core topic lecture: anemia cases
TRANSCRIPT

Core Topic Lecture: Anemia Cases

Case #1
•James C. is a 69-yo male with PMHx of HTN, HLD, and spinal stenosis who c/o generalized fatigue
•Meds: simvastatin 40 mg/day, lisinopril 10 mg/day, meloxicam 7.5 mg/day, ASA 81 mg/day
•Smoker 1 ppd, no EtOH, retired mechanic
•Exam: BP 110/67, P 106, T 98.3F, RR 15,• NAD, diffuse pallor, pale conjunctiva
• Diffuse ABD tenderness
• Trace pedal edema

7.9 8.8 316
26.6
Case #1 – Data
Questions: ◦ What does the data show?
◦ What is the cause for this patient’s fatigue?
◦ What are the next diagnostic steps?
◦ How do we help the patient with his fatigue?
◦ Transfusion?
MCV = 79 fL L
MCH = 26.8 pg L
RDW = 16.6% H
Ferritin = 6 ng/mL L
TIBC = 886 mcg/dL H
Iron level = 22 mcg/dL L
B12 = 675 ng/mL normal
Folate = 24 ng/mL normal
Retic count = 1.9% H

Case #1 Microcytosis
lead poisoning
Elevated RDW thalassemia
Decreased Ferritin level
Iron Deficiency

Take Home Points – Case #1
•Microcytic anemia with elevated RDW is almost always iron deficiency anemia
•Serum ferritin best determines total body iron stores, but ferritin is also an acute phase reactant
•Older adults often suffer iron deficiency anemia as a result of gastrointestinal bleeding
•There is no number (Hgb) at which transfusion is indicated• Patient’s clinical situation dictates transfusion, not the labs

Case #2
•Joann is a 49-yo female with PMHx of obesity s/p Roux-en-Y gastric bypass and depression who presents c/o severe LE numbness and tingling
•Meds: famotidine 20 mg/day, citalopram 40 mg/day, OTC melatonin 5 mg/day
•Non-smoker, no EtOH, school teacher
•Exam: VVS, BMI = 37.7, normal cardiovascular exam, decreased DTRs, and decreased sensation over LEs, normal gait
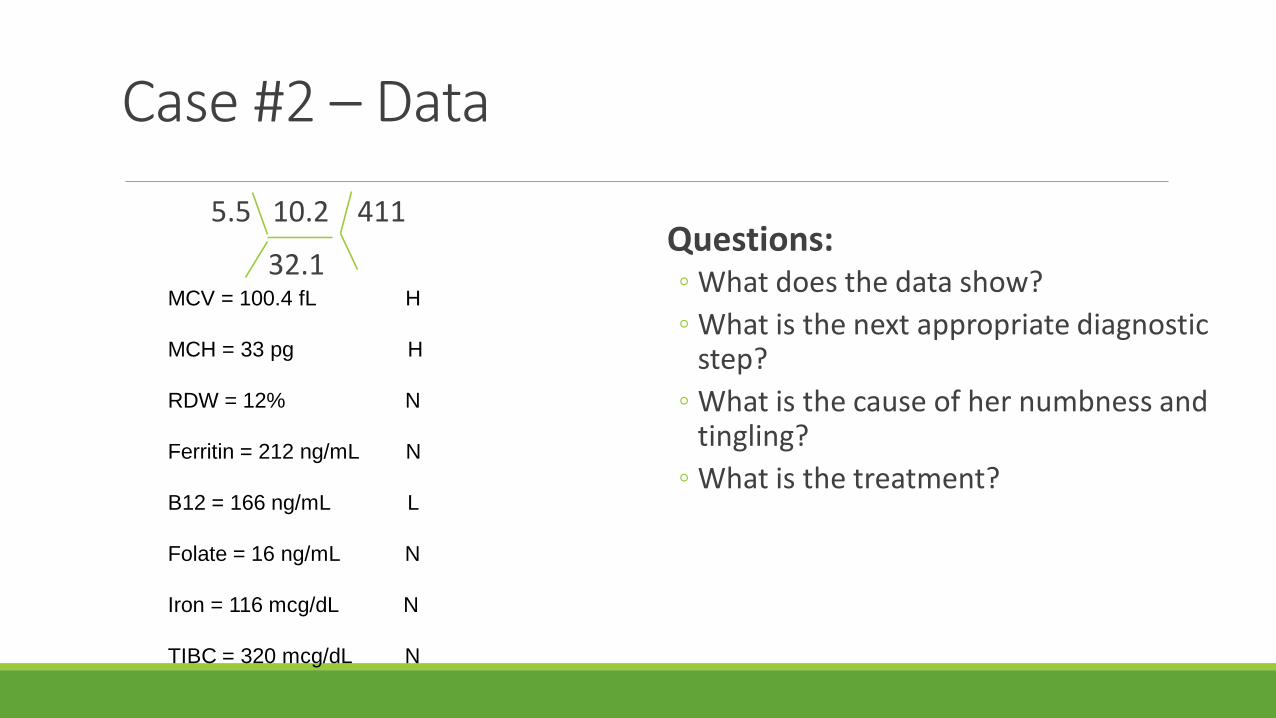
Case #2 – Data
Questions:◦ What does the data show?
◦ What is the next appropriate diagnostic step?
◦ What is the cause of her numbness and tingling?
◦ What is the treatment?
5.5 10.2 411
32.1MCV = 100.4 fL H
MCH = 33 pg H
RDW = 12% N
Ferritin = 212 ng/mL N
B12 = 166 ng/mL L
Folate = 16 ng/mL N
Iron = 116 mcg/dL N
TIBC = 320 mcg/dL N
Case #2
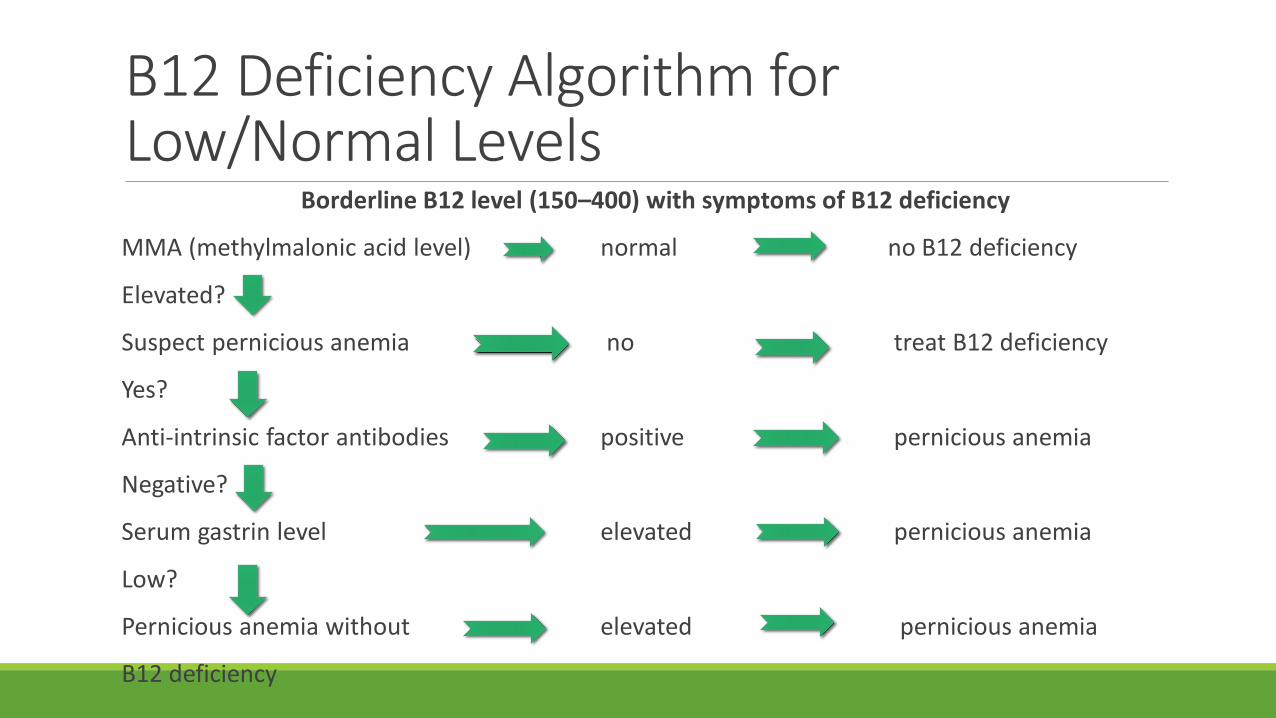
B12 Deficiency Algorithm for Low/Normal Levels
Borderline B12 level (150–400) with symptoms of B12 deficiency
MMA (methylmalonic acid level) normal no B12 deficiency
Elevated?
Suspect pernicious anemia no treat B12 deficiency
Yes?
Anti-intrinsic factor antibodies positive pernicious anemia
Negative?
Serum gastrin level elevated pernicious anemia
Low?
Pernicious anemia without elevated pernicious anemia
B12 deficiency

*Hypersegmented neutrophil, macroovalocytes
Take Home Points – Case #2
•Suspect B12 deficiency in patients with anemia after bariatric surgery
•B12 deficiency often causes neurologic or neuropsychiatric symptoms
•When B12 levels are low-normal, elevated MMA confirms deficiency (homocysteine also elevated)
•Positive anti-intrinsic factor antibodies or elevated gastrin levels confirm pernicious anemia

Case #3
•June is a 58-yo female with PMHx of COPD who presents to the ED 3 days after starting Bactrim (trimethoprim/sulfamethoxazole) for cystitis
• She complains of severe fatigue, skin discoloration, and dark urine
•Exam: BP 105/55, P=114, T99.2F, R=22 • Moderately-ill appearing, scleral icterus
• Tachycardia, clear lungs
•No CVAT, abdominal tenderness noted diffusely
• + mild jaundice
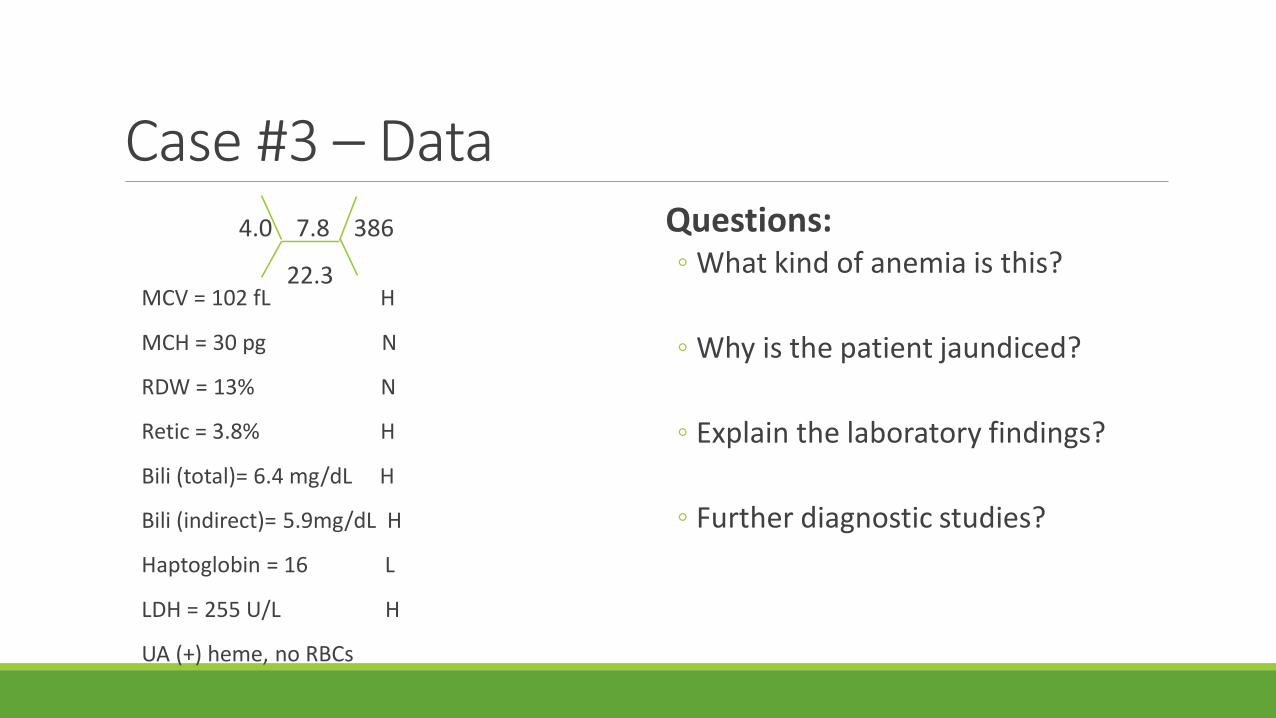
Case #3 – Data Questions:◦ What kind of anemia is this?
◦ Why is the patient jaundiced?
◦ Explain the laboratory findings?
◦ Further diagnostic studies?
4.0 7.8 386
22.3MCV = 102 fL H
MCH = 30 pg N
RDW = 13% N
Retic = 3.8% H
Bili (total)= 6.4 mg/dL H
Bili (indirect)= 5.9mg/dL H
Haptoglobin = 16 L
LDH = 255 U/L H
UA (+) heme, no RBCs



Case #3Direct Coombs test results are as follows:
DAT: Positive 3+◦ IgG: Positive 3+
◦ Complement: Negative
What type of immune-mediated anemia is this?
What conditions are typically associated with this type of antibody?
Case #3 - AIHA
•Categorized into two subgroups based on binding
temperatures
•Cold autoantibodies (IgM) bind to the RBCs and deposit
complement factor 3 on the cell surface
• A positive anti-C3 DAT occurs in cold AIHA
•Red blood cell agglutination with anti-IgG serum reflects warm AIHA
Case #3Management?
• Hematology consult
• Intravenous or oral corticosteroids
• Treatment of the underlying disorder
• Supportive care
• Refractory cases - splenectomy or plasmapheresis
• Transfusion therapy challenging because of the potential for cross-reacting antibodies
Take Home Points – Case #3
•Hemolytic anemia causes RBC destruction
•Lab findings: reticulocytosis, increased LDH, elevated unconjugated bilirubin, and decreased haptoglobin are classic
•A peripheral smear is essential – shows schistocytes, spherocytes, bite cells, and RBC fragments
•Direct antibody test (DAT) can distinguish immune from non-immune causes
•Treating the underlying cause

Case #4 •Betty is a 77-yo female with PMHx of CKD stage IV and rheumatoid arthritis
who complains of worsening arthralgias, and fatigue
•Meds: Lisinopril, Plaquenil, Crestor
•Non-smoker, no EtOH, retired cook
•PE: 126/80, P 70, T 99F, R=14
Frail elderly female NAD
MCPs are swollen and warm
Normal exam otherwise
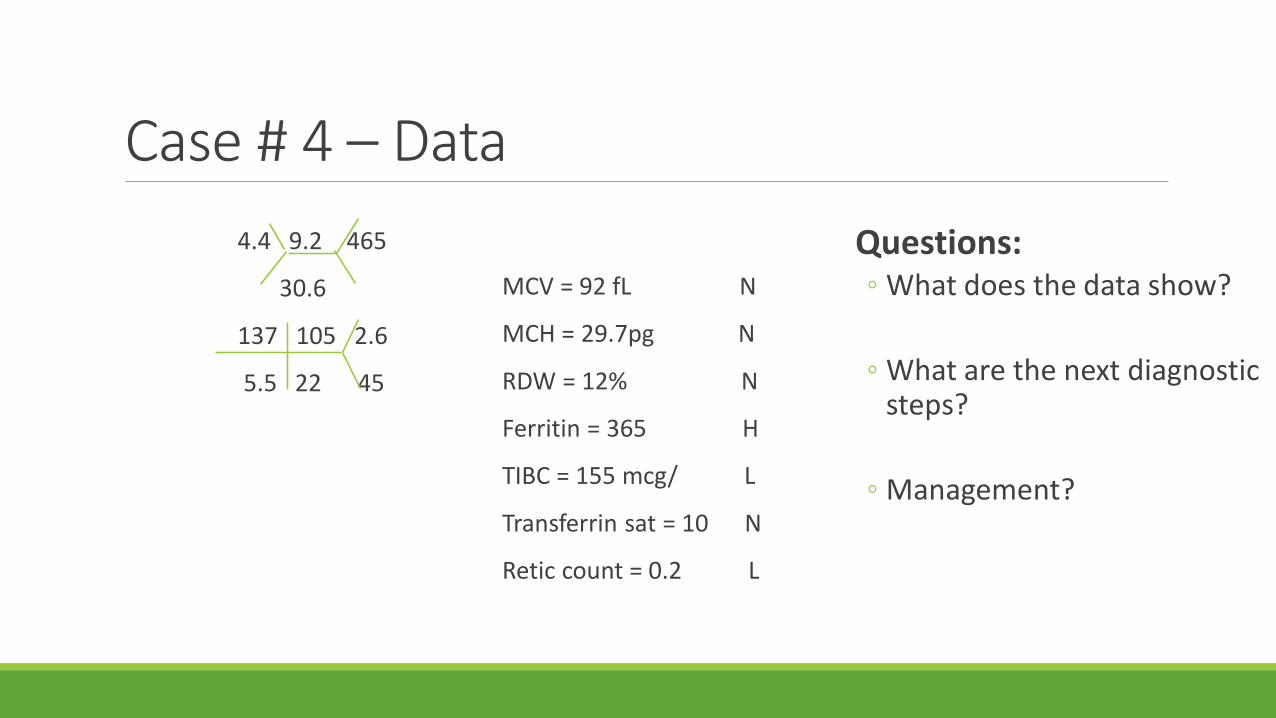
Case # 4 – Data
Questions:◦ What does the data show?
◦ What are the next diagnostic steps?
◦ Management?
4.4 9.2 465
30.6
137 105 2.6
5.5 22 45
MCV = 92 fL N
MCH = 29.7pg N
RDW = 12% N
Ferritin = 365 H
TIBC = 155 mcg/ L
Transferrin sat = 10 N
Retic count = 0.2 L
Take Home Points – Case #4
•Diagnosis of anemia of chronic disease reflects the presence of an underlying inflammatory condition (infection, autoimmune disease, renal disease, malignancy)
•Ferritin is an acute phase reactant and becomes less reliable as an indicator of iron stores
•Lab findings: Usually normocytic, sometimes microcytic, the TIBC is low, reticulocyte count is also low
•Correction of underlying disorder often leads to improvement in anemia
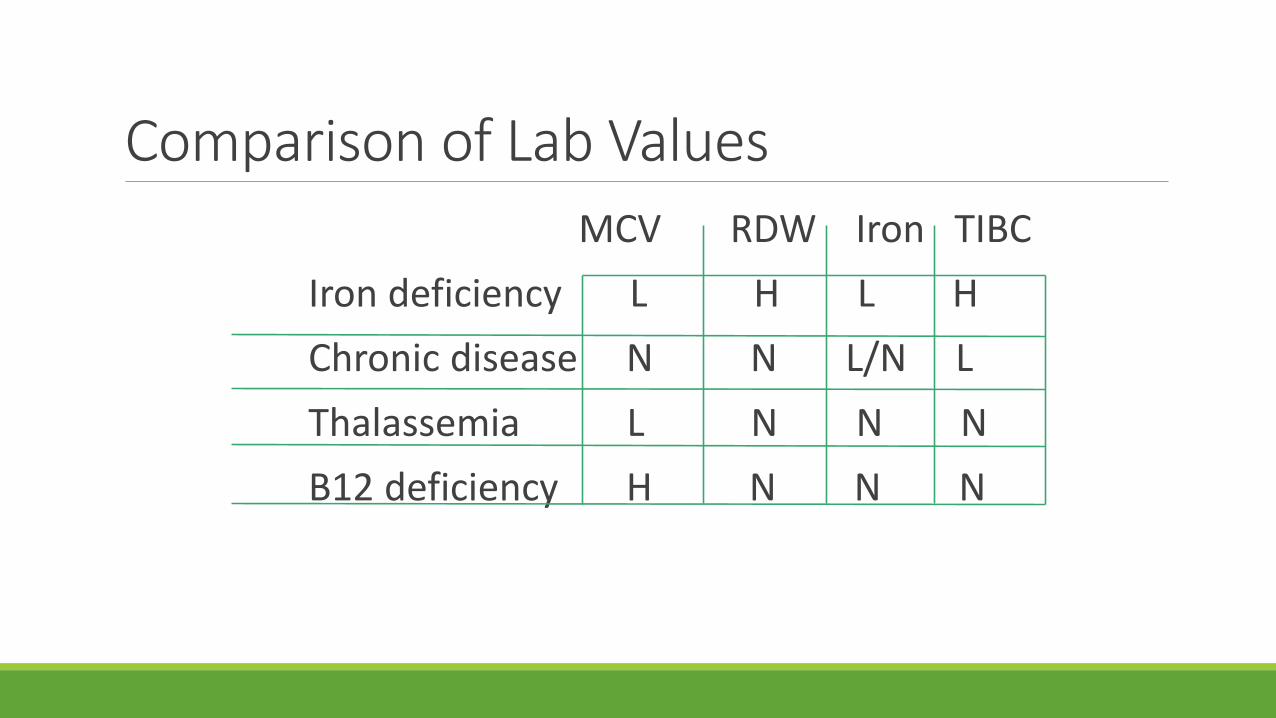
Comparison of Lab Values
MCV RDW Iron TIBC
Iron deficiency L H L H
Chronic disease N N L/N L
Thalassemia L N N N
B12 deficiency H N N N

Case #5
•Ryan is a 13-yo male of Mediterranean decent seen at urgent care last week for a sore throat and advised to follow-up due to an abnormal CBC
• He feels well and has no PMHx
• His sore throat is better, takes no medications
•PE: healthy male, VVS-afebrile, normal exam

Case #5 – Data
Questions:◦ What does the data show?
◦ How would you explain the laboratory findings?
◦ What other test (s) would you order?
6.0 9.9 277
31
MCV = 71 fL L
MCH = 26.2 L
RDW = 13% N
Ferritin level = 162 N
Iron = 88 mcg/dL N
TIBC = 255 mcg/dL N
B12 = 560 ng/mL N
Retic count = 0.3% N
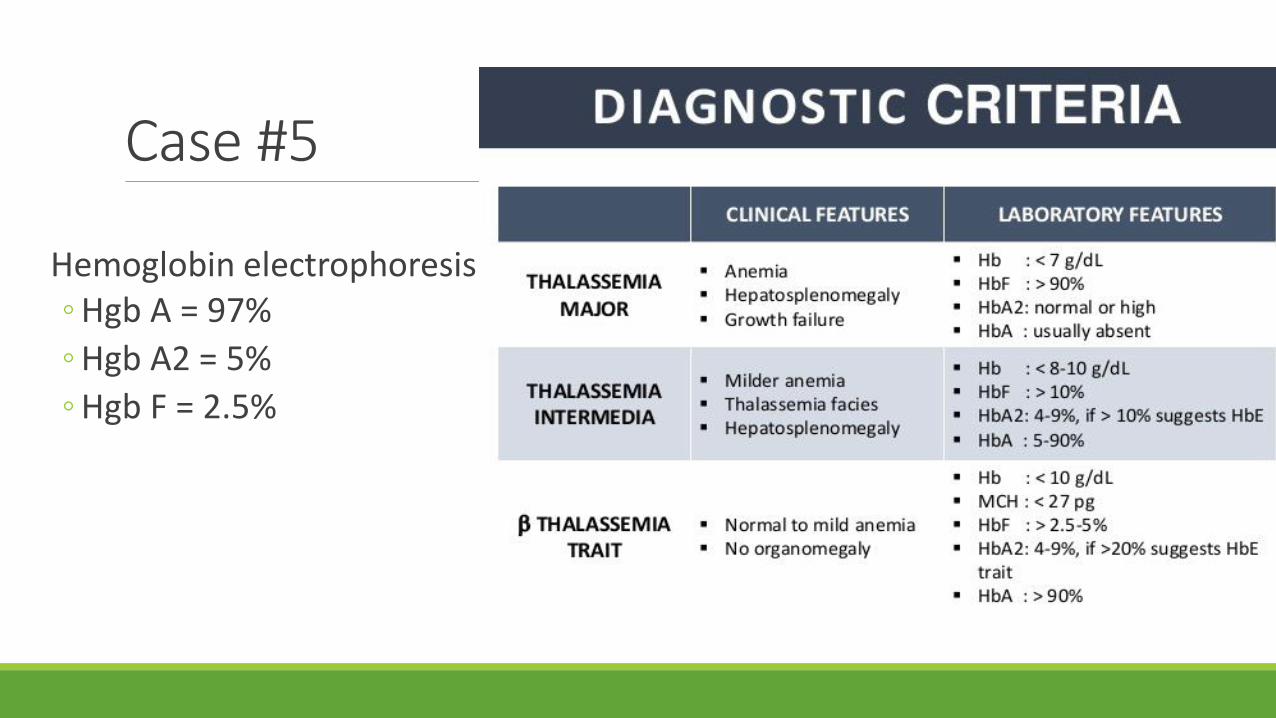
Case #5
Hemoglobin electrophoresis◦ Hgb A = 97%
◦ Hgb A2 = 5%
◦ Hgb F = 2.5%
Case #5
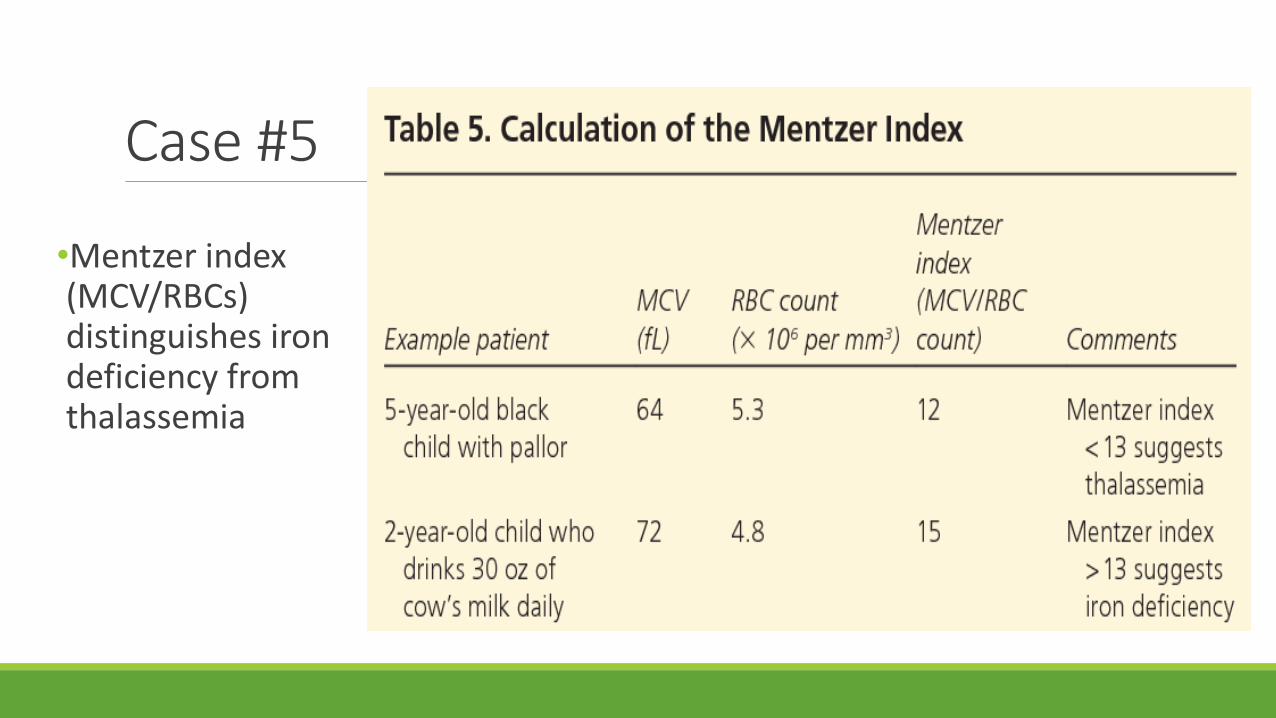
•Mentzer index (MCV/RBCs) distinguishes iron deficiency from thalassemia
Case #5 Take Home Points•Thalassemia trait is common and asymptomatic
•Causes very low MCV and mild anemia, normal serum ferritin
•A microcytic anemia with normal RDW usually indicates thalassemia
•Patients with thalassemia trait typically asymptomatic and require no treatment
• iron not needed unless co-existing iron def also present

Questions?