continuing professional education certificate of attendance … · 2017-12-08 · overfed....
TRANSCRIPT
Continuing Professional Education Certificate of Attendance ‐Attendee Copy‐
Participant Name:
Registration Number:
Activity Title:
Activity Number:
Date Completed: Number of CPEUs Awarded:
*Learning Need Code(s): CPE Level:
Provider Code:
Provider Signature RETAIN ORIGINAL COPY FOR YOUR RECORDS *Refer to your Professional Development Portfolio Learning Needs Assessment Form (Step 2)
Continuing Professional Education Certificate of Attendance ‐Licensure Copy‐
Participant Name:
Registration Number:
Activity Title:
Activity Number:
Date Completed: Number of CPEUs Awarded:
*Learning Need Code(s): CPE Level:
Provider Code:
Provider Signature RETAIN ORIGINAL COPY FOR YOUR RECORDS *Refer to your Professional Development Portfolio Learning Needs Assessment Form (Step 2)
16274
16274

Overfed. Undernourished. Pre-Conference Event
Wednesday, April 20, 2016 Red Lion Hotel, Pocatello, ID
MEET OUR SPEAKERS
Lisa Mays is the Nutrition Services Manager of the Idaho Foodbank, where she oversees the Cooking Matters, Backpack, Picnic in the Park, and School Pantry programs. She is devoted to providing food-insecure families with nutritious food and the skills they need to make healthier choices. She completed her Master’s in Public Health in a coordinated dietetics program at the University of Minnesota in Minneapolis, where she researched strategies to improve food pantry outreach to low-income persons, as well as associations between retail characteristics and WIC fruit and vegetable voucher redemption. She received a BS in nutrition from North Carolina State University, and worked as the Summer Food Service Coordinator for the Food Bank of Central & Eastern North Carolina while working towards this degree. Prior to returning to school to pursue a career in public health nutrition, Lisa worked in advertising, marketing, and sales.
Dr. Susan L. Johnson is Professor and Early Childhood Nutritionist in the Section of Nutrition, Department of Pediatrics, CU Anschutz Medical Campus. Dr. Johnson’s primary focus is research related to factors that influence the development of children’s food intake and eating patterns. She conducts research that centers on how child-feeding practices, both at home and in child care, impact children’s food preferences, their energy intake patterns and their weight outcome.
Julie Harker Buck is employed as an Assistant Professor at the University of Idaho Extension in Bannock county. As the Family and Consumer Sciences Educator, she specializes in health, nutrition and food safety. She is a registered dietitian with a Master in Health Education from Idaho State University and a Doctor of Education from University of Idaho. Research includes "Fruit and vegetable consumption as a predictor of weight in children" and "Instructor Influence on Self-efficacy in Women with Gestational Diabetes Mellitus". As the District IV administrator for Eat Smart Idaho, she manages the nutrition education to persons with low resources in eight southeast Idaho counties. She is a Lamaze certified childbirth educator, and birth and postpartum Doula (childbirth services).

Idaho Academy of Nutrition & Dietetics Annual Meeting
Thursday, April 21 –
Friday, April 22, 2016 Red Lion Hotel, Pocatello, ID
MEET OUR SPEAKERS
Barbara J. Mayfield is a nutrition educator and communicator specializing in helping children and families build healthy relationships with food and each other. Barb has worked directly with families as an early intervention nutrition specialist with Indiana’s First Steps Program, and spent 20 years with the WIC Program. She develops nutrition education resources, and consults, writes, and speaks to nutritionists and educators across the country about nutrition education. She has published nutrition curricula for preschoolers, early elementary, high school, college, and professional audiences. As a faculty member in the Nutrition Science Department at Purdue University, Barb teaches courses in Nutrition Communication, Dietary Guidance, Life Cycle Nutrition, and Public Health Nutrition. She directs the Promoting Family Meals Project through Purdue’s Center for Families. Her educational background includes a B.S. in Dietetics from Purdue University and an M.S. in Human Nutrition from Cornell University. She has received the Recognized Young Dietitian of the Year Award from the Academy of Nutrition and Dietetics, and the Outstanding Young Professional Award from the Purdue University Alumni Association. She has been nicknamed "The Singing Dietitian" for her unusual approach to teaching nutrition through the medium of music.
Dr. Joe Kuhl received his Bachelor of Science from Iowa State University, and Master of Science and PhD from University of Wisconsin - Madison. He conducted post-doctoral research at the Boyce Thompson Institute for Plant Research (Cornell University) and Michigan State University. He was employed by the USDA, Agricultural Research Service as a Research Geneticist from 2005-2009 in Palmer, Alaska. In 2009 he joined the University of Idaho as an Assistant Professor of Plant Molecular Genetics. Over the years he has conducted research on wheat, maize, asparagus, onion/garlic, rhubarb, tufted hairgrass, Arabidopsis thaliana and wild Solanum species.
Robert E. Ward received his BA from the University of Vermont and MS and PhDs from the University of California, Davis. Dr. Ward started in the Department of Nutrition, Dietetics and Food Sciences at Utah State University in 2005 and is currently an Associate Professor and Head of the Food Science program. Dr. Ward teaches courses in food chemistry and his research interest involves investigating the intersection between food chemistry and nutrition. More specifically, Dr. Ward focuses on polyunsaturated fatty acids and inflammation, milk bioactives and gut health.
Nancy Kure is a dietitian nutritionist and certified diabetes educator. She graduated from Washington State University in 1981. She has been the director of clinical nutrition, diabetes and food service, at Gritman Medical Hospital in Moscow, Idaho for 32 years. She started the first Diabetes Prevention Program in Moscow, in May of 2015.
Cynthia Curl earned her PhD in Environmental and Occupational Health Sciences from the University of Washington in 2014 and her MS from the same program in 2000. Dr. Curl has been an Assistant Professor in the Department of Community and Environmental Health at Boise State University since January of 2015. Her research focuses on understanding exposures to agricultural chemicals and their effects on farmworkers, agricultural communities, and the general public. She has authored numerous peer-reviewed publications on this topic, describing studies of the effectiveness of various agricultural re-entry periods on worker exposures, research on the "take-home" pathway of exposure on families of agricultural workers, and investigations of the effect of organic diets on pesticide exposures to the general public.
Lauren Heising, Registered Dietitian Nutritionist, worked at the University of Colorado within Housing & Dining Services for over 27 years. Through her work with individual student customers over the years, she saw more and more issues with food allergies and avoidances and realized a comprehensive program would need to be developed within Dining Services. Twelve years ago, the A9 Allergen Project was born. Through careful planning, implementation and continuous improvement, what is now known as A9 Identified, has been able to and continues to meet the needs of most customers with food allergies, intolerances and sensitivities.

Natalie Christensen currently holds the position of Sports Dietitian for Idaho State University. As a former athlete and graduate of ISU, she has been able to reach out to athletes, trainers, coaches, and administrators to educate them on the impact of nutrition in competitive performance. She provides nutrition education in a variety of settings: team talks, cooking classes, grocery store tours and one-on-one counseling. Natalie loves guiding athletes through such challenges as diet restrictions, IBS, fatigue, chronic injuries, weight gain, weight loss, body image concerns, and lack of time, money, or cooking skills. Natalie’s original work as a dietitian was in specialized long-term care settings, where she learned the importance of nutrition counseling, diabetes education, specialized menu planning and food systems management. Natalie is a graduate of Idaho State University with a BS degree. She and her husband are happy parents of five children who all enjoy sports, hiking, camping, and travelling.
Chef Robert Mattoch started his career working in his school kitchen washing dishes. From that first job, Chef Rob discovered his passion for cooking and continued on to complete degrees at both the Culinary Institute of America and Johnson and Wales University. He is a great communicator, and has gained vast experience working with chefs across the country. Chef Rob now helps a nonprofit, Live Well, that provides culinary training to public schools throughout the state of Colorado. Rob also travels the country training staffs in use of kitchen equipment, and the integration of cutting edge technology into their operations.
Michele H. Smith has been a nutrition support dietitian for over 20 years, earning her Certification in Nutrition Support in 1995, and maintaining this credential to present. She started her career in pediatrics at Primary Children's Hospital in Salt Lake City, specializing in TPN and tube feeding management of infants and children. After several years she moved into the adult population, working in the critical care and bone marrow transplant units at LDS hospital. Michele took the knowledge that she had acquired working with nutrition support in pediatrics and adults into the home infusion realm about 15 years ago where she has managed hundreds of TPN and tube feeding patients in the home. She has worked extensively with short bowel syndrome patients of every age and severity. Michele currently works as an Area Nutrition Manager for Coram CVS Specialty Infusion, managing and training nutrition support dietitians, and speaking to health care providers on nutrition support related topics.
Pamela Jett has had a life-long romance with words and their effect on human relationships. As a sought after keynote speaker, trainer, and coach, Pamela provides audiences worldwide with remarkable communication tools for success. After pursuing her Phd in Communication, spending time in prison (as a movie extra), and working as a university professor, Pamela decided to combine her love of the stage with her love of words and share her message of powerful communication with audiences worldwide. Audiences rave about Pamela’s high energy, her witty humor, and her practical tools for success.

Sue Linja is a Registered Dietitian Nutritionist specializing in geriatric nutrition. She is the co-founder and officer of three (3) nutrition corporations that provide consultative nutrition services to over 125 entities - nursing homes, hospitals, residential care facilities, and private health and wellness businesses. Sue has spent the past 25 years of her nutrition career working with those living the later years of their lives, both individuals in pursuit of nutritional health and longevity, and those at life’s end. Nutrition and aging is her passion. A successful entrepreneur, speaker, and published author, Sue’s most recent focus has been on studying the foods, dietary habits and lifestyles of centenarians.
Dr. SeAnne Safaii Waite serves as the Associate Professor for the Coordinated Program in Dietetics at the University of Idaho and is president of Nutrition and Wellness Associates, LLC. Her research emphasis includes the dietary habits of centenarians, diabetes and social media interventions and the use of virtual technology and simulations in nutrition and dietetics education. SeAnne has published in various research journals and authored book chapters. She loves sharing nutrition information in the media, writes for three newspapers, and makes appearances on local television networks.
Barbara Gordon is a registered dietitian nutritionist and principal consultant for HealthComm Solutions. In this role, she provides nutrition counseling, develops health education resources, and conducts health research. Barbara has a special interest in women’s health. She served as an expert reviewer for the Practice Paper of the Academy of Nutrition and Dietetics: Nutrition and Women’s Health. For the U.S. Department of Health and Human Services, she wrote two chapters of the book, The Healthy Women: A Complete Guide for All Ages. Research pursuits comprise the relationship between food, nutrition, and urological conditions. Recent studies include a review of the role of polyunsaturated fatty acids in urologic inflammation, nutrition interventions for interstitial cystitis/bladder pain syndrome (IC/BPS), and the use of complementary and alternative therapies reported by individuals with IC/BPS. She was the only RDN to serve on the American Urological Association (AUA) IC/BPS Clinical Guidelines Committee (2011 and 2014), thereby, contributing to the first-ever IC/BPS treatment protocol for urologists. She regularly publishes in peer-reviewed journals and industry communiqué, as well as presenting at medical conferences.
Jennie Davis is currently a graduate student specializing in Young Child Feeding under Dr. Samantha Ramsay at the University of Idaho-Moscow. She is also in the Coordinated Program in Dietetics with an expected graduation date of May 2017. Through this program and her time working with Dr. Ramsay, she has been given many exciting research opportunities in young child feeding, which has included international travel. She hopes to use these experiences in her future dietetics career.

Mackenzie Ferrante is a master's candidate at the University of Idaho studying child feeding and nutrition under Dr. Samantha Ramsay. Mackenzie is also a student in the coordinated program in dietetics and works as a pastry chef at Nectar Restaurant and Wine Bar. She is in love with research and travel, and is looking forward to doing more of those things in the future.
Lauren Keeney is passionate about food and nutrition, wellness, and travel. She received her undergraduate degree in Nutrition and International Studies from the University of Idaho and is currently working on her masters in Family and Consumer Sciences, and completing the Coordinate Program in Dietetics. She has worked on nutrition research both nationally and internationally, and plans to continue this work in the future. Lauren has traveled through SE Asia, Taiwan, Ghana, and Uganda, and is hoping to add many more countries to the list. She loves experiencing new cultures, traditions, and foods, and doesn't plan to stop the exploration any time soon.
Samantha Worden is currently a graduate student at the University of Idaho, specializing in Child Feeding and Sports Nutrition, as well as a student in the Coordinated Program in Dietetics. She has had the opportunity to conduct research both nationally and internationally. She looks forward to continuing to pursue her degree and conduct research by representing the University of Idaho and the Idaho Academy of Nutrition and Dietetics.
Professor Ralph Baergen received his PhD from Syracuse University, and teaches medical ethics at ISU. He also chairs the university's Institutional Review Board which oversees all research conducted using human subjects. He serves on the clinical ethics committee at Portneuf Medical Center, and watches a lot of hockey games on TV.

While completing her Master's degree online, Amanda Christensen worked as a clinical dietitian for Eastern Idaho Regional Medical Center. In this capacity, Amanda helped develop a strong presence of the dietitians in the Neonatal Intensive Care Unit. She helped initiate weekly measurements and growth chart assessment and was involved in quality assurance reports that helped better track growth and feeding goals. Amanda also conducted weight loss counseling with pre and post-op bariatric patients. She acted as a preceptor of students during clinical rotations and enjoyed teaching the students about dietetics. Amanda currently teaches at Brigham Young University-Idaho. Courses taught include Essentials of Human Nutrition, Human Metabolism, Sports Nutrition and Nutrition through the Life Cycle. She is the course lead over the Essentials of Human Nutrition course, and developed and is currently the adviser of the Dietetics Society on campus. Amanda enjoys running, traveling, camping, trying new food and teaching nutrition, not only to her students, but to her four children as well.
Dr. Stephen McGary has taught classes in the areas of farm/ranch management, agribusiness operations analysis, agricultural economics, policy and trade, agricultural development, price and market analysis, global agribusiness topics, as well as different macro and micro economic courses. He has been the principle investigator on several research and consulting projects. Dr. McGary’s areas of expertise include analyses in: the econometrics of demand/supply modeling; decision theory; resource allocation/utilization; public land use policy including many different aspects of environmental impact reviews. He has worked as an advisor and consultant in public and private land use planning. He was instrumental in developing agriculture and environmental resource analysis criteria for the State of California and the Counties of Ventura, Santa Barbara and San Luis Obispo. His work has received local, state, and national recognition through project reports and presentations. The California State Department of Food and Agriculture has praised his work on two specific environmental impact review studies, adopting many of his analysis techniques and procedures. He has testified before special U.S. Senate and House Subcommittees on agricultural resource usages, water and environmental resource issues. Dr. McGary has performed research/consulting with results being presented at professional conferences and seminars.
Megan Williams is a registered and licensed dietitian/nutritionist and certified diabetes educator. She earned a Bachelors of Science in Dietetics from Brigham Young University and received a Masters of Dietetic Administration from Utah State University. Originally from Utah, Megan has had the opportunity to work with populations in Atlanta, Georgia, San Jose, California, and Moscow, Idaho before settling in Jerome, Idaho for which she notes will be “forever.” Megan runs a small American Diabetes Association recognized diabetes education program out of Shoshone Family Medical Center, the only medical provider in Lincoln County and a patient centered medical home. She loves the opportunity to work closely with providers, in a rural setting, with patients from all walks of life and different types of diabetes. Megan continues to enjoy playing basketball and volleyball. She has also learned that she has an affinity for construction work and is quite at home on heavy machinery. In her spare time Megan can be found in her yard, taking care of her young sons, or playing the banjo.
Overfed. Undernourished. Pre-Conference Event
Wednesday, April 20, 2016 Red Lion Hotel, Pocatello, ID
PRE-CONFERENCE Total CPEs: 5
10:30am Attendee Check-in 11:00am-12:00pm
1 CPE/ Level 2
Addressing Hunger, Nutrition and Health in Idaho through Nutrition and Culinary Education | Lisa Mays, RDN, MPH, Boise, Idaho This session will help you understand more about food insecurity in Idaho, its potential effects on your clients, and how organizations in our communities are working together to address hunger and health. We will discuss the challenges with providing healthy foods through assistance programs. Learning Objectives: 1. Describe food insecurity in Idaho and ways to incorporate food insecurity screening and community program referral into their nutrition care process. 2. Discuss current community nutrition education initiatives in Idaho which address food insecurity and their potential impact on nutrition and health. Suggested Learning Codes/Performance Indicators: 4010/4070/6030/6040 Suggested Performance Indicators: 7.2.6/3.3.3/9.1.1/12.1.1
12:00pm-12:45pm 1 CPE/ Level 2
Food Demo and Luncheon | Lisa Mays, RDN, MPH, Boise, Idaho Ms. Mays will perform a cooking demonstration that will highlight one of the fast, affordable, and healthy recipes currently used in The Idaho Foodbank’s Cooking Matters classes. Learning Objectives: 1. Identify recipes that can easily be made with limited resources. Suggested Learning Codes/Performance Indicators: 4020/4070/8060 Suggested Performance Indicators: 7.2.6/8.4.3/12.1.1/13.2.3/13.2.8
Register online at http://www.eatrightidaho.org/annual-meeting/ 1 | P a g e

1:00pm – 2:30pm 2 CPE/ Level 2
Perspectives on Eating Patterns of Young Children at Risk for Development of Malnutrition and Poor Growth| Susan L. Johnson, PhD, Aurora, Colorado Significant research has been reported regarding the dietary intake of young children from at-risk families. However, less research has focused on the perspectives of families and child care providers and their goals for feeding young children. If nutrition professionals are to effectively intervene with these populations, understanding the motivations and practices of these caregivers is imperative. This session will describe caregiver influences on young children's eating behaviors, including the goals, concerns and perspectives of caregivers. Learning Objectives: 1. Describe the dietary intakes of young children, with specific emphasis on at risk populations. 2. Examine the feeding practices of caregivers of young children, including motivations and concerns related to poverty and time and the perspectives of different cultures. 3. Consider the implications of caregiver perspectives and how they may influence the nutrition professional's opportunities and strategies for facilitating positive change. Suggested Learning Codes/Performance Indicators: 4070/6070/9020 Suggested Performance Indicators: 1.2.5/6.2.1/6.3.1/12.1.1
2:45pm – 3:45pm 1 CPE/ Level 2
Eat Smart Idaho: Promoting Healthy Eating and Lifestyle Changes Through Statewide Partnerships | Julie Harker Buck Ed. D., MHE, RDN, Pocatello, Idaho Chronic diseases cost Idahoans $355 million annually. University of Idaho Extension's, Eat Smart Idaho program, conducts nutrition classes and community-wide efforts, with persons who have low resources, to improve healthy food choices. This session will review evidence-based community interventions, which include partnerships with area agencies, and the resulting lifestyle improvements. Learning Objectives: 1. Review programming efforts by University of Idaho Extension Eat Smart Idaho's interventions, partnerships, monitoring and evaluation. 2. State evaluation techniques for chronic health conditions which can be influenced by nutrition programming to persons with low resources. 3. Discuss and plan community efforts to help with hunger and food insecurity in Idaho. Suggested Learning Codes/Performance Indicators: 4010/6060/4070 Suggested Performance Indicators: 3.3.4/7.2.3/7.2.4/11.4.4/12.1.1
3:45pm – 4:00pm Closing remarks
EVENT SUPPORTERS ACADEMY OF NUTRITION AND DIETETICS AFFILIATE SPEAKER GRANT
IDAHO FOODBANK IDAHO WIC PROGRAM
UNIVERSITY OF IDAHO EXTENSION BANNOCK COUNTY
Register online at http://www.eatrightidaho.org/annual-meeting/ 2 | P a g e

General Sessions
Concurrent Sessions
Exhibits & Registration Area

Solving Hunger in Idaho Lisa Mays, RD, MPH
Nutrition Services Manager, The Idaho Foodbank
(20) 695-6637
1) Participants will be able to:
a) Describe food insecurity in Idaho, its potential effects on your clients, and how organizations in our
communities are working together to address hunger and health.
b) Discuss current nutrition education initiatives in Idaho which address food insecurity and their
potential impact on nutrition and health.
2) Neighbors in Need
a) “A job loss and medical bills that insurance refused to pay left us uncertain if we could put food on the
table. There is nothing worse than the feeling of not being able to provide for your children.” Food
Recipient, The Idaho Foodbank
3) Definitions
a) Food Insecurity:
i) Low food security / Food insecurity without hunger: “Reports of reduced quality, variety, or
desirability of diet. Little or no indication of reduced food intake.”
b) Very Low Food Security:
i) Food insecurity with hunger: “Reports of multiple indications of disrupted eating patterns and
reduced food intake”
4) Who Needs Food Assistance
a) 1 in 6 Idahoans is hungry
b) 1 in 5 Idaho children under 18 years is hungry
i) This includes 90,000 children
5) National Statistics
a) 14% = Food Insecure
b) 6% = Very Low Food Security
c) More likely for:
i) With Children
ii) Single Parent
iii) African American & Hispanic/Latino
6) Food Insecurity in the Life Cycle: Pregnancy
a) Higher Risk of:
i) Iron deficiency1
ii) Pregravid obesity2,3
iii) Gestational diabetes2,3

7) Food Insecurity in the Life Cycle: Early Childhood
a) Higher Risk of:
i) Cognitive & Behavioral Difficulties4,5
ii) Anemia4,8
iii) Asthma4
iv) Tooth Decay4
v) Obesity4,7,9
8) Food Insecurity in the Life Cycle: Adolescence
a) Higher Risk of:
i) Depression & Suicidal Ideation4,5,6,7,9,10
ii) Widening Gap in Cognitive Performance with Age8
iii) Decreased calcium & folate intake10
iv) Development of Diet-Related Conditions:4,7,9
9) Food Insecurity in the Life Cycle: Adulthood
a) Higher Risk of:
i) Less Nutritious Food Choices4,10,11
ii) Cycles of Food Restriction & Overeating4,10
iii) Increased Stress, Anxiety, Depression3,4,10
iv) Obesity & Associated Conditions4,5,6,7,9,11
10) Food Insecurity in the Life Cycle: Advanced Age
a) Higher Risk of:
i) Low nutrient intake12
(1) Energy, Protein,
(2) B-vitamins, Calcium, Iron
ii) Poorer Overall Health12
iii) Limitations on Activities of Daily Life12
11) Food Insecurity in the Life Cycle: Health Conditions – Diabetes
a) Higher Risk of:
i) Poor Glucose Control13
ii) High A1C14
iii) What Have You Seen?
iv) Choices: Medications/Medical Supplies vs. Food or other essentials leads to poor disease
management

12) The Idaho Foodbank
a) Mission: To help feed, educate and advocate for Idaho’s hungry through collaborative partnerships to
develop efficient solutions that strengthen individuals, families and communities.
b) Opened in 1984 in Boise: 420, 623 distributed the first year
i) 16,100,000 distributed in fiscal year 2015
c) 3 Distribution Facilities:
i) Boise
ii) Lewiston
iii) Pocatello
d) 230 Community partners (pantries)
e) 39 out of 44 Idaho counties served
f) Donors:
i) 56% Individuals
ii) 37% Corporations & Foundations
iii) 5% Government
iv) 2% Other Organizations
g) Responsibility:
i) 94% of funding to programs and services, 6% to administration
ii) Charity Navigator 4-star rating for 5 consecutive years
h) Food donations:
i) 56% Agriculture/Manufacturing
ii) 29% Fresh Rescue
iii) 11% Purchase
iv) 4% Food Drives
i) Meals distributed from food:
i) 9.5 million in 2012
ii) 13.4 million in 2015
j) Where the food goes:
i) Emergency food pantries
ii) Senior centers
iii) Community kitchens
iv) Emergency shelters
v) Residential programs
vi) 163,679 People served each month

13) Programs that Make a Difference:
a) Backpack: Weekend Meals for School Children
i) 63,791 Backpacks distributed
ii) 1,804 Children served statewide each week
b) School Pantry: Family Meals in a Familiar Setting
i) 9,534 People served during year
ii) 150,000 Pounds of food distributed
c) Picnic in the Park (Summer Food Service Program in Boise & Garden City)
i) 48,451 Meals served from June to August
ii) 1,250 Children served, daily
d) Share Our Strength’s Cooking Matters
i) 85 Six-week classes and In-Store tours
ii) 937 Students statewide
14) Nutrition Education at The Idaho Foodbank: Cooking Matters
a) What is Cooking Matters?
i) Hands-On, Six-Week Courses
ii) Team-taught by a volunteer chef and nutrition educator
iii) Covers meal preparation, grocery shopping, food budgeting and nutrition
iv) Adult and teen participants take home a bag of groceries at the end of each class
v) Curricula:
(1) Adults
(2) Familes (Adult & Child)
(3) Parents
(4) Teens
(5) Kids
(6) Adults Extra for Diabetes
(7) Adults Extra for Wellness
b) Why Cooking Matters?
i) After a course, adult and teen graduates are:
(1) Cooking meals instead of buying take-out 15% more often
(2) Using the “Nutrition Facts” label 88% more often
(3) Making meals with at least 3 food groups 38% more often
ii) After a course, adult and teen graduates report that:
(1) 66% are eating more vegetables
(2) 67% are eating more fruits
(3) 61% are eating more whole grains
(4) 90% improved their cooking skills

iii) Testimonial from St. Luke’s Cardiac Rehab Course
(1) “It’s absolutely changed my life. It was my third birth. My first was my mother, the second was
my Lord. The third was a heart attack. It’s the difference between having a life at this point and
having nothing.”
15) Volunteers Make It Possible!
a) Volunteer Activities:
i) Sort and repack food
ii) Unload and load donations
iii) Teach cooking classes
iv) Build backpacks
v) Distribute at mobile pantries
b) 61,379 volunteer hours in Fiscal Year 2015
i) The equivalent of 26 full time jobs
c) Special Opportunities for You!
i) Teaching & Hosting Cooking Matters Classes & Tours
ii) Screening for Food Insecurity
iii) Referring to Resources in Your Community
d) Screening for Food Insecurity in Your Clinic
i) Within the past 12 months, we worried about whether our food would run out before we got
money to buy more. (Yes or No)
ii) Within the past 12 months, the food we bought just didn’t last and we didn’t have money to get
more. (Yes or No)
e) American Academy of Pediatrics Policy Statement
i) Issued October 2015
ii) Recommends Food Security Screening in all Pediatric Care Settings
16) Who to Call for More Information:
i) Partnerships:
(1) Mary Ann Liby, Agency Relations Supervisor: 794-3627
(2) Kimberly Empey, Healthcare Partnerships VISTA: 407-8059
ii) Programs for Children & Seniors:
(1) Lauren Myers, Senior Hunger VISTA: 488-5487
(2) Sam Johnson, Nutrition Services Coordinator: 809-1312
iii) Nutrition Education:
(1) Jessica Trevino, Eastern: 404-6491
(2) Elizabeth Stratton, North Central: 794-1935
(3) Kyle Silverman, Treasure Valley: 629-9473
(4) Makenzie Ellsworth, Magic Valley: 577-2724

17) More Organizations Solving Hunger in Idaho!
a) There are more organizations you can partner with, like Eat Smart, WIC, Indian Health Services, &
More!
Make hunger a priority in your nutrition care process!
References: 1. Laraia, B.A., Siega-Riz, A.M., Gunderson, C. Household Food Insecurity is Associated with Pregravid
Weight Status, Gestational Weight Gain, and Pregnancy Complications. Journal of the American Dietetic Association. 2010; 110: 692-701.
2. Park, C., Eicher-Miller, H. Iron Deficiency is Assocaited with Food Insecurity in Pregnant Females in the United States: National Health and Nutrition Examination Survey 199-2010. Journal of the American Dietetic Association. 2014; 114: 1967-1973.
3. Olson, C.M. Food Insecurity and Maternal Health during Pregnancy. Journal of the American Dietetic Association. 2010; May: 690-691.
4. Gunderson, C., Ziliak, J.P. Food Insecurity and Health Outcomes. Health Affairs. 2015; 34(11): 1830-1839
5. Children’s Healthwatch. Too Hungry to Learn: Food Insecurity and School Readiness. http://www.childrenshealthwatch.org/wp-content/uploads/toohungrytolearn_report.pdf
6. Centers for Disease Control and Prevention. Childhood Obesity Facts. http://www.cdc.gov/healthyschools/obesity/facts.htm.
7. Food Research & Action Center. Understanding the Connections: Food Insecurity and Obesity. http://frac.org/pdf/frac_brief_understanding_the_connections.pdf
8. Lozoff, B. Jimenez, E., Smith, J.B. Double Burden of Iron Deficiency in Infancy and Low Socio-Economic Status: A Longitudinal Analysis of Cognitive Test Scores to 19 Years. Arch Pediatr Adolesc Med. November 2006; 160(11): 1108-1113.
9. Kaur, J., Lamb, M., Ogden, C. The Association between Food Insecurity and Obesity in Children – The National Health and Nutrition Examination Survey. Journal of Nutrition and Dietetics. 2015; 115(5) 751-758.
10. Position of the American Dietetic Association: Child and Adolescent Food and Nutrition Programs. Journal of the American Dietetic Association. 2006; 106(9): 1467-1475.
11. Mello, J.A. et al. How Is Food Insecurity Associated with Dietary Behaviors? An Analysis with Low-Income, Ethnically Diverse Participants in a Nutrition Intervention Study. Journal of the American Dietetic Association. 2010; 11(12): 1906-1911
12. Ziliak, J.P., Gundersen, C., Haist, M. The Causes, Consequences, and Future of Senior Hunger in America. The University of Kentucky Center for Poverty Research. http://www.mowaa.org/document.doc?id=13.
13. Berkowitz, S.A., Gao, X. Tucker, K.L. Food-Insecure Dietary Patterns Are Associated with Poor Longitudinal Glycemic Control in Diabetes: Results From the Boston Puerto Rican Health Study. Diabetes Care. 2014; 37: 2587-2592.
14. Lyles, C. R. et al. Food Insecurity in Relation to Changes in Hemoglobin A1C, Self-Efficacy, and Fruit/Vegetable Intake During a Diabetes Educational Intervention. Diabetes Care. 2013; 36: 1448-1453.

AIesftiiitopphMiiahsaanadliciucpttaaatJ1
PItsf
1
from the association
Position of the American Dietetic Association: FoodInsecurity in the United Statestiiitosgvs
AUsltfwh(ficdsa
srelmUtiel(a2Ughdrtar(
hcaddnhpghbFhih
tupcLtca
mftnowfs
RUAShSfSwiHUItaf
BSTRACTt is the position of the American Di-tetic Association that systematic andustained action is needed to achieveood and nutrition security for all inhe United States. To eliminate foodnsecurity, interventions are needed,ncluding adequate funding for andncreased utilization of food and nu-rition assistance programs, inclusionf food and nutrition education in suchrograms, and innovative programs toromote and support individual andousehold economic self-sufficiency.ore than 49 million individuals living
n the United States experienced foodnsecurity in 2008. Negative nutritionnd non–nutrition-related outcomesave been associated with food in-ecurity in children, adolescents, anddults, including substandard academicchievement, inadequate intake of keyutrients, poor health, increased risk fornd development of chronic disease, poorisease management, and poor psycho-ogical and cognitive functioning. Reg-stered dietitians and dietetic techni-ians, registered, can play key rolesn ending food insecurity and areniquely positioned to make valuableontributions through provision of com-rehensive food and nutrition educa-ion; competent and collaborative prac-ice; innovative research related toccessing a safe, secure, and sustain-ble food supply; and advocacy effortst the local, state, regional, and na-ional levels.
Am Diet Assoc. 2010;110:368-1377.
OSITION STATEMENTt is the position of the American Die-etic Association that systematic andustained action is needed to achieveood and nutrition security for all in
0002-8223/$36.00
“doi: 10.1016/j.jada.2010.07.015
368 Journal of the AMERICAN DIETETIC ASSOCIATI
he United States. To eliminate foodnsecurity, interventions are needed,ncluding adequate funding for andncreased utilization of food and nu-rition assistance programs, inclusionf food and nutrition education inuch programs, and innovative pro-rams to promote and support indi-idual and household economic self-ufficiency.
ccess to food is a basic humanneed and fundamental right. Thecitizens and residents of the
nited States are its most valuable re-ource. Yet, food insecurity, that is,imited or intermittent access to nutri-ionally adequate, safe, and acceptableoods accessed in socially acceptableays (1), continues in millions ofouseholds across the United States2). In light of the negative outcomes ofood insecurity across the life course,ncluding physical impairments, psy-hological suffering, and sociofamilialisturbances (3), it is unwise and short-ighted to allow this serious, yet avoid-ble, public health issue to continue.Using a broad-based approach to
ystematically address food insecu-ity in the United States will help tonsure community food security andead to nutrition security. The Com-
unity Food Security Initiative of theS Department of Agriculture has
he goal of cutting US food insecurityn half by 2015 through creation andxpansion of partnerships that buildocal food systems and reduce hunger4). The US Department of Healthnd Human Services’ Healthy People010 initiative identified preventableS health threats and established
oals to increase quality and years ofealthful life and to eliminate healthisparities (5). One of the nutrition-elated objectives for the nation iso “increase food security [to 94%]mong US households and in so doingeduce hunger” (4). In its draft form6), Healthy People 2020 envisions a
society in which all people live long, aON © 2010
ealthy lives.” The proposed overar-hing goals of Healthy People 2020re to eliminate preventable disease,isability, injury, and prematureeath; achieve health equity, elimi-ate disparities, and improve theealth of all groups; create social andhysical environments that promoteood health for all; and promoteealthful development and healthfulehaviors across every stage of life.ood security is the linchpin ofealthful living and must be achieved
n the United States to improve theealth of its citizens and residents.Although the safety and security of
he US food and water supply are oftmost importance, another positionaper of the American Dietetic Asso-iation focuses on those issues (7).ikewise, another position paper ofhe American Dietetic Association fo-uses on world hunger, malnutrition,nd food insecurity (8).This position paper focuses on do-estic food insecurity and relates to
ood availability and food access, ratherhan food safety from a bioterrorism oratural disaster standpoint. Through-ut the paper, the term food insecurityill be used to refer to all aspects of
ood and nutrition insecurity. Figure 1ummarizes relevant terms.
ATIONALE FOR THE POSITION PAPERPDATEchieving food security in the Unitedtates is paramount to improving theealth of its citizens and residents.ince the 2006 position paper (16), the
ood security status of the Unitedtates has been further documented,ith the most recent estimates of food
nsecurity continuing to fall short of theealthy People 2010 objective (94% ofS population will be food secure) (2,5).
n addition, several studies have fur-hered our understanding of nutritionnd non–nutrition-related outcomes ofood insecurity, including overweight
nd obesity, and reinforced that foodby the American Dietetic Association
ihrewW2icgS
KFSAewHmdsshmc
vtf
●
●
●
lmvhcbe1hrd
t
●
●
●
●
rnhhaacdm
epsashtrpd(mato(ku4hsa(hdt
(sopfgw3
Fte
nsecurity is of high priority for publicealth action. Finally, food insecurityates in the United States parallel pov-rty rates (17), and food insecurityorsens in recessionary times (18).ith the poor economic conditions in
009 and 2010 in the United States, its anticipated that food security will in-rease, further emphasizing the ur-ency of this health issue in the Unitedtates.
EY POINTSood Insecurity Is Prevalent in the Unitedtatesccording to the most recent nationalstimates (2), 85.4% of US householdsere food secure throughout 2008.owever, 14.6% of households (17.1illion), representing 49.1 million in-
ividuals, experienced food insecurityometime during the year due to re-ource constraints. Of all US house-olds, 8.9% of all households (10.4illion households) had low food se-
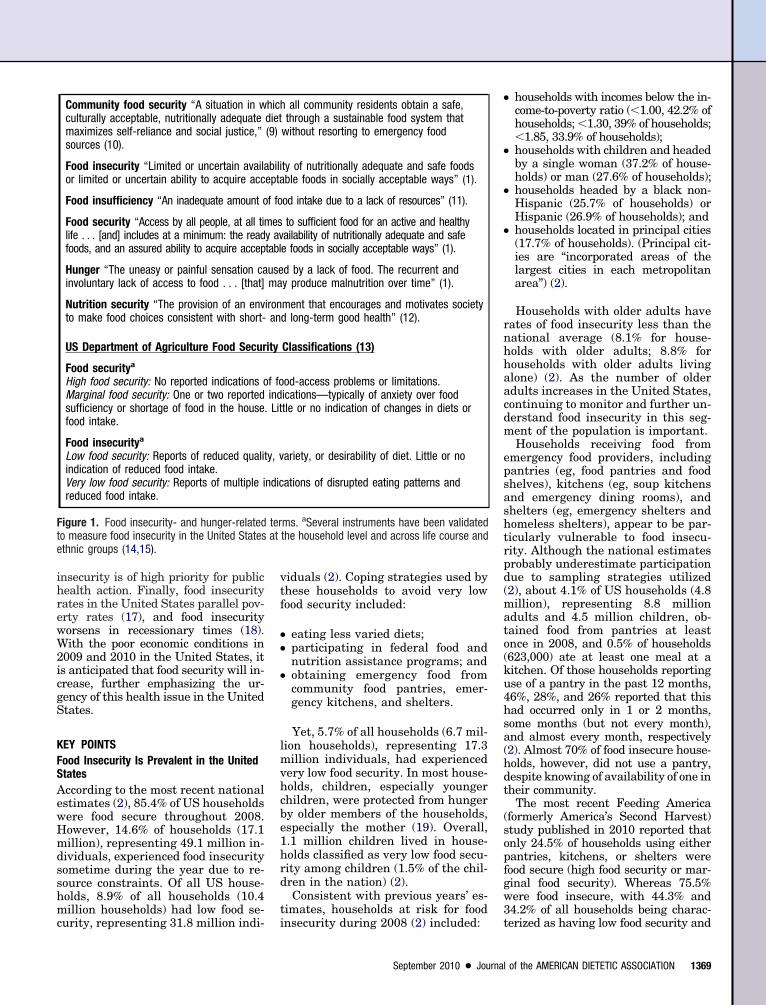
Community food security “A situation in wculturally acceptable, nutritionally adequatemaximizes self-reliance and social justice,”sources (10).
Food insecurity “Limited or uncertain availaor limited or uncertain ability to acquire acc
Food insufficiency “An inadequate amount o
Food security “Access by all people, at all timlife . . . [and] includes at a minimum: the readfoods, and an assured ability to acquire accep
Hunger “The uneasy or painful sensation cainvoluntary lack of access to food . . . [that]
Nutrition security “The provision of an envto make food choices consistent with short-
US Department of Agriculture Food Secur
Food securitya
High food security: No reported indications oMarginal food security: One or two reportedsufficiency or shortage of food in the house.food intake.
Food insecuritya
Low food security: Reports of reduced qualitindication of reduced food intake.Very low food security: Reports of multiple ireduced food intake.
igure 1. Food insecurity- and hunger-relatedo measure food insecurity in the United Statesthnic groups (14,15).
urity, representing 31.8 million indi- i
iduals (2). Coping strategies used byhese households to avoid very lowood security included:
eating less varied diets;participating in federal food andnutrition assistance programs; andobtaining emergency food fromcommunity food pantries, emer-gency kitchens, and shelters.
Yet, 5.7% of all households (6.7 mil-ion households), representing 17.3
illion individuals, had experiencedery low food security. In most house-olds, children, especially youngerhildren, were protected from hungery older members of the households,specially the mother (19). Overall,.1 million children lived in house-olds classified as very low food secu-ity among children (1.5% of the chil-ren in the nation) (2).Consistent with previous years’ es-
imates, households at risk for food
all community residents obtain a safe,through a sustainable food system that
without resorting to emergency food
ty of nutritionally adequate and safe foodsble foods in socially acceptable ways” (1).
od intake due to a lack of resources” (11).
to sufficient food for an active and healthyailability of nutritionally adequate and safee foods in socially acceptable ways” (1).
d by a lack of food. The recurrent andy produce malnutrition over time” (1).
ment that encourages and motivates societyd long-term good health” (12).
Classifications (13)
od-access problems or limitations.ications—typically of anxiety over foodtle or no indication of changes in diets or
ariety, or desirability of diet. Little or no
ations of disrupted eating patterns and
ms. aSeveral instruments have been validatedthe household level and across life course and
nsecurity during 2008 (2) included: t
September 2010 ● Journal
households with incomes below the in-come-to-poverty ratio (�1.00, 42.2% ofhouseholds; �1.30, 39% of households;�1.85, 33.9% of households);households with children and headedby a single woman (37.2% of house-holds) or man (27.6% of households);households headed by a black non-Hispanic (25.7% of households) orHispanic (26.9% of households); andhouseholds located in principal cities(17.7% of households). (Principal cit-ies are “incorporated areas of thelargest cities in each metropolitanarea”) (2).
Households with older adults haveates of food insecurity less than theational average (8.1% for house-olds with older adults; 8.8% forouseholds with older adults livinglone) (2). As the number of olderdults increases in the United States,ontinuing to monitor and further un-erstand food insecurity in this seg-ent of the population is important.Households receiving food from
mergency food providers, includingantries (eg, food pantries and foodhelves), kitchens (eg, soup kitchensnd emergency dining rooms), andhelters (eg, emergency shelters andomeless shelters), appear to be par-icularly vulnerable to food insecu-ity. Although the national estimatesrobably underestimate participationue to sampling strategies utilized2), about 4.1% of US households (4.8illion), representing 8.8 million
dults and 4.5 million children, ob-ained food from pantries at leastnce in 2008, and 0.5% of households623,000) ate at least one meal at aitchen. Of those households reportingse of a pantry in the past 12 months,6%, 28%, and 26% reported that thisad occurred only in 1 or 2 months,ome months (but not every month),nd almost every month, respectively2). Almost 70% of food insecure house-olds, however, did not use a pantry,espite knowing of availability of one inheir community.
The most recent Feeding Americaformerly America’s Second Harvest)tudy published in 2010 reported thatnly 24.5% of households using eitherantries, kitchens, or shelters wereood secure (high food security or mar-inal food security). Whereas 75.5%ere food insecure, with 44.3% and4.2% of all households being charac-
hichdiet(9)
biliepta
f fo
esy avtabl
usema
ironan
ity
f foindLit
y, v
ndic
terat
erized as having low food security and
of the AMERICAN DIETETIC ASSOCIATION 1369

v(imS
●
●
●
fucsmitiotehpdldpt
uPucesci
taN2s
isicsgfcochcAami(tlhehpgchpod
vireoggnRtcitjvnma
FNFpvt
bfpohpsdcor
●
●
●
●
●
●
tlf
Delaedgccsfido
avddlvwafcftesiu
1
ery low food security, respectively20). Similar to previous years, accord-ng to the most recent national esti-
ates of food insecurity in the Unitedtates (2):
about 31% of households using pan-tries were food secure (high food se-curity, marginal food security); yet,of those, 55% were classified as hav-ing marginal food security and were10 times as likely to have used apantry and five times as likely tohave eaten at a emergency kitchenas households classified as highfood security (those with no indica-tors of food insecurity);food pantry and emergency kitchenuse was strongly associated withfood insecurity, with food insecurehouseholds being 13 and 14 timesmore likely than their food securecounterparts to have obtained foodfrom a pantry or kitchen, respec-tively; andcompared to usage nationally (4.1%),pantry use was higher among house-holds with incomes below the povertyline (17%), with children (5.6%),headed by a single woman with chil-dren (11.5%), classified as non-His-panic black (8.1%) or Hispanic(5.7%), and located in principal cities(4.8%).
Important caveats to interpretingood security assessment measuressed for the annual estimates in-lude that questions are posed to re-pondents regarding the previous 12onths. Therefore, those experienc-
ng food insecurity any time duringhe previous year are classified as foodnsecure. Consequently, the daily ratesf food insecurity are substantially lesshan the annual rates. On average, it isstimated that 0.9% to 1.2% of house-olds (1.1 to 1.4 million households) ex-erience very low food security eachay (2). In addition, experiencing veryow food security and the associated re-uced food intake and disrupted eatingatterns appear to be episodic, ratherhan chronic, in nature (2).
The causes of food insecurity must benderstood before it can be eradicated.overty, high housing and utility costs,nemployment, medical and healthosts, mental health problems, lack ofducation, transportation costs, andubstance abuse are cited as factorsontributing to food insecurity in Amer-
can cities (21). Smoking also appears n370 September 2010 Volume 110 Number 9
o be associated with food insecurity,ccording to the National Health andutrition Examination Survey, 1999-002 (22), a nationally representativeample of households with children.
Rose (23) noted that food insecuritys often triggered by an event thattresses the household budget—los-ng a job or assistance benefits, in-luding Supplemental Nutrition As-istance Program (SNAP) benefits, oraining a household member. Overall,ood insecure households must oftenhoose between buying food and buyingr paying for other items or needs, in-luding medication (24,25), healthfulousing conditions (26), and utilityosts for heating or cooling (27,28).mong households using food pantriesnd other emergency food programs,any reported choosing between buy-
ng food and medical care/medication31.6%), rent/mortgage (35%), or utili-ies/heating (41.5%) (29). Cook and col-eagues (26) developed a measure ofousehold energy security, “access tonough of the kinds of energy needed [toeat/cool home and operate lighting/ap-liances] for a healthy and safe life in theeographic area.” Overall, household andhild food insecurity was associated withousehold energy insecurity, as well asoor health, hospitalizations, and devel-pmental risks among infants and tod-lers (26).Immediate and long-range inter-
entions targeting the causes of foodnsecurity will undoubtedly assist ineducing rates of food insecurity. Ad-quate funding for and increased usef food and nutrition assistance pro-rams, as well as innovative pro-rams to promote and support eco-omic self-sufficiency, is paramount.egistered dietitians (RDs) and die-
etic technicians, registered (DTRs),an encourage clients to access exist-ng programs providing food and nu-rition assistance, social services, andob training as an immediate inter-ention. RDs and DTRs can also part-er with key stakeholders in the com-unity to build local food systems
nd reduce hunger.
ood Insecurity Is Related to Nutrition andon-Nutrition Outcomesood insecurity is a high priority forublic health action, especially iniew of its potential negative affect onhe nation from public health and eco-
omic perspectives. As summarized by Nord and Prell (17), “it is clear thatood insecurity is part of a complex ofotentially serious health and devel-pmental conditions.” Overall, it canave grave consequences, includinghysical impairments related to in-ufficient food, psychological issuesue to lack of access to food, and so-iofamilial disturbances (3). As previ-usly reviewed (16,17), food insecu-ity is associated with:
inadequate intake of key nutrients;poor physical and mental health inadults and depression in women;overweight and weight gain (espe-cially among women from marginaland low food security households);adverse health outcomes for infantsand toddlers;behavior problems in preschool-agedchildren;lower educational achievement inkindergarteners; anddepressive disorder and suicidalsymptoms in adolescents.
The relationship of food insecurityo nutrition and non–nutrition-re-ated outcomes will be the primaryocus of this key point.
ietary Intake in Children and Adults. Sev-ral studies have demonstrated a re-ationship between food insecuritynd less-than-optimal food and nutri-nt intake, as well as risk for nutrienteficiencies among some life courseroups. Although children are typi-ally protected from very low food se-urity in the United States, evidenceuggests that food insecurity or insuf-ciency may be associated with lowerietary quality in children, especiallylder children (and adults) (30).Food insufficiency has been associ-
ted with decreased consumption ofegetables, particularly nutrient-richark green vegetables, among US chil-ren (31). In contrast, Lorson and col-eagues (32) found that total fruit andegetable intakes of all US childrenere at less than recommended levelsnd did not vary among children fromully food-secure, marginally food-se-ure, low food-secure, and very-low-ood-secure households. Compared toheir food secure counterparts, how-ver, the proportion of french fries con-umed by children and adolescents liv-ng in food insecure households madep a greater proportion of total vegeta-
le intake. Widome and colleagues (33)
fryfceairTibp
iaan(ctfnrspmodvefRfsmfToiwi
ildgrdtadfdtaDmStaeb
tgtaattitsmtclaksimigOmsnaihtccamivifrDtyaDaaCOcadtsrciVfhqcm
fb(ietcctcaamADcpt(c(camdwharoiCcshdrlrtdchstt
saphsPioaoftc
ocused on diet quality and food insecu-ity among middle and high schoolouth. They found that, compared toood secure youth, food insecure youthonsumed a greater percentage of en-rgy from fat, ate fewer family mealsnd breakfasts, had less food availabil-ty at home, and perceived greater bar-iers to eating a healthful diet (33).herefore, the authors suggested that
nterventions aimed at eliminatingarriers to healthful eating would berudent (33).Poor nutrition outcomes, including
nadequate intakes of key nutrients,mong food insecure adults and olderdults have been previously reported inationally representative samples
34,35). Olson (36) reviewed food inse-urity in women and emphasized thathe role of women in managing familyeeding makes them vulnerable to theegative consequences of food insecu-ity, with fruits and vegetables beingacrificed initially in the face of ap-roaching food insecurity. Women mayodify their dietary intake to spare
ther family members, especially chil-ren, from experiencing nutrient depri-ation (19). Nonetheless, in US adults,nergy intakes did not differ betweenood secure and food insecure adults.ather, meal and snack behaviors dif-
ered, with food insecure adults con-uming fewer (but larger) meals andore snacks, which may compensate
or the reduced meal frequency (37).his study underscores the importancef focusing on meal and snack behav-ors, rather than only total energy,hen monitoring diet quality of food
nsecure adults.The literature demonstrates that
ndividuals residing in householdsacking access to food may consumeiets deficient in particular foodroups and nutrients, increasing theisk of poor health, chronic diseaseevelopment, and other non–nutri-ion-related outcomes, if not immedi-tely, in the long term. Continuing toocument the dietary outcomes ofood insecurity is paramount, as isevelopment of appropriate interven-ions and provision of innovative foodnd nutrition education by RDs andTRs, including collaborative, com-unity-based education programs.ince gardening interventions havehe potential to enhance producevailability and intake (38,39), onexample of a potential community-
ased program is gardening educa- aion in collaboration with a masterardener or county extension educa-or to increase household producevailability. Adequate funding fornd increased use of food and nutri-ion assistance programs, includinghose providing nutrition education,s particularly important to improvehe dietary outcomes related to food in-ecurity. In addition, developing com-unity partnerships and networks
hat build local food systems are cru-ial. Examples include partnerships inocal communities with emergency foodnd feeding programs, farmers’ mar-ets, community gardens, and farm-to-chool programs. In the short term, tomprove community food security,
aximizing access to and use of exist-ng food and nutrition assistance pro-rams is vital (40).ther Nutrition and Non-Nutrition Outco-es. Collectively, the literature demon-
trates that food insecurity has negativeutrition and non-nutrition outcomesnd underscores the potential negativemplications of food insecurity on theealth of citizens and residents ofhe United States and US health careosts. Health status, chronic disease in-idence and risk, diabetes, overweightnd obesity, school performance, andental health are all related to food
nsecurity. Food insecurity is a pre-entable health threat. Therefore, it ismperative to document outcomes ofood insecurity through collaborativeesearch projects across the life course.evelopment of appropriate interven-
ions, especially for households withouth, and provision of innovative foodnd nutrition education by RDs andTRs and adequate funding for foodnd nutrition assistance programs islso vital.hild/Adolescent Health, Development, andther Outcomes. Food insecurity is asso-iated with adverse health, growth,nd development outcomes among chil-ren aged 0 to 18 years (41). In addi-ion, maternal food insecurity has beenhown to be associated with increasedisk of certain birth defects (42,43). Forhildren, food insecurity/insufficiencys associated with poor health (44-47).ery low food security among children
urther increases the odds of poorealth and is associated with more fre-uent hospitalizations among younghildren (46). Children of immigrantothers are especially prone to this neg-
tive outcome (48). Infants and toddlers r
September 2010 ● Journal
rom food insecure households have alsoeen shown to be at developmental risk49) and at risk for iron deficiency andron deficiency anemia, especially amongthnic minorities (50,51). Comparedo those from food secure households,hildren and adolescents in food inse-ure households are also more likelyo exhibit behavioral and psychologi-al problems, including suicide risk indolescents (52-56), as well as poorercademic performance and achieve-ent (52,57).
dult Health and Chronic Disease Risk andevelopment. Among adults, food inse-urity/insufficiency is associated withoor physical and mental health sta-us, as well as depression in women58-63) and risk for and incidence ofhronic diseases, including diabetes24,25,35,64). In US adults, food inse-urity appears to be associated with di-betes incidence, independent of bodyass index (65). Diabetes and chronic
isease management is also associatedith food insecurity (24,59,66). Finally,uman immunodeficiency virus infectionnd poorer human immunodeficiency vi-us infection management/treatmentutcomes have been associated with foodnsecurity (67-70).hild and Adult Overweight and Obesity. Forhildren, studies exploring the relation-hip between food insecurity and child-ood obesity have used a variety ofata sets and methods, yielding mixedesults—a positive, negative, or no re-ationship (47,71). Although additionalesearch should further explore therends, most recently, a study by Gun-erson and Kreider (47) found food se-urity to be positively associated with aealthful weight in a nationally repre-entative sample of US children (Na-ional Health and Nutrition Examina-ion Survey, 2001-2006).
For adults, research continues toupport that food insecurity is associ-ted with overweight and obesity, es-ecially among women from house-olds experiencing marginal foodecurity or low food security (71-73).ossible causes of this phenomenon
nclude a binge-like eating pattern orvereating when food is available (36)nd consumption of low-quality dietsf empty-energy, high-fat, and sugaryoods (74-76). As with children, addi-ional research is needed to furtherlarify the relationship of food insecu-
ity and weight status in adults.of the AMERICAN DIETETIC ASSOCIATION 1371

UtLAhctcppcroearstfgrHtaSas(ttvdFPepafcpdp
egt(nfhrstrlmv
nfini
nrtctweihpeHci1
clttif1lbcvhapSWbwceWf1
hScSfi(ef3WCtatiaaeS
io
●
●
●
●
spgcotsn
bgEpfd
●
●
●
●
●
●
●
1
S Food Insecurity Can Be Alleviatedhrough a Variety of Immediate andong-Range Interventions
variety of strategies are utilized byouseholds when faced with resourceonstraints. Federal food and nutri-ion assistance programs, along withommunity-based, nongovernmentalrograms, have been shown to im-rove food and nutrition security. Be-ause households undoubtedly expe-ience job transitions, layoffs, andther disruptions regardless of theconomy, robust safety net programsre vital to helping US citizens andesidents achieve food and nutritionecurity (77). As stressed in the posi-ion statement, adequate funding forood and nutrition assistance pro-rams is vital to maintain the integ-ity of the US nutrition safety net.owever, systematic, sustainable ac-
ions are also needed to achieve foodnd nutrition security in the Unitedtates. Overall, a long-term, system-tic, broad-based approach, as de-cribed by McCullum and colleagues40), appears appropriate to effec-ively sustain our economic social sys-ems and, in turn, preserve our mostital resource, the citizens and resi-ents of the United States.ederal and Nonfederal Food and Nutritionrograms. Several federal and nonfed-ral programs address a variety of as-ects of food security (Figure 2). Inddition to these organizations, stateood security and hunger centers oroalitions, several federal agencies,rofessional organizations, and foun-ations fund food security-relatedrograms and research.Generally, the most recent national
stimates support that those withreater difficulty accessing food par-icipate in food assistance programs2). It would be expected, since food andutrition assistance programs provide
ood and other resources, that house-olds would be more food secure aftereceiving the benefits. However, thoseeeking program assistance are typicallyhose with greater levels of food insecu-ity. As previously noted, households uti-izing community emergency food and
eal programs appear to be particularlyulnerable to food insecurity.Although additional research is
eeded to further understand the bene-ts of federal and community food andutrition assistance programs and their
nfluence on both nutrition and non– n372 September 2010 Volume 110 Number 9
utrition-related outcomes, the mostecent national estimates (2) supporthat those with greater difficulty ac-essing food participate in food assis-ance program. First, for householdsith incomes �130% of the federal pov-
rty level and receiving SNAP benefitsn the previous 12 months, more thanalf were food insecure, with 30.6% ex-eriencing low food security and 25.7%xperiencing very low food security.owever, of similar households not re-
eiving SNAP, only 30.5% were foodnsecure (17.1% low food security;3.4% very low food security) (2).Next, regarding households with in-
omes �185% of the federal povertyevel and with school-age children par-icipating in free or reduced-price Na-ional School Lunch Program (NSLP)n the previous 30 days, 49.4% wereood insecure (31.1% low food security;8.3% very low food security). Of simi-ar households not receiving NSLPenefits, 31.2% experienced food inse-urity (19.8% low food security; 11.4%ery low food security). Finally, forouseholds with children younger thange 5 years, incomes �185% of federaloverty level, and receiving Specialupplemental Nutrition Program foromen, Infants, and Children (WIC)
enefits in the previous month, 45.7%ere food insecure (30.7% low food se-
urity; 15% very low food security). How-ver, of similar households not receivingIC benefits, 38.8% were classified as
ood insecure (27.7% low food security;1.1% very low food security) (2).For 2008, 55% of food insecure
ouseholds participated in NSLP,NAP, or WIC during the month beforeompleting the food security survey.pecifically, 32.5%, 33.7%, and 14% of
ood insecure households participatedn NSLP, SNAP, and WIC, respectively2). Participation by households experi-ncing very low food security was 51.8%or one of the three programs, and 27.9%,4.4%, and 11.1% for NSLP, SNAP, andIC, respectively (2).
ommunity-Based Systematic Actions. Long-erm interventions are needed tochieve food and nutrition security inhe United States. Social capital, thats, social trust and community normsnd networks that facilitate collectivection, appears especially important tond food insecurity in the Unitedtates (78,79). As part of the Commu-
ity Food Security Initiative efforts formproving US food insecurity, a varietyf methods are planned (4):
creating or enhancing communityinfrastructures, as well as research,monitoring, and evaluation meth-ods, to reduce food insecurity;increasing job and economic secu-rity and empowering communitymembers to become self-sufficient;supporting full and efficient use offederal food and nutrition assis-tance programs and aiding in localsupplemental food donation anddistribution programs; andeducating the public on nutrition,food safety, and food security.
McCullum and colleagues (40)tressed that creating multisectorartnerships and networks, includingovernment and public health agen-ies, educational institutions, nonprofitrganizations, and the volunteer sec-or, is vital for developing the infra-tructure needed to achieve food andutrition security.Community-based programs can
oost the effectiveness of federal pro-rams in a variety of ways (80,81).xamples of community food securityrogram benefits for both farmers/ood producers and community resi-ents include (81):
SNAP outreach programs, whichhelp to increase the number of eli-gible participating households in acommunity, decreasing reliance onemergency food programs.Farmers’ markets boost incomes oflocal farmers, while increasing com-munity access to fresh produce.Community gardens help residentsin public housing and other low-in-come households supplement theirdiet with fresh produce.Food buying cooperatives save house-holds money by pooling resources.Community-supported agricultureprograms help stabilize small farm-ers economically, while providinghigh-quality, below-retail-cost pro-duce to consumers.Farm-to-school initiatives assist lo-cal farmers in selling fresh producedirectly to school meal programs.Food recovery programs rescuewholesome food from being thrownaway and provide food to groups
serving those in need.
RATstA
tenap
pasaf
F nd nge
OLES AND RESPONSIBILITIES OF RDsND DTRshe American Dietetic Association’s vi-ion is to “optimize the nation’s healthhrough food and nutrition.” And the
Program
Bread for the World
Child and Adult Care Food Program
Community Food Security Coalition
Community Food Security Initiative
Congressional Hunger Center
Expanded Food and Nutrition Education Prog
Federal nutrition assistance programs:● Child and Adult Care Food Program● Food Assistance For Disaster Relief● School Meals (Fresh Fruit and Vegetab
Lunch Program, School Breakfast ProgTeam Nutrition)
● Special Supplemental Nutrition ProgramChildren (WIC); WIC Farmers’ Market NFarmers’ Market Nutrition Program
● Summer Food Service Program● Supplemental Nutrition Assistance Prog
Pilot Program; see also SNAP Ed-ConnEducation
Federal nutrition assistance programs—food● Commodity Processing● Commodity Supplemental Food Program● Department of Defense Fresh Fruit and● Food Distribution Disaster Assistance● Food Distribution Program on Indian Re● Nutrition Services Incentive Program● Schools/Child Nutrition Commodity Prog● The Emergency Food Assistance Progra
Feeding America (formerly America’s Second
Food Recovery (A Citizen’s Guide to Food Re
Food Research and Action Center
Food Security in the United States Briefing Ron food security, including national estimsecurity measurement)
Mazon: A Jewish Response to Hunger
Meals on Wheels Association of America
Share Our Strength
SNAP-Ed Connection
SNAP Nutrition Education
WHY (World Hunger Year)
igure 2. Selected programs, organizations, a
ssociation values social responsibility; a
hat is, “Making decisions with consid-ration for . . . environmental, eco-omic, and social implications” (82). Inddition, one of the three core researchriorities of the Association centers on
W
w
w
w
h
w
w
rogram; National School; Special Milk Program;
r Women, Infants, andtion Program; Senior
(SNAP); Healthy Incentiveson and SNAP Nutrition
w
tribution programs:
getable Program
vations
s
w
rvest) h
ery) w
w
(an informational Web siteof food security and food
w
w
w
w
h
w
w
resources that address food insecurity and hu
“safe, secure, sustainable food sup- s
September 2010 ● Journal
ly” (83). In that light, RDs and DTRsre uniquely positioned to play leader-hip roles in developing, implementing,nd evaluating strategies to end USood insecurity. RDs and DTRs under-
site
.bread.org
.fns.usda.gov/cnd/care/default.htm
.foodsecurity.org
//attra.ncat.org/guide/a_m/cfsi.html
.hungercenter.org
.csrees.usda.gov/nea/food/efnep/efnep.html
.fns.usda.gov/fns
.fns.usda.gov/fdd
//feedingamerica.org/default.aspx
.usda.gov/news/pubs/gleaning/content.htm
.frac.org
.ers.usda.gov/briefing/foodsecurity
.mazon.org
.mowaa.org/Page.aspx?pid�183
.strength.org
//snap.nal.usda.gov/nal_display/index.php?x_level�1&info_center�15
.fns.usda.gov/fsp/nutrition_education
.whyhunger.org
r in the United States.
eb
ww
ww
ww
ttp:
ww
ram ww
le Pram
foutri
ramecti
ww
dis
Ve
ser
ramm
ww
Ha ttp:
cov ww
ww
oomates
ww
ww
ww
ww
ttp:ta
ww
ww
tand the effects of inadequate dietary
of the AMERICAN DIETETIC ASSOCIATION 1373

iasc
tus
len
F an of i
1
ntake and food insecurity on healthnd well-being and are trained in foodystems, management, negotiation, de-
Education and practice● Incorporate food security-related conce● Learn about food insecurity and its con
other professionals, legislators, policym● Provide appropriate nutrition care by ob
Know and understand the culture of thinclude about food and nutrition securit
� factors such as food and beverag� food planning and purchasing abi� food acquisition practices, includin� preparation abilities and limitation� food safety practices;� federal and community food and� information related to building and� anthropometric measurements, in� nutrition education needs regardin
● Realize that food insecurity may make● Screen clients for resource-constrained
statements best describes the food eatthe kinds of food we want to eat; 3) So
● Partner with other professionals to alle● Network with organizations and progra
programs, emergency food and meal pcommunity gardens, anti-hunger advoc
● Educate eligible clients on the availabilreferrals or recommend participation.
● Work to decrease the stigma of food a● Develop innovative interventions and pr
individuals, households, and communitifoods, focusing on the development ofprojects that foster economic developm
Research● In view of the core research priority of
conduct or collaborate on food insecuri� mapping community processes;� documenting the nutritional value� investigating the causes of food in
population groups;� exploring the influence of food sy
community;� assessing the distance of stores a
and� determining the effectiveness, suc
● Participate in evaluating community-ba
Advocacy and public policy● Support legislative and regulatory proce
education, and programs that support t● Serve as advocates for the nutritionally● Assist in efforts to improve food access● Partner with local and state anti-hunge● Serve on a local food policy council, w
changes.● Eliminate barriers to healthy eating am● Advocating that stores accepting the Su
igure 3. Contributions of registered dietitians
ision-making, and marketing/promo- c
374 September 2010 Volume 110 Number 9
ion. Clearly, RDs and DTRs areniquely positioned to play key leader-hip roles and to collaborate with poli-
into dietetics education programs using creatuences on individuals, households, and commrs, and community members to increase awaing/considering food access- and availability-
cal community to further assist in determininguring the nutritional care process. Informationtake (amount/variety/quality);s and limitations, including availability of transardening, farming, hunting/fishing, and/or be
ncluding availability of appliances and utilities
ition assistance program utilization;ilizing social networks;ing growth pattern and/or weight changes; aneal planning and purchasing, label reading, a
chasing food difficult for the client, preventingck of access to food using a single-item foodin your household: 1) Enough of the kinds oftimes not enough to eat; or 4) Often not enou
e food insecurity, including urban planners, puaddressing food insecurity in the local commuams, food recovery groups, farmers markets,organizations, and food cooperatives.nd benefits of federal and nonfederal resourc
tance programs to increase participation ratesams that provide nutrition education and buildincluding programs highlighting the benefits octive household management strategies and.
American Dietetic Association related to a “selated research. Examples include:
emergency foods and donor practices;urity and its effects on health, nutritional stat
issues, such as seasonal variation in food a
pting Supplemental Nutrition Assistance Prog
s cost-benefit analyses, of food recovery andprograms designed to address food insecurity
s that promote uniform, adequately funded foeconomic self-sufficiency of individuals and falnerable and those groups at increased risk fod acquisition by individuals and reduce ediblevocacy organizations.examines local food systems and provides r
those at risk for and experiencing food inseclemental Nutrition Assistance Program have n
d dietetic technicians, registered, to the goal
ymakers, government and community o
eaders, health departments, countyxtension programs, anti-hunger orga-izations, and other community-based
pedagogy.ties, and communicate this information toess of food insecurity and its outcomes.ted information during the assessment.propriate questions and/or information togather:
tation;g, borrowing, or stealing food;
food safety.mpliance to a prescribed diet.ficiency question, “Which of the followingwe want to eat; 2) Enough but not always
to eat” (30).health professionals, and others.
, including food and nutrition assistancemunity-supported agriculture farms,
available in the community and make
ills to improve the food security ofcal, seasonal, and sustainably grownpreparation, and creating food-based
secure, sustainable food supply” (83),
and well-being of special, at-risk
ability, on food insecurity in the
in a particular area to participant homes;
er programs.
and nutrition assistance programs, nutritionies.od insecurity.od loss through food recovery and gleaning.
mendations for social and public policy
y.nt-dense offerings for clientele.
mproving food insecurity in the United States.
pts iveseq uniake rentain rela
e lo apy d toe inlitie porg g ggin
s, i ;
nutrut
clud dg m ndpur co, la sufen foodme gh
viat blicms nityrogr comacyity a es
ssis .ogr skes, f loeffe foodent
the afe,ty-r
ofsec us
stem vail
cce ram
h a othsed .
sse odhe milvu r foan fo
r adhich ecom
ong uritpp utrie
rganizations to eliminate food insecu-

rlsmicac
R
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
3
4
4
4
4
4
4
4
4
4
ity in the United States and to estab-ish food secure communities. Figure 3ummarizes how RDs and DTRs canake valuable contributions toward
mproving food insecurity through edu-ation, practice, research, advocacy,nd public policy, especially throughommunity-based involvement.
eferences1. Anderson S. Core indicators of nutritional
state for difficult to sample populations. JNutr. 1990;102:1559-1660.
2. Nord M, Andrews M, Carlson S. HouseholdFood Security in the United States, 2008.Alexandria, VA: US Department of Agricul-ture, Economic Research Service; 2009. Eco-nomic Research Service Publication No.ERR-83.
3. Hamelin A-M, Habicht J-P, Beaudry M.Food insecurity: Consequences for thehousehold and broader social implications. JNutr. 1999;129(suppl):525S-528S.
4. Community Food Security Initiative. NationalCenter for Appropriate Technology Web site.http://attra.ncat.org/guide/a_m/cfsi.html. Ac-cessed February 24, 2010.
5. US Department of Health and Human Ser-vices. Healthy People 2010. http://www.healthypeople.gov/. Accessed September 11,2009.
6. US Department of Health and Human Ser-vices. Healthy People 2020. http://www.healthypeople.gov/hp2020/advisory/PhaseI/default.htm. Accessed September 11, 2009.
7. Albrecht JA, Nagy-Nero D. Position of TheAmerican Dietetic Association: Food and wa-ter safety. J Am Diet Assoc. 2009;109:1449-1460.
8. Struble MB, Aomari LL. Position of theAmerican Dietetic Association: Addressingworld hunger, malnutrition, and food inse-curity. J Am Diet Assoc. 2003;103:1046-1057.
9. Hamm MW, Bellows AC. Community foodsecurity and nutrition educators. J NutrEduc Behav. 2003;35:37-43.
0. Gottlieb R, Fisher A. Community food secu-rity and environmental justice: Searchingfor a common discourse. Ag Hum Values.1996;3:23-32.
1. Briefel R, Woteki C. Development of the foodsufficiency questions for the Third NationalHealth and Nutrition Examination Survey.J Nutr Educ. 1992;24(suppl):24S-28S.
2. Nutrition Action Themes for the UnitedStates: A Report in Response to the Interna-tional Conference on Nutrition. Washington,DC: US Department of Agriculture, Centerfor Nutrition Policy and Promotion; 1996.CNPP-2 Occasional Paper.
3. Food security and hunger in the US: Defini-tions of hunger and food security. US Depart-ment of Agriculture, Economic Research Ser-vice Web site. http://ers.usda.gov/Briefing/FoodSecurity/labels.htm. Accessed September13, 2009.
4. Food security and hunger in the US: Measur-ing household food security. US Departmentof Agriculture, Economic Research ServiceWeb site. http://ers.usda.gov/Briefing/FoodSecurity/measurement.htm. AccessedSeptember 13, 2009.
5. Bickel G, Nord M, Price C, Hamilton W,Cook J. Guide to Measuring Household Food 3
Security, Revised 2000. Alexandria, VA: USDepartment of Agriculture, Food and Nutri-tion Service; 2000.
6. Holben DH. Position of the American Die-tetic Association: Food insecurity and hun-ger in the United States. J Am Diet Assoc.2006;106:446-458.
7. Nord M, Prell M. Struggling to feed the fam-ily: What does it mean to be food insecure?Amber Waves. 2007;5:32-39.
8. Andrews M, Nord M. Food insecurity up inrecessionary times. Amber Waves. 2009;7:32-36.
9. McIntyre L, Glanville T, Raine KD, DayleJB, Anderson B, Battaglia N. Do low-incomelone mothers compromise their nutrition tofeed their children? J Canadian Med Assoc.2003;168:686-691.
0. Mabli J, Cohen R, Potter F. Zhanyun Z. Hun-ger in America 2010: National Report Pre-pared for Feeding America. Feeding AmericaWeb site. http://feedingamerica.org/faces-of-hunger/hunger-in-america-2010/hunger-report-2010.aspx. Accessed February 24,2010.
1. Hunger and Homelessness Survey: A statuson hunger and homelessness in America’scities: A 23-city survey. US Conference ofMayors Web site. http://usmayors.org/HHSurvey2007/hhsurvey07.pdf. PublishedDecember 2007. Accessed September 12,2009.
2. Cutler-Triggs C, Fryer GE, Miyoshi TJ,Weitzman M. Increased rates and severity ofchild and adult food insecurity in householdswith adult smokers. Arch Pediatr AdolescMed. 2008;162:1056-1062.
3. Rose D. Economic determinants and dietaryconsequences of food insecurity in theUnited States. J Nutr. 1999;129(suppl):517S-520S.
4. Biros MH, Hoffman PL, Resch K. The prev-alence and perceived health consequences ofhunger in emergency department patientpopulations. Acad Emerg Med. 2005;12:310-317.
5. Sullivan AF, Clark S, Pallin DJ, CamargoCA Jr. Food security, health, and medicationexpenditures of emergency department pa-tients. J Emerg Med. 2010;38:524-528.
6. Cook JT, Frank DA, Levenson SM, NeaultNB, Heeren T, Black MM, Berkowitz C, Ca-sey PH, Meyers AF, Cutts DB, Chilton M.Child food insecurity increases risks posedby household food insecurity to young chil-dren’s health. J Nutr. 2006;136:1073-1076.
7. Nord M, Kantor LS. Seasonal variation infood insecurity is associated with heatingand cooling costs among low-income elderlyAmericans. J Nutr. 2006;136:2939-2944.
8. Frank DA, Neault NB, Skalicky A, Cook JT,Wilson JD, Levenson S, Meyers AF, Heeren T,Cutts DB, Casey PH, Black MM, Berkowitz C.Heat or eat: The Low Income Home EnergyAssistance Program and nutritional andhealth risks among children less than 3 yearsof age. Pediatrics. 2006;118:e1293-e1302.
9. Cohen R, Kim M, Ohls J. Hunger in America2006: National Report Prepared for America’sSecond Harvest. Feeding America Web site.http://feedingamerica.org/our-network/�/media/Files/A2HNationalReport.ashx?.pdf.Accessed March 30, 2010.
0. Kaiser LL, Townsend MS. Food insecurityamong US children: Implications for nutri-tion and health. Top Clin Nutr. 2005;20:313-
320.1. Casey PH, Szeto K, Lensing S, Bogle M,
September 2010 ● Journal
Weber J. Children in food-insufficient, low-income families. Prevalence, health and nu-trition status. Arch Pediatr Adolesc Med.2001;155:508-514.
2. Lorson BA, Melgar-Quinonez HR, TaylorCA. Correlates of fruit and vegetable intakesin US children. J Am Diet Assoc. 2009;109:474-478.
3. Widome R, Neumark-Sztainer D, HannanPJ, Haines J, Story M. Eating when there isnot enough to eat: Eating behaviors and per-ceptions of food among food-insecure youths.Am J Public Health. 2009;99:822-828.
4. Bhattacharya J, Currie J, Haider S. Poverty,food insecurity, and nutritional outcomes inchildren and adults. J Health Econ. 2004;23:839-862.
5. Dixon LB, Winkleby M, Radimer K. Dietaryintakes and serum nutrients differ betweenadults from food-insufficient and food-suffi-cient families: Third National Health andNutrition Examination Survey, 1988-1994.J Nutr. 2001;131:1232-1246.
6. Olson CM. Food insecurity in women: A rec-ipe for unhealthy trade-offs. Top Clin Nutr.2005;20:321-328.
7. Zizza CA, Duffy PA, Gerrior SA. Food inse-curity is not associated with lower energyintakes. Obesity. 2008;16:1908-1913.
8. Robinson-O’Brien R, Story M, Heim S. Im-pact of garden-based youth nutrition inter-vention programs: A review. J Am Diet As-soc. 2009;109:273-280.
9. Heim S, Stang J, Ireland M. A garden pilotproject enhances fruit and vegetable con-sumption among children. J Am Diet Assoc.2009;109:1220-1226.
0. McCullum C, Desjardins E, Kraak VI, La-dipo P, Costello H. Evidenced-based strate-gies to build community food security. J AmDiet Assoc. 2005;105:278-283.
1. Cook JT, Frank DA. Food security, poverty,and human development in the UnitedStates. Ann NY Acad Sci. 2008;1136:193-209.
2. Carmichael SL, Shaw GM, Yang W, AbramsB, Lammer EJ. Maternal stressful lifeevents and risks of birth defects. Epidemiol-ogy. 2007;18:356-361.
3. Carmichael SL, Yang W, Herring A, AbramsB, Shaw GM. Maternal food insecurity isassociated with increased risk of birth de-fects. J Nutr. 2007;137:2087-2092.
4. Alaimo K, Olson CM, Frongillo EA Jr. Foodinsufficiency, family income, and health inUS preschool and school-aged children.Am J Public Health. 2001;91:781-786.
5. Casey PH, Szeto KL, Robbins JM, Stuff JE,Connell C, Gossett JM, Simpson PM. Childhealth-related quality of life and householdfood security. Arch Pediatr Adolesc Med.2005;195:51-56.
6. Cook JT, Frank DA, Casey PH, Rose-JacobsR, Black MM, Chilton M, Ettinger deCuba S,Appugliese D, Coleman S, Heeren T,Berkowitz C, Cutts DB. A brief indicator ofhousehold energy security: Associationswith food security, child health, and childdevelopment in US infants and toddlers. Pe-diatrics. 2008;122:e867-e875.
7. Gunderson C, Kreider B. Bounding the ef-fects of food insecurity on children’s healthoutcomes. J Health Econ. 2009;28:971-983.
8. Chilton M, Black MM, Berkowitz C, CaseyPH, Cook J, Cutts D, Rose Jacobs R, HeerenT, Ettinger de Cuba S, Coleman S, Meyers
A, Frank DA. Food insecurity and risk ofpoor health among US-born children of im-of the AMERICAN DIETETIC ASSOCIATION 1375

4
5
5
5
5
5
5
5
5
5
5
6
6
6
6
6
6
6
6
6
6
7
7
7
7
7
7
7
7
7
7
8
8
8
1
migrants. Am J Public Health. 2009;99:556-562.
9. Rose-Jacobs R, Black MM, Casey PH, CookJT, Cutts DB, Chilton M, Heeren T, Leven-son SM, Meyers AF, Frank DA. Householdfood insecurity: Associations with at-risk in-fant and toddler development. Pediatrics.2008;121:65-72.
0. Park K, Kersey M, Geppert J, Story M,Cutts D, Himes JH. Household food insecu-rity is a risk factor for iron-deficiency anae-mia in a multi-ethnic, low-income sample ofinfants and toddlers. Public Health Nutr.2009;12:210-2128.
1. Skalicky A, Meyers AF, Adams WG, Yang Z,Cook JT, Frank DA. Child food insecurityand iron deficiency anemia in low-incomeinfants and toddlers in the United States.Matern Child Health J. 2006;10:177-185.
2. Alaimo K, Olson CM, Frongillo EA Jr. Foodinsufficiency and American school-aged chil-dren’s cognitive, academic and psychosocialdevelopment. Pediatrics. 2001;108:44-53.
3. Alaimo K, Olson CM, Frongillo EA. Familyfood insufficiency, but not low family in-come, is associated with dysthymia and sui-cide symptoms in adolescents. J Nutr. 2002;132:719-725.
4. Fuller B, Caspary G, Kagan SL, Gauthier C,Huang D S-C, Carroll J, McCarthy J. Doesmaternal employment influence poor chil-dren’s social development? Early Child ResQ. 2002;17:470-497.
5. Kleinman RE, Murphy JM, Little M, PaganoJ, Wehler CA, Regal K, Jellinek MS. Hungerin children in the United States: Potentialbehavioral and emotional correlates. Pediat-rics. 1998;101:1-6.
6. Murphy JM, Wehler CA, Pagano ME, LittleM, Kleinman RE, Jellinek MS. Relationshipbetween hunger and psychosocial function-ing in low-income American children. J AmAcad Child Adolesc Psychiatry. 1998;37:163-170.
7. Reid LL. The Consequences of Food Insecu-rity for Child Well-Being: An Analysis ofChildren’s School Achievement, Psychologi-cal Well-Being, and Health. Chicago, IL:Joint Center for Poverty Research; 2000.JCPR Working Paper 137.
8. Huddleston-Casas C, Charnigo R, SimmonLA. Food insecurity and maternal depres-sion in rural, low-income families: A longi-tudinal investigation. Public Health Nutr.2009;12:1133-1140.
9. Nelson K, Cunningham W, Andersen R,Harrison G, Gelberg L. Is food insufficiencyassociated with health status and healthcare utilization among adults with diabetes?J Gen Intern Med. 2001;16:404-411.
0. Pheley AM, Holben DH, Graham AS, SimpsonC. Food security and perceptions of health sta-tus: A preliminary study in rural Appalachia.J Rural Health. 2002;18:447-454.
1. Siefert K, Heflin CM, Corcoran ME, Wil-liams DR. Food insufficiency and the physi-cal and mental health of low-income women.Women Health. 2001;32:159-177.
2. Stuff JE, Casey PH, Szeto KL, Gossett JM,Robbins JM, Simpson PM, Connell C, BogleML. Household food insecurity is associatedwith adult health status. J Nutr. 2004;134:2330-2335.
3. Vozoris NT, Tarasuk VS. Household food in-sufficiency is associated with poorer health.J Nutr. 2003;133:1200-126.
4. Holben DH, Pheley AM. Obesity and diabe-tes are greater in food insecure households
8
376 September 2010 Volume 110 Number 9
in rural Appalachian Ohio. Prev Chronic Dis[serial online]. Centers for Disease Controland Prevention Web site. http://www.cdc.gov/pcd/issues/2006/jul/05_0127.htm. Pub-lished July 2006. Accessed March 30, 2010.
5. Seligman HK, Bindman AB, Vittinghoff E,Kanaya AM, Kushel MB. Food insecurity isassociated with diabetes mellitus: Resultsfrom the National Health and Nutrition Ex-amination Survey (NHANES) 1999-2002.Soc Gen Intern Med. 2007;22:1018-1023.
6. Nelson K, Brown ME, Lurie N. Hunger in anadult patient population. JAMA. 1998;279:1211-1214.
7. Normén L, Chan K, Braitstein P, Anema A,Bondy G, Montaner JSG, Hogg RS. Food inse-curity and hunger are prevalent among HIV-positive individuals in British Columbia, Can-ada. J Nutr. 2005;135:820-825.
8. Weiser Bangsberg, Kegeles S, Ragland K,Kushel MB, Frongillo EA. Food insecurityamong homeless and marginally housed in-dividuals living with HIV/AIDS in SanFrancisco. AIDS Behav. 2009;13:841-848.
9. Weiser SD, Fernandes KA, Brandson EK,Lima VD, Anema A, Bangserg DR, Mon-taner JS, Hogg RS. The association betweenfood insecurity and mortality among HIV-infected individuals on HAART. J AcquirImmune Defic Syndr. 2009;52:342-349.
0. Weiser SD, Frongillo EA, Ragland K, HoggRS, Riley ED, Bangsberg DR. Food insecu-rity is associated with incomplete HIV RNAsuppression among homeless and margin-ally housed HIV-infected individuals in SanFrancisco. J Gen Intern Med. 2008;24:14-20.
1. Dinour LM, Bergen D, Yeh M-C. The foodinsecurity-obesity paradox: A review of theliterature and the role food stamps mayplay. J Am Diet Assoc. 2007;107:1952-1961.
2. Hanson KL, Sobal J, Frongillo EA. Genderand marital status clarify associations be-tween food insecurity and body weight. JNutr. 2007;137:1460-1465.
3. Wilde PE, Peterman JN. Individual weightchange is associated with household food se-curity status. J Nutr. 2006;136:1395-1400.
4. Drewnowski A. Obesity, diets, and social in-equalities. Nutr Rev. 2009;67(suppl 1):S36-S39.
5. Drewnowski A, Darmon N. The economics ofobesity: Dietary energy density and energycost. Am J Clin Nutr. 2005;82(suppl):265S-273S.
6. Drewnowski A, Specter SE. Poverty and obe-sity: The role of energy density and energycosts. Am J Clin Nutr. 2004;79:6-16.
7. Nord M, Andrews M. Reducing Food Insecu-rity in the United States: Assessing ProgressToward a National Objective. Alexandria,VA: Economic Research Service, US Depart-ment of Agriculture; 2002. Food Assistanceand Nutrition Research Report No. 26-2.
8. Martin KS, Rogers BL, Cook JT, Joseph HM.Social capital is associated with decreasedrisk of hunger. Social Sci Med. 2004;58:2645-2654.
9. Woolcock M. The place of social capital inunderstanding social and economic out-comes. Can J Policy Res. 2001;2:11-17.
0. Allen P. Reweaving the food security safetynet: Mediating entitlement and entrepre-neurship. Ag Hum Values. 1999;16:117-129.
1. Kantor LS. Community food security pro-grams improve food access. Food Rev. 2001;24:20-26.
2. ADA: Who we are, what we do. AmericanDietetic Association Web site. http://www.
eatright.org/cps/rde/xchg/ada/hs.xsl/home_404_ENU_HTML.htm. Accessed September13, 2009.
3. ADA research philosophy and framework.American Dietetic Association Web site.http://www.eatright.org/cps/rde/xchg/ada/hs.xsl/governance_500_ENU_HTML.htm. Ac-cessed September 13, 2009.

the supporting paper.
This American Dietetic Association (ADA) position was adopted by theHouse of Delegates Leadership Team on April 22, 1990 and reaffirmed onSeptember 4, 1994; June 22, 2000; May 24, 2004; and May 17, 2007. Thisposition is in effect until December 31, 2014. ADA authorizes republicationof the position, in its entirety, provided full and proper credit is given.Readers may copy and distribute this paper, providing such distribution isnot used to indicate an endorsement of product or service. Commercialdistribution is not permitted without the permission of ADA. Requests touse portions of the position must be directed to ADA headquarters at800/877-1600, ext 4835, or [email protected].
Authors: David H. Holben, PhD, RD, LD (Ohio University, Athens, OH).Reviewers: Latinos and Hispanics in Dietetics and Nutrition member
interest group (Hope T. Bilyk, MS, RD, LDN, Rosalind Franklin Universityof Medicine and Science, North Chicago, IL); Sharon Denny, MS, RD (ADAKnowledge Center, Chicago, IL); Anne Hoisington, MS, RD (Oregon StateUniversity, Portland, OR); Hunger and Environmental Nutrition dieteticpractice group (Gretchen Hunt, RD, LDN, Commission on Economic Oppor-tunity, Wilkes-Barre, PA); Linda Knol, PhD, RD (University of Alabama,Tuscaloosa AL); Public Health/Community Nutrition dietetic practice group(Lauren Melnick, MS, RD, LD, The Ohio State University Extension, Cuya-hoga County, Cleveland, OH); Esther Myers, PhD, RD, FADA (ADA Re-search & Strategic Business Development, Chicago, IL); National Organi-zation of Blacks in Dietetics and Nutrition member interest group (BeatriceW. Phillips, EdD, RD, LD, Tuskegee University, Tuskegee, AL); KimberlyPrendergast, MPP, RD (Karmana, Inc, Sudbury, MA); Lisa Spence, PhD, RD(ADA Research & Strategic Business Development, Chicago, IL); Jennifer A.Weber, MPH, RD (ADA Policy Initiatives & Advocacy, Washington, DC);Dietetic Educators of Practitioners dietetic practice group (Lauri Wright,PhD, RD, LD/N, University of North Florida, Jacksonville, FL).
Association Positions Committee Workgroup: Diane Sowa, MBA, RD(chair); Linda B. Godfrey, MS, RD, SNS, LD; April C. Tallant, PhD, RD,LDN (content advisor).
The authors thank the reviewers for their many constructive commentsand suggestions. The reviewers were not asked to endorse this position or
September 2010 ● Journal of the AMERICAN DIETETIC ASSOCIATION 1377

POLICY STATEMENT Organizational Principles to Guide and Define the Child HealthCare System and/or Improve the Health of all Children
Promoting Food Security for AllChildrenCOUNCIL ON COMMUNITY PEDIATRICS, COMMITTEE ON NUTRITION
abstractSixteen million US children (21%) live in households without consistent access toadequate food. After multiple risk factors are considered, children who live inhouseholds that are food insecure, even at the lowest levels, are likely to be sickmore often, recover from illness more slowly, and be hospitalized more frequently.Lack of adequate healthy food can impair a child’s ability to concentrate andperform well in school and is linked to higher levels of behavioral and emotionalproblems from preschool through adolescence. Food insecurity can affect childrenin any community, not only traditionally underserved ones. Pediatricians can playa central role in screening and identifying children at risk for food insecurity andin connecting families with needed community resources. Pediatricians shouldalso advocate for federal and local policies that support access to adequatehealthy food for an active and healthy life for all children and their families.
INTRODUCTION
In 2013, 17.5 million US households, or 14.3% of all households and 21%of all children, met the US Department of Agriculture (USDA) definition ofa food-insecure household, one in which “access to adequate food islimited by a lack of money or other resources.”1,2 Households withchildren are nearly twice as likely to be food insecure as householdswithout children. In 2013, 7.5 million American families with childrenlacked consistent access to adequate, nutritious food. The crisis becomeseven more pressing for families facing severe economic hardships. In2013, almost 60% of all food-insecure households had incomes below185% of the federal poverty thresholds, the income eligibility cutoff formany child nutrition programs. The federal poverty threshold for an averagefamily of 4 people in 2013 was $23 834; 185% of this threshold amount is$44 093, but the federal poverty level is not a definition of economic hardship,and the amount to provide basic needs for a family of 4 often far exceeds thisamount. Because 30% of food-insecure households have incomes above thislevel, it is clear the problem is not related solely to poverty.
The demographic of food-insecure Americans extends beyond the areas ofconcentrated urban poverty and into suburbs and rural America, areas
This document is copyrighted and is property of the AmericanAcademy of Pediatrics and its Board of Directors. All authors have filedconflict of interest statements with the American Academy ofPediatrics. Any conflicts have been resolved through a processapproved by the Board of Directors. The American Academy ofPediatrics has neither solicited nor accepted any commercialinvolvement in the development of the content of this publication.
Policy statements from the American Academy of Pediatrics benefitfrom expertise and resources of liaisons and internal (AAP) andexternal reviewers. However, policy statements from the AmericanAcademy of Pediatrics may not reflect the views of the liaisons or theorganizations or government agencies that they represent.
The guidance in this statement does not indicate an exclusive courseof treatment or serve as a standard of medical care. Variations, takinginto account individual circumstances, may be appropriate.
All policy statements from the American Academy of Pediatricsautomatically expire 5 years after publication unless reaffirmed,revised, or retired at or before that time.
www.pediatrics.org/cgi/doi/10.1542/peds.2015-3301
DOI: 10.1542/peds.2015-3301
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2015 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: The authors have indicated they have nofinancial relationships relevant to this article to disclose.
POTENTIAL CONFLICT OF INTEREST: The authors have indicated theyhave no potential conflicts of interest to disclose.
PEDIATRICS Volume 136, number 5, December 2015 FROM THE AMERICAN ACADEMY OF PEDIATRICSby guest on April 6, 2016Downloaded from

often mistakenly thought to beimmune to this problem.3 Likepoverty, food insecurity is a dynamic,intensely complex issue; the currenteconomic recovery has marginallydiminished food insecurity, but levelsremain near historic highs.4 For manyfamilies, seemingly small changes inincome, expenses, or access to federalor state assistance programs mayinstantly reduce the ability topurchase healthy food and result inincreased vulnerability to foodinsecurity. Moreover, families andchildren do not only feel the effects ofhunger just as missed or meagermeals; food insecurity manifests itselfin many other biopsychosocialoutcomes, including health,education, and economicprosperity.5–12 In fact, more than30% of families who identified asfood insecure indicated that they hadto choose between paying for foodand paying for medicine or medicalcare.13 Combined, these negativeeffects can contribute to a lesscompetitive workforce for the nationand higher health care costs borne bythe US government and employers.
Food insecurity is associated withmany factors in addition to poverty.Unemployment andunderemployment are also stronglyassociated with food insecurity.2
Certain populations, such as childrenin immigrant families14 and largefamilies, families headed by singlewomen, families with less education,and families experiencing parentalseparation or divorce are at greaterrisk.2,3 Families who are foodinsecure usually have at least 1parent who is working or has workedfor at least 6 months of the previousyear. Working poor families andsingle-parent families are atparticular risk of food insecurity. Inlow-income households with childrenand food insecurity, 84% participatedin at least 1 federal food assistanceprogram, such as the SupplementalNutrition Assistance Program (SNAP)or free or reduced-price school mealsin 2010 to 2011.2 Thus, 16% of
low-income, food-insecure householdswith children do not receive federalsupports. Federal benefits canattenuate the severity of foodinsecurity but might not eliminate it,particularly for children and in regionswith higher food costs.15,16
EFFECTS OF FOOD INSECURITY ONCHILD HEALTH AND DEVELOPMENTALOUTCOMES
The inability to consistently providefood creates stress in families,contributing to depression, anxiety,and toxic stress, which make optimalparenting difficult regardless of socialclass.12,17 Most parents strive toprotect their children as much aspossible from the physiologicsensation of hunger and, ultimately,nutritional deprivation. Studies on theeffects of food insecurity inhouseholds demonstrate low dietaryquality in adults but slightly betterquality for the household’s children,18
and qualitative studies reveal howparents strategically limit their ownintake in an effort to spare theirchildren.13
There are multiple adverse healthoutcomes strongly correlated withfood insecurity. Children 36 monthsold or younger who live in food-insecure households have pooreroverall health and morehospitalizations than do children wholive in food-secure households.7
Children with food insecurity aremore likely to be iron deficient, as areadolescents with food insecurity.8,9
Food insecurity also is associatedwith lower bone density inpreadolescent boys.19
Poverty is associated closely with thedevelopment of obesity. Although nota direct cause of obesity,20,21 foodinsecurity disproportionatelythreatens certain populations athighest risk of obesity, includingthose from racial and ethnic minoritygroups and the poor.22 Children infood-insecure households generallyhave limited access to high-qualityfood. Environmental realities in
low-income neighborhoods, includingdecreased presence of full-servicegrocery stores and increasedavailability of fast-food restaurantsand energy-dense, nutrient-poorfood,22 may create barriers for low-income families trying to adopthealthy behaviors. Adequate foodmay be available only intermittently,leading to unhealthy eating patternsand increased stress that may makeweight loss difficult and facilitate thedevelopment of obesity.20 Householdswith smokers are more likely to befood insecure, perhaps because of thediversion of money to tobacco inthese households.23
Among children of all ages, foodinsecurity is linked with lowercognitive indicators, dysregulatedbehavior, and emotional distress.Children between 4 and 36 months ofage who live in low-income, food-insecure households are at higherrisk of developmental problems,which presage impaired schoolfunction, compared with children ofthe same age living in low-income,food-secure households.10
Longitudinal studies have shown thatfood insecurity in kindergartenstudents predicts reduced academicachievement in math and readingover a 4-year period.11
Young children in food-insecurehouseholds are more likely to havebehavior problems above and beyondthose attributable to their mother’sdepression and anxiety.12 Adolescentsin food-insecure families are morelikely to experience dysthymia andsuicidal ideation.24 Theseobservations may be attributable,in part, to neurotransmitterperturbations from poor diet and thesensation of hunger and in part fromchildren’s emotional reactions to foodinsecurity itself and its socialmeaning.
School-aged children are aware ofand distressed by food insecurity intheir household. They often try tohelp manage food resources in thefamily, either by supporting the
e1432 FROM THE AMERICAN ACADEMY OF PEDIATRICSby guest on April 6, 2016Downloaded from

efforts of their parents or by initiatingtheir own strategies for reducing foodintake (including choosing to eatless than they want). Parents maybe unaware of their child’sunderstanding of the family’s plightand may believe their child isunaware of the family’s lack offood.25,26 Adolescents describe foodinsecurity in terms of quantity (eatingless than usual, eating more or fasterwhen food is available), quality(having only a few low-cost foods),affective states (worry, anxiety, orsadness about the family’s food,shame or fear of being labeled “poor,”feelings of having no choice or ofadults trying to shield them from foodinsecurity), and social dynamics(using social networks to get food orbeing socially excluded).27
As with many pediatric conditions,the health effects of food insecurityand associated malnutrition maypersist beyond early life intoadulthood. A substantial body ofliterature also links early childhoodmalnutrition to adult disease,including diabetes, hyperlipidemia,and cardiovascular disease.5,6 Studiesof the outcomes of food insecurity inchildhood suggest that it may be anexample of ecologic contextmodifying individual physiologicfunction. Overall, the effects of foodinsecurity on the physical, mental,and emotional health of children andfamilies are additive to the effects oflow income alone.
PROGRAMS TO MITIGATE FOODINSECURITY
Given the high prevalence of foodinsecurity among US families withchildren and given its potential healtheffects, pediatricians need to beaware of resources that can mitigatefood insecurity and know how torefer eligible families. Theseprograms serve as critical supportsfor the physical and mental healthand academic competence of children(Table 1).
WIC
The Special Supplemental NutritionProgram for Women, Infants, andChildren (WIC), first established inthe early 1970s, is a discretionaryfederal program for which Congressmust appropriate funding each year.Its mission is “to safeguard the healthof low-income women, infants andchildren up to age 5 who are atnutritional risk by providingnutritious foods to supplement diets,information on healthy eating, andreferrals to healthcare.” WICparticipants are pregnant women,breastfeeding women (up tothe child’s first birthday),nonbreastfeeding postpartum women(up to 6 months postpartum), infants(up to their first birthday), andchildren up to their fifth birthday.
Prenatal WIC participation has beenconsistently associated with higherbirth weight and longer gestation,
particularly among mothers athighest risk.28 Participation in WICalso is associated with more iron-dense diets and increased food andvegetable intake in preschoolers.28
WIC serves 53% of all infantsyounger than1 year old in the UnitedStates. Most states provide vouchersor electronic benefits transfer cardsfor use in the purchase of eligibleproducts and for nutrition counselingand connection to health and socialservices. In most states, WIC also hasan associated program, the WICFarmer’s Market Nutrition Program,which gives additional vouchers forthe purchase of fresh, locally grownproduce at farmers’ markets androadside stands.
WIC is an effective evidence-basedintervention for improving the healthof low-income women and theirchildren. WIC has a strongcommitment to increasebreastfeeding among its participants,providing counseling, peer support,enhanced food packages, and accessto breast pumps to support theinitiation and continuation ofbreastfeeding. WIC participation hasbeen linked to better infant healthand lower rates of overweight andunderweight status among infants.29
SNAP
SNAP is an entitlement program thatprovides nutrition assistance to low-income families and individuals.SNAP, piloted as the Food Stamp
TABLE 1 Web Sites With Nutritional Information on Programs to Mitigate Food Insecurity
Program Information Income Eligibility Web Site
WIC WIC food packages #185% of federal poverty levela http://www.fns.usda.gov/wic/final-rule-revisions-wic-food-packages
State agency WIC-approvedfood lists for food packages
http://www.fns.usda.gov/wic/links-state-agency-wic-approved-food-lists
SNAP Eligible food items ,130% of federal poverty levela http://www.fns.usda.gov/snap/eligible-food-itemsSNAP-Ed resources http://snap.nal.usda.gov/
National School Lunchand National SchoolBreakfast Programs
Nutritional standards for schoollunches and breakfasts
Reduced-cost meals: #185% offederal poverty levela; freemeals: #130% of federalpoverty levela
http://www.fns.usda.gov/school-meals/nutrition-standards-school-meals
Child and Adult CareFood Program
Meal patterns for infants,children, and adults
http://www.fns.usda.gov/cacfp/meals-and-snacks
Summer FoodService Program
Finding summer meal programsin the community and meal content
http://www.fns.usda.gov/sfsp/summer-food-service-program-sfsp
a Available at http://familiesusa.org/product/federal-poverty-guidelines.
PEDIATRICS Volume 136, number 5, December 2015 e1433by guest on April 6, 2016Downloaded from
Program in 1961 and confirmed withthe Food Stamp Act in 1964 (Pub LNo. 88-525), is the largest food andnutrition program of the USDA. Itserves 47 million Americans, 72% ofwhom are in families with children.Like WIC, it is a federal program,administered through state agencies.Although SNAP application andeligibility rules can be complex, theprogram has been shown to beeffective in reducing food insecurityand negative health anddevelopmental outcomes amongrecipients.30 SNAP provides monthlybenefits (usually via electronicbenefit transfer cards) to purchaseeligible food items at retailersparticipating in the program. SNAPallotment is calculated as 30% of thenet monthly household income,capped by number of members ofthe household (eg, the maximummonthly allotment for a family of 4 iscurrently $649, or a maximum of$1.80 per person per meal).31 A pilotprogram to increase monthly familySNAP allotments by $60 wassuccessful in reducing very low foodsecurity among children by 30%. Asubsequent pilot program found thata $30 per month allotment reducedvery low food security amongchildren as well as the higher benefitbut produced smaller reductions infood insecurity among adults and thefull household.32
National School Lunch and NationalSchool Breakfast Programs
The National School Lunch Programwas established in 1946, although theUSDA had provided funds and food toschools for many years before that.More than 32 million childrenannually are provided witha nutritionally balanced, low-cost orfree lunch in over 100 000 public andnonprofit private schools andresidential child care institutions. TheSchool Breakfast Program was startedas a pilot program in 1966 and wasmade permanent in 1975. It provides13 million children each year witha free, nutritionally balanced
breakfast in more than 89 000schools. In 1998, Congress expandedthe National School Lunch Program toinclude coverage for snacks servedto children in after-school educationaland enrichment programs. In 2010,the Healthy, Hunger-Free Kids Act(Pub L No. 111-296) established theCommunity Eligibility Provision,which allows schools in areas of highpoverty to offer both breakfast andlunch at no charge to all studentswhile eliminating the stigmatizingschool meal application process,which burdens both parents andschool personnel. Notable savings inadministrative costs also have beenattributed to the CommunityEligibility Provision.33
The Healthy, Hunger-Free Kids Actrequired the USDA to update the mealpattern and nutrition standards forschool meals and foods sold inschools during school hours based onthe latest Dietary Guidelines forAmericans. Some of the recentpositive changes to the meal patternsincluded more whole grains offered,0 grams of trans fat per portion,appropriate calories by age, morefruit offered, and reduction of sodiumcontent. Although all meals mustmeet federal meal requirements, localfood authorities make the decisionsabout which specific foods to serveand how they are prepared.Implementation of these changes hasincreased fruit consumption anddecreased wasted food amongstudents participating in the NationalSchool Lunch Program.34
Child and Adult Care Food Program
The Child and Adult Care FoodProgram, administered by the USDA,provides cash assistance to states toassist child and adult care institutionsand family or group child care homesin providing nutritious foods thatcontribute to the wellness, healthygrowth, and development of children.In fiscal year 2013, the programserved more than 3 million children.In the Child and Adult Care FoodProgram, the USDA establishes meal
patterns with minimum foodcomponent and quantityrequirements; these requirements arecurrently under revision to makethem more consistent with theDietary Guidelines for Americans.
Summer Food Service Program
The Summer Food Service Program(SFSP) began as a pilot program, theSpecial Food Service Program, in1968, serving children during thesummer and in child care. In 1975,the programs split and the SFSP cameto stand on its own. The SFSP ensuresthat low-income children continueto receive nutritious meals whenschool is not in session and sustainschildren’s physical and socialdevelopment, helping them returnto school ready to learn. Children18 years old and younger can receivefree meals and snacks at approvedcommunity sites, which may includehealth care institutions.
The SFSP serves approximately2 million children each summer.Despite its importance, participationin SFSP is far below the number ofchildren eligible for the programand also below the numberparticipating in school meals duringthe school year. In part, this reflectsthe challenge of reaching somepopulations of children during thesummer, particularly children in ruralareas, areas with dangerous levels ofsummer heat, or very urban areaswhere transportation or safety maybe a challenge. Within communities,advocacy by pediatricians isespecially important during thesummer, when school nutritionprograms may be insufficient orinaccessible for many children andfamilies.
Food Pantries and Soup Kitchens
Food pantries and soup kitchens areoften available in local areas andserve as another vital piece of thesafety net for children and familiesstruggling with food insecurity. Theseresources usually are funded bya combination of local philanthropic
e1434 FROM THE AMERICAN ACADEMY OF PEDIATRICSby guest on April 6, 2016Downloaded from

organizations, faith-basedcommunities, and governmentresources. Knowing what is availablein the community can help supportimproved nutrition and reduce foodinsecurity among families served bypediatricians. However, manycharitable food providers are notconsistently able to provide healthfulfood in general, nutritional itemsappropriate for infants and toddlers,or amounts adequate to protectfamilies from food insecurity for morethan a few days. Realizing the limitedcapacity of existing communityresources is essential to tailoringreferrals for families facing foodinsecurity.
SCREENING TOOLS FOR PEDIATRICIANS
Pediatricians can better assess thestress of food insecurity in individualfamilies by incorporating a screeningtool into their practice. The USDAuses an 18-item measure to assessfood insecurity with the HouseholdFood Security Scale,1 which is thestandard tool for research. A morepractical in-office tool is the 2-itemscreen designed by Hager et al35
(Table 2), which uses a subset of 2questions from the Household FoodSecurity Scale. Affirmative answers toeither of these 2 questions identifiedfood insecurity with a sensitivity of97% and a specificity of 83% (ascompared with the full 18-itemHousehold Food Security Scale).These screens are designed toidentify food insecurity in a family asa whole. In some cases, a single childin a family may be more or lessaffected by food insecurity that theothers; this difference will not bedetected by these screens. Someresources to address food insecuritywhen discovered at a clinic visit arelisted in Table 3.
ADVOCACY AND EDUCATION
At the federal level, pediatricianshave historically advocated insupport of expanded funding for andaccess to key nutritional assistance
programs such as WIC, SNAP, andthe school nutrition programs. It iscritical to maintain strong, evidence-based nutrition guidelines for allpublic programs that supportchildhood nutrition, including schoollunches. Because Congress isscheduled to reauthorize many of theaforementioned child nutritionprograms in the near future, attemptsto weaken nutrition standards inschool meals and other children’sprograms are anticipated. Advocacyby the American Academy ofPediatrics is crucial to ensure thatnutrition standards remain in placeand that access to effective assistanceprograms is expanded rather thanreduced.
Advocacy efforts at the federal,state, and community levels mustincorporate both obesity preventionand expanded nutritional access atthe federal, state, and local levelsto promote children’s health.Engagement of community residentsin understanding local context36 and
establishment of interdisciplinarycollaboration are key elementsof advocacy efforts that address foodinsecurity in communities.
Medical education offers a naturalopportunity to teach students andresidents to screen for food insecurityregularly as a part of pediatric care.National initiatives such as theCommunity Pediatrics TrainingInitiative increasingly emphasizecommunity- and population-basedobjectives throughout residencytraining,37,38 and evidence suggeststhat formal training in communityhealth is associated with communitychild health involvement amongpediatricians.39 The followingapproaches enhance training aboutfood insecurity within communitypediatrics: engaging on-site social andlegal resources to emphasizescreening and management of foodinsecurity40; using qualityimprovement methods to improvescreening and evaluate efforts,41
including obtaining data on theimpact of community-basedinitiatives such as farmers’ marketsand food pantries on food insecurity;establishing curriculum-basedcommunity site visits that exposemedical students and residents tosuccessful federal programs, such asWIC42; and encouraging medicalstudents and residents to participatein local, regional, and federaladvocacy efforts. More data areneeded to elucidate how curriculum
TABLE 2 Screening for Food Insecurity
1. Within the past 12 mo, we worried whether ourfood would run out before we got money to buymore. (Yes or No)
2. Within the past 12 mo, the food we bought justdidn’t last and we didn’t have money to getmore. (Yes or No)
Adapted from Hager et al.35 Although an affirmative re-sponse to both questions increases the likelihood of foodinsecurity existing in the household, an affirmative re-sponse to only 1 question is often an indication of foodinsecurity and should prompt additional questioning.
TABLE 3 Resources for Pediatricians Dealing With Food-Insecure Families
Program Web Site Description
2-1-1 211.org, then access by ZIP code or city Access to information onschool lunch programs,summer food programsfor children, and othergovernment-sponsoredprograms (eg, SNAP, WIC)as well as soup kitchensand community gardens
Healthy FoodBank Hub
Healthyfoodbankhub.feedingamerica.org Includes a food bank locatorand other tools andresources for food-insecurehouseholds
MyPlate http://www.choosemyplate.gov/budget/downloads/MeetingYourMyPlateGoalsOnABudget.pdf
Recipes and tip sheets forlow-cost healthy eating
PEDIATRICS Volume 136, number 5, December 2015 e1435by guest on April 6, 2016Downloaded from

elements can most effectively teachtrainees to assess food insecurity andadvocate for programs that mitigatefood insecurity.
RECOMMENDATIONS
The American Academy of Pediatricsrecommends that pediatriciansengage in efforts to mitigate foodinsecurity at the practice leveland beyond. The followingrecommendations offer practice-levelstrategies for pediatricians.
• A 2-question validated screeningtool (Table 2) is recommended forpediatricians screening for foodinsecurity at scheduled healthmaintenance visits or sooner, ifindicated.
• It is beneficial for pediatricians tofamiliarize themselves with com-munity resources so that whenchildren screen positively for foodinsecurity, referral mechanisms toWIC, SNAP, school nutrition pro-grams, local food pantries, summerand child care feeding programs,and other relevant resources areaccessible and expedient. This in-formation is particularly importantfor new mothers. New mothers infood-insecure households can beconnected to WIC and other com-munity resources during pregnancyand early in the postpartum periodto encourage breastfeeding.
• When advocating for programstargeted at families with food in-security, it is important that pedia-tricians be aware of the nutritionalcontent of food offered in supple-mental programs (Table 3).
• In the office setting, pediatricianswho are aware of the factors thatmay increase vulnerability of food-insecure populations to obesity andfactors that disproportionatelyburden food-insecure householdsmay address these issues at clinicvisits. These factors include lack ofaccess to healthy and affordablefoods, cost of healthy food (and thelow cost of many unhealthy foods),
media messaging that promotesnonnutritious foods and beverages,and the role of stress in decision-making related to food.
At a system level, pediatricians canadvocate for the needs of childrenand families facing food insecurity.
• Food insecurity, including screen-ing tools and community-specificresource guides, can be in-corporated into education of med-ical students and residents toprepare future generations ofphysicians to universally screen forand address food insecurity.
• Pediatricians can advocate for pro-tecting and increasing access toand funding for SNAP, WIC, schoolnutrition programs, and summerfeeding programs at the local, state,and national levels. Advocacy mustalso include keeping the food of-fered in these programs high innutrient quality and based onsound nutritional science. Pedia-tricians can promote access to nu-tritious foods in out-of-schoolsettings, particularly in child care,in preschool, and during the sum-mer. Advocacy for “express laneeligibility” (adjunctive eligibility),which permits a state to usefindings from enrollment in1 program to enroll the family inother programs for which theyqualify, also will increase access tofood and nutrition assistanceprograms.
• Pediatricians can strongly supportinterdisciplinary research that elu-cidates the relationship betweenstress, food insecurity, and adversehealth consequences; the barriersto breastfeeding for women understress in food-insecure households;and evidence-based strategies thatoptimize access to high-quality,nutritious food for families facingfood insecurity.
CONCLUSIONS
Food insecurity is a complex issuethat presents profound challenges for
children and families. Pediatriciansplay an essential role in recognition offood insecurity, practice-levelintervention, and advocacy tomitigate food insecurity within ourcommunities.
LEAD AUTHORS
Sarah Jane Schwarzenberg, MD, FAAPAlice A. Kuo, MD, PhD, FAAPJulie M. Linton, MD, FAAPPatricia Flanagan, MD, FAAP
COUNCIL ON COMMUNITY PEDIATRICSEXECUTIVE COMMITTEE, 2014–2015
Benjamin A. Gitterman, MD, FAAP, ChairpersonLance A. Chilton, MD, FAAP, Vice-ChairpersonWilliam H. Cotton, MD, FAAPJames H. Duffee, MD, MPH, FAAPPatricia Flanagan, MD, FAAPVirginia A. Keane, MD, FAAPScott D. Krugman, MD, FAAPAlice A. Kuo, MD, PhD, FAAPJulie M. Linton, MD, FAAPCarla D. McKelvey, MD, FAAPGonzalo J. Paz-Soldan, MD, FAAP
LIAISONS
Ricky Y. Choi, MD, FAAP – Chairperson, Immigrant
Health Special Interest Group
Jacqueline Dougé, MD, MPH, FAAP – Chairperson,
Prevention and Public Health Special Interest Group
Janna Gewirtz O’Brien, MD – Section on Medical
Students, Residents, and Fellowship Trainees
STAFF
Camille Watson, MS
COMMITTEE ON NUTRITION, 2014–2015
Stephen R. Daniels, MD, PhD, FAAP, ChairpersonSteven A. Abrams, MD, FAAPMark R. Corkins, MD, FAAPSarah D. de Ferranti, MD, FAAPNeville H. Golden, MD, FAAPSheela N. Magge, MD, MSCE, FAAPSarah Jane Schwarzenberg, MD, FAAP
LIAISONS
Leila Beker, PhD, RDN – Food and Drug Administration
Jeff Critch, MD, FAAP – Canadian Pediatric Society
Rear Admiral Van S. Hubbard, MD, PhD, FAAP– National Institutes of Health
Kelley Scanlon, PhD – Centers for Disease Control and
Prevention
Valery Soto, MS, RD, LD – US Department of
Agriculture
STAFF
Debra L. Burrowes, MHA
e1436 FROM THE AMERICAN ACADEMY OF PEDIATRICSby guest on April 6, 2016Downloaded from

ACKNOWLEDGMENTS
The authors thank Children’sHealthWatch for its valuable reviewof this policy statement.
ABBREVIATIONS
SFSP: Summer Food ServiceProgram
SNAP: Supplemental NutritionAssistance Program
USDA: US Department ofAgriculture
WIC: Special SupplementalNutrition Program forWomen, Infants, andChildren
REFERENCES
1. Coleman-Jensen A, Gregory C, Singh A.Household Food Security in the UnitedStates in 2013. Publication no. ERR-173.Washington, DC: US Department ofAgriculture, Economic Research Service;September 2014
2. Coleman-Jensen A, McFall W, Nord M.Food Insecurity in Households WithChildren: Prevalence, Severity, andHousehold Characteristics, 2010–11.Publication no. EIB-1. Washington, DC: USDepartment of Agriculture, EconomicResearch Service; May 2013
3. Gundersen C. Food insecurity is anongoing national concern. Adv Nutr.2013;4(1):36–41
4. US Food Security: Before and After theGreat Recession. Washington, DC: USDepartment of Agriculture, EconomicResearch Service; April 2015. Availableat: www.ers.usda.gov/data-products/food-security-in-the-united-states/interactive-chart-food-security-trends.aspx. Accessed August 12, 2015
5. Calkins K, Devaskar SU. Fetal origins ofadult disease. Curr Probl PediatrAdolesc Health Care. 2011;41(6):158–176
6. Portrait F, Teeuwiszen E, Deeg D. Early lifeundernutrition and chronic diseases atolder ages: the effects of the Dutchfamine on cardiovascular diseases anddiabetes. Soc Sci Med. 2011;73(5):711–718
7. Cook JT, Black M, Chilton M, et al. Arefood insecurity’s health impacts
underestimated in the US population?Marginal food security also predictsadverse health outcomes in youngUS children and mothers. Adv Nutr. 2013;4(1):51–61
8. Eicher-Miller HA, Mason AC, Weaver CM,McCabe GP, Boushey CJ. Food insecurityis associated with iron deficiencyanemia in US adolescents. Am J ClinNutr. 2009;90(5):1358–1371
9. Skalicky A, Meyers AF, Adams WG, Yang Z,Cook JT, Frank DA. Child food insecurityand iron deficiency anemia in low-income infants and toddlers in theUnited States. Matern Child Health J.2006;10(2):177–185
10. Rose-Jacobs R, Black MM, Casey PH,et al. Household food insecurity:associations with at-risk infant andtoddler development. Pediatrics. 2008;121(1):65–72
11. Jyoti DF, Frongillo EA, Jones SJ. Foodinsecurity affects school children’sacademic performance, weight gain, andsocial skills. J Nutr. 2005;135(12):2831–2839
12. Whitaker RC, Phillips SM, Orzol SM. Foodinsecurity and the risks of depressionand anxiety in mothers and behaviorproblems in their preschool-agedchildren. Pediatrics. 2006;118(3).Available at: www.pediatrics.org/cgi/content/full/118/3/e859
13. Mabli J, Cohen R, Potter F, Zhao Z. Hungerin America 2010. National ReportPrepared for Feeding America.Princeton, NJ: Mathematica PolicyResearch Inc; 2010
14. Chilton M, Black MM, Berkowitz C, et al.Food insecurity and risk of poor healthamong US-born children of immigrants.Am J Public Health. 2009;99(3):556–562
15. Mabli J, Worthington J. SupplementalNutrition Assistance Programparticipation and child food security.Pediatrics. 2014;133(4):610–619
16. Bartfeld JS, Ahn HM. The SchoolBreakfast Program strengthenshousehold food security among low-income households with elementaryschool children. J Nutr. 2011;141(3):470–475
17. Shonkoff JP, Garner AS; Committee onPsychosocial Aspects of Child and FamilyHealth; Committee on Early Childhood,Adoption, and Dependent Care; Section
on Developmental and BehavioralPediatrics. The lifelong effects of earlychildhood adversity and toxic stress.Pediatrics. 2012;129(1). Available at:www.pediatrics.org/cgi/content/full/129/1/e232
18. Hanson KL, Connor LM. Food insecurityand dietary quality in US adults andchildren: a systematic review. Am J ClinNutr. 2014;100(2):684–692
19. Eicher-Miller HA, Mason AC, Weaver CM,McCabe GP, Boushey CJ. Food insecurityis associated with diet and bone massdisparities in early adolescent malesbut not females in the United States.J Nutr. 2011;141(9):1738–1745
20. Institute of Medicine. Hunger andObesity: Understanding a Food InsecurityParadigm: Workshop Summary. Washington,DC: National Academies Press; 2011
21. Laraia BA. Food insecurity and chronicdisease. Adv Nutr. 2013;4(2):203–212
22. Larson NI, Story MT, Nelson MC.Neighborhood environments: disparitiesin access to healthy foods in the US.Am J Prev Med. 2009;36(1):74–81
23. Cutler-Triggs C, Fryer GE, Miyoshi TJ,Weitzman M. Increased rates andseverity of child and adult foodinsecurity in households with adultsmokers. Arch Pediatr Adolesc Med.2008;162(11):1056–1062
24. Alaimo K, Olson CM, Frongillo EA. Familyfood insufficiency, but not low familyincome, is positively associated withdysthymia and suicide symptoms inadolescents. J Nutr. 2002;132(4):719–725
25. Fram MS, Frongillo EA, Jones SJ, et al.Children are aware of food insecurityand take responsibility for managingfood resources. J Nutr. 2011;141(6):1114–1119
26. Fram MS, Ritchie LD, Rosen N, FrongilloEA. Child experience of food insecurity isassociated with child diet and physicalactivity. J Nutr. 2015;145(3):499–504
27. Connell CL, Lofton KL, Yadrick K, RehnerTA. Children’s experiences of foodinsecurity can assist in understandingits effect on their well-being. J Nutr.2005;135(7):1683–1690
28. Colman S, Nichols-Barrer IP, Fedline JE,Devaney BL, Ansell SV. Effects of theSpecial Supplemental Nutrition Programfor Women, Infants, and Children (WIC): AReview of Recent Research. US
PEDIATRICS Volume 136, number 5, December 2015 e1437by guest on April 6, 2016Downloaded from

Department of Agriculture, Food andNutrition Service, Office of Research andAnalysis. Report WIC-12-WM. Alexandria,VA: US Department of Agriculture; 2012
29. Black MM, Cutts DB, Frank DA, et al;Children’s Sentinel NutritionalAssessment Program Study Group.Special Supplemental Nutrition Programfor Women, Infants, and Childrenparticipation and infants’ growth andhealth: a multisite surveillance study.Pediatrics. 2004;114(1):169–176
30. Mabli J, Ohls J, Dragoset L, Castner L,Santos B. Measuring the Effect ofSupplemental Nutrition AssistanceProgram (SNAP) Participation on FoodSecurity. US Department of Agriculture,Food and Nutrition Service. Alexandria, VA:US Department of Agriculture; 2013
31. Supplemental Nutrition AssistanceProgram. How much could I receive.2014. Available at: www.fns.usda.gov/snap/how-much-could-i-receive.Accessed August 30, 2015
32. US Department of Agriculture. SummerElectronic Benefit Transfer for Children(SEBTC). Available at: www.fns.usda.gov/ops/summer-electronic-benefit-transfer-children-sebtc. Accessed August 12, 2015
33. Logan CW, Connor P, Harvill EL, et al.Community Eligibility Provision
Evaluation. Alexandria, VA: USDepartment of Agriculture, Food andNutrition Service; 2014
34. Schwartz MB, Henderson KE, Read M,Danna N, Ickovics JR. New schoolmeal regulations increase fruitconsumption and do not increase totalplate waste. Child Obes. 2015;11(3):242–247
35. Hager ER, Quigg AM, Black MM, et al.Development and validity of a 2-itemscreen to identify families at risk forfood insecurity. Pediatrics. 2010;126(1).Available at: www.pediatrics.org/cgi/content/full/126/1/e26
36. Larson C, Haushalter A, Buck T, CampbellD, Henderson T, Schlundt D. Developmentof a community-sensitive strategy toincrease availability of fresh fruits andvegetables in Nashville’s urban fooddeserts, 2010–2012. Prev Chronic Dis.2013;10:E125
37. Rezet B, Risko W, Blaschke GS; DysonCommunity Pediatrics Training InitiativeCurriculum Committee. Competency incommunity pediatrics: consensusstatement of the Dyson InitiativeCurriculum Committee. Pediatrics. 2005;115(4 suppl):1172–1183
38. Kuo AA, Etzel RA, Chilton LA, Watson C,Gorski PA. Primary care pediatrics and
public health: meeting the needs oftoday’s children. Am J Public Health.2012;102(12):e17–e23
39. Minkovitz CS, Grason H, Solomon BS, KuoAA, O’Connor KG. Pediatricians’involvement in community child healthfrom 2004 to 2010. Pediatrics. 2013;132(6):997–1005
40. O’Toole JK, Burkhardt MC, Solan LG,Vaughn L, Klein MD. Residentconfidence addressing social history:is it influenced by availability ofsocial and legal resources? ClinPediatr (Phila). 2012;51(7):625–631
41. Burkhardt MC, Beck AF, Conway PH, KahnRS, Klein MD. Enhancing accurateidentification of food insecurity usingquality-improvement techniques.Pediatrics. 2012;129(2). Available at:www.pediatrics.org/cgi/content/full/129/2/e504
42. Risko W, Chi G, Palfrey J, eds; Anne EDyson Community PediatricsTraining Initiative CurriculumCommittee. Community PediatricsCurriculum. Elk Grove Village, IL:American Academy of Pediatrics;2005. Available at: https://www2.aap.org/commpeds/cpti/Curriculum-Bod-2005.pdf. Accessed August 12,2015
e1438 FROM THE AMERICAN ACADEMY OF PEDIATRICSby guest on April 6, 2016Downloaded from
DOI: 10.1542/peds.2015-3301; originally published online October 23, 2015; 2015;136;e1431Pediatrics
COUNCIL ON COMMUNITY PEDIATRICS and COMMITTEE ON NUTRITIONPromoting Food Security for All Children
ServicesUpdated Information &
/content/136/5/e1431.full.htmlincluding high resolution figures, can be found at:
References
/content/136/5/e1431.full.html#ref-list-1at:This article cites 31 articles, 22 of which can be accessed free
Citations /content/136/5/e1431.full.html#related-urls
This article has been cited by 4 HighWire-hosted articles:
Subspecialty Collections
/cgi/collection/nutrition_subNutritionthe following collection(s):This article, along with others on similar topics, appears in
Permissions & Licensing
/site/misc/Permissions.xhtmltables) or in its entirety can be found online at: Information about reproducing this article in parts (figures,
Reprints /site/misc/reprints.xhtml
Information about ordering reprints can be found online:
rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Grove Village, Illinois, 60007. Copyright © 2015 by the American Academy of Pediatrics. All and trademarked by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elkpublication, it has been published continuously since 1948. PEDIATRICS is owned, published, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
by guest on April 6, 2016Downloaded from

DOI: 10.1542/peds.2015-3301; originally published online October 23, 2015; 2015;136;e1431Pediatrics
COUNCIL ON COMMUNITY PEDIATRICS and COMMITTEE ON NUTRITIONPromoting Food Security for All Children
/content/136/5/e1431.full.html
located on the World Wide Web at: The online version of this article, along with updated information and services, is
of Pediatrics. All rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Boulevard, Elk Grove Village, Illinois, 60007. Copyright © 2015 by the American Academy published, and trademarked by the American Academy of Pediatrics, 141 Northwest Pointpublication, it has been published continuously since 1948. PEDIATRICS is owned, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
by guest on April 6, 2016Downloaded from

Perspectives on Eating Patterns of Young Children at Risk for Development of Malnutrition and Poor Growth Susan L. Johnson, PhD, University of Colorado School of Medicine, Department of Pediatrics, Section of Nutrition Learning Objectives: 1. Describe the dietary intakes of young children, with specific emphasis on at risk populations.
a. Nutrient intakes of young children—in general, the nutrient profiles of young children’s dietary intakes are adequate.
b. Food intake patterns of young children—the food intake patterns of young children are best at about 1 year of age and decrease throughout early childhood.
c. Influences and relationships of SES with patterns of dietary intake—money and time matter but when low income mother buy and eat healthy foods, their preschoolers are more likely to eat them too.
d. Influence of setting on dietary intake patterns (home and child care).
2. Examine the feeding practices of caregivers of young children, including motivations and concerns related to poverty and time and the perspectives of different cultures. a. Feeding practices associated with poor child outcomes—using pressuring or restrictive
tactics to try to get children to eat can win the short term struggle but long term seems to relate to poor food acceptance patterns.
b. Positive feeding practices and children’s food intake—noticing when children do the right thing and pointing it out (as opposed to focusing on the negative) takes more effort but can lead to better habits.
c. Maternal perspectives on feeding young children—concerns, beliefs, goals. Mothers use different feeding strategies with “picky” children than they do with “good eaters.” Fears of wasting food, time and money are important barriers to healthy meals for children. Mothers may not believe that it is possible to help her child learn to like a new food.
d. Caregiver child feeding strategies sometimes relate to how they were fed as children.
3. Consider the implications of caregiver perspectives and how they may influence the nutrition professional's opportunities and strategies for facilitating positive change. a. The financial and time implications for offering children novel, less energy-dense foods is
critical for low income populations. b. Being empathetic to maternal concerns about children’s growth and development is
important for establishing relationship that allows you to offer nutrition advice. c. Focus on convenience for stressed mothers and caregivers. d. Encouraging understanding from the child’s point of view (what it’s like to be asked to eat
things you don’t like and what it is like to be unsure of when food will be available and offered).
Slides are available upon request by emailing me at: [email protected]

Resources:
http://www.nytimes.com/interactive/2016/04/11/upshot/for-the-poor-geography-is-life-and-death.html?hp&action=click&pgtype=Homepage&clickSource=story-heading&module=photo-spot-region®ion=top-news&WT.nav=top-news&_r=0
The Health Inequality Project
https://healthinequality.org/
Chetty R, Stepner M, Abraham S, Lin S, Scuderi B, Turner N, Bergeron A, Cutler D (2016). The Association Between Income and Life Expectancy in the United States, 2001-2014.
Hunger in America
http://www.worldhunger.org/articles/Learn/us_hunger_facts.htm
http://www.feedingamerica.org/hunger-in-america/impact-of-hunger/hunger-and-poverty/hunger-and-poverty-fact-sheet.html?referrer=https://www.google.com/
http://www.feedingamerica.org/hunger-in-america/impact-of-hunger/child-hunger/child-hunger-fact-sheet.html
The Hunger Obesity Paradox
http://frac.org/initiatives/hunger-and-obesity/
References:
The Hunger Obesity Paradox
1. Koh KA, Hoy JS, O’Connell JJ, Montgomery P. The hunger–obesity paradox: obesity in the homeless. Journal of Urban Health. 2012 Dec 1;89(6):952-64.
2. Scheier LM. What is the hunger-obesity paradox?. Journal of the American Dietetic Association. 2005 Jun 30;105(6):883-5.
3. Dinour LM, Bergen D, Yeh MC. The food insecurity–obesity paradox: a review of the literature and the role food stamps may play. Journal of the American Dietetic Association. 2007 Nov 30;107(11):1952-61.
What children are eating:
1. Fox MK, Condon E, Briefel RR, Reidy KC, Deming DM. Food consumption patterns of young preschoolers: are they starting off on the right path? Journal of the American Dietetic Association. 2010;110(12):S52-S59.
2. Manios Y, Kourlaba G, Kondaki K, et al. Diet quality of preschoolers in Greece based on the Healthy Eating Index: the GENESIS study. Journal of the American Dietetic Association. 2009;109(4):616-623.

3. Huybrechts I, Matthys C, Vereecken C, et al. Food intakes by preschool children in Flanders compared with dietary guidelines. International Journal of Environmental Research and Public Health. 2008;5(4):243-257.
Home influences on children’s eating:
1. Russell CG, Worsley A. Why don’t they like that? And can I do anything about it? The nature and correlates of parents’ attributions and self-efficacy beliefs about preschool children’s food preferences. Appetite. 2013;66:34-43.
2. Burdell A, Bellows, LL, Johnson, SL, Davies, PL, Gavin, WJ, Boles, RE. Home Food Availability Predicts Dietary Intake in a Diverse, Rural Sample of Preschool-aged Children International Journal of Behavioral Nutrition and Physical Activity. Submitted.
3. Cook LT, O’Reilly GA, DeRosa CJ, Rohrbach LA, Spruijt-Metz D. Association between home availability and vegetable consumption in youth: a review. Public Health Nutrition. 2014:1-9.
4. Cullen KW, Baranowski T, Owens E, Marsh T, Rittenberry L, de Moor C. Availability, accessibility, and preferences for fruit, 100% fruit juice, and vegetables influence children's dietary behavior. Health Education & Behavior. 2003;30(5):615-626.
Feeding practices of caregivers of young children:
1. Rhee K. Childhood overweight and the relationship between parent behaviors, parenting style ' and family functioning. Ann Am Acad Pol Soc Sci. 2008;615:12-37.
2. Blissett J. Relationships between parenting style, feeding style and feeding practices and fruit and vegetable consumption in early childhood. Appetite. 2011;57(3):826-831.
3. Baumrind D. Prototypical descriptions of 3 parenting styles. Psychology. 1966;37. 4. Black MM, Aboud FE. Responsive feeding is embedded in a theoretical framework of responsive
parenting. J Nutr. 2011;141(3):490-494. 5. Satter EM. The feeding relationship. J Am Diet Assoc. 1986;86(3):352-356. 6. O'Connor TM, Hughes SO, Watson KB, Baranowski T, Nicklas TA, Fisher JO, Beltran A, Baranowski
JC, Qu H, Shewchuk RM. Parenting practices are associated with fruit and vegetable consumption in pre-school children. Public Health Nutr. 2010;13(1):91-101.
7. Kiefner-Burmeister AE, Hoffmann DA, Meers MR, Koball AM, Musher-Eizenman DR. Food consumption by young children: a function of parental feeding goals and practices. Appetite. 2014;74:6-11.
8. Baranowski T, Chen TA, O'Connor T, Hughes S, Beltran A, Frankel L, Diep C, Baranowski JC. Dimensions of vegetable parenting practices among preschoolers. Appetite. 2013;69:89-93.
9. Murashima M, Hoerr SL, Hughes SO, Kaplowitz SA. Feeding behaviors of low-income mothers: directive control relates to a lower BMI in children, and a nondirective control relates to a healthier diet in preschoolers. Am J Clin Nutr. 2012;95(5):1031-1037.
10. Kaar JL, Shapiro AL, Johnson SL. Parental feeding practices, food neophobia and child food preferences: What combination of factors results in children eating their vegetables? Food Preference and Quality. 2016; 50:57-64.
11. Boles RE, Halbower AC, Daniels S, Gunnarsdottir T, Whitesell N, Johnson SL. Family Chaos and Child Functioning in Relation to Sleep Problems Among Children at Risk for Obesity. Behavioral Sleep Medicine. 2016;00:1-15.
12. Johnson SL, Goodell LS, Williams K, Power TG, Hughes SO (2014). Getting my child to eat the right amount: Mothers' considerations when deciding how much food to offer their child at a meal. Appetite, doi:10.1016/j.appet.2014.12.004

13. Johnson SL, Hughes SO, Cui X, Li X, Allison DB, Liu Y, Goodell S, Nicklas T, Power TG, Vollrath K (2014). Portion sizes for children are predicted by parental characteristics and the amounts parents serve themselves. American Journal of Clinical Nutrition. 99(4):763-770. PMID: 24477036
14. Johnson SL, Davies PL, Boles RE, Gavin WJ, Burdell A, Bellows LL. Relations among young children’s oral sensory characteristics, food neophobia and food intake. Journal of Nutrition.2016; 145:2610-2616.
15. Goodell, LS, Johnson, SL, Antono, AC, Power, TG, Hughes, SO. Strategies Low-Income Parents Use to Influence Their Children to Like Previously Rejected Foods. Early Childhood Research Quarterly. (Under review)
Socioeconomic influences on children’s dietary intake:
1. Dave JM, Evans AE, Saunders RP, Watkins KW, Pfeiffer KA. Associations among food insecurity, acculturation, demographic factors, and fruit and vegetable intake at home in Hispanic children. Journal of the American Dietetic Association. 2009;109(4):697-701.
2. Ebenegger V, Marques-Vidal P, Nydegger A, et al. Independent contribution of parental migrant status and educational level to adiposity and eating habits in preschool children. European Journal of Clinical Nutrition. 2011;65(2):210-218.
3. Darmon N, Drewnowski A. Does social class predict diet quality? The American Journal of Clinical Nutrition. 2008;87(5):1107-1117.

Eat Smart Idaho: Promoting Healthy Eating and Lifestyle Changes through Statewide Partnerships
Julie Harker Buck Ed. D., MHE, RDN, University of Idaho Extension
Learning Objectives:
1. Review programming efforts by University of Idaho Extension Eat Smart Idaho's interventions, partnerships, monitoring and evaluation.
• Intervention: Food pantries, both private and schools • Partnerships: Schools, Head Start, Summer feeding sites, Employment training,
Detention/probation, Crisis centers, Firemen, Local “heroes”, grocery stores, USPS, statewide campaign to be released June 1
• Monitoring and evaluation: Surveys, classes, grant programs
2. State evaluation techniques for chronic health conditions which can be influenced by nutrition programming to persons with low resources.
• Low literacy surveys • Picture surveys • Social media
3. Discuss and plan community efforts to help with hunger and food insecurity in Idaho.
• EatSmart Idaho http://www.uidaho.edu/extension/eat-smart-idaho Facebook #eatsmartidaho • Food Banks in Idaho 208-336-9643 [email protected] http://idahofoodbank.org • Farmers Markets in Idaho http://www.farmersmarketonline.com/fm/Idaho.htm
Eileen Stachowski, Idaho Farmers Market Association [email protected] (208) 639-0030 • Schools and churches may have food pantries not on a registry or be interested in starting one.
Resources for EatSmart Idaho programming
Northern District: Kali Gardner, Coordinator 208-446-1686 [email protected]
Western District: Bridget Aman, Coordinator 208-454-7672 [email protected]
Southern District: Cammie Jayo, Coordinator 208-734-9590 [email protected]
Eastern District: Sarah Hulse, Coordinator 208-236-7315 [email protected]
State Coordinator: Kristin Hansen 208-885-6872 [email protected]
Julie Harker Buck, EdD, MHE, RDN University of Idaho Extension, Bannock County 208.236.7310 [email protected]