cost-benefit of integrating cryptococcal antigen screening and preemptive treatment into routine hiv...
TRANSCRIPT

COST-BENEFIT OF INTEGRATING CRYPTOCOCCAL ANTIGEN SCREENING AND PREEMPTIVE TREATMENT INTO ROUTINE HIV CARE
Radha Rajasingham, David Meya, Melissa Rolfes, Kate Birkenkamp, David R Boulware
Presented by: Radha Rajasingham, MD
July 23, 2012

Background
• Cryptococcal Meningitis causes ~20-25% of AIDS-related attributable mortality in sub-Saharan Africa
• Cryptococcal Antigen (CrAg) can be detected >3 weeks before onset of symptoms
• Asymptomatic CrAg+ persons have a high risk of subsequent CM and death, despite ART.
• A new CrAg point of care lateral flow assay (LFA) is available with excellent sensitivity and specificity

Methods
• We assessed the cost-benefit of targeted CRAG screening for patients with CD4<100 using the LFA ($2.50/screen) coupled with preemptive fluconazole therapy for CRAG+ persons entering HIV care in sub-Saharan Africa
• CRAG LFA Cost Components• CRAG LFA Assay $2.00 www.Immy.com
• Lab Supplies $0.05 One pipette tip, one Eppendorf tube
• Labor $0.25• Overhead $0.20• LFA can be shipped/stored at room temperature

• Performed CRAG screening at the Infectious Disease Institute in Kampala Uganda between 2004 and 2007
• CRAG latex agglutination was $16.75 per test• Among HIV+ with a CD4<100, 8.8% (26/295) had
asymptomatic/subclinical cryptococcal antigenemia• 21 were treated with fluconazole (200-400mg x 2-4 weeks), 30-
month survival was 71%• 5 were not treated with fluconazole, and all died within 2 months of
starting ART
Clinical Infectious Diseases 2010; 51:448-55.

Cost-Effectiveness Analysis• Among CD4<100, the number needed to screen in order
to detect one CRAG+ was 11.3 (95% CI: 7.9-17.1)• NNS = 1 / prevalence• NNS = 1 / 0.088
• The number needed to be screened and treated to prevent one death was 15.9 people • NNT life-saved = 1 / (prevalence * survival)
• NNT life-saved = 1 / (0.088 * 0.71)

Based on $16.75 CRAG, this translates to:
• $190 (95% CI: $132-$286) to detect one asymptomatic person with cryptococcal antigenemia
• $266 (95% CI: $185 to $402) to save one person’s life with preemptive fluconazole
• Assuming an average increase in life expectancy of 18 years for a 30yo Ugandan initiating ART with a CD4<100,* this is $14.77 per DALY saved
* Mills EJ, Bakanda C, Birungi J, et al. Life expectancy of persons receiving combination antiretroviral therapy in low-income countries: a cohort analysis from Uganda. Ann Intern Med 2011; 155: 209-216

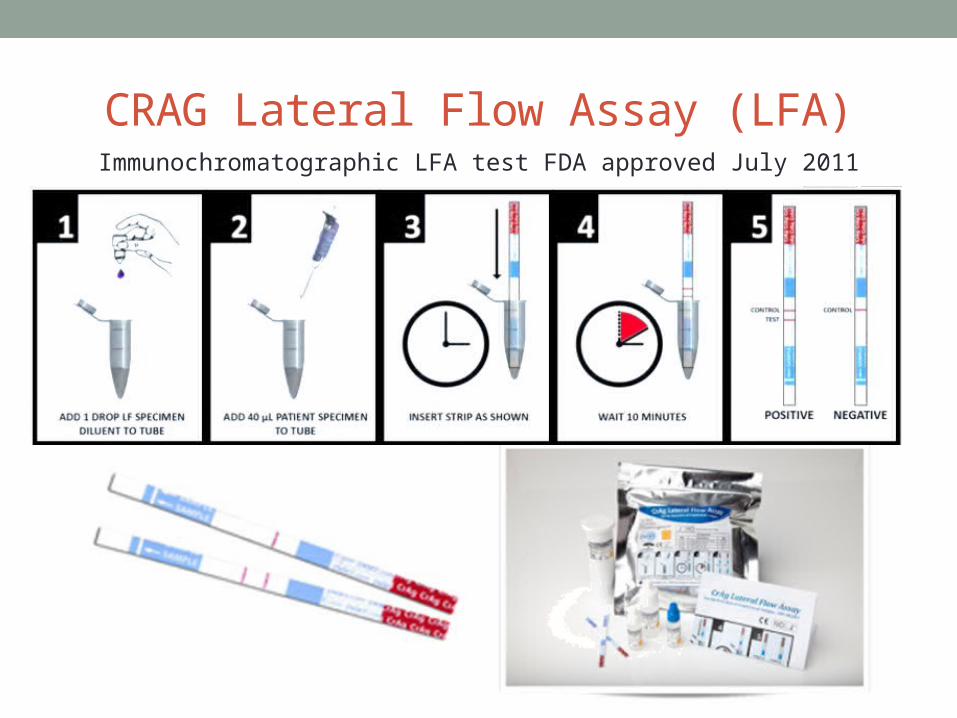
CRAG Lateral Flow Assay (LFA)Immunochromatographic LFA test FDA approved July 2011

Using the same assumptions
• Among HIV+ with CD4<100 cells/µL with CRAG+ prevalence of 8.8%:
• To detect one CRAG+, the number need to screen was 11.3 (95% CI: 7.9-17.1)
• To prevent one death, 15.9 people would need to be screened and treated

Based on CRAG LFA cost of $2.50:
• The cost of detecting one person with subclinical antigenemia with the LFA is $28.37
(95% CI: $20 to $43)
• The cost of saving one life is $39.73 (95% CI: $28 to $60)
• Assuming an average increase in life expectancy of 18 years for a 30yo Ugandan initiating ART with a CD4<100,* this is $2.21 per DALY saved
* Mills EJ, Bakanda C, Birungi J, et al. Life expectancy of persons receiving combination antiretroviral therapy in low-income countries: a cohort analysis from Uganda. Ann Intern Med 2011; 155: 209-216

Prevalence of asymptomatic antigenemia with corresponding cost per life saved based on LFA cost of $2.50 per test
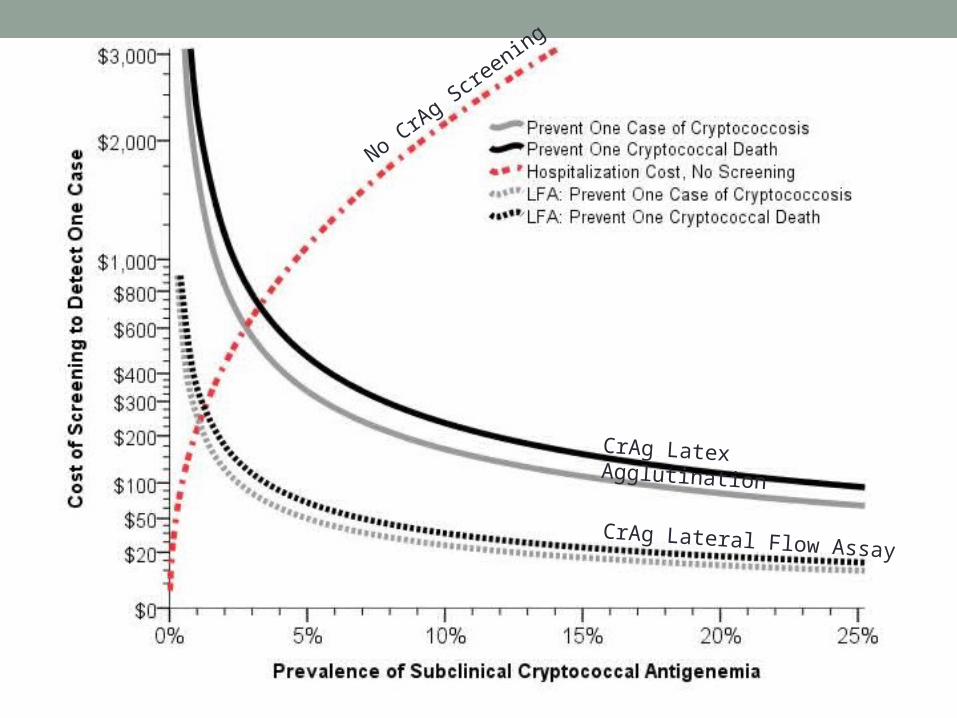
CrAg Latex Agglutination
CrAg Lateral Flow Assay
No CrA
g Screening

• Conversely, the cost of hospitalization and 14 days of
amphotericin for treatment of cryptococcal meningitis is:• $425 per episode in Uganda• $2883 per episode in South Africa
• Thus for the treatment costs of 1 cryptococcal meningitis episode, one could perform CRAG LFA screening on: • 170 persons in Uganda• 1153 persons in South Africa
• Above a CRAG+ prevalence of 1%, pre-ART CRAG screening is COST SAVING compared to the cost of amphotericin and CM treatment
CRAG Screening is Cost Saving

Conclusions
• Targeted CRAG screening and preemptive fluconazole therapy is cost-saving to health care systems and should be integrated into routine HIV care for persons with CD4<100.
• Better understanding of the implementation science is needed to determine how best to scale up CRAG screening and define optimal treatment.