confidential - international stillbirth alliance · confidential overview •the association of...
TRANSCRIPT
ConfidentialThe Autopsy and Fetal
Growth RestrictionAdrian CharlesPaediatric/Perinatal Pathologist, PathwestKing Edward Memorial Hospital Perth, Western
Australia
Confidential
2+ Million25,000 Births
170 SB65-70% PM at Kemh
Confidential
Avicenna Ibn Sina Canon 980-1037
ConfidentialOverview• The association of Growth restriction
and stillbirth• Assessment of growth restriction• Causes of growth restriction - IUGR• Autopsy -document and identify cause
– Problems in maceration– Findings -Fetus, Placenta
• Stillbirths, Growth restriction and the Barker hypothesis.
ConfidentialCause of death in stillbirth
• Depends on classification• Depends on gestational age• Depends on investigations, particularly the
post mortem and placenta
Confidential
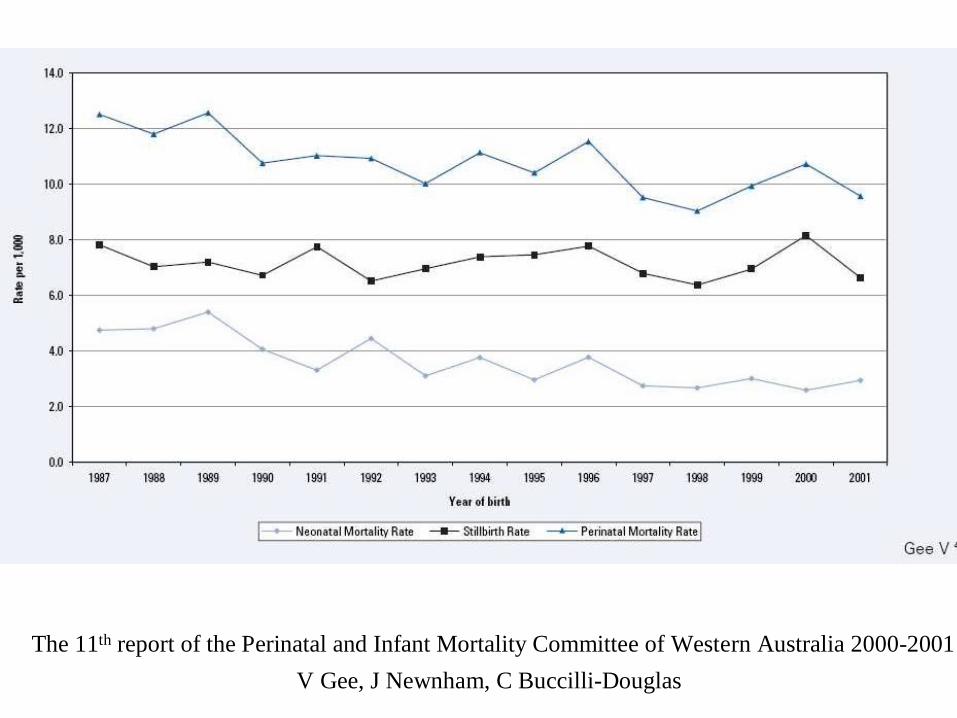
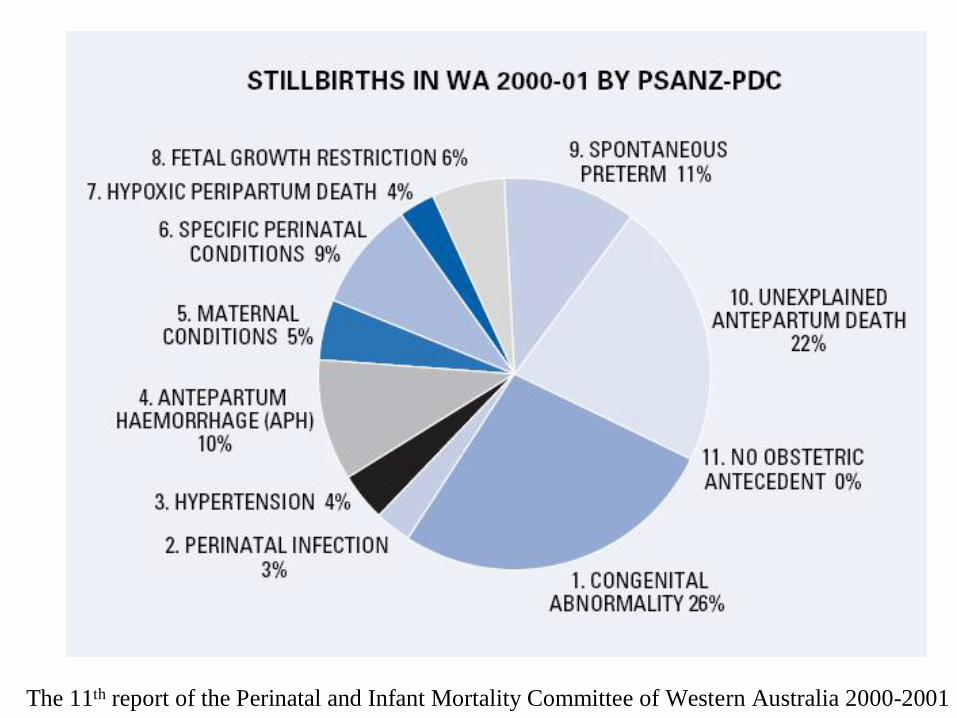
The 11th report of the Perinatal and Infant Mortality Committee of Western Australia 2000-2001V Gee, J Newnham, C Buccilli-Douglas
Confidential
0
2
4
6
23 28 32 36 40
Yudkin
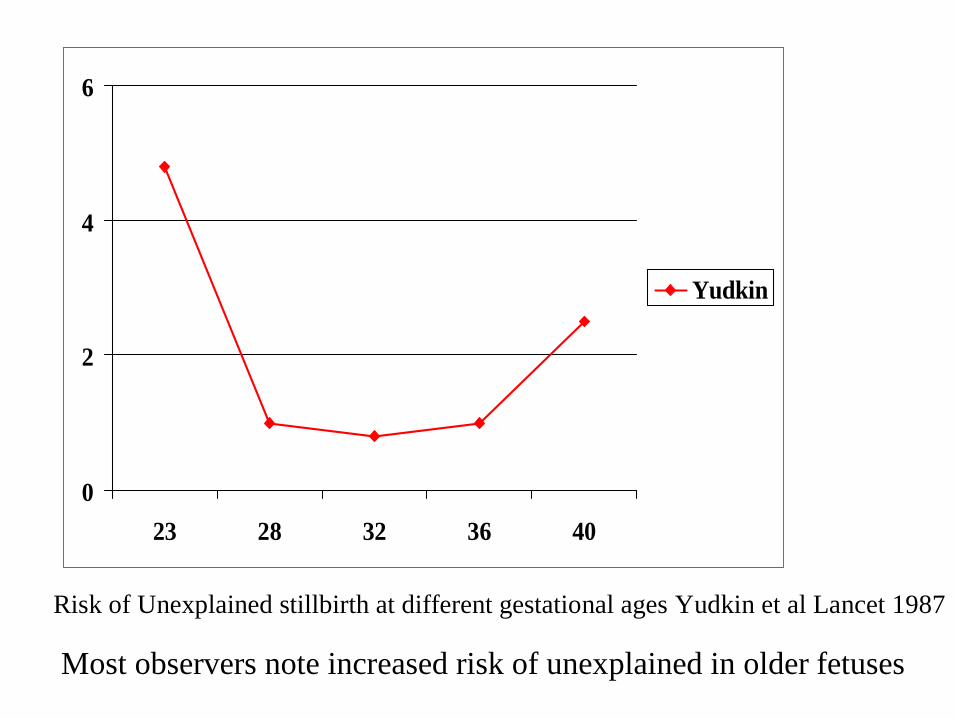
Risk of Unexplained stillbirth at different gestational ages Yudkin et al Lancet 1987
Most observers note increased risk of unexplained in older fetuses
ConfidentialClassification systems for stillbirths
• 30 or so different systems– Aberdeen– Wigglesworth– PSANZ– ReCoDe: Jason Gardosi
(http://www.perinatal.nhs.uk/main.htm)
– Inside: F Froen (http://www.med.uio.no/inside/frames_html)
– TULIP Erwich• Vary whether IUGR is included
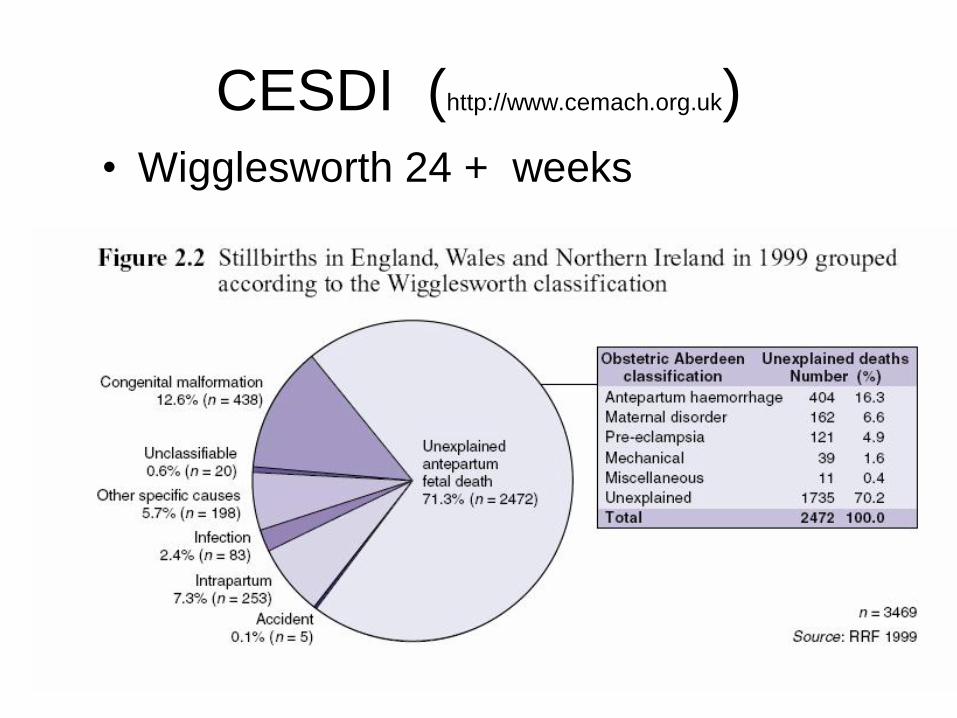
ConfidentialCESDI (http://www.cemach.org.uk)• Wigglesworth 24 + weeks
Confidential
The 11th report of the Perinatal and Infant Mortality Committee of Western Australia 2000-2001
ConfidentialBirmingham UK - Suboptimal Growth
• 2625 SB 1997-2003• 66% Unexplained with Wigglesworth• 15% Unexplained using ReCoDe• 58% of the Wigglesworth unexplained
were IUGR
• RR of SB x 5 at 10th Centile customised, x 10 on 3rd Centile customised
» Gardosi et al BMJ 2005, 331:1113-7
ConfidentialPathophysiology vs epidemiology• Some causes are directly related to fetal
death e.g. Fetal maternal haemorrhage, infection are fatal.
• Other causes are chronic with increased risk of stillbirth: Death is acute and not clearly causally related, mechanism unclear.– E.g. Trisomy 21, IUGR, IDDM
• E.g. Myocardial infarct directly may cause death. Old age risk factor for
ConfidentialIntrauterine growth restriction (IUGR)
• Determine IUGR - Easier said than done!
• IUGR vs Small for gestational age• Individualised weight projection based on
parental indices appears better indication• Accurately know gestational age.• What to do if macerated Stillbirth
Confidential
ConfidentialIntrauterine growth restriction (IUGR)
• Increases risk of stillbirth• Often not appreciated before delivery (and
often not appreciated after delivery)
• BUT – IUGR is not one condition.
ConfidentialCauses of IUGR • Maternal e.g.
• Malnourished• Diabetes
• Placental disease e.g.• Ischaemic - unreconstructed vessels• Villitis• Maternal floor infarction• Confined placental chromosomal mosaicism
• Fetal e.g.• Chromosomal• Anomaly e.g. renal agenesis, gastroschisis• Disease e.g. viral infection• Metabolic e.g. SLO, neonatal
Autopsy information useful
ConfidentialThe role of the autopsy• The autopsy is helpful because it allows
– Detailed external examination– Detailed internal examination– Detailed Placental examination– Photographs– Xrays– Taking of samples
•Histology•Bacteriology•Virology
•Cytogenetic•Molecular•Metabolic
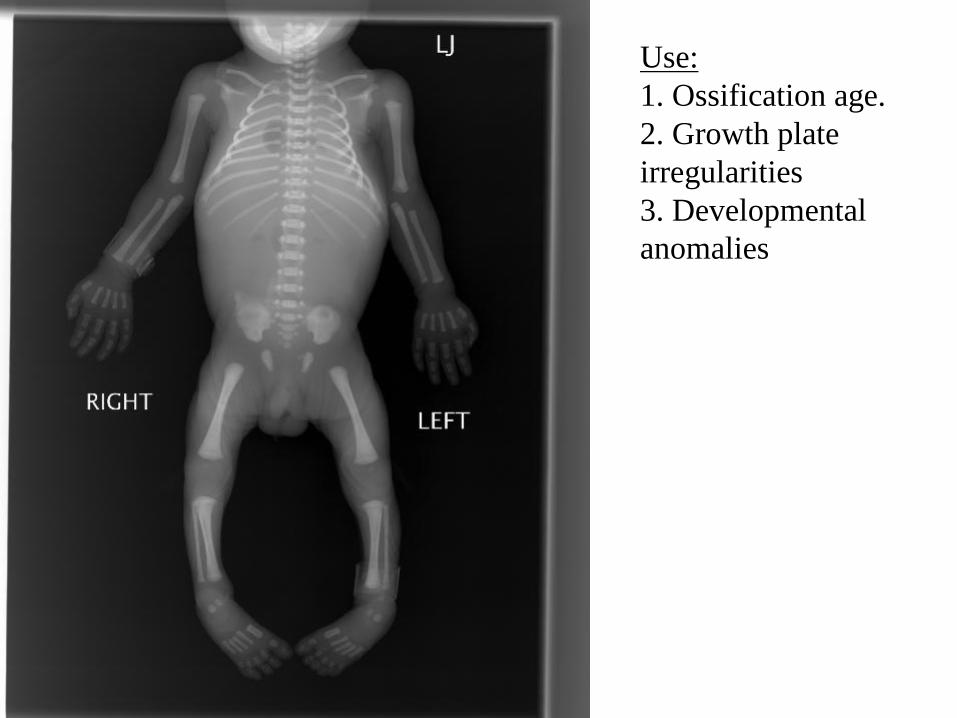
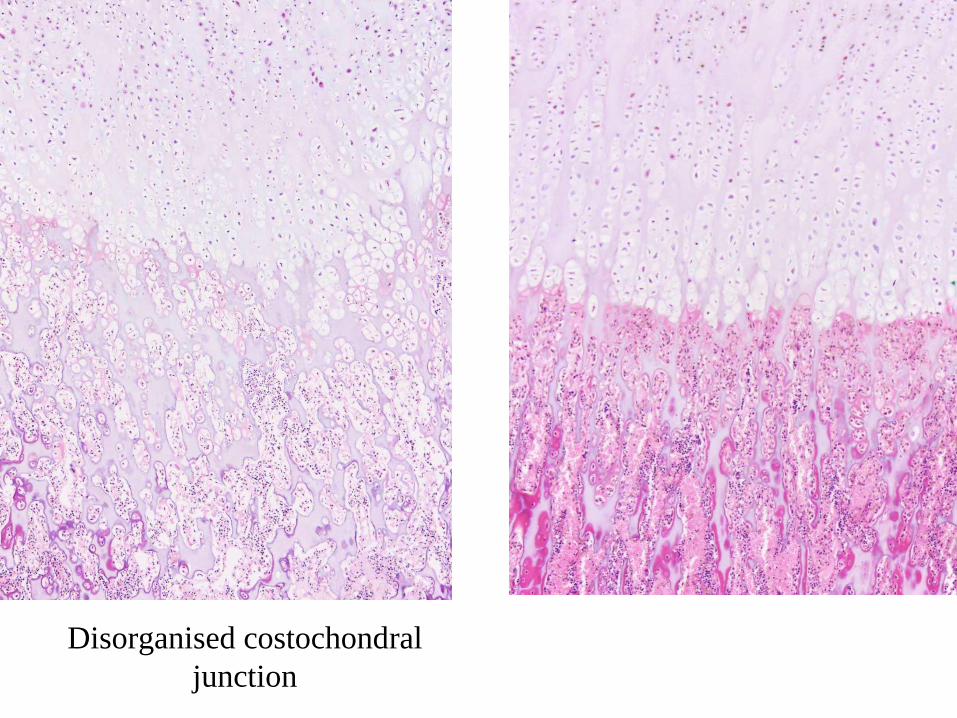
ConfidentialUse:1. Ossification age.2. Growth plate irregularities3. Developmental anomalies
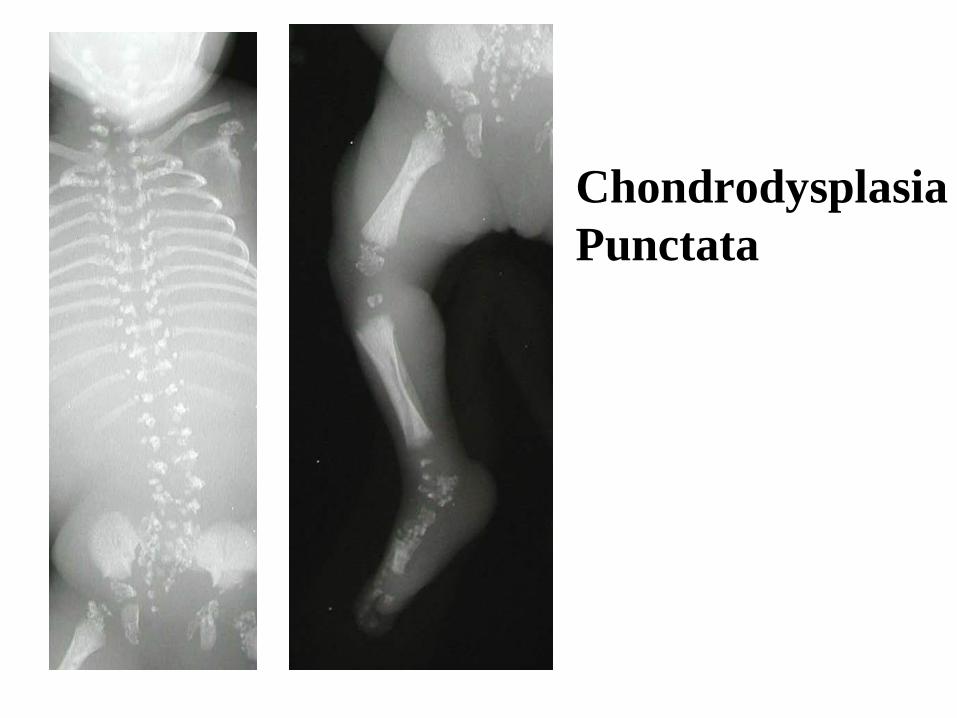
ConfidentialChondrodysplasiaPunctata
ConfidentialThe limitations of the autopsy• The autopsy does not tell everything
(Snapshot after the horse has bolted).• Limited to anatomical changes.• Many acute physiological conditions leave
little specific histological changes. E.g. arrhythmias, epilepsy, suffocation, metabolic conditions, sepsis.
• Autopsy identifies and excludes anatomical and histological changes BUT limited by maceration and post mortem associated changes.
ConfidentialHow helpful is the Autopsy?• Provides a lot of data, macroscopic,
histologic and also the potential data in the histology for future research.
• How often does the autopsy– Alter the diagnosis?– Add additional information?– Confirm
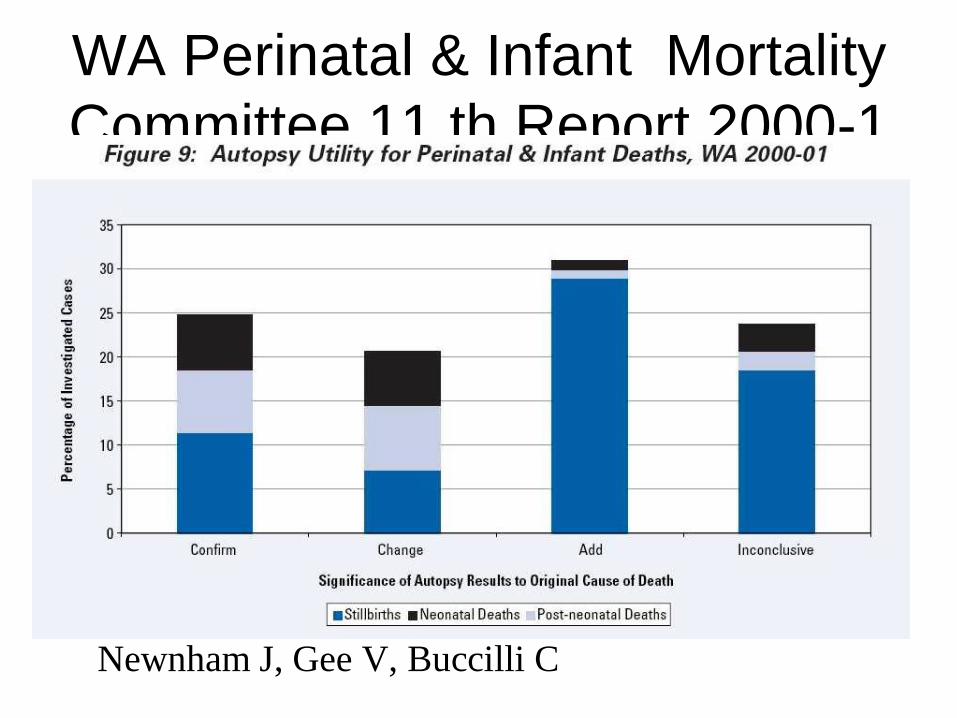
ConfidentialWA Perinatal & Infant Mortality Committee 11 th Report 2000-1
Newnham J, Gee V, Buccilli C
ConfidentialAutopsy and growth restriction• Identify IUGR• Problems
– Weight charts • (based on abnormal babies stillborn or preterm)• Accurate gestational age (USS, footlength,
ossification)– Maceration
• Rough timings– Skin peeling starts around 12 hours– Skull collapse around 3-4 days– But can be influenced by post delivery storage and
also infection.
ConfidentialMaceration - Problems• When did fetus die? • Possible weight changes after death• Dysmorphic features lost (+ often ?
Hydrops)• Measurements (weights and length) less
easy • The brain very rapidly becomes soft • Histological loss of detail
• Reduced nuclear staining - reflects DNA loss • Some tissue autolyse rapidly, e.g. pancreas,
compared to others e.g. Lung.
• Cytogenetics (use placenta or better
Confidential
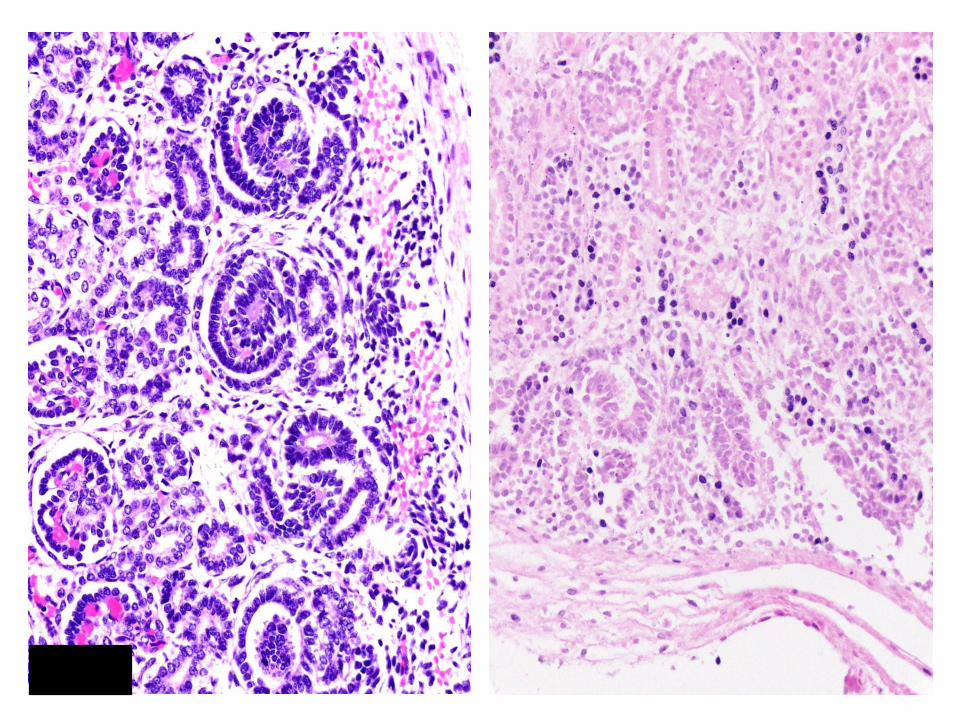
Kidney
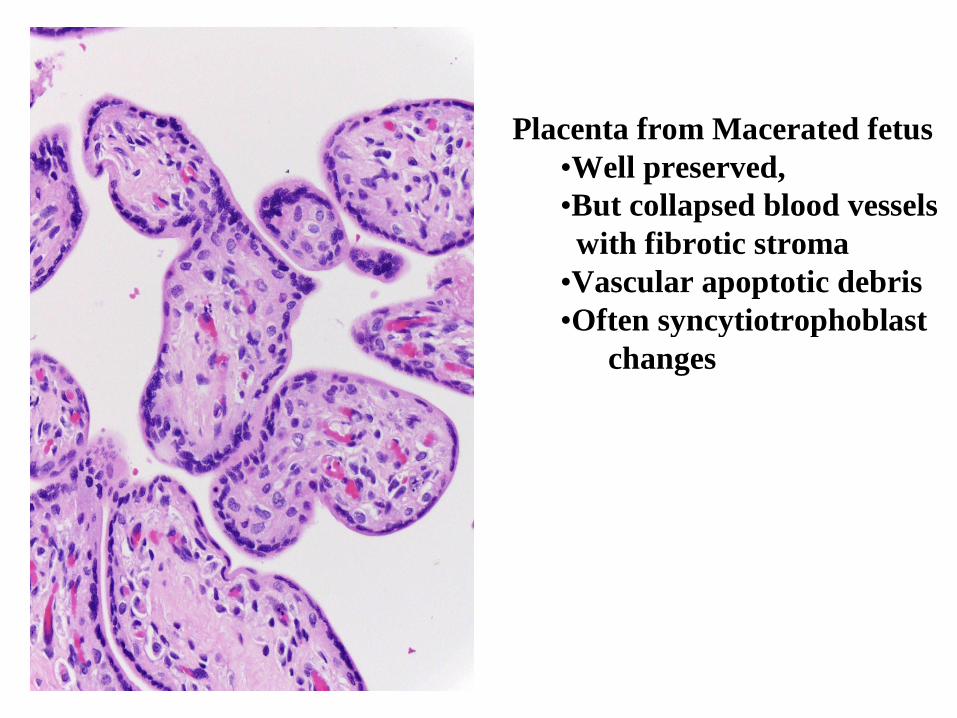
ConfidentialPlacenta from Macerated fetus•Well preserved,•But collapsed blood vessels
with fibrotic stroma•Vascular apoptotic debris•Often syncytiotrophoblast
changes
ConfidentialFetal Changes seen in IUGR at autopsy
• External– appearance and measurements– Dysmorphic features– Assess maceration if present and time
(under 24 hours, few days, week or so, weeks)
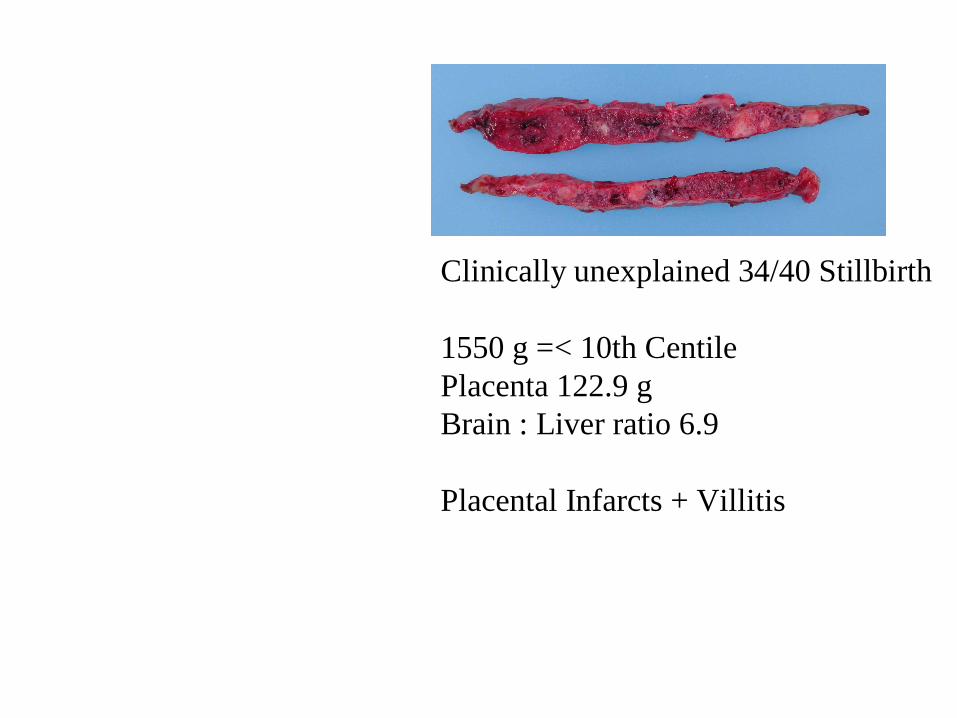
ConfidentialClinically unexplained 34/40 Stillbirth
1550 g =< 10th CentilePlacenta 122.9 gBrain : Liver ratio 6.9
Placental Infarcts + Villitis
ConfidentialFetal Changes seen in IUGR at autopsy
• Internal– Subcutaneous fat– Brain: Liver ratio (normal < 3:1)– Reduced renal glomeruli (research)
• Exclude infection and malformation
Confidential
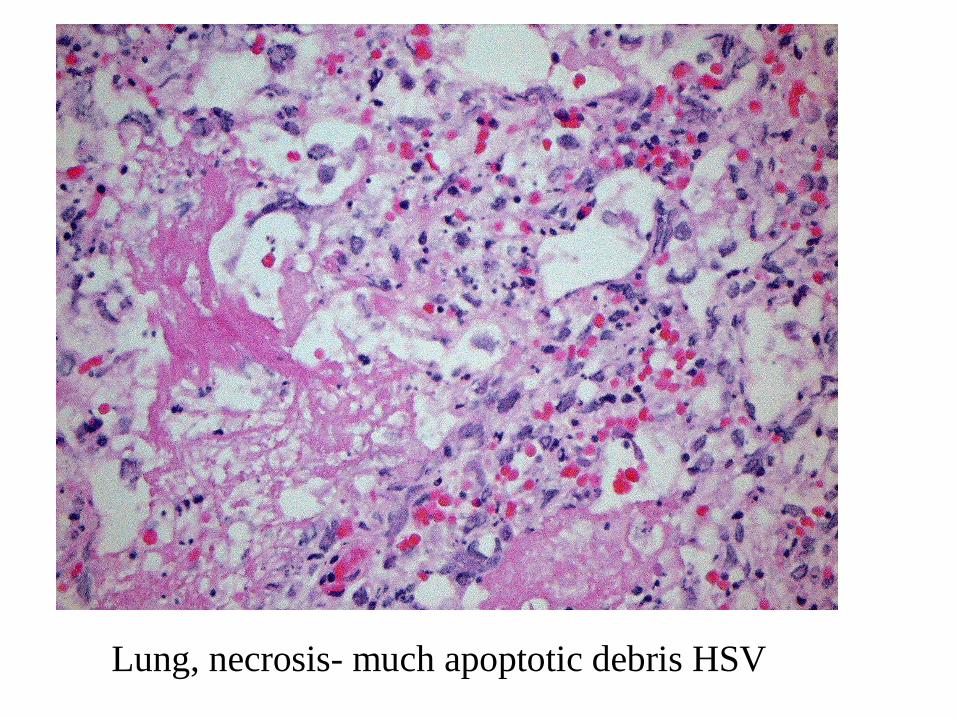
Lung, necrosis- much apoptotic debris HSV
Confidential
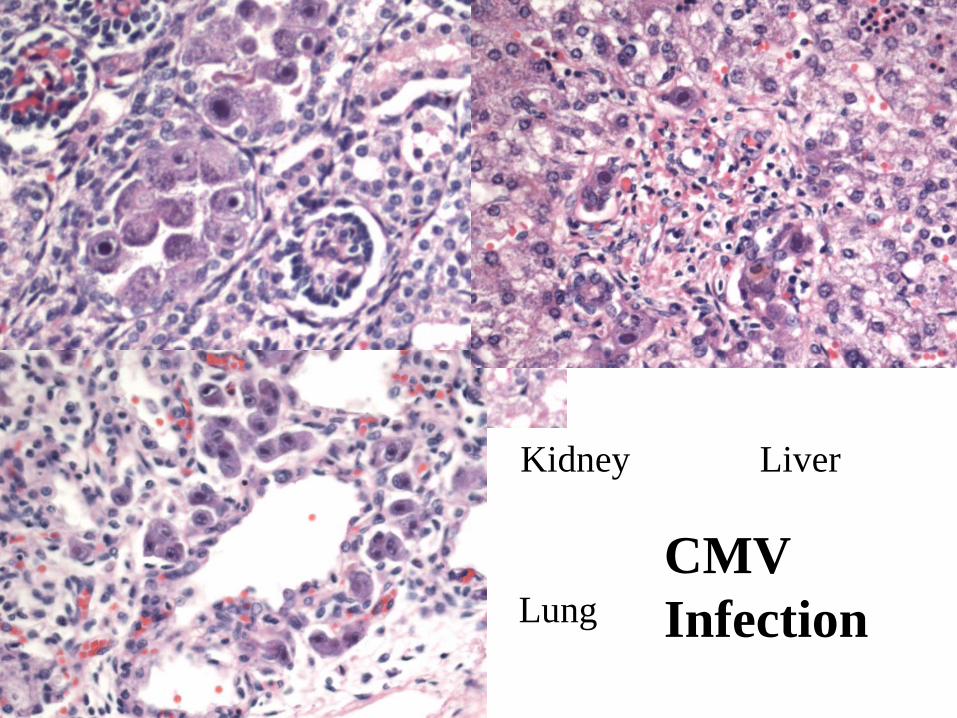
Kidney Liver
LungCMV Infection
ConfidentialFetal Changes seen in IUGR at autopsy
• Non specific stress changes– Radiology– Histology
• Altered Adrenal fat, • Thymus small and involuted,• Disturbed costochondral junction• Petechial haemorrhages
Confidential
Disorganised costochondral junction