conditions of the carpus in the dog
TRANSCRIPT

Simultaneous carpal hyperextensionand disruption of the medial supportof the carpus in a dog that hadjumped from a first floor window
Conditions of the carpus
Antebrachiocarpal joint
Middle carpal joint
Carpometacarpal joint
in the dog
Richard Whitelockqualified from theRoyal VeterinaryCollege in 1989 andspent two years inmixed practice inGloucestershirebefore electing tofocus on small animalsurgery. He wasawarded the diplomain veterinaryradiology in 1994, theECVS diploma in smallanimal surgery in1997, and the RCVSdiploma in smallanimal surgery(orthopaedics) in1998. He is currentlya director of DaviesWhite VeterinarySpecialists nearHitchin, Hertfordshire,where he runs theorthopaedic service.He is an RCVSSpecialist in SmallAnimal Surgery(Orthopaedics) and aEuropean Specialist inSmall Animal Surgery.
70% of carpal movement
25% of carpal movement
5% of carpal movement
100° of flexion10° of hyperextension
40° of flexion
10° of flexion
RICHARD WHITELOCK
THIS article draws together the pertinent anatomy of the complex carpal joint, and outlines theinvestigation of carpal disease in the dog. The aetiology, presenting signs and treatment optionsfor orthopaedic conditions of the canine carpus are discussed.
FUNCTIONAL ANATOMY
The carpus is defiiied analtomlica-llyas a hinge joint withMosn lemet in onlC plane ( ainglymius joint). Althouohthis is essentially tr^ue, there is somile rotatory and lateiiam11OVemnent due to the comilposite artiCuLlationis betweeCnthe indi idual ctarpal bones. Ther-e .are tswo ros s of car-palbones between the distal radiUs /n-inati'and the mnetacarpalbones and conisequelltly therc arc threc joint Icvels: theproximi-.al Joint lev el is ter-miled the anitebrCachiocarpaldjoint, the intermedilte level is the middle carpal Joint anidthe dlistal level is the carpomeitacarpadl joint. The atd'Jacentbones of each rosw articulate xwith each other sia inter-
carp,al joints. The antebrachiocarpal joint accounts forthe majority of joint moiement (arounld 70 per cent),the Iiddle ccarpal jOllnt accounts for 25 pcr cCnt landthe carpomietacarpal joint tor only 5 per cenit ( Yalden1970).
The individucal rowAs of bones that comprise the calr-pus are stacked vecrtically and do not have the inherl-cnitstability that is found, for examplc, betseen the cochle.aof thc distalI tibial and the trochlea of the talus. Carpalstability is pros ided AIlmost exClusively by soft tissueconstrainits, anid it is this property that enables the joint tocope with the extreme hyper-extensionl that occuIs dulilngpropulsion Cat a gallop. Consversely, it is this propertythaltresults in such debilitating injuries xhen the soft Dorsopalmar view of the bones of the carpus.t SA Antebrachiocarpal joint, B Middle carpal joint,tissue constraints fail. Ther-e are nO continuos collaterl c Carpometacarpal joint
licyments thalt crcoss the threc ross s ot the joint, butinstead therc are strategic thicken ings of the perialrticulalr-fiascica that pros ide ligamentous Support. The prelomiii-nant collateral lig(aments ai-e the shoi-t radial (striaiglt andioblique aind short ulnar collateral ligTanimcnts. Nume-roussmlall ligamenrts uinitc the carpal boncs transversely land,are intimatcls associated with the joinit capsule, formilng
In Practice * JANUARY 2001
--, 0 0l S"
2
group.bmj.com on September 9, 2014 - Published by inpractice.bmj.comDownloaded from

Short radial - --collateral ligament
C2 LCi- -1
Radioulnar ligament
Dorsal radiocarpalligamentShort ulnarcollateral ligamentUlnar carpal bone
Short radial collateralligament
Palmar radiocarpal ligamentPalmar ulnocarpal ligament
Accessorycarpal bone
The ligaments of the leftcarpus. Reproduced, withpermission, from Miller'sAnatomy of the Dog, 3rdedition, Ed H. E. Evans,Philadelphia, W. B. Saunders
a strong restraining 'sleeve' around the entire carpus.These smaller ligaments are difficult to isolate by palpa-tion or dissection. The predominant disruptive forcesacting on the carpus are hyperextension and, to a lesserextent, lateromedial bending. Consequently it is thepalmar and abaxial aspects of the carpus that have thegreatest thickening and support.
Hyperextension is largely prevented by the palmarradiocarpal and ulnocarpal ligaments, the flexor retinac-ulum and the very substantial palmar carpal fibrocarti-lage. The palmar fibrocartilage is attached to the palmarsurfaces of all the carpal bones except the accessorycarpal bone where it has a dorsomedial attachment.Distally the fibrocartilage has a strong attachment to thedistal row of carpal bones and the proximal aspects ofmetacarpal bones III, IV and V. There are two strongligaments between the accessory carpal bone and theheads of metacarpals IV and V, which support thepalmar aspect of the middle carpal joint (accessoro-metacarpal ligaments).
The tendons, blood vessels and nerves that cross thecarpus do so superficially to this inner supportive sleeve.The superficial digital flexor, deep digital flexor and theflexor carpi radialis tendons lie within the carpal canalon the palmar aspect of the carpus. The radial, ulnar andpalmar interosseous vessels and the distal branches ofthe median and ulnar nerves also pass through this canal.
The lateral digital extensor, extensor carpi radialisand common digital extensor tendons cross the dorsalaspect of the carpus superficially to the fibrous jointcapsule. These extensor tendons lie within shallow sulcion the dorsal aspect of the distal radius and are boundeddorsally by the extensor retinaculum. Synovial sheathsenclose the tendons of both the flexor and extensor
muscles as they cross the carpus. The abductor pollicislongus crosses the dorsal aspect of the distal radiusobliquely, originating from the ulna and inserting on thefirst digit. Its tendon of insertion passes between the twoparts of the short radial collateral ligament. There is asesamoid bone within the tendon of this muscle whichlies medial to the antebrachiocarpal joint and whichshould not be confused with a fracture.
The small, round, structuredbone shadow (arrow)distomedial to theradiocarpal bone is asesamoid associated withthe abductor pollicislongus tendon, and notan avulsion fracture. Notethe fragmentation ofmetacarpophalangealsesamoid bones 4 and 7
The ligamentous support of the palmar aspect of the carpus.Hyperextension leads to disruption of one or more of thesestructures. Reproduced, with permission, from Miller's Anatomy ofthe Dog, 3rd edition, Ed H. E. Evans, Philadelphia, W. B. Saunders
In Practice * JANUARY 2001 3
group.bmj.com on September 9, 2014 - Published by inpractice.bmj.comDownloaded from
CLINICAL EXAMINATION ANDDIAGNOSTIC AIDS
The lack of muscle and fat between the skin and thecarpal joint favours direct palpation of many of the indi-vidual structures of the carpus. Mild synovial effusionsor periarticular swellings are readily identified, and paincan be accurately localised. Changes in the range of jointmotion are readily detected, as are joint instability andcrepitus. Comparison with the contralateral limb is oftenhelpful.
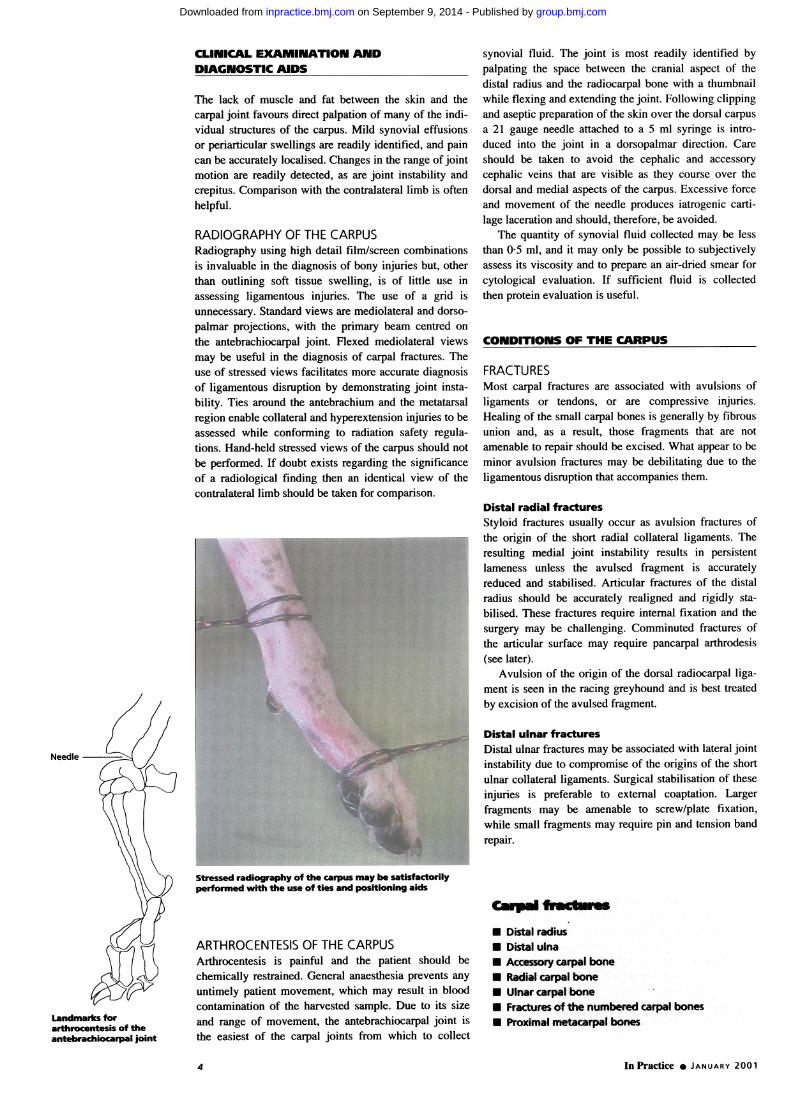
RADIOGRAPHY OF THE CARPUSRadiography using high detail film/screen combinationsis invaluable in the diagnosis of bony injuries but, otherthan outlining soft tissue swelling, is of little use inassessing ligamentous injuries. The use of a grid isunnecessary. Standard views are mediolateral and dorso-palmar projections, with the primary beam centred onthe antebrachiocarpal joint. Flexed mediolateral viewsmay be useful in the diagnosis of carpal fractures. Theuse of stressed views facilitates more accurate diagnosisof ligamentous disruption by demonstrating joint insta-bility. Ties around the antebrachium and the metatarsalregion enable collateral and hyperextension injuries to beassessed while conforming to radiation safety regula-tions. Hand-held stressed views of the carpus should notbe performed. If doubt exists regarding the significanceof a radiological finding then an identical view of thecontralateral limb should be taken for comparison.
Needle
Stressed radiography of the carpus may be satisfactorilyperformed with the use of ties and positioning aids
ARTHROCENTESIS OF THE CARPUSArthrocentesis is painful and the patient should bechemically restrained. General anaesthesia prevents anyuntimely patient movement, which may result in bloodcontamination of the harvested sample. Due to its size
and range of movement, the antebrachiocarpal joint is
the easiest of the carpal joints from which to collect
synovial fluid. The joint is most readily identified bypalpating the space between the cranial aspect of thedistal radius and the radiocarpal bone with a thumbnailwhile flexing and extending the joint. Following clippingand aseptic preparation of the skin over the dorsal carpusa 21 gauge needle attached to a 5 ml syringe is intro-duced into the joint in a dorsopalmar direction. Careshould be taken to avoid the cephalic and accessorycephalic veins that are visible as they course over thedorsal and medial aspects of the carpus. Excessive forccand movement of the needle produces iatrogenic carti-lage laceration and should, therefore, be avoided.
The quantity of synovial fluid collected may be lessthan 0-5 ml, and it may only be possible to subjectivelyassess its viscosity and to prepare an air-dried smear forcytological evaluation. If sufficient fluid is collectedthen protein evaluation is useful.
CONDITIONS OF THE CARPUS
FRACTURESMost carpal fractures are associated with avulsions ofligaments or tendons, or are compressive injuries.Healing of the small carpal bones is generally by fibrousunion and, as a result, those fragments that are notamenable to repair should be excised. What appear to beminor avulsion fractures may be debilitating due to theligamentous disruption that accompanies them.
Distal radial fracturesStyloid fractures usually occur as avulsion fractures ofthe origin of the short radial collateral ligaments. Theresulting medial joint instability results in persistentlameness unless the avulsed fragment is accuratelyreduced and stabilised. Articular fractures of the distalradius should be accurately realigned and rigidly sta-bilised. These fractures require internal fixation and thesurgery may be challenging. Comminuted fractures ofthe articular surface may require pancarpal arthrodesis(see later).
Avulsion of the origin of the dorsal radiocarpal liga-ment is seen in the racing greyhound and is best treatedby excision of the avulsed fragment.
Distal ulnar fracturesDistal ulnar fractures may be associated with lateral jointinstability due to compromise of the origins of the shortulnar collateral ligaments. Surgical stabilisation of theseinjuries is preferable to external coaptation. Largerfragments may be amenable to screw/plate fixation,while small fragments may require pin and tension bandrepair.
Carpal fractures
* Distal radius* Distal ulna* Accessory carpal bone* Radial carpal bone* Ulnar carpal bone* Fractures of the numbered carpal bones* Proximal metacarpal bones
In Practice a JANUARY 2001
Landmarks forarthrocentesis of theantebrachiocarpal joint
4
group.bmj.com on September 9, 2014 - Published by inpractice.bmj.comDownloaded from

The ulnar styloid is fractured and displaced in a palmar direction. The lateral support of the joint has been lost and there ispalpable instability in both lateral and dorsopalmar directions
Accessory carpal bone fracturesFractures of the accessory carpal bone are common inracing greyhounds and have been classified into fivetypes (Johnson 1987):* TYPE I FRACTURES affect the distal margin of the artic-ular surface of the accessory carpal bone as a result ofavulsion of the accessoroulnarocarpal ligament.* TYPE II FRACTURES affect the proximal margin of thearticular surface of the accessory carpal bone and areavulsion fractures of the palmar radiocarpal and ulno-carpal ligaments. These fractures are usually seen inassociation with type I injuries.
Type I and II fractures are articular fractures andresult in joint instability.* TYPE III FRACTURES are associated with avulsion ofthe origins of the accessoronietacarpal ligaments.* TYPE IV FRACTUREs are avulsion fractures of the
flexor carpi ulnaris tendon from the accessory carpalbone, and are most common in young animals.* TYPE V FRACTURES are comminuted fractures of theaccessory carpal bone.
Extended and flexed mediolateral projections aremost useful in identifying the fracture type.
Type I, II and III fractures may be amenable to screwfixation if the fragments are large enough. The surgeryis difficult, and requires specialist instrumentation.Excision of fragments is performed when repair is notpossible; however, the joint subluxation that accompa-nies type I and II injuries may persist.
Radial carpal bone fracturesFractures of the radial carpal bone are most often seen inboxers and the clinical findings, treatment and outcomehave been described in a recent study (Li and others 2000).
Chronic radial carpal bonefracture in a five-year-oldmale boxer. Note thefragmentation of the secondsesamoid bone of themetacarpophalangeal jointof digit 2
The classification of accessory carpal fractures, as describedby Johnson (1987)
InPractice * JANUARY 2001 5
group.bmj.com on September 9, 2014 - Published by inpractice.bmj.comDownloaded from

These fi-actures are thought to be due to failure of Corn1-plete fLusion ot' the embryological radial c arpal bone xviththe central and intermediate car-pal bones (Miller 1994).The tractures commonly occur in a sagitial plaine and ina dorsopalmar direction. SuchI fractur-es may be sponta-nleous, and ar-e usually associalted xvith a jUMlp or a 'fall,although they may be chronic injuries of- unknoxxn dur-al-tion. Slab fractures of the dorsal aspect of the r(adioccarpalbone mcay coexist.
Acute traumatic saaittal fractures that are accuratelyreduced anld stabilised (2(0 or 2 7 mm lag screw) can
hase a good prognosis. Long-standing fractur-es may be asource of intermittent but only mnoderatc lCtmneness andare occasionLally seen as anl incidental finding wxithout
The sagittal radiolucent linein the ulnar carpal bone is afracture. This dog had aconcurrent hyperextensioninjury and required apancarpal arthrodesis
lameness. Clhronic radioc-arpal fractures has e a p°°lprognosis foI rcpair antd paricarpal a-tlrodsio s InCees'sary in those dogs wx ith intr-actable joint pain.
Small chip fractures of the dorsal aspect ol the rLadio-carpCal bone oCCuIr as a result of hyper-extenlsioll of theantebrachiocarpal joint. Conservxative treatment oftenlresults in ai fibrous 1non unLionI with associated sot't tissLlethickening and ieduced joint flexion. Excisionl maVtheref'ore be necessarv.
Ulnar carpal bone fracturesFra-ctuLrCes of thlC ulnarlt- ccarpal bonie are Xery rare, anid arcusually associated xxwith carpal liTamcntous dcran-ecmicnt.Repail of the fractueC itsClf is unlikcly to resolxc thelamInenress and carpal arthrodesis may bc necessary.
Chip fractures of the small, numbered carpal bonesJoint hyperextension can lead to chip fractures of- thesmall carpalI bones. The fragments ire usually located onlthe dorsal aspect of the affccted bone. Point palin landswelling over the affected bone is a reliable sign, butradiogra-lphic exidence of the fracture may be difficult toobtain duc to the smlall size of the fragments andl bonysuperimposition. Surgical exploration and renoxval ofsmall friagments will often produce a more rapid retunllto functioni thaan conserv ati\xe manateuement.
Proximal metacarpal bone fracturesFractures of dicits II or V are associated with disruptioniof the collater-al support of the carpus. They are com-monly seen with hyperextension injuries and, as a result,repair of the fractul-e wxill not resolx e the lameness.Fractut-es of the first digit are easily overlooked anidmay producc marlked lameness even though this is nota wveightbearini bone. Strcss fractures of the metacar-palbones may be confused with carpal pain as pain is oftendetected on forced flexioIn and axial rotaition of the
CarPLus. Radio-raphy aidls in the diagnosis.
In Practice 0 JANUARY 2001
(A) Acute radial carpal bonefracture, once again in aboxer. Immediate (B) andsix-week (C) postoperativeradiographs showinghealing of the fracture
6
group.bmj.com on September 9, 2014 - Published by inpractice.bmj.comDownloaded from
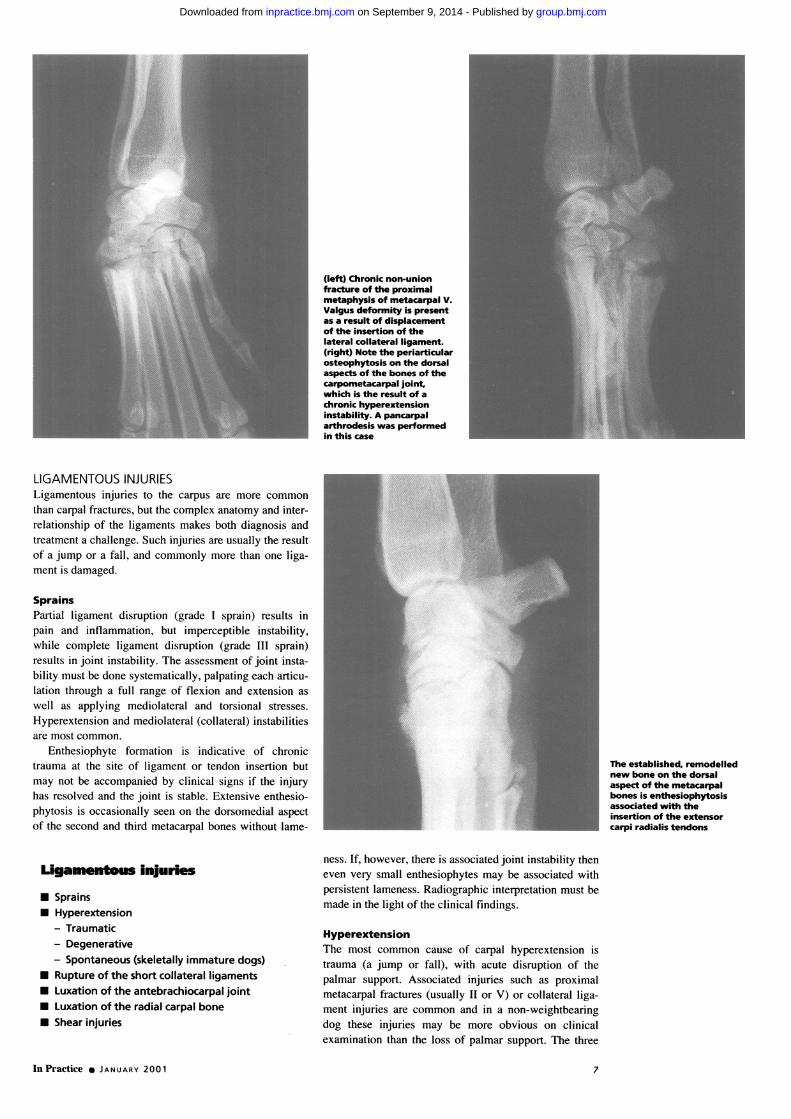
(left) Chronic non-unionfracture of the proximalmetaphysis of metacarpal V.Valgus deformity is presentas a result of displacementof the insertion of thelateral collateral ligament.(right) Note the periarticularosteophytosis on the dorsalaspects of the bones of thecarpometacarpal joint,which is the result of achronic hyperextensioninstability. A pancarpalarthrodesis was performedin this case
LIGAMENTOUS INJURIESLigamentous injuries to the carpus are more commonthan carpal fractures, but the complex anatomy and inter-relationship of the ligaments makes both diagnosis andtreatment a challenge. Such injuries are usually the resultof a jump or a fall, and commonly more than one liga-ment is damaged.
SprainsPartial ligament disruption (grade I sprain) results inpain and inflammation, but imperceptible instability,while complete ligament disruption (grade III sprain)results in joint instability. The assessment of joint insta-bility must be done systematically, palpating each articu-lation through a full range of flexion and extension aswell as applying mediolateral and torsional stresses.Hyperextension and mediolateral (collateral) instabilitiesare most common.
Enthesiophyte formation is indicative of chronictrauma at the site of ligament or tendon insertion butmay not be accompanied by clinical signs if the injuryhas resolved and the joint is stable. Extensive enthesio-phytosis is occasionally seen on the dorsomedial aspectof the second and third metacarpal bones without lame-
Ligamentous injuries
UU
UUUU
SprainsHyperextension- Traumatic- Degenerative- Spontaneous (skeletally immature dogs)Rupture of the short collateral ligamentsLuxation of the antebrachiocarpal jointLuxation of the radial carpal boneShear injuries
The established, remodellednew bone on the dorsalaspect of the metacarpalbones is enthesiophytosisassociated with theinsertion of the extensorcarpi radialis tendons
ness. If, however, there is associated joint instability theneven very small enthesiophytes may be associated withpersistent lameness. Radiographic interpretation must bemade in the light of the clinical findings.
HyperextensionThe most common cause of carpal hyperextension istrauma (a jump or fall), with acute disruption of thepalmar support. Associated injuries such as proximalmetacarpal fractures (usually II or V) or collateral liga-ment injuries are common and in a non-weightbearingdog these injuries may be more obvious on clinicalexamination than the loss of palmar support. The three
In Practice * JANUARY 2001 7
group.bmj.com on September 9, 2014 - Published by inpractice.bmj.comDownloaded from

Carpal hyperextension -(stressed view) caused by ajump off a bridge. Hand-held Erosive arthritis. Note the irregular edges to the articularstressed views must not be surfaces of the carpal bones and the marked periarticularperformed soft tissue swelling
rows of carpal bones may be disrupted individually or
collectively and accurate diagnosis is complicated by-E .the associated soft tissue swelling and proximity of the
joint levels. Stressed (hyperextended) radiographs are
required to demonstrate the level of disruption. Attemptshave been made to repair the palmar support using auto-
genous tendon grafts and wire sutures (Earley 1978) butarthrodesis is most commonly performed (see later).
- Carpal hyperextension may be seen as a degenerativecondition in middle-aged to elderly collie types with nohistory of trauma. Bilateral carpal hyperextension isoften present but the joints do not appear to be particu-larly painful. There is periarticular thickening withreduced flexion and the dogs have a shuffling forelimbgait. Treatment depends on the level of joint discomfortor disability and is either conservative or by jointarthrodesis. Chronic erosive arthritis (immune mediated)
(above) Degenerative carpal hyperextension in a rough collie. may affect the carpi, producing joint thickening and(below) Spontaneous carpal hyperextension in a St Bernard deformity.puppy
Spontaneous carpal hyperextension is seen in skele-tally immature dogs as a result of poor tone in the flexortendons. Inadequate exercise is thought to be responsiblefor the loss of muscle tone and the German shepherd dogis predisposed. The condition is not painful and willusually resolve spontaneously. Affected dogs should beencouraged to exercise. External coaptation is con-
. traindicated; hyperextension of the carpus is often pre-sent following prolonged external coaptation of the distal
-~ -. A ~ limb in puppies.
E Collateral ligament disruptionShort radial and ulnar collateral ligament disruptions are
- s.. traumatic injuries. Radial collateral injuries are more
common as the medial aspect of the joint is under ten-sion whenever the joint is loaded (a normal joint mayhave up to 150 of valgus deviation). Rupture of the radialcollateral ligament results in instability of the medial
- - aspect of the antebrachiocarpal joint and subsequent
In Practice * JANUARY 20018
group.bmj.com on September 9, 2014 - Published by inpractice.bmj.comDownloaded from

carpal valgus. It is important to assess stability with thejoint in extension, as a normal joint has a degree ofmedial instability in flexion. Acute injuries should betreated by repair of the ruptured ligament using a non-absorbable suture material (polypropylene, Prolene;Ethicon) or a slowly absorbed suture material (polydiox-anone, PDS II; Ethicon). The primary repair should besupported with a synthetic permanent suture materialsuch as braided polyester and the joint immobilised inpartial flexion for four weeks (Piermattei and Flo 1997).The position and tension of the prosthetic repair is criti-cal due to the complexity of joint movement. Despitecareful attempts to repair the collateral ligaments, mostaffected joints have a reduced range of flexion.
Luxation of the antebrachiocarpal jointTotal disruption of the antebrachiocarpal joint is a severeinjury. Acute injuries may be treated by primary repair(Butterworth 1991) but, in most cases, the prognosis isguarded. Pancarpal arthrodesis may be necessary torestore good limb function.
Luxation of the radial carpal boneThis is an uncommon condition but it has been reportedin both the dog and cat (Miller and others 1990, Pitcher1996). The injury is thought to occur through hyper-extension, pronation and then supination. The shortradial collateral ligament, dorsal radiocarpal ligamentand associated intercarpal ligaments are ruptured and theradial carpal bone rotates caudal to the distal radius.Palpation reveals carpal pain, reduced flexion and adepression in the dorsal aspect of the carpus immediatelydistal to the radius. Primary repair is possible and has afair prognosis, as the palmar support is unaffected.
Shear injuries of the carpusShear injuries usually occur when an animal's limb is
Transarticular external fixator for the support of a carpalshear injury
run over by a braking car. The limb becomes trappedbetween the tyre and the road surface and the tissues incontact with the road are ground away. Varying amountsof skin, soft tissue and bone may be lost, leaving a largecontaminated wound and joint instability. The medialaspect of the joint is most often affected with loss of theshort radial collateral ligaments.A two-stage approach to treatment is advised with
treatment of the deeply contaminated wound as a priori-ty, and stabilisation of the collateral support at a laterdate. Placement of permanent suture materials in such awound is likely to result in persistent infection andshould be delayed until the wound is clean. Temporarystabilisation of the carpus using a transarticular externalskeletal fixator reduces patient discomfort and enablesthe wound to be debrided, lavaged and bandaged, asappropriate. Only when the wound is clean shouldattempts be made to support the joint instability usingprosthetic ligament techniques or to close the skindefect(s). Attempts to salvage joint function have a vari-able prognosis depending on the degree of ligamentousdisruption; those joints with extensive loss of supportare best managed by delayed pancarpal arthrodesis.Treatment of these injuries is time consuming and costlyand the owners should be fully informed before treat-ment is instigated.
ANGULAR LIMB DEFORMITIES OF THE CARPUSAsynchronous growth of the radius and ulna will lead todeformity of the carpus with deviation of the foottowards the side of the shorter bone. The most commoncause of asynchronous growth is traumatic disturbanceof physeal growth, the distal physes being more com-monly involved than the proximal ones. The conicalshape of the distal ulnar physis predisposes it to com-pression regardless of the direction of any traumaticforce. This fact, allied with the major contribution ofthis physis towards ulnar growth, results in short ulnasyndrome being far more common than short radius
In Practice v JANUARY 2001
Luxation of the radial carpalbone. (left) Dorsopalmarprojection. (right)Mediolateral projection
Angular limbdefonnmifes* Carpal valgus* Carpal varus* Flexon tendoncontracture
9
group.bmj.com on September 9, 2014 - Published by inpractice.bmj.comDownloaded from

Carpal valgus in a six-month-old Irish wolfhound
syndrome. Skeletally immature dogs suffering trauma tothe distal antebrachium should be re-examined regularlyto assess their limb alignment, as physeal injury may notbe apparent at the time of initial examination.
Carpal valgusIn young dogs, carpa,l valgus (lateral decviation of' thefoot) may be caused by short ulna syndrome. distailradius/ulna fracture or dexelopmental laxity of the shortradial collateral ligament. Radiography allows differenti-ation of these conditions. Premature closure of the distalulnar physis leads to retraction of the styloid process,carpal valgus, cranial bowing of the radius (radiuscurvus) and externa1l rotation of the foot. The continuedgrowvth of the radius may lead to secondary elbow jointdeformity, which mfay bc mnore significcant than thecarpal valgus.
Consideration must be gliven to the treatment not onlyof the limb deformity but also of the elbow incongruity.
Carpal valgus as a 'normal' finding in a basset hound
The options for cor-ectioni of thc deformity depend onthe ac,e of the animal anid the anticipated grossth poten-tial of' the distal radial physis. Correctisve techniquesinclude partial distal ulnar- ostectomy w!ith o0 withouttemporary transphyseal bridging on the mediail aspect of'the distal radius (VauThan 1976). coirecti\c osteotomsof' the radius Cand ulna (Miller 994. Pieiriattei and Flo1997) or distraction osteooenesis usinl" a rimo tfixatoi(Stallintzs and others 1998). Corrcction of the hlUmeIro0-ulnar incongruity is roost simliply trcatcd hy pioximilaldyn,amic ulnar osteotomy.
Carpal valgus is a normal finding, in ma1ny clhonidr-o-dystrophic breeds and there may be radiographicevidencc of humeroulnar inconeruity without lamIeCnCssin thesc brceds.
Carpal varusCarpal alrUs isISlicoilniolO)and 111max hC caused by stiortl adius syvrdromic, distail radius/ulna Ifractulrc or dcxclop-
(right) Craniocaudalprojection of the carpusin a four-month-oldBernese mountain dogwith carpal valgus. Thedistal ulnar physis isabnormal. Note therelative overgrowth ofthe radius, resulting inboth lateral deviation ofthe foot and elbowmalalignment. The hazyperiosteal reaction on themedial aspect of thedistal radial metaphysis,adjacent to the physis, isa normal finding inyoung, rapidly growingdogs. On the mediolateralprojection (far right)there is premature closureof the distal ulnar physis,resulting in proximalretraction of the styloid,radius curvus and elbowjoint deformity
Varus deformity due to laxity of the soft tissue support onthe lateral aspect of the carpi
In P'ractice X JANUARY 200110
group.bmj.com on September 9, 2014 - Published by inpractice.bmj.comDownloaded from

mental laxity of the short ulnar collateral ligament. Oncea,-ain, radiography is useful in differentiating these con-ditions. Premature closure of the medial portion of thedistal radial physis is more likely to produce varus thanpremature closure of the entire physis, which tends toproduce a shortened limb rather than an angular limbdeformity.
Flexural deformityFlexural deformity is seen in skeletally immature dogs ataround six to 12 weeks of age as a developmentalcondition, and is frequently bilateral. Affected animalsknuckle over on the carpus when walking and there isexcessive tautness in the flexor carpi ulnaris tendon. Thecondition is not painful and is thought to be due torelative shortening of the flexor carpi ulnaris muscle. Noradiographic abnormalities are present in such cases. Inmost puppies the contracture resolves with time andcareful exercise but, in severely affected cases, transec-tion of the tendon of insertion of the flexor carpi ulnarisis required. Dobermanns appear to be predisposed to thiscondition (Vaughan 1992).
(above and below) Flexor tendon contracture in a12-week- old puppy. Not only is there an inability toextend the carpus, but this dog also knuckles over
ARTH RITISOsteoarthritisOsteoarthritis of the carpus invariablyoccurs secondarily to trauma (eg, fracture,instability). Periarticular soft tissueswelling, reduced joint flexion and painare reliable clinical findings. Jointinstability may be evident on manipulation.Radiographic changes typically includeosteophytosis, irregular joint spaces,periarticular soft tissue swelling and,possibly, instability on stressed projections.Osteophytes and periarticular soft tissuethickening may be present in the absenceof clinical signs. Conservative treatmentwith weight control, moderation of exer-cise and the judicious use of non-steroidalanti-inflammatory drugs is usually effec-tive. Animals with intractable joint painmay be candidates for arthrodesis (seeoverleaf).
Inflammatory arthritisInflammatory arthritis (immune mediated)is a complicated condition with manyunderlying causes (May and Bennett1994). The carpus is commonly affected,resulting in carpal swelling and pain.Affected animals usually suffer from
Carpal ostegeneralised stiffness and some show signs chronic shoof malaise and pyrexia. Careful clinical injury. Thei
dorsal aspeexamination may also reveal multiple joint carpal boneinvolvement, generalised stiffness and bones as wpyrexia. Arthrocentesis of multiple joints is bone. Noteinvaluable in the diagnosis of this condi-tion, but synovial membrane biopsy maybe required for definitive diagnosis in some cases.Prednisolone at immunosuppressive doses (2 to 4 mg/kgdaily) is the mainstay of treatment. Once the clinicalsigns are controlled, this dose may be reduced over aperiod of weeks or months. Complete withdrawal ofmedication is possible in some cases, but others requirelong-term medication at the lowest effective dose(ideally on an alternate day basis).
Infective arthritisInfective arthritis may affect any joint including the car-pus. In addition to periarticular soft tissue swelling andpain, cellulitis of the limb is often present along withpitting oedema. Palpation may reveal a penetratinginjury but haematogenous spread may also occur.Arthrocentesis is usually diagnostic. A positive cultureis most likely following incubation of synovial fluidin blood culture medium prior to culture (Montgomeryand others 1989). Treatment relies on early diagnosisand identification of the causative agent as well as itsantibiotic sensitivity profile (Abercromby 1994). Earlyinfections usually respond to treatment with a broadspectrum antibiotic such as clavulanate-potentiated
Loarthritis secondary to aart radial collateral ligamentre are osteophytes on theects of the distal radius, thees and the proximal metacarpaltell as on the accessory carpalthe periarticular soft tissue
amoxycillin or cephalexin. Treatment should be instigat-ed immediately and changed if necessary once the labo-ratory results are known. The presence of foreign bodymaterial will result in persistent infection and surgicalremoval is indicated. Established, purulent infectionrequires surgical drainage, lavage and debridement ofnecrotic tissue from within the joint.
In Practice * JANUARY 2001 11 1
group.bmj.com on September 9, 2014 - Published by inpractice.bmj.comDownloaded from

Metaphyseal osteopathy. This dog had pain and swellingof the distal radius but the typical radiographic featuresof metaphyseal osteopathy are present in the proximalradial metaphysis as well as in the distal radial and ulnarphyses
Partial carpal arthrodesis using a T-plate
METAPHYSEAL OSTEOPATHYMetaphyseal osteopathy (hypertrophic osteodystrophy)is an idiopathic bone disease of young, large-breed dogs(Muir and others 1996) that may potentially be confusedwith carpal pathology. It is usually polyostotic but mostcommonly affects the distal radial metaphyses and mayat first presentation appear to affect the carpi. Carefulpalpation will localise the pain to the adjacent distalantebrachium and not the carpus. The clinical signs varyfrom mild lameness to reluctance to stand, and affecteddogs are often systemically ill and pyrexic. Theradiographic features are usually strongly suggestive ofmetaphyseal osteopathy, but haematogenous osteo-myelitis cannot be ruled out (Dunn and others 1992).The condition is usually self-limiting, and most mildlyaffected dogs spontaneously recover over a period oftwo to three weeks. Treatment is supportive. Affectedanimals require analgesia and a balanced diet. Severelyaffected dogs should be hospitalised and intravenous flu-ids administered. The use of antibiotics is only indicatedif bacterial osteomyelitis or bacteraemia (blood culture)is present. Severely affected dogs have a poor prognosisand may require euthanasia on humane grounds.
CARPAL ARTHRODESIS
Carpal arthrodesis is a surgically induced osseous unionof the carpus and is indicated for the treatment ofintractable joint pain, hyperextension injury, carpalfracture or dislocation, joint instability and end-stageosteoarthritis where conservative treatment has failed.Carpal arthrodesis has been advocated for the treatmentof selected neurological defects of the distal limb but isinappropriate if there is loss of sensation in the foot.
Pancarpal arthrodesis (six weeks postsurgery)
In Practice 0 JANUARY 200112
group.bmj.com on September 9, 2014 - Published by inpractice.bmj.comDownloaded from

PARTIAL CARPAL ARTHRODESISPartial carpal arthrodesis is appropriate for hyper-extension of the middle or carpometacarpal joints. It isachieved either by retrograde insertion of k-wires in themetacarpal and carpal bones or by the application of a'T' plate on the dorsal aspect of the radial carpal bone,distal carpal bones and third metacarpal bone.
PANCARPAL ARTHRODESISPancarpal arthrodesis is more commonly performed thanpartial carpal arthrodesis regardless of the level of injuryas it is simpler and has a higher success rate for return tosoundness (Denny and Barr 1991). It is most commonlyachieved by the use of a dorsally applied bone plate overthe cranial aspect of the radius and the dorsal aspects ofthe radial carpal and third metacarpal bones. Plateapplication on the palmar aspect of the joint has beendescribed but is technically more demanding (Chambersand Bjorling 1982). The cartilage is removed from alljoint surfaces and the joint spaces packed with autoge-nous cancellous bone graft prior to joint immobilisation.Postoperatively, the distal limb should be supported in atubular cast for six weeks at which time follow-up radio-graphs are taken.
ReferencesABERCROMBY, R. (1994) Infective arthritis. In BSAVA Manual ofArthrology. Eds J. E. F. Houlton and R. Collinson. Cheltenham,BSAVA Publications. pp 100-1 12BUTTERWORTH, S. J. (1991) Open antebrachiocarpal luxation in agreyhound. Journal of Small Animal Practice 32, 474-476CHAMBERS, J. N. & BJORLING, D. E. (1982) Palmar surface platingfor arthrodesis of the canine carpus. Journal of the AmericanAnimal Hospital Association 18, 876-882
DENNY, H. R. & BARR, A. R. S. (1991) Partial carpal and pancarpalarthrodesis in the dog: a review of 50 cases. Journal of Small AnimalPractice 32, 329-334DUNN, J. K., DENNIS, R. & HOULTON, J. E. F. (1992) Successfultreatment of two cases of metaphyseal osteomyelitis in the dog.Journal of Small Animal Practice 33, 85-89EARLEY, T. (1978) Canine carpal ligament injuries. Veterinary Clinicsof North America 8(2), 183-199JOHNSON, K. A. (1987) Accessory carpal bone fractures in the racinggreyhound: Classification and pathology. Journal of VeterinarySurgery 17, 60-64Li, A., BENNETT, D., GIBBS, G., CARMICHAEL, S., GIBSON, N., OWEN,M., BUTTERWORTH, S. & DENNY, H. (2000) Radial carpal bonefractures in 15 dogs. Journal of Small Animal Practice 41, 74-79MAY, C. & BENNETT, D. (1994) Immune mediated arthritides.In BSAVA Manual of Arthrology. Eds J. E. F. Houlton andR. Collinson. Cheltenham, BSAVA Publications. pp 86-99MILLER, A. (1994) The carpus. In BSAVA Manual of Small AnimalArthrology. Eds J. E. F. Houlton and R. Collinson. Cheltenham,BSAVA Publications. pp 211-233MILLER, A., CARMICHAEL, S., ANDERSON, J. & BROWN, I. (1990)Luxation of the radial carpal bone in four dogs. Journal of SmallAnimal Practice 31, 148-154MONTGOMERY, R. D., LONG, I. R., MILTON, J. L., DIPINTO, M. N. &HUNT, J. (1989) Comparison of aerobic culturette, synovial biopsyand blood culture medium in detection of canine bacterial arthritis.Veterinary Surgery 18, 300-303MUIR, P., DUBIELZIG, R., JOHNSON, K. & SHELTON, G. (1996)Hypertrophic osteodystrophy and calvarial hyperostosis.Compendium on Continuing Education for the PracticingVeterinarian 18(2), 143-151PIERMATTEI, D. L. & FLO, G. L. (Eds) (1997) Brinker, Piermattei, andFlo's Handbook of Small Animal Orthopaedics and Fracture Repair,3rd edn. Philadelphia, W. B. Saunders. pp 344-389PITCHER, G. D. (1996) Luxation of the radial carpal bone in a cat.Journal of Small Animal Practice 37, 292-295STALLINGS, J. T., LEWIS, D. D., WELCH, R. D., SAMCHUKOV, M. &MARCELLIN-LITTLE, D. J. (1998) An introduction to distractionosteogenesis and the principles of the llizarov method. VeterinaryCompendium of Orthopaedics and Traumatology 11, 59-67VAUGHAN, L. C. (1976) Growth plate defects in dogs. Journal ofSmall Animal Practice 20, 711-736VAUGHAN, L. C. (1992) Flexoral deformity of the carpus in puppies.Journal of Small Animal Practice 33, 381-384YALDEN, D. W. (1970) The functional morphology of the carpalbones in carnivores. Acta Anatomica 77, 481-500
WOOF WOOF WOOF WOOF WOOF WOOFWOOF WOOF WOOF WOOF WOOF WOOFWOOF WOOF WOOF WOOFWOOF MEOW.
FELINE BETTER SOON....6) NOVARTIS
In Practice * JANUARY 2001 13
group.bmj.com on September 9, 2014 - Published by inpractice.bmj.comDownloaded from
doi: 10.1136/inpract.23.1.2 2001 23: 2-13In Practice
Richard Whitelock Conditions of the carpus in the dog
http://inpractice.bmj.com/content/23/1/2Updated information and services can be found at:
These include:
serviceEmail alerting
the box at the top right corner of the online article.Receive free email alerts when new articles cite this article. Sign up in
Notes
http://group.bmj.com/group/rights-licensing/permissionsTo request permissions go to:
http://journals.bmj.com/cgi/reprintformTo order reprints go to:
http://group.bmj.com/subscribe/To subscribe to BMJ go to:
group.bmj.com on September 9, 2014 - Published by inpractice.bmj.comDownloaded from