
roximately20%
drank
alcoho
latleaston
cepe
rday
inthepast2weeks
75–80%
took
oneor
more
med
icationin
previous
2weeks
18%
repo
rted
concurrent
useof
alcoho
land
AI
med
ications
Forster
1993
[24]
57.1%
repo
rted
usingalcoho
l16.9%
admitted
todrinking
enou
ghto
become“ligh
theade
d”
Not
Repo
rted
25%
repo
rted
concurrent
useof
alcoho
land
AI
med
ications.C
oncurren
talcoho
land
specificAI
Holton et al. BMC Geriatrics (2017) 17:148 Page 10 of 16

Table
3Summaryof
results;p
revalenceof
alcoho
lcon
sumption,
alcoho
linteractivemed
icationuseandconcurrent
useam
ongolde
radults(Con
tinued)
med
ications:19%
OTC
analge
sics,6.9%
antih
ypertensives,5.4%
diuretics;4.3%
OTC
cold
prep
arations,2.1%
mind
alterin
gdrug
s,1.5%
diabetes
pills,1.5%
prescriptio
npain
med
ication,
1.2%
sleeping
pills,0.6%
prescriptio
nbloo
dthinne
rs,
0.6%
insulin
&0.3%
seizure
med
ications
Immon
en2013
[27]
62.6%
drankalcoho
lAtriskdrinking
(>7drinks/w
eek,
or≥5drinks
ontypicald
rinking
day,or
≥3drinks
severaltim
es/
week):7.9%
42%
took
oneor
moreof
the
following:
metronidazole,
tinidazole,disulfiram,g
riseo
fulvin,
prazosin,m
etform
in&tacrolim
us.
CNSagen
ts,hypog
lycaem
icsand
warfarin
OverallAIm
edication
users:62.2%
drankalcoho
lHeavy
orat
riskdrinkers:42.2%
%took
AIm
edications
(2.2%
used
antip
sychotics,4.4%
used
anti-
depressant,6.7%
used
anxiolytics,
11.1%
used
hypn
otics/sedatives,
5.6%
used
anti-ep
ileptics,3.3%
used
opioids,11.1%
used
warfarin
&13.3%
used
metform
in)
Ond
er2002
[29]
54.2%
drank≤40
gof
wine/day
priorto
hospitaladm
ission
(68.
1%of
men
&42.8%
ofwom
en)
27%
used
diuretics,23%
digo
xin,
17.7%
calcium
channelb
lockers,
16%
ACEinhibitors,15%
aspirin
&anti-platelets,9%
oral
hypo
glycaemicagen
ts,6%
NSA
IDs,
6%antib
iotics,5.2%
nitrates,5%
insulin,4%
steroids
&3.2%
antip
sychotics
Overallwinedrinkers:26%
used
diuretics,3.8%
oralhypo
glycaemic
agen
ts,2.6%
antip
sychotics&1.8%
insulin
Pringle
2005
[30]
20.3%
drankalcoho
lHeavy
(>30
drinks/m
onth):1.2%
77.4%
used
onor
moreAI
med
ication
OverallAIm
edication
usersconcurrent
useof
alcoho
l:19%
drankalcoho
l(18.4%
cardiovascular
agen
tusers,18%
CNSagen
tusers
(20%
ofNSA
IDusers,16.8%
anxiolytic/hypno
tic/sed
ative
users&
16%
antid
epressant
users),20%
antih
istamine
users,14%
bloo
dmed
icationusers,13%
antid
iabe
ticagen
tusers,
16%
anti-infectiveusers,
14%
GIage
ntusers&16%
musclerelaxant
users)
Qato2015
[31]
41%
wereregu
lardrinkersin
the
past3mon
ths(59.3%
ofmen
&40.7%
ofwom
en)
Heavy
(2–3
drinks/day):19.7%
57.7%
used
atleaston
eAIm
edication.
21%
repo
rted
concurrent
useof
alcoho
land
AI
med
ications
Overalldrinkers(Reg
ular
drinkers):
51%
used
AIm
edications
(8.4%
used
antid
iabe
ticagen
ts,6.6%
used
analge
sics,2.4%
used
narcotics,5.3%
used
acetam
inop
hen,26.7%
used
Holton et al. BMC Geriatrics (2017) 17:148 Page 11 of 16

Table
3Summaryof
results;p
revalenceof
alcoho
lcon
sumption,
alcoho
linteractivemed
icationuseandconcurrent
useam
ongolde
radults(Con
tinued)
aspirin
,18.9%
used
psycho
trop
icmed
ication,8.5%
used
antid
epressants,6%
used
anxiolytic/sed
ative/hypn
otics&
4%used
warfarin
)
Swift
2007
[33]
18%
drankalcoho
ldailyin
past
12mon
ths
87.3%
used
atleaston
eAIm
edicationin
last
24h
35.4%
repo
rted
concurrent
useof
alcoho
land
AI
med
ications
inprevious
24h
Won
g2016
[35]
38%
consum
edalcoho
lHeavy
(>31
drinks/m
onth):6%
83%
repo
rted
anymed
ication
use
31%
repo
rted
concurrent
useof
alcoho
land
med
ications&1.4%
repo
rted
concurrent
heavyalcoho
lconsum
ptionandmed
ication
use
Stud
iesrepo
rtingon
psycho
trop
icmed
icines
(n=8stud
ies)
DelRio
2002
[22]
Not
Repo
rted
13.4%
used
benzod
iazepine
sin
previous
2weeks
Overallbe
nzod
iazepine
usersconcurrent
useof
alcoho
l:23%
(56–66
years),
approx.15%
(66–75
years)
&approx.10%
(>75
years)
Du2008
[14]
47.3%
drankalcoho
latleaston
cein
thelast-w
eek
Heavy
drinking
(≥10
g/dayfor
wom
en/≥20
g/dayformen
):14.8%
20%
repo
rted
useof
atleaston
epsycho
trop
icmed
ication.
7.4%
repo
rted
concurrent
useof
alcoho
land
psycho
trop
icmed
ications
&2.4%
repo
rted
concurrent
heavyalcoho
lcon
sumption
andpsycho
trop
icmed
ication
use
Overallpsycho
trop
icmed
icationusersconcurrent
useof
alcoho
l:37.5%
Overalldrinkers:16%
used
psycho
trop
icmed
ication
Ilomaki
2008
[25]
76.7%
drankalcoho
linprevious
year
(87.5%
ofmen
&68.9%
ofwom
en)
Heavy
drinking
(>14
units/w
eek
men
&>7un
its/w
eekwom
en):
12.6%
(16.6%
ofmen
&7.9%
ofwom
en)
11.5%
repo
rted
useof
atleaston
epsycho
trop
icmed
ication
Overallpsycho
trop
icmed
icationusersconcurrent
useof
alcoho
l:38.9%
ofmaleusers&14.7%
offemale
userswerefre
quen
tdrinkers,
25.9%
ofmaleusers&8.3%
offemaleuserswerehe
avy
drinkers
Ilomaki
2013
[26]
33.7%
drankalcoho
ldailyin
the
past12
mon
ths
Heavy
drinking
(>2drinks/day):
19.2%
Prob
lem
drinkers(CAGE):11%
13.6%
repo
rted
useof
atleaston
epsycho
trop
icmed
ication(8%
repo
rted
antid
epressantuse,
5.7%
sedativeor
anxiolyticsuse&1.6%
both
drug
classes)
Overallantid
epressantusers:
27.1%
consum
edalcoho
ldaily
&15%
heavydrinkers
Sedativeor
hypn
oticusers:
42.7%
consum
edalcoho
ldaily
&26%
heavydrinkers
John
2007
[28]
Prevalen
ceno
trepo
rted
Riskydrinking
(>20
g/daywom
en&>30
g/daymen
):15.1%
ofmen
&3.2%
ofwom
en(exclude
susers
Men
:3.8%
used
sedative,hypn
otic,anxiolytic;1%
used
opioids
Wom
en:6.8%
used
sedative,hypn
otic,anxiolytic;
1.6%
used
opioids
Men
:Riskdrinkers(non
-smoker)
useof
sedative,hypn
oticor
anxiolytic:4.3%
of60–79year
olds
Holton et al. BMC Geriatrics (2017) 17:148 Page 12 of 16

Table
3Summaryof
results;p
revalenceof
alcoho
lcon
sumption,
alcoho
linteractivemed
icationuseandconcurrent
useam
ongolde
radults(Con
tinued)
ofsedative-hypn
otic-anxiolytics
andop
ioids)
Men
:Riskdrinkers(smokers)useof
sedative,hypn
oticor
anxiolytic:
0%of
60–79year
olds
Wom
en:Riskdrinker(non
-smoker)
useof
sedative,hypn
oticor
anxiolytic:13%
of60–79year
olds
Wom
en:Riskdrinkers(smokers)
useof
sedative,hypn
oticor
anxiolytic:0%
of60–79year
olds
Lagn
aoui
2001
[36]
56.3%
drankwine(77.2%
ofmen
&41.1%
ofwom
en)
Heavy
drinking
>0.25
lwine/day:
15.3%
(32.3%
ofmen
&3.1%
ofwom
en)
32%
used
benzod
iazepine
s15.7%
repo
rted
concurrent
useof
alcoho
l(wine)
and
benzod
iazepine
s&2.9%
repo
rted
concurrent
heavy
alcoho
lcon
sumption(wine)
andbe
nzod
iazepine
use
Overallbe
nzod
iazepine
users:49%
consum
edwine
&9.2%
heavydrinkers
Overallwinedrinkers:28.1%
used
benzod
iazepine
s&he
avywine
drinkers:5.3%
used
benzod
iazepine
s
Sheahan
1995
[32]
38%
drankalcoho
linthepast
12mon
ths
28%
repo
rted
useof
atleast
onepsycho
trop
icmed
ication
2%repo
rted
concurrent
useof
alcoho
land
psycho
trop
icmed
ication
Veldhu
izen
2009
[34]
Not
repo
rted
Not
repo
rted
Overallbe
nzod
iazepine
users:33.9%
consum
edalcoho
l&5.1%
werehe
avy
drinkers
Holton et al. BMC Geriatrics (2017) 17:148 Page 13 of 16

likely among men, white respondents, wealthier re-spondents, and those with higher education levels andgreater comorbidities [31]. The prevalence of concur-rent use was lower in studies which focused on psy-chotropic medications, ranging between 2 and 15.7%[14, 32, 36]. Only one study was identified as havinga low risk of misclassifying concurrent use in olderadults [14], with an estimated prevalence of 7.4%among the total study sample and 2.4% for concur-rent heavy alcohol consumption and psychotropicmedications. Older age (70–79 years), residing inrural or small town areas, living alone, higher socialstatus, polypharmacy and a poor social network wereindependently associated with concurrent use of alco-hol and psychotropic medications [14]. While ahigher proportion (15.7%) of older adults in a Frenchstudy [36] were identified as concurrent users of wineand benzodiazepines, the methods of ascertaining ex-posure to benzodiazepines was unclear, as was the as-sessment of concurrent use. Similarly, the lowerestimate of 2% for concurrent use of alcohol and psy-chotropic medications in Sheahan et al. [32] is likelyan artefact of their sample including patients in con-gregate care facilities.Five studies assessed the prevalence of alcohol con-
sumption among users of a broad range of alcohol inter-active medications (Table 3) [19–21, 27, 30]. Breslow[20] and Cousins [21] were identified as having a lowrisk of misclassifying concurrent use, and reportedprevalence estimates of 45 and 60% respectively. Cousinset al. [21] found that older adults using AI medicationswere significantly less likely to report alcohol consump-tion compared to those unexposed to AI medications.Younger age (60–64 years), men, urban dwelling, higherlevels of education and a history of smoking were inde-pendently associated with concurrent use of alcohol andAI medications [21]. A further six studies focused onpsychotropic medication users [14, 22, 25, 26, 34, 36],four of which were identified as having a low risk of mis-classification bias [14, 25, 26, 34]. Du et al. estimated theprevalence of alcohol consumption among users of psy-chotropic medications at 37.5% [14]. Similarly, Ilomakiet al. [25] reported that 38.9% of male psychotropicmedication users, and 14.7% of their female users, con-sumed alcohol, with 26% of male and 8.3% of femaleusers identified as heavy drinkers. Male psychotropicmedication users consumed greater quantities of alcohol,and more often, than non-users. This pattern was notobserved among women [25]. Between one-third and ahalf of all sedative or hypnotic users (34–54%) have beenshown to consume alcohol [20, 21, 26, 34] with between5 and 13% drinking heavily [21, 34]. Consistent withthese findings, Ilomaki et al. [15] found that 26% of menaged greater than 70 years who use sedatives or
hypnotics drink heavily; heavy drinking and daily drink-ing was significantly higher among male sedative or hyp-notic users compared to non-users [26]. Concurrent useof alcohol among older adults taking antidepressantsranged between 42 and 53%, [20, 21] with 27% of maleusers aged greater than 70 years reporting concurrentuse [26].
Adverse outcomes associated with concurrent use ofalcohol and alcohol interactive medicationsOnly four studies reported on adverse outcomes. Threestudies reported on falls, all three studies were cross-sectional [27, 32, 35]. A study by Immonen et al. [27] of2100 older adults in Finland found that falls and injurieswhen a person has consumed alcohol in the past12 months were more common among at risk drinkers(>7 drinks/week, or ≥5 drinks drinking days or ≥3 drinksseveral times/week) using AI medications (13.8%) com-pared to AI medication-users who were not consideredas at risk drinkers (4.1%) (p < 0.001) [27]. In contrast tothese findings, Sheahan et al.’s [32] study of older adultsin America, which included patients in congregate carefacilities, found that although the number of psycho-tropic drugs was associated with an increased odds offalling, the concurrent use of alcohol and psychotropicdrugs was not. Similar non-significant associations werereported in Wong et al.’s [35] convenience sample ofolder adults in the US. One study examined the associ-ation between moderate alcohol consumption (≤ 40 g ofwine per day) and adverse drug reactions among olderadults at the point of admission to one of 81 acute carehospitals in Italy [29]. Among 22,778 participants, 3.9%were identified as having one or more adverse drug reac-tions. Moderate alcohol consumption was associatedwith a 24% increase in the odds of having an adversedrug reaction [29].
DiscussionOverall, the results of this review suggest that betweenone-in-five and one-in-three older adults are potentiallysusceptible to alcohol-medication interactions, withmore than half of AI medication users reporting alcoholconsumption [20, 21, 31]. However, these estimates needto be interpreted with caution as studies differed intheir classification of AI medications. In the absenceof an explicit list of alcohol-interactive medications,multiple drug reference sources were used acrossstudies [20, 21, 27, 30, 31]. Use of different medica-tion compendia led to a lack of consistency in the inclu-sion of AI medications across studies and may have led tothe over or under inclusion of medications [31, 37], result-ing in an over-or-under estimate of concurrent use. Therewas however consensus with regards to CNS agents; allstudies that reported on AI medicines classified CNS
Holton et al. BMC Geriatrics (2017) 17:148 Page 14 of 16

agents as alcohol interactive, specifically psychotropicmedications [14, 18–22, 24–32, 34, 36]. Based on thequality assessment of studies, the most reliable esti-mates for the concurrent use of psychotropic medica-tions and alcohol ranged between 7.4% [14] and7.75% [20].Despite the high prevalence of concurrent use among
older adults, no study examined longitudinal associa-tions with adverse outcomes. Three cross-sectional stud-ies reported on falls with mixed findings [27, 32, 35];with one study reporting on an association betweenmoderate alcohol consumption and adverse drug reac-tions among older adults at the point of admission tohospital [29]. An evidence based list of medicationswhich have a significant risk of harm to older patientswhen combined with alcohol would be useful in a clin-ical setting, allowing for the identification of older adultswhose alcohol consumption places them at increasedrisk and who would benefit from a preventative inter-vention. While recent studies have shown that cliniciansrarely undertake screening and brief interventions to re-duce alcohol consumption [38–40], flagging patients atthe point of prescribing an alcohol-interactive medica-tion may facilitate targeted screening and interventionsto reduce harm. Brief alcohol interventions in primarycare are effective in significantly reducing weekly alcoholconsumption [41]. Additionally, educating older adultsin relation to the risks associated with concurrent use ofalcohol and medications has been shown to increaseolder adults’ awareness of potential risks [42]. However,whether this intervention results in a behaviour changefor those at risk is unclear [42].This is the first systematic review to examine the
prevalence of concurrent use of alcohol and alcoholinteractive medications and associated adverse out-comes in older adults. An explicit and robust method-ology was applied to identify, critically appraise andsynthesise the study findings. However, the findings ofthe review need to be interpreted in the context of thestudy limitations. The risk of misclassification bias forboth alcohol and AI medications was high across manystudies, undermining internal validity. Furthermore, nostudy directly measured the concurrent use of alcoholand AI medications, rather all studies inferred concur-rent use. Finally, heterogeneity across studies in relationto classifying medications as alcohol interactive and inthe methods used to quantify alcohol consumption,prevent statistical pooling of data from existing studies.Variation in study setting and age restrictions, alsomake it difficult to compare prevalence of concurrentuse across studies. Furthermore, due to the current gapin the literature, the available evidence for this reviewwas restricted to three continents, Europe, NorthAmerica and Australia.
ConclusionsWhile there appears to be a high propensity for alcohol-medication interactions in community dwelling olderadults, there is a lack of consensus regarding what con-stitutes an alcohol interactive medication. An explicit listof alcohol interactive medications needs to be derived,and validated prospectively to quantify the magnitude ofrisk posed by the concurrent use of alcohol and alcoholinteractive medications for adverse outcomes in olderadults. This will allow for risk stratification of olderadults at the point of prescribing, and prioritise alcoholscreening and brief alcohol interventions in high-riskgroups.
Additional files
Additional file 1: Database search: this document describes theretrieval process of studies for the systematic review. (DOCX 14 kb)
Additional file 2: Search strategy: This file describes the searchstrategies used in Embase, PubMed, Web of Science and Scopus in orderto identify studies for this systematic review. (DOCX 15 kb)
Additional file 3: Newcastle-Ottawa Scale (NOS) adapted for cross-sectional studies. (DOC 35 kb)
Additional file 4: Table S1. Most common alcohol interactive (AI)medicines across included studies. (DOCX 281 kb)
AbbreviationsADRs: Adverse drug reactions; AI: Alcohol interactive; AUD: Alcohol usedisorder; NSAIDs: Nonsteroidal anti-inflammatory drugs; OTC: Over thecounter
AcknowledgementsNot applicable.
FundingThis study was funded by the Royal College of Surgeons in Ireland (RCSI),School of Pharmacy. The funder had no role in the design of the study andcollection, analysis, and interpretation of data or in writing the manuscript.
Availability of data and materialsAll data generated or analysed during this study are reported in themanuscript (and its Additional files 1, 2, 3 and 4).
Authors’ contributionsAH defined the research question and the methodology including thesearch strategy, performed the literature search, and reviewed all includedstudies, extracted data, performed quality assessment and drafting of themanuscript. GC conceived the research study, defined the research questionand methodology and reviewed full text articles, extracted data, and performedquality assessment. GC was also involved in writing of the paper and approvedthe final manuscript. TF defined the research question, and the methodology,reviewed the manuscript and approved this manuscript to be published. PGdefined the research question, and the methodology, reviewed the manuscriptand approved the manuscript to be published. All authors read and approvedthe final manuscript.
Ethics approval and consent to participateNot applicable.
Consent for publicationNot applicable.
Competing interestsThe authors declare that they have no competing interests.
Holton et al. BMC Geriatrics (2017) 17:148 Page 15 of 16

Publisher’s NoteSpringer Nature remains neutral with regard to jurisdictional claims in publishedmaps and institutional affiliations.
Author details1School of Pharmacy, Royal College of Surgeons in Ireland (RCSI), Dublin 2,Ireland. 2HRB Centre for Primary Care Research, Department of GeneralPractice, Royal College of Surgeons in Ireland (RCSI), Dublin 2, Ireland.
Received: 18 January 2017 Accepted: 4 July 2017
References1. United Nations, Department of Economic and Social Affairs PD. World
Population Prospects: The 2015 Revision, Key Findings and Advance Tables.New York: 2015.
2. Britton A, Ben-Shlomo Y, Benzeval M, Kuh D, Bell S. Life course trajectoriesof alcohol consumption in the United Kingdom using longitudinal datafrom nine cohort studies. BMC Med. 2015;13:47.
3. Meng Y, Holmes J, Hill-McManus D, Brennan A, Meier PS. Trend analysis andmodelling of gender-specific age, period and birth cohort effects onalcohol abstention and consumption level for drinkers in great Britain usingthe general lifestyle survey 1984–2009. Addiction. 2014;109
4. Wadd S, Papadopoulos C. Drinking behaviour and alcohol-related harm amongstolder adults: analysis of existing UK datasets. BMC Res Notes. 2014;7:741.
5. Moore AA, Whiteman EJ, Ward KT. Risks of combined alcohol/medicationuse in older adults. Am J Geriatr Pharmacother. 2007;5(1):64–74.
6. NHS Information Centre: Statistics for Alcohol : England 2010. 2011.7. Office for National Statistics: 2010 Based Subnational Population Projections
for England 2012.8. Hovstadius B, Hovstadius K, Astrand B, Petersson G. Increasing polypharmacy -
an individual-based study of the Swedish population 2005-2008. BMC ClinPharmacol. 2010;10:16.
9. Sumukadas D, McMurdo ME, Mangoni AA, Guthrie B. Temporal trends inanticholinergic medication prescription in older people: repeated cross-sectionalanalysis of population prescribing data. Age Ageing. 2014;43(4):515–21.
10. Richardson K, Moore P, Peklar J, Galvin R, Bennett K, RA. K. Polypharmacy inadults over 50 in Ireland: Opportunities for cost saving and improvedhealthcare. A report from The Irish Longitudinal Study on Ageing (TILDA).TILDA Trinity College Dublin 2012 December 2012. Report No.
11. Moriarty F, Hardy C, Bennett K, Smith SM, Fahey T. Trends and interaction ofpolypharmacy and potentially inappropriate prescribing in primary care over 15years in Ireland: a repeated cross-sectional study. BMJ Open. 2015;5(9):e008656.
12. Weathermon R, Crabb DW. Alcohol and medication interactions. AlcoholRes Health. 1999;23(1):40–54.
13. Adams WL. Interactions between alcohol and other drugs. Int J Addict.1995;30(13–14):1903–23.
14. Du Y, Scheidt-Nave C, Knopf H. Use of psychotropic drugs and alcoholamong non-institutionalised elderly adults in Germany. Pharmacopsychiatry.2008;41(6):242–51.
15. Ilomaki J, Paljarvi T, Korhonen MJ, Enlund H, Alderman CP, Kauhanen J, et al.Prevalence of concomitant use of alcohol and sedative-hypnotic drugs inmiddle and older aged persons: a systematic review. Ann Pharmacother.2013;47(2):257–68.
16. Moher D, Liberati A, Tetzlaff J, Altman DG, Group P. Preferred reportingitems for systematic reviews and meta-analyses: the PRISMA statement. AnnIntern Med. 2009;151(4):264–9. W64
17. Herzog R, Alvarez-Pasquin MJ, Diaz C, Del Barrio JL, Estrada JM, Gil A. Arehealthcare workers’ intentions to vaccinate related to their knowledge,beliefs and attitudes? A systematic review. BMC Public Health. 2013;13:154.
18. Adams WL. Potential for adverse drug-alcohol interactions amongretirement community residents. J Am Geriatr Soc. 1995;43(9):1021–5.
19. Aira M, Hartikainen S, Sulkava R. Community prevalence of alcohol use andconcomitant use of medication - a source of possible risk in the elderlyaged 75 and older? Int J Geriatr Psychiatry. 2005;20(7):680–5.
20. Breslow RA, Dong C, White A. Prevalence of alcohol-interactive prescriptionmedication use among current drinkers: United States, 1999 to 2010. AlcoholClin Exp Res. 2015;39(2):371–9.
21. Cousins G, Galvin R, Flood M, Kennedy M-C, Motterlini N, Henman MC, et al.Potential for alcohol and drug interactions in older adults: evidence fromthe Irish longitudinal study on ageing. BMC Geriatr. 2014;14
22. Del Rio MC, Prada C, Alvarez FJ. Do Spanish patients drink alcohol whileundergoing treatment with benzodiazepines? Alcohol. 2002;26(1):31–4.
23. Del Río MC, Prada C, Alvarez FJ. The use of medication and alcohol amongthe Spanish population. Br J Clin Pharmacol. 1996;41(3):253–5.
24. Forster LE, Pollow R, Stoller EP. Alcohol use and potential risk for alcohol-related adverse drug reactions among community-based elderly. J CommunityHealth. 1993;18(4):225–39.
25. Ilomaki J, Korhonen MJ, Enlund H, Hartzema AG, Kauhanen J. Risk drinkingbehavior among psychotropic drug users in an aging Finnish population:the FinDrink study. Alcohol. 2008;42(4):261–7.
26. Ilomaeki J, Gnjidic D, Hilmer SN, Le Couteur DG, Naganathan V, CummingRG, et al. Psychotropic drug use and alcohol drinking in community-dwelling older Australian men: the CHAMP study. Drug Alcohol Review.2013;32(2):218–22.
27. Immonen S, Pitkälä K. The prevalence of potential alcohol-drug interactionsin older adults. Eur Geriatr Med. 2012;3:S134.
28. John U, Baumeister SE, Volzke H, Meyer C, Ulbricht S, Alte D. Sedative,hypnotic, anxiolytic and opioid medicament use and its co-occurrence withtobacco smoking and alcohol risk drinking in a community sample. BMCPublic Health. 2007;7:337.
29. Onder G, Landi F, Della Vedova C, Atkinson H, Pedone C, Cesari M, et al.Moderate alcohol consumption and adverse drug reactions among olderadults. Pharmacoepidemiol Drug Safety. 2002;11(5):385–92.
30. Pringle KE, Ahern FM, Heller DA, Gold CH, Brown TV. Potential for alcoholand prescription drug interactions in older people. J Am Geriatr Soc. 2005;53(11):1930–6.
31. Qato DM, Manzoor BS, Lee TA. Drug-alcohol interactions in older US adults.J Am Geriatr Soc. 2015;63(11):2324–31.
32. Sheahan SL, Coons SJ, Robbins CA, Martin SS, Hendricks J, Latimer M.Psychoactive medication, alcohol use, and falls among older adults. J BehavMed. 1995;18(2):127–40.
33. Swift W, Stollznow N, Pirotta M. The use of alcohol and medicines amongAustralian adults. Aust N Z J Public Health. 2007;31(6):529–32.
34. Veldhuizen S, Wade TJ, Cairney J. Alcohol consumption among Canadianstaking benzodiazepines and related drugs. Pharmacoepidemiol Drug Saf.2009;18(3):203–10.
35. Wong H, Heuberger R, Logomarsino J, Hewlings S. Associations betweenalcohol use, polypharmacy and falls in older adults. Nurs Older People.2016;28(1):30–6.
36. Lagnaoui R, Moore N, Dartigues JF, Fourrier A, Begaud B. Benzodiazepineuse and wine consumption in the French elderly. Br J Clin Pharmacol. 2001;52(4):455–6.
37. Vitry AI. Comparative assessment of four drug interaction compendia. Br JClin Pharmacol. 2007;63(6):709–14.
38. Brown J, West R, Angus C, Beard E, Brennan A, Drummond C, et al.Comparison of brief interventions in primary care on smoking and excessivealcohol consumption: a population survey in England. Br J Gen Pract. 2016;66(642):e1–9.
39. Hamilton FL, Laverty AA, Gluvajic D, Huckvale K, Car J, Majeed A, et al. Effectof financial incentives on delivery of alcohol screening and brief intervention(ASBI) in primary care: longitudinal study. J Public Health. 2014;36(3):450–9.
40. Deehan A, Templeton L, Taylor C, Drummond C, Strang J. Low detectionrates, negative attitudes and the failure to meet the “health of the nation”alcohol targets: findings from a national survey of GPs in England andWales. Drug Alcohol Rev. 1998;17(3):249–58.
41. Kaner EF, Beyer F, Dickinson HO, Pienaar E, Campbell F, Schlesinger C, et al.Effectiveness of brief alcohol interventions in primary care populations.Cochrane Database Syst Rev. 2007;2:CD004148.
42. Benza AT, Calvert S, McQuown CB. Prevention BINGO: reducing medicationand alcohol use risks for older adults. Aging Ment Health. 2010;14(8):1008–14.
43. National Consumers League (2013). Avoid Food Drug Interactions Food andDrug Administration Publication No. (FDA) CDER 10–1933.
44. Alcoholism NIoAAa (2014). Harmful Interactions: mixing alcohol withmedicines National Institutes of Health, US Department of Heath andHuman Services 2014.
Holton et al. BMC Geriatrics (2017) 17:148 Page 16 of 16