copd: diagnosis and assessment - amga.org · copd diagnosis and assessment objectives: • improve...
TRANSCRIPT

COPD:
Diagnosis and Assessment
Barry Make, MD
Co-Director, COPD Program
Director, Pulmonary Rehabilitation; Respiratory Care
National Jewish Health
Professor of Medicine
University of Colorado Denver School of Medicine

COPD Diagnosis and Assessment
Objectives:
• Improve patient assessment in your office setting
• Improve diagnosis in your office

COPD Challenges
What are your challenges in caring for patients with COPD?

COPD Challenges
What are your challenges in caring for COPD? A. Recognizing patients who might have COPD B. Making a diagnosis of COPD C. Assessing COPD severity D. Reducing shortness of breath E. Taking medications regularly F. Preventing hospital admissions G. Improving survival H. Improving activities I. Improving quality of life
Learning Objectives
• Make an appropriate diagnosis of COPD
– Record smoking history in all patients
– Assess respiratory symptoms in all patients
with a history of cigarette smoking
– Perform spirometry in all patients with
respiratory symptoms and a history of
cigarette smoking
– Correctly interpret spirometry

Let’s Discuss . . .
• What is COPD

COPD: Definition
• Common, preventable and treatable
• Persistent airflow limitation
• Airflow limitation usually progressive
• Enhanced inflammatory response to noxious
particles or gases
• Exacerbations and co-morbidities contribute to
overall severity in individual patients
Global Initiative for Chronic Obstructive Lung Disease. Global strategy of the
diagnosis, management, and prevention of COPD. http://www.goldcopd.org
Updated 2011.

COPD: What Are The Diagnostic
Criteria?
• Common, preventable and treatable
• Persistent airflow limitation
• Airflow limitation usually progressive
• Enhanced inflammatory response to noxious
particles or gases
• Exacerbations and co-morbidities contribute to
overall severity in individual patients
Global Initiative for Chronic Obstructive Lung Disease. Global strategy of the
diagnosis, management, and prevention of COPD. http://www.goldcopd.org
Updated 2011.
COPD Diagnostic Criteria
Two major criteria and one minor criterion
Major criteria:
1) Airflow limitation “post-bronchodilator”
2) Exposure to noxious particles or gases
(primarily cigarette smoking)
Minor criteria:
Exclusion of other conditions
Celli BR et al. Eur Respir J. 2004;23:931-946
GOLD Guidelines 2011. www.goldcopd.com Barry Make, MD

Chronic
Bronchitis Emphysema
Asthma Airflow
Obstruction ATS. AJRCCM. 1995;152:S77-121.

Chronic Bronchitis:
American Thoracic Society. AJRCCM. 1995.
Chronic productive
cough
for 3 months in each of
2 successive years
in a patient in whom
other causes of
chronic cough have
been excluded
Clinical Definition

Emphysema: Pathologic Definition
Abnormal permanent
enlargement of the
airspaces
distal to the terminal
bronchioles,
accompanied by
destruction of their
walls without
obvious fibrosis
American Thoracic Society. AJRCCM. 1995.

COPD Symptoms ? What is the most common
complaint that you hear from your
patients with COPD?
A. Chest tightness
B. Cough (productive or non-productive)
C. Dyspnea (with or without exertion)
D. Wheezing
E. Other

Can History & Physical Examination
Make a Diagnosis of COPD?
A. Yes
B. No
?

COPD Diagnosis:
History and physical exam :
• Relatively normal in early disease
• Not helpful when negative to exclude mild
disease
• Only positive in the presence of severe disease
(severe airflow limitation)
Are History and Physical Sufficient?

Suspected COPD Patients: Insight from the Basic History & Physical Exam

COPD Diagnosis:
Most patients present initially with:
1. cough and/or sputum,
2. dyspnea - but only with increased activity, or
3. a hospitalization for worsening dyspnea, with
or without increased cough, sputum
(acute exacerbation of COPD)
Insights from Medical History

Suspected COPD Patients:
Is your patient:
• A current or former smoker?
• Having a morning cough with or without sputum?
• Restricted in physical activity?
• Complaining about activity intolerance?
• Experiencing a decline in activities of daily living?
Not going grocery shopping
Using a golf cart instead of walking
No longer shopping in the mall
Reduced job performance
Insight from the Basic History & Physical Exam
Ferguson GT et al. Chest. 2000;117:1146-1161.

COPD Diagnosis:
Physical examination:
• Increased forced expiratory time (>5 seconds)
• In severe disease:
• Unable to speak complete sentences without
stopping to take a breath
• Decreased breath sounds
• Hyper-resonant percussion note
• Use of accessory respiratory muscles
Are History and Physical Sufficient?

COPD Diagnosis:
“Persistent airflow limitation” can only be
diagnosed with certainty by post-bronchodilator
spirometry
• More sensitive and accurate than peak flow
Persistent Airflow Limitation?

How can you improve assessment
for possible presence of COPD?
How should you use spirometry?

Qaseem A et al. Ann Intern Med. 2007;147:633-638.
Who Should Have Spirometry?
A) Case-finding in patients at risk – screening
B) Make a diagnosis in patients with symptoms

1) National Lung Health Education Program: www.nlhep.org.
2) Global Initiative for Chronic Obstructive Lung Disease. www.goldcopd.com.
3) ATS/ERS Task Force. Eur Respir J. 2004;23:932-946.
4) U.S. Preventive Services Task Force. Ann Intern Med. 2008;148:529-534.
5) Qaseem A et al. Ann Intern Med. 2007;147:633-638.
Use of Screening Spirometry: Summary of Recommendations
In Favor of Screening Against Screening
National Lung Health
Education Program 1
U.S Preventive Services Task
Force 4
Global Initiative for Chronic
Obstructive Pulmonary
Disease (GOLD) 2
American College of
Physicians 5
American Thoracic Society 3
European Respiratory Society 3

1. Make a diagnosis in patients with symptoms
Mandatory
2. Case-finding in patients at risk:
• Not uniformly recommended
• Lack of studies to assess whether early
diagnosis improves outcomes or smoking
cessation efforts
• Most patients with COPD do not present with
symptoms until FEV1 is < 50% of predicted
Qaseem A et al. Ann Intern Med. 2007;147:633-638.
Who Should Have Spirometry?

How can you improve your efficiency
in assessing the possible presence
of COPD?

How can you improve your efficiency
in assessing the possible presence
of COPD?
Can you use a Questionnaire?
COPD Population Screener
www.copd.org

COPD Population Screener™ (COPD-PS)
• 5 items completed by the patient – Shortness of breath (past 4 weeks)
– Productive cough
– Activity limitations (past year)
– Smoking history (entire life)
• Add up score: 0 - 10 – Score 6 to 10, breathing problems likely to be caused
by COPD
— Perform spirometry
– Score 0-5, breathing problems (if present) may have other cause, discuss with health care provider

COPD Population Screener
COPD Questionnaires
• There is currently no perfect questionnaire
• Efforts are under way to develop a better questionnaire for use with peak flow meter
– NHLBI COPD Case-Finding Grant
• ? What is the target population in need of diagnosis
• ? Can a questionnaire and peak flow identify those at high risk and indicate need for spirometry

Let’s Discuss . . .
• Spirometry
– Spirometry in your office

Spirometry in Your Office?
• Barriers to routine office spirometry use:
• Cost – equipment, personnel, time
• Complexity – equipment, personnel time, personnel training, incorporation into office and patient flow
• Knowledge deficit – spirometry role, performance, and importance
BARRIERS CAN BE OVERCOME!
Perceived Barriers

Spirometry - Perceived Barriers
Cost – equipment costs $1,000 - $2,000
• Mouthpiece & nose clip - < $2 per test
• Spirometers: www.nlhep.org

Billing for Spirometry
• Billing codes and reimbursement for simple
spirometry vary by region
Reimbursement - about $25
• Use spirometry code 94010 in conjunction with an
ICD-9-CM code representing symptoms or suspected
diagnosis
Spirometry code 94060 for before and after
bronchodilator testing
National Lung Health Education Program: www.nlhep.org

Billing for Spirometry
Diagnostic codes for use with spirometry:
• Cough (786.2)
• Simple chronic bronchitis (491.0)
• Muco-purulent chronic bronchitis (491.1)
• Acute bronchitis (466.0)
• COPD (496.0)
• Shortness of breath (786.05)
• Restrictive lung disease (515)
• Asthma (493.91)
National Lung Health Education Program: www.nlhep.org
Spirometry Procedure
• Maximal, forced exhalation after a maximal
inhalation into a spirometer
• Need two reproducible efforts to assure
maximum values are obtained
• Patient may be seated (preferred) or standing,
but use the same position on subsequent tests
• Nose clip is preferred
• Coaching is essential
AAFP and ATS statements on spirometry
http://www.aafp.org/afp/20040301/1107.htm (Accessed 01/03/2009)
http://www.thoracic.org/sections/publications/statements/pages/pfet/pft2.html (Accessed 01/03/2009)

Spirometry Measures
• FVC (FEV6) – Forced Vital Capacity
Total volume of air exhaled with a maximally
forced effort from a full inspiration
• FEV1 - Forced Expiratory Volume in One Second
Maximal volume of air exhaled in the first second
of a forced expiration from full inspiration
• FEV1 /FVC – Ratio of FEV1 divided by FVC (FEV6)
©Copyright 2011 National Jewish
Health

Spirometry in Normal & Airflow Limitation
Normal
0 1 2 3 4 5 6
Time (seconds)
Vo
lum
e (
lite
rs)
1
2
3
4
5
6

Spirometry in Normal & Airflow Limitation
Normal
0 1 2 3 4 5 6
Time (seconds)
Vo
lum
e (
lite
rs)
1
2
3
4
5
6

Spirometry in Normal & Airflow Limitation
Normal
FEV1
0 1 2 3 4 5 6
FVC
Time (seconds)
Vo
lum
e (l
iter
s)
1
2
3
4
5
6
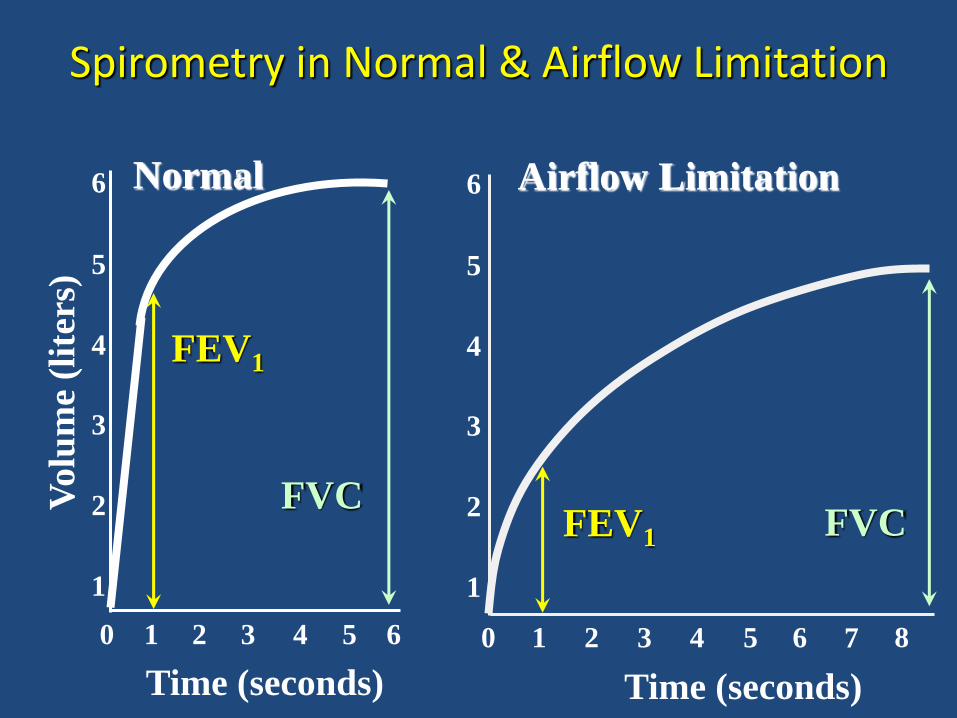
Spirometry in Normal & Airflow Limitation
Airflow Limitation
FEV1
0 1 2 3 4 5 6
1
2
3
4
5
6
7 8
FVC
Time (seconds)
Normal
FEV1
0 1 2 3 4 5 6
FVC
Time (seconds)
Vo
lum
e (l
iter
s)
1
2
3
4
5
6

COPD SPIROMETRY - PATTERN RECOGNITION
Normal
FEV1 / FVC > 70%
FEV1 > 80%
pred
FVC
> 80%
pred

COPD SPIROMETRY - PATTERN RECOGNITION
Normal Airflow
Limitation
FEV1 / FVC > 70% < 70%
FEV1 > 80%
pred
< 80%
pred
FVC
> 80%
pred
usually
> 80%
pred
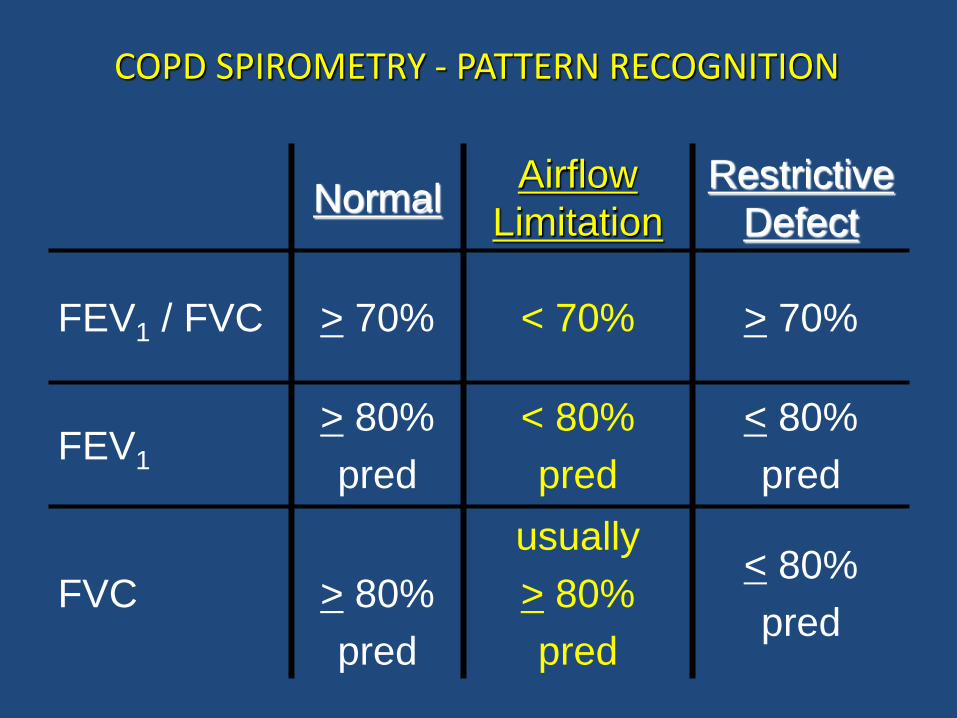
COPD SPIROMETRY - PATTERN RECOGNITION
Normal Airflow
Limitation
Restrictive
Defect
FEV1 / FVC > 70% < 70% > 70%
FEV1 > 80%
pred
< 80%
pred
< 80%
pred
FVC
> 80%
pred
usually
> 80%
pred
< 80%
pred

Importance of FEV1
• Single best predictor of survival
• Used in composite indices predicting survival
• Generally correlates with symptoms (dyspnea,
health-related quality of life and exercise)
• Marker for exacerbations (FEV1 < 50%
predicted)
• Marker for hypoxia (FEV1 < 30% predicted)
• Guide to therapy (GOLD and ATS/ERS
guidelines)

Stratification of Severity in COPD by FEV1%
Celli BR et al. Eur Respir J. 2004;23:932-946. Global Initiative for Chronic Obstructive Lung Disease. Executive Summary Updated 2004. Available at: http://www.goldcopd.com/workshop/ toc.html. Accessed February 21, 2005.
I* (Mild)
IV (Very Severe)
III (Severe)
II (Moderate)
100%
80%
30%
50%
0%
ATS/ERS and GOLD Guidelines FE
V1%
*COPD is defined as FEV1/FVC <70%.

COPD Diagnosis:
• Spirometry is necessary to diagnose COPD,
particularly early in the course of the disease
• Also useful to determine severity (stage) and assess
prognosis
• Barriers to increased spirometry use:
Cost - equipment
Complexity - personnel time required
Knowledge deficit - role, performance, importance
BARRIERS CAN BE OVERCOME!
Importance of Spirometry

How Can We Implement
COPD Diagnosis?
Goal: Make patients with COPD better Method: Integrate all office personnel in the management of patients with COPD

It Takes A Village . . .
• How can your office effectively and efficiently operate to:
– Determine which patients might have COPD (COPD screening questionnaire?)
– Perform spirometry

What Are the Roles of Your
Office Health Care Team?
It takes a village . . .
A. Greeter B. Medical Assistant C. Physician D. Nurse practitioner E. Physician assistant F. Nurse G. Patient health advocate
What Happens To A Patient
With COPD When They Are In Your Office?
1. Enter through the front door 2. 3. 4. 5. Go into room to be seen by prescribing
health-care provider 6. 7. 8.

Assessment of Dyspnea
MMRC Questionnaire Dyspnea Score
0. SOB with strenuous exercise
1. SOB hurrying on level or walking up slight hill
2. Stop when walking on level, or slower than people of the same age
3. Stop after walking ~100 m, or after a few minutes on level
4. Too short of breath to leave the house or while dressing / undressing
Global Initiative for Chronic Obstructive Lung Disease. Global strategy of the diagnosis, management, and prevention of
COPD. http://www.goldcopd.org/Guidelines/guidelines-global-strategy-for-diagnosis-management.html. Published
December 2011. Accessed September 19, 2012.

Assessment of Symptoms
COPD Assessment Test
(CAT)
– 8 item measure of
health status
– Score 0 - 5
– Impact
< 10 – low
11 - 20 – medium
21 - 30 – high
31 - 40 – very high
0 Cough 5
0 Phlegm 5
0 Chest tightness 5
0 Short of breath on hill
or flight of stairs
5
0 Limitation in
home activities
5
0 Confidence
leaving home
5
0 Sleep 5
0 Energy 5
None All the
time
Jones PW, et al. Eur Respir J. 2009;34(3):648-654.
COPD Assessment Test. (CAT). http://www.catestonline.org/. Accessed September 25, 2012.
• COPD exacerbation: acute increase in respiratory
symptoms beyond the usual day-to-day variation,
leading to a medication change
• Exacerbations increase decline in lung function,
health status, and the risk of death
• Greatest risk factor for future exacerbations is a
history of previous exacerbations
– ≥ 2 exacerbations per year is considered
high risk
Assessment of Exacerbation Risk
Global Initiative for Chronic Obstructive Lung Disease. Global strategy of the diagnosis, management, and prevention of
COPD. http://www.goldcopd.org/Guidelines/guidelines-global-strategy-for-diagnosis-management.html. Published
December 2011. Accessed September 19, 2012.

Combined COPD Assessment R
ISK
GO
LD
Sta
ge o
f A
irfl
ow
Lim
itati
on
RIS
K
Exa
ce
rbati
on
his
tory
≥ 2
0 - 1
C D
A B
MMRC 0 - 1
CAT < 10
4
3
2
1
MMRC ≥ 2
CAT ≥ 10
Risk
Symptoms
Global Initiative for Chronic Obstructive Lung Disease. Global strategy of the diagnosis, management, and prevention of
COPD. http://www.goldcopd.org Update 2011. Accessed September 19, 2012.

Additional Assessment of COPD
• Current smoking
• Oxygenation
– Pulse oximetry at rest
• Comorbidities
– Treat comorbidities as medically indicated
Global Initiative for Chronic Obstructive Lung Disease. Global strategy of the diagnosis, management, and prevention of
COPD. http://www.goldcopd.org/Guidelines/guidelines-global-strategy-for-diagnosis-management.html. Published
December 2011. Accessed September 19, 2012.

COPD: Personalize Goals of Management
• Relieve symptoms (SOB)
• Improve exercise tolerance
• Improve health status
• Prevent disease progression
• Prevent and treat exacerbations
• Reduce mortality
Reduce
symptoms
OR
Reduce
risk
Global Initiative for Chronic Obstructive Lung Disease. Global strategy of the diagnosis, management, and prevention of
COPD. http://www.goldcopd.org/Guidelines/guidelines-global-strategy-for-diagnosis-management.html. Published
December 2011. Accessed September 19, 2012.

COPD: Pharmacologic Therapy
FIRST CHOICE
Ex
ac
erb
ati
on
s p
er
ye
ar
≥ 2
1
0
MMRC 0-1
CAT < 10
GOLD 4
MMRC ≥ 2
CAT ≥ 10
GOLD 3
GOLD 2
GOLD 1
SAMA prn
or
SABA prn
LABA
or
LAMA
ICS + LABA
or
LAMA
A B
D C
ICS + LABA
or
LAMA
Global Initiative for Chronic Obstructive Lung Disease. Global strategy of the diagnosis, management, and prevention
of COPD. http://www.goldcopd.org/Guidelines/guidelines-global-strategy-for-diagnosis-management.html. Published
December 2011. Accessed September 19, 2012.
ICS= inhaled corticosteroid
LAMA=long-acting antimuscarinic antagonist
SAMA=short-acting antimuscarinic antagonist
SABA=short-acting beta2 agonist

MMRC 0-1
CAT < 10
GOLD 4
GOLD 3
GOLD 2
GOLD 1
LAMA or
LABA or
SABA and
SAMA
LAMA and
LABA
ICS and LAMA or ICS + LABA and
LAMA or ICS + LABA and
PDE4-inh or LAMA and LABA or LAMA and PDE4-inh
LAMA and LABA
COPD: Pharmacologic Therapy
SECOND CHOICE
A
D
C
B
Exacerb
ati
on
s p
er
year
≥ 2
1
0
MMRC ≥ 2
CAT ≥ 10
Global Initiative for Chronic Obstructive Lung Disease. Global strategy of the diagnosis, management, and prevention
of COPD. http://www.goldcopd.org/Guidelines/guidelines-global-strategy-for-diagnosis-management.html. Published
December 2011. Accessed September 19, 2012.
PDE4-inh=phosphodiesterase-4 inhibitor

≥ 2
1
0
MMRC 0-1
CAT < 10
GOLD 4
MMRC ≥ 2
CAT ≥ 10
GOLD 3
GOLD 2
GOLD 1
Theophylline
PDE4-inh.
SABA and/or SAMA
Theophylline
Carbocysteine SABA and/or
SAMA Theophylline
SABA and/or SAMA
Theophylline
COPD: Pharmacologic Therapy
ALTERNATIVE CHOICES
A
D C
B
Ex
ac
erb
ati
on
s p
er
ye
ar
Global Initiative for Chronic Obstructive Lung Disease. Global strategy of the diagnosis, management, and prevention
of COPD. http://www.goldcopd.org/Guidelines/guidelines-global-strategy-for-diagnosis-management.html. Published
December 2011. Accessed September 19, 2012.

Other Therapies for COPD
• Smoking cessation
• Oxygen
– Resting SpO2 ≤ 88%
• Pulmonary rehabilitation
– For all patients
• Lung volume reduction surgery
– FEV1 < 45% predicted and emphysema
Global Initiative for Chronic Obstructive Lung Disease. Global strategy of the diagnosis, management, and prevention
of COPD. http://www.goldcopd.org/Guidelines/guidelines-global-strategy-for-diagnosis-management.html. Published
December 2011. Accessed September 19, 2012.

Smoking Cessation Slows Lung Function Decline in Mild COPD
Adapted from: Anthonisen NR, et al. Am J Respir Crit Care Med. 2002;166(5):675-679.
Anthonisen NR, et al. Ann Intern Med. 2005;142(4):233-239.
Calverley P, et al. Lancet. 2003;361(9356):449-456.
Sustained
Quitters
Intermittent
Quitters
Continuous
Smokers
HR mortality in usual care vs special
Intervention: 1.18 (95% CI:1.02-1.37)
FE
V1 (
L)
Year

Smoking Cessation and Mortality
0
4
8
12
16
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14
Follow-up (years)
% P
ati
en
ts D
yin
g
Smoking Cessation
Usual Care
-15%
Anthonisen NR, et al. Ann Int Med. 2005:142(4):233-239.

Smoking Cessation Therapies
Varenicline 2 mg/day
Bupropion SR
NRT nasal spray
NRT patch
NRT gum
NRT patch + bupropion SR
NRT patch + spray
33.2%
24.2%
26.7%
23.4%
19.0%
28.9%
25.8%
Medication Cessation Rates
Fiore MC, Jaén CR, Baker TB, et al. Treating Tobacco Use and Dependence: 2008 Update. Clinical Practice
Guideline. Rockville, MD: US Department of Health and Human Services. Public Health Service; 2008.
NRT=nicotine replacement therapy

Ries AL, et al. Chest. 2007;131(5 Suppl):4S-42S.
Evidence-Based Pulmonary Rehabilitation Guidelines
• Pulmonary rehabilitation:
– Improves the symptom of dyspnea - 1A
– Improves health-related quality of life - 1A
– Lower extremity exercise training at high
intensity produces greater physiologic
benefits than lower intensity training - 1B

Pulmonary Rehab Improves Dyspnea
Adapted from Salman GF, et al. J Gen Intern Med. 2003;18(3):213-221.
Effect Size With 95% CI
-1 0 1 2
Guyatt et al, 19922
Simpson et al, 1992
Bauldoff et al, 1996
Bendstrup et al, 1997
Wijkatra et al, 1995
Goldstein et al, 1994
Overall-mild/moderate
Overall-severe
Cambach et al, 1997
Griffiths et al, 2000
Wedzicha et al, 1998
Troosters et al, 2000
Wedzicha et al, 1998
Guell et al, 2000

Pulmonary Rehabilitation Improves Exercise And Health Status At One Year
Griffiths TL, et al. Lancet. 2000;355(9201):362-368.
P = 0.002
Dis
tan
ce W
alk
ed
(m
ete
rs)
1 year
100
175
212
137
6 weeks Before
P = 0.000
Exercise
Rehab
Control
Quality of Life
Qu
ality
of
Lif
e (
SG
RQ
)
1 year 6 weeks Before
50
62
69
56 P <0.000
P = 0.010
Rehab
Control
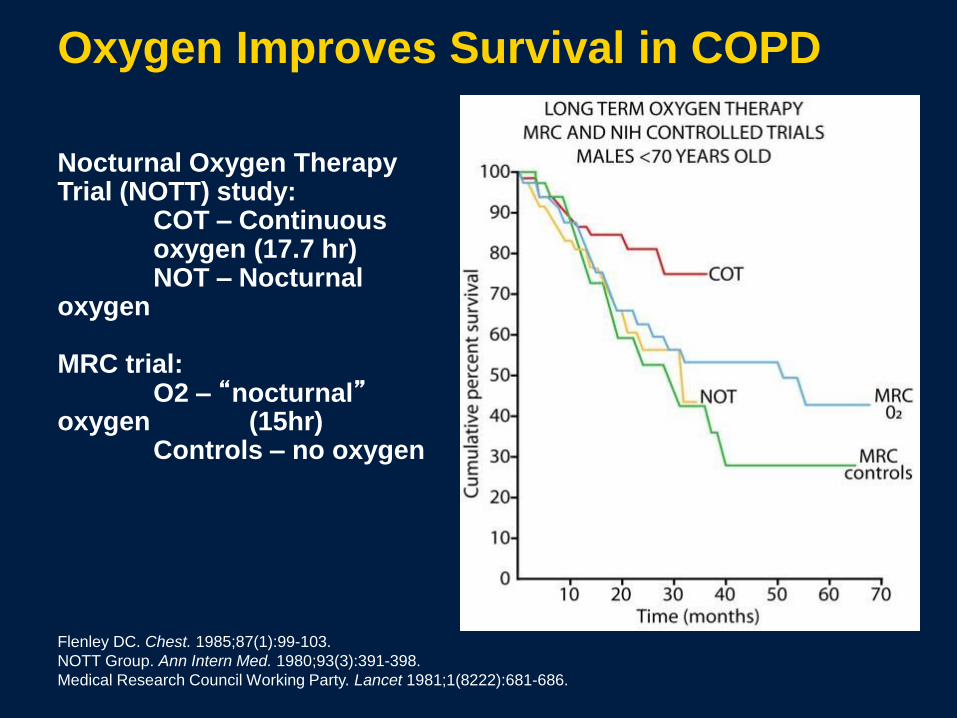
Oxygen Improves Survival in COPD
Flenley DC. Chest. 1985;87(1):99-103.
NOTT Group. Ann Intern Med. 1980;93(3):391-398.
Medical Research Council Working Party. Lancet 1981;1(8222):681-686.
Nocturnal Oxygen Therapy Trial (NOTT) study: COT – Continuous oxygen (17.7 hr) NOT – Nocturnal oxygen MRC trial: O2 – “nocturnal” oxygen (15hr) Controls – no oxygen

Let’s Discuss . . .
• Smoking cessation

Communication Strategies to Improve Adherence
1. Build a relationship
2. Focus on listening
3. Collaborate on the treatment plan
4. Manage time
5. Follow up
Bender BG. Pediatric Allergy: Principles and Practice. D. Leung, H. Sampson, R. Geha, and S. Szefler (eds.). New York: Elsevier; 455-462..

Tobacco Use: 2005 Prevalence
USA Colorado Rural Colorado
Current
Smokers 20.9% 17.3% 19.8%
http://www.cdphe.state.co.us/cohid/tabsdata.html
Deadly and linked with medical co-morbidities
Associated with lost work productivity and high costs
Associated with negative perceptions in social situations
Discouraged by many state governments and discouraged, limited, or barred in the workplace
And yet, about 20% of adults in Colorado
continue to smoke
Almost Everybody Seems to Know
That Smoking Is . . .

Jarvis MJ. BMJ. 2004;328(7434):277-279.
Dani JA, De Biasi M. Pharmacol Biochem Behav. 2001;70:439-446.
Addiction is Why People Continue
to Smoke
People smoke because they are addicted to nicotine
Smoking is a stronger addiction than heroin
addiction
There is a clear link between smoking, nicotine
receptors, and addiction

Challenges for Providers in the “Real World”
• Time (“I have too many other things to do”)
• Clinician Doubt (“Nothing helps people quit”)
• Provider “burn out” (“I’ve tried everything”)
• Remember: It’s a marathon, not a sprint

Physician Intervention
When physicians advise patients to quit
smoking, smoking cessation rates increase by
30%
Even very brief interventions by physicians can
be very effective
"Advising Smokers to Quit" is a measure of
physician performance in the US.

Physician Approach to Smoking
Cessation: 2 As and an R
1. ASK about tobacco use at each visit
2. ADVISE to quit at each visit
3. REFER for appropriate smoking cessation
help
Ask About Smoking
Ask all patients about smoking at each visit.
• The “fifth vital sign” or the “first vital sign”
Document smoking status routinely
Incorporate tobacco use as a vital sign assessed at
every visit to all health care providers
Increases smoking cessation interventions and may
increase quit rate

Advise
Strongly urge every patient to quit at every
visit.
• Use a clear, strong approach
• A < 3-minute message is sufficient
• Personalize the message for each
individual

Refer
• Refer to appropriate smoking cessation therapy
• Refer to support services
• QuitLine
• Other community services
• Provide pharmacotherapy options

QuitLine Fax Referral

Goals of Management in COPD
www.goldcopd.org
• Relieve symptoms
• Prevent disease progression
• Improve exercise tolerance
• Improve health status
• Prevent and treat complications
• Prevent and treat exacerbations
• Reduce mortality
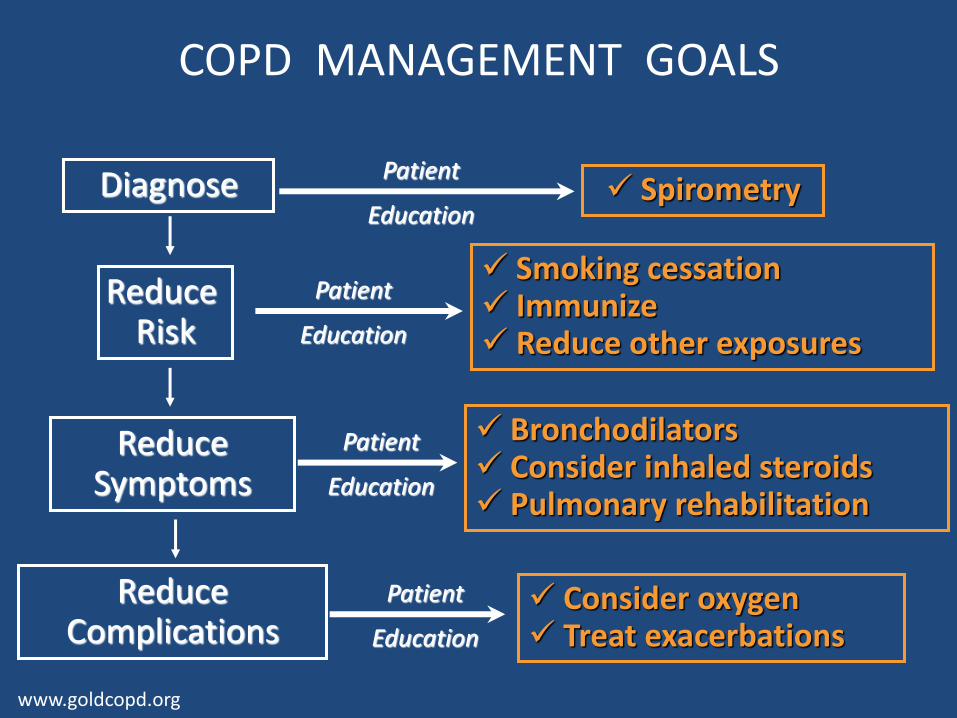
COPD MANAGEMENT GOALS
Diagnose
Reduce Risk
Smoking cessation Immunize Reduce other exposures
Reduce Symptoms
Reduce Complications
Bronchodilators Consider inhaled steroids Pulmonary rehabilitation
Consider oxygen Treat exacerbations
Spirometry
Patient
Education
Patient
Education
Patient
Education
Patient
Education
www.goldcopd.org
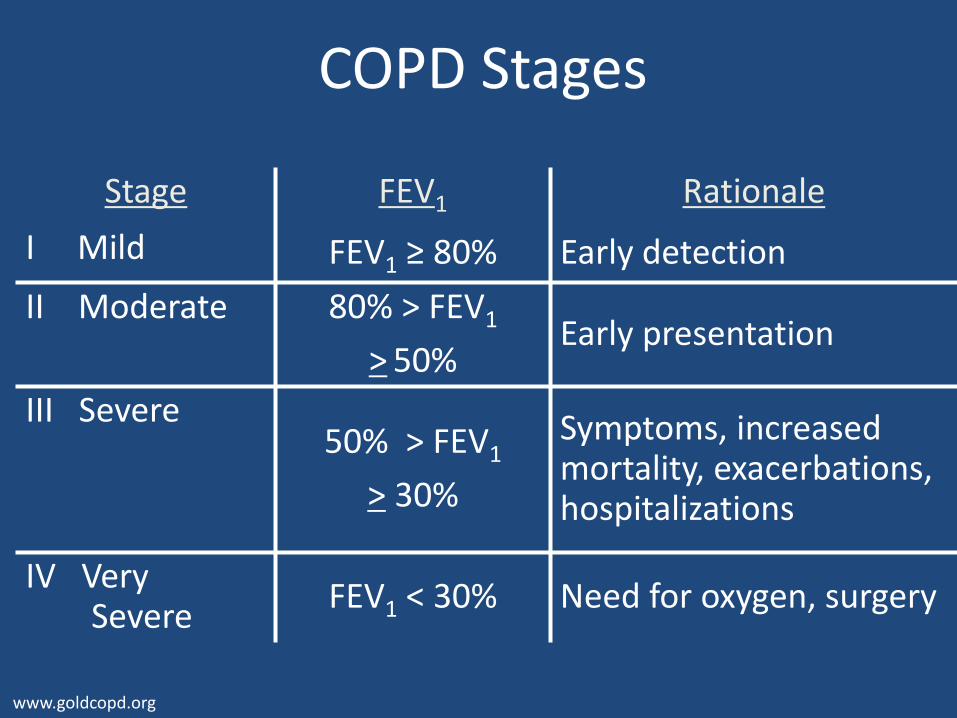
COPD Stages
www.goldcopd.org
Stage FEV1 Rationale
I Mild FEV1 ≥ 80% Early detection
II Moderate 80% > FEV1
> 50% Early presentation
III Severe
50% > FEV1
> 30%
Symptoms, increased mortality, exacerbations, hospitalizations
IV Very Severe
FEV1 < 30% Need for oxygen, surgery

National Jewish Health COPD Toolkit
• Tools for the Healthcare Provider and Patient
– COPD Toolkit Provider Training
– Provider Manual
– Spirometer
– Patient COPD Toolkit Workbook
– Follow-up office visits
NJH COPD
Tools for Managing COPD
Why COPD Toolkit?
To improve care of COPD patients through:
– Evidence based education on diagnosis and management
• Achieved through one-day workshop followed by two in-the-clinic review and practice
– Patient education to increase effective self-management and medication adherence
• Achieved by helping providers to educate and support patients through multidisciplinary trainings and patient materials