continuing medical education - nsuoco files/ce/20180202-prk... · continuing medical education prk...
TRANSCRIPT

Continuing Medical Education
PRK Certification Course
February 2, 2018
Held at
NSU Broken Arrow Campus-Les Walls Vision Center Room BAED 220 on the
second floor & nJoy Vision

Friday, February 2, 2018
8:00-9:00 AM Breakfast & Registration
1 CR 9:00-9:50 AM PRK Pre-Operative Patient Selection/Education/Post-Operative
Care
Dr.’s Sturm & Holsted
1 CR 10:00-10:50 AM
PRK Surgical Treatment Methods/Informed Consent/Surgical
Complications Management
Dr.’s Sturm & Holsted
1 CR 11:00-11:50 AM
PRK Post Operative Management Dr.’s Sturm & Holsted
12:00-1:00 PM Lunch
3 CR 1:00-4:00 PM Visx Surgeon Training Course Dr. Brad Britton
1 CR 4:00-5:00 PM PRK Exam
5:00-6:00 PM Dinner & Travel to nJoy Vision
3 CR 6:00-9:00 PM PRK Wet Lab
Dr.’s Sturm & Holsted
Page 2 of 91

NSUOCO 2018 PRK Certification Course
NSUOCO2018PRKCertificationCourseFebruary 2018
CERTIFICATIONREQUIREMENTS
1. Course Completion
2. Test
3. 4 proctored eyes
1.Within 12 months of course completion
2.Unilateral Cases
3. Submit to NSUOCO
4. Final certification issued by NSUOCO
SummaryofCourseDidactic Course
Pre Op Selection
Patient Education
Patient Options
Surgical Methods
Post Operative Care
VISX Surgeons Course
Wet Lab
Pentacam
Wavescan
Informed Consent
Debridement Techniques
Laser Treatment
Page 3 of 91

NSUOCO 2018 PRK Certification Course
PreOperativePatientSelection,Education
WhyPRK?•Corneal Thickness
•At risk Corneal Topography
•History of EBMD
•Occupational or Recreational
•Military, Police, Martial Arts
‘When Is Surface Ablation Recommended?
Surface ablation techniques remain good alternatives to LASIK for correcting low to intermediate levels of myopia (6.00 D) and astigmatism. Surface ablation can also be a viable alternative for treating higher levels of myopia if it is performed with mitomycin C for haze prophylaxis.
Several results report faster recovery of visual acuity after LASIK in comparison to PRK; however, long-term follow-up shows little, if any, long-term advantage to LASIK.
Most classical indications are patients with thin corneas, epithelial basal membrane dystrophies, or asymmetric corneal topography. In professions or sports with contraindications for a lamellar cut, surface ablation remains as the procedure of choice’
Page 4 of 91

NSUOCO 2018 PRK Certification Course
ConversiontoPRKHighly probable conversion to surface treatment for any refractive surgeon:
Central (thinnest) Pachymetry under 500mm Keratometry > 47.5 D
Severe DES, especially women
Non-orthogonal astigmatism with suspicious topo
Inferior steepening w/o other KC/FFKC signs
Advantages Disadvantages• “Flap – less” appeals to the patient
•Dry Eye Risk
•No Flap Complications
• Slower VA recovery
•Risk of Haze
•Risk of infection
•Discomfort
Consultation
1.Determine expectations/Motivation
2.Review Informed Consent
3.Discuss Goals and Limitations
IS EVERYONE A CANDIDATE FOR REFRACTIVE SURGERY AS LONG AS CLINICAL FINDINGS ARE NORMAL?
Page 5 of 91

NSUOCO 2018 PRK Certification Course
EducationEvery potential candidate needs to understand all options
• Spectacles
•Contact lenses
• LASIK
•PRK
• ICL
•RLE
UnrealisticExpectations:SurgeonBeware!
•Desire to be 20/15
•Complaints about every form of correction
•History reveals they have never been happy with correction from any doctor
U.S. Trends in Refractive Surgery: 2016 ISRS
Survey
U.S. Trends in Refractive Surgery: 2016 ISRS
Survey
Walter Bethke, Managing Editor
PUBLISHED 5 JANUARY 2016
Refractive Surgery Trends of the ISRS
Page 6 of 91

NSUOCO 2018 PRK Certification Course
U.S. Trends in Refractive Surgery: 2016 ISRS SurveyU.S. Trends in Refractive Surgery: 2016 ISRS Survey
The ratio of PRK to the total number of laser vision correction procedures remained the same 2015 and 2016 at 28 percent
U.S. Trends in Refractive Surgery: 2016 ISRS Survey
U.S. Trends in Refractive Surgery: 2016 ISRS Survey
61 percent of surgeons prefer LVC for a low hyperope (<+3 D), vs. 17 percent who would prefer RLE. The situation flips for high hyperopes (+5 D), however, with 74 percent preferring RLE vs. just 8 percent who would do LVC
U.S. Trends in Refractive Surgery: 2016 ISRS SurveyU.S. Trends in Refractive Surgery: 2016 ISRS Survey
Respondents say they’d perform on a high (> -9.00 D) myope:
PRK (15 percent)
LASIK (29 percent)
Phakic IOL (33 percent)
Refractive lens exchange (14 percent)
“It’s amazing to me that we’re still doing more LVC than lenses for high myopes,” says Dr. Duffey
Page 7 of 91

NSUOCO 2018 PRK Certification Course
Candidacy:Whatare“acceptedranges”oftreatment?
General Treatment Continuum for Refractive Surgery
‐0.75 to ‐6.00 ‐6.00 to ‐8.00 > ‐8.00
PRK/Lasik/ICL Lasik/ICL ICL/RLE
CandidacyGeneral Treatment Continuum for Refractive Surgery
+1.00 to +2.50 > +2.50
PRK/Lasik RLE
PRKRefractiveNonCandidates
•Greater than ‐8.00
•Greater than +2.50
• Younger than 18 Years
•Unstable Refraction
•Prism requirement or binocular issues
Page 8 of 91

NSUOCO 2018 PRK Certification Course
PRKRefractiveConsiderations
•Refraction > ‐6.00
•High Cylinder
• Young Hyperopes
• Early Lens Changes
•Possible binocular issues
•Overly High Expectations
Education‐ Limitations•Presbyopia
•Monovision: Contact Lens Trial for 2 weeks minimum
•Patient should be very happy with monovision to proceed
• “No one is glasses free”: Possible night driving correction, eventual near vision correction
SystemicConsiderations• STOP
• Herpes Zoster
• Pregnancy
• Autoimmune Disease
• Keloid History
• CAUTION VS STOP
• Herpes Simplex
• Diabetes
• Collagen Vascular Disease
Page 9 of 91

NSUOCO 2018 PRK Certification Course
OcularConditionsSTOP
• Keratoconus
• Pellucid
• Glaucoma
• Monocular
• Severe Dry Eye
• Corneal Thickness under 470
• Post Operative Corneal Thickness
< 400
CAUTION
• Irregular Topography
• Ocular Hypertension
• Dry Eye Risk
• Amblyopia
• Corneal Thickness < 500
• Patients Under 21 YO
PreOperativeDryEye
•Treat Aggressively
•Proceed only if well controlled
UNDERSTAND AND UTILIZE ALL DRY EYE THERAPIES AND INDICATIONS
CONTRAINDICATIONSLABELWARNINGS/MEDICATIONS•ACCUTANE
• IMITREX
•CORDARONE
•PACEMAKER
WARNING: The effects of electromagnetic emissions from the excimer laser system on other devices, such as cardiac pacemakers or implanted defibrillators, is unknown. Operation of the laser in proximity to such devices is not recommended.www.accessdata.fda.gov/cdrh_docs/pdf/P930016S025c.pdf
Page 10 of 91

NSUOCO 2018 PRK Certification Course
PREOPEVALUATION
•Contact Lens Protocol•Soft Lenses: 2 weeks prior to testing
•Soft Toric Lenses: 3‐4 weeks prior to testing
•Rigid Lenses: 2 to 6 months
Refraction, Wavescan, Pentacam all stable one month apart
PREOPFINDINGS•UCVA
• DEPENDENCE ON CORRECTION
•BCVA• 20/20
• IF NOT –WHY NOT?
•AMBLYOPIA
• MUST BE 20/40 OR BETTER
PREOPERATIVETESTING/DOCUMENTATION
•MOTIVATION FOR SURGERY
•UCVA
•CURRENT LENSES/LENGTH OF WEAR
•DEPENDENCE
•ADAPTION TO CURRENT CORRECTION
•STABILITY
•BINOCULAR ASSESSMENT
Page 11 of 91

NSUOCO 2018 PRK Certification Course
PREOPERATIVETESTING/DOCUMENTATION•DRY REFRACTION
• PUSH PLUS
• PUSH PENTACAM OR WAVESCAN CYLINDER
•PENTECAM/K’S
•WAVESCAN
•CYCLOPLEGIC REFRACTION
•DOMINANT EYE
• INFORMED CONSENT OPTIONS – RISKS ‐ BENEFITS
PREOPERATIVETESTING/DOCUMENTATION
•ANTERIOR SEGMENT
•Blepharitis, lagophthalmos
• Small Lid Aperture
•Deep Set Eyes
•Dry Eye
•Guttata
• EBMD
•Dry Eye/MGD
PREOPERATIVETESTING/DOCUMENTATION
• IOP Baseline (IOP reduced 1mmHg for every 20 microns ablated)
•Rule out Glaucoma
•Full Retinal Exam
Page 12 of 91

NSUOCO 2018 PRK Certification Course
Recommendation
Recommend PRK to increase function for ________________
and reduce dependence on correction. Ed on presbyopia, options, risks and benefits.
PRKRISKSCOMPAREDTOLASIKDISCUSSION• INFECTION
• SCARRING/HAZE
• PAIN
• ENHANCEMENT
• RISK 1/500 AND GREATER THAN LASIK
• 1/100
• 1/10
• WAIT UNTIL STABLE – USUALLY LONGER THAN LASIK PATIENTS
CornealThickness• PRK is often considered for LASIK non candidates with at risk topography and thin corneas
• Estimating Stromal Bed Depth
• CUSTOM TREATMENT
• APPROX 18 MICRONS PER DIOPTER
PRE OP PACHS – EPI THICKNESS ‐ ABLATION = RSB
EXAMPLE:
‐5.00D MYOPE WITH 510 CENTRAL PACHS
Page 13 of 91

NSUOCO 2018 PRK Certification Course
PREOPERATIVEKERATOMETRY•DO NOT FLATTEN TO < 36.00 (FDA 34.00)
•DO NOT STEEPEN TO > 48.00 (FDA 49.00)
MYOPIC TREATMENTS FLATTEN 0.7D PER 1D
HYPEROPIC TREATMENT 1 TO 1 STEEPENING
EXAMPLES: ‐3.00D MYOPE WITH 43.00 K’S
+1.50D HYPEROPE WITH 43.00 K’S
Scheimpflug Image
+ 3D Anterior Chamber Analyzer
+ Pachymetry Map
+ Topography Maps (ant. & post.)
+ Elevation Maps (ant. & post.)
+ Anterior Chamber Depth Map
+ Cataract Analyzer
+ Holladay Report
+ Tomography
= Pentacam
With only 1 measurement in less than 2 seconds
Pentacam,thecomprehensiveanalysis
SHALLHORN, S. MEDICAL DIRECTOR OPTICAL EXPRESS DATA –ASCRS, 2012
Why front and back surface corneal evaluation…and what do we pay attention to?
N= 81,715
Both Femtosecond and Mechanical Flaps
CCT <500: 2181 CCT >500: 79534
Page 14 of 91

NSUOCO 2018 PRK Certification Course
ScheimpflugExample
Schematiccourseofascan
ScreeningPatientforRefractiveSurgery
• Recommend using Pentacam as only topographic method of analyzing the cornea
• Additional forms of technology (Orbscan or Humphrey Atlas) actually decrease NOT increase the sensitivity and specificity of the screening process
Page 15 of 91

NSUOCO 2018 PRK Certification Course
Pentacam– RecommendedSettingsforRefractiveSurgeryScreening
• Scan Default ‐ 25 images per scan
• Elevation maps
• BFS – Best Fit Sphere• Float• Diameter – Manual = 8.0mm
• K‐Value Presentation• Diopter• R flat / R steep
Pentacam– RecommendedSettingsforRefractiveSurgeryScreening
• Form Factor Present ‐ Asphericity (Q)
• Q < 0 untreated cornea, normal case
• Q > 1 treated cornea LASIK/PRK/RK• Color Scale American Style
• Curvature Color Bar – 1.00 D
• Pachy Color Bar ‐ 10 um• Elevation Color Bar 2.5um
• Curvature Unit ‐ Diopter
Pentacam– RecommendedSettingsforRefractiveSurgeryScreening
• Map Overlay Settings
• Show Thinnest Location (hollow black ring)
• Show Pupil Center (Black dot)
• Show Apex Position (White dot)
• Show Pupil Edge (Black & White line)
• Show Nasal/Temp
• Show OS/OD
Page 16 of 91

NSUOCO 2018 PRK Certification Course
SuggestedInstallationSettings• "REFRACTIVE" 4 composite display
• PACH ‐ Right click on the scale and set to "ABS NORMAL" Right click on the actual display for the drop down menu. Turn ON the following (Apex (#1), Thinnest (#2), Pupil Edge (#6), Nasal/Temp (#7), Max Diam 9.0 (#11) and Show Numeric (#13).
• ANTERIOR ELEVATION & POSTERIOR ELEVATION ‐ Right click on scale and set to BELIN INTUITIVE and REL 2.5 mm. Right click on display and turn ON (Apex (#1), Thinnest (#2), Pupil Edge (#6), Nasal/Temp (#7), Max Diam 9.0 (#11), and Numeric (#12).
• SAGITTAL CURVE ‐ Right click on scale and set to ABS NORMAL, AMERICAN, and Diopter. Right click on the display and set to (Min Radius (#3), Pupil Edge (#6), Nasal/Temp (#7), Max Diam 9.0 (#11), Numeric (#12), and Min/Max (#13).
• MAIN SETTINGS go to MISC SETTINGS and make sure the following are ON• Startup Display ‐ STORE LAST
• Elevation Ref Shape – Sphere, Float, Diameter Manual = 8.0mm
RefractiveScreening• Print the following for all patient eyes
• 4 Map Refractive Display
• Belin Intuitive Color
• Belin‐Ambrosio Enhanced Ectasia Display
• Print the following for all patients whose BAD Maps are not 100% normal
• 4 Map Display
• American Style Color
PentacamDisplays4‐MapsRefractive
American Color Belin Intuitive Color
Page 17 of 91

NSUOCO 2018 PRK Certification Course
PentacamDisplayBAD– EnhancedEctasiaDisplay
4-Maps Refractive – American Color BAD – Enhanced Ectasia Display
NormativeDatabase>1400myopiceyes
PentacamInterpretation4‐MapsRefractive
• Ectasia is a disease of corneal thinning that begin on the back of the cornea
• Thinning causes changes in elevation at the corneas thinnest point
• Ectasia screening must primarily focus on cornea thinnest point
• Keratoconus is a bilateral often asymmetric disease
Page 18 of 91
NSUOCO 2018 PRK Certification Course
PentacamInterpretation4‐MapsRefractive
• Secondary consideration is elevation around the corneal apex
• Limited consideration to areas of elevation away from thinnest point
• Limited consideration to curvature (Sagittal/Axial) maps
Howare“Elevation”MapsDisplayed?
Reference surface (sphere)
The most common method is to compare the data against a suitable reference surface.
NormalValueMethods• Elevation values used to calculate the BFS were taken from within an 8mm circle centred on the apex.
• No extrapolated data was used.
Page 19 of 91

NSUOCO 2018 PRK Certification Course
Effect of BFS Diameter on the Appearance of the Elevation map
Diameter = 7.0 mm Diameter = 9.0 mm Diameter = 11.94 mm
NormalElevationValues•Patients with anterior corneal elevation at the apex or thinnest point >6µm represent <5% of the population.
• Patients with posterior corneal elevation at the apex or thinnest point >13µm represent <5% of the population.
NormalElevationValues•Patients with anterior corneal elevation at the apex or thinnest point >8µm represent <0.5% of the population.
• Patients with posterior corneal elevation at the apex or thinnest point >18µm represent <0.5% of the population.
Page 20 of 91

NSUOCO 2018 PRK Certification Course
• Individuals with > 17 micron difference between their eyes represent less than 5% of the population
• Individuals with a > 25 micron difference occur in less than 1%.
•Pachymetric asymmetry outside the normal range should alert the clinician to carefully examine for other parameters that may be more established surgical risk factors.
Belin/AmbrosioEnhancedElevationMaps
3.5mm exclusion zonecentered on thinnest point
Page 21 of 91

NSUOCO 2018 PRK Certification Course
EnhancedBestFitSphere• In eyes with Keratoconus the area of steepening causes a steepening of the BFS
• This causes the early forms of keratoconus to be less obvious
• Eliminating the area of steepening from the BFS calculation increases the sensitivity of keratoconus detection
BADIIEnhancedEctasiaDisplay• Elevation
• Front Difference Map• Green = Normal < 1.6 SD
• Red = Keratoconus > 2.6 SD
• Yellow = Suspect >1.6 and < 2.6 SD
• Back Difference Map• Green = Normal < 1.6 SD
• Red = Keratoconus > 2.6 SD
• Yellow = Suspect >1.6 and <2.6SD
• Pachymetry
• CTSP and PTI within 95% confidence interval
• Thinnest point difference between eyes > 25 microns
• Average Progression Index > 1.35
• Thinnest Decentration > 1.0mm and coincident with max elevation
BADII– BelinAmbrosioEctasiaDisplayII•Df – front surface
•Db – Back surface
•Dp – Pachymetric Progression
•Dt – Thinnest point
•Dy – Thinnest point displacement
•D – Overall
Page 22 of 91

NSUOCO 2018 PRK Certification Course
BADIIEnhancedEctasiaMap
•Uses multivariant regression analysis to give relative risk score for each eye
• 5 key variables
•Red – abnormal no LASIK possible PRK
• Yellow Suspicious – PRK and LASIK depending on which variable yellow and risk tolerance
•Green = Normal Safe for LASIK or PRK
PentacamInterpretation4MapsRefractive&PachymetricAnalysis
• 4‐Maps Refractive
• Check Quality (QS)
• Shape/Symmetry of Anterior Elevation
• Thinnest Point Anterior Elevation
• Shape/Symmetry of Posterior Elevation
• Thinnest Point Back Elevation
• Presence of elevated island formation/coincidence
• Evaluate BAD Enhanced Ectasia Display Indices
• Enhanced Elevation Difference Maps – Grren/Yellow /Red
• PTI and CTSP Maps within 2SD
• Average Progressive Thickness Progression
• Pachymetry Map Thinnest point and decentration
• Pachymetric Map thinnest point fellow eye comparison
• Overall Map D‐values (5 individual and overall)
PentacamInterpretation• Evaluate fellow eye and all available clinical data
• Loss of BCVA• Asymmetric Astigmatism
• Oblique astigmatism
• Slit lamp biomicroscopy
• Ultrasound pachymetry
• Wavefront Aberrometry • Elevated vertical coma > 35 microns @ 6.0mm
• Clinical History• Family History of Keratoconus
• Eye Rubbing
Page 23 of 91
NSUOCO 2018 PRK Certification Course
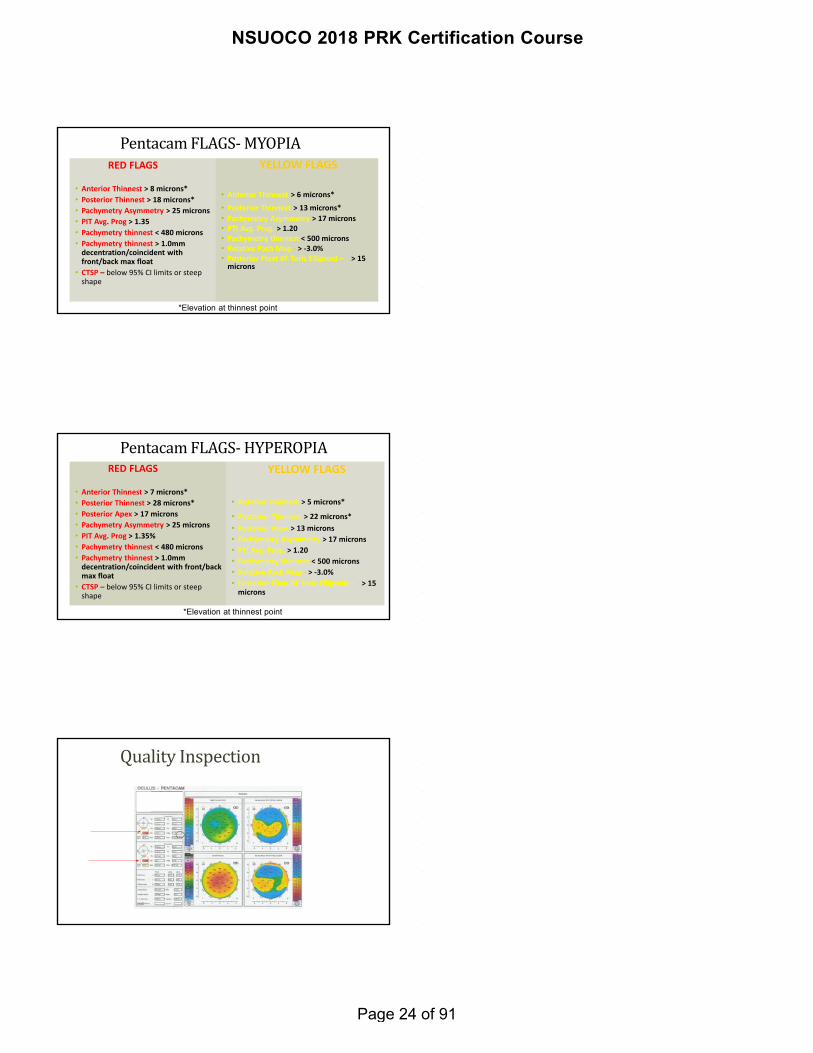
PentacamFLAGS‐MYOPIARED FLAGS
• Anterior Thinnest > 8 microns*
• Posterior Thinnest > 18 microns*
• Pachymetry Asymmetry > 25 microns
• PIT Avg. Prog > 1.35
• Pachymetry thinnest < 480 microns
• Pachymetry thinnest > 1.0mm decentration/coincident with front/back max float
• CTSP – below 95% CI limits or steep shape
YELLOW FLAGS
• Anterior Thinnest > 6 microns*
• Posterior Thinnest > 13 microns*
• Pachymetry Asymmetry > 17 microns• PTI Avg. Prog. > 1.20• Pachymetry thinnest < 500 microns• Relative Pach Map ‐ > ‐3.0%• Posterior Float BF Toric Ellipsoid – > 15 microns
*Elevation at thinnest point
PentacamFLAGS‐ HYPEROPIARED FLAGS
• Anterior Thinnest > 7 microns*
• Posterior Thinnest > 28 microns*
• Posterior Apex > 17 microns
• Pachymetry Asymmetry > 25 microns
• PIT Avg. Prog > 1.35%
• Pachymetry thinnest < 480 microns
• Pachymetry thinnest > 1.0mm decentration/coincident with front/back max float
• CTSP – below 95% CI limits or steep shape
YELLOW FLAGS
• Anterior Thinnest > 5 microns*
• Posterior Thinnest > 22 microns*
• Posterior Apex > 13 microns
• Pachymetry Asymmetry > 17 microns
• PTI Avg. Prog. > 1.20
• Pachymetry thinnest < 500 microns
• Relative Pach Map ‐ > ‐3.0%
• Posterior Float BF Toric Ellipsoid – > 15 microns
*Elevation at thinnest point
QualityInspection
Page 24 of 91

NSUOCO 2018 PRK Certification Course
PentacamInterpretation• Check quality of exam• QS: Quality Specifications
• White – Normal test
• Yellow – reduced reliability (repeat)
• Red – must repeat test
• Click on “QS” for details
Page 25 of 91

NSUOCO 2018 PRK Certification Course
Page 26 of 91

NSUOCO 2018 PRK Certification Course
Page 27 of 91

NSUOCO 2018 PRK Certification Course
Page 28 of 91

NSUOCO 2018 PRK Certification Course
Page 29 of 91

NSUOCO 2018 PRK Certification Course
Page 30 of 91

NSUOCO 2018 PRK Certification Course
QUESTIONSANDDISCUSSION
Page 31 of 91

NSUOCO 2018 PRK Certification Course
PATIENTEDUCATION
•CANDIDACY
•OPTIONS
•RISK VS BENEFIT
•EXPECTATIONS
CANDIDACY‐ EDUCATION
• ‘You are or are not a candidate’
• ‘The safest option is not to have surgery’
• ‘My goal is to reduce not eliminate correction’
• ‘Your options for correction are “
• ‘Risks are summarized in your consent form, and I would like you to understand surgery has risk’
DEVELOP A CONSISTENT EDUCATION PROTOCOL AND PROCESS
DISCUSSINGPATIENTEXPECTATIONS
•DISCUSSING EPITHELIAL REMOVAL AS OPPOSED TO A LASIK FLAP
•HEALING AND PAIN EXPECTATIONS
•VISUAL RECOVERY
Page 32 of 91

NSUOCO 2018 PRK Certification Course
SURFACEABLATIONSURGICALMETHODS
•PRK•Laser/mechanical/chemical
•EPI – LASIK
•LASEK
PRKPROCEDURE
• Epithelium Removal is done using one of the following methods: Each will be discussed again in detail during wet lab
• CHEMICAL DEBRIDEMENT: Uses dilute alcohol 5 to 20%
• MECHANICAL DEBRIDEMENT: Brush/Scrape/EBK manually with a mechanical brush, surgical spatula, instrument
• TRANSEPITHELIAL REMOVAL: Ablate epi with laser followed by manual scrape
Page 33 of 91

NSUOCO 2018 PRK Certification Course
EpiBowmanKeratectomy
https://www.youtube.com/watch?v=JV‐Y2_9bAu4
ALCOHOLMETHODS
EPITHELIALREMOVAL
Start at nasal edge of optical zone, use rapid vertical strokes across the visual axis. Once the majority of the epi is removed, swipe to assure no cells are left, surface should appear smooth.
Page 34 of 91

NSUOCO 2018 PRK Certification Course
EPI‐LASIK LASEK
PRKPROCEDURE• PATIENT IS ASKED TO FIXATE
• TRACKER IS ENGAGED
• ABLATION INITIATED
• PAUSE AS NEEDED, BUT MINIMIZE TIME TO MINIMIZE CORNEAL
DEHYDRATION
• MITOMYCIN‐C APPLIED
• BANDAGE LENS PLACED
• REMOVE SPECULUM
• MORE DETAIL COVERED IN SURGEON COURSE/HANDS ON WET LAB
PRKPOSTOP
•BEFORE PATIENT LEAVES THE CENTER
•CHECK FOR BCL POSITION
•REVIEW ALL INSTRUCTIONS
•MEDICATIONS
• FOLLOW UP
•PAIN CONTROL
•RELEASE TO DRIVER
Page 35 of 91

NSUOCO 2018 PRK Certification Course
WhathaschangedaboutPRKtoday?• New NSAID’s
• Prolensa (Bromday/(Xibrom), Ilevro (Nevenac), Acuvail
• BANDAGE BCL’s‐less hypoxia
• Healthier epithelium = faster re‐epithelialization
• Slow VA recovery but minimal discomfort
• Mitomycin‐C
• Less haze
BandageContactLenses(BCL’s)
• LENS APPROVED AS BANDAGE LENS/ EQUIVALENT
• BCL USED FOR PATIENT COMFORT
• FLOAT LENS FOR REMOVAL OR USE FORCEPS
SecondEye
TIMING
• FDA states 3 month apart
•MOST patients desire bilateral simultaneous PRK
• Recommend minimum of 5 to 7 days for visual recovery
• Educate regarding functional limitations with post
operative bilateral blur
• Infection risk
Page 36 of 91

NSUOCO 2018 PRK Certification Course
POSTOPREGIMEN• FLUOROQUINOLONE ANTIBIOTIC
• STEROID
• NSAID
• PF TEARS
• FOX SHIELDS
• SUNGLASSES
• PAIN MEDS
ZYMAXID QID
LOTEMAX QID
PROLENSA BID
EVERY HOUR
WHILE SLEEPING
WHILE AWAKE FOR 3 DAYS
NORCO VS LYRICA VS TYLENOL #3
PRKPOSTOP
• SLEEP AS MUCH AS POSSIBLE
• DO NOT RUB
• USE FOX SHIELD WHILE SLEEPING
• DISCOMFORT IS NORMAL
• PAIN MEDICATION OPTIONS
• ICE PACKS
• REST
• VISION AND DISCOMFORT WORSEN OFTEN AT DAY 2
POSTOPREGIMEN
•ANTIBIOTIC FOR 5 TO 7 DAYS
• STEROID FOR TWO WEEKS, THEN TAPER BID FOR TWO WEEKS AND QD FOR TWO WEEKS
•NSAID UNTIL EPI HEALED, THEN DC
• TEARS FOR 3 MONTHS – MINIMUM OF QID
Page 37 of 91

NSUOCO 2018 PRK Certification Course
POSTOPSCHEDULE
• SEE PATIENT DAILY UNTIL EPI IS SEALED AND BANDAGE IS REMOVED
• 1‐2 WEEK VISIT (USUALLY ONE WEEK POST BCL REMOVAL)
•MONTHLY AT MONTH 1, 2, 3
• Enhancement considerations USUALLY not until after month 6
DAY1
•20/30 TO 20/80 VISION
•CENTRAL DEFECT 5 TO 6 MM
•ASSESS PAIN CONTROL
Page 38 of 91

NSUOCO 2018 PRK Certification Course
DAY2
•20/30 TO 20/80 VISION
•CENTRAL DEFECT 3 TO 5 MM – SHOULD BE SMALLER THAN DAY ONE
•ASSESS PAIN CONTROL
2 Day post-op
2 Day post-op
Page 39 of 91

NSUOCO 2018 PRK Certification Course
2 Day post-op
2 Day post-op
DAY3to4• 20/40 TO 20/100 VISION
•CENTRAL DEFECT 0 TO 1 MM
• 99% OF PATIENTS ARE COMPLETELY RE ‐EPITHELIALIZED BY DAY 4
• Float BCL for removal
• Use forceps
• Remember this is not normal or smooth epithelium. BLUR IS NORMAL
Page 40 of 91

NSUOCO 2018 PRK Certification Course
3 Day post-op
3 Day post-op
3 Day post-op
Page 41 of 91

NSUOCO 2018 PRK Certification Course
3 Day post-op
5 Day post-op
5 Day post-op
Page 42 of 91

NSUOCO 2018 PRK Certification Course
5 Day post-op
5 Day post-op
• 2 wks PO: approaching NL VA (at least OU)
• UCVA approx 20/25
• May be worse if high Preop RX (myop., hyper., astig.)
• May see the overshoot (opposite sign of pre‐op RX)
•RTC at One Month
•Pt. Ed. re: VA fluctuation and improvement gradually over next several weeks
PRK:WhattoExpect
Page 43 of 91

NSUOCO 2018 PRK Certification Course
• 1‐3 month PO
• Settling near PO end result
•UCVA should be near 20/20
•Check for PRK Haze. Peak haze is at 3 mos.
•With Mito – C it is unusual to see more than trace to 1+ haze
•Pt. Ed. re: slow improvement in VA quality over next few months.
PRK:WhattoExpect
1 month post-op
1 month post-op
Page 44 of 91

NSUOCO 2018 PRK Certification Course
1 month post-op
1 month post-op
1 month post-op
Page 45 of 91

NSUOCO 2018 PRK Certification Course
PRK:PostOperativeComplicationsDuringEpiHealing
• Infectious keratitis
•Tight LensSyndrome
•Epithelial erosion
•Steroid Response
ASCRS 2001 Survey: Infections after LASIK 2001
48%
33%
3%10%
3%3%
Mycobacterium
Staph
Strep
Fungal
Nocardia
Gram Negative
ASCRS Survey: Infections after LASIK 2004
4%
62%
12%
5%
5%
12%
Mycobacterium
Staph
Strep
Fungal
Nocardia
Gram Negative
Page 46 of 91

NSUOCO 2018 PRK Certification Course
ASCRS Survey: Infections after LASIK 2008
28%
18%
9%9%
9%
27%
MRSA
Staphylococcus
Streptococcus
Fungal
Culture Negative
Other
MRSA–MostCommonInfectioninLaserVisionCorrection
HowtoIdentifyMRSAInfection
•Presents Day 2‐4 – Day 1 looks normal and then patient call in pain between day 2 and 4
• Slow to heal – example, 4mm defect in one eye with fellow eye healed
• Significant Pain – Break through pain from neurontin, pain greater than expected for small infiltrate
•Non‐healing Peripheral Infiltrates – QID PF should resolve non‐infectious infiltrates within few days
Page 47 of 91

NSUOCO 2018 PRK Certification Course
PatientsatRisk• Health Care Workers
• Known carriers of MRSA
• Blepharitis
ProphylaxisofpatientsatriskPre‐op• Aggressive treatment of blepharitis to reduce lid colonization by staphylococcus
• (Hot compresses, lid hygiene)• SteriLid lid prep – (http://www.theratears.com/sterilid.aspx) • Regular Zymar or Vigamox QID x 5‐7 days
Intra‐op• Regular Betadine lid prep
Post‐op• Regular Zymar or Vigamox QID• Add Polytrim or Neosporin drops QID
Unimpressivebeginnings
Page 48 of 91

NSUOCO 2018 PRK Certification Course
RightEye
LeftEye
MRSAInfiltrateunderLASIKFlap
Page 49 of 91

NSUOCO 2018 PRK Certification Course
Treatmentofpostrefractivesurgerycornealinfiltrate(anysize)
• Presume MRSA infection resistant to Zymar/Vigamox until proven otherwise by culture
• Lift flap (LASIK) and culture (PRK or LASIK)• Irrigate Vancomycin 25mg/ml under the flap
• Increase Zymar/Vigamox Q1H
• Add Vancomycin 25 mg/ml Q30min
• If Vancomycin not immediately available, add Bacitracin ointment/Polytrim/Neosporin
until Vancomycin available.
• Follow‐up every 12‐24 hours until resolution.
PRK:Complications
Inflammation• Usually due to dryness, exacerbated by allergy and trauma of surgery
• Increase lubrication/Chill Lubricating drops
• Increase Steroid/Decrease Activity
• BCL exchange – Look for signs of tight lens
DryEye
• The most common reason for poor vision, delayed recovery
• Tears ARE PRESCRIBED not recommended
•Restasis
•Plugs
• Treat MGD
Page 50 of 91

NSUOCO 2018 PRK Certification Course
PostOpComplications
Corneal Haze: Steps to avoidMitomycin C
Steroid Use
• Slow taper
• Will not eliminate haze
UV protection
Page 51 of 91

NSUOCO 2018 PRK Certification Course
PostOpComplications
Corneal Haze: • Myopic Shift
Treatment Options
Initiate Steroid and Taper
Time
Retreat
PRK:ManagingPost‐OpComplications
Epithelial Erosion• Treat like recurrent corneal erosion
• Muro Ung qhs
• Muro gtts or FreshKote 3‐4x/day
• Frequent pres. free artificial tears
• May require BCL early
Page 52 of 91

NSUOCO 2018 PRK Certification Course
QUESTIONSANDDISCUSSION
Page 53 of 91

Physician Certification Course for the STAR S4 Excimer Laser System
Physician Certification Course forthe STAR S4 Excimer Laser System
Place of Conference or Author
Month Day, 201X
LIB04893 Rev 01
2
Purpose•The purpose of this presentation is to certify physicians to use the STAR S4 Excimer Laser System
•In addition to completing this course, it is the responsibility of physicians to read and understand the:
• STAR S4 IR Excimer Laser System Operator’s Manual•Professional Use Information•Patient Information Booklet
3
• Introduction to the STAR S4 IR Excimer Laser System
• Indications, Contraindications, Warnings and Precautions for Conventional Procedures
• Pre‐Operative Evaluation
• STAR S4 IR Excimer Laser System Hardware Overview
• STAR S4 IR Excimer Laser System Calibration
• Initial Surgical Recommendations
• Steps in the STAR S4 IR Excimer Laser System Conventional Procedure
Agenda
Page 54 of 91

Physician Certification Course for the STAR S4 Excimer Laser System
4
Introduction to the STAR S4 IR Excimer Laser System
Introduction to theSTAR S4 IR Excimer Laser System
•The STAR S4 IR Excimer Laser System is a 193 nm excimer laser system capable of delivering:
• Conventional (manifest‐refraction‐based) treatments
• Therapeutic treatments (PTK)
5
Introduction to the STAR S4 IR Excimer Laser System
•STAR S4 IR Excimer Laser System features include:•Non‐Gaussian (top hat) 193 nm beam• 3 D ActiveTrak eye tracking system•Variable Spot Scanning (VSS)•Adjustable Optical and Ablation Zones•Ozone compensation
6
Page 55 of 91

Physician Certification Course for the STAR S4 Excimer Laser System
7
Indications, Contraindications, Warnings and Precautions
8
•Physicians should refer to the STAR S4 IR Excimer Laser System Operator’s manual and the Professional Use Information for a complete discussion of Indications, Contraindications, Warnings and Precautions for LASIK and PRK.
Indications, Contraindications, Warnings and Precautions
9
•The STAR S4 IR Excimer Laser System is indicated for Photorefractive Keratectomy (PRK) in patients:
•Who are 18 years of age or older for the treatment of spherical myopia up to ‐6.00 D
•Who are 21 years of age or older for the treatment of myopic astigmatism and hyperopic astigmatism
•With refractive stability
Refractive Indications
Page 56 of 91

Physician Certification Course for the STAR S4 Excimer Laser System
Conventional PRK Treatment Limits
Manifest Refraction
Sphere CylinderSpherical
Equivalent
Myopic Astigmatism
-12.00 D -4.00 D -12.00 D
Hyperopic Astigmatism
+5.00 D +4.00 D +6.00 D
Mixed Astigmatism
Not Approved Not Approved Not Approved10
11
•A stable manifest refraction as evidenced by less than or equal to the following change in the spherical and the cylindrical component of the manifest refraction over the previous year is required:
•Myopia: ±0.50D ( < ‐6.00D MRSE)
•Hyperopia: ± 1.00D
•High Myopia: ±1.00D ( ≥ ‐6.00D MRSE)
Refractive Stability
12
Contraindications•Laser refractive surgery for Conventional PRK is contraindicated in:
• Patients with collagen vascular, auto‐immune or immunodeficiency diseases
• Women who are pregnant or nursing
• Patients with signs of keratoconus or abnormal corneal topography
• Patients who are taking the following medications
• Isotretinoin (Accutane®)
• Amiodarone hydrochloride (Cordarone®)
Accutane is a registered trademark of Hoffman-La Roche, Inc.Cordarone is a registered trademark of Sanofi
Page 57 of 91

Physician Certification Course for the STAR S4 Excimer Laser System
13
Warnings•PRK is not recommended in patients who have:
•Diabetes
•A history of Herpes simplex or Herpes zoster keratitis
• Significant dry eye that is unresponsive to treatment
• Severe allergies
14
•ELECTROMAGNETIC FIELD (EMF): The thyratron emits an electromagnetic pulse which is shielded by the metal coverings of the STAR S4 IR Excimer Laser System. This metal covering reduces the EMF below the limits set by applicable standards for electromagnetic compliance.
•WARNING: The effects of electromagnetic emissions from the excimer laser system on other devices, such as cardiac pacemakers or implanted defibrillators, are unknown.
•Operation of the laser in proximity to such devices is not recommended.
Warnings
15
•The safety and effectiveness of the STAR S4 IRExcimer Laser System has not been established in:
• Patients with corneal neovascularization within 1.0 mm of the ablation zone
• PRK patients under the age of 21 years• With the exception of
• PRK patients who are 18 years of age or older for the treatment of spherical myopia up to ‐6.00D
Precautions
Page 58 of 91

Physician Certification Course for the STAR S4 Excimer Laser System
16
•The safety and effectiveness of the STAR S4 IR Excimer Laser System for LASIK correction have not been established in patients with:
• Progressive myopia, hyperopia or astigmatism• Ocular disease, corneal abnormality, previous corneal or intraocular surgery, or trauma in the ablation zone
• A history of glaucoma• Residual corneal thickness < 250 microns at the completion of the ablation
• The medication Sumatriptan (Imitrex®)
Precautions
Imitrex is a registered trademark of GlaxoSmithKline
17
•To avoid corneal ectasia, the posterior 250 microns of the corneal stroma should not be violated by the laser or the microkeratome
•Patient pachymetery – (Non–nomogram adjusted depth of treatment + flap thickness) = >250
microns
Precautions
18
•Prospective patients, as soon as they express an interest in laser vision correction and prior to undergoing surgery, must receive from the treatment provider the Patient Information Booklet.
•Prior to undergoing surgery, prospective patients must be informed of the alternatives for correcting their refractive error including eyeglasses, contact lenses, and other refractive surgeries.
•All surgeons should read the Professional Use Information prior to performing procedures with the STAR S4 IR Excimer Laser system.
Patient Information Booklet and Professional Use Information
Page 59 of 91

Physician Certification Course for the STAR S4 Excimer Laser System
19
•Abbott Medical Optics, as a medical device manufacturer, and Device User Facilities are required by law to report any of the following events (MDR = Medical Device Reporting):
• Serious Injury or Death
• Permanent impairment of a body function
• An injury that necessitates medical or surgical intervention by a health care professional
• A malfunction occurred that if it were to reoccur may likely cause or contribute to death or serious injury
•Device User Facilities are defined as a hospital, an ambulatory surgical facility, a nursing home, an outpatient treatment facility, or an outpatient diagnostic facility which is not a physician’s office.
FDA Reporting Requirement MDR Program
20
•In addition to the MDR Report that Abbott is required to file, users are encouraged to file:
•Voluntary MedWatch Reporting for Patients, Health Professionals and Consumers (Form FDA 3500)
•MedWatcher mobile app that allows individuals to submit voluntary reports of serious medical device problems to the FDA using a smart phone or tablet.
•For Questions about Medical Device Reporting, including interpretation of MDR policy:
•Call: (301) 796‐6670 •Email: [email protected]
FDA Reporting Requirements MedWatch Program
21
Pre‐Operative Evaluation
Page 60 of 91

Physician Certification Course for the STAR S4 Excimer Laser System
22
•Baseline evaluation of patients requesting Conventional treatments should be performed within 30 days of laser refractive surgery
Pre‐Operative Examination
23
• Soft lenses ‐ discontinue lens wear at least two weeks prior to examination and treatment
• Hard (PMMA) or RGP lenses ‐ discontinue lens wear at least three weeks prior to examination and treatment with stable topography (keratometry) and refraction
• 3 topographic maps (central keratometry readings) and MR taken at 1 week intervals. The last two readings must not differ by > 0.5D
Discontinuance of Contact Lenses
24
Discontinuance of Contact Lenses
•Contact lenses cause: •Reversible corneal topographic changes•Alterations in corneal thickness
•Contact lenses must be discontinued prior to refractive evaluation to allow these reversible corneal changes to resolve
Page 61 of 91

Physician Certification Course for the STAR S4 Excimer Laser System
25
Sequence of Pre‐Op ExamCustomVue Treatments
• Manifest Refraction
• Keratometry
• Corneal Topography
• SLE/Tonometry/Pachymetry
• Cycloplegic Refraction
• DFE
• Post‐Cycloplegic Refraction if necessary
26
• Uncorrected Visual AcuityManifest Refraction
• Myopia ‐ resolution based, not contrast based end point of refraction
• Least minus to see most letters
• Astigmatism ‐ Jackson Cross Cylinder ‐ maximize magnitude of cylinder
• Hyperopia ‐ Pushed Plus technique
• Best Spectacle Corrected Visual Acuity• Do not stop at 20/20
Pre‐Operative Exam
27
•Refractive, keratometric and topographic cylinder occasionally do not match in axis or magnitude
•Treatment is based on the Manifest cylinder
•When a disparity occurs, proceed cautiously and ascertain stability by repeated measurements over time
Astigmatism
Page 62 of 91

Physician Certification Course for the STAR S4 Excimer Laser System
28
•Cycloplegic Refraction (1% cyclopentolate)
•True cycloplegia reduces accommodation and allows evaluation of:
an over‐minused myope
maximum hyperopia (manifest and latent)
•Only refine the sphere during the cycloplegic refraction
Cycloplegic Refraction
29
•Keratometry is required
•Manual K’s are preferred
•Auto K’s are acceptable
•Simulated Topography K’s (Sim K) are sub‐optimal
•K1 = flat K
•K2 = steep K
•K2 Axis= axis of steep K
Keratometry
30
•Pupillometry:
•Bright and dim illumination measurement
•Corneal Topography ‐ necessary in all patients:
•R/O keratoconus or any other abnormality
•R/O CL related abnormalities
•Verify post‐operative results
Pre‐Operative Examination
Page 63 of 91

Physician Certification Course for the STAR S4 Excimer Laser System
31
• Slit Lamp Exam
• Tonometry
• Pachymetry
•Ultrasonic pachymetry required for PRK
• Dilated Media and Fundus Exam
Pre‐Operative Examination
32
•There must be at least 250 microns of stroma remaining following the ablation to reduce the likelihood of iatrogenic keratoectasia
Residual Posterior Stroma
33
•The ablation depth should be based on the actual depth of the non‐nomogram adjusted desired correction as this is indicative of the amount of tissue that is effectively removed
Residual Posterior Stroma
Page 64 of 91

Physician Certification Course for the STAR S4 Excimer Laser System
34
STAR S4 IR Excimer Laser System Hardware Overview
•Emergency StopButton
35
Laser SafetyKnow where the EMERGENCY STOP button is located
36
•The Premix cylinder contains Argon and Fluorine (toxic)
•The laser operating voltage ranges from 25,000 to 32,000 volts
•Never operate the laser in the presence of flammable anesthetics or other volatile substances such as alcohol
•Nominal hazard zone is 40 cm
Laser Safety
Page 65 of 91

Physician Certification Course for the STAR S4 Excimer Laser System
37
As ozone builds up it decreases the amount of energy that passes through the optical pathway
Ozone compensation increases energy stability
To assess the required ozone compensation, the laser system will fire ten internal pulses prior to the treatment
Ozone Compensation
38
• VSS is used in the Blend Zone (if selected) during conventional treatments
• Combines advantages of larger and smaller diameter beams
• Creates a smooth ablation
Variable Spot Scanning (VSS)
39
User can vary Repetition Rate from 1.5 to 10 Hz
Conventional Repetition Rate
Page 66 of 91

Physician Certification Course for the STAR S4 Excimer Laser System
40
•During clinical trials for Conventional ablations the environmental conditions were controlled as follows:
•Temperature ranged from 60 to 80º F
•Relative humidity ranged from 35% to 65%
Environmental Conditions
41
Patient Alignment
• When the patient is positioned in the patient chair, align the patient’s head perpendicular to the system with the fiducial line
Fiducial Line Button
Fiducial Line
42
• Wild Leica™ Microscope
Variable Magnification
• 0.63x
• 1.0x
• 1.6x
• 2.5x
• 4.0x
• All treatments should be performed at 1.6x magnification
Microscope
Page 67 of 91

Physician Certification Course for the STAR S4 Excimer Laser System
43Doctor’s Keypad
IR Button
Fiducial Line
Doctor’s Keypad
ActiveTrak Button
44
•Joystick controls the position of the Patient Chair•The microscope does not move
Joystick
45
VisionKey Cards• Purchased from Abbott Medical Optics
• Allow use of the STAR S4 IR Excimer Laser
Are laser specific
• There are different VisionKey Cards for:
• Conventional Ablations
• CustomVue Ablations
• CustomVue Retreatments
• PreVue Lenses
• Phototherapeutic Keratectomy (separate certification course)
Page 68 of 91

Physician Certification Course for the STAR S4 Excimer Laser System
46
•Automatic OD/OS pre‐positioning
•Automatic “Y” centering button
•Pillow evacuation button
Patient Chair
47
•Ring Illumination ‐ allows visualization of stromal surface
•Oblique Illumination ‐ allows visualization of iris and pupil
Ring Illumination
Oblique Illumination
Operative Illumination
48
•Use the lowest level of illumination possible to
•Allow patient comfort
•Help with patient fixation on the flashing fixation target
Operative Illumination
Page 69 of 91

Physician Certification Course for the STAR S4 Excimer Laser System
49
• Reticle is projected into each ocular
• Reticle can be turned off during
• Epithelial Removal
• The Reticle must be on to proceed with the ablation
• Reticle brightness can be adjusted
• Reticle Dimensions (independent of magnification)
• Inner Ring 4mm
• Middle Ring 6mm
• Outer Ring 9mm
Reticle
50
• Aspirator can be moved out of position to allow
• Removal of corneal epithelium
• The Aspirator must be in the proper position to proceed with the ablation
• AIRBORNE CONTAMINANTS: Airborne contaminants which are produced by the ablation process are captured in proximity to the cornea near the point of production and fed into anaspirator with a filter. This aspirator is designed to prevent any of the products of ablation from contaminating the surgical suite.
Aspirator
51
•Laser Footswitch has two positions
• First position activates the aspirator
• Second position activates the laser
Laser Footswitch
Page 70 of 91

Physician Certification Course for the STAR S4 Excimer Laser System
52
ActiveTrak Eye Tracking System
53
ActiveTrak Eye Tracking SystemThe ActiveTrak System should be used during Conventional Procedures
54
• Directs the laser beam to compensate for eye movements
• 3D infrared eye tracker
• Side‐mounted infrared cameras monitor x, y, and z (up and down) motion
ActiveTrak Eye Tracking System
Page 71 of 91

Physician Certification Course for the STAR S4 Excimer Laser System
55
•Side‐mounted, infrared cameras monitor x, y, and z movements
•Oblique IR lighting does not interfere with procedure
ActiveTrak Eye Tracking System
56
ActiveTrak Eye Tracking System
57
•The surgeon can choose to set the treatment center manually or use the automatic centering mode.
•If using automatic centering, the ActiveTrak System will locate the pupil and set the treatment center.
Automatic Centering should always be used
ActiveTrak Eye Tracking System
Page 72 of 91

Physician Certification Course for the STAR S4 Excimer Laser System
58
ActiveTrak Use•Press ActiveTrak Button on Doctor’s Keypad
•The entire reticle will begin flashing
•The ActiveTrak Eye Tracking System will locate the pupil and set the treatment center
59
• Once the pupil is located, the outside ring on the reticle will stop flashing
• Once the treatment center is set, the center cross of the reticle will flash slowly
• The ActiveTrak System will maintain this position throughout the treatment
ActiveTrak Use
60
• Fully depress the laser footswitch to begin the treatment
• The center cross of the reticle will flash slowly during the treatment when the ActiveTrak System is on and tracking the pupil
• When the ActiveTrak System is activated, you may use the joystick to correct for head motion during the treatment
• Do NOT use the joystick to correct for eye rotation when the eye tracker is activated
ActiveTrak Use
Page 73 of 91

Physician Certification Course for the STAR S4 Excimer Laser System
61
•Treatment will stop or pause when the ActiveTrak System detects the following conditions:
• The patient’s eye moves more than 1.5 mm from the treatment center (the initial position from which the ActiveTrak System begins tracking).
• The vertical position (z axis) of the corneal surface moves more than 2.0 mm from theinitial treatment position.
• The pupil diameter is not circular to within 32% or becomes smaller than 1.5 mm orlarger than 6.0 mm during treatment.
• Eye motion exceeds 0.2 mm between video frames.
• Dark objects or reflective objects are in the ActiveTrak System’s field of view.
• Surgical instruments or the surgeon’s hands cross the ActiveTrak System’s field of view.
ActiveTrak Use
62
•Use the lowest level of illumination possible to
•Allow patient comfort
•Help with patient fixation on the flashing fixation target
Operative Illumination
63
•Change the illumination as little as possible or preferably not at all after the ActiveTrak System has been engaged.
•If illumination is changed after engaging the ActiveTrakSystem, consider restarting the ActiveTrak System
Optimal Surgical Environment
Page 74 of 91

Physician Certification Course for the STAR S4 Excimer Laser System
64
•Procedure should be performed at magnification 16x (the microscope dial may read 16 or 1.6, depending on the system microscope model)
Microscope Magnification
65
STAR S4 IRExcimer Laser System Calibration
66
•Complete calibration is required each day when the system is powered up
•Abbott Medical Optics requires that a –4.00 D sphere calibration be performed after every third ocular treatment
System Calibration Requirements
Page 75 of 91

Physician Certification Course for the STAR S4 Excimer Laser System
67
•Fluence calibration adjusts the laser system energy to maintain a targetfluence of 160 mJ/cm2.
•Fluence calibration is performed:
• at system startup
• before each patient treatment procedure (or before each eye depending on selected default)
• any time the operator selects SET FLUENCE on the Lens Calibration screen
Fluence Calibration
68
•Calibration Platform with Calibration Plastic
System Calibration
69
Myopic Sphere
Myopic Cylinder
Flat/Block
Flat
Hyperopic Sphere
Centering
Lens Calibration
Page 76 of 91

Physician Certification Course for the STAR S4 Excimer Laser System
70
ActiveTrak System Calibration in conjunctionwith Beam Centering required
• The ActiveTrak System Calibration and Beam Centering are accessed on the Lens Calibration screen by selecting “Centering”.
• The ActiveTrak System aligns the treatment center as defined by the eye tracker in relation to the laser beam. Beam centering, done in conjunction with the ActiveTrak System calibration, aligns the reticle in relation to the laser beam. This test ablation must be done as a part of the daily calibration procedure.
Lens Calibration
71
•Check the laser beam/reticle alignment
Reticle adjustment knobs
Reticle Alignment
72
Calibration Plastic
Page 77 of 91

Physician Certification Course for the STAR S4 Excimer Laser System
73
STAR Excimer Laser SystemConventional AblationDimensions & Shapes
74
•Spherical Myopia
• Standard Zone 6.0 mm
• Larger Zone 6.5 mm
•Myopic Astigmatism (Ellipse)
• Standard Zone 6.0 x 4.5 mm (minimum minor axis)
• Larger Zone 6.5 x 5.0 mm (minimum minor axis)
Ablation Dimensions & Shapes
75
Myopic Astigmatism
•The width of the ellipse is determined by the relationship between sphere and cylinder
• For any given sphere, the less the cylinder the larger the minor axis
•Larger Zone treatment depth is 15‐20% more than Standard Zone
Page 78 of 91

Physician Certification Course for the STAR S4 Excimer Laser System
76
Used in combination with Myopic/Myopic Astigmatic Ablation
Can be used with Standard or Larger Zone treatment
Last diopter of spherical myopia is treated at 8.0 mm diameter
Must have at least one diopter of spherical myopia at the corneal plane
Ablation Dimensions & ShapesBlend zone
77
1.0 mm 1.0 mm
Ablation Diameter
Blend ZoneBlend Zone
8.0 mm
Blend Zone Option with VSS Treatment Profile
Creates gradual slope from optical zone to un‐ablated cornea
78
•Last ‐1.00 D is treated at 8.0 mm
•e.g. ‐6.00 D with Larger Zone and Blend Zone Option Selected
‐ 5.00 D at 6.5 mm
‐1.00 D at 8.0 mm
Blend Zone Option with VSSHow Does it Work?
Page 79 of 91

Physician Certification Course for the STAR S4 Excimer Laser System
79
Myopia/Astigmatism Treatment Screen
80
•Desired Correction Field
• Enter amount of myopia and astigmatism to be eliminated during the treatment
• Enter axis of astigmatism
• Enter vertex distance
• Enter K’s if not previously entered • (K’s affect the number of pulses delivered to cornea)
Myopia/Astigmatism Treatment Screen
81
•A value must be entered in the astigmatism field even if it is zero
•Results Field
•Summarizes pulse rate, depth and number of pulses
Myopia/Astigmatism Treatment Screen
Page 80 of 91
Physician Certification Course for the STAR S4 Excimer Laser System
82
•The computer will accept a plus cylinder manifest refraction or a minus cylinder manifest refraction in the desired correction field at the spectacle plane
•NOTE: The final treatment is corrected for the refractive error at the corneal plane expressed in minus cylinder
Myopia with Astigmatism Desired Correction Field
83
Treatment Algorithms Myopia
•< 6.00 D Single Zone• 6.0 mm(Standard)
• 6.5 mm(Larger)
•> 6.00 D to <12.00 D Multi‐zone
• 6.0/6.5 mm
• 5.5 mm diameter
•> 12.00 D Multi‐zone
• 6.0/6.5mm
• 5.5mm
• 5.0mm
84
•Hyperopia
•Ablation Diameter 9.0 mm
•Correction Diameter 5.0 mm
Ablation Dimensions & Shapes
Page 81 of 91

Physician Certification Course for the STAR S4 Excimer Laser System
85
Hyperopia/Astigmatism Ablation Profile
•In order to produce a steeper central cornea, the peripheral cornea is flattened
•Astigmatism is corrected by differentially steepening the flat axis
•An eccentrically rotating lens in the hyperopia module displaces laser beam out to 9 mm
•Slit blades shape laser beam to rectangular scanning slit b
86
• The ablation extends out to 9.0 mm
• The zone of deepest treatment is at approximately 5 mm
• Ablation depth at 5 mm is ~ 8 microns/diopter
0.8 mm
Optical zone ‐ 5 to 6 mm
Ablated area ‐ 9.0 mm
Transition zone
Hyperopia Ablation Profile
87
Hyperopia/Astigmatism Treatment Screen
Page 82 of 91

Physician Certification Course for the STAR S4 Excimer Laser System
88
•All U.S. clinical trials were conducted at 9 mm total diameter and 5 mm diameter zone of correction
•Always verify pupil diameter in bright and dim illumination before treatment
Hyperopia/Astigmatism Ablation Diameters
89
Mixed Astigmatism Cross Cylinder Ablation
Cylindrical Steepening with Cylindrical Flattening
Example: ‐1.00 +3.00 x 090
Hyperopic Cylinder Surface Power
+2.00 x 090
Myopic Cylinder Surface Power
‐1.00 x 180
90
Initial Surgical Recommendations
Page 83 of 91

Physician Certification Course for the STAR S4 Excimer Laser System
91
Initial Surgical Recommendations
•“Everything that goes on in and around the laser room is the responsibility of the
operating surgeon !!!”
92
STAR S4 IR Excimer Laser System Nomogram Recommendations
93
WARNING
•The following nomogram recommendations serve as a guideline for Conventional
Page 84 of 91

Physician Certification Course for the STAR S4 Excimer Laser System
94
•The following nomogram recommendations are made based on adherence to the refraction techniques, treatment dimensions, surgical techniques and environmental conditions discussed in this course
WARNING
95
• Nomograms developed for other laser systems CANNOT be used with the STAR S4 IR Excimer Laser System
• Nomograms for Conventional and CustomVue procedures are different
Nomogram Warning
Recommended Initial Nomogram Adjustments Conventional LASIK for Myopia
•Most surgeons program a reduction in desired correction relative to manifest refraction by 5 to 20% depending on•Refractive Error•Age• Temperature •Humidity• Elevation
96
Page 85 of 91

Physician Certification Course for the STAR S4 Excimer Laser System
Recommended Initial Nomogram forHyperopic LASIK Based on FDA Clinical Study
• Based on the patient’s age, the surgeon should apply this adjustment to the spherical portion of the manifest refraction (in this study no adjustment was made to cylinder) before entering it into the desired correction field on the S4 IR laser using the following guidelines:
• 35 years and under + 7% (107% total)
• 36 to 50 years + 5% (105% total)
• 51 to 65 years + 3% (103% total)
• Over 65 years + 2% (102% total)
• For all study treatments, the mean room temperature and humidity was 70°F ±3.6°F and 43.4% ± 6.4%.
• Although a direct cause and effect relationship between room humidity and refractive outcome cannot be determined from this study, there is some evidence (p = 0.019) that lower humidity produces better outcomes (MRSE ± 0.50D).
• The study supporting this indication (hyperopia with or without astigmatism) used the Hansatome®* Microkeratome for all treatments.
97
Recommended Initial Nomogram Conventional LASIK Mixed Astigmatism
Provided the manifest and cycloplegic refractions are within + 0.75D, program manifest refraction in desired correction field
98
Recommended Nomogram Conventional PRKMyopia and Hyperopia
•Program the manifest refraction in the desired correction field
99
Page 86 of 91

Physician Certification Course for the STAR S4 Excimer Laser System
100
Treatment Preferences Page
101
•Any default can be overwritten
•Surgeon MUST verify all data in every field in every screen
STAR Excimer Laser SystemSystem Software
102
Patient Manager Patient Information Screen
Page 87 of 91

Physician Certification Course for the STAR S4 Excimer Laser System
103
Select Treatment Button
104
AndYellow bar on bottom left of screen says“ No manifest refraction”
Pre‐Operative Examination ScreenRefractive Warnings
105
Operative Parameters Screen
Page 88 of 91

Physician Certification Course for the STAR S4 Excimer Laser System
106
Epithelium removal is for information on the Operative Report Only ‐ Does Not Control Treatment
Notes Screen
107
Epithelium Removal Screen
108
Treatment Button
Treat Button can only be selected from treatment screens
Page 89 of 91

Physician Certification Course for the STAR S4 Excimer Laser System
109
Treatment Summary Screen
Steps in Conventional LASIK and PRK Procedures
• Program Desired Correction on the S4 IR Excimer Laser system
• Verify correct treatment parameters
• Verify Repetition Rate on Operative Parameters screen
• Set microscope magnification to 1.6x
• Adjust Ring and Oblique illumination
• Adjust Reticle illumination
110
Steps in Conventional LASIK and PRK Procedures
• Create flap (if LASIK)• Properly Position Patient under S4 IR Excimer Laser system
• Perform Fluence check
• Elevate flap or remove corneal epithelium
• Focus on exposed anterior stromal surface
• Center Reticle over pupil
• Engage ActiveTrak system
111
Page 90 of 91

Physician Certification Course for the STAR S4 Excimer Laser System
Steps in Conventional LASIK and PRK Procedures
•Depress Footswitch•Deliver treatment
• Only Interrupt treatment to remove fluid on the exposed anterior stromal surface or if patient moves head
•Replace flap
112
113
©2014 Abbott Medical Optics Inc. Advanced CustomVue, CustomVue, STAR, STAR S4 IR, WaveScan, WaveScan Wavefront, ActiveTrak, and VSS are trademarks owned by or licensed to Abbott Laboratories, its subsidiaries or affiliates. Accutane is a registered trademark of Hoffman‐La Roche, Inc. Cordarone is a registered trademark of Sanofi. Imitrex is a registered trademark of GlaxoSmithKline.
Page 91 of 91