consent to examination or treatment policy
TRANSCRIPT

Consent to Examination or Treatment Policy – January 2020
Lewisham and Greenwich NHS Trust Page 1 of 41
Consent to Examination Or Treatment Policy
If being read as a paper copy, please refer to Trust intranet to ensure this is the current version
Version: 3 Ref P0714
Date issued: 6th February 2020
Author: Head of Patient Safety
Equality Impact Assessment:
Undertaken – no inequalities highlighted
Impact highly positive
Consultation: Head of Legal Services
Divisional Medical Directors
Divisional Directors of Nursing, Governance and Quality
Heads of Departments
Corporate Teams
Divisional Clinical Governance Managers
Approved by and date: Quality and Safety Committee – 06/02/2020
Ratified by and date: Quality Governance Committee – Date TBC
Where available: Trust Intranet
Target audience: All staff who work with patients
Next review due: 6th February 2023
Responsible for review: Head of Patient Safety

Consent to Examination or Treatment Policy – January 2020
Lewisham and Greenwich NHS Trust Page 2 of 41
Review and Amendment Log
Version Date Author Status Changes made
3.0 Jan 2020
Ruth Dean - Head of Patient Safety
3 yearly update
Update to roles and responsibilities, definitions, contact details and legal references.
Reviewed monitoring compliance with the policy
2.0 August 2016
Interim Head of Governance
Update of Consent
Forms and Policy
Document
This Document is the full Consent Policy for Lewisham & Greenwich NHS Trust. Minor textual amendments only to the Policy.
Added Forms 1 – 5 updated and added to the Policy.
1.0 2015 Julie Rochefort – Head of Patient Safety
Interim update pending
revision of all the Trust’s
main consent forms
This document was an interim first Consent Policy for Lewisham and Greenwich NHS Trust; it is an amalgamation of the consent policies of the two previous Trusts SLHT and LHT which had similar content and has been updated with a recent case p16.
Guidance on documenting the application of the Mental Capacity Act will be published separately.
Added: page 16 following the Supreme court judgment in Montgomery v Lanarkshire Health Board in March 2015
Removed: template for consent forms (currently being redesigned to cover whole Trust) with the exception of Form 4 (for Adults who lack mental capacity) which has already been redesigned for LGT to make it compliant with the Mental Capacity Act, and is available to print from the Trust intranet.
This version is reissued for LGT with the above changes, pending full review due by March 2016.
Lewisham Healthcare NHS Trust amended to read Lewisham and Greenwich NHS Trust; names of committees updated since changes post-merger.

Consent to Examination or Treatment Policy – January 2020
Lewisham and Greenwich NHS Trust Page 3 of 41
Section Contents Page
Foreword 6
1.0 Introduction and Legal Principles 6
1.1 Why Consent is crucial 6
1.2 Purpose and Scope 6
1.3 Definitions 6
1.4 Roles and Responsibilities 7
1.5 What consent is and is not 8
1.6 Sources of Guidance on consent 9
1.7 The Mental Capacity Act (MCA) – principles 9
1.8 5 statutory principles of the Act (MCA) 10
1.9 Determining what is in an incapacitated patient’s best interests 11
1.10 Consulting others 11
1.11 Exceptions to the Best Interests principle 11
1.12 Who can be a Decision Maker? 12
1.13 Doubt or Dispute 12
2.0 Documentation 12
2.1 Written consent 12
2.2 Procedures to follow when patients lack capacity to give or withhold consent
13
2.3 When to instruct an Independent Mental Capacity Advocate 13
2.4 How to contact an IMCA 14
2.5 Availability of consent forms 14
3.0 When should consent be sought? 15
3.1 Single stage process 15
3.2 Two or more stage process 15
3.3 Seeking consent for anaesthesia 15
3.4 Emergencies 16
3.5 Treatment of Children and Young People 16
4.0 Provision of information 16
4.1 Patient information leaflets and other media 18
4.2 Withholding information 18
4.3 Provision for patients whose first language is not English 18
4.4 Access to more detailed or specialist information 19

Consent to Examination or Treatment Policy – January 2020
Lewisham and Greenwich NHS Trust Page 4 of 41
Section Contents Page
4.5 Access to health professionals between formal appointments 19
4.6 Open access clinics 19
5.0 Who is responsible for seeking consent 19
5.1 Process for documenting the discussion and provision of information to patients
20
5.2 Completing consent forms 20
5.3 Capability of the health professional and delegated consent 20
5.4 Process for following up those who have obtained consent for a procedure without authorisation
21
5.5 Confirmation of consent 21
5.6 Responsibilities of health professionals 21
6.0 Refusal of treatment 22
7.0 Withdrawal of Consent 22
8.0 Tissue (Human Tissue Act) 23
9.0 Clinical Photography - conventional or digital video recordings 23
10.0 Training 25
10.1 Delegated consent training 25
11.0 Monitoring Compliance with and the Effectiveness of this Policy 26
12.0 References 29
13.0 Associated Documents 29
APPENDICES
A 12 key points on consent: the law in England 30
B Contacting an IMCA 32
C Template consent forms used in this Trust 33
D Useful contact details 34
E How to seek a court declaration 35
F Seeking consent: remembering the patient’s perspective 37
G Audit Tools 38
H Equality Impact Assessment 42

Consent to Examination or Treatment Policy – January 2020
Lewisham and Greenwich NHS Trust Page 5 of 41
Foreword
This policy reflects the Department of Health Model Consent Policy introduced under Health Service Circular HSC 2001/023 on 22 November 2001. The Trust has supplemented the Model Consent Policy by the inclusion of its own and further guidance, particularly incorporating the provisions of the Mental Capacity Act 2005 (enacted 2007).
1.0 Introduction
1.1 Why consent is crucial Patients have a fundamental legal and ethical right to determine what happens to their own
bodies. Valid consent to treatment is therefore absolutely central in all forms of healthcare, from providing personal care to undertaking major surgery. Seeking consent is also a matter of common courtesy between health professionals and patients.
Any treatment or investigation (and this can extend, in the extreme, to mere touching)
carried out without consent may give rise to accusations of battery and/or negligence. This may result in an action for damages or even criminal proceedings, and a finding of misconduct by the relevant professional body.
For consent to be valid, it must be given voluntarily by an appropriately informed person who has the capacity to consent to the intervention in question. The informed person may either be the patient, a parent or a person who has parental responsibility or a person who has authority under a Power of Attorney, or someone who has the authority to make treatment decisions as a court appointed deputy. Consent will not be legally valid if the patient has not been given adequate information or where they are under the undue influence of another. Acquiescence where the person does not know what the intervention entails is not ‘consent’. Where a patient does not have capacity to give consent, then treatment may be given providing it is given in accordance with the Mental Capacity Act 2005.
The Department of Health (DH) has issued a range of guidance documents on consent (see Section 1.6), and these should be consulted for details of the law and good practice requirements on consent. Healthcare regulatory bodies and professional colleges also issue helpful guidance that can be accessed on their websites.
1.2 Purpose and Scope
This policy sets out the standards and procedures in the Lewisham & Greenwich NHS Trust
(the Trust) which aim to ensure that staff are able to comply with the guidance issued by the DH so far as it remains good practice to do so.
This policy applies to all Trust staff seeking consent to examination or treatment, and the general principles to all staff who administer care directly to patients.
1.3 Definitions Health professional – this term is used in this document to apply to all registered
healthcare professionals including: nurses, doctors, midwives, allied health professionals such as physiotherapists, occupational therapists, operating department practitioners, podiatrists, pharmacists, speech and language therapists, dieticians
Mental Capacity Act 2005 – this act enshrined into statute (Act of Parliament) elements of what was previously known as ‘common law’ (decisions made by judges in individual cases). It was brought into force in English law in April and October 2007. It introduced

Consent to Examination or Treatment Policy – January 2020
Lewisham and Greenwich NHS Trust Page 6 of 41
additional safeguards for people lacking mental capacity. It was amended in May 2019 with changes only to the Deprivation of Liberty Safeguards (DoLS) which are to be known as Liberty Protection Safeguards. Lasting Power of Attorney for Personal Welfare - introduced in October 2007 as part of the Mental Capacity Act. For the first time in English law, this allows a person aged 18 yrs. and over to appoint someone else (the ‘attorney’) to make healthcare decisions on their behalf should they subsequently lose mental capacity. Healthcare professionals must be aware of what makes such an LPA valid and applicable. Advance Decision (AD) – (formerly known as an Advance Directive) decision about their care made by the patient in advance should they subsequently lose mental capacity. In healthcare these are common amongst Jehovah’s Witnesses – but anyone can make an AD. The term ‘Living Will’ is a type of advance decision as it relates to the person’s preferences for their healthcare expressed while they still have capacity. Valid and applicable ADs must be taken into account by treating healthcare professionals. Independent Mental Capacity Advocate (IMCA) – the role of the IMCA is to help particularly vulnerable people who lack the capacity to make important decisions about serious medical treatment and changes of accommodation, and who have no family or friends that it would be appropriate to consult about those decisions. IMCAs will work with and support people who lack capacity, and represent their views to those who are working out their best interests.
1.4 Roles and Responsibilities
1.4.1 Chief Executive and Trust Board
o the overall implementation, monitoring and effectiveness of this policy o the allocation of resources to ensure compliance with this policy o that managers are aware of their responsibilities and implement the policy
1.4.2 Medical Director
The Chief Executive has delegated the overall responsibility for implementing this policy to the Medical Director who ensures that:
o effective policy and practice is in place throughout the Trust o operational responsibility for the implementation of this policy is delegated to Directors
of Services and to Heads of Nursing / Midwifery o the Trust Board is advised of the effectiveness of this policy and of any shortfalls in
meeting the standard set via her membership of the Board and chairmanship of the Quality and Safety Committee
1.4.3 Quality and Safety Committee
o Ensures compliance with and the effectiveness of this policy is reviewed on an annual
basis at minimum o Issues arising from reported incidents, complaints and claims related to consent issues
are monitored
1.4.4 Divisional Triumvirates, Directorate Triumvirates and Heads of Nursing / Midwifery
o Ensure the policy is distributed in their Division and implemented and that clinicians are
aware of their own individual responsibilities for updating themselves on the law on consent
o The policy is easily accessible to all staff within their area via the intranet

Consent to Examination or Treatment Policy – January 2020
Lewisham and Greenwich NHS Trust Page 7 of 41
o Appropriate staff are afforded training opportunities in the consent process
1.4.5 Consultant Medical Staff and Heads of Professional Practice
o Staff unable to undertake a procedure without supervision are identified as soon as they start employment within the Trust and a programme put in place for competency assessment and conferment of delegated authority to obtain consent put in place
1.4.6 Individual health professionals
o Are to ensure that they have read and understood the guidance in this policy,
particularly section 5.0 o always use one of the Trust’s template consent forms for procedures where the
patient will be anaesthetised or sedated o only undertake the consent process with a patient if they are themselves capable of
carrying out the proposed procedure or for which they have been assessed and received delegated authority
o actively seek out advice, training / updates for any identified gaps in their knowledge related to consent to examination or treatment
o document all elements of the consent process in the patient’s clinical notes
All staff providing direct care to patients should be aware of the basic principles of this policy (as touching a patient without their consent could be challenged as an assault).
1.5 What consent is – and is not
“Consent” is a patient’s agreement for a health professional to provide care. Patients may
indicate consent non-verbally (for example by presenting their arm for their pulse to be taken), orally, or in writing. For the consent to be valid, the patient must:
• have the mental capacity to take the particular decision; • have received sufficient information to make the decision for themselves; and • not be acting under duress.
It must be noted that patients with learning difficulties and / or mental illness are not in
themselves necessarily sufficient grounds to determine that the patient lacks capacity to consent. A patient may lack capacity for some decisions but have the capacity to make others (capacity is ‘decision specific’ and should be assessed for each decision to be made). Where doubt exists concerning the capacity to take the decision then a second opinion may be sought and this must be fully documented in the patient’s clinical notes. A form for recording a mental capacity assessment for individual decisions is available on the Trust’s intranet.
The context of consent can take many different forms, ranging from the active request by a patient of a particular treatment (which may or may not be appropriate or available) to the passive acceptance of a health professional’s advice. In some cases, the health professional will suggest a particular form of treatment or investigation and after discussion the patient may agree to accept it. In others, there may be a number of ways of treating a condition, and the health professional will help the patient to decide between them. Some patients, especially those with chronic conditions, become very well informed about their illness and may actively request particular treatments. In many cases, ‘seeking consent’ is better described as ‘joint decision-making’: the patient and health professional need to come to an agreement on the best way forward, based on the patient’s values and preferences and the health professional’s clinical knowledge.

Consent to Examination or Treatment Policy – January 2020
Lewisham and Greenwich NHS Trust Page 8 of 41
Patients who lack capacity to make valid consent
Where an adult patient lacks the mental capacity (either temporarily or permanently) to give or withhold consent for themselves, no-one else can give consent on their behalf except a person acting under a valid and applicable Lasting Power of Attorney for Health and Care Decisions (Form LP1H) or a Court Appointed Deputy.
A Lasting Power of Attorney and a Court Appointed Deputy are only valid for the time that the patient lacks capacity. The patient should have their mental capacity assessed on a regular basis to ensure that such they still require such measures to remain in place.
However, if the patient has not made a valid and applicable Lasting Power of Attorney, treatment may be given if it is in their best interests, as long as it has not been refused in advance in a valid and applicable Advance Decision. For further details on advance decisions see the Department of Health’s Reference guide to consent for examination or treatment and the Mental Capacity Act 2005.
1.6 The Mental Capacity Act - principles
The Mental Capacity Act (MCA) (2005) was enacted in 2007. It applies to people aged 16 years and over (with the exception of Advance Decisions and Lasting Power of Attorney for Personal Welfare, which only apply to adults – 18 years and above).
It aims to protect people who lack capacity to make particular decisions, but also to maximise their ability to make decisions or to participate in decision making, as far as they are able to do so. The MCA provides that a person is unable to make a decision if they are unable to:
understand the information relevant to the decision, and
retain that information, and
use or weigh that information as part of the process of making the decision, and
communicate her or his decision, whether by talking, using sign language or any other means
If a person fails to meet one or more of the above criteria they will not have capacity to make a decision. If a person is assessed as not having capacity to make a particular decision it should not be assumed that they do not have capacity to make any decisions. Assessing capacity is not just a “tick box” exercise but that the assessor should be framing
the question and then reporting what the patient actually says and adding this to the MCA
form as well as ticking yes or no.
1.7 The five statutory principles of the Mental Capacity Act are:
o A person must be assumed to have capacity unless it is established that they lack
capacity o A person is not to be treated as unable to make a decision unless all practicable steps,
to help him/her to do so, have been taken without success o A person is not to be treated as unable to make a decision merely because she/he
makes an unwise decision o An act done, or decision made, under this Act for or on behalf of a person, who lacks
capacity must be done, or made, in his/her best interests o Before the act is done or the decision is made, regard must be given to whether the
purpose for which it is needed can be as effectively achieved in a way that is less restrictive of the person’s rights and freedom of action

Consent to Examination or Treatment Policy – January 2020
Lewisham and Greenwich NHS Trust Page 9 of 41
A patient’s capacity to understand may be temporarily affected by factors such as confusion, panic, shock, fatigue, pain or medication. In such circumstances however it should not be assumed that they do not have capacity to consent. If a patient is suffering from a temporary incapacity then the way in which she/he is treated should be discussed further to see if the decision can wait until they may regain capacity. Capacity should not be confused with a health professional’s assessment of the reasonableness of the patient’s decision. The patient is entitled to make a decision which is based on their own religious belief or value system. Even if it is perceived by others that the decision is unwise or irrational, the patient may still make that decision if she/he has capacity to do so. An irrational decision has been defined as one which is so outrageous in its defiance of logic or accepted moral standards that no sensible person who had applied his or her mind to the question could have arrived at it. This does not necessarily mean that the person lacks capacity. However if the decision is based upon the patient’s misperception of reality stemming from a disturbance or impairment of the mind or brain then s/he may not have capacity to make that decision. For example, if a patient who is schizophrenic refuses treatment because s/he wrongly believes that the doctor is trying to murder her/him, or a patient with anorexia nervosa refuses food because s/he is unable to comprehend her/his failing physical condition – then these would be relevant factors in assessing whether the patient has capacity. Some cases may not be that clear, and the patient who would normally have capacity may refuse treatment because of a phobia. The courts have held that a woman who required a Caesarean to save her and her baby’s life and refused anaesthetic because of a phobia of needles was suffering from a temporary lack of capacity brought about by panic and fear. The patient might refuse consent because s/he does not believe the advice that s/he is being given. In these cases the professional must make further enquires as to why the patient does not believe that advice. The patient may be refusing treatment because they have a poor relationship with the health professional and simply do not trust them, or the patient may consider that the professional is not sufficiently senior to give the advice. Care should be taken not to underestimate the capacity of a patient with a learning disability. Many people with learning disabilities have the capacity to consent if time is spent explaining to the individual the issues in simple language, using visual aids and signing if necessary. Further information about assessing the capacity of patient generally can be found in the Mental Capacity Act 2005 Code of Practice, and in the Trust’s and local borough’s joint Guide to Assessing Mental Capacity.
1.8 Determining what is in a patient’s Best Interests
When trying to work out the best interests of a person who lacks capacity to make a particular decision the healthcare professional acting as ‘decision maker’ should:
o Encourage participation o Identify all relevant circumstances o Find out the patient’s views o Avoid discrimination o Assess whether the person might regain capacity o If the decision concerns life-sustaining treatment – not be motivated in any way by a
desire to bring about the patient’s death. (Do not make assumptions about the patient’s quality of life)
o Consult others (see section 1.9)

Consent to Examination or Treatment Policy – January 2020
Lewisham and Greenwich NHS Trust Page 10 of 41
o Avoid restricting the patient’s rights – see if there are other options that may be less restrictive
o Take all of the above into account in weighing up and working out what is in the patient’s best interests
1.9 Consulting Others
If it is practical and appropriate to do so (and having regard for the patient’s privacy) the decision maker must consult others for their views about the patient’s best interests and to see if they have any information about their wishes and feelings, beliefs and values. In particular you should try to consult:
o Anyone previously named by the patient as someone to be consulted on either the decision in question or on similar issues
o Anyone engaged in caring for the person o Close relatives, friends or others who take an interest in the person’s welfare o Any attorney appointed under a Lasting Power of Attorney or Enduring Power of
Attorney made by the person o Any deputy appointed by the Court of Protection to make decisions for the person o For decisions about major medical treatment or where the person should live and
where there is no-one who fits into any of the above categories, an Independent Mental Capacity Advocate must be consulted (see section 2.3).
1.10 Exceptions to the Best Interests principle
Where a patient previously (while they had the capacity to do so) made a valid and applicable Advance Decision to refuse medical treatment, has now lost capacity, their advance decision should be respected, even if others think that the decision to refuse treatment is not in their best interests.
1.11 Who can be a decision maker?
Under the Mental Capacity Act many different people may be required to make decisions or act on behalf of someone who lacks capacity to make decisions for them self. The person making the decision is referred to as the ‘decision maker’ and it is their responsibility to work out what is in the person’s best interests. Where the decision involves the provision of medical treatment the doctor or other member of healthcare staff responsible for carrying out the particular treatment or procedure is the decision maker.
If a Lasting Power of Attorney for Personal Welfare has been made and registered, or deputy appointed under a court order, the attorney or deputy will be the decision maker for decisions within the scope of their authority. A member of the healthcare team should normally ask to see such documents to ensure that the scope of this authority is understood by everyone and documented in the patient’s notes.
1.12 Doubt or dispute
Occasionally, there will not be a consensus on whether a particular treatment is in an incapacitated patient’s best interests. Where the situation is not urgent the Decision Maker should where possible hold a Best Interests meeting where all parties involved should discuss their position. The Decision Maker must take the views of all parties into account when weighing up the decision to be made for the person who lacks capacity.
Where there is (or after a Best Interests meeting remains) doubt or dispute as to the patient’s capacity or best interests, and the consequences of having, or not having, the treatment are potentially serious, unresolved or urgent, a court declaration may be sought.

Consent to Examination or Treatment Policy – January 2020
Lewisham and Greenwich NHS Trust Page 11 of 41
Seek further legal advice either via a senior clinician, matron, head of nursing or midwifery or from the Trust’s Legal Department on x6209, Head of Patient Safety x3084 (or mobile via switchboard), or out of hours from the Clinical Site Management Team who if necessary will be able to contact solicitors via the Executive on Call for urgent matters. In the meantime use the guidance in Appendix D for details of information to have ready.
1.13 Sources of Guidance on consent The DH has issued a guidance document on consent, that was update in July 2009;
Reference guide to consent for examination or treatment, 2nd Edition. Any guidance issued before October 2007 may be incorrect to the extent that it fails to take
into account the provisions of the Mental Capacity Act 2005 (MCA).
Health professionals must also be aware of any guidance on consent issued by their own regulatory bodies.
• Reference guide to consent for examination or treatment provides a comprehensive
summary of the current law on consent, and includes requirements of regulatory bodies such as the General Medical Council where these are more stringent. See: www.doh.gov.uk/consent
• 12 key points on consent: the law in England has been distributed widely to health
professionals working in England. This one-page document summarises those aspects of the law on consent which arise on a daily basis and is attached in modified form at Appendix A (amended to comply with the Mental Capacity Act).
• Specific guidance, incorporating both the law and good practice advice, is available
for health professionals working with children, with people with learning disabilities and with older people.
All of the above documents are available via the Department of Health website.
For patients who may lack the mental capacity to give or withhold consent, reference should be made to the Mental Capacity Act 2005 and the accompanying Code of Practice – full guidance can be found at: http://www.publicguardian.gov.uk/
2.0 Documentation
For significant procedures, it is essential for health professionals to document clearly both a patient’s agreement to the intervention and the discussions which led up to that agreement. This may be done either through the use of a consent form (with further detail in the patient’s notes if necessary), or through documenting in the patient’s notes that they have given oral consent.
2.1 Written consent
Consent is often wrongly equated with a patient’s signature on a consent form. A signature
on a form is evidence that the patient has given consent, but is not proof of valid consent. If a patient is rushed into signing a form, on the basis of too little information, the consent may not be valid, despite the signature. Similarly, if a patient has given valid verbal consent, the fact that they are physically unable to sign the form is no bar to treatment. Patients may, if they wish, withdraw consent after they have signed a form: the signature is evidence of the process of consent-giving, not a binding contract.

Consent to Examination or Treatment Policy – January 2020
Lewisham and Greenwich NHS Trust Page 12 of 41
It is rarely a legal requirement to seek written consent but it is good practice to do so if any
of the following circumstances apply:
o the treatment or procedure is complex, or involves significant risks (the term ‘risk’ is used throughout to refer to any adverse outcome, including those which some health professionals would describe as ‘side-effects’ or ‘complications’)
o the procedure involves general / regional anaesthesia or sedation o providing clinical care is not the primary purpose of the procedure o there may be significant consequences for the patient’s employment, social or
personal life o the treatment is part of a project or programme of research approved by this Trust
Completed forms should be kept with the patient’s notes. Any changes to a form, made
after the form has been signed by the patient, should be initialled and dated by both patient and health professional.
It will not usually be necessary to document a patient’s consent to routine and low-risk
procedures, such as providing personal care or taking a blood sample. However, if you have any reason to believe that the consent may be disputed later or if the procedure is of particular concern to the patient (for example if they have declined, or become very distressed about, similar care in the past) it would be helpful to do so.
2.2 Procedures to follow when patients lack capacity to give or withhold consent (please
refer also to sections 1.7 to 1.13 above) Where an adult patient does not have the capacity to give or withhold consent to a
significant intervention, this fact should be documented in Consent Form 4 (form for adults who lack the capacity to consent to investigation or treatment), along with the assessment of the patient’s capacity, why the health professional believes the treatment to be in the patient’s best interests, and the involvement of people close to the patient (as defined in section 1.9). The standard consent forms should never be used for adult patients unable to consent for themselves. For more minor interventions, this information should be entered in the patient’s notes.
An apparent lack of capacity to give or withhold consent may in fact be the result of
communication difficulties rather than genuine incapacity. You should involve appropriate colleagues in making such assessments of incapacity, such as specialist learning disability teams and speech and language therapists, unless the urgency of the patient’s situation prevents this. If at all possible, the patient should be assisted to make and communicate their own decision, for example by providing information in non-verbal ways where appropriate.
2.3 When to instruct an Independent Mental Capacity Advocate (IMCA)
The Trust as a ‘responsible body’ has a duty to instruct and then consult with an IMCA for patients who lack mental capacity and who are otherwise ‘unfriended’ (apart from paid carers) when decisions about serious medical treatment, or changes of accommodation have to be made. The prescribed circumstances are:
o providing, withholding or stopping serious medical treatment o moving a person into long-term care in hospital or a care home, where the person
will stay in hospital longer than 28 days or in a care home for more than 8 weeks
Consent to Examination or Treatment Policy – January 2020
Lewisham and Greenwich NHS Trust Page 13 of 41
o moving the person to a different hospital or care home An IMCA may also be instructed to support someone who lacks capacity to make decisions concerning:
o care reviews, where no-one else is available to be consulted o adult protection cases, whether or not family, friends or others are involved.
The IMCA’s role is to support and represent the person who lacks capacity. Because of this IMCAs have the right to see relevant healthcare and social care records. They also have the right to meet the person they are supporting in private. Any information or reports provided by an IMCA must be taken into account as part of the process of working out whether a proposed decision is in the person’s best interests. The involvement of an IMCA in a case and any information the IMCA provides to help decision making must be documented in the patient’s notes. All relevant people must be informed when an IMCA is working on a person’s case. Decision makers (i.e.: usually the doctor in charge of the patient’s care) must inform the IMCA of the final decision taken and the reason for it.
2.4 How to contact an IMCA for Lewisham & Greenwich NHS Trust patients
See Appendix B and / or the flyers on the Trust intranet (type IMCA into the search box). 2.5 Availability of consent forms
Standard consent forms and forms for adults who are unable to consent for themselves are reproduced in Appendix B and are available in ward areas. There are three versions of the standard consent form: form 1 for adults or competent children, form 2 for parental (or person who has parental responsibility) consent to investigation and treatment for a child or young person and form 3 for cases where it is envisaged that the patient will remain alert throughout the procedure and no anaesthetist will be involved in their care. The use of form 3 is optional but may be thought more appropriate than form 1 in situations where patients do not need to be made aware of issues surrounding general or regional anaesthesia and do not need to make any advance decisions about additional procedures because they will be in a position to make any such decisions at the time if necessary. In addition there are two further consent forms. Form 4 (as referred to in previous sections) for adults who lack the capacity to consent to investigation or treatment; and consent form 5 for medical treatment of a patient who refuses to have a blood transfusion (including Jehovah’s Witness patients.
Individual specialties may choose to have the model consent forms pre-printed to include certain common treatments or investigations (such as endoscopy). These should be submitted to the Head of Legal Services for approval before being introduced.
3.0 When should consent be sought?
When a patient formally gives their consent to a particular intervention, this is only the endpoint of the consent process. It is helpful to see the whole process of information provision, discussion and decision-making as part of ‘seeking consent’. This process may take place at one time, or over a series of meetings and discussions, depending on the seriousness of what is proposed and the urgency of the patient’s condition.

Consent to Examination or Treatment Policy – January 2020
Lewisham and Greenwich NHS Trust Page 14 of 41
3.1 Single stage process In many cases, it will be appropriate for a health professional to initiate a procedure
immediately after discussing it with the patient. For example, during an ongoing episode of care a physiotherapist may suggest a particular manipulative technique and explain how it might help the patient’s condition and whether there are any significant risks. If the patient is willing for the technique to be used, they will then give their consent and the procedure can go ahead immediately. In many such cases, consent will be given orally.
If a proposed procedure carries significant risks, it will be appropriate to seek written
consent, and health professionals must take into consideration whether the patient has had sufficient chance to absorb the information necessary for them to make their decision. As long as it is clear that the patient understands and consents, the health professional may then proceed.
3.2 Two or more stage process In most cases where written consent is being sought, treatment options will generally be
discussed well in advance of the actual procedure being carried out. This may be on just one occasion (either within primary care or in a hospital out-patient clinic), or it might be over a whole series of consultations with a number of different health professionals. The consent process will therefore have at least two stages: the first being the provision of information, discussion of options and initial (oral) decision, and the second being confirmation that the patient still wants to go ahead. The consent form should be used as a means of documenting the information stage(s), as well as the confirmation stage.
Patients receiving elective treatment or investigations for which written consent is appropriate should be familiar with the contents of their consent form before they arrive for the actual procedure, and should have received a copy of the page documenting the decision-making process. They may be invited to sign the form, confirming that they wish treatment to go ahead, at any appropriate point before the procedure: in out-patients, at a pre-admission clinic, or when they arrive for treatment. If a form is signed before patients arrive for treatment, however, a member of the healthcare team must check with the patient at this point whether they have any further concerns and whether their condition has changed. This is particularly important where there has been a significant lapse of time between the form being signed and the procedure. When confirming the patient’s consent and understanding, it is advisable to use a form of words which requires more than a yes/no answer from the patient: for example beginning with “tell me what you’re expecting to happen”, rather than “is everything all right?”
While administrative arrangements will vary, it should always be remembered that for
consent to be valid, the patient must feel that it would have been possible for them to refuse, or change their mind. It will rarely be appropriate to ask a patient to sign a consent form after they have begun to be prepared for treatment (for example, by changing into a hospital gown), unless this is unavoidable because of the urgency of the patient’s condition.
3.3 Seeking consent for anaesthesia Where an anaesthetist is involved in a patient’s care, it is their responsibility (not that of a
surgeon) to seek consent for anaesthesia, having discussed the benefits and risks. However, in elective treatment it is not acceptable for the patient to receive no information about anaesthesia until their pre-operative visit from the anaesthetist: at such a late stage the patient will not be in a position genuinely to make a decision about whether or not to undergo anaesthesia. Patients should therefore either receive a general leaflet about anaesthesia in out-patients, or have the opportunity to discuss anaesthesia in a pre-assessment clinic. The anaesthetist should ensure that the discussion with the patient and their consent is documented in the anaesthetic record, in the patient’s notes or on the

Consent to Examination or Treatment Policy – January 2020
Lewisham and Greenwich NHS Trust Page 15 of 41
consent form. Where the clinician providing the care is personally responsible for anaesthesia (e.g. where local anaesthesia or sedation is being used), then he or she will also be responsible for ensuring that the patient has given consent to that form of anaesthesia.
In addition, where general anaesthesia or sedation is being provided as part of dental treatment, the General Dental Council currently holds dentists responsible for ensuring that the patient has all the necessary information. In such cases, the anaesthetist and dentist will therefore share that responsibility.
3.4 Emergencies
Clearly in emergencies, the two stages (discussion of options and confirmation that the patient wishes to go ahead) will follow straight on from each other, and it may often be appropriate to use the patient’s notes to document any discussion and the patient’s consent, rather than using a form. The urgency of the patient’s situation may limit the quantity of information that they can be given, but should not affect its quality.
3.5 Treatment of Children and Young People
For the purposes of this policy ‘children’ refers to patients aged below 16 and ‘young people’ refers to patients aged 16-17. 3.5.1 Validity of Consent:
Although a child or young person may have the capacity to give consent, this is only valid if it is given voluntarily.
This requirement must be considered carefully as children and young people may be subject to undue influence by their parent(s), other carers or a sexual partner (current or potential), and it is important to establish that the decision is that of the individual him or herself.
Consent will also be valid if it meets the same criteria as that for adults i.e. consent is given voluntarily by an appropriately informed young person capable of consenting to the particular intervention.
The legal position concerning consent and refusal by those under the age of 18 is different from the position of adults.
3.5.2 Young people aged 16 – 17
Young people aged 16 – 17 are presumed to be capable of consenting to their own medical treatment, and any ancillary procedures involved in that treatment, such as an anaesthetic[1].
The refusal of treatment of a competent person aged 16 – 17 may in some circumstances be overridden by either a person with parental responsibility or a court.
In order to ascertain whether a young person has the capacity to consent to treatment the same requisite for adults should be applied as per the Mental Capacity Act and Deprivation of Liberty Safeguards Policy.
However if a young person is unable to make the decision not because they lack mental capacity but because they are overwhelmed by the implications of the decision then the Mental Capacity Act[2] will not apply.
In situations when it’s unclear whether a young person lacks capacity within the meaning of the Act a court declaration should be sought.
[1]
Section 8 – Family Law Reform Act 1969 [2]
www.publicguardian.gov.uk/mca/code-of-practice.htm

Consent to Examination or Treatment Policy – January 2020
Lewisham and Greenwich NHS Trust Page 16 of 41
If the 16/17 year old is capable of giving valid consent then it is not legally necessary to obtain consent from a person with parental responsibility for the young person in addition to the consent of the young person.
However it is good practice to involve the young person’s family in the decision making process unless the young person specifically wishes to exclude them.
3.5.3 Children under 16
In the case of Gillick[3], the court held that children who have sufficient understanding and intelligence to enable them to understand fully what is involved in a proposed intervention will also have the capacity to consent to that intervention.
This is sometimes described as being ‘Gillick competent’. A child of under 16 may be Gillick competent to consent to medical treatment, research, donation or any other activity that requires their consent.
As the concept of Gillick competence reflect a child’s increasing development to maturity, thus a child under 16 may have the capacity to consent to some interventions but not to others. Therefore the child’s capacity to consent should be assessed carefully in relation to each decision that needs to be made.
If the child is Gillick competent and is able to give voluntary consent after receiving appropriate information, that consent will be valid and additional consent by a person with parental responsibility will not be required.
It is, however, good practice to involve the child’s family in the decision-making process, if the child consents to their information being shared.
If the child seeks advice or treatment in relation to abortion and cannot be persuaded to inform her parent(s), every effort should be made to help the child find another adult (such as another family member or a specialist youth worker) to provide support to the child.
3.5.4 Child or young person refusing treatment
Where a young person of 16 or 17 who could consent to treatment, or a child under 16 but Gillick competent, refuses treatment, it is possible that such a refusal could be overruled if it would in all probability lead to the death of the child/young person or to severe permanent injury.
Courts[4] have in the past stated that it has jurisdiction to override a refusal of a child/young person, where the refusal of treatment would in all probability lead to the death of the child/young person or to severe permanent injury; or where there is a serious and imminent risk that the child/young person will suffer grave and irreversible mental or physical harm.
The courts[5] have also agreed for parents to consent to their competent child being treated even where the child/young person is refusing treatment.
However, there is no post-Human Rights Act 1998 authority for this proposition, therefore cases similar to this should be referred to the Legal Services Manager to seek a court declaration or decision if faced with a competent child or young person who is refusing to consent to treatment, to determine whether it is lawful to treat the child.
Where the treatment involved is for mental disorder, clinicians should consider using the mental health legislation.
The changes made to section 131 of the Mental Health Act 1983 by section 43 of the Mental Health Act 2007 mean that when a young person of 16 or 17 has capacity (as defined in the Mental Capacity Act 2005) and does not consent to admission for treatment for mental disorder (either because they are overwhelmed, do not want to consent or refuse to consent), they cannot then be admitted informally on the basis of the consent of a person with parental responsibility (see chapter 36 of the Code of Practice to the Mental Health Act 1983, as amended 2008).
[3]
Gillick v West Norfolk and Wisbech AHA (1986) AC 112 [4]
Re W (a minor) (medical treatment) [1992] 4 All ER 627 52 [5]
Re R (a minor) (wardship: medical treatment) [1991] 4 All ER 177

Consent to Examination or Treatment Policy – January 2020
Lewisham and Greenwich NHS Trust Page 17 of 41
A life-threatening emergency may arise when consultation with either a person with parental responsibility or the court is impossible, or the person with parental responsibility refuses consent despite such emergency treatment appearing to be in the best interests of the child. In such cases the courts have stated that doubt should be resolved in favour of the preservation of life, and it will be acceptable to undertake treatment to preserve life or prevent serious damage to health.
3.5.5 Child lacking capacity
Where a child under the age of 16 lacks capacity to consent (i.e. is not Gillick competent), consent can be given on their behalf by any one person with parental responsibility or by the court.
As is the case where patients are giving consent for themselves, those giving consent on behalf of child patients must have the capacity to consent to the intervention in question, be acting voluntarily and be appropriately informed.
The power to consent must be exercised according to the ‘welfare principle’: that the child’s ‘welfare’ or ‘best interests’ must be paramount. Even where a child lacks capacity to consent on their own behalf, it is good practice to involve the child as much as possible in the decision-making process.
Where necessary, the courts can overrule a refusal by a person with parental responsibility. It is recommended that certain important decisions, such as sterilisation for contraceptive purposes, should be referred to the Legal Services Manager refer to Appendix D, even if those with parental responsibility consent to the operation going ahead.
In situations where there is continuing disagreement or conflict between those with parental responsibility and doctors, and where the child is not competent to provide consent, the Legal Services Manager should be contacted so that court can be involved to clarify whether a proposed treatment, or withholding of treatment, is in the child’s best interests. Parental refusal can only be overridden in an emergency.
3.5.6 Parental Responsibility The Children Act 1989 sets out persons who may have parental responsibility. These include:
the child’s mother
the child’s father, if he was married to the mother at the time of birth
unmarried fathers, can acquire parental responsibility in several different ways please contact the Legal Services Manager for further information
unmarried fathers who register their child’s birth jointly with the mother will automatically acquire parental responsibility the child’s legally appointed guardian
a person in whose favour the court has made a residence order concerning the child
a local authority designated in a care order in respect of the child
courts may appoint a guardian for a child who has no parent with parental responsibility
parents with parental responsibility may also appoint a guardian in the event of their own death
a local authority or other authorised person who holds an emergency protection order in respect of the child. Such a person might choose to do this, for example, if a child minder or the staff of a boarding school have regular care of their child. As only a person exercising parental responsibility can give valid consent, in the event of any doubt then specific enquiry should be made.
Foster parents do not automatically have parental responsibility.
Consent given by one person with parental responsibility is valid, even if another person with parental responsibility withholds consent. However, it is good practice that a ‘small group of important decisions’ should not be taken by one person with parental responsibility against the wishes of another, e.g. on-therapeutic male
circumcision and immunisation.
Consent to Examination or Treatment Policy – January 2020
Lewisham and Greenwich NHS Trust Page 18 of 41
Where persons with parental responsibility disagree as to whether these procedures are in the child’s best interests, it is advisable to refer the decision to the courts via the Legal Services Manager.
Where there is doubt about whether a parent is acting in the interest of the child or young person, then the health professional would be unwise to rely on the parent’s consent, for example if a child alleges abuse and the parent supports psychiatric treatment for the child. The Government’s guidance Working Together to Safeguard Children covers situations involving parental consent where abuse or neglect is suspected[6].
In order to consent on behalf of a child, the person with parental responsibility must themselves have capacity. Where the person with parental responsibility for a child is themselves under 18, they will only be able to give valid consent for the child’s treatment if they themselves are Gillick competent.
Where a child is a ward of court, no important step may be taken in the life of the child without the prior consent of the court. This is likely to include more significant medical interventions but not treatment for minor injuries or common diseases of childhood.
In an emergency, it is justifiable to treat a child who lacks capacity without the consent of a person with parental responsibility, if it is impossible to obtain consent in time and if the treatment is vital to the survival or health of the child.
3.5.7 Research in children/young persons
Where children lack capacity to consent for themselves, parents may give consent for their child to be entered into a trial where the evidence is that the trial therapy may be at least as beneficial to the patient as the standard therapy.
It may also be compatible with the welfare principle for a person with parental responsibility to give consent to a research intervention that is not strictly in the best interests of the child, but is not against the interests of the child either. Such an intervention must involve only minimal burden to the child.
Decisions about experimental treatment must be made in the child’s best interests. 3.5.8 Using children as bone marrow donors
This is covered by the Human Tissue Authority’s code of practice on donation of allogeneic bone marrow and peripheral blood stem cells for transplantation, and healthcare professionals should consult this for detailed information on the legal requirements and how to proceed.
4.0 Provision of information
The provision of information is central to the consent process. Before patients can come to a decision about treatment, they need comprehensible information about their condition and about possible treatments/investigations and their risks and benefits (including the risks/benefits of doing nothing). They also need to know whether additional procedures are likely to be necessary as part of the procedure, for example a blood transfusion, or the removal of particular tissue. Once a decision to have a particular treatment/investigation has been made, patients need information about what will happen: where to go, how long they will be in hospital, how they will feel afterwards and so on.
Patients and those close to them will vary in how much information they want: from those who want as much detail as possible, including details of rare risks, to those who ask health
[6]
HM Government (2006) Working Together to Safeguard Children: A guide to inter-agency working to
safeguard and promote the welfare of children. London: HM Government.
www.dh.gov.uk/en/PublicationsandStatistics/Publications/PublicationsPolicyAndGuidance/ DH_4007781

Consent to Examination or Treatment Policy – January 2020
Lewisham and Greenwich NHS Trust Page 19 of 41
professionals to make decisions for them. There will always be an element of clinical judgement in determining what information should be given. However, the presumption must be that the patient wishes to be well informed about the risks and benefits of the various options. Where the patient makes clear (verbally or non-verbally) that they do not wish to be given this level of information, this should be documented. A decision by the House of Lords established that a health professional can be liable even in cases where it cannot be proved on the balance of probabilities that their negligence caused harm to the patient. In the case a Miss Chester could not prove that she would never have consented to the operation if she had been informed of the risks, but the surgeon was still liable because Miss Chester had not given her informed consent. This decision has serious implications for health professionals. Failure to take adequate consent now over-rides any argument that such failure did not cause the adverse outcome, provided that the warning ought to have been given, and the condition or consequence which ought to have been mentioned actually develops. The GMC states that doctors should do their best to find out about patient’s individual needs and priorities when providing information about treatment options. If the patient asks specific questions about the procedure and associated risks these should be answered truthfully. When giving advice about proposed treatment health professionals should:
take extreme care in the taking of consent, which is more crucial than ever
give careful and comprehensible warnings about all significant possible adverse outcomes and any material risks, and of any reasonable alternative or variant treatment; also the risks of not accepting the proposed treatment
ensure that warnings are properly recorded in the clinical notes
invite the patient to sign the relevant entry to confirm that s/he has been given the warning, has understood it and accepts the risks
make a full entry in the notes, preferably signed by the patient, if treatment is refused, including the reason when given
The Supreme Court judgment in the case of Montgomery v Lanarkshire Health Board in clarified the law in relation to consent in relation to the GMC’s guidance on ‘materiality’ of risk, thus: • The test of materiality is whether, in the circumstances a reasonable person in the
patient’s position would be likely to attach significance to the risk, or the doctor is or should reasonably be aware that the particular patient would be likely to attach significance to it.
• The assessment of whether a risk is material cannot be reduced to percentages. Factors include the nature of the risk, the effect its occurrence would have on the life of the patient, the importance to the patient of the benefits from the treatment, the alternatives available and their risks. The assessment is fact-sensitive and specific to the characteristics of the patient.
• The doctors’ duty is not fulfilled simply by providing technical information which the patient cannot understand, or by routinely demanding a signature on a consent form.
• There is a therapeutic exception, where disclosure of a particular matter would be detrimental to the health of a patient, but this is a very limited exception.
It is therefore important that consenting practices move quickly away from focusing on the percentage risk of occurrence and instead consider the materiality of the risk from the perspective of the patient.

Consent to Examination or Treatment Policy – January 2020
Lewisham and Greenwich NHS Trust Page 20 of 41
4.1 Patient Information Leaflets and other media The use of patient information leaflets is considered to be an effective tool that can be used by health professionals to provide patients with the information they need to help them to arrive at an informed decision. Patients can review the information after a consultation which may prompt them to ask further questions so that they fully understand the treatment being proposed. In this context the use of patient information leaflets is considered to be an example of best practice.
• Patient information leaflets / media (produced in house or obtained from third parties) in
use in the Trust must be registered with the Head Librarian. The Trust Policy on producing Patient Information is available on Trust intranet and sets out the standard required for the production of in house patient information leaflets, videos or other sources of information. All such information must include the benefits, risks and available alternatives and their known benefits and risks. (See also section 5.1 re documentation).
• Some patients may need access to information in large font or to non-written material if they have visual difficulties or are not able to read. The Trust supports the practice of staff offering to tape record specified consultations where complex information may be given, so that the patient can listen to it more than once.
Archive of Information Given to Patients
• All in house produced patient information will contain a reference number, a date of introduction and a review date and is archived by the Trust’s Head Librarian. Where clinical areas use externally produced printed information a sample must be sent to the Librarian for archiving.
4.2 Withholding Information
Some patients may wish to know very little about the treatment which is being proposed and may ask that the health professional or other person should make decision on their behalf. In such circumstances the health professional should explain the importance of knowing about the treatment and try to encourage the patient to make the decisions for him or herself. If the patient still declines any information offered, it is essential to record this fact in the notes and to ask the patient to sign the record to confirm their decision. It is possible that a patient’s decision may change over time and it is important to provide opportunities for them to express this. GMC guidance encourages doctors to explain to patient the importance of knowing the options open to them and states that basic information should always be provided.
4.3 Provision for patients whose first language is not English
This Trust is committed to ensuring that patients whose first language is not English receive the information they need and are able to communicate appropriately with healthcare staff. It is not appropriate to use children to interpret for family members who do not speak English.
How to contact local interpreting services Enter ‘Interpreter’ into the search box on the front page of Trust intranet. This also includes contact details for interpreting support for deaf / blind people.

Consent to Examination or Treatment Policy – January 2020
Lewisham and Greenwich NHS Trust Page 21 of 41
4.4 Access to more detailed / specialist information Patients may sometimes request more detailed information about their condition or about a
proposed treatment than that provided in general leaflets.
Most clinical specialists will be in a position to recommend or provide more detailed information. Further information may be accessed via the PALS and Complaints Department based at QEH site - (Monday to Friday 0900 – 1630) on x4592 (answerphone if no one available to take call)
4.5 Access to health professionals between formal appointments
After an appointment with a health professional in primary care or in out-patients, patients will often think of further questions which they would like answered before they take their decision. Where possible, it will be much quicker and easier for the patient to contact the healthcare team by phone than to make another appointment or to wait until the date of an elective procedure (by which time it is too late for the information genuinely to affect the patient’s choice). The consent form includes a space in which the contact number of a suitable member of staff should be inserted, through whom the patient can seek further information.
Many patient information leaflets are being developed at the Trust that include telephone numbers of staff with specialist knowledge that the patient can contact for further information (see Trust intranet).
4.6 Open access clinics
Where patients access clinics directly, it should not be assumed that their presence at the clinic implies consent to particular treatment. You should ensure that they have the information they need and have given valid consent before proceeding with an investigation or treatment.
5.0 Who is responsible for seeking consent?
The health professional carrying out the procedure is ultimately responsible for ensuring that the patient is genuinely consenting to what is being done: it is they who will be held responsible in law if this is challenged later.
Where oral or non-verbal consent is being sought at the point the procedure will be carried out, this will naturally be done by the health professional responsible. However, team work is a crucial part of the way the NHS operates, and where written consent is being sought it may be appropriate for other members of the team to participate in the process of seeking consent.
5.1 Process for documenting the discussion and provision of information to patients • The reference number and title of any written or recorded information given to the
patient should be recorded (normally on the Consent Form, or in the patient’s clinical record) by the person giving it to a patient. This will help to provide evidence of the current information given to a patient should a challenge to the consent process be made in future.
• The information giving process may be one session or take place over several encounters between the patient and professional staff depending on the decision to be made in the patient’s individual situation.

Consent to Examination or Treatment Policy – January 2020
Lewisham and Greenwich NHS Trust Page 22 of 41
• All information provided verbally to patients about the benefits and risks and any alternatives of a proposed procedure and discussions supporting a patient to make their decision must be clearly documented in the patient’s notes and the key points on the appropriate Consent Form (Appendix C) when used.
5.2 Completing consent forms
The standard consent form provides space for a health professional to provide information to patients and to sign confirming that they have done so. Completed consent forms must be secured into the patient’s health record / clinical notes. Any changes made to a form after it has been signed by the patient should be dated and initialled by both patient and health professional. Consent is often wrongly equated with a patient’s signature on a consent form. A signature on a consent form is evidence that the patient has given consent but is not proof of valid consent. If a patient is rushed into signed a form on the basis of too little information the consent may not be valid despite the signature. Similarly if a patient has given valid verbal consent the fact that they are physically unable to sign the form is no bar to treatment. Patents may if they wish withdraw consent after they have signed a form; the signature is evidence of the process of consent giving, not a binding contract.
5.3 Capability of the Health Professional and Delegated Consent
The health professional providing the information must be competent to do so: either because they themselves carry out the procedure, or because they have received specialist training in advising patients about this procedure, have been assessed, are aware of their own knowledge limitations and are subject to audit.
Lewisham and Greenwich NHS Trust requires that the health professional obtaining consent is also capable of undertaking the procedure, OR…. where the health professional is not yet capable of carrying out the procedure without supervision (e.g.: a doctor in training, or specialist nurse taking consent for a procedure which another professional will carry out), they must be assessed and authorised as competent by their consultant to obtain consent for that specific procedure. The assessment and authorisation must be documented and submitted to a register kept by the Governance Lead for each Division. This process will be subject to audit.
All healthcare professionals will be made aware of this requirement at induction and Consultants should assess their juniors as soon as practicable after starting at the Trust. Professional heads of practice for professions other than medicine are responsible for ensuring that systems are in place in their areas for identifying any procedures for which their practitioners will need to obtain consent and ensuring that a competency framework is in place for obtaining consent.
5.4 Process for following up those who have obtained consent for a procedure without
authorisation If it is identified that a health professional has obtained consent for a procedure in a non-urgent situation without being authorised to do so, the reasons will be reviewed and remedial action taken. The healthcare professional will be stopped from undertaking the consent process until an individualised competency assessment can be undertaken and authorisation conferred.

Consent to Examination or Treatment Policy – January 2020
Lewisham and Greenwich NHS Trust Page 23 of 41
If there is an opportunity the consultant will speak with the affected patient personally and / or check the evidence of the information given by the unauthorised person. The incident will be reported on an incident report form in order that the root cause may be investigated. Where a concern is identified the GMC will be notified by the Director of Medical Education using the required form (GMC website: Consent and Induction Form). http://www.gmcuk.org/NHSLA_Consent_Form.doc_47409657.doc
5.5 Confirmation of Consent
If the patient signs the form in advance of the procedure (for example in out-patients or at a pre-assessment clinic), a health professional involved in their care on the day should sign the form to confirm that the patient still wishes to go ahead and has had any further questions answered. It will be appropriate for any member of the healthcare team (for example a nurse admitting the patient for an elective procedure) to provide the second signature, as long as they have access to appropriate colleagues to answer questions they cannot handle themselves.
Any member of staff who is asked a supplementary question by a patient which is outside their immediate professional expertise to be able to answer, should not countersign the form unless or until they are satisfied that: i. an appropriate professional has addressed any outstanding concerns of the patient
(the person confirming consent must ensure this is arranged before the procedure goes ahead), and
ii. the patient had received full information to enable him/her to make a decision on
whether or not they wish the proposed procedure to go ahead. 5.6 Responsibility of health professionals
It is a health professional’s own responsibility:
• to ensure that when they require colleagues to seek consent on their behalf they are confident that the colleague is competent to do so; and
• to work within their own competence and not to agree to perform tasks which
exceed that competence. If you feel that you are being pressurised to seek consent when you do not feel competent to do so please contact one of the following for advice:
i. the Director of Service for your specialty / Division ii. the Medical Director or Deputy Medical Director for Quality and Safety iii. Legal Services Manager via QEH Switchboard
6.0 Refusal of treatment
If the process of seeking consent is to be a meaningful one, refusal must be one of the patient’s options. A competent adult patient is entitled to refuse any treatment, except in circumstances governed by the Mental Health Act 1983. The situation for children is more complex: see the Department of Health’s Seeking consent: working with children for more detail. The following paragraphs apply primarily to adults.

Consent to Examination or Treatment Policy – January 2020
Lewisham and Greenwich NHS Trust Page 24 of 41
If, after discussion of possible treatment options, a patient refuses all treatment, this fact should be clearly documented in their notes. If the patient has already signed a consent form, but then changes their mind, you (and where possible the patient) should note this on the form.
Where a patient has refused a particular intervention, you must ensure that you continue to provide any other appropriate care to which they have consented. You should also ensure that the patient realises they are free to change their mind and accept treatment if they later wish to do so. Where delay may affect their treatment choices, they should be advised accordingly.
If a patient consents to a particular procedure but refuses certain aspects of the intervention, you must explain to the patient the possible consequences of their partial refusal. If you genuinely believe that the procedure cannot be safely carried out under the patient’s stipulated conditions, you are not obliged to perform it. You must, however, continue to provide any other appropriate care. Where another health professional believes that the treatment can be safely carried out under the conditions specified by the patient, you must on request be prepared to transfer the patient’s care to that health professional. If a patient lacks the mental capacity to give or withhold consent but has made an Advance Decision refusing the treatment, this must be followed (if it is valid and applicable to the situation). If the treatment is life-sustaining the Advance Decision to refuse treatment must comply with the requirements of the Mental Capacity Act 2005.
7.0 Withdrawal of Consent
A person with capacity is entitled to withdraw consent at any time, including during the performance of a procedure. Where a person does object during treatment, it is good practice for the practitioner, if at all possible, to stop the procedure, establish the person’s concerns and explain the consequences of not completing the procedure. At times, an apparent objection may in fact be a cry of pain rather than withdrawal of consent, and appropriate reassurance may enable the practitioner to continue with the person’s consent. If stopping the procedure at that point would genuinely put the life of the person at risk, the practitioner may be entitled to continue until that risk no longer applies. Assessing capacity during a procedure may be difficult and, as noted above, factors such as pain, panic and shock may diminish capacity to consent. The practitioner should try to establish whether at that time the person has capacity to withdraw a previously given consent. If capacity is lacking, it may sometimes be justified to continue in the person’s best interests, but this should not be used as an excuse to ignore distress.
8.0 Tissue (Human Tissue Act)
The legal position regarding the use of human tissue (including blood samples and other bodily fluids provided for testing) raises some difficult issues. Such tissue can be very valuable in education and research, and its use may lead to developments in medical knowledge and hence improvements in healthcare for all. At present, this Trust requires that patients should be given the opportunity to refuse permission for tissue taken from them during surgery or other procedure to be used for education or research purposes.
The Human Tissue Act 2004 does not require consent to be obtained if tissue is to be stored and/or used for education or training. The Act also does not require consent for research provided that the research is ethically approved and the tissue is anonymised; although consent is preferable. For further guidance contact the Research and Development Manager or The Trust’s Designated Individual under the Human Tissue Act
Consent to Examination or Treatment Policy – January 2020
Lewisham and Greenwich NHS Trust Page 25 of 41
The Act also established the Human Tissue Authority (HTA) which is responsible for approving the transplantation of organs from living donors and bone marrow and peripheral blood stem cells from adults who lack the capacity to consent and children who lack the competence to consent. Further guidance on consent and codes of practice are available on the HTA’s website www.hta.gov.uk. The Trust’s Designated Individual under the Human Tissue Act may also be contacted for advice. The professional obtaining consent should discuss with the patient any specimens or tissue that may be taken when considering the section on the consent form ‘other procedures that may be necessary’. If the patient objects or has special requests for the tissue this must be clearly recorded on the consent form. In this event the laboratory and operating theatre staff must also be informed so that they can ensure the patient’s wishes are respected. If the patient’s wishes for the body parts give rise to any concern, this must be explored in detail and resolved before any procedure goes ahead. (For example, the pathologist must be able to give advice on proposed storage or disposal methods to the patient, to reach a mutually acceptable plan for any tissue to body part removed).
Explicit consent is not necessary for public health surveillance using the unlinked
anonymous method but a well-publicised opt-out policy must apply. This is applied to the universal HIV status screening of women in the antenatal clinic.
Tissue samples may be used for quality assurance purposes without requiring specific
patient consent provided there is an active policy of informing patients of such use. This is essential to ensure the high quality of service that all patients have the right to expect. Wherever possible, samples of tissue used in this way should be anonymised or pseudonymised.
9.0 Clinical photography and video recordings Photographic and video recordings made for clinical purposes form part of a patient’s
record. Although consent to certain recordings, such as X-rays, is implicit in the patient’s consent to the procedure, health professionals should always ensure that they make clear in advance if any photographic or video recording will result from that procedure.
If the need for photographic or video recordings arises during anaesthesia the patient should be advised retrospectively and this consent documented in the patient’s clinical records; if the patient declines to consent the records must be destroyed,
Photographic and video recordings which are made for treating or assessing a patient must
not be used for any purpose other than the patient’s care or the audit of that care, without the express consent of the patient or a person with parental responsibility for the patient. The one exception to this principle is set out below. If you wish to use such a recording for education, publication or research purposes, you must seek consent in writing, ensuring that the person giving consent is fully aware of the possible uses of the material. In particular, the person must be made aware that you may not be able to control future use of the material once it has been placed in the public domain. If a child is not willing for a recording to be used, you must not use it, even if a person with parental responsibility consents.
Photographic and video recordings, made for treating or assessing a patient and from
which there is no possibility that the patient might be recognised, may be used within the clinical setting for education or research purposes without express consent from the patient, as long as this policy is well publicised. However, express consent must be sought for any form of publication.
If you wish to make a photographic or video recording of a patient specifically for education,
publication or research purposes, you must first seek their written consent (or where

Consent to Examination or Treatment Policy – January 2020
Lewisham and Greenwich NHS Trust Page 26 of 41
appropriate that of a person with parental responsibility) to make the recording, and then seek their consent to use it. Patients must know that they are free to stop the recording at any time and that they are entitled to view it if they wish, before deciding whether to give consent to its use. If the patient decides that they are not happy for any recording to be used, it must be destroyed. Patients have the right to withdraw consent for the use of their recordings at any time. If a patient decides to withdraw consent, the records must be destroyed (subject to ongoing legal and/or coroner’s considerations)
As with recordings made with therapeutic intent, patients must receive full information on the possible future uses of the recording, including the fact that it may not be possible to withdraw it once it is in the public domain.
The situation may sometimes arise where you wish to make a recording specifically for education, publication or research purposes, but the patient is temporarily unable to give or withhold consent because, for example, they are unconscious. In such cases, you may make such a recording, but you must seek consent as soon as the patient regains capacity. You must not use the recording until you have received consent for its use, and if the patient does not consent to any form of use, the recording must be destroyed.
If the patient is likely to be permanently unable to give or withhold consent for a recording to be made, you should seek the agreement of some-one close to the patient. You must not make any use of the recording which might be against the interests of the patient. You should also not make, or use, any such recording if the purpose of the recording could equally well be met by recording patients who are able to give or withhold consent. Further guidance on the limited situations where it may be acceptable to proceed without explicit consent are available from the General Medical Council. Even in these circumstances, consent should be sought unless it is impractical to do so. For further information and a consent form for clinical photography see the Trust’s Code of Responsible Practice for Photographic and Video Recording available on Trust intranet; guidance available from the Design and Photography Department Manager. It should be noted that the Mental Capacity Act requires certain research carried out on, or in relation to, a person who lacks capacity to consent to be authorised under the procedure set out in the Act.
10.0 Training
All staff involved in the consent process must access and familiarise themselves with this policy.
General training on the principles of consent to examination and treatment in English law is available as below:
Principles of Consent – taught revision session on Corporate Induction, (45 minutes using a quiz / answers format)
3 yearly update via e-learning including a training package and a test
Junior doctors receive a lecture on consent as part of their training programme 10.1 Delegated Consent Training (refer to section 5.3) The GMC’s standards in relation to postgraduate medical education and training state that ‘before seeking consent both trainee and supervisor must be satisfied that the trainee understands the proposed intervention and its risks, and is prepared to answer questions the patient may ask. If they are unable to do so they should have access to a supervisor

Consent to Examination or Treatment Policy – January 2020
Lewisham and Greenwich NHS Trust Page 27 of 41
with the required knowledge. Trainees must act in accordance with the GMC’s guidance Consent: patients and doctors making decisions together (2008)’. (The Trainee Doctor, mandatory requirement 1.4) This Trust requires that all practitioners obtaining consent must be capable of undertaking the procedure, however there may be occasions where the practitioner is unable to undertake the procedure independently (i.e.: supervision is still required). Consultants will assess their juniors as soon as practicable after starting at the Trust and ensure that specific training is provided as required. Procedure specific training must consist of the following:
theoretical input into the legal, ethical and professional aspects of consent
the benefits, risks and any alternatives to the procedure
identification of how to seek assistance if unable to answer the patient’s questions
the consultant should when possible observe the member of staff undertaking the consent process with a patient before they are allowed to undertake the task alone

Consent to Examination or Treatment Policy – January 2020
Lewisham and Greenwich NHS Trust Page 28 of 41
11.0 Monitoring Compliance With and the Effectiveness of this policy Failure to manage the risks inherent in obtaining valid consent from a patient would expose the Trust and individual practitioners to the risk of challenge through the clinical negligence process and risk to reputation, and individual practitioners to civil and / or criminal action, and / or disciplinary action by their professional regulatory body. It is therefore crucial that the appropriate implementation of this policy is monitored and changes made where deficiencies are identified. The Quality and Safety Committee will therefore monitor the quality of the consent process within the Trust through the methods set out below:
Element to be monitored Lead Tool Frequency Reporting arrangements
Action Lead(s) Change in practice and lessons to be shared
Quality of the consent process to include at a minimum:
process for obtaining consent
evidence of the process for providing patients with information to support their decision making (which includes benefits/ risks / where appropriate alternatives, and the consequences of not accepting the proposed procedure)
process for documenting the discussion and provision of information to patient
process for recording consent (on consent forms / in clinical records)
Divisional Directors of Nursing, Governance and Quality
Audit of completion of consent forms using audit tool in Appendix G
Annually Quality and Safety Committee
Medical Director / Head of Medical Education / Divisional Governance Leads / Heads of Nursing (where other healthcare practitioners take consent for procedures they are competent to perform)
Required changes to practice will be identified and actioned within a specific time frame. The Director of Service will be required to take each change forward within their Directorate and report back to the Medical Director on effectiveness. Lessons will be shared with all the relevant stakeholders.
Numbers and types of incidents, complaints and claims related to consent issues
Patient Safety Manager
Extractions from database – Patient Safety Report
Annually (with notable events included in quarterly Patient Safety Report to PSC)
Quality and Safety Committee (PSC)
Medical Director / Head of Medical Education / Directors of Service
Required changes to practice will be identified and actioned within a specific time frame. A lead person will be identified to take each change forward within their Directorate and report back to the Medical Director on effectiveness. Lessons will be shared with all the relevant stakeholders.

Consent to Examination or Treatment Policy – January 2020
Lewisham and Greenwich NHS Trust Page 29 of 41
12.0 References
DH Model Consent Policy and Key Documents - http://www.dh.gov.uk/en/Publichealth/Scientificdevelopmentgeneticsandbioethics/Consent/Consentgeneralinformation/index.htm
Mental Capacity Act 2005 and Code of Practice - http://www.dca.gov.uk/legal-policy/mental-capacity/
Office of the Public Guardian – key documents and forms including Lasting Power of Attorney - http://www.publicguardian.gov.uk/ Reference Guide to consent for examination and treatment (2nd edition July 2009) The Children’s Act 1989 The Adoption and Children Act 2002 Human Tissue Act 2004 Code of Practice – Consent (Human Tissue Authority) Making and Using Visual and Audio Recordings (General Medical Council) Working Together to Safeguard Children: a guide to inter-agency working to safeguard and promote the welfare of children. London: HM Government (2006).
13.0 Associated Documentation
How to Contact an IMCA – Trust intranet Safeguarding Adults at Risk, Policy and Procedure – Trust intranet Patient Information Policy – Trust intranet Therapeutic Restraint Policy (Restrictive Interventions) of Adults Under the Mental Capacity Act 2005 Deprivation of Liberty Safeguards (DOLS) and Procedure for DOLS Authorisation – Trust intranet
Mental Capacity Act – What you need to know
Lasting Power of Attorney
Assessing Capacity and Establishing Best Interests: Guidance for Staff
Mental Capacity Assessment Form

Lewisham and Greenwich NHS Trust Page 30 of 41
Appendix A - 12 key points on consent: the law in England When do health professionals need consent from patients? 1. Before you examine, treat or care for competent adult patients you must obtain their
consent. 2. Adults are always assumed to be competent unless demonstrated otherwise. If you
have doubts about their competence, the question to ask is: “can this patient understand and weigh up the information needed to make this decision?” Unexpected decisions do not prove the patient is incompetent, but may indicate a need for further information or explanation. Please note that the test required is set out in the Mental Capacity Act.
3. Patients may be competent to make some health care decisions, even if they are not
competent to make others. 4. Giving and obtaining consent is usually a process, not a one-off event. Patients can
change their minds and withdraw consent at any time. If there is any doubt, you should always check that the patient still consents to your caring for or treating them.
Can children and young people (16 and 17 year olds) give consent for themselves? 5. Before examining, treating or caring for a child, you must also seek consent. Young
people aged 16 and 17 are presumed to have the competence to give consent for themselves. Younger children who understand fully what is involved in the proposed procedure (‘Gillick’ competent) can also give consent (although their parents will ideally be involved). In other cases, someone with parental responsibility must give consent on the child’s behalf, unless they cannot be reached in an emergency. If a competent child consents to treatment, a parent cannot over-ride that consent.
Where a young person of 16 or 17 or a Gillick competent child under 16 refuses treatment, it is possible that such a refusal could be overruled if it would in all probability lead to the death of the child or to severe permanent injury. It would be prudent to obtain a court declaration or decision if faced with a competent child or young person who is refusing to consent to treatment, to determine whether it is lawful to treat the child.
Who is the right person to seek consent? 6. It is always best for the person actually treating the patient to seek the patient’s
consent. However, you may seek consent on behalf of colleagues if you are capable of performing the procedure in question.
What information should be provided? 7. Patients need sufficient information before they can decide whether to give their
consent: for example information about the benefits and risks of the proposed treatment, any alternative treatments, and the benefits and risks of those. If the patient is not offered as much information as they reasonably need to make their decision, and in a form they can understand, their consent may not be valid.
8. Consent must be given voluntarily: not under any form of duress or undue influence
from health professionals, family or friends.

Lewisham and Greenwich NHS Trust Page 31 of 41
Does it matter how the patient gives consent? 9. No: consent can be written, oral or non-verbal. A signature on a consent form does
not itself prove the consent is valid – the point of the form is to record the patient’s decision, and also increasingly the discussions that have taken place. Your Trust or organisation may have a policy setting out when you need to obtain written consent.
Refusal of treatment 10. Competent adult patients are entitled to refuse treatment, even when the treatment
would clearly benefit their health. The only exception to this rule is where the treatment is for a mental disorder and the patient is detained under the Mental Health Act 1983. A competent pregnant woman may refuse any treatment, even if this would be detrimental to the foetus.
Adults who are not competent to give consent 11. No-one can give consent on behalf of an adult who lacks capacity unless they have
been given the authority to do so under a valid and applicable Lasting Power of Attorney or as a court appointed deputy. However, you may still treat such a patient if the treatment would be in their best interests. ‘Best interests’ go wider than best medical interests, to include factors such as the wishes and beliefs of the patient when competent, their current wishes, their general well-being and their spiritual and religious welfare. People close to the patient may be able to give you information on some of these factors. Where the patient has never been competent, relatives, carers and friends may be best placed to advise on the patient’s needs and preferences.
12. If a patient who lacks capacity to consent has clearly indicated in the past, whilst
having capacity, that they would refuse treatment in certain circumstances (an ‘advance decision to refuse treatment’), and those circumstances arise, you must abide by that refusal. An advance decision to refuse treatment does not have to be in any particular format unless it is refusing life-sustaining treatment; in which case it must be in writing, signed by the patient (or on their direction) and witnessed (see the Mental Capacity Act for more information).
This summary cannot cover all situations. For more detail, consult the Reference guide to consent for examination or treatment, available at www.dh.gov.uk/consent.

Lewisham and Greenwich NHS Trust Page 32 of 41
Appendix B - Obtaining an IMCA (Independent Mental Capacity Advocate) for an inpatient Current supplier to LGT For Greenwich and Bexley patients is: Advocacy for All Tel: 0345 310 1812 Email: [email protected] Postal address: The Civic Centre, St. Mary’s Road, Swanley, BR8 7BU Website: www.advocacyforall.org.uk – to download a referral form Current supplier to LGT for Lewisham Patients is: POHWER Telephone number: 0300 456 2370 Email: [email protected] Website: www.pohwer.net/make-a-referral to download a referral form Further information on Trust intranet – put ‘IMCA’ into search box

Lewisham and Greenwich NHS Trust Page 33 of 41
Appendix C – Trust’s Consent Forms The Trust has transferred to electronic patient record (EPR) but consent forms remain on paper and will do for the foreseeable future. It is important to ensure that you are using the correct consent form and there are 5 to choose from: Consent Form 1 – White Patient’s agreement to investigation or treatment; adults and competent children Consent Form 2 – Blue Parental (or person who has parental responsibility) Agreement to investigation or treatment for a child or young person (For procedure where consciousness will be impaired by anaesthetic) Consent Form 3 – Light Blue Patient / Parental Agreement to investigation (procedures where consciousness not impaired) Consent Form 4 – Green Form for Adults (18 years old and above) who are unable to consent to investigation or treatment. All section to be completed by health profession proposing the procedure Consent Form 5 – Pink For medical treatment of a patient who refuses to have a blood transfusion Including Jehovah’s Witness patients Procedure specific consent forms may be developed using these templates where required, and used once they have been reviewed by the Head of Patient Safety.

Lewisham and Greenwich NHS Trust Page 34 of 41
Appendix D - Useful contact details Urgent Out Of Hours Advice Clinical Site Managers – will contact the Director on Call who has access to a 24 hour legal help line. General queries around consent issues / training on consent: Head of Legal Services – via switchboard or UHL 8836 / QEH 5996 Head of Patient Safety – via switchboard or UHL 3084 / QEH 5999 Head of Medical Education – via switchboard Leads for associated policies and procedures: Head of Design and Photography – clinical photography – via switchboard Caldicott Guardian – information governance issues – via switchboard

Lewisham and Greenwich NHS Trust Page 35 of 41
Appendix E – How to seek a declaration about consent issues from the Court of Protection This process can be lengthy and time consuming, however it is rarely necessary. 1 Adults Most adult patients have capacity to decide whether or not they agree to a procedure and their decision must be respected. For many patients who: a) Do not currently have capacity to consent, and b) Will not regain capacity within the timescale within which the lifesaving treatment (or
treatment to avoid irreversible deterioration) is required, and c) Who have not made any valid and applicable advance decision or Lasting Power of
Attorney to which the proposed treatment is subject d) And where there is no Court Appointed Deputy It is lawful to give treatment that is in the patient’s best interest without any declaration from the Court. However, there are occasionally circumstances in which a declaration from the Court is required. These include, but are not limited to, any procedure for a patient who does not have the capacity to consent which:
i. involves transplantation ii. affects the patient’s fertility iii. may or may not be the subject of an advance decision (i.e.: there is doubt whether it
applies to the current circumstances) iv. involves the withdrawal of artificial nutrition and hydration from a patient in PVS v. there are doubts/a dispute about whether or not it is in the patient’s best interests
2 Children and Young People (16 – 17 year olds) A Court declaration might be required if there is a conflict between a person with parental responsibility and a child under 16 years old on whether or not a procedure should be carried out, if the consultant were minded to proceed in such circumstances. A declaration might also be required if the parents of a non-competent minor refuse treatment which is believed to be in the child’s best interests. The Court should always be consulted where there is a refusal of life sustaining treatment or where the refusal could result in severe long term harm in a Gillick competent child or young person (16 – 17 years old). 3 Whom to contact Please contact the Head of Legal Services as soon as the possibility that a Court declaration may be needed is identified. Out of hours contact the Clinical Site Manager via switchboard, who will be able to enable contact with the Trust’s legal advisors via the Executive on call. 4 Information Required You will need the following information before any hearing: a) Patient name and full identification details, age, gender, ward

Lewisham and Greenwich NHS Trust Page 36 of 41
b) Details of the steps that have been taken to establish whether or not the patient has capacity – when done, by whom and is the incapacity likely to fluctuate or remain permanently? (Before approaching the Court it is usually necessary to have the patient assessed by a suitable psychiatrist to confirm whether or not the patient has the capacity to give or refuse consent)
c) Reasons for seeking the declaration from the Court – i.e.: reasons for the proposed
treatment, including why it is considered to be in the patient’s best interests to proceed
d) Risks involved in proceeding (or not proceeding) with the proposed treatment e) Whether any alternative treatment exists f) Reasons, if these can be ascertained, why the patient or parent is refusing treatment
recommended by the medical staff g) If a child – who has parental responsibility and what efforts have been made to
contact them h) In some circumstances the patient may require a solicitor or guardian ad litem
– it is helpful if the doctor is able to ascertain (e.g.: from family members if the patient is not able to provide such information) whether the patient already has a solicitor. Alternatively the Head of Legal Services will contact the Trust’s solicitors for assistance
i) Consultant in charge of the care j) Treating doctor / contact numbers
The Court of Appeal guidelines do recognise that ‘there may be occasions where the situation may be so urgent and the consequences so desperate that it is impracticable to attempt to comply with these guidelines. Where delay itself may cause serious damage to the patient’s health or put their life at risk then formulaic compliance with these guidelines would be inappropriate’.

Lewisham and Greenwich NHS Trust Page 37 of 41
Appendix F - Seeking consent: remembering the patient’s perspective

Lewisham and Greenwich NHS Trust Page 38 of 41
Appendix G – Audit of Consent Forms (and clinical notes) Tool and methodology Consent forms 1, 2, 3, 4 & 5 Methodology: use the checklist below to examine consent form and case notes of 100 patients who have undergone procedures requiring a general or regional anaesthetic in month / year. Select from a range of specialties e.g.: General surgery 20 ENT 20 Orthopaedics 20 Gynaecology 10 Maternity 10 Children’s Surgery 20

Lewisham and Greenwich NHS Trust Page 39 of 41
Consent Form Audit Proforma for Forms 1, 2, 3 and 5
YES NO N/A
1 Is the patient’s NHS number present on the form?
2 Is the consent form present in the patient’s notes?
3 Date of Birth
4 Specialty
5 Is name of procedure recorded? Not legible
6 Are any intended benefits recorded? Not legible
7 Are any significant, unavoidable or frequently occurring risks recorded?
Not legible
8 Are any extra procedures which may become necessary during the procedure recorded?
9 Are any leaflets / tapes provided recorded?
10 If yes - is there evidence that written (or other media) information was given prior to the date of surgery ? (e.g.: in outpatients / pre admissions / sent with apt. letter)
11 Is the Patient Information leaflet (etc.) registered on the PALS database?
12 If yes – is the title / Trust ref no documented?
13 Where no – is ‘No Leaflet’ circled?
14 Is there evidence that the patient raised any concerns about the proposed procedure?
15 Is the patient’s first language English?
16 If no – is there evidence that information was provided in a format that the patient could understand? (e.g.: use of interpreter)
17 Is the type of anaesthetic used recorded?
18 Is the consent form signed (by a registered health care practitioner)?
19 Date form signed by registered health care practitioner
20 Job title /Grade of clinician recorded (FY1 / FY2 / Spr / ST1 / ST2 / ST3 / Consultant / other
21 Are contact details provided?
22 Date procedure performed Date:
23 Is there evidence that the patient / parent was offered a copy of the consent form?
Copy accepted by patient circled?
24 Has the patient listed any procedures they did not wish to be carried out without further discussion?
25 Has the patient signed the consent form?
26 Has a witness signed the consent form?
27 Is the ‘Confirmation of Consent’ signed?
28 Designation of person signing confirmation
29 Is there evidence of an Advance Decision / Directive?
30 Is there evidence that the patient withdrew consent?
31 If yes – is there a signature supporting this?
Comments:

Lewisham and Greenwich NHS Trust Page 40 of 41
Consent Audit Proforma for when Consent Form 4 was used
Ref Circle
Comments
1 Is the patient’s full name recorded
YES / NO
2 Is the patient’s date of birth recorded
YES / NO
3 Is the patient’s NHS number recorded
YES / NO
4 Is the name of the Responsible Healthcare Professional recorded
YES / NO
5 Is the HCP’s designation recorded
YES / NO
6 Are any special requirements recorded
YES / NO
7 If yes – describe
8 Are details of the procedure or course of treatment proposed recorded?
YES / NO
9 Has an assessment of the patient’s capacity been recorded appropriately
YES / NO
10 Are further details recorded
YES / NO
11 Has the doctor indicated why they believe the procedure to be in the patient’s best interests?
YES / NO
12 Is there documented evidence of involvement of a person close to the patient? (either documented or telephone discussion)
YES / NO
13 If no – is there evidence of involvement of an IMCA?
YES / NO
14 Is there evidence of discussion about whether the patient has previously made any valid and applicable Advance Decision?
YES / NO
15 Is there evidence of a discussion about whether there is someone with a Lasting Power of Attorney for this patient, or whether there is a court appointed deputy?
YES / NO
16 Is the form signed by a Health Care Professional?
YES / NO
17 HCP 1 designation
18 HCP 2 designation (if any)
19 Comments
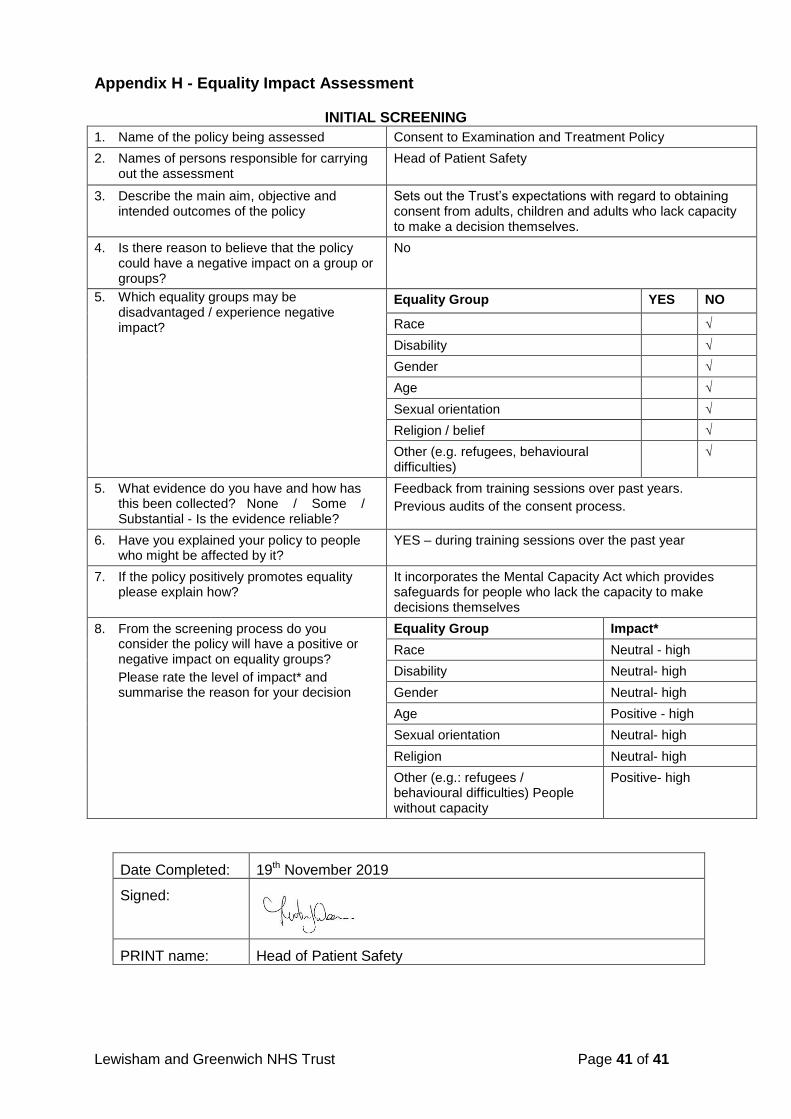
Lewisham and Greenwich NHS Trust Page 41 of 41
Appendix H - Equality Impact Assessment
INITIAL SCREENING
1. Name of the policy being assessed Consent to Examination and Treatment Policy
2. Names of persons responsible for carrying out the assessment
Head of Patient Safety
3. Describe the main aim, objective and intended outcomes of the policy
Sets out the Trust’s expectations with regard to obtaining consent from adults, children and adults who lack capacity to make a decision themselves.
4. Is there reason to believe that the policy could have a negative impact on a group or groups?
No
5. Which equality groups may be disadvantaged / experience negative impact?
Equality Group YES NO
Race √
Disability √
Gender √
Age √
Sexual orientation √
Religion / belief √
Other (e.g. refugees, behavioural difficulties)
√
5. What evidence do you have and how has this been collected? None / Some / Substantial - Is the evidence reliable?
Feedback from training sessions over past years.
Previous audits of the consent process.
6. Have you explained your policy to people who might be affected by it?
YES – during training sessions over the past year
7. If the policy positively promotes equality please explain how?
It incorporates the Mental Capacity Act which provides safeguards for people who lack the capacity to make decisions themselves
8. From the screening process do you consider the policy will have a positive or negative impact on equality groups?
Please rate the level of impact* and summarise the reason for your decision
Equality Group Impact*
Race Neutral - high
Disability Neutral- high
Gender Neutral- high
Age Positive - high
Sexual orientation Neutral- high
Religion Neutral- high
Other (e.g.: refugees / behavioural difficulties) People without capacity
Positive- high
Date Completed: 19th November 2019
Signed:
PRINT name: Head of Patient Safety