conflicts - namcp cprc.pdf · • allergic reaction • alopecia (50%) ... immunotherapy:...
TRANSCRIPT

10/30/2015
1
Optimal Treatment Strategies in the Management of Castration‐Resistant
Prostate Cancer
Julie N. Graff, MD, MCR
Portland VA Medical CenterAssistant Professor of MedicineKnight Cancer Institute, OHSU
Conflicts
• Research funding from Medivation/Astellas, Sanofi
• Honoraria from Dendreon, Bayer
• Travel from Bayer

10/30/2015
2
Objectives
• Define metastatic Castration Resistant Prostate Cancer (mCRPC)
• Agents that prolong survival in mCRPC
– Mechanism of action, safety, efficacy
– When to use which agent
• Challenges and barriers of multidisciplinary models of CRPC regarding prognosis, treatment options, potential adverse events, and quality‐of‐life considerations
• Best practices for clinical decision‐making based on line of treatment, duration of response, pain associated with metastases, and comorbidities
2015: Cancer Estimates
Stage at Diagnosis
• 4% of men present with metastatic disease• Many more men develop metastatic cancer
after presenting with localized cancer

10/30/2015
3
Disease States in Prostate Cancer
Localized disease
Biochemical Recurrence
(BCR)
mHSPC
nmCRPC
mCRPCL1
mCRPCL2
mCRPCL2+
Focus of today’s talk:therapy selection here
Metastatic Prostate Cancer
• Definition
• Sites of metastases: – bone (90%)– lymph nodes (60%)– liver/lungs (25‐45%)
• Initial Therapy: Androgen Suppression

10/30/2015
4
Decreasing Androgens
Surgical Castration1940s
LHRH Agonist Therapy (1980s)
Testosterone < 50 ng/dl
Decreasing Androgens
Surgical Castration1940s
LHRH Agonist Therapy (1980s)
Testosterone < 50 ng/dl

10/30/2015
5
Androgen Insensi ve → Castration Resistant
• In a metastatic lymph node from a hormone-refractory patient
Androgen receptor expressed
PSA expressed
Androgen responsive genes expressed
Montgomery RB, Cancer Res 68:4457-54, 2008
Mechanisms of Castration Resistance in Prostate Cancer
Nature Clinical Practice Urology (2009) 6, 76‐85

10/30/2015
6
Metastatic, Castration Resistant Prostate Cancer
+Nuclear Medicine Bone scan
OR
+CT Scan
Testosterone < 50 ng/dl
Timeline for FDA Approval
2004
2010
2011
2012
2013
Docetaxel
Sipuleucel‐T
Radium‐223
Abiraterone post‐chemotherapy
Abiraterone pre‐chemotherapy
2014 Enzalutamide pre‐chemotherapy
Enzalutamide post‐chemotherapy
Cabazitaxel
IMMUNOTHERAPY
CHEMOTHERAPY
HORMONE THERAPY
RADIATION THERAPY
CHEMOTHERAPY

10/30/2015
7
Chemotherapy
• Taxanes
– First line: Docetaxel + prednisone 5 mg bid
– Second line: Cabazitaxel + prednisone 5 mg bid
Clin Cancer Res. 2008;14:7167‐7172.
• Median OS: 18.9 vs 16.5 mo• HR: 0.76 (CI: 0.62‐0.94); P = .009
Tannock IF et al. N Engl J Med. 2004;351:1502-1512.
TAX 327Outcome, % DOC Q3W DOC Q1W M
Pain response
35
P = .01
31
P = .0722
PSA response
45
P = .005
48
P < .00132%
QOL response
(FACT‐P)
22
P = .009
23
P = .00513
Objective response
12 8 7
Docetaxel: First to Improve Overall Survival

10/30/2015
8
Docetaxel Toxicities
• Fatigue
• Allergic Reaction
• Alopecia (50%)
• Tear duct scarring
• Myelosuppression (neutropenic fever 2‐3%)
• Neuropathy
Immunotherapy: Sipuleucel‐T (aka Provenge)
Nature Review Clinical Oncology 2011; 8: 551‐561.

10/30/2015
9
Improved Survival
NEJM 2010; 363: 411‐422
• Overall survival: 25.8 versus 21.7 months
• No significant PSA decreases, tumor size decreases
• Used in minimally symptomatic patients
Side Effects of Sipuleucel‐T
• Related to cytokine release
• Risk of receiving someone else’s cells
• Risk of receiving infected cells

10/30/2015
10
Chemotherapy:Cabazitaxel + Prednisone (aka Jevtana)
Overall survival: 15.1 months versus 12.7 months
Pain control
Lancet Oncology 2010; 376: 1147‐54.
Cabazitaxel + Prednisone Toxicity
• Significant myelosuppression
• Rate of neutropenia and neutropenic fever = 8%; consider dose reduction or prophylactic GM‐CSF or G‐CSF
• Fatigue

10/30/2015
11
Hormone Therapy
• More complete suppression of androgen production
– Abiraterone
• More complete blockade of androgen receptor signaling
– Enzalutamide
Hormone Therapy: Abiraterone (+ Prednisone) (aka Zytiga)
Mineralocorticoids Glucocorticoids Androgen hormones
Inhibits 17 hydroxylase and 17,20 lyase enzymes (green arrows)
10/30/2015
12
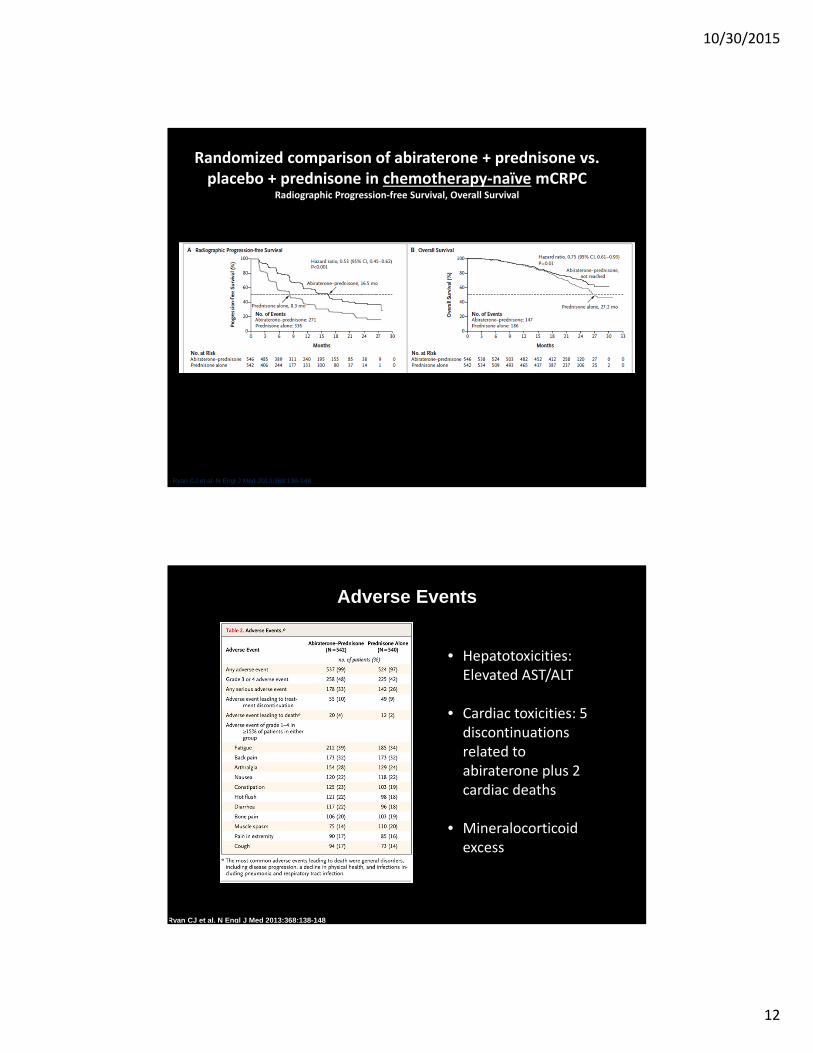
Randomized comparison of abiraterone + prednisone vs. placebo + prednisone in chemotherapy‐naïve mCRPC
Radiographic Progression‐free Survival, Overall Survival
Ryan CJ et al. N Engl J Med 2013;368:138-148.
Adverse Events
Ryan CJ et al. N Engl J Med 2013;368:138-148
• Hepatotoxicities: Elevated AST/ALT
• Cardiac toxicities: 5 discontinuations related to abiraterone plus 2 cardiac deaths
• Mineralocorticoid excess

10/30/2015
13
Updated Survival Data
Enzalutamide: An Androgen Receptor Inhibitor
Enzalutamide improved overall survival and radiographic progression‐free survival in patients with metastatic castration‐resistant prostate cancer post‐docetaxel1
1
T
AR
T
Cell nucleus
AR
Cell cytoplasm
2
3
Inhibits binding of androgens to AR
Inhibits AR nuclear translocation
Inhibits AR‐mediatedDNA binding
Enzalutamide:
AR=androgen receptor; T=testosterone.
Scher et al. N Engl J Med 2012; 367:1187-97.
10/30/2015
14
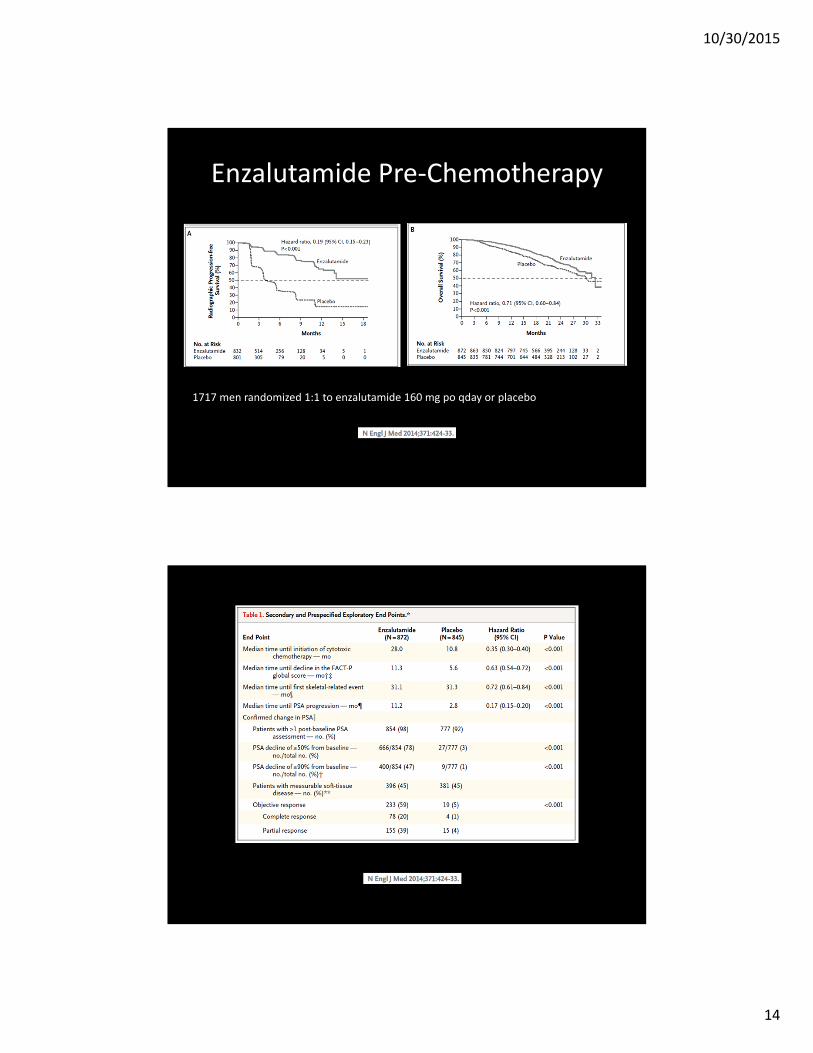
Enzalutamide Pre‐Chemotherapy
1717 men randomized 1:1 to enzalutamide 160 mg po qday or placebo

10/30/2015
15
Enzalutamide Toxicity
• Special concern Seizure– Dose limiting toxicity in phase I study (360 mg/day, 600 mg/day and questionable 480 mg/day)
– Six in the post‐chemotherapy study
– Two In the pre‐chemotherapy study
• Fatigue
• Hypertension
• Falls
Radiation Therapy:Radium‐223 (aka Xofigo)

10/30/2015
16
Radium‐223
Radium‐223
NEJM 2013; 369(3): 213‐223
Clinical trial required painful bone metastatic disease without visceral disease.
• Improved survival• Pain relief• Fewer fractures and other skeletal related events

10/30/2015
17
Radium‐223 Toxicity
• Flare in bone pain
• Myelosuppression: requires good marrow function prior to treatment (platelet count > 100,000/mm3 and leukocyte count > 3000/mm3)
• Nausea, emesis, dehydration
Elderly
CA Cancer J Clin 2014;64:9‐29.
15,188 will be men ≥ 80 years

10/30/2015
18
Considerations for the Elderly
Agent Analysis Conclusion
Sipuleucel‐T Survival: > 71 years vs ≤ 71 yearsProduct integrity: ≥ 80 vs < 80 years old
No difference
Cabazitaxel/Prednisone 19% in study were ≥ 75 years No analysis
Abiraterone/Prednisone Adverse events ≥ 75 years vs. < 75 years
Similar
Enzalutamide Post‐chemotherapy, survival: < 75 years and men ≥ 75 years
No difference in survivalMore fatigue, edema, diarrhea men ≥ 75 years
Radium‐223 Survival < 67 years, 67‐74 years, and ≥ 75 years
Good in all groups
Name Confusion
Radium‐223 XofigoGoserelin Zoladex
FDA Response
10/30/2015
19
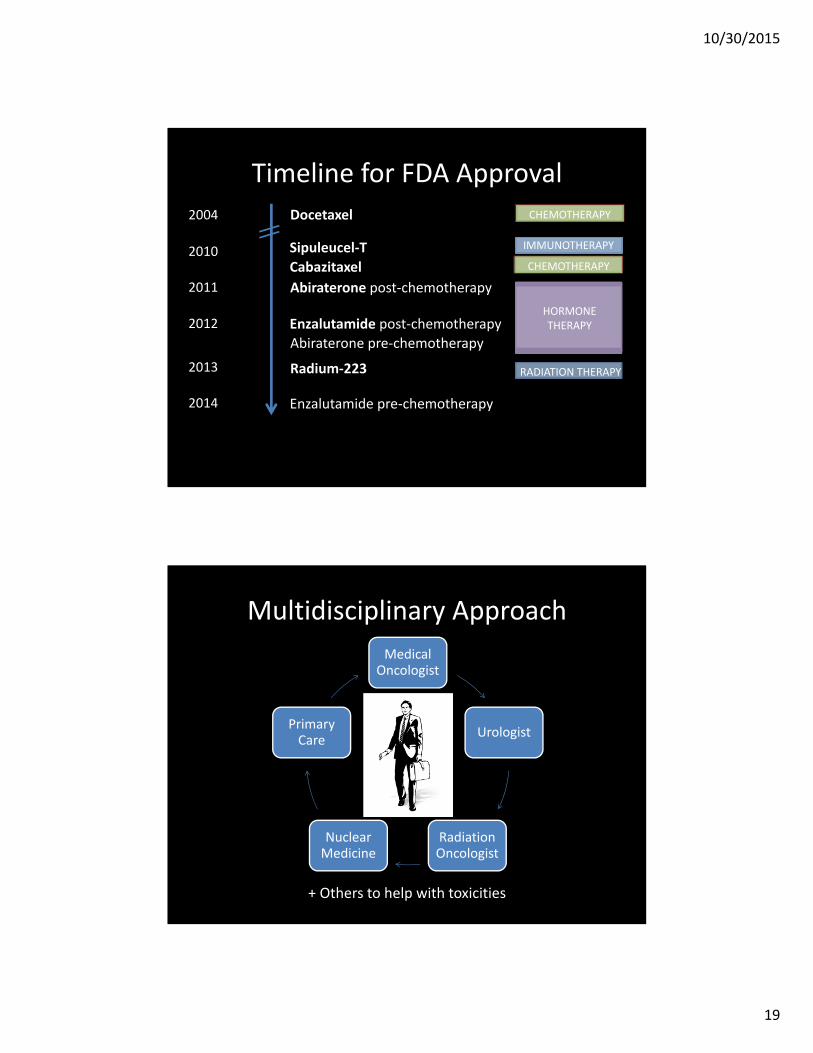
Timeline for FDA Approval
2004
2010
2011
2012
2013
Docetaxel
Sipuleucel‐T
Radium‐223
Abiraterone post‐chemotherapy
Abiraterone pre‐chemotherapy
2014 Enzalutamide pre‐chemotherapy
Enzalutamide post‐chemotherapy
Cabazitaxel
IMMUNOTHERAPY
CHEMOTHERAPY
HORMONE THERAPY
RADIATION THERAPY
CHEMOTHERAPY
Multidisciplinary Approach
Medical Oncologist
Urologist
Radiation Oncologist
Nuclear Medicine
Primary Care
+ Others to help with toxicities

10/30/2015
20
Toxicities from Androgen Suppression
• Physical Therapist/Trainer• Dietician• Therapist – individual, couples
Case 1• 71 year old man diagnosed with prostate cancer in 2001. Underwent prostatectomy. PSA recurrence in 2009. Started LHRH agonist at that time, with an excellent PSA response until January when his PSA starts to rise again.
Date PSA (ng/ml)
1/5/14 2.5
2/10/14 3.0
3/18/14 3.2
4/15/14 4.0
5/20/14 4.2

10/30/2015
21
Other investigations
• No symptoms, ECOG PS = 1
• Testosterone: <10 ng/dl
• CT scan: No evidence of metastatic disease
• NM bone scan: Two metastatic lesions, one in skull and one at left humerus
• Meets criteria for metastatic, castration resistant prostate cancer
Discussion with Patient
• He tells you he has no pain.
• Options:– Clinical trial – Docetaxel/prednisone– Abiraterone/prednisone– Enzalutamide– Sipuleucel‐T– Cabazitaxel/prednisone– Radium‐223– Hospice

10/30/2015
22
Decision
• Options:
– Clinical trial
– Abiraterone/prednisone
– Enzalutamide
– Sipuleucel‐T
– Cabazitaxel/prednisone
– Radium‐223
– Hospice
Case 2
• 53 year old man with prostate cancer diagnosed metastatic in 2012 when he presented with back pain. Had a bilateral orchiectomy at that time. PSA initially decreased, but came back quickly. He received first‐line chemotherapy (docetaxel/prednisone) in 2013, but his cancer is now progressing through it. He is having “unusual” headaches.
10/30/2015
23
Other investigations
• Performance Status (ECOG) = 1
• CT scan shows multiple liver lesions that are new since 2013.
• NM bone scan shows new lesions in bilateral ribs, skull, pelvis.
• MRI brain shows a tumor
• He having significant bone pain.
Discussion with Patient
• Radiation to the brain tumor, PLUS
• Options:– Clinical trial
– Docetaxel re‐treatment
– Abiraterone/prednisone
– Enzalutamide
– Sipuleucel‐T
– Cabazitaxel/prednisone
– Radium‐223
– Hospice

10/30/2015
24
Case 3
• 92 year old patient who was diagnosed with prostate cancer 20 years ago and was initially treated with prostatectomy. He had a biochemical relapse in 2002. He was just observed until he developed metastatic cancer to the bones in 2008 when he started an LHRH agonist. His PSA reached undetectable, but started to rise again in 2011. He is currently in tremendous pain (bones).
Other investigations
• ECOG = 2
• PSA currently 50 ng/ml
• Testosterone < 10 ng/dl
• NM bone scan shows lesions in skull, humerus, femurs, pelvis.
• CT scan shows mild lymphadenopathy
• Echo shows EF 25%

10/30/2015
25
Discussion with Patient
• Options:– Clinical trial
– Docetaxel/prednisone
– Abiraterone/prednisone
– Enzalutamide
– Sipuleucel‐T
– Cabazitaxel/prednisone
– Radium‐223
– Hospice
Case 4
• 75 year old man presents with a cord compression from prostate cancer metastatic to the bone. He receives androgen deprivation therapy (degarelix), which brings his PSA down, plus radiation to his spine. Unfortunately, he never regains the ability to walk. Less than one year later, his cancer is progressing.

10/30/2015
26
Other investigations
• ECOG = 3, in wheelchair but able to do ADLs• PSA currently 770 ng/ml• Testosterone < 10 ng/dl• CT scan shows metastatic disease to the liver, lungs, lymph nodes and bones
• NM bone scan show involvement of nearly all bones and is termed a “superscan” by the radiologist.
• MRI of brain negative• No symptoms concerning for heart failure• Labs within normal limits
Discussion with Patient
• Options:– Clinical trial
– Docetaxel/prednisone
– Abiraterone/prednisone
– Enzalutamide
– Sipuleucel‐T
– Cabazitaxel/prednisone
– Radium‐223
– Hospice

10/30/2015
27
Unanswered Questions
• Ordering of the agents
• Combination of agents
• Effects of longer term androgen suppression therapy on the body
• Tumor characteristics after multiple treatments
OHSU Prostate Cancer Team