conducting a feasibility analysis for freestanding ambulatory surgery centers
TRANSCRIPT

AORN JOURNAL DECEMBER 1986, VOL. 44. NO 6
Ambulatory Surgery
Conducting a feasibility analysis for freestanding ambulatory surgery centers
s competition in the health care industry A intensifies, hospitals are providing an increasing number of services to outpatients that have traditionally been provided to inpatients. This trend has led to a rapid increase in the number of freestanding ambulatory surgery centers.
Many of these surgery centers are profitable businesses. The competitive market, however, has caused some freestanding centers to incur substantial losses, and they are now facing the possibility of closure. Nevertheless, many areas still exist in which a profitable, freestanding ambulatory surgery center could be established.
The key to establishing a profitable surgical center in the competitive outpatient surgery market is performing a quality feasibility analysis. Feasibility analysis provides information on the
advantages and disadvantages of establishing a freestanding surgical center on a specific site. The site-evaluation criteria, which rely on volume as an indicator of probable success, can be separated into two groups: market size and market characteristics.
The overall rating of a site based on these two criteria does not necessarily mean a surgery center should or should not be established. Often additional strategic planning considerations override the results of the feasibility analysis.
Market Size Assessment Method
he probable volume to be experienced by a T surgery center at a specific location can be
and master of science degrees in economics from Brigham Young University. He also h a a doctorate of philosophy in economics from the University of California, Riverszde.
Robert E. Tonkinson, Jr, BA, k a research assistant and graduate student in the health administration program, Brigham Young Univer- sity, Provo, Utah. He received h k bachelor of arts degree in public policy from Brigham Young University.
Robert J. Parsons Robert E. Tonkinson, Jr
Robert J. Parsons, PhD, is a professor of health adminktration, Brigham Young Universiiy, Provo, Utah He received both hii bachelor of science
The authors thank Dan Burrows, Mike Wells, Steve Payne, Richard Perkins, Kelb Roundy, and Scott Shieldr for their preliminary research for thkarticle.
1026

AORN JOURNAL DECEMBER 1986, VOL. 44, NO 6
The probable volume to be experienced by a surgery center can be estimated by
the market size assessment method.
estimated by the market size assessment method. This method includes five steps: market area definition, market area population estimate, overall outpatient surgery rate estimate, total market potential estimate, and break-even level determination.
Market area definition. First, the primary market must be defined. The primary market of a freestanding surgical center is the area from which 80% of all surgeries will come. Generally, this includes a contiguous area within a four-mile radius of the center. The market area definition may vary, however, depending on geographic barriers, traffic patterns, and the location of other facilities offering similar services.
One method of estimating market size is to examine the outpatient surgery patient-origin study of a hospital near the area where the center is to be located. If this information is available, it will show the distances patients are accustomed to traveling to receive outpatient surgical care. This information could also be obtained through survey research.
If the above alternatives are not feasible, market area definitions can be estimated according to two major factors. First, the proximity of competitors to the proposed site can affect the distance people are willing to travel for surgery. The four-mile radius market proposed above is appropriate for areas with no more than two hospitals that perform outpatient surgery, with no freestanding surgical centers, and with few doctors who perform surgery in their offices. Areas with more competitors will have smaller market areas.
Second, patterns of residential and commercial activity and geographic barriers can affect the market area.
Market area population estimate. After the market area has been defined, an estimate is made of the population within that area. United States Census Bureau population estimates may be used to determine the market area population. Market
research firm estimates by zip codes may also be used. Historical and projected population information can provide useful indications about population trends.
Overall outpatient surgery rate estimate. Next, an overall outpatient surgery rate must be estimated. The average outpatient surgery rate is approximately 26 procedures per 1,000 popula- tion, but that is expected to rise to about 40 procedures per 1,000 by 1990.' This national rate may not be appropriate for all areas because of demographic and economic variables. A surgical rate for the market area should be developed by adjusting the national rate to reflect local conditions.
Total market potential estimate. Multiplying the surgery rate by the market area population gives the total number of outpatient surgeries that can be expected in an area. That number can then be used to estimate the market potential for the surgical center. Of the 26 outpatient surgeries per 1,000 population, national averages indicate that freestanding surgical centers perform 9%, hospitals 69%, and physician offices 2 2 % ~ ~ However, these percentages are based on data that include areas that do not have access to freestanding surgical centers. Therefore, a freestanding surgical center could expect to capture between 15% and 27% of the outpatient surgery market (between four and seven operations [per center] per 1,000 population at the total rate of 26 outpatient surgeries [all facilities together] per 1,000, depending on the competition in the market area).
Break-even level determination. Finally, the number of surgeries that must be performed to cover the costs of the surgical center must be determined. The break-even level is determined by the size and cost of the surgical center, labor, administration, and utilities.
The American Operating Room Society has stated that the optimum level of use is 1,000
1028

AORN JOURNAL DECEMBER 1986, VOI.. 44, NO 6
If certain market characteristics are favorable, an area that requires a high market share
to be successful may still be feasible.
operations per operating room per year.3 To establish a new center, at least 800 operations should be performed per operating room per year. If the center is expected to gain a market share of 19% in an area with a surgical rate of 26 per 1,000 population, the population in the market area must be at least 161,000 before a surgical center can be successfully established. If the population in the market area is 81,000, a 38% market share would be required for the center to be successful.
Market Characteristics Assessment Method
he five steps described above assess market T desirability from the perspective of market potential based strictly on market size. But other market characteristics can also influence the patient volume of a surgical center. If certain market characteristics are highly favorable, an area that requires a high market share to be successful may still be feasible.
Distance from the nearest freestanding surgical center. If the surgical center is located near an existing center, the ability to achieve a high market share will be decreased. Because most of the patients will live within about four miles of the center, the closest surgical center should be eight miles or more from the proposed site.
Number of hospitals in the market area. Hospitals provide the majority of outpatient surgeries in the United States4 A surgical center will have difficulty achieving a high market share if more than two hospitals have market areas that substantially overlap its market area (unless the center is tied to one of the hospitals). No more than two hospitals should be located within six miles of the proposed site.
Number of surgeons in the market area. Because surgeons provide customers for surgical centers, the more surgeons in the market area,
the better. From another perspective, however, surgeons compete with surgical centers because many surgeons perform simple procedures in their offices that could be performed at a surgical center. Therefore, the market area should contain a few surgeons who perform surgery in their offices and many surgeons who are willing to use the surgical center. The number of surgeons needed to support a center depends on the type and strength of each practice.
Average household income. Surveys indicate that people most likely to have outpatient surgery come from families with combined incomes totaling more than $40,000 per year.5 The higher the average income of the people in the market area, the more likely the center is to succeed.
Average household size. Because many surgical procedures performed at surgical centers are done for children, locating in a market area with a large population of children is more likely to be profitable.
Local economy. Many surgeries performed at a surgical center are elective procedures that can be postponed during poor economic times. Locating a surgical center in a community with a growing economy and with unemployment rates historically lower than the national average is more favorable than locating in an area of economic decline.
Percent of population older than 65. Elderly people are generally not frequent users of outpatient surgery facilities because they prefer the traditional inpatient arrangement. The market area selected for the surgical center should contain a population with less than 7.5% of the people 65 years of age or older.
Outpatient surgery rate. Outpatient surgery rates vary widely among different areas (between about 10% and 50% of all surgeries). Locating a center in an area with a high outpatient surgery rate (more than 26 procedures per 1,000 population) is preferable to locating in an area
1030
AORN JOURNAL DECEMBER 1986, VOL. 44. NO 6
Criteria
Marker size Total population Outpatient surgery market
potential Market share for break-
even
Market characteristics Distance from nearest
freestanding center Number of hospitals within
six miles Average household income Average household size Local unemployment rate
compared to national Population more than
age 65 Outpatient surgery rate Market area growth rate
Percent of target market characterhtics met
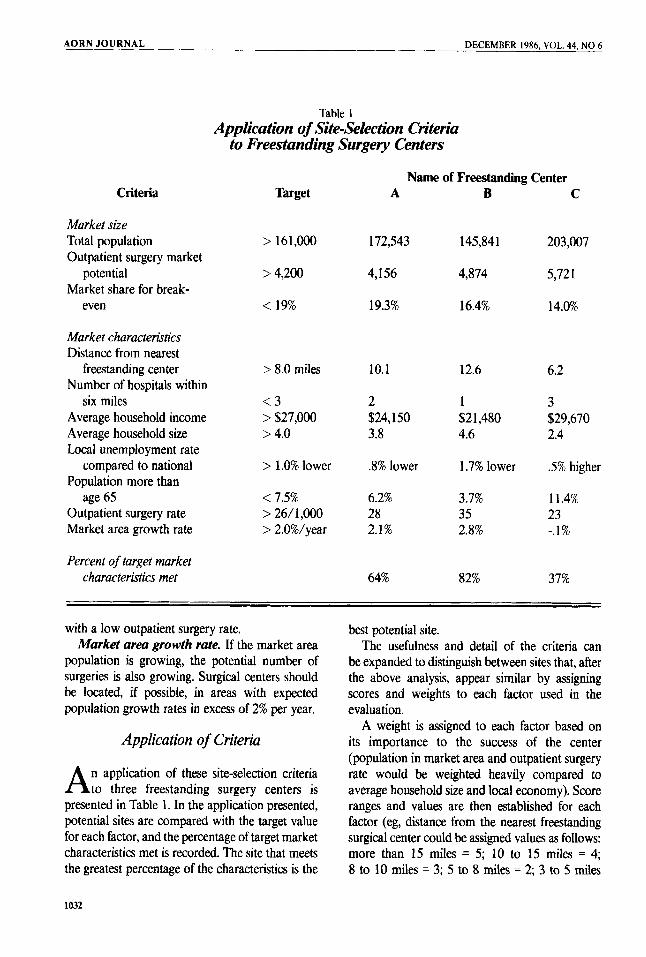
Table 1 Application of Site-Selection Criteria
to Freestanding Surgery Centers
Name of Freestanding Center Target
> 161,000
> 4,200
< 19%
> 8.0 miles
< 3 > $27,000 > 4.0
> 1.0% lower
< 7.5% > 26/ 1,000 > 2.0%/year
A
172,543
4,156
19.3%
10.1
2 $24,150 3.8
3% lower
6.2% 28 2.1%
64%
B
145,841
4,874
16.4%
12.6
1 $2 1,480 4.6
1.7% lower
3.7% 35 2.8%
82%
C
203,007
5,72 1
14.0%
6.2
3 $29,670 2.4
.5% higher
11.4% 23 -.I%
37%
with a low outpatient surgery rate. Market area growth rate. If the market area
population is growing, the potential number of surgeries is also growing. Surgical centers should be located, if possible, in areas with expected population growth rates in excess of 2% per year.
Application of Criteria
n application of these site-selection criteria A to three freestanding surgery centers is presented in Table 1. In the application presented, potential sites are compared with the target value for each factor, and the percentage of target market characteristics met is recorded. The site that meets the greatest percentage of the characteristics is the
best potential site. The usefulness and detail of the criteria can
be expanded to distinguish between sites that, after the above analysis, appear similar by assigning scores and weights to each factor used in the evaluation.
A weight is assigned to each factor based on its importance to the success of the center (population in market area and outpatient surgery rate would be weighted heavily compared to average household size and local economy). Score ranges and values are then established for each factor (eg, distance from the nearest freestanding surgical center could be assigned values as follows: more than 15 miles = 5; 10 to 15 miles = 4; 8 to 10 miles = 3; 5 to 8 miles = 2; 3 to 5 miles
1032

DECEMBER 1986, VOL. 44, NO 6
= 1; less than 3 miles = 0), then each site is scored on each factor based on the range of the factor. Next, each score is multiplied by its corresponding weight, and the results are added for each center. The center with the highest total score is the best potential site.
Conclusion
0th the market size assessment method and B the market characteristics assessment method are used to evaluate the feasibility of a freestanding surgical center site. When used together, they provide a comprehensive system for evaluating a proposed location for the center based on environmental characteristics. However, surgical centers have been located in areas that appeared excellent and failed; they have also been located in areas that appeared marginal and succeeded. Although a feasibility analysis can aid in selecting an excellent surgical center location, it cannot ensure success. The ultimate success of a surgical center depends on its ability to meet both the needs of the consumer and the needs of the physician.
ROBERT J. PARSONS ROBERT E. TONKINSON, JR
Notes I . K Shannon, “Outpatient surgery up 77 percent:
Data,” Hospitals 59 (May 16,1985) 54. 2. J Inguanzo, M Harju, “What’s the market for
outpatient surgery?” Hospitals 59 (Aug 1, 1985) 56. 3. K Shannon, “Maximizing outpatient surgery could
cut 600 million patient days yearly,” Hospitals 59 (May 16, 1985) 61.
4. Inguanzo, Harju, “What’s the market for outpatient surgery?” 56.
5. Ibid, 55.
Suggested reading Parsons, R Willson, W Youkstetter, D. “Applied
feasibility analysis for urgent care centers.” Journal of Ambulatory Care Management 8 (November
Riffer, J. “Freestanding emergency and surgery centers proliferate.” Hospitals 58 (Dec 16, 1984) 50.
Shannon, K. “Company targets local doctors as surgicenter partners.” Hospikzls 59 (May 16, 1985) 62.
Stetson, P. “Hospital-affiliated or freestanding units: Which are best?“ AORN Journal 38 (December
1985) 18-31.
1983) 1049-1054.