continuing education care of patien ts after · pdf file · 2013-12-15care of...
TRANSCRIPT

16 CRITICALCARENURSE Vol 24, No. 1, FEBRUARY 2004
Donna J. Mackenzie works in the surgical intensive care unit in the Veterans Affairs Puget Sound Health Care System, Seattle, Wash,where she has been a staff nurse for the past 6 years. She has a special interest in the care of patients after esophagectomy and has devel-oped a teaching module for the nurses in her unit.
Pamela K. Popplewell is the clinical staff coordinator for the surgical wards and the progressive care unit in the Veterans Affairs PugetSound Health Care System. Her expertise is nursing care of postoperative patients. She is in the final year of a nurse practitioner pathwayat Seattle Pacific University.
Kevin G. Billingsley is a staff surgeon in the Veterans Affairs Puget Sound Health Care System and an assistant professor in the depart-ment of surgery at the University of Washington School of Medicine. His clinical and research interests focus on the multidisciplinarytreatment of patients with gastrointestinal tumors.
With approx i m ately 12 0 0 0new cases diagnosed each year in theUnited States and a nearly equivalentnumber of deaths, esophageal cancerremains one of the most lethal of allmalignant diseases.1,2 The tumoroccurs more often in men than inwomen and more often in AfricanAmericans than in whites. The inci-dence of esophageal cancer incre a s e swith age.3,4
Squamous cell and adenocarci-noma are the 2 most common histo-pathologic forms of esophagealcancer. Squamous cell carcinoma
occurs more often in African Ameri-cans and Asians than in othergroups, and the incidence is higherin China, Japan, and Iran than inother countries.3 Squamous cell car-cinoma mainly occurs in the upperand middle parts of the esophagus.Adenocarcinoma arises mainly inthe distal part of the esophagus andat the gastroesophageal junction.Esophageal cancer may spread toother parts of the body via the bloodor lymphatic system. Distant metas-tases most often occur in the liverand lungs.3,5,6
CoverArticle
Authors
CE This article has been designated for CEc redit. A closed-book, multiple-choice examinat i o nf o l l ows this article, which tests your knowledge ofthe following ob j e c t i v e s :
1 . Identify the clinical findings associated with esophageal cancer
2 . Describe the postoperative complications of esophagectomy
3. Discuss important aspects of nursing care of p atients after esophagectomy
Donna J. Mackenzie, RN, BSN, CCRNPamela K. Popplewell, RN, MSN, CCRNKevin G. Billingsley, MD
To purchase reprints, contact The InnoVision Group, 101 Columbia, Aliso Viejo, CA 92656. Phone, (800) 809-2273 or (949) 362-2050 (ext 532); fax, (949) 362-2049; e-mail,[email protected].
CEContinuing Education
Care of Patien ts After Esophagectomy

EtiologyThe precise etiology of esophageal
cancer is not known. How e v e r, severa lrisk factors are associated with itso c c u r rence. He avy alcohol use inconjunction with cigarette smokingor chewing tobacco is a major riskfactor for squamous cell cancer. Ina reas of the world where esophagealcancer is endemic (eg, Iran, Ru s s i a ,Pu e rto Rico, Singapore, China, Japan,and parts of Africa), dietary factorsa re associated with increased risk ofesophageal cancer. In these countries,diets are high in nitrosamines, pick-led and fermented foods, and hotteas. Re s e a rchers speculate that thechronic mucosal inflammationcaused by drinking hot liquids andc re ated by re p e ated exposure to tox-ins increases the likelihood of malig-nant tra n s f o r m ation within cells ofthe esophageal mucosa.3, 5
Another possible etiologic factori n volved in the development ofesophageal cancer is chronic irritat i o nof the esophageal mucosa re l ated tog a s t roesophageal acid reflux. Barre t tesophagus develops in the distal partof the esophagus in a subset of pat i e n t swith chronic re f l u x .7 In this condition,the esophageal epithelial surface isa l t e red to become more like the stom-ach lining. This alteration, which i sdescribed as columnar metaplasia, isa s s o c i ated with a markedly incre a s e drisk of progression to adenocarci-noma. To detect changes within theesophagus before they pro g ress toc a n c e r, patients with known Barre t t
hoarseness, coughing, sialorrhea( e xcessive salivation), and nocturnala s p i rat i o n .5,6, 8, 9
PrognosisThe ov e rall prognosis for pat i e n t s
with locally advanced esophagealcancer is poor. The age of the pat i e n t ,the stage of cancer at diagnosis, andthe location of the tumor are all pre-dictors of surv i va l .10 For patients withdisease extending through the wallof the esophagus and or invo l v e m e n tof regional lymph nodes, 5-year sur-v i val is less than 15 % .1
Surgical ManagementSurgical resection is the mainstay
of tre atment for patients with local-ized esophageal cancer. How e v e r, inan effort to improve cure rates, chemo-t h e rapy and ra d i ation therapy areoften used in conjunction with sur-g e ry.11-14 We address the nursing careof patients who have surgical re s e c-tion of esophageal neoplasms andp atients who have prophylactic sur-g e ry for tre atment of Barrett e s o p h a-g u s with high-grade dysplasia.
Preoperative EvaluationPatients may undergo multiple
diagnostic tests in pre p a ration foresophageal surgery4 (Table 1). Thedefinitive diagnostic study forpatients suspected of having anesophageal tumor is flexible fibero p-tic esophagoscopy with biopsy. Aswell as indicating the presence ofdisease, a biopsy also can prov i d ei n f o r m ation about cell differe n t i at i o n .
In addition to a biopsy, manyp atients undergo computed tomog-ra p h y, positron emission tomogra-p h y, and endoscopic ultrasound todetermine local stage and inva s i v e-ness of the tumor and to survey for
e s o p h a g u s should undergo re g u l a re n doscopic examinations andesophageal biopsies.
Re c e n t l y, a genetic component ofesophageal cancer has been investi-g ated. Overe x p ression and mutat i o nof the gene that encodes the tumors u p p ressor protein p53 have beenfound in esophageal cancer. Thisgenetic link is one of the most com-monly studied links associated withcancer development.3 Other tumors u p p ressor genes may also be associ-ated with esophageal cancer.8
Clinical FindingsEarly-stage esophageal cancer is
ra rely associated with notable signsand symptoms; there f o re, early detec-tion is difficult.8 Dysphagia is themost common initial symptom butusually occurs in late-stage esophagealc a n c e r.3 The esophagus is very pliable;
t h e re f o re, tumors are usually quitea d vanced before a person perc e i v e sdifficulty with swallowing. By thetime patients go to a physician, theyoften have had dysphagia for severa lmonths. It may have started with theinability to swallow solid foods andthen pro g ressed eventually to liquids.They may have experienced signifi-cant weight loss, malnutrition, andw e a kness.3 In addition to dysphagia,p atients with esophageal tumorsm ay have pain with swallow i n g( o d y n o p h agia). Other late clinicalm a n i f e s t at i o n s of esophageal cancera re substernal pain, hiccups, re s p i ra-t o ry difficulty, heartburn, halitosis,
18 CRITICALCARENURSE Vol 24, No. 1, FEBRUARY 2004
Early-stage esophageal cancer is rarelyassociated with significant symptoms andtherefore early detection is difficult

any local lymph node metastasis.3
Regional lymph nodes include lymphnodes in the mediastinum and nodesa round the gastric cardia and alongthe left gastric art e ry. Distant lymphnodes include lymph nodes aro u n dthe celiac axis and re t ro p e r i t o n e u mand in the cervical (neck) chains.I n volvement of these distant nodesis considered distant metastatic dis-ease (stage IV), and aggressive sur-g ical treatment is generally notconsidered in patients with nodali n volvement in these areas. Distantmetastases may also involve the liver,lungs, peritoneum, or adrenal glands.For patients with distant metastat i cdisease, palliative chemothera p y,ra d i ation thera p y, or both are thep r i m a ry tre at m e n t s .2 Once esophagealcancer is detected, it may be stagedby using the TNM (tumor- n o d e -metastasis) classification system
(Table 2). In this system, tumors areclassified according to size, lymphnode involvement, and the pre s e n c eof metastases. The course of tre at m e n tand the prognosis of the diseasedepend on the stage at diagnosis.Su r g e ry for esophageal cancer maybe performed with either a curat i v eor palliative intent.16 See Table 3 forfactors that increase surgical risk.
Surgical TechniquesSurgical resection of the esopha-
gus for cancer is a technicallydemanding pro c e d u re. It usuallyi n volves re m oving part or all of theesophagus, part of the stomach,lymph nodes in the surro u n d i n ga rea, and occasionally the spleen (ifit is injured or bleeding). Most com-
m o n l y, the stomach is used to re c o n-s t ruct the gastrointestinal tract. Ifthe entire esophagus and stomachmust be re m oved, part of the bow e lis used to cre ate a tube to maintaing a s t rointestinal continuity. Themost common surgical pro c e d u re sfor esophageal cancer are tra n s h i at a l
CRITICALCARENURSE Vol 24, No. 1, FEBRUARY 2004 19
Table 1 Preoperative diagnosticstudies for esophageal surgery
Blood and urine testsChemistry panel Complete blood cell countSerum albumin levelLiver function testsUrinalysis
Radiological studiesChest radiographyBarium swallowComputed tomography of the
abdomen Computed tomography of the
mediastinumBone scanEsophageal ultrasound for depth
of invasionPositron emission tomography
Cardiac and pulmonary studiesPulmonary function testsElectrocardiography
Tissue typing and tumor identificationCytology of tumor brushings or
biopsy specimensCervical lymph node biopsyEndoscopy with biopsy or brushingsBronchoscopy and laryngoscopy for
cervical or thoracic esophageallesions
Table 2 TNM staging system for esophageal carcinoma15
Primary tumor (T)Tx Primary tumor cannot be assessedT0 No evidence of primary tumor (eg, after treatment with radiation and chemotherapy)Tis Carcinoma in situT1 Tumor invades lamina propria or submucosa but not beyond itT2 Tumor invades muscularis propriaT3 Tumor invades adventitiaT4 Tumor invades adjacent structures (eg, aorta, tracheo-bronchial tree,
vertebral bodies, pericardium
Regional lymph nodes (N)Nx Regional lymph nodes cannot be assessedN0 No regional lymph node metastasisN1 Regional node metastasis
Distant metastasis (M)Mx Presence of distant metastasis cannot be assessedM0 No distant metastasisM1 Distant metastasis
Stage groupingStage 0 Tis No MoStage 1 T1 No MoStage IIA T2 No M oStage IIB T1 N1 M o
T2 N1 M oStage III T3 N1 Mo
T4 Any N M oStage IV Any T Any N M 1
Used with the permission of the American Joint Committee on Cancer (AJCC), Chicago, Illinois. The origi-nal source for this material is the AJCC Cancer Staging Manual, Sixth Edition (2002) published bySpringer-Verlag New York, www.springer-ny.com.
Table 3 Factors that increase surgicalrisk in esophageal cancer17,18
Age >60 yearsChronic or recent illness, especially
pneumoniaObesity, smokingPoor nutritional statusExcessive alcohol consumptionUse of drugs such as antihypertensives,
muscle relaxants, tranquilizers, sleep inducers, insulin, sedatives, narcotics,b-adrenergic blockers, or cortisone

esophagectomy and transthora c i ce s o p h a g e c t o m y.
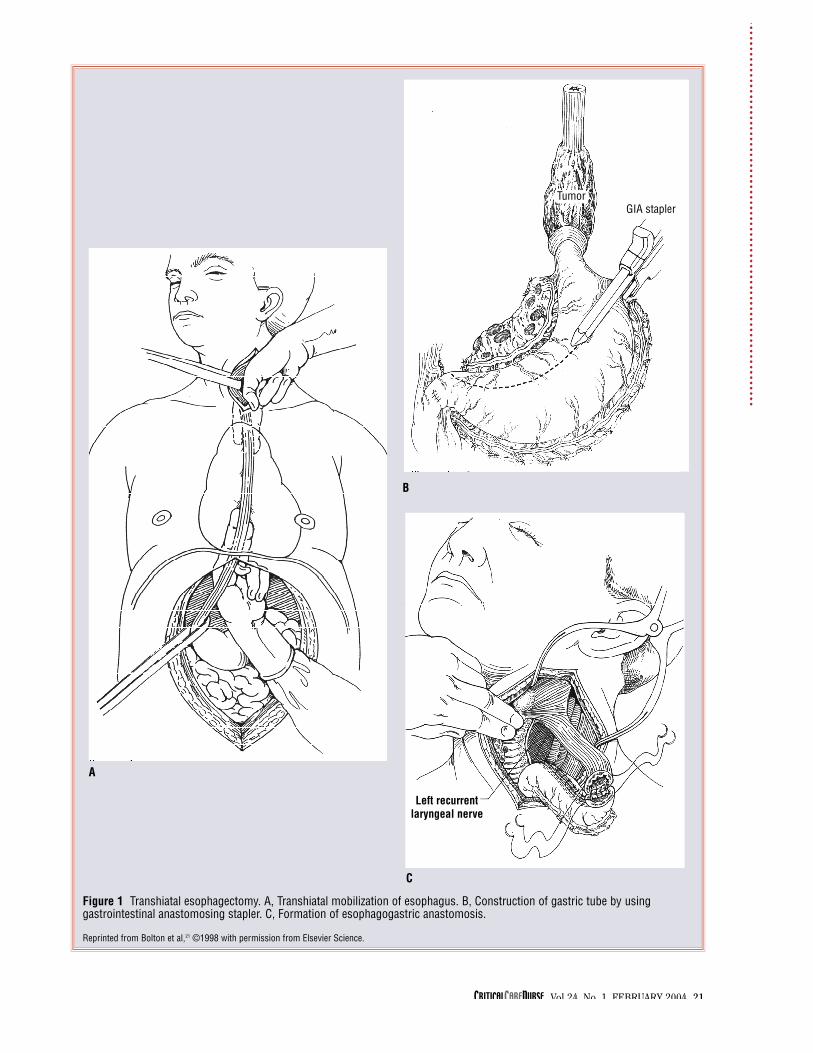
Tra n s h i atal esophagectomyi n volves both an abdominal incisionand a cervical (neck) incision. Thet h o racic cavity is not opened. Thea b dominal component of the pro c e-d u re involves complete mob i l i z at i o nof the stomach. Lymph nodes aro u n dthe distal part of the esophagus, thegastric cardia, and the left gastrica rt e ry are resected in continuity withthe specimen. The intrat h o racic partof the esophagus is then dissectedaw ay from adjacent thoracic stru c-t u res by using a blunt technique. Top e rform this maneuver, the surgeonopens the diaphra g m atic hiatus andm obilizes the esophagus by care f u lmanual dissection up into the tho-racic cav i t y.19
The cervical component of theo p e ration involves opening the neckand re t racting the sternocleido m a s-toid muscle lat e ra l l y. The part of theesophagus in the neck is encirc l e dand dissected aw ay from the adjacenttrachea. The esophagus is thendivided in the neck and passeddown t h rough the chest. The upperp a rt of the stomach is then divided,and the specimen, which includesthe esophagus and the upper part ofthe stomach, is sent to the pathologyl a b o rat o ry for examination. Gastro i n-testinal continuity is re e s t a b l i s h e dby constructing a tube out of theremaining part of the stomach andpassing the tube up through the chestand anastomosing the cervical partof the esophagus to the stomacht u b e2 0,21 ( Fi g u re 1).
Tra n s t h o racic esophagectomyi n volves an abdominal incision anda thora c o t o m y. The mid and low e rp a rts of the esophagus are re m ov e dalong with the upper part of the
in 1 second of less than 65% are atg re atest risk for postoperative pul-m o n a ry failure .17 Additional risk fac-tors for pulmonary complicat i o n sinclude the pat i e n t ’s age and per-formance stat u s .2 3 For patients withpoor pre o p e rative lung function, aperiod of pre o p e rative card i o p u l-m o n a ry re h a b i l i t ation should bec o n s i d e re d .2 3
If the surgery is done to tre atc a n c e r, nearby lymph nodes also arere m oved. Each operative appro a c hhas strengths and weaknesses. Thet ra n s h i atal esophagectomy spare sp atients a thoracotomy incision, thusdiminishing postoperative pain andp u l m o n a ry complicat i o n s .16 In addi-tion, the tra n s h i atal esophagectomyplaces the esophageal anastomosishigh in the neck. If the anastomosisleaks in this position, the leak is easilymanaged by opening the neck incisionfor drainage. Doing so ra re l y re s u l t sin systemic sepsis or mort a l i t y. T h et ra n s h i atal approach, how e v e r, do e snot allow complete dissection of intra-thoracic lymph nodes and thus maylimit the surgeon’s ability to removeall disease-bearing lymph nodes.
In contrast, tra n s t h o ra c i cesophagectomy involves a thora c o-tomy incision and re q u i res placementof the anastomosis in the chest. If theanastomosis leaks in the chest, medi-astinitis, which may be life thre at e n-ing, often develops. The clearadvantage of the tra n s t h o racic pro-c e d u re is that the surgeon can dissectthe intrat h o racic part of the esopha-gus and the regional mediastinalnodes under direct vision via thet h o racotomy incision. Doing so pro-vides a theoretical advantage in dis-ease control. Results of a recent clinicaltrial suggest that the tra n s t h o ra c i cp ro c e d u re may have a small adva n-
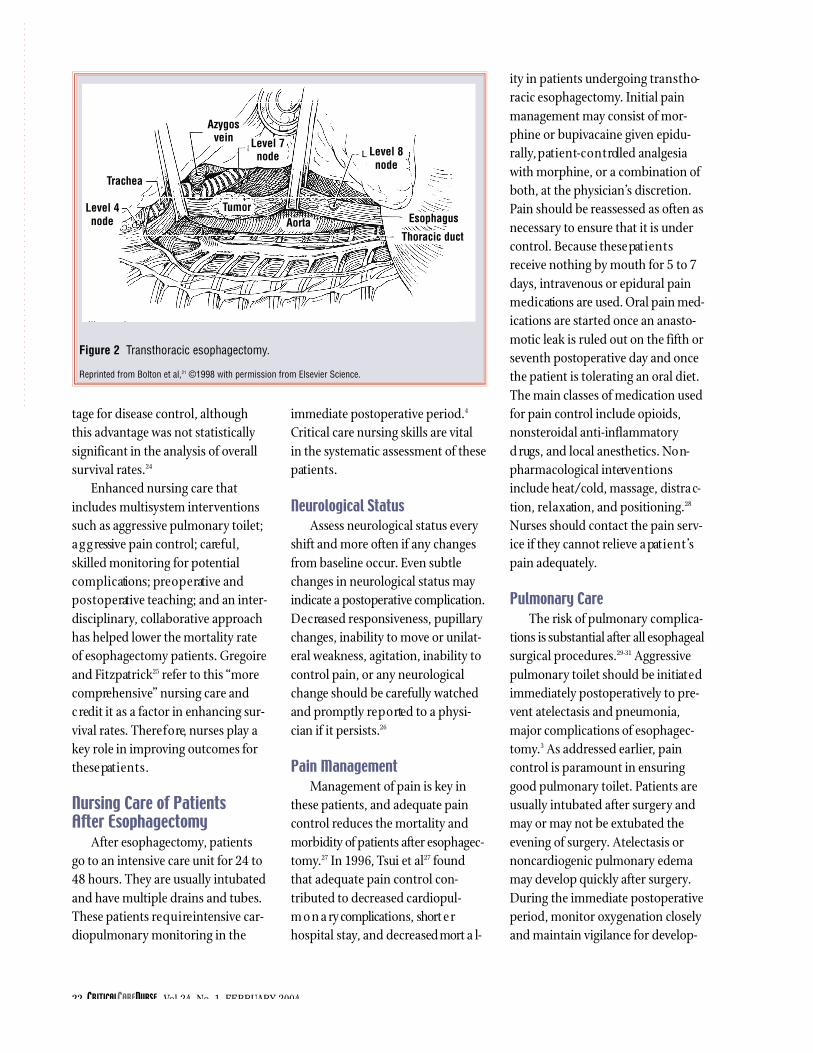
stomach. The abdominal componentof the pro c e d u re involves completem ob i l i z ation of the stomach. Thelymph nodes associated with the dis-tal part of the esophagus, the gastricc a rdia, and the left gastric art e ry areresected in continuity with the speci-men. When the stomach and the dis-tal part of the esophagus arecompletely dissected, the abdo m i-nal incision is closed and the pat i e n tis repositioned for a right thora c o-t o m y.2 2 Once the chest is opened, thei n t rat h o racic part of the esophagusis dissected, and specimens of lymphnodes associated with the para-esophageal space and the subcarinala rea are obtained for pat h o l o g i c a lexamination. The esophagus isdivided in the chest. The upper partof the stomach is also divided, andthe specimen, which includes theesophagus and the upper part of thestomach, is sent for pat h o l o g i c a le x a m i n ation. In order to re s t o re theg a s t rointestinal tract, the stomach isre c o n f i g u red, and a gastric tube isc re ated and passed into the chest.The stomach is anastomosed to theesophagus in the chest cav i t y. Pat i e n t swho have tra n s t h o racic esophagec-tomy have no neck incision and hav eone or more chest tubes postopera-t i v e l y21 ( Fi g u re 2).
The choice of operation dependson the location of the tumor, thep at i e n t ’s pulmonary function, and thes u r g e o n ’s experience and pre f e re n c e .
S e v e ral investigators have stud-ied the pre o p e rative factors that canbe used to predict postoperative pul-m o n a ry complications. One of themost consistent predictors of pul-m o n a ry complications is compro-mised pre o p e rative lung function asi n d i c ated by spiro m e t ry.2 3 Pat i e n t swho have a forced expirat o ry vo l u m e
20 CRITICALCARENURSE Vol 24, No. 1, FEBRUARY 2004
CRITICALCARENURSE Vol 24, No. 1, FEBRUARY 2004 21
Figure 1 Transhiatal esophagectomy. A, Transhiatal mobilization of esophagus. B, Construction of gastric tube by using gastrointestinal anastomosing stapler. C, Formation of esophagogastric anastomosis.
Reprinted from Bolton et al,21 ©1998 with permission from Elsevier Science.
C
A
B
GIA staplerTumor
Left recurrentlaryngeal nerve
tage for disease control, althoughthis advantage was not stat i s t i c a l l ysignificant in the analysis of ov e ra l ls u rv i val rat e s .2 4
Enhanced nursing care thatincludes multisystem interv e n t i o n ssuch as aggressive pulmonary toilet;a g g ressive pain control; care f u l ,skilled monitoring for potentialc o m p l i c ations; pre o p e rative andp o s t o p e rative teaching; and an inter-d i s c i p l i n a ry, collaborative appro a c hhas helped lower the mortality rat eof esophagectomy patients. Gre g o i reand Fi t z p at r i c k2 5 refer to this “morec o m p re h e n s i v e” nursing care andc redit it as a factor in enhancing sur-v i val rates. There f o re, nurses play akey role in improving outcomes forthese pat i e n t s .
Nursing Care of Patients After Esophagectomy
After esophagectomy, pat i e n t sgo to an intensive care unit for 24 to48 hours. They are usually intubat e dand have multiple drains and tubes.These patients re q u i re intensive car-d i o p u l m o n a ry monitoring in the
ity in patients undergoing tra n s t h o-racic esophagectomy. Initial painmanagement may consist of mor-phine or bupivacaine given epidu-rally, p at i e n t-c o n t rolled analgesiawith morphine, or a combination ofboth, at the physician’s discre t i o n .Pain should be reassessed as often asn e c e s s a ry to ensure that it is underc o n t rol. Because these pat i e n t sreceive nothing by mouth for 5 to 7d ays, intravenous or epidural painm e d i c ations are used. Oral pain med-i c ations are started once an anasto-motic leak is ruled out on the fifth orseventh postoperative day and oncethe patient is tolerating an oral diet.The main classes of medication usedfor pain control include opioids,n o n s t e roidal anti-inflammat o ryd rugs, and local anesthetics. No n-pharmacological interv e n t i o n sinclude heat/cold, massage, distra c-tion, re l a x ation, and positioning.2 8
Nurses should contact the pain serv-ice if they cannot relieve a pat i e n t ’spain adequat e l y.
Pulmonary CareThe risk of pulmonary complica-
tions is substantial after all esophagealsurgical pro c e d u re s .2 9 -31 A g g re s s i v ep u l m o n a ry toilet should be initiat e di m m e d i ately postoperatively to pre-vent atelectasis and pneumonia,major complications of esophagec-t o m y.3 As addressed earlier, painc o n t rol is paramount in ensuringgood pulmonary toilet. Patients areusually intubated after surgery andm ay or may not be extubated theevening of surgery. Atelectasis orn o n c a rdiogenic pulmonary edemam ay develop quickly after surgery.During the immediate postoperat i v eperiod, monitor ox y g e n ation closelyand maintain vigilance for develop-
i m m e d i ate postoperative period.4
Critical care nursing skills are vitalin the systematic assessment of thesep at i e n t s .
Neurological StatusAssess neurological status every
shift and more often if any changesf rom baseline occur. Even subtlechanges in neurological status mayi n d i c ate a postoperative complicat i o n .D e c reased responsiveness, pupillarychanges, inability to move or unilat-e ral weakness, agitation, inability toc o n t rol pain, or any neuro l o g i c a lchange should be carefully wat c h e dand promptly re p o rted to a physi-cian if it persists.2 6
Pain Management Management of pain is key in
these patients, and adequate painc o n t rol reduces the mortality andmorbidity of patients after esophagec-t o m y.2 7 In 19 9 6, Tsui et al2 7 f o u n dthat adequate pain control con-tributed to decreased card i o p u l-m o n a ry complications, short e rhospital stay, and decreased mort a l-
22 CRITICALCARENURSE Vol 24, No. 1, FEBRUARY 2004
Figure 2 Transthoracic esophagectomy.
Reprinted from Bolton et al,21 ©1998 with permission from Elsevier Science.
Level 4node
Trachea
Azygosvein Level 7
node
Tumor
Level 8node
Esophagus
Thoracic ductAorta

ments that may be associated with asudden decrease in ox y g e n at i o n .Patients may re q u i re suctioning, chestp h y s i o t h e ra p y, and nebulizers toi m p rove pulmonary status. Once ap atient is extubated, initiate coughing,deep bre athing exe rcises, and use ofthe incentive spirometer. Avoidnasot ra c h e a l suctioning because o fthe risk of passing a catheter thro u g hthe new anastomosis.8,2 5 Te a c hp at i e n t s to splint their incision witha pillow. Early mobilization willassist in reducing the pulmonaryrisk of atelectasis, a precursor top n e u m o n i a .3 2 M o n i t o r patientsclosely for fever.
Depending on the type of surgery,a chest tube may be in place. Fo rp atients with chest tubes, assess thed rainage every shift. The dra i n a g eshould become sero s a n g u i n e o u swithin a few hours. Expect no morethan 100 to 200 mL/h on the firstd ay. Drainage should decrease gra d-u a l l y. A sudden change in the colorof chest tube drainage may indicat ean anastomotic leak and should becalled to the attention of a physician.2 5
Check the chest tube site for d ra i n a g e ,and keep the chest tube dre s s i n gclean, dry, and intact. Keep thechest tube free of any kinks ordependent loops,33 and palpate thesurrounding area for subcutaneousemphysema.9
If subcutaneous emphysemadoes develop, it is a harbinger ofpotentially significant complicat i o n s ,and the medical staff should be noti-fied. Subcutaneous emphysema maybe due to an air leak from a pleura li n j u ry sustained during the operat i o n .Such an air leak is not necessarily ofg rave significance, but additionalsuction may be needed or placementof a new chest tube may be re q u i re d .
Of gre ater concern, how e v e r, new -onset subcutaneous emphysemam ay indicate a leak of the esophagealanastomosis. In such instances, airf rom the gastrointestinal tract dissectsu pw a rd through the mediastinumand manifests as subcutaneousemphysema in the chest and neck.Fe v e r, tachyc a rdia, and hypoxe m i aalso may develop in patients withthis complication. Medical staffshould be notified immediat e l y.Esophageal leak can be confirmed bya swallowing study with wat e r- s o l u-ble contrast mat e r i a l .3 4 Po s t o p e rat i v echest ra d i o g raphs should be checked
for pneumothorax and for place-ment of any chest tube.
Acute respiratory distress syn-drome can develop as soon as theevening of surgery. Patients are par-ticularly prone to acute re s p i rat o ryd i s t ress syndrome after tra n s h i at a lesophagectomy because the medi-astinal lymphatics, which dra i np u lm o n a ry interstitial fluid, areextensively disrupted during the sur-g e ry. Although the mechanisms thatlead to the postoperative develop-ment of the syndrome are not fullyunderstood, the vigorous systemici n f l a m m at o ry response that accom-panies the operation may play ani m p o rtant role. This extensive medi-astinal dissection may also initiate ag e n e ralized systemic inflammat o ryre s p o n s e .3 5 Un f o rt u n at e l y, the com-p l i c ation of acute re s p i rat o ry distre s ss y n d rome remains difficult to pre d i c t ,but all patients should be monitore d
for abrupt changes in ox y g e n ation inthe perioperative period.
HemodynamicsPatients are given intrav e n o u s
maintenance fluid (isotonic sodiumchloride solution or lactated Ringersolution) at a rate of 100 to 200 mL/hfor the first 12 to 16 hours after sur-g e ry. These fluids help maintain ade-q u ate circ u l ating blood volume top rotect vital organs and ensure ade-q u ate blood supply to the newly cre-ated anastomosis. Major fluid shiftsoccur in the first few days after sur-g e ry, and hypovolemia may be a
p rob l e m .8 Patients may re q u i re fluidboluses in the immediate postopera-tive period. Crystalloids or bloodp roducts may be used to re s t o re cir-c u l ating volume, but ov e r l o a d i n gwith fluids must be avoided. Thelungs a re already compro m i s e dbecause lymph clearance has beendiminished by the surgical re m ova lof the mediastinal lymphatics andn o d e s .2 5 Reduced clearance of lymphp redisposes these patients to inter-stitial pulmonary edema. Malnutri-tion and low protein levels can furt h e rc o m p l i c ate the situat i o n .
These patients re q u i re a delicat ebalance between adequate fluidreplacement and fluid ov e r l o a d .8 T h eextent and duration of the surgicalprocedure in esophagectomyinevitably results in tra n s u d ation offluid into the interstitium. Theref o re ,p atients need volume support andre h yd ration. How e v e r, because they
CRITICALCARENURSE Vol 24, No. 1, FEBRUARY 2004 23
These patients require a delicate balancebetween adequate fluid replacement and
fluid overload

a re also susceptible to pulmonaryedema, hyd ration should not bee xcessive. In most instances, mainte-nance of 30 mL/h of urine output isevidence of adequate postoperat i v efluid re s u s c i t at i o n .
Determination of body weightand careful documentation of fluidintake and output should be donedaily. Patients usually have an arte-rial catheter in place. If their hemo-dynamic status is unstable, theymay have a pulmonary arterycatheter. Postoperative edema maybe significant, depending on theamount of fluid required to main-tain hemodynamic stability, someticulous skin care is necessary.Fluid in the tissues will seek outdependent areas and cause the skinin those areas to be at greater riskfor breakdown. When hemody-namic status is stable, patientsshould be turned at least every 2hours to assist in maintaining skinintegrity. Patients who cannot toler-ate frequent turning or who are dif-ficult to mobilize will need apressure-relieving surface.36
Nasogastric TubesIn general, all patients have a
nasogastric tube after esophagectomy.Do not move, manipulate, or irrigat ethe nasogastric tube. If the tube comesout for any reason, do not at t e m p tto replace it. The nasogastric tubegoes through the anastomosis and isnot sutured in place.9, 19,2 2 At t e m p t i n gto replace the nasogastric tube mayresult in damage to the anastomosis.Be sure to notify a physician imme-d i ately if the tube becomes dislodgedor does not appear to be functioningp ro p e r l y.2 5 Monitor the tube forp atency and assess the drainage forcolor and amount.
to start tube feedings via the jejunos-tomy tube or to start patients ontotal pare n t e ral nutrition. If no leakis detected, patients are started on aclear liquid diet and advanced to softfoods as tolerat e d .3
Patients should be instructed toeat 6 to 8 small frequent meals eachday, because large meals may not bewell tolerated.3 Also, instructpatients to avoid very hot or coldbeverages and spicy foods. Proteinsupplements, high-energy foods, ora soft dysphagia diet may be indi-cated. A dietician is usually involvedin patients’ care, and laboratoryresults from a weekly nutritionalpanel can guide nutritional decisionmaking. Having patients sit upright,chew slowly, and eat more than 3hours before bedtime assists inreducing reflux.
H aving patients drink fluidsbetween meals rather than with mealsassists in controlling signs and symp-toms of the dumping syndro m e ,which may arise in patients whoh ave had their vagus nerves divided.This common adverse effect aftervagotomy is re l ated to unre g u l at e dgastric emptying and rapid deliveryof carbohyd rates and part i a l l ydigested food products into thesmall intestine. Minimizing liquidswith meals and the consumption off requent, small, low -c a r b o h yd rat emeals also assists in controlling thesesigns and symptoms.3
Patients whose oral intake is notadequate by the time of dischargemay be discharged with plans forsupplemental tube feeding. Suchfeeding requires that patients orcaregivers be taught how to admin-ister tube feedings, and the correctsupplies must be ordered and givento the patients before discharge.
Gastrointestinal CareAfter esophagectomy, pat i e n t s
a re restricted from taking anythingby mouth for 5 to 7 days to pre v e n tan anastomotic leak or fistula forma-t i o n .2 5 Patients have nasogastric tubeswith low -level continuous or inter-mittent suction. Oral medications, ifo rd e red, are crushed and put dow nthe nasogastric tube; they are nevers w a l l owed. Diligent mouth carei m p roves pat i e n t s’ comfort andreduces the risk for infection andshould be maintained while pat i e n t sa re intubated and throughout theperiod when they cannot take any-thing by mouth.
A jejunostomy feeding tube isoften placed during surgery and isleft clamped until used.3 7 Flush thetube with 10 to 20 mL of isotonicsodium chloride solution every shift.Jejunostomy site care should be per-formed on a daily basis. Wash thes u r rounding skin with a gentle soap,and assess the skin for any signs ofi r r i t ation or bre a k down. Apply an o n – p e t ro l e u m -based pro t e c t i v eointment, and make sure that thetube is well secured. Patients may orm ay not be started on tube feedings2 to 3 days after surgery, dependingon the surgeon’s pre f e re n c e .3 8, 3 9
Pre o p e rat i v e l y, patients may hav ebeen receiving total pare n t e ral nutri-tion or some other high-energy liquid supplement. If so, total par-e n t e ral nutrition may be re s u m e dafter surgery.
At 5 to 7 days after surgery, a flu-o roscopic swallowing examinat i o nwith wat e r-soluble contrast mat e r i a lis done to check the anastomosis forleaks before oral intake of anythingis allow e d .2 5 If a leak is suspected, ana l t e r n ative form of nutrition shouldbe started. The physician may choose
24 CRITICALCARENURSE Vol 24, No. 1, FEBRUARY 2004

Genitourinary CarePatients have Foley cat h e t e r s
d raining to gravity after esophagec-t o m y. Monitor fluid intake and outputhourly during the initial postopera-tive period. Call a physician if urineoutput is less than 30 mL/h for 2consecutive hours. Discontinue thec atheter as soon as possible to avo i du r i n a ry tract infections.
Incision CareKeep all dressings clean, dry,
and intact. The surgical dressing isremoved by a surgeon on postopera-tive day 2. Patients may have a neckincision, which can be opened by asurgeon at the bedside if an anasto-motic leak is suspected. Neck inci-sions that are opened up require wetto dry dressing changes 2 to 3 timesa day for several weeks, unless other-wise specified by the physician. Ininstances in which the anastomosishas separated, patients often havesaliva leaking out through the cervi-cal incision. Such leakage is oftenlow in volume and can be managedby simple dressing changes to theneck wound. How e v e r, if a pat i e n tis leaking saliva in large volumes(>250 mL every 8 hours), applica-tion of a wound drainage bag to thelower part of the neck incision maybe required. The leak is allowed toseal on its own, but sealing couldtake several weeks.
DrainsPatients may have a Jackson-
Pratt drain to bulb suction comingout of one of the incisions. Monitorthe amount and color of dra i n a g eeach shift. If the bulb drain will nothold suction, notify the medicalteam. A Pe n rose drain also may bein the neck incision. Change the
d ressing for the Pe n rose drain as oftenas necessary to protect and maintainskin integrity around the dra i n .
Infection RiskPatients who have esophagec-
tomy have many potential sites ofinfection. They often have compro-mised nutritional status, they hav ei n vasive catheters in the early postop-e rative period, and they have theusual risk of infection at the surgicalsites. Meticulous wound and skinc a re, hand washing, avoidance ofc ro s s -c o n t a m i n ation with organismsf rom other patients, and changing ofi n vasive catheters per the facility’sp rotocol assist in reducing thechance of infection. Judicious use ofantibiotics and adequate nutritionalso help avoid infection.
Prophylaxis of Deep Vein Thrombosis
Heparin shots are given subcuta-neously twice a day and compre s s i o nstockings are applied to both low e re x t remities to prevent deep veint h rombosis. Until patients are ambu-l ating independently, they shouldkeep the stockings on when in bed.E n c o u rage early ambulation as wellas leg and ankle exe rcises. Early mob i-l i z ation of patients includes gettingthem out of bed to a chair the firstp o s t o p e rative day and 3 times eachd ay there a f t e r.
Psychosocial AspectsDiagnosis of esophageal cancer
can be a deva s t ating event in a per-s o n ’s life. Patients may struggle withd e p ression, mort a l i t y, and fear pre-o p e rat i v e l y, and most likely they willexperience some fear and anxietyafter surgery. Patients need supportand re a s s u rance postoperat i v e l y.
They may fear mort a l i t y, have con-cerns about body image, or have feel-ings of guilt that their lifestyle habits(eg, smoking and drinking) may hav econtributed to the development oftheir disease.4 E n c o u rage them tofind a counselor with whom they canw o rk through these issues. In addi-tion, some patients may drool; caus-ing embarrassment and adding totheir feelings of isolation. Thesep atients need assistance in learningmethods to manage their secre t i o n s ,such as using a portable suctiondevice, discreet use of tissues, andp roper disposal of potentially infec-tious mat e r i a l .4
Offer explanations and supportto pat i e n t s’ family members andfriends to promote healthy intera c-tions with the patients. Encoura g ep atients to express their feelings andfears in a safe environment. Consideryour own filters or issues with theirdisease and possible causative factors.Help patients focus on the futureand set goals for a healthier diet andlifestyle. Offer community re s o u rc e swhen available (see list in “DischargeI n s t ru c t i o n s” ) .
Other ConsiderationsA high pro p o rtion of pat i e n t s
who have esophageal surgery hav ea history of heavy smoking andalcohol use. Be aw a re of possibledelirium tremens on postoperat i v ed ay 3 or 72 hours after the pat i e n t ’slast drink. Early identification (pre-o p e rative) of patients at risk forsigns and symptoms of withdraw a lis the best prevention, and earlyt re atment is safest for both pat i e n t sand staff members. Be n z o d i a z e p i n e s(most commonly lorazepam) areo rd e red to manage alcohol with-d rawal. For patients experiencing
CRITICALCARENURSE Vol 24, No. 1, FEBRUARY 2004 25

Table 4 Postoperative complications of esophagectomy*
nicotine withdrawal, consider anicotine pat c h .
Postoperative ComplicationsEsophageal resection is an invo l v e d
o p e ration with multiple potential com-plications, of which the nursing staff
p o s t o p e rative complications ofe s o p h a g e c t o m y, their signs andsymptoms, and management techniques. Prevention and earlydetection are the keys to successfulmanagement of postoperative com-p l i c at i o n s .
and the physicians should be aw a re .The postoperative mortality rat ea s s o c i ated with esophagectomy pro-c e d u res ranges from 5% to 13%. Themost common causes of morbidityand mortality are card i o p u l m o n a ryc o m p l i c ations. Table 4 lists possible
26 CRITICALCARENURSE Vol 24, No. 1, FEBRUARY 2004
Complications
Esophageal anastomotic leak
Pneumonia, adult respiratorydistress syndrome, atelectasis
Deep vein thrombosis and/orpulmonary emboli
Gastric necrosis
Cardiac arrhythmias, myocardial infarction
Signs and symptoms Prevention strategies
Fever (≥38.6°C [101°F])Inflammation, painDrainage from the neck
wound or accumulation offluid at the wound site
Subcutaneous emphysemaUnexplained tachycardia or
tachypneaHypoxemiaChange in color of chest tube
drainage25
TachypneaDiminished breath soundsIncreased temperatureHypoxemiaPoor pulmonary complianceInterstitial infiltrates evident
on chest radiographDyspnea/shortness of breathChange in mentationConfusion
Difficulty breathingLeg swellingInflammation of involved legTachypneaArrhythmiasPain in leg
FeverOliguriaAcidosisTachycardiaHypotension
Atrial fibrillationContinuous supraventricular
tachycardiaChest painShortness of breathElectrocardiographic changesElevated cardiac enzyme
levels
Use skilled surgical techniques
Do not feed the patient tooearly
Maintain strict status of nooral intake
Manage pain adequatelyAvoid nasotracheal suctioning
after extubation14
Have patient stop smokingbefore surgery
Frequently turn patient, andprovide use of incentivespirometry, nebulizers
Chest physiotherapy,suctioning
Feed early after surgery38
Have patient ambulate earlyafter surgery
Have patient ambulate earlyafter surgery
Have patient do leg exercisesProvide antiembolism
stockings and sequentialcompression devices
Administer subcutaneousheparin
Use skilled surgical technique
Maintain adequate bloodpressure in perioperativeperiod
Maintain electrolyte balanceProvide adequate pain
managementMaintain normal body
temperatureMaintain hemoglobin level at
100 g/L (10 g/dL)orgreater25
Management
Use esophagography withwater-soluble contrastmaterial to diagnose theleak
Increase tube feedingsAfter several days, dilate the
esophagus if neededOpen neck wound at bedsideIrrigate and pack with wet-to-
dry dressingStop oral intake
Reintubate patient and provide respiratory supportas needed
Provide appropriate antibiotictherapy
Promote aggressive pulmonary toilet
Monitor arterial blood gases
Infuse heparinMaintain bed restUse a Greenfield filterProvide pulmonary support
Provide operative management
Administer digoxin, diltiazem,b-blockers
Use cardioversionReplace electrolytes Use percutaneous
transluminal coronaryangioplasty
Provide oxygen therapyAdminister aspirinAdminister morphineAdminister nitroglycerin
Continued

CRITICALCARENURSE Vol 24, No. 1, FEBRUARY 2004 27
Complications
Prolonged ileus
Wound infection
Sepsis
Gastrointestinal bleeding
Esophageal stenosis or anastomotic stricture
Diarrhea
Bleeding
Chylothorax
Signs and symptoms Prevention strategies
Lack of bowel soundsIncreased nasogastric tube
drainageNausea/vomitingNo evidence of bowel function
for more than 10 days aftersurgery
Decreased appetite
Redness at incisionIncreased pain at incisionFoul odor from woundSwelling at incisionDiscolored drainage from
incisionFever
Change in neurological statusConfusionDecreased systemic vascular
resistanceHypotension
Bloody drainage from nasogastric tube
Tarry stoolsDecreased hematocrit
Difficulty swallowing
Increased loose stoolsFluid and electrolyte
imbalancesWeakness and fatigue
HypotensionDecreased hematocrit
Milky white drainage from thechest tube
Provide adequate pain management with use ofnonnarcotic agents (non-steroidal anti-inflammatorydrugs)
Administer metoclopramideHave patient increase activity
level
Administer prophylacticantibiotics
Use sterile technique at timeof surgery
Maintain adequate tissue oxygenation during surgery
Maximize nutritional statuspreoperatively
Have staff use meticuloushand washing
Administer appropriate andtimely antibiotics
Administer fluidsMaintain strict hand washing
proceduresChange invasive catheters per
the facility’s protocol
Administer H2-blockers
Use meticulous surgical t e c h n i q u e
Choose proper tube feedingHave patient drink liquids
between meals not withmeals
Have staff practice strict hand washing
Use meticulous surgical technique
Use meticulous surgical technique
Management
Administer metoclopramideGive stool softeners,
suppositories, enemas,bowel stimulants
Place a nasogastric tube (byphysician) to prevent vomiting
Open wound and startdressing changes
Administer systemic antibiotics if surroundingerythema significant
Treat underlying causeInsert a pulmonary artery
catheterAdminister vasoactive
medicationsAdminister antibioticsAdminister fluids
Give blood transfusionsDo endoscopy with
coagulationIntervene surgically if needed
Dilate the esophagus
Treat underlying causeAdminister loperamide before
mealsMonitor for infection with
Clostridium difficile
Give blood transfusionsAdminister intravenous fluidsSupport blood pressureIdentify sourceCorrect the causeIntervene surgically if needed
Monitor amount: if chyle output is 400-600 mL per8 hours continuously for 2-3 days, transthoracic ligation of the thoracic ductwill be required14
*If any complications are suspected, notify a physician immediately.
Table 4 Continued

Esophageal anastomotic leakageis the most serious postoperat i v ec o m p l i c ation and may occur 2 to 10d ays after surgery.3
Discharge InstructionsDischarge instructions for pat i e n t s
and their families or caregivers shouldinclude the follow i n g :
• Take a few minutes each day toinspect the surgical incision for anysigns or symptoms of infection orother complications (increased pain,swelling, inflammation, fever,drainage, s a l i va leaking at incisionsite). Re p o rt any problems to yo u rdoctor immediat e l y. See your do c t o rright aw ay if you experience any dif-ficulty swallow i n g .
• Avoid smoking. You may find ithelpful to join a stop smoking supportg ro u p.
• Bathe and shower as usual.Wash the incision gently with a mildunscented soap.
• Avoid strenuous activity for 12weeks after surgery. You may re s u m eyour daily activities, work, and sexualre l ations as soon as you feel able todo so. How e v e r, avoid driving for thefirst 3 weeks after returning home.
• Avoid coffee, tea, cocoa, coladrinks, alcoholic beverages, and anyfood or spices that cause indigestion.Try to eat 6 to 8 small meals a day.Avoid drinking liquids with meals toavoid rapid transit of food thro u g hyour bowel. Drink fluids betweenmeals instead. Eating more than 3hours before bedtime will reducereflux.
• Weigh yourself several times aweek. Re p o rt any significant weightchanges to your doctor (>4.5 kg [10lb] in 2 weeks).
• Try not to take pain re l i e v e r slonger than 4 to 7 days. Talk with
3. Quinn KL, Reedy A. Esophageal cancer:therapeutic approaches and nursing care.Semin Oncol Nurs. 1999;15:17-25.
4. Held JL, Peahota A. Nursing care of patientswith esophageal cancer. Oncol Nurs Forum.1992;19:627-634.
5. Fisher T. Esophageal cancer. Centers for D i s-ease Control and Prevention. Available at :http://atoz.iqhealth.com/HealthAnswers/encyclopedia/HTMLfiles/2524.html.Accessed December 1, 2003.
6. McNamara JP. Esophageal cancer. Nursing82. March 1982;12:64.
7. National Cancer Institute. What you needto know about cancer of the esophagus.Available at: http://www.nci.nih.gov/cancerinfo/wyntk/esophagus. AccessedJanuary 17, 2003.
8. Sideranko S. Esophagogastrectomy. CritCare Nurs Clin North Am. 1993;5:177-184.
9. Hampton B, Dixon L, Wasson D, Bressler C,Caffery L. Esophageal and laryngeal can-cers: the continuum of care from hospital tohome. Symposium conducted at NationalTeaching Institute for Critical Care Nurses;May 2000; Orlando, Fla.
10. Billingsley KG, Maynard C, Schwartz DL,Dominitz JA. The use of trimodality therapyfor the treatment of operable esophagealcarcinoma in the veteran population. Cancer. 2001;92:1272-1279.
11. Walsh TN, Noonan N, Hollywood D, KellyA, Keeling N, Hennessy TP. A comparisonof multimodal therapy and surgery foresophageal adenocarcinoma. N Engl J Med.1996;335:462-467.
12. Minsky BD. Carcinoma of the esophagus, I:primary therapy. Oncology. 1999;13:1225-1232, 1235-1236.
13. Urba SG, Orringer MB, Turrisi A, Iannet-toni M, Forastiere A, Strawderman M. Ran-domized trial of preoperativechemoradiation versus surgery alone inpatients with locoregional esophageal carci-noma. J Clin Oncol. 2001;19:305-313.
14. Orringer MB. Transhiatal esophagectomy:avoiding and managing complications. Car-diothoracic Surgery Network. Available at:http://www.ctsnet.org/doc/106. AccessedMay 9, 2001.
15. American Joint Committee on Cancer.Esophageal cancer: TNM staging system.Available at: http://www. u p m c c a n c e rc e n t e r s.com/cancer/esophageal/tnm.cfm.Accessed February 12, 2003.
16. Orringer MB, Marshall B, Iannettoni MD.Transhiatal esophagectomy: clinical experi-ence and refinements. Ann Surg. 1999;230:392-403.
17. Avendano CE, Flume PA, Silvestri GA, KingLB, Reed CE. Pulmonary complicationsafter esophagectomy. Ann Thorac Surg.2002;73:922-926.
18. Nozoe T, Kimura Y, Ishida M, Saeki H,Korenaga D, Sugimachi K. Correlation ofpre-operative nutritional condition withpost-operative complications in surgicaltreatment for oesophageal carcinoma. Eur JSurg Oncol. 2002;28:396-400.
19. Trastek VF. Esophagectomy: transhiatal. In:Donohue JH, Van Heerden JA, Monson JRT,eds. Atlas of Surgical Oncology. Boston,Mass: Blackwell Science Inc; 1995:121-125.
20. Gandhi SK, Naunheim KS. Complicationsof transhiatal esophagectomy. Chest SurgClin North Am. 1997;7:601-612.
your doctor if you continue to hav epain that re q u i res pain medicat i o nafter a few days. To prevent consti-p ation, take stool softeners at leastas long as you take pain medicat i o n .If you are sent home with antibiotics,please take all of them even if yo ufeel fine. Crush all pills to pro m o t eeasy swallow i n g .
• Notify your doctor if any of thef o l l owing occur: increased pain,swelling, redness, draining, orbleeding at the incisional site; vom-iting; excessive weakness; tarry(black) stools; new, unexplainedsymptoms (they may be adverseeffects of drugs used in tre at m e n t ) ;unexplained pro g ressive weight loss;or continuous diarrhea.
• Keep follow-up appointmentsso that your physician can monitoryour pro g ress and condition.
The American Cancer Society,s u rv i val support groups, social work-ers, chaplains, counselors, and smok-ing (nicotine) cessation pro g rams maybe helpful.8
ConclusionEsophageal cancer remains diffi-
cult to tre at. Patients who undergoesophagectomy experienced e c reased morbidity and mort a l i t ywith more comprehensive nursingc a re. This article provides a basis fornurses to better understandesophageal cancer and the perioper-ative management of risks and com-p l i c ations of esophageal surgery.
References1. G reenlee RT, Hill-Harmon MB, Mu r ray T,
Thun M. Cancer statistics, 2001 [publishedc o r rection appears in CA Cancer J Clin.2 0 01 ; 51 : 144]. CA Cancer J Clin. 2 0 01 ; 51 : 15 -3 6.
2. Schrump DS, Altorki NK, Forastiere AA,Minsky BD. Cancer of the esophagus. In:DeVita VT, Hellman S, Rosenberg SA, eds.Cancer: Principles and Practices of Oncology.Philadelphia, Pa: Lippincott Williams &Wilkins; 2001:1051-1092.
28 CRITICALCARENURSE Vol 24, No. 1, FEBRUARY 2004

21. Bolton JS, Fuhrman GM, Richardson WS. Esophageal resection forcancer. Surg Clin North Am. 1998;78:773-794.
22. Trastek VF. Esophagectomy: Ivor Lewis. In: Donohue JH, Van Heer-den JA, Monson JRT, eds. Atlas of Surgical Oncology. Boston, Mass:Blackwell Science Inc; 1995:126-130.
23. Ferguson MK, Durkin AE. Preoperative prediction of the risk of pul-monary complications after esophagectomy for cancer. J Thorac Car-diovasc Surg. 2002;123:661-669.
24. Hulscher JB, Van Sandick JW, Offerhaus GJ, Tilanus HW, Obertop H,Van Lanschot JJ. Prospective analysis of the diagnostic yield ofextended en bloc resection for adenocarcinoma of the oesophagus orgastric cardia. Br J Surg. 2001;88:715-719.
25. Gregoire AS, Fitzpatrick ER. Esophageal cancer: multisystem nursingmanagement. Dimens Crit Care Nurs. 1998;17:28-38.
26. Nettina SM, ed. The Lippincott Manual of Nursing Practice. 7th ed.Philadelphia, Pa: Lippincott; 2001:458-459.
27. Tsui SL, Law S, Fok M, et al. Postoperative analgesia reduces mortal-ity and morbidity after esophagectomy. Am J Surg. 1997;173:472-478.
28. American Pain Society. Principles of Analgesic Use in the Treatment ofAcute Pain and Cancer Pain. 4th ed. Glenview, Ill: American Pain Soci-ety; 1999.
29. Amar D. Cardiopulmonary complications of esophageal surgery.Chest Surg Clin North Am. 1997;7:449-456.
30. Horvath OP, Lukacs L, Cseke L. Complications following esophagealsurgery. Recent Results Cancer Res. 2000;155:161-173.
31. Griffin SM, Shaw IH, Dresner SM. Early complications after IvorLewis subtotal esophagectomy with two-field lymphadenectomy:risk factors and management. J Am Coll Surg. 2002;194:285-297.
32. Fujita T, Sakurai K. Multivariate analysis of risk factors for postoper-ative pneumonia. Am J Surg. 1995;169:304-307.
33. Gordon PA, Norton JM, Guerra JM, Perdue ST. Positioning of chesttubes: effects on pressure and drainage. Am J Crit Care. 1997;6:33-38.
34. Lerut T, Coosemans W, Decker G, De Leyn P, Nafteux P, van Raem-donck D. Anastomotic complications after esophagectomy. Dig Surg.2002;19:92-98.
35. S ato N, Koeda K, Ikeda K, et al. Randomized study of the benefits ofp re o p e rative cort i c o s t e roid administration on the postoperative mor-bidity and cytokine response in patients undergoing surgery foresophageal cancer. Ann Surg. 2 0 0 2 ; 2 3 6 : 18 4 -19 0.
36. Nixon J, McGough A. Principles of patient assessment: screening forpressure ulcers and potential risk. In: Morison MJ, ed. The Preventionand Treatment of Pressure Ulcers. St Louis, Mo: Mosby; 2001:69-72.
37. Wakefield SE, Mansell NJ, Baigrie RJ, Dowling BL. Use of a feedingjejunostomy after oesophagogastric surgery. Br J Surg. 1994;82:811-813.
38. Bagrie RJ, Devitt PG, Watkin DS. Enteral versus parenteral nutritionafter oesophagogastric surgery: a prospective randomized compari-son. Aust N Z J Surg. 1996;66:668-670.
39. Watters JM, Kirkpatrick SM, Norris SB, Shamji FM, Wells GA.Immediate postoperative enteral feeding results in impaired respira-tory mechanics and decreased mobility. Ann Surg. 1997;226:369-380.

30 CRITICALCARENURSE Vol 24, No. 1, FEBRUARY 2004
CE Test Form
Care of Patients After Esophagectomy
Objectives:
1. Identify the clinical findings associated with esophageal cancer
2. Describe the postoperative complications of esophagectomy
3. Discuss important aspects of nursing care of patients after esophagectomy
Mark your answers clearly in the appropriate box. There is only 1 correct answer. You may photocopy this form.
To receive CE credit for this test (ID C041), mark your answers on the form below, complete the enroll-ment information, and submit it with the $12 processing fee (payable in US funds) to the American Asso-ciation of Critical-Care Nurses (AACN). Answer forms must be postmarked by February 1, 2006. Within 3to 4 weeks of AACN receiving your test form, you will receive an AACN CE certificate.
This continuing education program is provided by AACN, which is accredited as a provider of continuing education in nursing by theAmerican Nurses Credentialing Center’s Commission on Accreditation. AACN has been approved as a provider of continuing educa-tion by the State Boards of Nursing of Alabama (#ABNP0062), California (01036), Florida (#FBN2464), Iowa (#332), Louisiana(#ABN12), and Nevada. AACN programming meets the standards for most other states requiring mandatory continuing educationcredit for relicensure.
Program evaluationAgree Neutral Disagree
Objective 1 was met � � �Objective 2 was met � � �Objective 3 was met � � �The content was appropriate � � �My expectations were met � � �This method of CE is effective � � �
for this content
The level of difficulty of this test was:� easy � medium � difficultTo complete this program, it took me
hours / minutes.
Mail this entire page to AACN, 101 Columbia, Aliso Viejo, CA 92656, (800) 899-2226
Test ID: C041Test writer: Ruth Kleinpell-Nowell, RN, PhD, CS, CCNS
Form expires: February 1, 2006Contact hours: 2.0
Passing score: 7 correct (70%)Category: A
Test fee: $12
Name
Address
City State ZIP
Phone ( )
E-mail address
AACN member number
� I would like to receive my certificate via e-mail (check box)
CE Test Instructions
1. � a 2. � a 3. � a 4. � a 5. � a 6. � a 7. � a 8. � a 9. � a 10. � a 11. � a 12. � a 13. � a 14. � a� b � b � b � b � b � b � b � b � b � b � b � b � b � b� c � c � c � c � c � c � c � c � c � c � c � c � c � c� d � d � d � d � d � d � d � d � d � d � d � d � d � d
CEContinuing Education
CRITICALCARENURSE Vol 24, No. 1, FEBRUARY 2004 31
6. Which of the following is a common early sign of
esophageal cancer?
a. Dysphagia
b. Hiccups
c. Heartburn
d. No notable sign
7. Involvement of the regional lymph nodes is
associated with what type of 5-year survival rate?
a. ≥ 45%
b. ≥ 30%
c. ≥ 20%
d. ≤ 15%
8. In the TNM staging system for esophageal cancer,
what stage corresponds to a tumor invading
adventitia?
a. Stage 0
b. Stage 1
c. Stage IIB
d. Stage III
9. What is the most common cause of morbidity and
mortality after esophageal resection?
a. Bleeding
b. Infection
c. Cardiopulmonary complications
d. Gastric necrosis
10. After esophagectomy, patients are restricted from
taking anything by mouth for how many days?
a. 3 to 5 days
b. 5 to 7 days
c. 7 to 9 days
d. 9 to 11 days
1. How many new cases of esophageal cancer are
diagnosed each year?
a. 2000
b. 5000
c. 8000
d. 12 000
2. Squamous cell carcinoma mainly occurs in what
part of the esophagus?
a. Lower part
b. Gastroestophageal junction
c. Upper part
d. Epithelial surface of stomach
3. Adenocarcinoma arises mainly in what part of the
esophagus?
a. Upper part
b. Middle part
c. Upper and middle parts
d. Distal part
4. Where do distal metastases of esophageal cancer
most often occur?
a. Pancreas
b. Lower colon
c. Lungs
d. Brain
5. In what country is esophageal cancer endemic?
a. China
b. Germany
c. Italy
d. Turkey
CE Test QuestionsCare of Patients After Esophagectomy