corneal infections from a-z...with exposure keratopathy and those on ventaltory assistance....
TRANSCRIPT

8/28/16
1
Corneal Infections from A-Z (Acanthamoeba to Zoster)
Joseph P. Shovlin, OD, FAAO Scranton, PA
I. Risk Factors In Ulcerative Keratitis
II. Differential Diagnosis of Infiltrative Keratitis
III. Treatment and Management of Ulcerative Keratitis
IV. Fungal and Protozoan Infection of the Cornea
V. The Herpes Family
DisclosuresAllergan Pharmaceutical Advisory Panel
AMO Global Medical Advisory Panel
-Acanthamoeba Outbreak Panel (ad hoc)
Bausch & Lomb Scientific Advisory Panel
-Global Steering Committee
-Panel On Fusarium Keratitis (ad hoc)
Ciba Vision Post-Market Surveillance Study Group
-Johns Hopkins Adjudication Committee (ad hoc)
Center for Disease Control & Prevention- Contact Lens Advisory Panel
Johnson & Johnson Global Professional Advisory Panel
Shire, Ophthalmic Advisory Panel
Speaker’s Bureau: Vistakon, Ciba Vision, CooperVision, Bausch & Lomb, AMO, Alcon, Genzyme, Shire

8/28/16
2
Infectious Keratitis
Herpes Keratitis Bacterial Keratitis
Fungal Keratitis
Amoebic Keratitis
“Swine Flu”: H1N1

8/28/16
3
Case 7 -- corneal haze
Stem Cell Deficiency Tear Film Defenses

8/28/16
4
Risk Factors for Ulcerative Keratitis
¤Exogenous¤Ocular Adnexal Dysfunction¤Corneal Abnormalities¤Systemic Disease¤Immunosuppressive Therapy
Epidemiology: Relative Risk
¤Population at risk: approximately 44 million in US and 120 million worldwide
¤Overnight wear the overwhelming risk factor¤Relative risk of extended wear v. daily wear: 10-15:1
¤Overnight wear of disposable lenses equal risk¤Additional risks: aphakia, smoking, lens case, minimal protective effect of hygiene
Incidence Rates for Microbial Keratitis
Any MK Severe MK
¤ Daily Wear GP 1.2 (1.1-1.5), 1.2
¤ Daily Wear DDCL 2.0 (1.7-2.4), .5
¤ Occasional CW 2.2 (2.0-2.5), 1.8¤ CW soft 19.5 (14.6-29.5), 13.3
¤ CW silicone 25.4 (21.2-31.5), 16.9From: Stapelton F. et al, The incidence of contact lens related microbial keratitis in Australia, Ophthalmol, 2008.
Microbial Keratitis Rates for Orthokeratology/Corneal Reshaping
¤ Incidence for microbial keratitis is estimated @ 7.7/10,000
¤ Children carry a higher rate @ 13.9/10,000
¤ Overall, the infection rate is similar to overnight soft lens use.
¤ CDC MMWR Report: 37 GP cases of AK (2005-2011); nearly 25% Ortho-K wearers and 50% used tap water to store lenses overnight
Bullimore M, Sinnott LT, and Jones-Jordan LA: The risk of microbial keratitis with overnight corneal reshaping lenses. Optom & Vis Sci. 2013; 90(9):937-944.
The Incidence of Microbial Keratitis amongWearers of a 30-Day Silicone HydrogelExtended-Wear Contact Lens
Oliver D. Schein, MD, MPH,1 John J. McNally, OD,2 Joanne Katz, ScD,3 Robin L. Chalmers, OD,4
James M. Tielsch, PhD,3 Eduardo Alfonso, MD,5 Mark Bullimore, MCOptom, PhD,6 Denis O’Day, MD,7
Joseph Shovlin, OD8
Purpose: To estimate the incidence of presumed microbial keratitis with and without loss of visual acuityamong wearers of a silicone hydrogel contact lens (Lotrafilcon A, Night & Day, CIBA Vision, Inc., Duluth, GA),recently approved for up to 30 days of continuous wear.
Design: Prospective cohort postmarket surveillance study.Participants: Contact lens wearers (recruited from 131 practices) who had been prescribed the lens for
intended continuous wear of as many as 30 nights.Methods: The occurrence of a corneal infiltrate was ascertained through a combination of center report and
direct contact with participants at 3 and 12 months. Whenever a corneal infiltrate was suspected, study andtreatment medical records were systematically reviewed by an Endpoints Committee using a predeterminedclassification scheme for corneal infiltration. Cases of presumed microbial keratitis were determined based onthe constellation of presenting signs and symptoms and clinical course.
Main Outcome Measures: The incidence of presumed microbial keratitis with and without loss of visualacuity.
Results: A total of 6245 participants were recruited between August 13, 2002 and July 2, 2003. Of these,4999 subjects (80%) completed 12 months of follow-up, and these participants contributed a total of 5561person years of lens wearing experience. Approximately 80% of participants routinely wore their lenses contin-uously for 3 or more weeks. The overall annual rate of presumed microbial keratitis was 18 per 10,000 (95%confidence interval (CI): 8.5–33.1). There were 2 cases of presumed microbial keratitis with loss of visual acuity,an annual rate of 3.6 per 10,000 (95% CI: 0.4–12.9), and an additional 8 cases without loss of visual acuity, anannual rate of 14.4 per 10 000 (95% CI: 6.1–28.4). The rate of presumed microbial keratitis was lower for usersreporting typical wear of 3 or more weeks than for those wearing the lens for less than a 3-week continuousperiod (P ! 0.02).
Conclusions: The incidence of loss of visual acuity due to microbial keratitis among users of the siliconehydrogel contact lens was low. The overall rate of presumed microbial keratitis with the wearing schedule of asmany as 30 nights was similar to that previously reported for conventional extended-wear soft lenses worn forfewer consecutive nights. Ophthalmology 2005;112:2172–2179 © 2005 by the American Academy of Ophthal-mology.
In 1981, the United States Food and Drug Administration(FDA) approved the first of a series of soft contact lenses forextended wear for as many as 30 days. The most serious
potential complication of contact lens extended wear isulcerative keratitis causing loss of vision. This condition ispresumed to be of microbial origin, although corneal cul-
Originally received: June 9, 2005.Accepted: September 8, 2005. Manuscript no. 2005-518.1 Department of Ophthalmology, Johns Hopkins University School ofMedicine, Baltimore, Maryland.2 CIBA Vision Corporation, Duluth, Georgia.3 Department of International Health, Johns Hopkins University BloombergSchool of Public Health, Baltimore, Maryland.4 Clinical Trials Consultant, Atlanta, Georgia.5 Bascom Palmer Eye Institute, University of Miami, Miami, Florida.6 Ohio State University College of Optometry, Columbus, Ohio.7 Department of Ophthalmology and Visual Sciences, Vanderbilt Univer-
sity School of Medicine, Nashville, Tennessee.8 Northeastern Eye Institute, Scranton, Pennsylvania.
This study was supported by a research grant from CIBA Vision Corpo-ration, Duluth, Georgia, to the Johns Hopkins University School of Med-icine. Dr Chalmers is a paid consultant to CIBA Vision, and Dr McNallyis a full-time employee of CIBA Vision. Dr O’Day was supported in partby a challenge grant from Research to Prevent Blindness, New York, NewYork. None of the other authors has a consultative or proprietary interestin the product or company.
Correspondence to Oliver D. Schein, MD, 116 Wilmer Building, JohnsHopkins Hospital, 600 N Wolfe Street, Baltimore, MD 21287-9019. E-mail:[email protected].
2172 © 2005 by the American Academy of Ophthalmology ISSN 0161-6420/05/$–see front matterPublished by Elsevier Inc. doi:10.1016/j.ophtha.2005.09.014
December 2005 PublicationOphthalmology
Journal of the American Academy of Ophthalmology
Associated Publication:

8/28/16
5
Modifiable Risk Factors for MK
¤Occasional CW Use: 1.87-3.96X
¤Regular CW Use: 5.28X¤Smoking: 2.96X
¤Poor Hygiene: 3.7X
¤Purchase Lens from Internet/Mail Order: 4.76X
¤Not Always Washing Hands: 1.49X
¤>2 Days Wear/Wk.: 3.46XFrom: Stapelton F. et al, The incidence of contact lens related microbial keratitis in Australia,
Ophthalmol, 2008.
Non-Modifiable Risk Factors
¤ < 6 Months CL Use: 4.42X
¤ High Socioeconomic Class: 2.66X
¤ Hyperopia 1.77X
¤ Age >50: .45X (protective)
¤ Male: 1.48X
From: Stapelton F. et al, The incidence of contact lens related microbial keratitis in Australia, Ophthalmol, 2008.
Can We Prevent MK?
¤ Lens wear: 80X relative risk
¤ Rate of infection has not changed over the past 20 years
¤ Longer wearing times, poor lens care hygiene are modifiable risks.
¤ Daily disposable lens wear is associated with a reduction in severity of infection and silicone hydrogel wear materials in disease duration.
¤ Severe cases of infection tend to be associated with environmental organisms, a delay in seeking treatment and travel overseas.
¤ Higher daytime temperatures carry a higher risk for severe infection.
From: Stapelton F-BCLA Medal Address, 2015.
Pathogenesis of Contact Lens Associated Microbial Keratitis
¤Lack of basic knowledge on how the ocular surface defends itself¤Would it help if patients were more compliant?¤Why is EW a risk factor?¤ Does fluorescein staining predict risk of infection?¤Why Pseudomonas aeruginosa?¤What is the relationship between infection and inflammation?
Fleiszig SM and Evans DJ. Pathogenesis of contact lens associated microbial keratitis. Optometry & Vision Science 2010;;87(4):1-7.
Measures for Preventing Microbial Keratitis
¤Minimize overnight wear ¤Monitor contact lens induced changes:
surface temperature, epithelial compromise, tear film stagnation, and reduced oxygen surface changes
¤Minimize lens care contamination: wash hands, remove lenses at pre-determined interval, small bottles of saline, lens case replacement, antibiotic prophylaxis usually not recommended
Lens Storage Cases and Risk for Infection
¤ Hall BJ and Jones L. Contact lens cases: The missing link in CL safety?. Eye & Contact Lens 2010;;36(2): 1-5.
¤ Wu Y, Carndt N, Wilcox M and Stapleton F. Contact lens and lens storage case cleaning instructions: Whose advice should we follow?. Eye & Contact Lens 2010;;36(2): 6-10.
¤ Wu Y, Zhu H, Harmis NY, et al. Profile and frequency of microbial contamination of contact lens cases. Optometry & Vision Science 2010;;87(3):152-158.
8/28/16
6
Bacterial Flora of the Normal Eye
Staphylococcus epidermidis 75-90%*
Diphteroids (C. xerosis) 20-33%
Staphylococcus Aureus 20-25%*
Streptococcus (S. viridan) 2-6%
Hemophilus influenza 3% or more
Streptococcus pneumoniae 1-3%*
Gram negative rods 1% or more*
Pseudomonas aeruginosa 0-5%*
* Dominant organisms in microbial keratitis
Common Organisms Encountered
¤Northeast: Staph. species, Moraxella, Pseudomonas aeruginosa, Streptococcus pneumonia
¤Southeast: Pseudomonas aeruginosa common¤Pseudomonas aeruginosa still a common
organism in contact lens wear. Also commonly found in burn patients, patients with exposure keratopathy and those on ventaltory assistance.
Common Organisms Encountered
¤Corneal injury including foreign body: Serratia, Proteus, Azotobacter, Neisseria, Bacillus species
¤Concern for organisms that can penetrate an intact epithelium: N. gonorrhoeae, Corynebacterium diphtheriae, Listeria,Hemophilus aegyptius
Classification of Infiltrates
Ambiguity in Diagnosis of CIEs
Venn diagram show how the 111 CIEs are classified based on the
categorization proposed by Sweeney 2003. Each dot represents a single CIE.
vAnalysis assuming 70% of clinical descriptors must be met for a given CIE subtype to be diagnosedo Only 20% could be
classified unambiguously as a single CIE subtype
o 69% could be classified as 2 or more CIE subtypes
o 11% could not be classified as any of the CIE subtypes
Efron N, Morgan PB. Cornea. 2006;;25(5):540-4.
8/28/16
7
Solution Related Keratopathy
Before insertion After 2 hours of lens wear
Solution Related Keratopathy
Before insertion After 2 hours of lens wear
8/28/16
8
CORNEAL INFILTRATE STUDIESFactor Associated Not Associated
Known Association with CIEsImproper lens care Bates 1989 ;; M ah-Sadorra 2005 ;; M a tthews 1992 ;; M cNa lly , Cha lm ers ARVO 2004 ;; M e ly 2001
Lens Bioburden Corrigan 2001 ;; Ho lden 1996 ;; Key 2000 ;; K ie rnan 2009 ;; O zkan 2010 ;; Sanka ridu rg 2000 ;; Sweeney ARVO 2003 ;; S zczo tka -F lynn IOVS 2010
Case contamination Bates 1989 ;; Ho lden 1996 ;; K ie rnan 2009
Overnight/EW Bates 1989 ;; Cha lm ers 2010 ;; Cu tte r 1996 ;; Donsh ik 1995 ;; E fron 2005 ;; G ran t 1998 ;; M ah-Sadorra 2005 ;; M organ BJO 2005 , IOVS 2005 ;; N ilsson 1994 ;; San todom ingo -Rub ido 2007 ;; S tap le ton 1992 ;; Sucheck i 1996 ;; V iko ren 1990
Smoking Cha lm ers 2007 (trend );; Cu tte r 1996 ;; M organ IOVS 2005 ;; M cNa lly 2003 ;; S zczo tka -F lynn 2010 Sucheck i 1996
Tight fit/reduced movement Carn t ARVO 2007 ;; G ordon 1985 ;; M ertz 1990 ;; O zkan 2010 ;; S te in 1988 ;; Sweeney ARVO 2003 M cNa lly 2003
No Association with CIEs
Asymptomatic corneal staining Szczo tka -F lynn A rch O ph tha lm o l 2007 Szczo tka -F lynn IOVS 2010 ;; Carn t IER M a trix 2007 ;; Cha lm ers 2010
PATH Carn t 2007 Carn t 2009 ;; W illcox FDA 2008
Gender Morgan IOVS 2005 Cha lm ers 2007 , OVS 2010 ;; Fo ris te r 2009 ;; M cNa lly 2003 ;; N ilsson 1994 ;; Sweeney ARVO 2003 ;; S zczo tka -F lynn IOVS 2010
Rx Cha lm ers 2007 M cNa lly 2003 ;; Cha lm ers OVS 2010 ;; Sanka ridu rg 1999
No Conclusive Consensus
Age Cha lm ers 2007 , ARVO 2010 ;; M cNa lly 2003 ;; M cNa lly , Cha lm ers ARVO 2004 Morgan IOVS 2005 ;; Sanka ridu rg 1999 ;; Sweeney 2003 ;; S zczo tka -F lynn IOVS 2010
Lens care solution Carn t ARVO 2007 , 2009 ;; Cha lm ers ARVO 2010 ;; D iec ARVO 2009 , ARVO 2010 ;; K ie rnan 2009 ;; K is lan ARVO 2010 , ARVO 2011 ;; M e ly CLAO 2001 ;; Reeder GSLS 2011 ;; Re inde l AOA 2009 ;; Sacco GSLS 2011 , CLS 2011 ;; W illcox FDA 2008
Donsh ik 1995 ;; M organ IOVS 2005 ;; Roseman1994 ;; Z ig le r 2007
Soft contact lens material B rennan 2002 ;; Carn t 2009 ;; Cha lm ers 2010 ;; Fonn 2002 ;; Fo ris te r 2009 (trend );; Ke ir 2010 ;; M organ BJO 2005 , IOVS 2005 ;; San todom ingo -Rub ido 2007 ;; Sweeney 2003 ;; S zczo tka -F lynn 2007 ;; US FDA , Bausch & Lomb 2001 (US );; US FDA , C IBA V is ion ,2001 ;; US FDA , V is takon 2005
D illehay 2007 ;; E fron 2005 ;; Fonn 2002 , US FDA , C IBA V is ion 2001 (US )
Solution/Lens combinations Carn t 2007 , 2009 ;; Ke ir 2010 ;; K is lan ARVO 2010 D iec ARVO 2009 ;; Z ig le r 2007
Mucin balls Carn t ARVO 2007 ;; Sweeney ARVO 2003 ;; S zczo tka -F lynn ARVO 2010 (p ro tective ) Dumb le ton AAO 1999 ;; Tan AAO 1999
Season Cha lm ers OVS 2010 ;; M organ IOVS 2005
Duration of lens wear Cha lm ers 2007 N ilsson 2001
Swimming Cha lm ers AAO 2004 ;; M cNa lly , Cha lm ers ARVO 2004 Morgan IOVS 2005
Prior inflammatory event, CL-related issues, or injury
Cha lm ers 2007 ;; Ion ides 1997 ;; M cNa lly 2003 Morgan IOVS 2005
Conjunctival or limbal redness Szczo tka -F lynn A rch O ph tha lm o l 2007 Carn t 2007 ;; Sweeney ARVO 2003
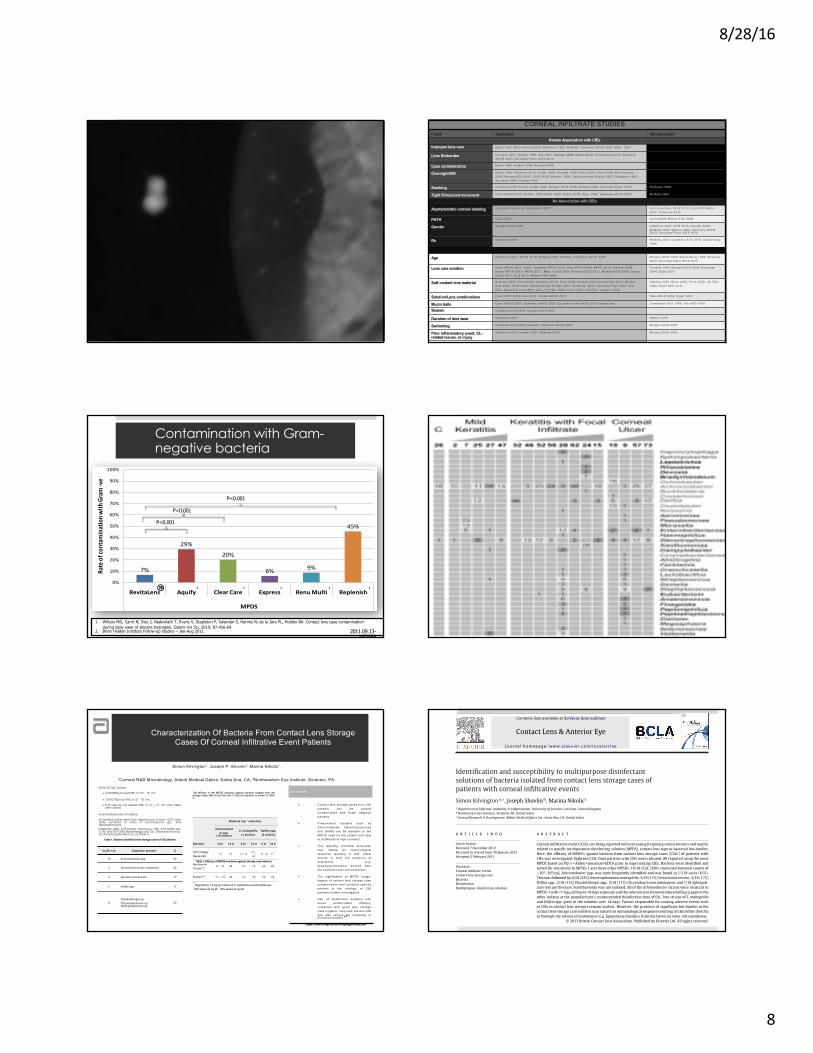
Contamination with Gram-negative bacteria
7%
29%
20%
6% 9%
45%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
RevitaLens Aquify Clear Care Express Renu Multi Replenish
MPDS
Rate of con
tamination with
Gram -‐ve
P<0.001
P<0.001
P<0.001
1. Willcox MD, Carnt N, Diec J, Naduvilath T, Evans V, Stapleton F, Iskandar S, Harmis N, de la Jara PL, Holden BA. Contact lens case contamination during daily wear of silicone hydrogels. Optom Vis Sci. 2010;; 87:456-64
2. Brien Holden Institute Follow-up studies – Jan-Aug 2011 2011.09.13-ME3999
® 1 1 1 12 1
Characterization Of Bacteria From Contact Lens Storage Cases Of Corneal Infiltrative Event Patients
Simon Kilvington1, Joseph P. Shovlin2, Marina Nikolic1.
1Corneal R&D Microbiology, Abbott Medical Optics, Santa Ana, CA;; 2Northeastern Eye Institute, Scranton, PA.
Conclusions
Table 3. Efficacy of MPDS solutions against storage case bacteria
Contact: Simon Kilvington ([email protected])
Bacteria log1 0 reduction
Achromobacter spp.
(10 strains)
S. maltophilia(4 strains)
Delftia spp.(2 strains)
Solution 6 hr 14 d 6 hr 14 d 6 hr 14 d
OPTI-FREE®
RepleniSH® <1 <1 <1 - 2 <1 -
>4a <1 - 2 <1
b
RevitaLens Ocutec™
2 – >4c
≥4 >4 >4 ≥4 ≥4
Biotrue™ <1 – >4d
≥4 >4 >4 ≥4 ≥4
a,b
Regrowth by 1-2 log for 2 strains of S. maltophilia and bothDelftia spp.C
90% strains ≥4 log kill.D
50% strains ≥4 log kill
Of the 18 CLSC studied:
Ø 16/18 (89%) showed TVBC of ≥104 – 108 /mL.
Ø 13/18 (72%) had TVBC of 106 – 108 /mL.
Ø 2/18 were dry but yielded TVBC of 104 – 105 /mL when sterilesaline added.
Acanthamoeba was not isolated.
All bacterial isolates were Gram negative rods of which 10/18 cases(56%) contained 13 strains of Achromobacter spp., 4/18Stenotrophomonasmaltophilia (22%), 3/18 Serratia marcescens (17%), 2/18 Delftia spp.(11%), and 6/18 (33%) Elizabethkingia spp. (3), Chryseobacterium sp.(2) and Sphingobacterium sp. (1) (Table 1).
CLSC +ve Organism present %
10 Achromobacter spp. 56
4 Stenotrophomonas maltophilia 22
3 Serratia marcescens 17
2 Delftia spp. 11
6Elizabethkingia sp. Chryseobacterium sp. Sphingobacterium sp.
33
Table 1. Bacteria identified from storage cases of CIE patients
The efficacy of the MPDS solutions against bacteria isolated from thestorage cases after 6 hour (hr) and 14 day (d) exposure is shown in Table3.
Ø Con tact lens sto rage cases from C IEpa tien ts can be gross lycon tam ina ted w ith G ram nega tivebacte ria .
Ø P redom inan t bacte ria such asAchromobacte r, S teno trophomonasand De lftia can be res is tan t to theMPDS used by the pa tien t and ab leto p ro life ra te to h igh numbers.
Ø The resu lting m icrob ia l b iobu rdenmay in itia te an immuno log ica lresponse resu lting in C IE , e ithe rd irectly o r from the presence o fendo tox ins (e .g .lipopo lysaccha rides) de rived fromthe bacte ria l ou te r ce ll m embrane .
Ø The sign ificance o f MPDS usage ,deg ree o f con tact lens sto rage casecon tam ina tion and bacte ria l spec iesp resen t in the e tio logy o f C IEwarran ts fu rthe r investiga tion .
Ø Use o f d is in fection system s w ithb road an tim icrob ia l e fficacy,comb ined w ith good lens sto ragecase hyg iene , m ay he lp p reven t C IEand a lso reduce the inc idence o fm icrob ia l ke ra titis .4-5
Please cite this article in press as: Kilvington S, et al. Identification and susceptibility to multipurpose disinfectant solutions ofbacteria isolated from contact lens storage cases of patients with corneal infiltrative events. Contact Lens Anterior Eye (2013),http://dx.doi.org/10.1016/j.clae.2013.02.001
ARTICLE IN PRESSG Model
CLAE-601; No. of Pages 5
Contact Lens & Anterior Eye xxx (2013) xxx– xxx
Contents lists available at SciVerse ScienceDirect
Contact Lens & Anterior Eye
jou rn al h om epa ge: www.elsev ier .com/ locate /c lae
Identification and susceptibility to multipurpose disinfectantsolutions of bacteria isolated from contact lens storage cases ofpatients with corneal infiltrative events
Simon Kilvingtona,∗, Joseph Shovlinb, Marina Nikolicc
a Department of Infection, Immunity & Inflammation, University of Leicester, Leicester, United Kingdomb Northeastern Eye Institute, Scranton, PA, United Statesc Corneal Research & Development, Abbott Medical Optics Inc., Santa Ana, CA, United States
a r t i c l e i n f o
Article history:Received 7 December 2012Received in revised form 30 January 2013Accepted 2 February 2013
Keywords:Corneal infiltrate eventsContact lens storage caseBacteriaDisinfectionMultipurpose disinfection solution
a b s t r a c t
Corneal infiltrative events (CIEs) are being reported with increasing frequency in lens wearers and may berelated to specific multipurpose disinfecting solution (MPDS), contact lens type or bacterial bio-burden.Here, the efficacy of MPDS’s against bacteria from contact lens storage cases (CLSC) of patients withCIEs was investigated. Eighteen CLSC from patients with CIEs were cultured. All reported using the sameMPDS based on PQ-1 + Aldox + nonanoyl-EDTA prior to experiencing CIEs. Bacteria were identified andtested for sensitivity to MPDS-1 and three other MPSDs. 16/18 CLSC (89%) contained bacterial counts of≥104–108/mL. Achromobacter spp. was most frequently identified and was found in 11/18 cases (61%).This was followed by 4/18 (22%) Stenotrophomonas maltophilia, 3/18 (17%) Serratia marcescens, 3/18 (17%)Delftia spp., 2/18 (11%) Elizabethkingia spp., 2/18 (11%) Chryseobacterium indologenes and 1/18 Sphingob-acterium spiritivorum. Acanthamoeba was not isolated. All of the Achromobacter strains were resistant toMPDS-1 with <1 log10 kill up to 14 days exposure and the solution also showed reduced efficacy against theother isolates at the manufacturer’s recommended disinfection time of 6 h. Two strains of S. maltophiliaand Delftia spp. grew in the solution over 14 days. Factors responsible for causing adverse events suchas CIEs in contact lens wearers remain unclear. However, the presence of significant bio-burden in thecontact lens storage case and lens may initiate an immunological response resulting in CIEs either directlyor through the release of endotoxins (e.g. lipopolysaccharides) from the bacterial outer cell membrane.
© 2013 British Contact Lens Association. Published by Elsevier Ltd. All rights reserved.
1. Introduction
Contact lens wear is a risk factor for microbial keratitis andoccurs at an incidence rate of approximately 40 cases per 100,000users [1–5]. Bacteria are the most common cause of infection, withStaphylococcus spp., Pseudomonas spp. and Serratia spp., notablyP. aeruginosa, and Serratia marcescens, commonly reported as theprimary causes of infection in this group [6,7]. Routine contactlens wear can result in colonisation of the contact lens storagecase by substantial numbers of bacteria and this may be encour-aged through poor lens care hygiene practices [8,9]. Such bacteria,although not directly pathogenic, can result in a substantial bio-burden (including biofilm production) inside the storage case and
∗ Corresponding author at: Department of Infection, Immunity & Inflammation,University of Leicester, Maurice Shock Building, University Road, Leicester LE1 9HN,United Kingdom. Tel.: +44 0116 252 2942; fax: +44 0116 252 5030.
E-mail address: [email protected] (S. Kilvington).
on the lenses which can afford protection from disinfectant activ-ity and provide a suitable environment for colonisation by primarypathogenic species [3,8–12]. Furthermore, the bacteria can serveas a food source for the free-living amoeba Acanthamoeba whichcan cause severe keratitis, with 90% of reported cases occurring incontact lens wearers [13,14].
Accordingly, good hygiene practices, including the correct useof disinfection systems, are fundamental to safe contact lens wear.Multi-purpose disinfecting solutions (MPDS) are most commonlyused for soft contact lens care and represent a single solution for therinsing, disinfection and storage of lenses [15,16]. Typically, theyare composed of biocidal preservatives, buffer system and otheragents to aid lens comfort and cleaning [15–17]. To qualify as aMPDS, such solutions must satisfy the requirements of ISO 14729and produce a 3 log10 reduction in reference strains of the bacte-ria P. aeruginosa, S. marcescens and S. aureus, and a 1 log10 for theyeast Candida albicans and the mould Fusarium solani within themanufacturer’s recommended contact lens disinfection time [18].However, there is no requirement to establish efficacy against other
1367-0484/$ – see front matter © 2013 British Contact Lens Association. Published by Elsevier Ltd. All rights reserved.http://dx.doi.org/10.1016/j.clae.2013.02.001

8/28/16
9
Risk Factors for Infiltrative Events and Contact Lenses¤ Bioburden on eyelid
¤ 5X higher
¤ Prior CIE’s¤ 7X higher
¤ Patient age¤ <25 or >50 3X higher
¤ Smoking ¤ 3X higher
¤ MPS vs H2O2¤ 2X higher with MPS
¤ DW DD lenses ¤ 12.5X lower risk
¤ Bioburden on CL or storage case¤ 6.4% higher
¤ Sihy vs hydrogel¤ Sihy 2X higher IOVS January 2015, vol 56, No1, pp 654- 663
Does Lens Material Affect Pathogenesis?¤ May be greater bacterial adhesion to silicone
hydrogel lenses¤ P aeruginosa and S Aureus
¤ Lens-attached bacteria form biofilms¤ Enhance resistance to anti-microbial agents¤ Adapt gene-expression¤ May be factor for increased infiltrative
events
¤ Lens material may: ¤ Suppress innate corneal epithelial defense
mechanisms¤ Decrease epi proliferation and renewal(>
for low Dk)
¤ Solution interactions
¤ Volume of postlens tear film/ composition¤ Absorption/ adsorption¤ Posterior tear fluid loses antimicrobial
activity during wear Optom Vis Sci. 2015 Jun;92(6):659-64
Eye Contact Lens. 2013 Jan; 39(1): 73–78.
Material properties that Influence Bacterial Adhesion
¤ Lens surface hydrophobicity influences bacterial adhesion
¤ Bacteria have higher affinity ¤ to low energy hydrophobic
surfaces than high energy hydrophilic surfaces.
¤ Rougher surfaces¤ Material dependent- some SiHy
rougher than others¤ Worn lenses are rougher surface
¤ Both SiHy and HEMA¤ Absorption/ Adsorption
¤ Tear film components (m uc in , Ig A , Lyso zym e , La cto fe rrin )
¤ Preferential binding to depositsIncreased inflammatory cells in cornea of asymptomatic DW sihy wearer
Prevalence of Risk BehaviorsTABLE 2. Prevalence of risk behaviors for eye infections* among contact lens wearers, stratified by type of contact lens — United States, 2014
Risk factor/Behavior % of wearers, by type of contact lensDaily disposable (n = 154)
Planned replace, soft (n = 730)
Overnight, soft†
(n = 182)
Rigid(n = 85)
Overall(n = 1,141)
Sleeping overnight in contact lens (ever)§ (48.7) (45.1) (88.6) (17.3) (50.2)Napping in contact lens (ever) (85.1) (86.9) (96.4) (74.1) (87.1)
Topping off solution (ever) (72.0) (51.3) (59.3) (60.5) (55.1)
Replacing lenses at interval longer than recommendedor when problem
(39.0) (48.5) (47.4) NA¶ (49.9)
Not using contact lens case (39.6) (1.9) (13.4) (0.0) (8.9)
Replacing contact lens case at interval longerthan recommended
(83.9)** (81.1) (82.0) (91.4) (82.3)
Storing lenses in tap water (ever) (28.0)** (12.4) (20.9) (33.3) (16.8)
Rinsing lenses in tap water (ever) (40.3) (27.2) (38.3) (91.4) (35.5)
Showering in contact lens (ever) (85.1) (84.6) (94.6) (67.5) (84.9)
Swimming in contact lens (ever) (59.1) (61.7) (64.9) (50.6) (61.0)
Infrequently or never washing hands before inserting lenses
(1.3) (4.8) (2.4) (2.5) (3.7)
Infrequently or never washing hands beforeremoving lenses
(19.5) (12.5) (9.0) (17.3) (13.3)
Center for Disease Control: August 21, 2015 64(32); 865-870
Where lenses were purchased
Provider office (66.9) (64.7) (67.5) (84.0) (66.9)
Retail store without eye exam
(8.4) (11.8) (7.5) (8.6) (10.4)
Internet (23.4) (21.3) (24.4) (4.9) (20.8)
Had a red/painful eye while wearing contact lensthat required a doctor's visit (ever)
(29.2) (29.3) (35.3) (28.9) (30.2)
% of wearers, by type of contact lens
Daily disposable(n = 154)
Planned replace, soft (n = 730)
Overnight, soft†
(n = 182)Rigid(n = 85)
Overall(n = 1,141)
Center for Disease Control: August 21, 2015 64(32); 865-870
Lens-Solution Combinations¤ Solution Induced
Corneal Staining¤ Greater risk of low
grade inflammation¤ Increase tear cytokines
¤ Poor tear quality¤ Deposits
¤ MPS higher incidence of inflammatory events than H2O2¤ Incidence depends on
lens/ solution combination

8/28/16
10
Characterizing Corneal Infiltrates from a 2010 Case Control Study of SCL Wearers
1RL Chalmers, OD; 2L Keay, PhD; 3J Kern, PhD; 4M Jansen, OD, MS; 5D Lam, OD, MS; 6B Kinoshita, OD; 7H Wagner, OD, MPH; 8G Sorbara, OD, MS; 9Mark Bullimore, PhD; 10Joseph Shovlin, OD; and 11L Sczcotka-Flynn, OD, PhD
1Clinical Trial Consultants, Atlanta, GA, 2The George Institute for Global Health, Sydney, Australia, 3Alcon Research, Ltd, Ft. Worth, TX, 4Indiana University School of Optometry, 5Southern California College of Optometry, 6Pacific University College of Optometry, 7NOVA Southeastern University School of Optometry, 8University of Waterloo, 9Ohio State University, 10 Northeastern Eye Institute, Scranton, PA, 11Case Western Reserve
This study was designed by Robin L Chalmers and funded by Alcon Research, Ltd
Minor revision submitted to Optometry & Vision Science Sept 6, 2011
Eye & Contact Lens, April 2012. Published ahead of print.
¤Eye & Contact Lens, April 2012. Published ahead of print.
¤Study estimated the economic burden of illness imposed by contact lens associated corneal infiltrative events (CL-CIEs) on both the healthcare system and individual patients in the U.S.
¤The cost per non-severe and severe CL-CIEs was estimated to be $1,002.90 and $1,496.00, respectively. Overall, the total estimated direct and indirect cost of non-severe CL-CIEs and severe CL-CIEs in the U.S. in 2010 was estimated to be $58 million.
Potential Risks & Results of Patient Behavior
¤Patients are poorly compliant even though they often believe they are not.
¤Disposable lens replacement schedules (Dart, et al.-DDCL), Dumbleton, et al.
¤Benefits of rub & rinse
¤Case care and accoutrement issues

8/28/16
11
Tarantula Hairs
What’s Missing Here?

8/28/16
12
Clinical Features of Ulcerative Keratitis
Symptomotology: pain, photophobia, decreased acuity, foreign body sensation
Signs: significant lid edema and reactive ptosis, conjunctival and ciliary injection, discharge, papillary response, stromal infiltration, surrounding edema, epithelial defect, anterior chamber reaction, cellular debris of tear meniscus and hypopyon
Differential Diagnosis of Ulcerative Lesions
¤ Herpes simplex keratitis
¤ Neurotrophic keratitis
¤ Peripheral marginal infiltrates
¤ Chemical keratopathy
¤ Keratoconjunctivitis sicca
Culture Media
¤Blood: aerobic organisms, saprophytic fungi¤Chocolate: Neisseria, Moraxella,
Hemophilus¤Sabouraud’s: fungi¤Thioglycolate broth: aerobic and anaerobic bacteria
¤Lowenstein–Jensen or Middlebrook 7H-9: Nocardia, Mycobacteria species

8/28/16
13
When To Culture Corneal Ulcers
¤ History of organic trauma¤ Atypical ulcer or if a rare infection is suspected¤ Infiltrate/suppuration involves the visual axis, infiltrate at 25% depth, 50% corneal thinning or scleral extention
¤ Immunocompromised or hospitalized patient¤ Unresponsive to seemingly appropriate treatment
Post Lasik Infiltrate
8/28/16
14

8/28/16
15
Laboratory Work-up
Up to 50% of properly performed cultures will reveal no growth in the setting of an actual bacterial keratitis (false negative) Tissue biopsy after treatment may be necessary!
¤ Direct inoculation of solid and liquid media is best method to increase the culture yield.
¤ Kimura spatula: culture the edge and base of the ulcer, serves to debreed the lesion
¤ Gram stain: only 12-60% accurate at predicting organism
¤ Giemsa stain: provides better morphologic characteristics of organisms and helps to distinguish bacteria from fungi
Corneal Scrapings
¤ Useful to use two solid media (blood and chocolate). Helps to R/O contaminants and aids in ID if there’s sparse growth If only one is used chocolate is preferred.
¤ Add Lowenstein/Jensen, amoeba culture or HSV swab if necessary.
¤ Hold fungal cultures longer!
¤ If you use non-solid medias such as thioglycolate broth use a cotton-tip applicatot that’s plastic, not wood broken into the tube.
Additional Clinical Features of Bacterial Keratitis
Gram Positive Organisms¤ localized
¤ round or oval gray-white infiltrates
¤ distinct borders
¤ minimal surrounding edema
Gram Negative Organisms¤ increased suppuration
¤ adherent exudate to base
¤ larger, less defined infiltrate
¤ more rapid progression and stromal necrosis/excavation
Principles of Treatment
¤ Utilize broad spectrum of coverage: single agent v. multiple agents (with or without culture)
¤ Use rapid, intensive topical therapy. Best to avoid “heavy” pain medication.
¤ Daily evaluation until significant improvement is shown.
¤ Tailor antibiotic choice by culture results and clinical impression.

8/28/16
16
Treatment and Management
¤ In-patient v. out-patient therapy depends on patient profile
¤ Initial treatment should be broad spectrum despite gram stain results with severe infections
¤ Reasons for systemic medications: N. gonorrhoeae
¤ Fortified antibiotics v. fluoroquinolone use¤ Strep. is a deficiency, low toxicity, good corneal penetration, greater duration of use, off-the-shelf availability, cost, prolonged tear film concentration
Design for Drug Penetration
Topical: every 15 min.-1 hr. for initial 24-48 hrs. or an altered loading doseSubconjunctival injection: once or twice daily for 1-2 days
Intravenous/oral antibiotics: only for impending perforation or scleral suppuration
Modification Of Therapy
Objectives: eliminate replicating bacteria, avoid adverse reaction to the medication, control the destructive components of the inflammatory process
Guidelines: avoid abrupt changes in therapy until the response can adequately be assessed and until the sensitivity tests are completed at the lab
Termination of Therapy
¤Measures of improvement: blunting of the perimeter of stromal suppuration, reduction in density of suppuration, reduction in cellular infiltrate and surrounding edema, reduction in anterior chamber reaction, progressive re-epithelialization
¤Reducing anti-microbials and adjuvants: avoid abrupt cessation, prolonged therapy needed for Pseudomonas, Mycobacterium, Nocardia, anaerobes
Fourth Generation Fluoroquinolones
¤ Provide greater gram+ coverage and equivalent gram- coverage
¤ Alternatives: fortified tobramycin 14mg/ml or ceftazidime 50mg/ml with adequate gram+ coverage of vancomycin 30mg/ml or cefazolin.
¤ Decreased chance for resistance¤ “quorem sensing and auto-induction”¤ hydrophobic regions limit bacterial efflux¤ attacks and binds DNA gyrase (gram-) and
topoisomerase II/IV (gram+)

8/28/16
17
Resistant Bacteria
¤ Methicillin resistant Staphylococcus aureus¤ Enterococcus Fecalis (group D
Streptococcus)
¤ Aminoglycoside resistant Pseudomonas aeruginosa
¤ Beta lactamase producing Neisseria¤ Atypical Mycobacteria
Gram positive: Vancomycin 20-30 mg/ml,
.28% Lysostaphin, IV Linezolid (Zyvos)
Gram negative: Amikacin 20 mg/ml, .19% Colistin
Fluoroquinolone Resistance
¤ UCSF Study (1996) Hwuang et al.: topical ciprofloxacin qid. S. aureus resistance rose from 12%-50% with in-vitro testing
¤ Wills Eye Hospital Study (1996) Rodman:¤ S. aureus resistance - Strep. resistance1992-4% 1992-20%1996-13% 1996-26%
¤ LV Prasad Institute (1999) Kunimoto et al:¤ 30.7% corneal isolates not sensitive to ciprofloxacinBascom Palmer Eye Institute (1999) Chaudry et al: P. aeruginosa resistance rose from .44% (1991-1994) to 4.1% (1995-1998)
Newer Generation FluoroquinoloneResistance Trends
¤ Ocular Trust data found 3rd and 4th generation fluoroquinolone effective against 30% of MRSA isolates, while Polytrim effective against 95% of the same isolates
¤ McDonald & Blondeau Cat & Ref Surg 36(9): 2010¤ Up to 85% MRSA strains resistant to moxifloxacin &
gatifloxacin¤ Besifloxacin showed greater efficacy against multi-
drug resistant S. aureus
Causes of Antimicrobial Resistance
¤Inappropriate use of antibiotics
¤Tendency to use broader spectrum antibiotics
¤Use of antimicrobials in an agricultural setting
¤Spread of resistant organisms by increased international travel
Ocular TRUST 2: Overview
¤Methicillin resistance in staphylococci marker for multi-drug resistance
¤Fluoroquinolones most consistently active agents across ocular pathogens
¤Fluoroquinolone susceptibility profilel Gatifloxacin = Levofloxacin = Moxifloxacinl Modest diminution in S. pneumoniae
susceptibility to ciprofloxacin
¤Polymixin B and penicillin most limited activity
ARMOR Surveillance Data¤ Antibiotic Resistance Monitoring in Ocular Microorganisms
(ARMOR) initiated in 2009-2013
¤ S. aureus and CoNS were non-susceptible to oxacillin/methicillin (43-59%), ciprofloxacin (33-43%) and azithromycin (60-63%) >3 drug resistance increased (38-39%).
¤ Besivance was one-fold less effective than vancomycin for MRSA/MRSE. Ciprofloxacin was 100 fold less effective than vancomycin. Twenty-five-thirty-seven percent of S. aureus and 50% of CoNS is MR (ARVO 2105).
¤ 4th generation fluroquinoloes show “holes” in Pseudomonas coverage. Ciprofloxacin faired reasonably well.
¤ Overall, updated data (2014) showed multi-drug resistance among CoNS and MRSE increased, but slightly decreased among S. aureus and MRSA

8/28/16
18
MRSA ¤MRSA must be a consideration in any external
ocular infection unresponsive to standard antibiotic therapy over 2 weeks.
¤Suspicion for ocular MRSA must increase with:¤ Malignancy¤ Debilitating systemic disease¤ History of ocular surface disorder
¤Resistance to fluoroquinolones is increasing, even with 4th generation.
¤Vancomycin and gentamicin remain effective treatments.
¤Community-associated MRSA is an evolving ocular pathogen most often found in “hospital-naive” patients.
After 3 days of Abx
CA-MRSA MRSE¤ S. epidermidis and MRSE are ubiquitous commensal
organisms in the human body. Most common cause of bacterial endophthalmitis.
¤ Among ophthalmic S. epidermidis isolates, MRSE rates may exceed 50%.
¤ Resistance to fluoroquinolones is common among MRSE isolates.
¤ Biofilm formation fortifies S. epidemidis against antimicrobial therapies and immune defenses.
¤ Biofilms enable adhesion of bacteria to artificial surfaces such as IOLs and contact lenses.
¤ Additional therapies include quorem sensing and immunotherapy against biofilm antigens and anti-biofilm activity.
New Antimicrobials
¤ 4th and 5th Generation Fluoroquinolones and Isothiozoquinolones(ITQs):
Trovofloxacin (Pfizer), Moxifloxacin (Bayer, Alcon), Gatifloxacin (Bristol-Myers/Squibb, Allergan), Temafloxacin (Allergan), Gemifloxacin (Pharmacia)
¤ Peptide Antimicrobials and Inhibitors:¤ deformylase, quorum sensing and efflux pump inhibitors
¤ Exazolidinones
¤ Pleuromutulins
¤ Oxazalidone linezolid
¤ Bacteriophages- new classes of viruses
¤ Aganocides
Adjuvant Therapy
¤ Cycloplegia
¤ Collagenase inhibitors¤ Steroids
¤ NSAIDs/Analgesics¤ Tissue adhesives
¤ Glaucoma medications¤ Recombinant bacterial/permeability increasing protein

8/28/16
19
Adjuvant Therapy (cont.)
¤ Debridement/biopsy
¤ Cryotherapy
¤ Bandage lens therapy/Pro-Kera/Bio-Tissue
¤ Continuous antibiotic infusion devices
¤ Therapeutic keratoplasty
¤ Bio-erodible mini tablets (fluoroquinolone)
¤ Hyperbaric oxygen
¤ Collagen cross linkage (Riboflavin/UV)
Collagen Cross-linking
Guidelines: The Use of Topical Steroids in Bacterial Keratitis
¤ Risks vs. Benefit: - the rationale for and the case against using topical steroids
¤ For: Steroids do not interfere with the ability of a bactericidal antibiotic (in sufficient concentration) to kill susceptible organisms.
¤ Against: Difficult to quantify scarring, therefore it’s never been proven that steroids minimize scarring. If you kill the organisms, patients are “cured”. “The anti-inflammatory effects of an effective antibiotic are frequently sufficient in treating bacterial ulcers.”(Baum)
Guidelines: The Use of Topical Steroids in Bacterial Keratitis
¤Meta-analysis of past studies:¤ Steuhl et al. underscores the potential benefit and justification for anti-inflammatory therapy.
¤ Leibowitz and Kupferman: cytokine induced expressions significantly down-regulated by corticosteroids.
¤ Vemuganti et al.: HLA-DR down-regulated and may inhibit keratocyte apoptosis induced by bacterial infection.
¤ Flesizig et al.: Pseudomonas shows an invasive v. cytotoxic genotype and respond diffferently to steroids (invasive best response).
Wilhelmus (50 year review): Indecision about corticsteroids for bacterial keratitis: An evidence based update
¤ (2002) This study did not demonstrate a clear cut beneficial effect of topical steroids on course of bacterial keratitis.
¤ Results: (1) steroid use before the diagnosis of bacterial keratitis significantly predisposes eyes with pre-exiting disease to severe ulcerative keratitis [odds ratio: 2.63], (2) once microbial keratitis occurred, prior steroid use significantly increased the odds of antibiotic treatment failure or other infectious complications [odds ratio: 3.75], (3) the effect of topical steroid use with antibiotics after the onset of bacterial keratitis was unclear.
** 24 studies summarized- 37.5% beneficial;; 50% neutral and 12.5% adverse

8/28/16
20
Guidelines: The Use of Topical Steroids in Bacterial Keratitis
Randomized Clinical Trial is sorely needed (NEI/NIH funded RO1): similar to the herpetic eye disease study
Pilot study: Srinivasan M, Lalitha P, Mahalakshmi R, et al: Corticosteroids for bacterial corneal ulcers. BJO: Oct, 2008.
¤Cochrane Systematic Review: only 1 randomized clinical trial to date with “ major methodological inadequacies”. Challenges include: type of organism, severity of infection, antibiotic and steroid selection, length of time before treatment, location of ulcer and additional patient factors.
Steroids for Corneal Ulcers Trial (SCUT)
¤ Topical steroids offer no significant benefit (or risk) in treating bacterial keratitis.*
¤ Adjunctive steroid therapy may improve visual outcome in severe bacterial ulcers (and may be most beneficial when used early).**
¤ Steroids should not be used in Nocardia infections.
¤ MIC correlates with clinical results; antibiotics with lower MIC are associated with better outcomes.
*Srinivarsan M, Mascarenhas J, Rajaraman R et al: Corticosteroids for bacterial keratitis: The Steroids for Corneal Ulcers Trial (SCUT). Arch Ophthalmol (2012); 130(2):143-150.
**Ray KJ, Srinivasan M, Mascarenhas J et al: Early addition of topical corticosteroids in the treatment of bacterial keratitis. JAMA Ophthalmology (2014); 132(6):737-41.
Steroids for Corneal Ulcers Trial (SCUT) Update¤ 12 month SCUT data published on BSCVA and corneal scar size in
399 cases from the original sample.¤ Myofibroblasts and fibroblasts, which are active during wound healing,
may help restore corneal transparency.¤ Topical corticosteroid benefit may be delayed but little benefit shown
after 12 mos..
¤ Immune-mediated tissue damage may be reduced, corneal remodeling may occur and scar density may be reduced long after steroid use has been discontinued.
¤ There may be a benefit with adjunctive topical corticosteroids if application occurs earlier in the course of bacterial corneal ulcers.
Srinivasan M, Mascarenhas J, Rajaaraman R, et al. The steroids for corneal ulcers trial: secondary 12-month clinical outcomes of a randomized controlled trial. Am J Ophthalmol. 2014;157(2):327-33.
Ray K, Srinivasan M, Mascarenhas J et al. Early addition of topical corticosteroids in the treatment of bacterial keratitis. JAMA Ophthalmol. 2014; 132(6):737-41.
Guidelines: The Use of Topical Steroids in Ulcerative Keratitis
¤ Principles for successful use of corticosteroids: (1) scrapings for stain and culture, (2) use of adequately dosed bactericidal antibiotics, (3) delay initiation of steroids until a clearly beneficial effect to antibiotic has been determined, (4) continue concurrent use of antibiotic with steroids, and (5) delay use of steroids if causative organism is not identified. USE 2-5 days after appropriate antibiotic therapy.
¤ Avoid if fungal infection or atypical mycobacterium is suspected, if there is severe thinning, enlarging epithelial defect, poor wound healing (diabetes), or immuno-suppression.
¤ In Acanthamoeba keratitis, steroids may increase potential for pathogenicity and steroids likely cause an increase in the rate of excystment and suppress macrophages.
Non-Bacterial Corneal Ulcers
¤Bascom Palmer Series (Alphonso et al.):¤ 1986: 3.1% of corneal ulcers treated were not
bacterial¤ 2004-05: 64.7% of corneal ulcers treated were
not bacterial
** some of the increase shift is due to 4th
generation fluoroquinolone usage
Fungal Infections
CLASSIFICATION/MOST COMMON ORGANISMS
¤ Filamentous Fungi; Molds¤ Septated: pigmented, non-pigmented¤ Non -Septated
¤ Yeasts

8/28/16
21
Risk Factors for Fungal Keratitis
¤ MOLDS: corneal injury, soft contact lens wear, chronic topical medications, systemic steroid usage, diabetes, radial keratotomy
¤ YEASTS: protracted healing, topical steroids, penetrating keratoplasty, bandage contact lenses
Clinical Features of Fungal Infections
¤ MOLDS - epithelium can be intact or ulcerated, usually non-suppurative with feathery infiltrates (focal or multi-focal / satellite)
¤ YEASTS - epithelium is usually ulcerated, generally suppurative (focal or diffuse)
Specific: infiltrates with gray/brown pigmentation, elevated edges with rough texture

8/28/16
22

8/28/16
23
Diagnosis of Keratomycoses
¤ Clinical Suspicion
¤ Corneal Scrapings and Suture Passes¤ Smears: gram, giemsa, acridine orange, calcofluor white¤ Cultures: blood agar, Sabouraud’s media¤ Polymerase chain reaction
¤ Superficial Keratectomy/Biopsy
¤ Paracentesis
¤ Confocal Microscopy

8/28/16
24
Antifungal Drugs
¤Sterol Binding
¤Inhibition of Sterol Synthesis
¤Interference of RNA Synthesis
¤Inhibition of Mitosis
¤Cationic Antiseptic
Initial Anti-fungal Treatment
¤ Hyphae: Natamycin 5% suspension*, topical and oral Voriconazole, oral Ketoconazole, Fluconazole or Itraconazole
¤ Yeast or Pseudo-hyphae: Amphotericin B, Natamycin, Miconazole, Clotrimazole, Posaconazole or Flucytosine
Subconjunctival injections of Fluconazole or intrastromalinjection of Amphotericin B are helpful in recalcitrants.
*generally most effective especially in Fusarium treatment
MIC values (sensitivity) may be predictive of outcome for Natamycin.
Treatment and Management of Fungal Keratitis
¤SUPPORTIVE AND ADJUNCT THERAPY¤ Debridement¤ Heat (40 degrees C)¤ Conjunctival Flaps¤ Debulking Procedures / Excimer ablation¤ Drug Delivery Devices¤ Cycloplegics¤ Glaucoma Medications¤ Tissue Glue
Surgical Therapy
¤Biopsy ¤Keratectomy ¤Penetrating keratoplasty¤Conjunctival flaps¤Cryotherapy¤Excimer ablation

8/28/16
25
Prevention of Fungal Infections in CL Wear
¤Minimize use of overnight wear including bandage lenses
¤Avoid indiscriminate use of topical medications
¤Stress proper maintenance and care of lenses and case
Unusual Outbreaks of Fusarium Keratitis
¤ Background: Fusarium keratitis is a relatively rare infection around the world, except in humid climates and especially in contact lens wearers (about 5%-Bascom Plamer)
¤ Disproportionate number of ReNu with Moisture Loc users (Singapore, Hong Kong)
¤ Alphonso series: 2005-about 50% CL wear and 2006-over 70% CL wear
¤ Script trac experienced a 150% increase in Natamycin prescriptions written in 2005.
CDC Fusarium Keratitis Update
¤86 cases are confirmed, 9 listed a ”possible”and 96 are under investigation
¤Complete data are available in 58 cases (56 are contact lens wearers)
¤Products used were:¤ 32 B&L ReNu with MoistureLoc™¤ 15 B&L ReNu® MultiPlus™¤ 7 B&L ReNu (unspecified)¤ 3 Advanced Medical Optics (AMO)¤ 3 Alcon product (unspecified)
* Total adds up to more than 56

8/28/16
26
Fusarium Keratitis:“The Perfect Storm”
¤Focus on: ReNu with MoistureLoc™ (disinfectant/surfactant), system failure unlikely, cross contamination likely
¤Pathogenesis: repeated inoculation not enough, epithelial micro-dehiscense is necessary
¤Multifactorial etiology: (lens type, lens case and bottle tips, biofilm/mycelium, “polymer film”/surfactant, environment/natural disasters)
¤Similarities to the protozoan mini-epidemic: (uptick, recognition, morbidity, inoculation, masking antigens, attack rate, host defenses)
CDC/MMWR Dispatch05-19-06
¤130 confirmed cases (onset after June, 2005, no history of trauma and positive culture)
¤Median age: 41 (12-83);; Sex: 67% female¤37/120 (31%) evaluated have been grafted¤125/130 were CL wearers¤118 identified their CL solution(s): 75 (64%) ReNu with MoistureLoc™, 14 (12%) MoistureLoc™ with another solution, 8 (7%) unspecified B&L product, 21(18%) using another product
CDC Case Control Study
¤CDC enrolled a sub-set of patients (50 cases and 79 controls) to evaluate relative risk [April, 2006]
¤“For the most stringent test for product association analysis was limited to 25 cases and 37 controls.”
¤Multivariable analysis: after controlling for poor compliance and reported exposure within 1 month prior to symptoms
CDC Case Control Study Results
¤ Adjusted odds ratio: ¤ ReNu with MoistureLoc™-19 (2.4-944.9) p<.001¤ ReNu®MultiPlus™-3.6 (0.3-189) p=0.5
Conclusion: “ReNu®MultiPlus™ was not significantly associated with the recent outbreak of Fusarium keratitis;; Cause of strong association with ReNu with MoistureLoc™ is unclear”.
On-going studies looking at environmental and formulation under stress risks are continuing.
Medical Management of Fusarium Keratitis
¤ Topical: Natamycin 5%, Voriconazole 10mg/ml, Chlorhexidine 0.2%
¤ Oral and IV: Voriconazole (Vfend/Pfizer) 200mg BID
¤ Surgical: debridement, full thickness grafting
*if unresponsive, systemic posaconazole or liposomal or lyophilized Amphotericin B
** Natamycin may respond better than Voriconazole in monotherapy especially in filamentous infections. (MycoticTreatment Trial, JAMA Ophthalmol. 131/4:422-29)
Fusarium Outbreak: Is It Over?
¤4 case reported since the ReNu®MoitureLoc recall
¤None of the patients reported using ReNu®MoistureLoc
¤Associated with other MPDS
BBJeng, G Hall, L Schoenfield, and D Meisler: Fusarium Outbreak: Not done Yet? Arch Ophthalmol, 2007, 125(7):981-982.

8/28/16
27
Paecilomyces lilacinus
Uptick in recently reported cases in Florida in contact lens wearers
¤Responds to Natamycin and Voriconazole
¤ Important to realize that unusual infections do occur in non-lens wearers.
Protozoan Infections in CL Wear
¤ ACANTHAMOEBA-at least 7 species show ocular parasitology, 23 species show systemic parasitology
[A.castellani, A.guina, A.culbertsoni, A.lugdunesis, A.polyphaga, A.hatchetti, A.rysades, A.griffini]
¤ Genotype (15)- 97% of isolates are of the T4 genotype
¤ Forms- 2 different life cycles
Acanthamoeba Morphology
† Tests follow FDA/ISO stand-alone criteria but are not FDA-required.
Acanthamoebatrophozoite
Acanthamoebacyst
Image from: Hughes R, Kilvington S: Comparison of Hydrogen Peroxide Contact Lens Disinfection Systems and Solutions against Acanthamoeba polyphaga. Antimicrobial Agents and Chemotherapy: 2038-2043, 2001.

8/28/16
28
Acanthamoeba Keratitis can be an Outbreak disease: History in the USA
Time period Totalcases
Cases averagePer year
Comments
1974-1983 31 3(new infection hard to diagnose)
50% wore contact lenses but no correlation made;; this is the beginning normal disease rate
1984-1991 Outbreak
1150 estimate
115(6 x normal rate) (1990=200 cases)
85% soft contact lens wearers, nearly all used non-Sterile solutions to soak lenses due to FDA approved salt tablets
1994-2003(June ‘03)
190 estimate
19 excludes 137 cases in theIowa flooding outbreak ‘93-’96;; this is the normal disease rate
June 2004-June 2007 Outbreak
485Data from CDC
121(2008 continues at 85 cases/yr or 4.5x the normal rate)
Outbreak cause? EPA decrease of water disinfection level and a constant small number of patients using water in their lens care regimen?
Annualized Incidence Rate of Acanthamoeba Keratitis
¤ One case/ 30,000-million contact lens wearers/ year
¤ Mathers data following Iowa floods (1/10,000)
¤ England incidence study: 17.53-21.42/mil.
¤ Chicago data-19/mil. (Joslin);; 1/8-10,000 CMP users (Schein)
¤ Proctor increase: 1.8/yr (2000-2005) to 5/yr. (2005-2006)
¤ Higher prevalence in Scotland and S. Korea
Seals D: Incidence of acanthamoeba keratitis in contact lens wearers. Eye, 2003;; 17:893
0 20 4010 Miles
-
Chicago-Gary-Kenosha 2000 Metropolitan Statistical Area
LakePorter
Kenosha
CookDeKalb
DuPage
Grundy
Kane
Kankakee
Kendall
LakeMcHenry
Will
Incident AK Cases: 6/03 – 6/05
nactual = 33Nexpected* = 3.7 – 4.4*Schaumberg DA et al, Cornea 1998
Uptick of Acanthamoeba Keratitis
¤ 40 confirmed cases from 6/03-11/05 in the Chicago area.*
¤ Clinical and demographic factors: chlorine levels in municipal water supplies, change in pathogenicity, environmental shifts in biofilms, attachment to new materials
¤ 88% hydrogel wearers, 12% RGP wearers
¤ Orthokeratolgy incidence: 30% of cases of microbial keratitis
¤ Kids may lack antibodies needed to ward off the infection
* *Joslin CE, Tu EY, McMahon TT et al: Epidemiologic characteristics of a Chicago-area acanthamoebakeratitis outbreak. Am J Ophthalmol, 142(2), 2006.

8/28/16
29
Insurgence of AcanthamoebaKeratitis in Contact Lens Wear
¤Background: Acanthamoeba keratitis remains a relatively rare infection among contact lens wearers with recent reports of outbreaks in some geographic areas.
¤CDC reports a disproportionate number of Complete® MoisturePlus™ users in data set.
¤Complete®Moisture Plus™ contains propylene glycol, taurine and new surfactant and lower concentration of EDTA
AMO Recall of Complete Moisture®Plus™ Solutions June 25, 2007
¤CDC interview of 79 soft lens wearers with AK: 45 (60%) reported at least some use of Complete® MoisturePlus™ in the month prior to symptom onset.
¤Patients who used Complete® MoisturePlus™ had a relative risk of 16X or greater for contracting acanthamoeba keratitis
¤Complete®Moisture Plus™ contained propylene glycol, taurine and surfactants with a lower EDTA concentration.
Acanthamoeba Keratitis Case Control Studies: Relative Risk
¤ CDC: Complete® MoisturePlus™- 16.9, "top off" solution 2.8, <5 years wear 2.8
Verani JR, Lorick SA, Yoder JS, et al. National outbreak of Acanthamoeba keratitis associated with the use of a contact lens solution. Emerg. Infect. Dis. 2009;;15(8):1236-1242.
¤ Joslin: Complete® MoisturePlus™- 18.51, Re-use of solution (.5/mo.)- 3.17, "rub" (<10/mo.)- 9.05, showering with lenses (>5/mo.)- 9.07, case replacement (>3 mos.)- 2.79
Joslin CE, Tu E, Shoff ME, et al. The association of contact lens solution use and Acanthamoebakeratitis. Am J Ophthalmol 2007;;29(5):1-8.
Parallels with Fusarium Keratitis 2006 Outbreak
¤ Concurrent outbreaks of keratitis among CLU
¤ Multi-purpose solution implicated¤ Fusarium: Bausch & Lomb ReNu with MoistureLoc¤ No contamination¤ Insufficient anti-microbial efficacy
¤ “Topping off” solution in case common risk factor¤ Reduce anti-microbial efficacy
¤ Concern about safety of multi-purpose solutions
Epidemic Intelligence Conference CDC, April, 2012
¤ Elevated Acanthamoeba Keratitis Incidence Despite a 2007 Outbreak-Associated Product Recall-A Multi-State Investigation, 2008-2011 Brown AC, Ross J, Yoder J, Ayers T, Roy S and Beach M.¤ Multiple CL hygiene practices were associated with increased risk of
AK. The observed persistence of AK might be due to enhanced disease awareness and clinical suspicion following the 2007 investigation.
¤ To prevent infection, CL wearers should observe recommended CL care practices.
RISK FACTORS: topping off solutions 4.54X, recently starting CL use 3.22X, storing CL in water 5.37X, and handling CLs with wet hands 2.17X
Acanthamoeba Keratitis Among RGP Lens Wearers¤ 37 patients in 2 investigations (case control study)
¤ Significant risk factors: ortho-keratology (OR-undefined), sleeping while wearing lenses (OR-8.00), storing lenses in tap water (OR-16.0), and topping-off care solution in case (OR-4.80)
¤ “Nearly one quarter of patients were ortho-keratologywearers. Using tap water and topping off care solutions were identified as modifiable risks. RGP wearers should avoid exposing their lenses to tap water.”
¤ Cope JR, Collier SA, Schein OD, et al: Acanthamoeba keratitis among RGP contact lens wearers in the United States, 2005 through 2011. Ophthalmol.; June,2016.

8/28/16
30
MANNOSE-BINDING PROTEIN (MBP) IS A CRUCIAL LIGAND FOR ADHESION TO THE CORNEAL EPITHELIUM
Acanthamoeba Proxy
¤Legionellosis- live inside amoeba¤Increased reporting in Japan (2004)¤Causes Legionnaires’ disease (gram negative bacteria)
Neil K. Acanthamoeba and its association with Legionellosis. Clin Infect Dis, 14(9), 2000
“Wheat and Rice” Food Source
¤ Stenotrophomonas maltophilia and Delftia acidovorans are bacteria commonly found in cases where there is contamination with Acanthamoeba.
¤ Strategies in designing new MPS: minimizing encystment (1.5X evaporation from “topping off”doubled encystment rate with Complete®MoisturePlus)
Nikolic M, Kilvington S, Cheung S, et al. Survival and growth of Stenotrophomonas maltophilia, ARVO abstract #1540-D831, May 2010, Fort Lauderdale.
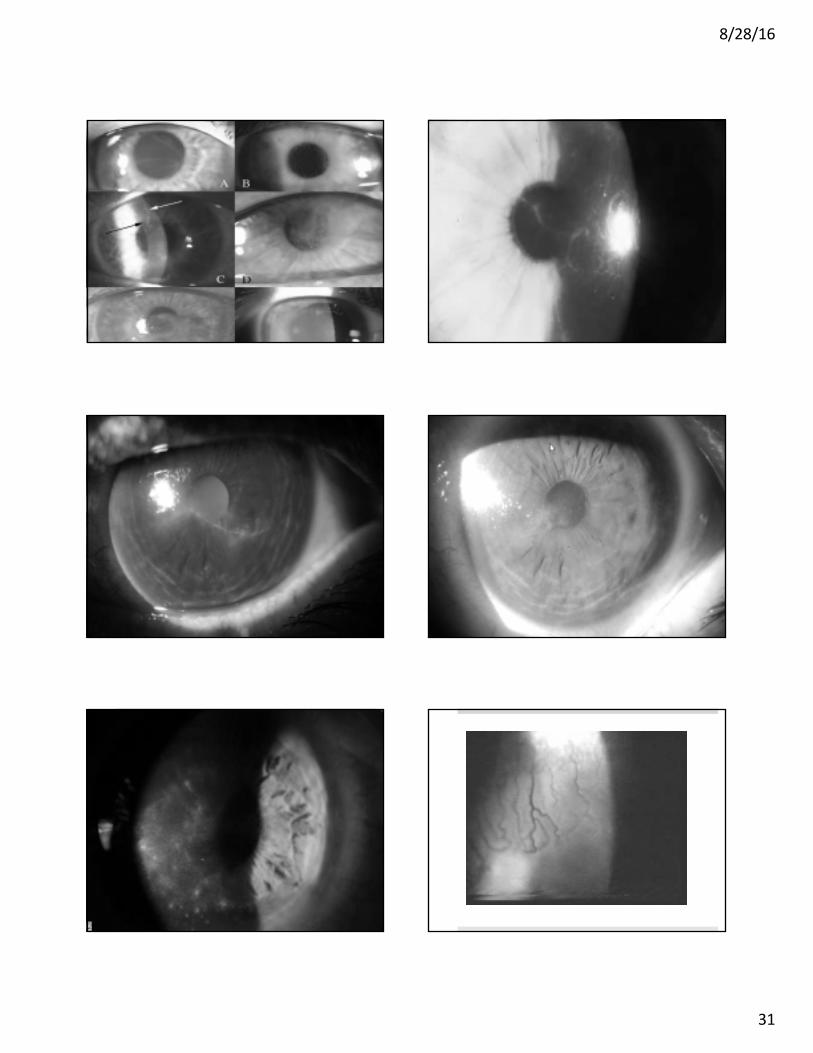
Symptomotology in AcanthamoebaKeratitis
¤ Symptoms: Usually unilateral,* pain disparate to findings, history to trauma and/or contact lens wear, symptoms wax and wane with chronicity
*Large series shows 7-11% bilaterality at time of initial presentation or a few months later. (Tu et al.)
¤ EPITHELIAL: patchy epithelial involvement (stellate, irregular or pleomorphic epitheliopathy) “bull’s eye”lesion, white spots, persistent epithelial defect, elevated corneal lines
¤ STROMAL: lack of vascularization, granulomatous or non-suppurative inflammation, radial nerve infiltrates (“lightning flash”), ring infiltrate
¤ OTHERS: pseudoguttata, hyphema, hypopyon, pseudomembrane, scleritis, episcleritis, adenopathy, decreased corneal sensation (initial)
**poor response to therapy may suggest co-infection
Clinical Features of Acanthamoeba Keratitis
Comparison of Clinical Features With Early vs. Late Diagnosis
Early(%) Late (%)
¤ Punctate keratitis 46 21
¤ Dendritiform ulcer 14 4
¤ Epithelial loss 38 75
¤ Perineural infiltrates 57 29
¤ Limbitis 95 96
¤ Ring infiltrtate 19 83
¤ Uveitis 5 79
Dart JK, Saw VP and Kilvington S: Perspective: Acanthamoeba keratitis-diagnosis and treatment update 2009. Am J Opththalmol 2009;;487-500.
8/28/16
31

8/28/16
32
Diagnostic Confusion With Other Corneal Dendritiform
¤ Acanthamoeba elevated corneal line
¤ Herpes simplex dentrite
¤ Herpes zoster keratopathy
¤ Contact lens “pseudo-dendrite”
¤ Thygeson’s superficial keratopathy
¤ Tryosinemia (Richner-Hanhart)
¤ Other corneal fascinations-edematous formations, verticillata, filaments, stromal dystrophy, post PK hypertrophic epitheliopathy
8/28/16
33
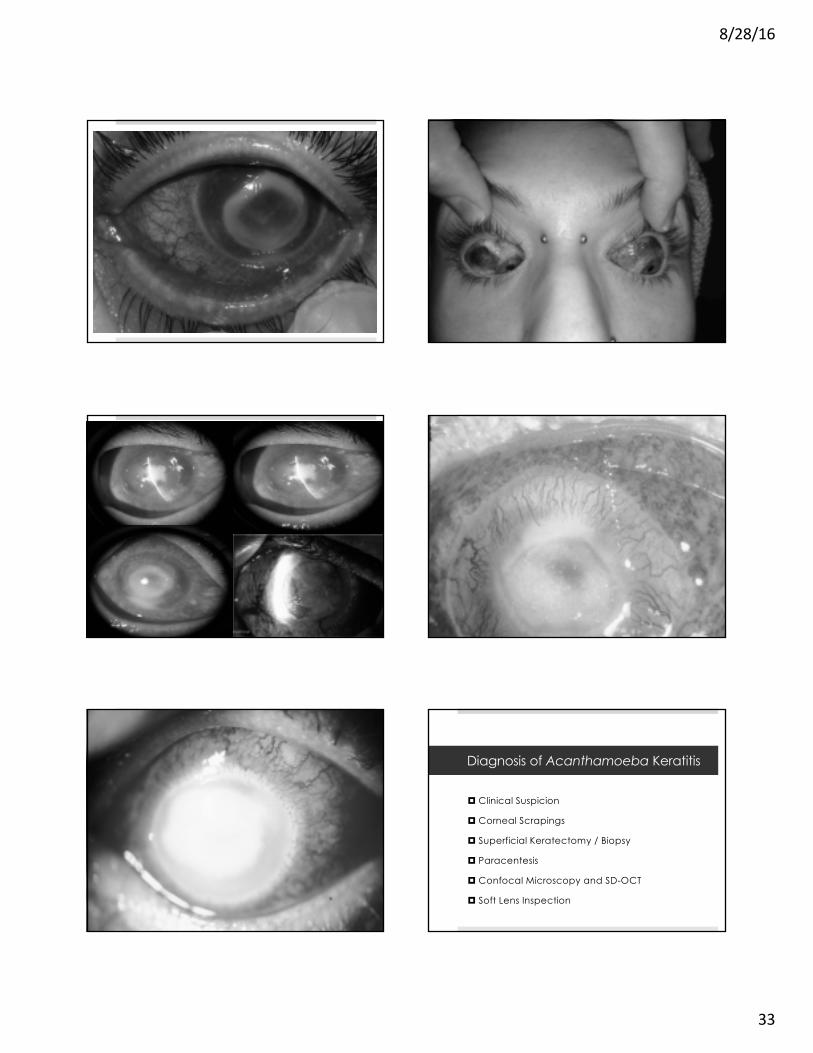
¤ Clinical Suspicion
¤ Corneal Scrapings
¤ Superficial Keratectomy / Biopsy
¤ Paracentesis
¤ Confocal Microscopy and SD-OCT
¤ Soft Lens Inspection
Diagnosis of Acanthamoeba Keratitis
8/28/16
34
8/28/16
35
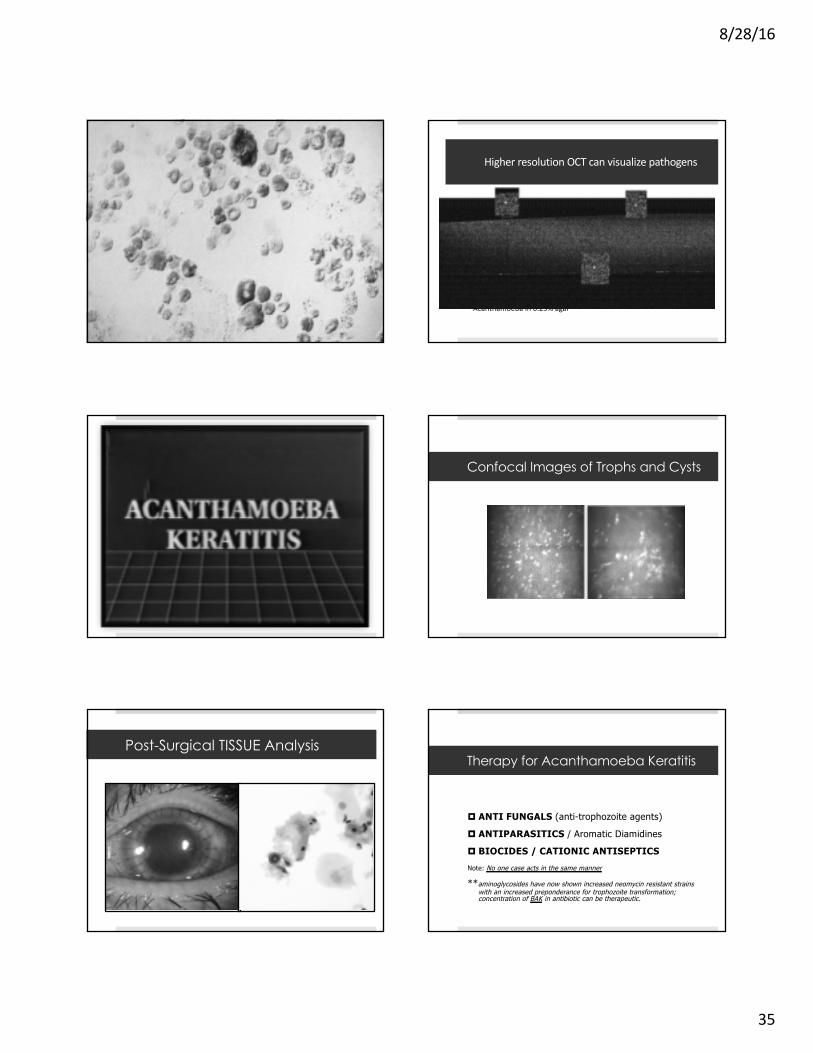
Higher resolution OCT can visualize pathogens
Acanthamoeba in 0.25% agar
Confocal Images of Trophs and Cysts
Post-Surgical TISSUE Analysis
¤ ANTI FUNGALS (anti-trophozoite agents)
¤ ANTIPARASITICS / Aromatic Diamidines
¤ BIOCIDES / CATIONIC ANTISEPTICSNote: No one case acts in the same manner
**aminoglycosides have now shown increased neomycin resistant strains with an increased preponderance for trophozoite transformation;; concentration of BAK in antibiotic can be therapeutic.
Therapy for Acanthamoeba Keratitis
8/28/16
36
Recalcitrant Disease
¤ Can result from drug resistance, polymicrobial infection, infectious/non-infectious inflammation, neurotrophic epithelial disease
¤ Treatment: increase dosage/concentration, change medications, add medication(s)
¤ Additional secondary therapy: voriconazole(topical/oral), pentamide, miltefosine
Treatment and Management of Acanthamoeba Keratitis
¤ SUPPORTIVE AND ADJUNCT THERAPY¤ Debridement**¤ Conjunctival Flaps/Amniotic Membrane Transplants¤ Bandage Lenses¤ Debulking Procedures¤ Cryotheraphy¤ Steroids¤ Cycloplegics¤ Pain Medications
Note: Steroids increase pathogenicity by suppressing macrophages and accelerating trophozoite proliferation.
Clinical Outcome In Treating Acanthamoeba Keratitis¤ Propamidine and neomycin: 9/19 (47%) Meisler¤ Propamidine and PHMB: 8/10 (80%) McCulley
105/111 (96%) Wilhelmus¤ Propamidine and chlorhexidine: 40/42 (96%)
Seals
¤ Miltefosine and PHMB: (unknown) Cope/MMWR** Role of corticosteroid treatment is controversial!Robaei D et al: Ophthalmology. 2014 [Epub ahead of print]-30 days or > of steroid use: 7.92X risk for
poor visual outcome; any steroid use nearly 4X.
Intensive monotherapy with either PHMB or chlorhexidine may be equally as effective (Wills Series), but oral Voriconazole may be beneficial with deep corneal disease. (Tu et al.)
Acanthamoeba Keratitis Outcomes
¤ Keratoplasty was 5X more likely in pts. > 40 years old.
¤ Ring infiltrate pts. were 40X more likely to proceed to keratoplasty and also predicted worse acuity with 3x risk of blindness.
¤ Any sign of stromal invasion was 10X more likely to proceed to keratoplasty.
¤ More advanced disease (late diagnosis) equates to poorer outcomes.
Ross J, Roy SL, Mathers WD, et al: Clinical characteristics of Acanthamoebakeratitis infections in 28 states, 2008-2011. Cornea, 2013 (12).
Prevention of Acanthamoeba Keratits in CL Wear
¤Avoid use of saliva, distilled and tap/well water.¤Avoid swimming and hot tubs while wearing
contact lenses.¤Precautions while showering with lenses in place.¤Hygiene related variables: proper maintenance and
care of lenses includes a ”rub and rinse”, not “topping off”, and replacing lenses and cases regularly.
¤Oxidative disinfection has reasonably good cysticidal effects.
¤Naegleria
¤Hartmanella
¤Vahlkampfiid
¤Microsporidia
¤Rhinosporidia
Additional Protozoan

8/28/16
37
¤ Presents as a superficial punctate, multifocal keratitis and a stromal keratitis is possible following trauma
¤ Nasopharyngeal or urinary colonization in HIV infected patients
¤ Improvement with voriconazole, albendazole and topical fumagillin bicyclohexyl ammonium salts
¤ Repeated debridement (perhaps even swabbing) seems to be therapeutic especially in immunocompetent patients.
*may be best classified as a fungus
Microsporidia Keratitis

8/28/16
38
The Herpesviridae Family
¤ 8 distinct DNA viruses
¤ HSV and HZV are the most common; Epstein Barr is also found to cause corneal insult.
¤ HSV-1 is the most common ocular pathogen; HSV-2 is more responsible for genital infections.
¤ Neonates often infected with HSV-2.
¤ Healthcare costs for the herpes group are over $1 billion each year.
Herpes Simplex Prevalence
¤ 25% are seropositive by age 4, nearly 100% are affected by age 60.
¤ Most are asymptomatic on primary infection.
¤ Skin eruptions are not common after primary infection.
¤ Recurrent HSV is commonly found along the oral or nasal mucosa.
Herpes Simplex Features
¤ Initial ocular presentation occurs on lid and conjunctiva 50% of the time. (anterior cornea 60% and stroma 6%).
¤ Unilateral follicular conjunctivitis is always suspicious for HSV infection. Steroids will trigger infectious keratitis.
¤ Conjunctival dendrites may be present without corneal findings. An iritis with high IOP is concern for HSV!
¤ In children, primary infection manifests with fever and cutaneous outbreak around the lids. Outbreak is prolonged and less responsive to therapy.
¤ Bilateral involvement or prolonged HSV suggests comorbid disease (i.e. atopy, immunodeficiency or immunosuppression). Two or more atopic conditions increases risk 8.9 fold for HSV (2.9 fold for HZO)*
* Borkar DS et al: Association between atopy and herpetic eye disease results from the Pacific Ocular Inflammation Study. JAMA Ophthalmol. 2013; 132(3):326-41.

8/28/16
39
Corneal Presentations
¤ Four clinical presentations: epithelial, stromal, endotheliitis, and neurotrophic keratopathy
¤ Epithelial (Infectious): corneal vesicles, dendritic ulcer, geographic ulcer, marginal ulcer
¤ Stromal (Immune): infiltration, vascularization and scarring/ necrotizing
¤ Endotheliitis: an infectious and inflammatory reaction (HSV or CMV); use anti-viral orals and topical steroids
¤ Neurotrophic: results from altered corneal innervation and decreased tear production

8/28/16
40
Both Stains ?? Additional Value Case 14 - painless Herpes Simplex(not a classic dendrite)
Viral Detection
¤ Cell Cultures
¤ ELVIS (enzyme-linked virus inducible system)**
¤ PCR (polymerase chain reaction/DNA detection)-Intelligent MDx
HSV can be recovered by swabbing an untreated dendrite with a soft tipped applicator inoculating it into viral transport media or a viral culturette.
** high degree of sensitivity and specificity within 24 hrs.
Eczema Herpeticum
¤ Manifests as a rash, fever with typical viral lab results; buccal mucosal swabs will likely show active virus.
¤ Bilateral eye involvement (simultaneous) includes disciform corneal findings and atopic dermatitis or other pre-existing skin disorders.
¤ Diagnosis: culture for HSV, secondary bacterial infections are common
¤ Treatment: compresses, antiviral therapy (topical and systemic); anti-pruritics; patients are in great need of desensitization therapy.

8/28/16
41
Pediatric Herpes Simplex
¤ Frequently misdiagnosed as simply blepharitis or conjunctivitis.
¤ Recurrence rates are higher than adults (50%).
¤ Generally show severe inflammation and stromal disease; adults most commonly have dendritic keratitis.
¤ Managed best with adjusted oral doses of acyclovir.
Liu S, Pavan-Langstan D, Colby KA, Pediatric herpets simplex of the anterior segment, Ophthalmology; 119(10):2003-8, 2012.
Herpes Simplex Masquerades
¤ Various conditions present with branching lesions (dendritiform): Acanthamoeba, healing abrasions, stromal dystrophy, Fabry, tyrosinemia, HZV, and Darrier.
¤ Drug Corneal Toxicty
¤ HSV is the only ulcerative lesion; the rest are excavated!

8/28/16
42

8/28/16
43
Tyrosinemia (Type II)
¤Richner-Hanhart syndrome: rare protein and amino acid metabolic disorder.
¤Characterized by: corneal dendriformlesions, painful planar and plantar hyperkerotosis and retardation.
¤Treatment: dietary restrictions of tyrosine and phenyalanine
Indolent Ulcerations of the Cornea
¤Sterile ulcerations: vitamin A deficiency, vernal shield ulcers, HSV, other corneal irritants
¤Must be differentiated from an infectious process
¤Often difficult to manage without surgical intervention that includes flaps, tarsorrhaphy, autologous serum, or amniotic membrane transplant.
Crack Keratopathy¤ Neurotrophic ulcer results from:
¤ hypesthesia and reduced tearing (inherent), chemical burn (alkali), direct toxic irritant to the cornea (smoke), and mechanical rubbing due to eye irritation.
¤ Ulceration is oval with smooth, rolled edge.
¤ Diagnosis by exclusion when suppuration is present and pain is not proportional.
¤ Persistent ulcers may continue even after cessation.¤ Treatment: tarsorrhaphy, amniotic membrane
transplant or Pro-Kera graft, support for chemical dependency

8/28/16
44
Treatment and Management of HSV
¤ Topical and orals can be used for any infectious process.
¤ Steroids are the mainstay for stromal/immune disease
¤ Avoid prolonged use of topical agents beyond 14-21 days. Limbal deficiency and conjunctival scarring are possible due to toxicity. At >10-14 days, a neurotrophic state is playing a role.
¤ Debridement is only indicated if there are new epithelial lesions with a history of stromal disease in the past.
¤ Oral prophylaxis is indicated with 2 or more episodes of infectious keratitis. Must monitor renal function.
Treating Principles
¤ Treat the epithelial disease first (virtually ignoring the immune/stromal response) and then treat stromal disease.
¤ When using steroids, use a prophylactic dose of orals to hopefully prevent epithelial recurrence.
¤ Taper steroids using a “full” dose of orals and/or topicals until the dendrite has cleared watching for medicamentosa effects. Steroids can be increased with a prophylactic oral dosing (Valtrex 500mg daily, ACV 400mg BID, Famvir 500mg daily).
¤ When stromal disease is controlled taper steroid gradually. You might never be able to DC completely to control stromal disease. Prophylactic orals may be required indefinitely.
HEDS Studies
¤ Oral Acyclovir 400mg BID for one year significantly reduced the risk for recurrence of ocular HS, stromal keratitis (only in those who had a history of stromal disease)and oro-facial HSV. Can be adjusted peri-operatively.
¤ No benefit of oral prophylaxis to prevent progression from surface (epithelial) involvement to stromal disease.
¤ Oral antivirals are considered for epithelial disease to reduce the viral load in the ciliary ganglion and associated nerves. Its value in acute disease is still being debated.
Herpetic Eye Disease Study (Barron et al, 1994)
The Herpetic Eye Disease Study Group (1997)
Neurotrophic Keratopathy
¤ Loss of trigeminal innervation in recurrent HSV and HZV
¤ Full range of corneal signs: PEK/PEE to frank ulceration/melt
¤ Management: D/C meds that are toxic, taping at night to ensure adequate closure (tarsorrhaphy may be necessary)
¤ Topical Treatment: glue, autologous serum, amniotic membrane application (multi-layer), scleral lenses
¤ Experimental: Substance P and insulin-like growth factor with nerve growth factor
HSV Resistance
¤ If viral resistance is suspected, send a viral culture for PCR and sensitivities.
¤ “Super” strains (TK mutants)do encode for key enzyme and prolonged prophylactic use of orals may play a role. Consider Vira A under these circumstances.
¤ Non-compliance can certainly mimic resistance.
¤ GI absorption of polar medications, even with a pro-drug may limit serum concentrations of antiviral medications (especially with lactose intolerant). In this case, IV ACV may be helpful.
¤ Viral resistance in an immuno-competent patient is rare, but if suspected HSV-DNA polymerase inhibitors can be injected intavenously(i.e. Foscarnet) Any resistance raises the concern for immuno-supression or compromised state.
8/28/16
45
Herpes Zoster: Shingles
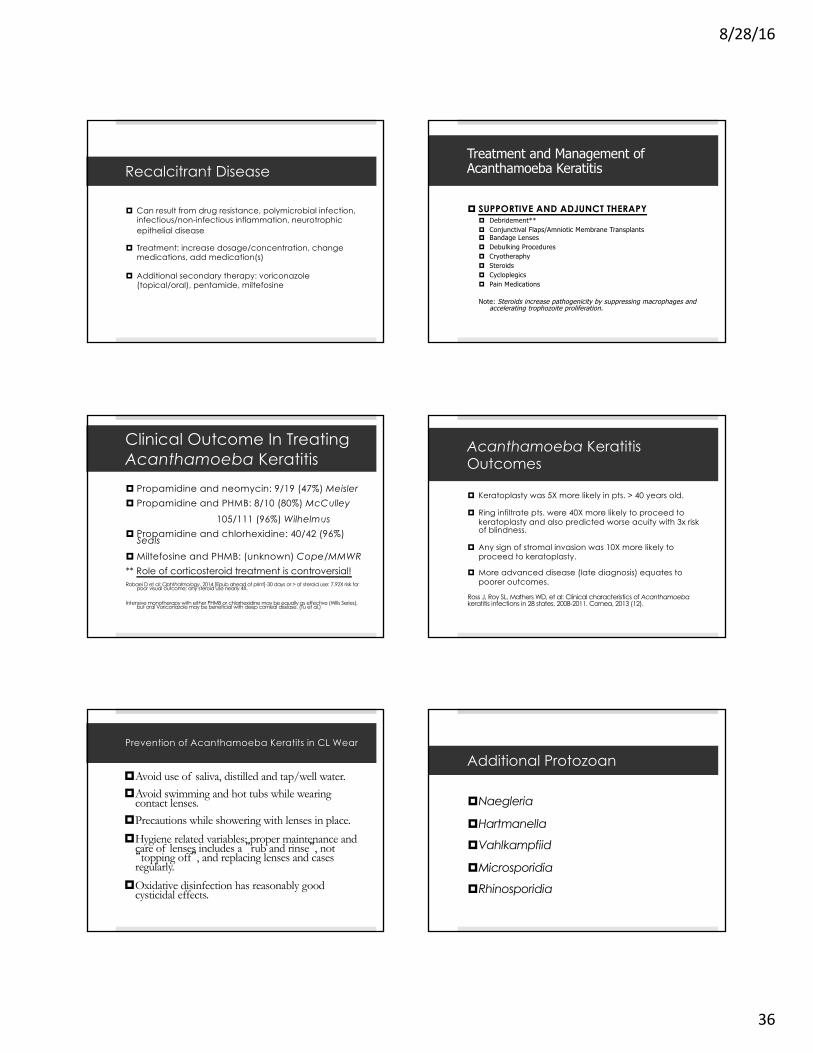
¤ HZV is the etiologic agent of both varicella (chickenpox) and reactivation (shingles)
¤ Unlike HSV, HZV typically happens once in life (30% of adults). Half of adults who live to age 85 will get zoster. The rate rises sharply after 50.
¤ HZV established latency in the sensory root ganglia (maintained by a T-cell immune response that wanes with advancing age)
Herpes Zoster: Shingles
¤ Exposure to cases of chickenpox may serve as a “booster vaccine”.
¤ Recurrent disease: concern for reduced cell mediated immunity…..HIV, thymoma, occult CA (especially lymphoid malignancies), etc.
¤ Most common diseases associated with HZV infection are pulmonary, diabetes mellitus and cardiovascular. IBD increases risk and certain medications are independent risks such as corticosteroids, thiopurinesand ant-TNF.
¤ **Overall, increased risk for CA (lymphatic tumors) among HZV patients. Risk for multiple myeloma is increased in older women; risk for bone and soft tissue cancers in men following HZV infection.
**Does Herpes Zoster Increase Cancer Risk? CME Medscape Education

8/28/16
46
Zoster Sine Herpete
¤ Atypical episode of HZV: chronic radicular pain/sensitivity without rash and vanes from sub-acute to chronic.
¤ Reactivation may result in meningitis, cerebellitis, isoalted cranial nerve palsies (ophthalmoplegia or Ramsey Hunt), vasculopathy, myelopathy and various inflammatory disorders of the eye.
¤ VZV DNA in cerebrospinal fluid or blood mononuclear cells or the presence of IgG antibody in CSF or IgM antibody in CSF or serum.
¤ Continuing challenge is establishing a diagnosis at a time when treatment will still provide a benefit. Can have a severe uveitis.
Gilden D, Cohrs RJ, Mahalingam R and Nagel MA: Neurological disease produced by VZV reactivation without a rash. Curr Top Microbiol Immunol. 2010: 342:243-253.
Herpes Zoster Ophthalmicus
¤ Involves the ophthalmic division of the fifth cranial nerve.
¤ Without oral antivirals, 50% of HZV patients will experience ocular involvement. 30% will be chronic
¤ Long list of ocular complications including: persistent keratitis, uveitis, acute retinal necrosis, cranial nerve palsies and optic neuropathy.
¤ ASSOCIATED COMPLICATIONS- HZO increases the risk of stroke by 4.5X within one year of infection; varicella zoster vasculopathy causes stroke secondary to chronic viral infection of large and small cerebral arteries; VZV has been associated with temporal arteritis (possible trigger?).
Pseudodendrites in Herpes Zoster
¤ Part of the list of corneal complications of acute/chronic infectious and immune keratitis (4-13%).
¤ Can be found in the acute stages or months to years later (Herpes zoster pseudodendrites, dendritic plaques, or late Varicella zoster dendritiform keratitis).
¤ The lesions harbor viral DNA and warrant antiviral treatment to prevent further corneal damage.
¤ CASE SERIES: Pavan-Langstan et al.): topical 0.15% ganciclovir gel (and maybe a repeat of orals) is an effective treatment for persistent pseudodendrites.
8/28/16
47
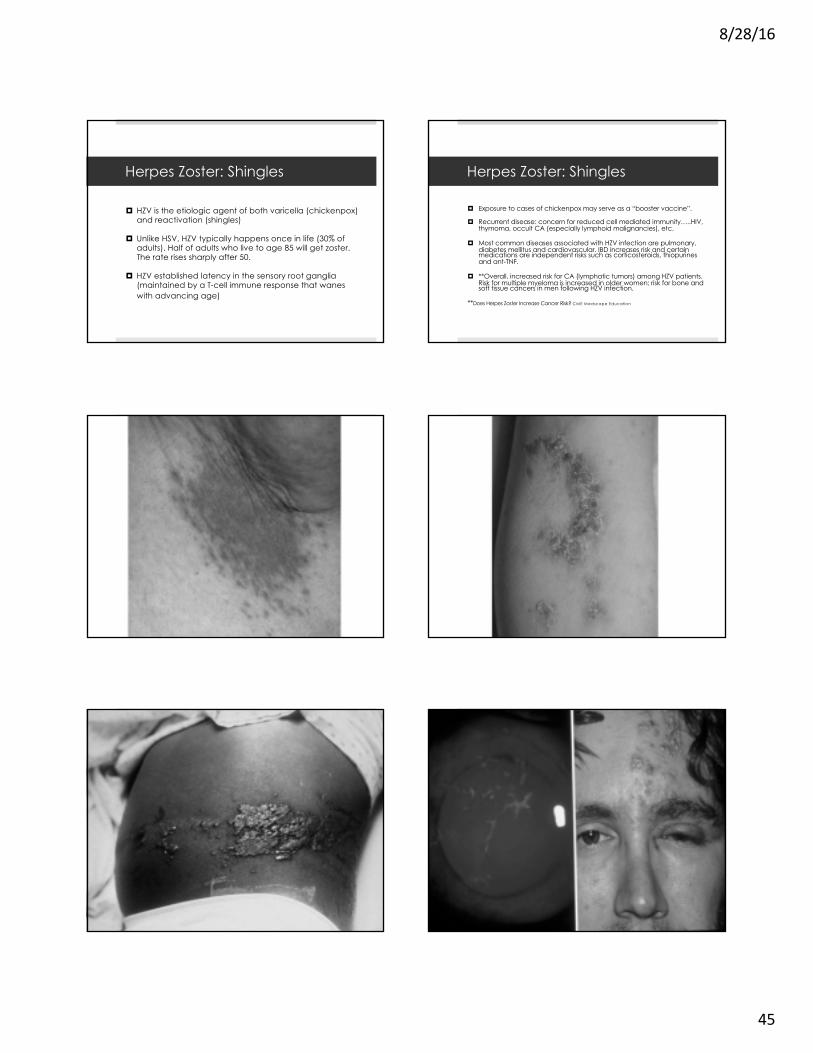
Zoster Kerato-uveitis
¤ Complications are similar to HSV keratitis and include: punctate or pseudo dendritic keratitis (mucous plaque), stromal infiltrates, endotheliitis and neurotrophickeratopathy.
¤ Uveitis is not uncommon in severe cases.
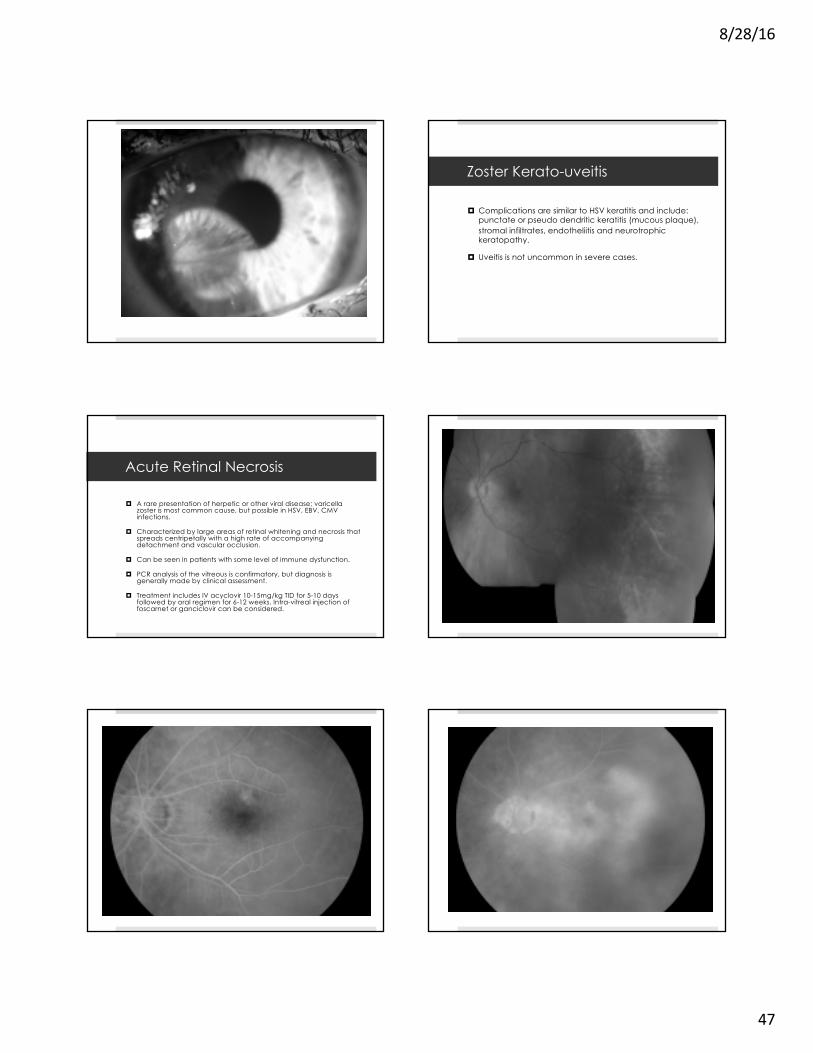
Acute Retinal Necrosis
¤ A rare presentation of herpetic or other viral disease; varicella zoster is most common cause, but possible in HSV, EBV, CMV infections.
¤ Characterized by large areas of retinal whitening and necrosis that spreads centripetally with a high rate of accompanying detachment and vascular occlusion.
¤ Can be seen in patients with some level of immune dysfunction.
¤ PCR analysis of the vitreous is confirmatory, but diagnosis is generally made by clinical assessment.
¤ Treatment includes IV acyclovir 10-15mg/kg TID for 5-10 days followed by oral regimen for 6-12 weeks. Intra-vitreal injection of foscarnet or ganciclovir can be considered.

8/28/16
48
Post Herpetic Neuralgia
¤ A neuropathic pain syndrome that persists or develops after shingles’ rash has resolved (10-18%).
¤ Most frequent and debilitating complication of HZV regardless of the dermatomal distribution.
¤ Main PHN risks: advancing age (>60), severity of acute zoster pain and rash, a painful prodrome and ocular or upper body involvement.
¤ Treatment: cool compresses, topical capsaicin, analgesics, lidocaine patch, cimetidine, amitriptyline, gabapentin, nerve block, and acupuncture
Antivirals
¤ Oral AgentsAcyclovirValacyclovir*Famciclovir*Penciclovir*
¤ Topical AgentsTrifluridine (Viroptic/non-selective)Ganciclovir (Zirgan/selective)
*Better bioavailability and longer intracellular half-life than AcyclovirInterferon has been used as an adjunct
Prevention Through Vaccination
¤ Controversies…..¤ Should healthcare providers be vaccinated?¤ When is vaccination appropriate after having the shingles?¤ Is vaccination appropriate for the high risk groups in certain
cancer protocols/therapies.¤ When should one stop antivirals before/after vaccination?¤ Should patients with active kerato-uveitis or corneal
dendritiform be vaccinated?
Zostavax (Merck & Co.) Vaccine
¤ Vaccination does not confer lifelong immunity (most studies suggest 5-7 years, but exact duration is unknown). Protection likely wanes significantly after 5 years.
¤ About a 50% reduction in HZV occurrence after vaccination. Only a 60% reduction of the risk of experiencing post-herpetic neuralgia.
¤ Should probably be avoided in individuals who are experiencing any significant post-HZV corneal/intraocular inflammation.
¤ FDA recommendation over 50 yrs. of age and CDC is 60.(age for neuralgia is >60 and concern for duration without a booster). However, average age of onset is 52 and half are under 60.
New Vaccine for Shingles (HZ/su)
¤ Phase 3 sub-unit herpes zoster vaccine consisting of a single protein heat inactivated virus
¤ Unlike the live attenuated vaccine the HZ/su vaccine has an efficacy of 97.2% without decline as one ages.
¤ HZ/su is adjuvanted with AS01B that activates antigen-specific CD4+ T cells and antibody.
¤ Single protein that doesn’t replicate and may be suitable for immunosuppressed and compromised patients.
Recurrent Herpes Zoster
¤ Recurrent episodes (different locations) are somewhat atypical and practitioners must consider a sinister etiology.
¤ Patients should be worked up for occult malignancy or other reduced cell mediated immunity concerns (body scans, T4 and T8 subsets may be needed).
¤ HIV/CMV titers are suggested.
¤ Thymus gland imaging may reveal a thymoma.
.

8/28/16
49
Key Points to Remember……..
• New “bugs” are emerging and showing variable resistance with significant geographic differences (Nocardia, Cladosporium, Paecilomyces, Microsporidia, Rhinosporidia)
• There’s a paucity of anti-fungals and most penetrate the cornea poorly. Consider frequent corneal debridement.
• Polymicrobial infection is not uncommon.
• It’s important to culture the edge and base of most infiltrates/ulcers using assorted media. Suture-pass technique may be required for best yield.
• Secondary glaucoma is not unusual due to the direct effect on the trabecular meshwork and carries a poor prognosis especially in fungal disease.
ü5 DAY RULE: a CL related non-specific keratitis should show significant improvement with seemingly appropriate therapy after 5- 7 days.
Key Points to Remember……..
• Bilateral HSV and recurrent HZV may signal a more sinister condition due to reduced cell mediated immunity.
• Poor treatment responses may be due to resistant conditions (including prolonged prophylaxis), poor compliance and a neurotrophic state.
• Vaccine concerns include inoculating corneal graft patients, those already taking oral antivirals, and patients with persistent ocular disease following an initial HZV infection. This doesn’t impart life-time immunity. Varivaxfor kids reduces immunity exposure for adults.
• Antiviral suppression therapy (prolonged) may have a role in chronic HZV as in HSV.
Key Points to Remember……..
• A “spider bite” is often MRSA or shingles, and not a bug bite.
• A review of systems is paramount. Be concerned for systemic viral dissemination in those with debilitating diseases (ie. diabetes, rheumatoid conditions, etc.), especially when oral steroids are used.
• Acute retinal necrosis may not be as obvious as expected in an immuno-compromised or suppressed individual.
• Avoid the use of Valtex in HIV+ patients (concern for TTP/HUS).
• Iritis with high IOP is generally HSV until proven otherwise!