controversies in prehospital endotracheal intubation · do not reproduce without permission. 1...
TRANSCRIPT

Henry E. Wang, MD, MS 1/6/2019
Do not reproduce without permission. 1
Controversies in Prehospital Endotracheal Intubation
Henry E. Wang, MD, MS
Professor and Vice Chair for Research
Department of Emergency Medicine
The University of Texas Health Science Center at Houston
McGovern Medical School at UTHealth
McGovern Medical School at UTHealth
Disclosures
• NIH Grant Support• UH2/UH3-HL125163
• PI, Pragmatic Airway Resuscitation Trial

Henry E. Wang, MD, MS 1/6/2019
Do not reproduce without permission. 2
McGovern Medical School at UTHealth
Why Intubate in the Field?
• Provide direct conduit to lungs
• Improve ventilation
• Prevent aspiration
• Parallels in-hospital care
• Ultimate goal � “Save lives”
www.trauma.org
McGovern Medical School at UTHealth
“Does Prehospital Intubation
Improve Outcomes
(Save Lives)?”

Henry E. Wang, MD, MS 1/6/2019
Do not reproduce without permission. 3
McGovern Medical School at UTHealth
Does Intubation Save Lives?
• >20 studies of prehospital intubation and outcome (survival)
• Recurrent theme:• Prehospital intubation associated with increased risk of death
• Prehospital intubation associated with poorer neurological outcome
McGovern Medical School at UTHealth
Prehospital Intubation of Children
• Gausche, JAMA 2000
• RCT
• [BVM ± ETI] vs. BVM-only
• 830 children
• No difference in survival
• No difference in neurological outcome

Henry E. Wang, MD, MS 1/6/2019
Do not reproduce without permission. 4
McGovern Medical School at UTHealth
Prehospital RSI for TBI
• Davis, J Trauma 2003
• Implementation of Prehospital
Rapid Sequence Intubation
• 209 pts compared with 627
historical controls
• RSI associated with increased
death
• OR: 1.6 [1.1-2.2]
McGovern Medical School at UTHealth
Prehospital Intubation and TBI
• Wang, et al., Ann Emerg Med 2004
• Pennsylvania statewide trauma data
• 4,098 TBI• Prehospital vs. Emergency Department ETI
• Excluded non-intubated cases
• Prehospital Intubation • 4x increased death
• 1.6x increased poor neuro outcome

Henry E. Wang, MD, MS 1/6/2019
Do not reproduce without permission. 5
McGovern Medical School at UTHealth
“Are Poor Outcomes Due to Errors?”
McGovern Medical School at UTHealth
Endotracheal Tube Misplacement
• Katz and Falk, Ann EmergMed 1999
• N=108 prehospital intubations
• Systematic reconfirmation in ED
• 25% tube misplacement rate
• 2/3 esophageal
• 1/3 above vocal cords

Henry E. Wang, MD, MS 1/6/2019
Do not reproduce without permission. 6
McGovern Medical School at UTHealth
Oxygen Desaturation and Bradycardia
• Dunford, Annals EM 2004
• San Diego RSI Trial
• N=152 RSI patients
• Continuously recorded waveforms:
• Heart Rate
• Oxygen Saturation
• End-Tidal Capnography
McGovern Medical School at UTHealth
Dunford, et al. Ann Emerg Med 2004
ETCO2ETCO2
HRHR
SaO2SaO2
Oxygen Desaturation and Bradycardia

Henry E. Wang, MD, MS 1/6/2019
Do not reproduce without permission. 7
McGovern Medical School at UTHealth
Oxygen Desaturation and Bradycardia
• Oxygen desaturation: 31 (57%)
• Median duration: 160 seconds (IQR 48 to 272)
• Median desaturation (SpO2): 22%
• Bradycardia: 6 (19%)
• Pulse rate <50 beats/min
• Paramedics described intubation as "easy" in 84%
“Does Intubation Interact with
other Interventions?”

Henry E. Wang, MD, MS 1/6/2019
Do not reproduce without permission. 8
McGovern Medical School at UTHealth
Intubation � Hyperventilation � BAD
• Harmful in TBI
• ↑ Vent � ↓ pCO2
� ↓ Cerebral Perfusion
• Davis, J Trauma 2004
• May be harmful during CPR
• ↑ Vent � ↑ Intrathoracic Pressure
� ↓ Coronary Perfusion
• Aufderheide Crit Care Med 2004
• Aufderheide Circulation 2004
McGovern Medical School at UTHealth
CPR Chest Compressions
• ACLS Guidelines:
• “Avoid CPR Chest
Compression Interruptions”
• New CPR detection
technology
• Can “see” delivered chest
compressions

Henry E. Wang, MD, MS 1/6/2019
Do not reproduce without permission. 9
Example of CPR Interruption from Intubation
ET Tube
Placement
30 sec CPR
Interruption
ETCO2
Signal
McGovern Medical School at UTHealth
Intubation-Associated Chest Compression Interruptions
• Wang, Annals EM 2009
• Pittsburgh
• N=100
• Review of CPR process files and audio recordings
• Identified all CPR interruptions due to intubation efforts

Henry E. Wang, MD, MS 1/6/2019
Do not reproduce without permission. 10
McGovern Medical School at UTHealth
010
20
30
40
Perc
enta
ge o
f P
atients
1 2 3 4 5 6 7 8 9Total Number of CPR Interruptions
Intubation-Associated CPR Interruptions
Median: 2 Interruptions
(IQR: 1-3)
Min 1, Max 9
30% >2 Interruptions
Wang, et al., Ann Emerg Med 2009
Pittsburgh, n=100
0 30 60 90 120 150 180 210 240 270 300 330 360 390 420 450Duration (sec)
Sum
Subsequent
First
Duration of Intubation-Associated CPR Interruptions
First CPR Interruption
Median: 46.5 sec (IQR: 23.5-73)
Min 7, Max 221
~30% >60 sec
Subsequent CPR Interruptions
Median: 35 sec (IQR: 21-58)
Min 7, Max 199
~20% >60 sec
Sum of All CPR Interruptions
Median: 109.5 sec (IQR: 54-198)
Min 13, Max 446
~25% >180 sec
Wang, et al., Ann Emerg Med 2009

Henry E. Wang, MD, MS 1/6/2019
Do not reproduce without permission. 11
“Does Training Play a Role?”
Intubation is Difficult in Prehospital Mosh Pit
“There’s no such
thing as an easy
prehospital airway”
“Paramedics need
exceptional
intubation skills”

Henry E. Wang, MD, MS 1/6/2019
Do not reproduce without permission. 12
McGovern Medical School at UTHealth
How Many Intubations Do You Need to Graduate in the US?
• Emergency Med Residents 35
• Anesthesia Residents 20-57
• CRNA Students 200
• Paramedic Students 5
010
20
30
40
Perc
enta
ge o
f P
rogra
ms
1-4 hrs 5-8 hrs 9-16 hrs 17-32 hrs >32 hrsOR Hours
Paramedic Student Operating Room Training Hours
Median 17-32 hours
Johnston, et al., Acad Emerg Med 2006

Henry E. Wang, MD, MS 1/6/2019
Do not reproduce without permission. 13
McGovern Medical School at UTHealth
Paramedic Student Operating Room Barriers
• Competition from other
students
• Widespread Laryngeal
Mask Airway use
• Anesthesiologists’
medicolegal concerns
McGovern Medical School at UTHealth
“Skill”
(“Proficiency”)=
Baseline
Training+
Regular
Application
Intubation Skill

Henry E. Wang, MD, MS 1/6/2019
Do not reproduce without permission. 14
Intubations Per ParamedicPennsylvania 2003
Median ETI: 1 (IQR 0-3)
39% performed no ETI
67% performed 2 or fewer ETI
Wang, et al. Crit Care Med 2005
McGovern Medical School at UTHealth
“We Have a Problem . . .”
• Prehospital ETI clinical benefit not proven
• Prone to error
• Difficult
• Interacts with other interventions
• Performed under worst possible conditions
• Limited training

Henry E. Wang, MD, MS 1/6/2019
Do not reproduce without permission. 15
McGovern Medical School at UTHealth
“There is an Alternative…”
Supraglottic Airways (SGA)
• Easier technique
• Less training required
• Similar ventilation to ETI
• Increasing use as primary airway in OHCA
King Laryngeal Tube (LT) Laryngeal Mask Airway
(LMA)
i-gel

Henry E. Wang, MD, MS 1/6/2019
Do not reproduce without permission. 16
McGovern Medical School at UTHealth
Supraglottic Airways Instead of Intubation� COMMON SENSE
• Simple, easy, reliable
• “Put it in… Forget about it…”
• “Move on to the more important parts of resuscitation”
McGovern Medical School at UTHealth
“SGA vs ETI – Unexpected Results”

Henry E. Wang, MD, MS 1/6/2019
Do not reproduce without permission. 17
ETI vs. SGA in Cardiac ArrestROC PRIMED Trial
10,455 OHCA
8,457 ETI 1,968 SGA
296 Combitube 239 LMA909 King 518 Unknown

Henry E. Wang, MD, MS 1/6/2019
Do not reproduce without permission. 18
ETI Wins over SGA (Oops…)
Wang, Resuscitation 2012

Henry E. Wang, MD, MS 1/6/2019
Do not reproduce without permission. 19
McMullan, Resuscitation 2014
Favo
r E
TI
Favo
r S
GA
N=5,591 ETI
N=3,110 SGA
N=5,591 ETI
N=3,110 SGA
McGovern Medical School at UTHealth
This is Not What We Expected
• ETI • Difficult, slow, error-prone
• SGA• Easier, faster
• Less impact on CPR
• Similar Ventilation
SGA Should WinSGA Should Win

Henry E. Wang, MD, MS 1/6/2019
Do not reproduce without permission. 20
Could SGAs Impede Carotid Blood Flow?Segal, Resuscitation 2012
N = 4 pigs
McGovern Medical School at UTHealth
A Randomized Trial is Necessary
• Confounding-by-indication
• Randomization is only way to
overcome confounding-by-indication

Henry E. Wang, MD, MS 1/6/2019
Do not reproduce without permission. 21
McGovern Medical School at UTHealth
“Three Landmark
Airway Management Clinical Trials”
Cardiac Arrest Airway
Management Trial
(CAAM)
Jabre, et al., JAMA 2018

Henry E. Wang, MD, MS 1/6/2019
Do not reproduce without permission. 22
CAAM Design
• RCT
• France and Belgium SAMUs
• 20 EMS centers
• MD + RN + Driver
• Adult OHCA
• BVM vs. ETI• Intervention by “medical team”
• ETI post-ROSC
• Per-Patient Randomization• Sealed envelopes
• 28d Survival with Favorable Neuro Status
• “Non-inferiority” design• 1% N-I margin
• Estimated n=2,000
• March 2015 - Jan 2017
Primary Result28-day Survival with Favorable Neuro Status (CPC 1-2)
• BVM � 44 / 1018 (4.3%)
• ETI � 43 / 1022 (4.2%)
• Difference = 0.11% (1-sided 97.5% CI: -1.64% to infinity)
• Noninferiority p=0.11
“This is an uninterpretable result…”

Henry E. Wang, MD, MS 1/6/2019
Do not reproduce without permission. 23
What is a Noninferiority Margin?
NI Margin
Important Secondary Findings

Henry E. Wang, MD, MS 1/6/2019
Do not reproduce without permission. 24
Very Important Secondary Findings
%
Pragmatic Airway Resuscitation Trial (PART)
Wang, et al, JAMA 2018

Henry E. Wang, MD, MS 1/6/2019
Do not reproduce without permission. 25

Henry E. Wang, MD, MS 1/6/2019
Do not reproduce without permission. 26

Henry E. Wang, MD, MS 1/6/2019
Do not reproduce without permission. 27

Henry E. Wang, MD, MS 1/6/2019
Do not reproduce without permission. 28

Henry E. Wang, MD, MS 1/6/2019
Do not reproduce without permission. 29
Airway Management Characteristics
64.4%
94.2%
89.9%
95.5%
33.1%
91.5%
51.3%
90.7%
0% 20% 40% 60% 80% 100%
ED Intubation
Overall Airway Success
Initial Airway Success
Protocol Compliance
11.0
13.6
Arrive � Airway Start
(min)
ETI
“LT better than ETI over all outcomes”

Henry E. Wang, MD, MS 1/6/2019
Do not reproduce without permission. 30
Airways-2 Trial
Benger, et al, JAMA 2018
Airways-2 Design
• RCT
• United Kingdom• 4 EMS agencies
• Population 21 million
• 40% of UK population
• Adult OHCA
• Intubation vs i-gel
• Cluster randomized • By study paramedic
• N=1,523 medics
• Hospital Survival with Favorable Neuro Status
• Estimated n=9,070 patients
• June 2015 – August 2017
Henry E. Wang, MD, MS 1/6/2019
Do not reproduce without permission. 31
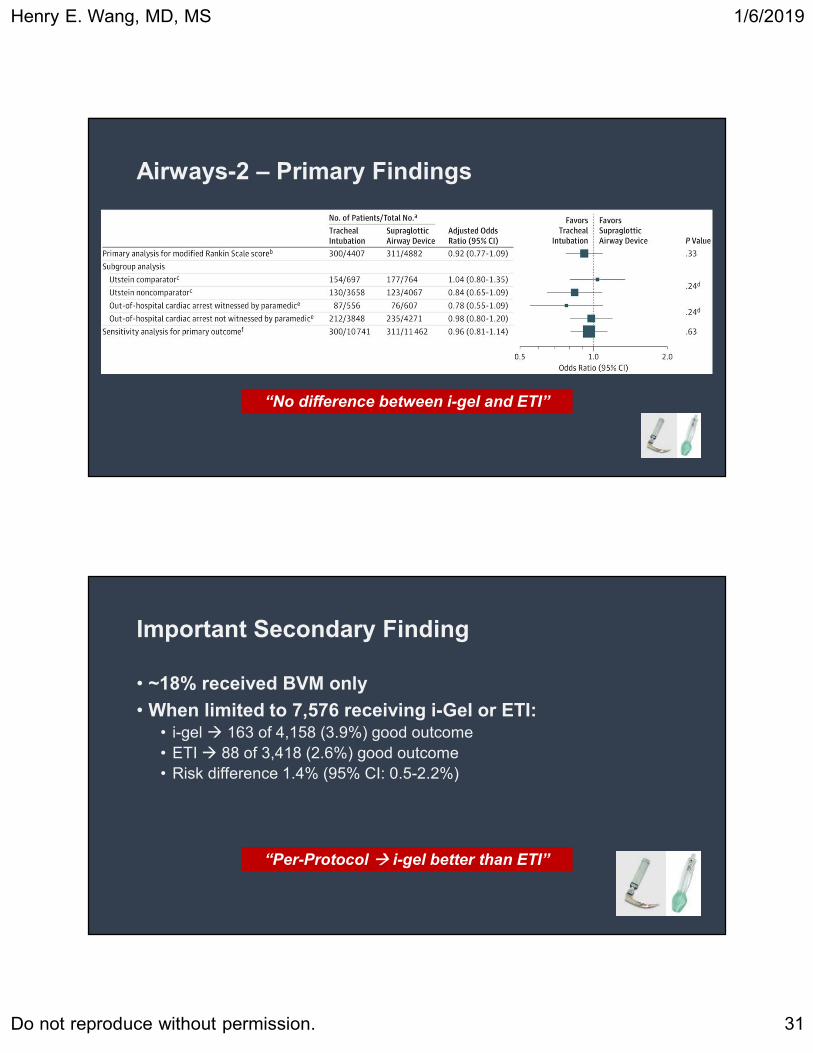
Airways-2 – Primary Findings
“No difference between i-gel and ETI”
Important Secondary Finding
• ~18% received BVM only
• When limited to 7,576 receiving i-Gel or ETI:• i-gel � 163 of 4,158 (3.9%) good outcome
• ETI � 88 of 3,418 (2.6%) good outcome
• Risk difference 1.4% (95% CI: 0.5-2.2%)
“Per-Protocol � i-gel better than ETI”
Henry E. Wang, MD, MS 1/6/2019
Do not reproduce without permission. 32
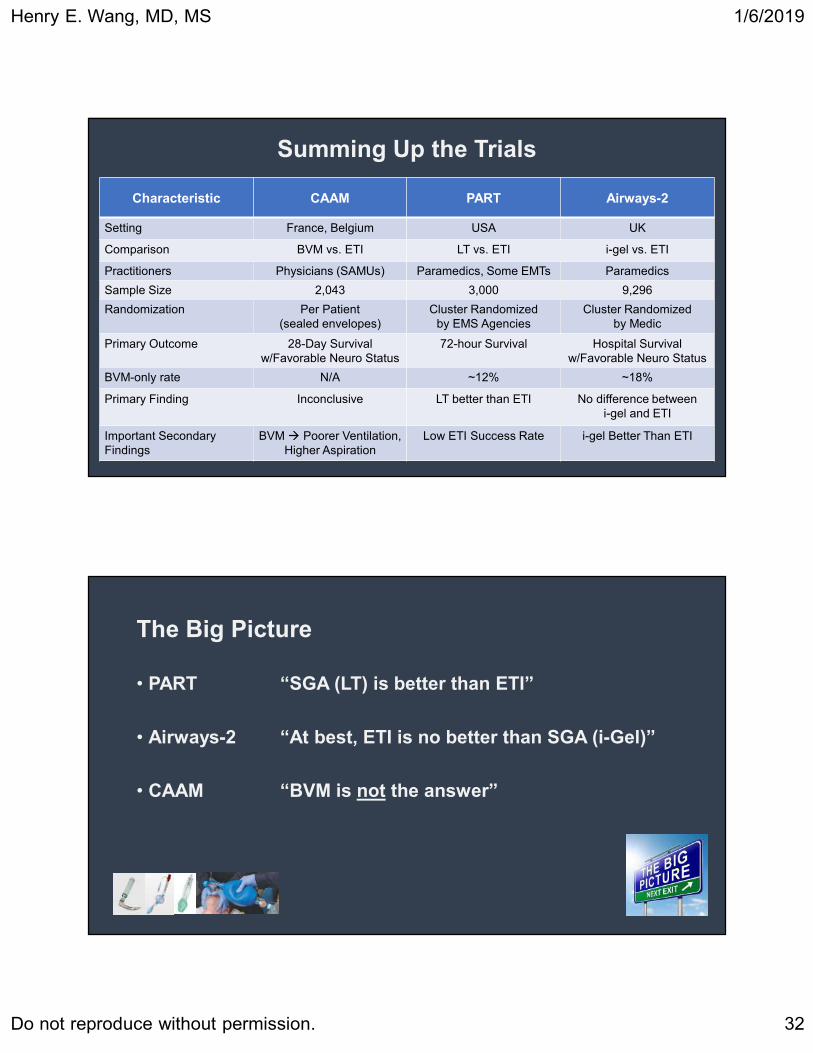
Summing Up the Trials
Characteristic CAAM PART Airways-2
Setting France, Belgium USA UK
Comparison BVM vs. ETI LT vs. ETI i-gel vs. ETI
Practitioners Physicians (SAMUs) Paramedics, Some EMTs Paramedics
Sample Size 2,043 3,000 9,296
Randomization Per Patient
(sealed envelopes)
Cluster Randomized
by EMS Agencies
Cluster Randomized
by Medic
Primary Outcome 28-Day Survival
w/Favorable Neuro Status
72-hour Survival Hospital Survival
w/Favorable Neuro Status
BVM-only rate N/A ~12% ~18%
Primary Finding Inconclusive LT better than ETI No difference between
i-gel and ETI
Important Secondary
Findings
BVM � Poorer Ventilation,
Higher Aspiration
Low ETI Success Rate i-gel Better Than ETI
The Big Picture
• PART “SGA (LT) is better than ETI”
• Airways-2 “At best, ETI is no better than SGA (i-Gel)”
• CAAM “BVM is not the answer”

Henry E. Wang, MD, MS 1/6/2019
Do not reproduce without permission. 33
McGovern Medical School at UTHealth
What About Chest Compression Fraction?
• CAAM• N=115
• No difference in CCF
• Airways-2• N=66
• No difference in CCF
• PART• >2,500 CPR Process Files
• Analysis in progress
How Do I Sell This to My Medics?
• “Don’t stop intubating”• “Have a healthy respect for
intubation”
• “The clinical objective is airway management”
• “Intubation is one tool for achieving airway management”
• “Choose the right mouse trap for the right time”
Henry E. Wang, MD, MS 1/6/2019
Do not reproduce without permission. 34
McGovern Medical School at UTHealth
Questions?
Henry E. Wang, MD, MS
Department of Emergency Medicine
The University of Texas Health Science Center at Houston