corporate presentation -...
TRANSCRIPT

Corporate Presentation December 2015
Corporate Presentation January 1st, 2018

2
This document does not constitute or form part of any offer or invitation to sell or issue, or any solicitation of any offer to purchase or subscribe for, any shares in the Company, nor shall any part of it nor the fact of its distribution form part of or be relied on in connection with any contract or investment decision relating thereto, nor does it constitute a recommendation regarding the securities of the Company.
This document may contain forward-looking statements and estimates made by the Company, including with respect to the anticipated future performance of TiGenix and the market in which it operates. They include all statements that are not historical facts. Such statements, forecasts and estimates are based on various assumptions and assessments of known and unknown risks, uncertainties and other factors, which were deemed reasonable when made but may or may not prove to be correct. Actual events are difficult to predict and may depend upon factors that are beyond the Company's control. Therefore, actual results, the financial condition, performance or achievements of TiGenix, or industry results, may turn out to be materially different from any future results, performance or achievements expressed or implied by such statements, forecasts and estimates. Forward-looking statements, forecasts and estimates only speak as of the date of this document and no representations are made as to the accuracy or fairness of such forward-looking statements, forecasts and estimates. TiGenix disclaims any obligation to update any such forward-looking statement, forecast or estimates to reflect any change in the Company’s expectations with regard thereto, or any change in events, conditions or circumstances on which any such statement, forecast or estimate is based.
Forward-Looking Statements

3
Compelling Investment Case Lead product near market in Europe, strong partner
ü Seasoned management team with deep experience in drug development
ü Well capitalized: Strong cash position at June 30, 2017 of EUR 56.5 million
ü Traded on the Nasdaq and Euronext (TIG)
Commercial launch expected in 2018: ü Ex-US rights licensed to Takeda, leading company in the GI field ü Up to EUR 380M in potential milestones plus double-digit royalties
First allogeneic stem cell product to receive positive CHMP opinion in Europe ü First indication: treatment of complex perianal fistulas in adult Crohn’s disease
patients 1 => high unmet medical need ü Global pivotal phase III trial for BLA registration started in 2017. Expedite pathway
to market in the US being explored ü US Orphan Drug Designation granted in October 2017
Pipeline: ü Cx611 in phase II for the treatment of severe sepsis ü Three follow-on indications for Cx601 identified
1 Expected label in EU: treatment of complex perianal fistulas in adult patients with non-active/mildly active luminal Crohn’s disease, when fistulas have shown an inadequate response to at least one conventional or biologic therapy

4
Accomplishments in 2017 A year of significant achievements sealed by the positive CHMP opinion for Cx601
• First patient recruited on the SEPCELL study with Cx611 – January 2017
• 52 week data of Cx601 presented at ECCO – February 2017
• Positive 104 week data for Cx601 in Admire-CD – March 2017
• Top line results of CAREMI trial – March 2017
• Launch of Cx601 global phase III trial to support BLA with FDA – June 2017
• Opening of US offices in Cambridge, MA – June 2017
• Granting of commercial production license for expanded facility – September 2017
• Orphan Drug designation of Cx601 in the US – October 2017
• Approval of trade name (Alofisel) and INN (darvadstrocel) for Cx601 – November 2017
• Positive CHMP opinion for Cx601 – December 2017
5
Cx601 (darvadstrocel): Novel, locally administered therapy for the treatment of complex perianal fistulas in Crohn’s disease patients
Positive CHMP opinion received in December 2017
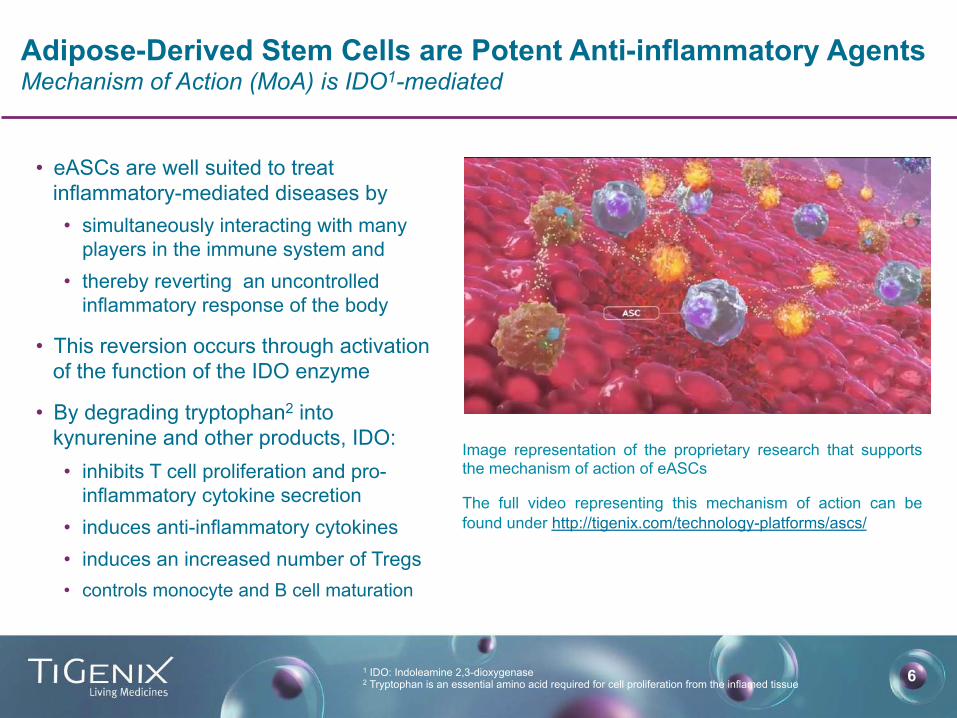
6 1 IDO: Indoleamine 2,3-dioxygenase 2 Tryptophan is an essential amino acid required for cell proliferation from the inflamed tissue
Image representation of the proprietary research that supports the mechanism of action of eASCs
The full video representing this mechanism of action can be found under http://tigenix.com/technology-platforms/ascs/
Adipose-Derived Stem Cells are Potent Anti-inflammatory Agents Mechanism of Action (MoA) is IDO1-mediated
• eASCs are well suited to treat inflammatory-mediated diseases by • simultaneously interacting with many
players in the immune system and • thereby reverting an uncontrolled
inflammatory response of the body
• This reversion occurs through activation of the function of the IDO enzyme
• By degrading tryptophan2 into kynurenine and other products, IDO: • inhibits T cell proliferation and pro-
inflammatory cytokine secretion • induces anti-inflammatory cytokines • induces an increased number of Tregs • controls monocyte and B cell maturation

7
Complex Perianal Fistulas A chronic, common and severe complication of Crohn’s disease
Fistula
Fistula
1 Infliximab- Remicade® and Adalimumab - Humira®
ü Chronic, abnormal communication between the epithelialized surface of the anal canal and the perianal skin
ü Complication of Crohn’s disease for 30−50% of patients
ü Perianal fistulas in Crohn’s disease are difficult to treat with currently available therapies and often lead to pain, swelling, infection, incontinence and social, sexual and employment restrictions
ü Current treatments for perianal fistulas lack long term efficacy and present safety issues1
8
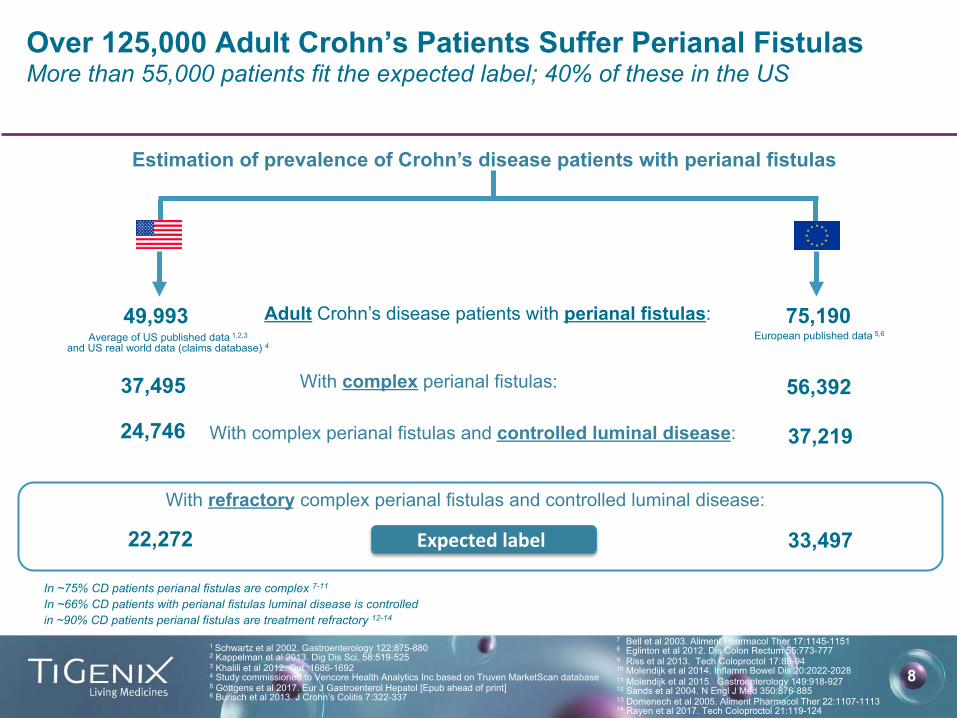
Estimation of prevalence of Crohn’s disease patients with perianal fistulas
75,190
49,993
Over 125,000 Adult Crohn’s Patients Suffer Perianal Fistulas More than 55,000 patients fit the expected label; 40% of these in the US
1 Schwartz et al 2002. Gastroenterology 122:875-880 2 Kappelman et al 2013. Dig Dis Sci, 58:519-525 3 Khalili et al 2012. Gut :1686-1692 4 Study commissioned to Vencore Health Analytics Inc based on Truven MarketScan database 5 Göttgens et al 2017. Eur J Gastroenterol Hepatol [Epub ahead of print] 6 Burisch et al 2013. J Crohn’s Colitis 7:322-337
Adult Crohn’s disease patients with perianal fistulas: Average of US published data 1,2,3
and US real world data (claims database) 4
With complex perianal fistulas: 37,495
24,746
22,272
With complex perianal fistulas and controlled luminal disease:
With refractory complex perianal fistulas and controlled luminal disease:
56,392
37,219
33,497 Expectedlabel
In ~75% CD patients perianal fistulas are complex 7-11
In ~66% CD patients with perianal fistulas luminal disease is controlled in ~90% CD patients perianal fistulas are treatment refractory 12-14
European published data 5,6
7 Bell et al 2003. Aliment Pharmacol Ther 17:1145-1151 8 Eglinton et al 2012. Dis Colon Rectum 55:773-777 9 Riss et al 2013. Tech Coloproctol 17:89-94 10 Molendijk et al 2014. Inflamm Bowel Dis 20:2022-2028 11 Molendijk et al 2015. Gastroenterology 149:918-927 12 Sands et al 2004. N Engl J Med 350:876-885 13 Domenech et al 2005. Aliment Pharmacol Ther 22:1107-1113 14 Rayen et al 2017. Tech Coloproctol 21:119-124
9
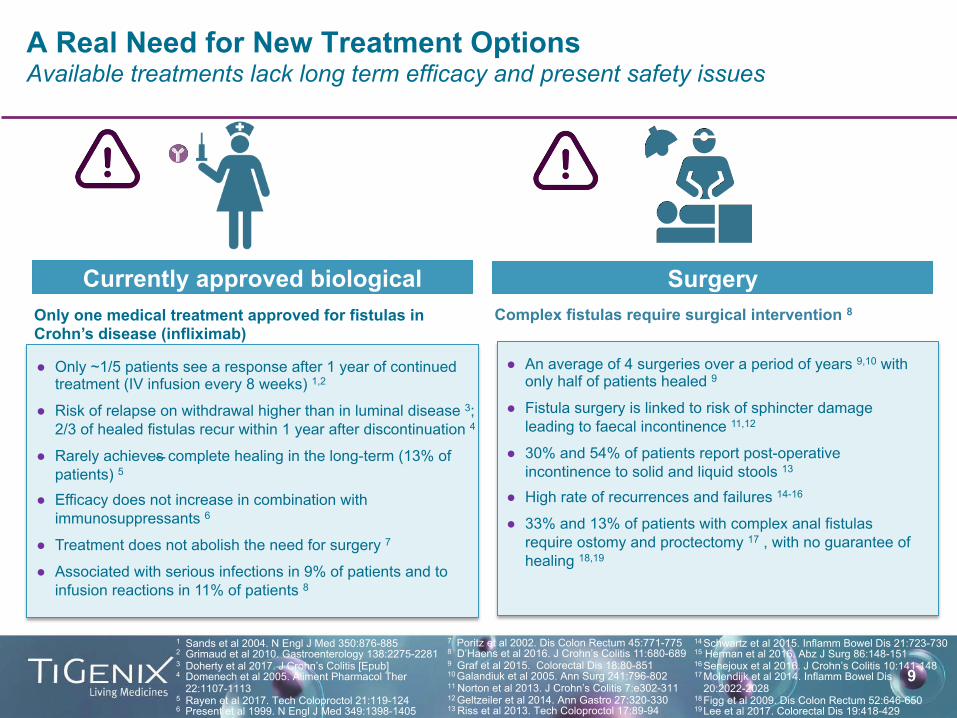
A Real Need for New Treatment Options Available treatments lack long term efficacy and present safety issues
1 Sands et al 2004. N Engl J Med 350:876-885 2 Grimaud et al 2010. Gastroenterology 138:2275-2281 3 Doherty et al 2017. J Crohn’s Colitis [Epub] 4 Domenech et al 2005. Aliment Pharmacol Ther
22:1107-1113 5 Rayen et al 2017. Tech Coloproctol 21:119-124 6 Present et al 1999. N Engl J Med 349:1398-1405
● Only ~1/5 patients see a response after 1 year of continued treatment (IV infusion every 8 weeks) 1,2
● Risk of relapse on withdrawal higher than in luminal disease 3; 2/3 of healed fistulas recur within 1 year after discontinuation 4
● Rarely achieves complete healing in the long-term (13% of patients) 5
● Efficacy does not increase in combination with immunosuppressants 6
● Treatment does not abolish the need for surgery 7
● Associated with serious infections in 9% of patients and to infusion reactions in 11% of patients 8
● An average of 4 surgeries over a period of years 9,10 with only half of patients healed 9
● Fistula surgery is linked to risk of sphincter damage leading to faecal incontinence 11,12
● 30% and 54% of patients report post-operative incontinence to solid and liquid stools 13
● High rate of recurrences and failures 14-16
● 33% and 13% of patients with complex anal fistulas require ostomy and proctectomy 17 , with no guarantee of healing 18,19
Currently approved biological
7 Poritz et al 2002. Dis Colon Rectum 45:771-775 8 D’Haens et al 2016. J Crohn’s Colitis 11:680-689 9 Graf et al 2015. Colorectal Dis 18:80-851 10 Galandiuk et al 2005. Ann Surg 241:796-802 11 Norton et al 2013. J Crohn’s Colitis 7:e302-311 12 Geltzeiler et al 2014. Ann Gastro 27:320-330 13 Riss et al 2013. Tech Coloproctol 17:89-94
Surgery
14 Schwartz et al 2015. Inflamm Bowel Dis 21:723-730 15 Herman et al 2016. Abz J Surg 86:148-151
16 Senejoux et al 2016. J Crohn’s Colitis 10:141-148 17 Molendijk et al 2014. Inflamm Bowel Dis
20:2022-2028 18 Figg et al 2009. Dis Colon Rectum 52:646-650 19 Lee et al 2017. Colorectal Dis 19:418-429
Only one medical treatment approved for fistulas in Crohn’s disease (infliximab)
Complex fistulas require surgical intervention 8
10
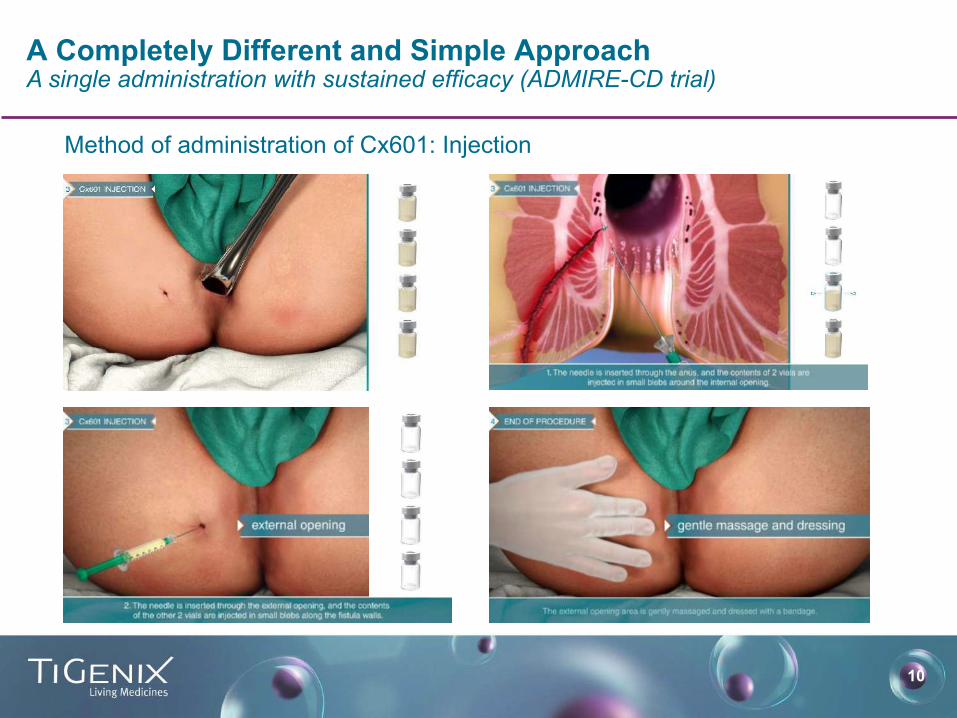
A Completely Different and Simple Approach A single administration with sustained efficacy (ADMIRE-CD trial)
Method of administration of Cx601: Injection

11
Pivotal Phase III Design Validated by EMA and FDA Complex fistulas refractory to best available standard of care • Randomized, double-blind, placebo controlled
• 212 patients randomized 1:1
• Patients with non-active or mildly-active Crohn’s disease
• 40% of patients with multiple tract fistulas
• Draining fistulas despite active treatment (majority anti-TNF)
• All patients stayed on their best standard of care treatment
• All draining tracts treated
• Efficacy defined as combined remission1: clinical remission and lack of abscesses on magnetic resonance imaging => Highly stringent endpoint vs. other studies targeting closing of external opening(s) and cessation of drainage
• Efficacy measured at 24 and 52 weeks. Safety follow up to 104 weeks
1 Closure of all treated external openings draining at baseline despite gentle finger compression, and absence of collections > 2cm by MRI (Magnetic Resonance Imaging)

12
• Cx601-treated patients had a 44% greater probability of achieving Combined Remission than placebo patients
• Shorter median time to Clinical Remission (6.7 weeks for Cx601 vs. 14.6 weeks in the control group)
51.5%
35.6%
0
20
40
60 % Patients
CombinedRemission1atW24(mITT2 Population n= 204)
p=0.021
1 Closure of all treated external openings draining at baseline despite gentle finger compression, and absence of collections > 2cm by MRI (Magnetic Resonance Imaging)
2 mITT: modified Intention To Treat i.e. patients randomized, treated and with ≥1 post-baseline assessment. Efficacy results are consistent across all statistical populations
Cx601 Control
Primary Endpoint Met at Week 24 Results published in The Lancet in July 2016

13
Benefit Sustained, Lower Relapse1 Rate at Week 52
1 Relapse: reopening of any of the treated external openings with active drainage as clinically assessed, or development of perianal collection ≥2cm of the treated perianal fistula confirmed by centrally blinded MRI assessment in patients with clinical remission at any previous visit
2 mITT: modified Intention To Treat i.e. patients randomized, treated and with ≥1 post-baseline assessment. Efficacy results are consistent across all statistical populations
3 Closure of all treated external openings draining at baseline despite gentle finger compression, and absence of collections > 2cm by MRI (Magnetic Resonance Imaging)
• More than 50% of the patients receiving Cx601 had all treated fistulas in Combined Remission3 one year after a single administration of the product
• 75.0% of the patients treated with Cx601 who were in combined remission at W24 did not relapse, compared to 55.9% for patients in the placebo arm
• Safety profile: rate of (serious) adverse reaction comparable to that of the control group
75.0%
55.9%
0
20
40
60
80
56.3%
38.6%
0
20
40
60
Combined Remission at W52 (mITT2 Population n= 204)
p = 0.010
No Relapse Rate at W52
Cx601 Control Cx601 Control
% Patients % Patients
14
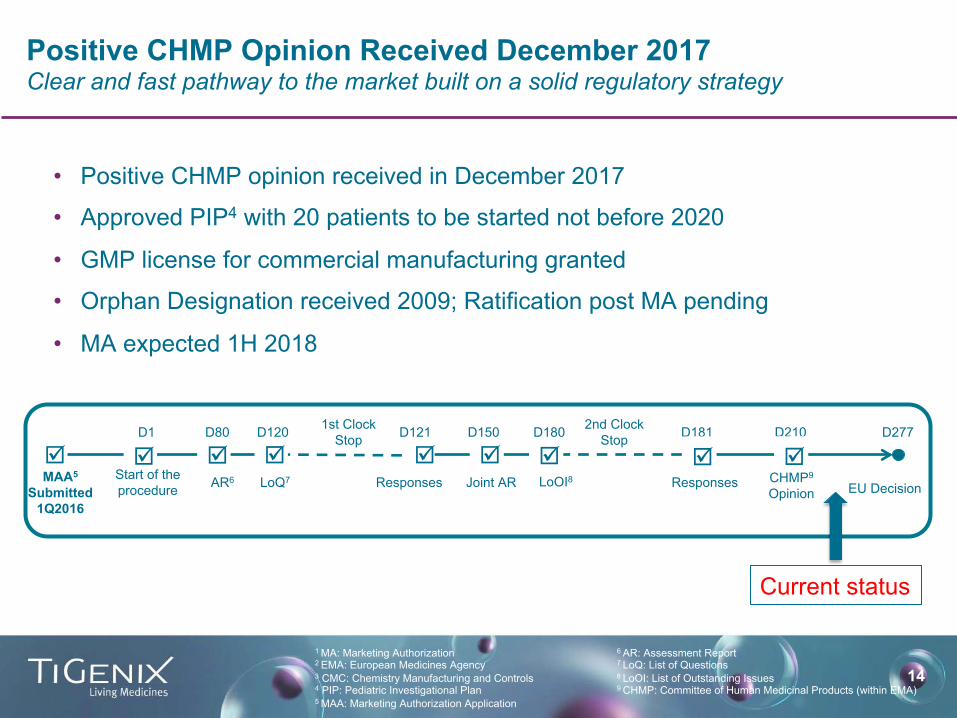
• Positive CHMP opinion received in December 2017
• Approved PIP4 with 20 patients to be started not before 2020
• GMP license for commercial manufacturing granted
• Orphan Designation received 2009; Ratification post MA pending
• MA expected 1H 2018
Positive CHMP Opinion Received December 2017 Clear and fast pathway to the market built on a solid regulatory strategy
1 MA: Marketing Authorization 2 EMA: European Medicines Agency 3 CMC: Chemistry Manufacturing and Controls 4 PIP: Pediatric Investigational Plan
5 MAA: Marketing Authorization Application
6 AR: Assessment Report 7 LoQ: List of Questions
8 LoOI: List of Outstanding Issues
9 CHMP: Committee of Human Medicinal Products (within EMA)
þAR6 LoQ7 Responses Joint AR LoOI8 Responses
D121 D181 D210 1st Clock Stop
2nd Clock Stop
MAA5 Submitted
1Q2016 EU Decision
D277
þ þ þ þD1 D80 D120
Start of the procedure
þD150
þD180
Current status
þ þCHMP9 Opinion

15
Leading experts discuss Cx601’s potential as a new treatment for complex perianal fistulas in Crohn’s disease
1 Analyst and Investor event webcast: https://www.webcaster4.com/Webcast/Page/359/23083
“This drug is going to make a significant contribution to patients in need for this debilitating condition.”1
Dr. Isabelle Lugan, PhD, VP, Global Program Lead at Takeda
“…we as surgeons are so excited by the prospect of a therapy which will both cure the fistula and spare the patient having any loss of control of their bowels. This combination is critically important … we are thrilled that we have something that’s finally an alternative … where we can ideally get these fistulas cured without disturbing the muscle.” 1
Pr. Steven D. Wexner, MD, PhD
“The last drug approved for fistulas was approved in 1988 … so [there has been] no incremental progress in the last 20 years. There remains a considerable number of patients whose fistula tracks don’t close … there is a lot of room to improve the outcomes for these patients.” 1 Pr. William J. Sandborn, MD, PhD
“Cx601 demonstrated significantly greater efficacy compared to control in achieving the primary endpoint, combined remission at week 24, which is a very tough endpoint, in modified ITT populations … Of those patients who achieved combined remission at week 24, numerically a greater proportion of patients receiving Cx601 vs control had non relapse.” 1
Pr. Jean-Frederic Colombel, MD, PhD
16
Ex-US Rights of Cx601 Licensed to Takeda TiGenix retains significant upside potential
• Exclusive ex-US development and commercialization rights to Cx601 for the treatment of complex perianal fistulas in Crohn’s disease patients
• EUR 25M up front plus EUR 10M equity investment
• TiGenix eligible to receive potentially up to EUR 355M in regulatory and sales milestones, including a EUR 15M EU marketing approval milestone
• Double-digit royalties on net sales, tiered to reimbursement price
• Takeda will assume manufacturing responsibilities for Cx601 after an initial period of product supply by TiGenix for the EU
• TiGenix retains full rights to the US market
• TiGenix retains full rights to develop Cx601 in new indications

17
Takeda is the Best Potential Partner for Cx601 Cx601 is the perfect fit for Takeda’s existing IBD portfolio
Source: Takeda presentation (JPM event 2017)
18
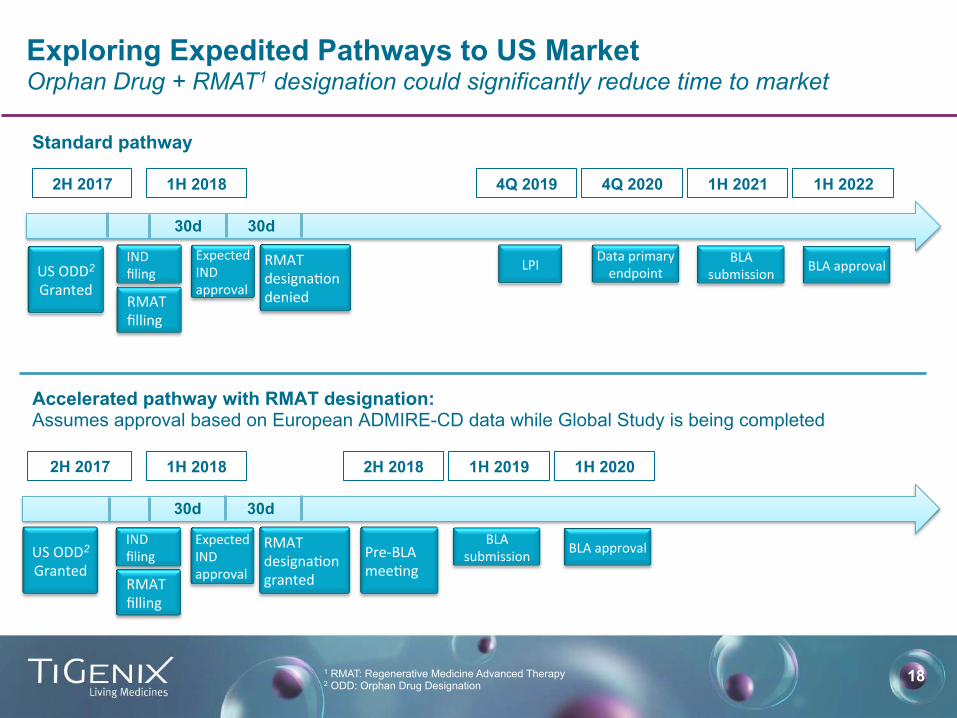
Exploring Expedited Pathways to US Market Orphan Drug + RMAT1 designation could significantly reduce time to market
30d
30d
INDfiling
ExpectedINDapproval
RMATdesigna:ondeniedRMAT
filling
Standard pathway
Accelerated pathway with RMAT designation: Assumes approval based on European ADMIRE-CD data while Global Study is being completed
1H 2018
30d
30d
INDfiling
ExpectedINDapproval
RMATdesigna:ongrantedRMAT
filling
1H 2018
LPI
4Q 2019 4Q 2020
Dataprimaryendpoint
1H 2021
BLAsubmission
1H 2022
BLAapproval
2H 2018
Pre-BLAmee:ng
BLAsubmission BLAapproval
1H 2019 1H 2020
1 RMAT: Regenerative Medicine Advanced Therapy 2 ODD: Orphan Drug Designation
USODD2Granted
2H 2017
2H 2017
USODD2Granted
19
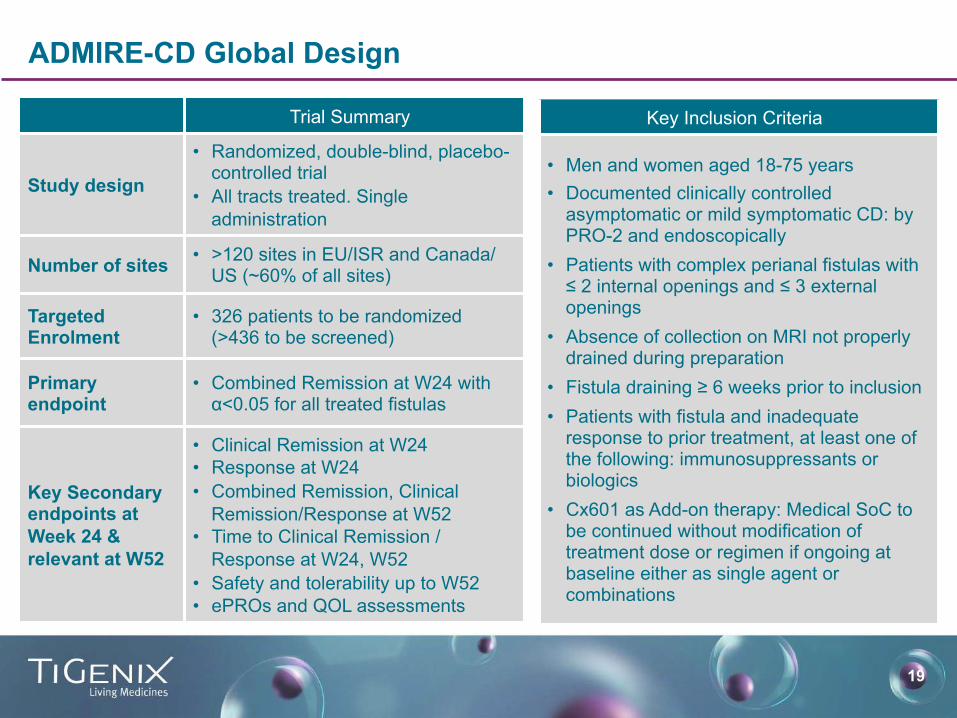
ADMIRE-CD Global Design
Trial Summary
Study design
• Randomized, double-blind, placebo-controlled trial
• All tracts treated. Single administration
Number of sites • >120 sites in EU/ISR and Canada/US (~60% of all sites)
Targeted Enrolment
• 326 patients to be randomized (>436 to be screened)
Primary endpoint
• Combined Remission at W24 with α<0.05 for all treated fistulas
Key Secondary endpoints at Week 24 & relevant at W52
• Clinical Remission at W24 • Response at W24 • Combined Remission, Clinical
Remission/Response at W52 • Time to Clinical Remission /
Response at W24, W52 • Safety and tolerability up to W52 • ePROs and QOL assessments
Key Inclusion Criteria
• Men and women aged 18-75 years • Documented clinically controlled
asymptomatic or mild symptomatic CD: by PRO-2 and endoscopically
• Patients with complex perianal fistulas with ≤ 2 internal openings and ≤ 3 external openings
• Absence of collection on MRI not properly drained during preparation
• Fistula draining ≥ 6 weeks prior to inclusion • Patients with fistula and inadequate
response to prior treatment, at least one of the following: immunosuppressants or biologics
• Cx601 as Add-on therapy: Medical SoC to be continued without modification of treatment dose or regimen if ongoing at baseline either as single agent or combinations

20
“Group A” Controlled
luminal disease
Antib. / Immuno. Not responding
“Group B” Controlled
luminal disease Infliximab
Not responding
“Group C” Controlled
luminal disease
Second biologic Not responding
“Group D” Controlled
luminal disease After failure of repair surgery
Non-controlled luminal disease
Infliximab Not responding
21% 38% 17% 24% ∆54%pa@entsupside
50% 45% 85% 90% 60%
11%
17%
14%
21%
∆51%
pa@entsupside
%ofpa'entsinUSwithineachsubgroup
20
Pa'entsubgroupswithinexpectedlabelinUS
%pa'entsinUSwithineachgrouptreatedwithCx601
%pa'entsinUStreatedwithCx601(fromtotalwithinexpectedlabel)
Sources:Simon-Kucher&Partners;ExpertdiscussionsinJune2016with5medicaldirectors,2ex-Medicarecarriers,2hospitalpharmacydirectors,5KOLsand16HVPs(gastroenterologistsandcolorectalsurgeons)intheUS
Cx601 Product Profile is Extremely Competitive
Prescribing expected to around 2/3 of all patients in the expected label in the US
63%pa@entswithinexpectedlabelinUS

21
Favorable Coverage and Coding Expected for Cx601 in the US Expected coverage by Medicare Part B and commercial medical benefit
Hospital / ASC1 visit:
Diagnosis and treatment decision
If there is an abscess…
Current existing bill for preparation procedure: CPT 46050 and 46020
Conditioning of fistula2:
Bill for procedure
Intra-lesional injection of
Cx601
Bill for drug3 Existing CPT
codes expected to be used
• Cx601 reimbursement will consist of separate bills: one for the drug and another for the administration procedure
• Preparation surgery and conditioning of fistula expected to be billed as independent procedures under currently existing codes
• Expected reimbursement of Cx601 through miscellaneous codes during first year likely not a hurdle for targeted centers of excellence
Sources: Simon-Kucher & Partners; expert discussions June 2016 1 ASC: Ambulatory Surgical Center 2 Removal of seton, curettage and suturing of internal opening 3 Physicians may receive an administration fee
Preparation: Incision,
drainage and seton
placement (Current SoC)
22
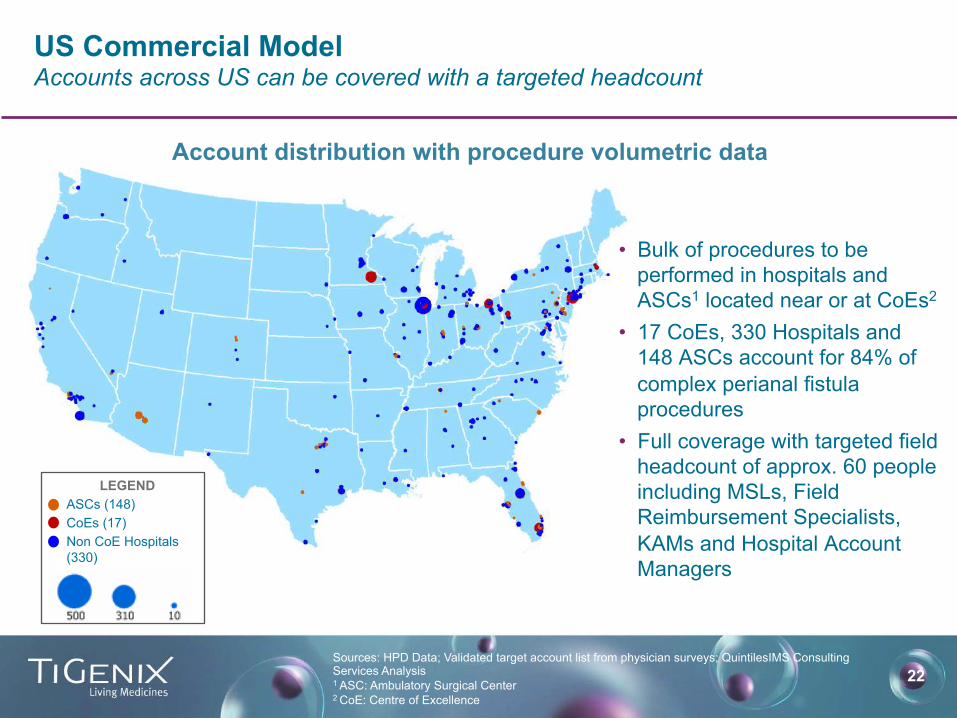
US Commercial Model Accounts across US can be covered with a targeted headcount
Account distribution with procedure volumetric data
LEGEND ASCs (148) CoEs (17) Non CoE Hospitals (330)
• Bulk of procedures to be performed in hospitals and ASCs1 located near or at CoEs2
• 17 CoEs, 330 Hospitals and 148 ASCs account for 84% of complex perianal fistula procedures
• Full coverage with targeted field headcount of approx. 60 people including MSLs, Field Reimbursement Specialists, KAMs and Hospital Account Managers
Sources: HPD Data; Validated target account list from physician surveys; QuintilesIMS Consulting Services Analysis 1 ASC: Ambulatory Surgical Center 2 CoE: Centre of Excellence

23
Cx601 Peak Year Sales Analysts’ Consensus1 for US market Several variables kept today on the “conservative side” provide future upside
1 Sources: Analyst research reports from Bank of America Merrill Lynch, Cowen & Co., Canaccord Genuity, BTIG
Addressable patient population 70,000 – 37,000
10% - 30%
USD 40,000 – 50,000
Penetration rate
Price per dose
PeakYearSalesUSD 270M – 663M
USD 205M – 300M
A commercial opportunity assessment including extensive payer and physician research conducted by Simon-Kucher & Partners in 2016 revealed that potential feasible prices for Cx601 in the US may be significantly above the price range indicated by the analyst reports quoted on this slide. This slide does not represent a recommendation or endorsement of a particular pricing strategy for Cx601 on behalf of TiGenix

24
Cx601 Pipeline Expansion Potential developments for Cx601 beyond complex perianal fistulas in Crohn’s
Other gastrointestinal fistulas Gastrointestinal indications other than fistulas Other indications
25
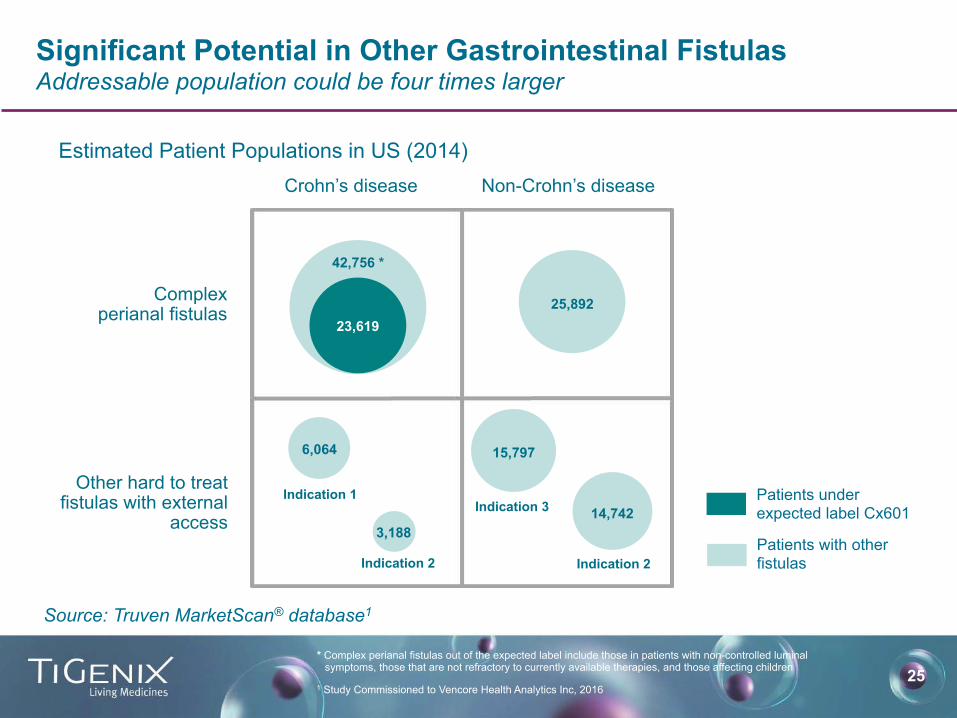
Significant Potential in Other Gastrointestinal Fistulas Addressable population could be four times larger
1 Study Commissioned to Vencore Health Analytics Inc, 2016
Patients under expected label Cx601
Patients with other fistulas
* Complex perianal fistulas out of the expected label include those in patients with non-controlled luminal symptoms, those that are not refractory to currently available therapies, and those affecting children
Source: Truven MarketScan® database1
Estimated Patient Populations in US (2014) Crohn’s disease Non-Crohn’s disease
Complex perianal fistulas
Other hard to treat fistulas with external
access
42,756 *
23,619
6,064
3,188
Indication 1
Indication 2
25,892
Indication 3
Indication 2
15,797
14,742
26
Pipeline
Cx611 – Novel Treatment for Severe Sepsis
27 1 The Lancet Infectious Diseases; Volume 12; issue 2; page 89; February 2012 2 Martin GS Expert Rev Anti Infect Ther. 2012 June ; 10(6): 701–706. 3 Adapted from Lagu, T., et al. Critical Care Medicine, 40(3):754-761; 2012 4 Adapted from: Elixhauser et al. Septicemia in U.S. Hospitals 2009, AHRQ, Healthcare Cost Brief No. 122 October 2011
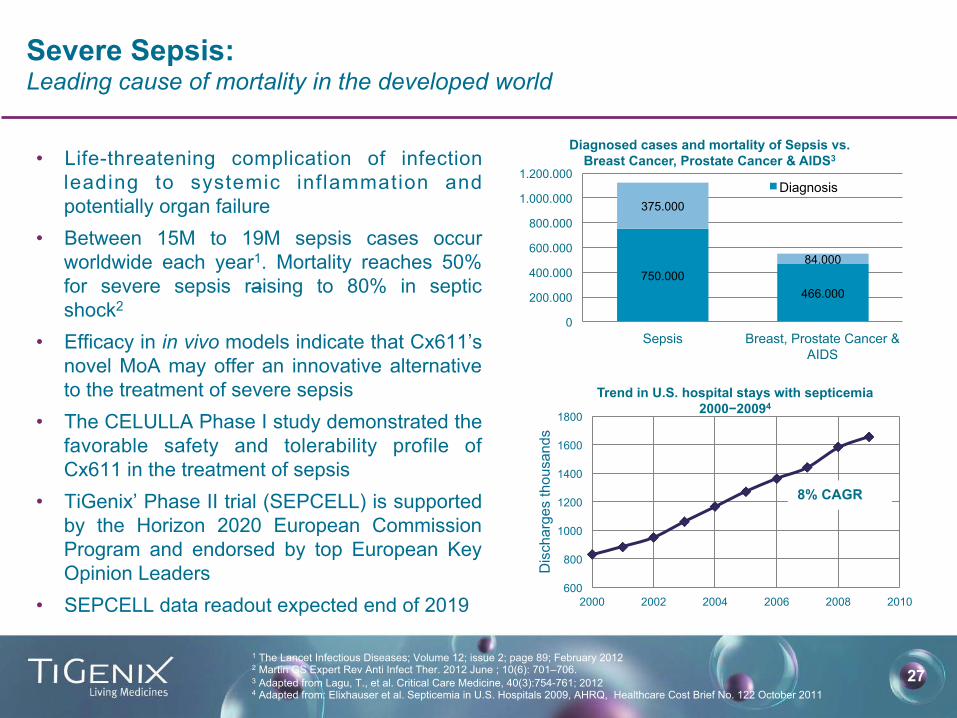
Severe Sepsis: Leading cause of mortality in the developed world
• Life-threatening complication of infection leading to systemic inflammation and potentially organ failure
• Between 15M to 19M sepsis cases occur worldwide each year1. Mortality reaches 50% for severe sepsis raising to 80% in septic shock2
• Efficacy in in vivo models indicate that Cx611’s novel MoA may offer an innovative alternative to the treatment of severe sepsis
• The CELULLA Phase I study demonstrated the favorable safety and tolerability profile of Cx611 in the treatment of sepsis
• TiGenix’ Phase II trial (SEPCELL) is supported by the Horizon 2020 European Commission Program and endorsed by top European Key Opinion Leaders
• SEPCELL data readout expected end of 2019 600
800
1000
1200
1400
1600
1800
2000 2002 2004 2006 2008 2010
Dis
char
ges
thou
sand
s
Trend in U.S. hospital stays with septicemia 2000−20094
8% CAGR
750.000 466.000
375.000
84.000
0
200.000
400.000
600.000
800.000
1.000.000
1.200.000
Sepsis Breast, Prostate Cancer & AIDS
Diagnosed cases and mortality of Sepsis vs. Breast Cancer, Prostate Cancer & AIDS3
Diagnosis
28 28
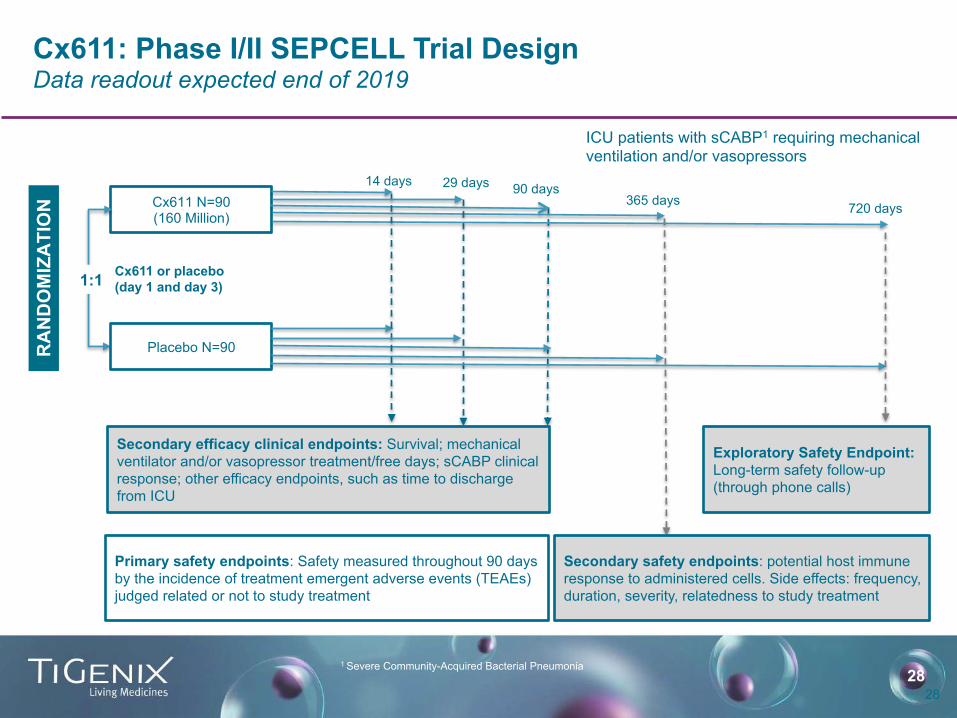
Cx611: Phase I/II SEPCELL Trial Design Data readout expected end of 2019
ICU patients with sCABP1 requiring mechanical ventilation and/or vasopressors
Cx611 N=90 (160 Million)
Placebo N=90
1:1
RA
ND
OM
IZA
TIO
N
Primary safety endpoints: Safety measured throughout 90 days by the incidence of treatment emergent adverse events (TEAEs) judged related or not to study treatment
14 days 90 days 365 days
Cx611 or placebo (day 1 and day 3)
Secondary safety endpoints: potential host immune response to administered cells. Side effects: frequency, duration, severity, relatedness to study treatment
Exploratory Safety Endpoint: Long-term safety follow-up (through phone calls)
720 days
29 days
Secondary efficacy clinical endpoints: Survival; mechanical ventilator and/or vasopressor treatment/free days; sCABP clinical response; other efficacy endpoints, such as time to discharge from ICU
1 Severe Community-Acquired Bacterial Pneumonia
29
Financials
30
Financial Position Significant fundraising completed in 2016
• EUR 23.75 million raised in private placement with specialized investors
• USD 35.65 million raised with NASDAQ IPO (TIG). 4 US analysts covering the stock
• EUR 10 million equity investment from Takeda
• Cash position at June 30, 2017 of EUR 56.5 million
• Main shareholders1
• Grifols (15%) • Cormorant (5%) • Takeda (4%) • JPMorgan Chase & Co (3%)
• Source (1): transparency notification, 13-F Reports, Nasdaq IR insight
31