conservative vs conventional oxygen therapy on mortality...
TRANSCRIPT

Conservative vs Conventional oxygen therapy on mortality among patients
in an intensive care unit: The Oxygen-ICU trial
slides and [email protected]

POTENTIAL CONFLICT OF INTEREST
Unrestricted grants, lectures, advisory
boards, etc.
Astra Zeneca
Baxter
Biotest
Eli-Lilly
CSL-Behring
Kedrion
MSD
Novartis
NovoNordisk
Orion Pharma
Pfizer
Thermofisher
I trust in PHYSIOLOGY & EBM,
but the latter is more ‘voluble’, particularly in these days
Disclosures

MILD HYPOXIA
PaO2 50-60 mmHg
Mild Hypoxia for reducing
the harmful effects of
reactive oxygen species
HYPEROXIA
PaO2 >100 mmHg
High level of PaO2 for
avoiding tissue hypoxia
Which is the appropriate level of Arterial PO2 in critically ill patients ?
STRICT NORMOXIA
PaO2 60-100 mmHg

O2 therapy in critically ill patients:Which evidence ?
→ Oxygen is a ‘drug’ essential for human life; tissue hypoxia(uncertain the level) cause organ dysfunction
→ Oxygen is the most widely prescribed therapy in critically illpatients to prevent and/or correct hypoxemia
→ The use of supplemental oxygen therapy is recommended innumerous clinical practice guidelines but specific limits forthe PaO2 (or SaO2) maximum levels are not provided
→ ICU patients spend substantial periods in hyperoxemia thatis rarely corrected (de Graff et al, Intensive Care Med 2011; Suzuki et al,
J Crit Care 2013)
→ Mild hyperoxemia is considered safe and useful since it mayprovide a safety buffer

Hyperoxemia: Possible Effects in Critically ill Patients
BENEFICIAL- Prevention of tissue hypoxia- Vasoconstriction- Reduction of inflammation
Depend on- duration and dose of O2 exposure (lung and blood) ,- concomitant conditions (ARDS, endothelial dysfunction, bacteremia),
other
DETRIMENTAL- Pulmonary effects (hyperoxia)- Impairment of microcirculation- Immune-paralysis

HYPEROXEMIA: IS IT SAFE ?
→ Observational or interventional studies: hyperoxemia (defined as supranormal arterial O2 tension) and mortality in adult ICU patients
→ 17 studies (2008-2014)• mechanically ventilated ICU (k=4 studies, n=189,143 ), • post-cardiac arrest (k=6, n=19,144), • stroke (k=2, n=5,537), • traumatic brain injury (k=5, n=7,488).
O2 therapy in critically ill patients:Which evidence ?

HYPEROXEMIA: IS IT SAFE ?
Heterogeneity: 91.85, p<0.001; I2 = 96.73
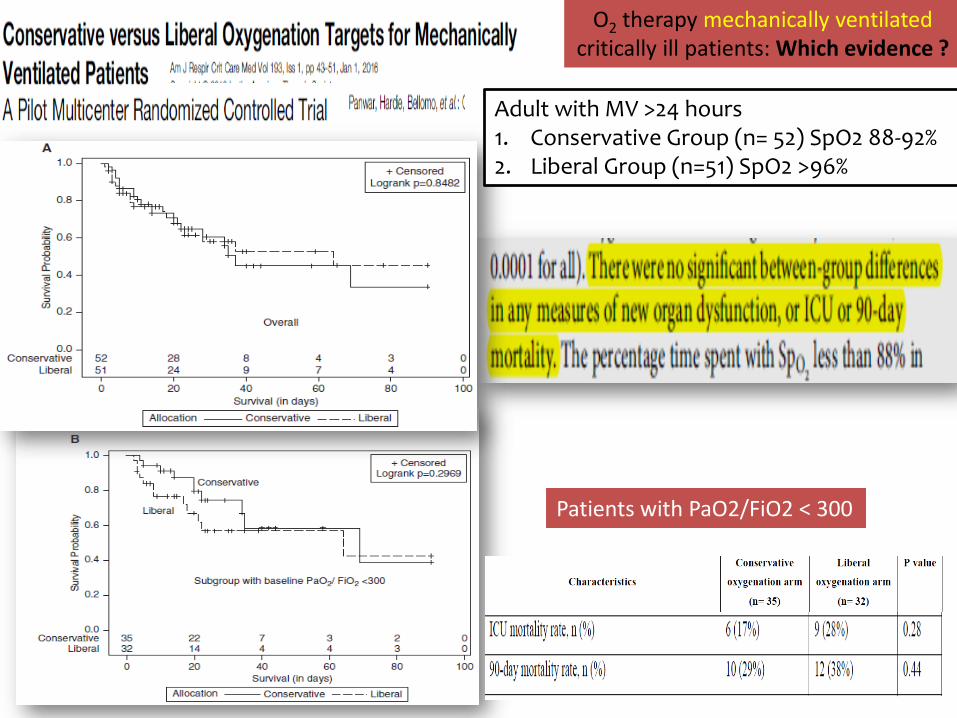
O2 therapy mechanically ventilatedcritically ill patients: Which evidence ?
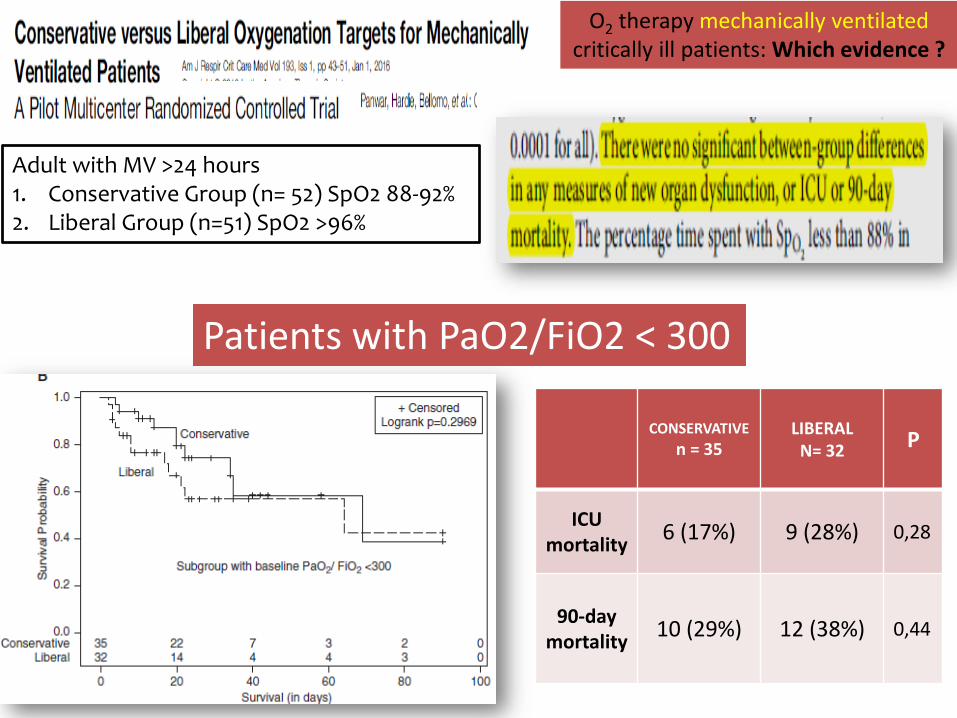
Patients with PaO2/FiO2 < 300
Adult with MV >24 hours1. Conservative Group (n= 52) SpO2 88-92%2. Liberal Group (n=51) SpO2 >96%
O2 therapy mechanically ventilatedcritically ill patients: Which evidence ?
CONSERVATIVE
n = 35LIBERAL
N= 32P
ICU mortality
6 (17%) 9 (28%) 0,28
90-day mortality
10 (29%) 12 (38%) 0,44

jamanetwork.com
Available at jama.com and on The JAMA Network Reader at mobile.jamanetwork.com
Girardis and coauthors
Effect of Conservative vs
Conventional Oxygen Therapy on
Mortality Among Patients in an
Intensive Care Unit: The Oxygen-
ICU Randomized Clinical Trial
Published online October 5, 2016

Oxygen-ICU trial ClinicalTrials.gov: NCT01319643
DESIGN: Single-centre, prospective, open-label, randomized controlled trialperformed in the 12 beds medical-surgical ICU of the Modena University Hospital(800 beds) from March 2010 to October 2012
PATIENTS: aged 18 years of age or older admitted to our ICU with an expected lengthof stay ≥72 hours.Exclusion criteria: pregnancy, ICU re-admission, acute decompensation of chronic pulmonarydisease, acute respiratory distress syndrome with an PaO2/FiO2 ratio <150, a decision towithhold life-sustaining treatment, immunosuppression and/or neutropenia, and enrolment inanother study.
OBJECTIVE: To evaluate whether the application of aconservative protocol for O2 supplementation, in order tomaintain PaO2 within physiological limits, could improveoutcomes in critically ill ICU patients.
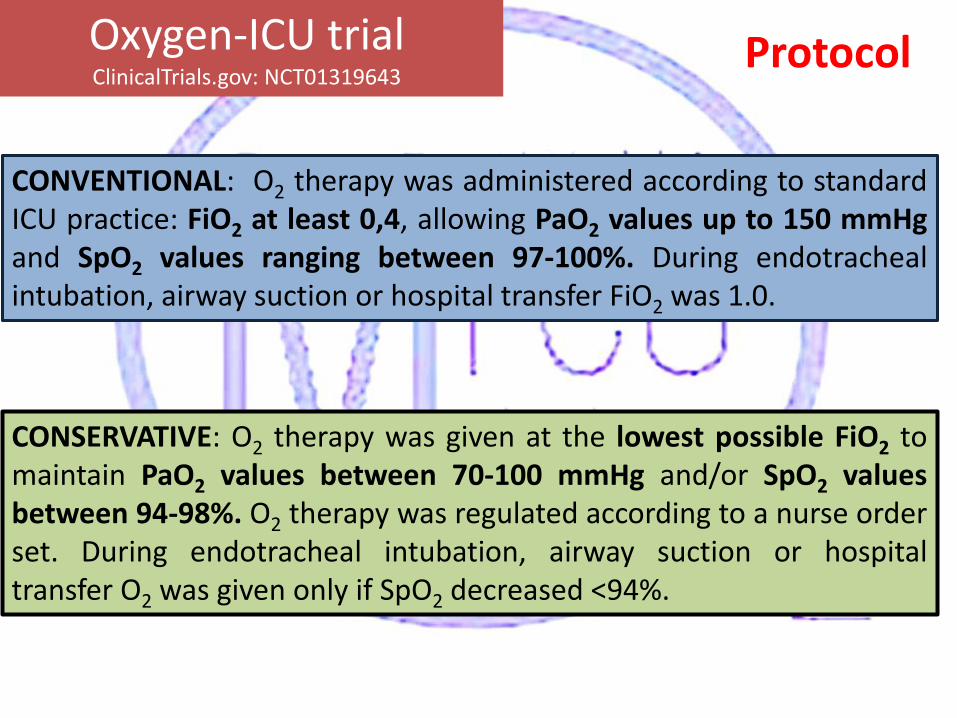
CONVENTIONAL: O2 therapy was administered according to standardICU practice: FiO2 at least 0,4, allowing PaO2 values up to 150 mmHgand SpO2 values ranging between 97-100%. During endotrachealintubation, airway suction or hospital transfer FiO2 was 1.0.
CONSERVATIVE: O2 therapy was given at the lowest possible FiO2 tomaintain PaO2 values between 70-100 mmHg and/or SpO2 valuesbetween 94-98%. O2 therapy was regulated according to a nurse orderset. During endotracheal intubation, airway suction or hospitaltransfer O2 was given only if SpO2 decreased <94%.
ProtocolOxygen-ICU trial ClinicalTrials.gov: NCT01319643

OUTCOMEPRIMARY OUTCOME: ICU mortalitySECONDARY OUTCOMES:– Hospital mortality– New respiratory, cardiovascular, liver and renal failure (SOFA score ≥3) (≥48 hours
after admission)– re-operation in surgical patients ( ≥48 hours after admission)– bloodstream, respiratory and surgical site infections ( ≥48 hours after admission)
POWER SIZE and ANALYSIS– Data from our institution showed an ICU mortality of 23% in patients staying >72 hours. – 660 patients over a 24 months in order to have the capacity to detect an absolute difference
in mortality of 6% (RRR 25%) between the 2 different groups (two-sided alpha level 0.05, power 80%).
– Due to low inclusion rate, we stopped the study after 32 months (480 patients randomized) as indicated by our EC/statistical review after an interim analysis (not defined at priori).
– A modified intent-to-treat (MITT) population, consisting of all randomized patients with an ICU length of stay ≥72 hours and with at least 1 ABG per day, was the primary population for analysis.
Oxygen-ICU trial ClinicalTrials.gov: NCT01319643

From 1st March 2010 to 30th October 2012
Results
Consort diagram
Oxygen-ICU trial ClinicalTrials.gov: NCT01319643

Conservative
O2 therapy
N = 216
Conventional
O2 therapy
N = 218
Female, no. (%) 95 (44,0) 93 (42,7)
Age, median (IQR) 63 (51-74) 65 (52-76)
Type of ICU admission, no.(%)
Medical 77 (35,7) 86 (39,5)
Surgical 139 (64,3) 132 (60,7)
SAPS II, median (IQR) 37 (26-49) 39 (28-55)
Respiratory Failure, no.(%) 121 (56,0) 129 (59,2)
Mechanical Ventilation, no.(%) 143 (66,2) 148 (67,9)
Shock , no.(%) 68 (31,4) 72 (33,0)
Liver Failure , no.(%) 40 (18,5) 45 (20,6)
Renal Failure, no.(%) 32 (14,8) 35 (16,1)
Documented Infections, no.(%) 81 (37,5) 88 (40,4)
Characteristics of the patients at study inclusion
ResultsOxygen-ICU trial ClinicalTrials.gov: NCT01319643

O2 control
Results
P<0.001
Time-weighted PaO2 average during ICU stay
Median PaO2
102 mmHg [IQR 88-116]
P<0.001
Time-weighted FiO2 average during ICU stay
Median FiO2
0,39 [IQR 0,35-0,42]
Median PaO2
87 mmHg [IQR 79-97]
Median FiO2
0.36 [IQR 0,30-0,40]
Oxygen-ICU trial ClinicalTrials.gov: NCT01319643
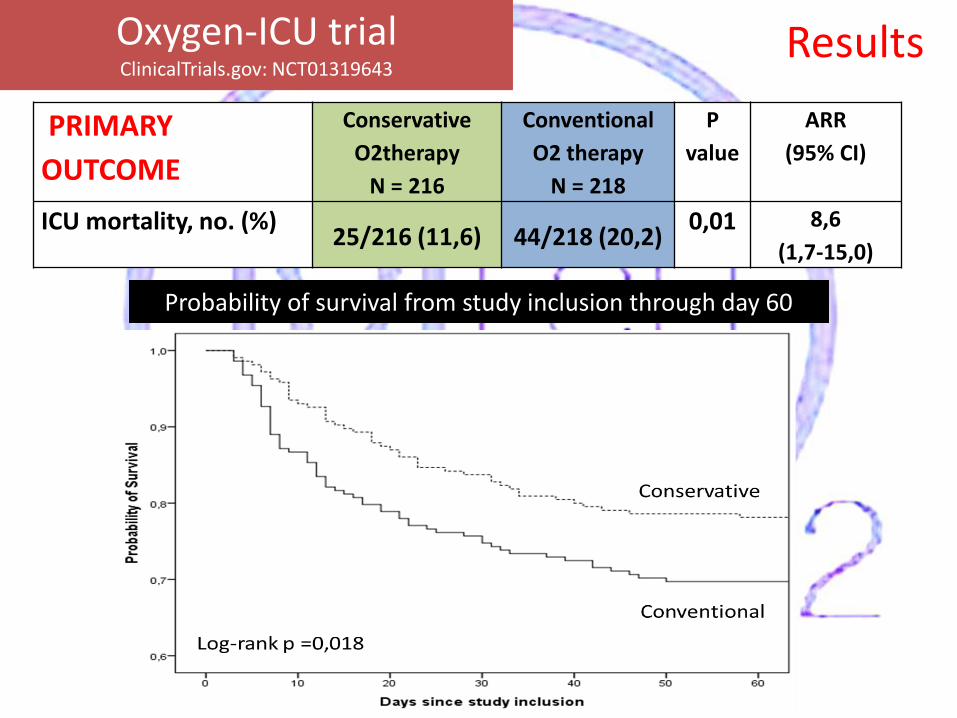
Probability of survival from study inclusion through day 60
Results
PRIMARY
OUTCOME
Conservative
O2therapy
N = 216
Conventional
O2 therapy
N = 218
P
value
ARR
(95% CI)
ICU mortality, no. (%)25/216 (11,6) 44/218 (20,2)
0,01 8,6
(1,7-15,0)
Oxygen-ICU trial ClinicalTrials.gov: NCT01319643

Results
New organ dysfunctionduring ICU stay * *
* p< 0,01
New documented infectionduring ICU stay
*
* p< 0,05
Oxygen-ICU trial ClinicalTrials.gov: NCT01319643

Oxygen-ICU trial ClinicalTrials.gov: NCT01319643
Results
Hypothesis Effects of the high O2 concentration (in the lung and in the blood) on the innate immune system and host inflammatory response
→ High blood level of reactive oxygen species and IL 6, IL 10 duringperitoneal infection (Rodriguez-Gonzalez R et al Shock 2014).
→ Structural and functional changes of the alevolar macrophageswith impairment of antimicrobial activity and dissemination ofinfection (Baleeiro et al, Journal of immunology 2003; Morrow et al, Free radical
biology & medicine 2007)
→ Liver dysfunction due to the high immune-mediate oxidativeburst after Ischemia/reperfusion model (Zangl Q et al, Anesthesiology
2014)
Oxygen-ICU trial ClinicalTrials.gov: NCT01319643

Limitations of the study → Design: single-center, open-label. sample-size limited for subgroup
analysis (Stroke, TBI, AMI ?)
→ Unplanned early stop may have exaggerated the effect size
→ Time weighted median PaO2 is a rough approximation of true O2exposure in patients with only 1 or 2 ABG for day. EC did not allowto perform more arterial blood gas analysis to avoid influences onthe study results introduced by changes in in the standard of careand for patient safety reasons
→ Underestimation of the infection rate due to the use of onlydocumented infections
→ The high percentage of patients with respiratory failure at studyinclusion (58%) hinders a proper analysis on the possible protectiveeffects of the conservative O2 strategy on the respiratory function.
Oxygen-ICU trial ClinicalTrials.gov: NCT01319643

In critically ill patients with ICU length of stay > 72 Hours, aconservative oxygen strategy aimed to maintain SpO2/PaO2 levelswithin the physiological range→ Is safe
→ Resulted in lower ICU mortality as compared to a liberal oxygentherapy.
→ Due to limitations of the study (e.g. early termination)the results should be considered preliminary
Oxygen-ICU trial ClinicalTrials.gov: NCT01319643
Confirmatory trial is urgently needed
Conclusions

MILD HYPOXIA
PaO2 50-60 mmHg
Mild Hypoxia for reducing
the harmful effects of
reactive oxygen species
HYPEROXIA
PaO2 >100 mmHg
High level of PaO2 for
avoiding tissue hypoxia
Which is the appropriate level of Arterial PO2 in critically ill patients ?
STRICT NORMOXIA
PaO2 60-100 mmHg

RESEARCH STAFF
Massimo Girardis, MD
Stefano Busani, MD
Rinaldi Laura, MD
Andrea Marudi, MD
Marta Buoncristiano, MS
Oxygen-ICU trial
RESEARCH AND CLINICAL STAFF
REST MODE
IN ACTION

TAKE HOME PICTURE
O2 therapy mechanically ventilatedcritically ill patients: Which evidence ?
Patients with PaO2/FiO2 < 300
Adult with MV >24 hours1. Conservative Group (n= 52) SpO2 88-92%2. Liberal Group (n=51) SpO2 >96%
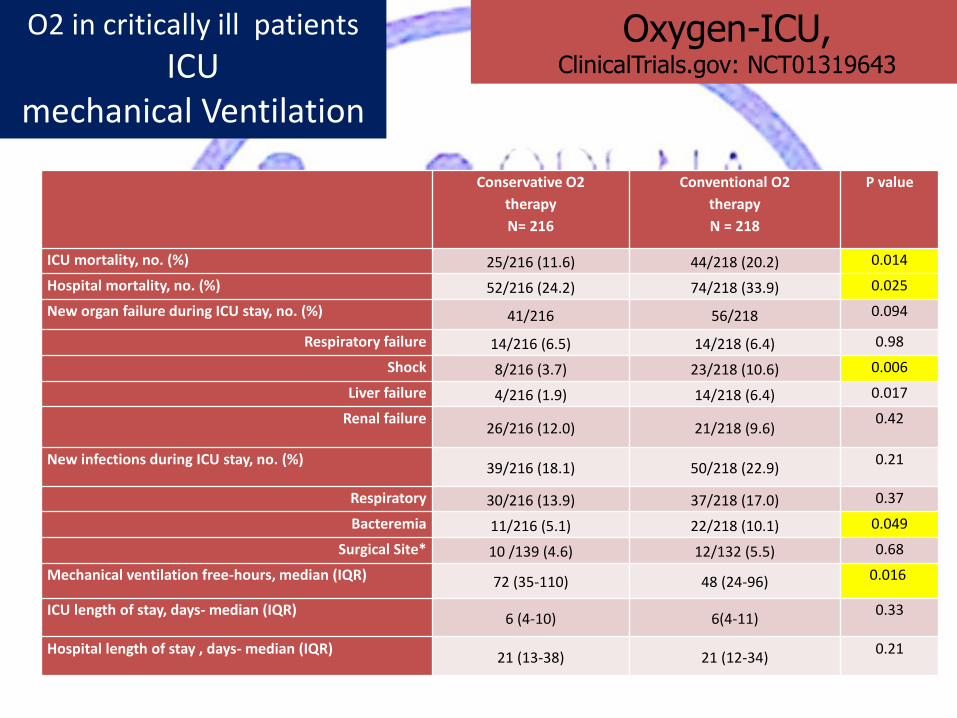
O2 in critically ill patients
ICU mechanical Ventilation
Oxygen-ICU, ClinicalTrials.gov: NCT01319643
Conservative O2
therapy
N= 216
Conventional O2
therapy
N = 218
P value
ICU mortality, no. (%) 25/216 (11.6) 44/218 (20.2) 0.014
Hospital mortality, no. (%) 52/216 (24.2) 74/218 (33.9) 0.025
New organ failure during ICU stay, no. (%) 41/216 56/218 0.094
Respiratory failure 14/216 (6.5) 14/218 (6.4) 0.98
Shock 8/216 (3.7) 23/218 (10.6) 0.006
Liver failure 4/216 (1.9) 14/218 (6.4) 0.017
Renal failure26/216 (12.0) 21/218 (9.6)
0.42
New infections during ICU stay, no. (%)39/216 (18.1) 50/218 (22.9)
0.21
Respiratory 30/216 (13.9) 37/218 (17.0) 0.37
Bacteremia 11/216 (5.1) 22/218 (10.1) 0.049
Surgical Site* 10 /139 (4.6) 12/132 (5.5) 0.68
Mechanical ventilation free-hours, median (IQR) 72 (35-110) 48 (24-96) 0.016
ICU length of stay, days- median (IQR)6 (4-10) 6(4-11)
0.33
Hospital length of stay , days- median (IQR)21 (13-38) 21 (12-34)
0.21

O2 in critically ill patients
ICU mechanical Ventilation
Oxygen-ICU, ClinicalTrials.gov: NCT01319643

O2 in critically ill patients
ACC
Hyperoxia. Heterogeneity = 12.4, p = 0.015; I2 = 67.73


O2 in critically ill patientsICU
mechanical Ventilation
HyperoxiaHeterogeneity: 91.85, p<0.001; I2 = 96.73
Study Design Country Comparator Outcome
de Jonge 2008 retrospective cohort, multi-center Netherlands PaO2 between 66-80 mmHgIn-hospital
mortality
Eastwood 2012 retrospective cohort, multi-centerAustralia, New
Zealand
PaO2 <120 mmHg for unadjusted
analysis; PaO2 75-85 mmHg for
adjusted analysis
In-hospital
mortality
Suzuki 2013 prospective observational cohort, single-
centerAustralia Non-exposed to hyperoxia
In-hospital
mortality
Suzuki 2014 prospective before-after, single-center AustraliaConservative period: SpO2 between
90-92%28-day mortality

O2 therapy mechanically ventilatedcritically ill patients: Which evidence ?
Adult with MV >24 hours1. Conservative Group (n= 52) SpO2 88-92%2. Liberal Group (n=51) SpO2 >96%

POTENTIAL CONFLICT OF INTEREST
Unrestricted grants, lectures, advisory
boards, etc.
Astra Zeneca
Baxter
Biotest
Eli-Lilly
CSL-Behring
Kedrion
MSD
Novartis
NovoNordisk
Orion Pharma
Pfizer
Thermofisher
I trust in Physiology & EBM,
but the latter is more ‘voluble’
Disclosures

MILD HYPOXIA
PaO2 50-60 mmHg
Mild Hypoxia for reducing
the harmful effects of
reactive oxygen species
HYPEROXIA
PaO2 >100 mmHg
High level of PaO2 for
avoiding tissue hypoxia
Which is the appropriate level of Arterial PO2 in critically ill patients ?
STRICT NORMOXIA
PaO2 60-100 mmHg