course objectives cpr: ongoing challenges. new solutions. october 2007 © 2007 zoll medical...
TRANSCRIPT

Course Objectives
CPR: Ongoing Challenges. New Solutions.October 2007
© 2007 ZOLL Medical Corporation
This program was made possible by an educational grant from
ZOLL Medical Corporation.
Faculty & Planning Committee Disclosures
Benjamin S. Abella, MD, MPhil1. Paid honorarium for participation in this program. Has also
received honoraria for other educational activities (article, speaking
engagement) performed on behalf of the sponsoring organization.2. No product that is not labeled for the use under
discussion was discussed.3. No preliminary research data was disclosed.
Joseph P. Ornato, MD, FACP, FACC, FACEP1. Paid honorarium for participation in this program. Serves as a member of the Scientific Advisory Board of the sponsoring organization.2. No product that is not labeled for the use under discussion
was discussed.3. No preliminary research data was disclosed.

Target Audience
• Physicians
• Nurses
• Paramedics
• EMTs
• Resuscitation Researchers
Objectives• Upon completion of this program,
the viewer will be able to:– Discuss the effects of chest compression on
Coronary Perfusion (CPP) and Return of Spontaneous Circulation (ROSC)
– List at least three changes in the 2005 AHA Guidelines that relate to CPR performance
– Discuss the outcome of at least one clinical study and one pre-hospital study on the effects of survival with load-distributing band CPR
– Discuss the rationale for implementing CPR prior to defibrillation in cases with extended down time

Key Terms and Abbreviations• AHA American Heart Association• A-CPR AutoPulse CPR• C-CPR Conventional CPR• CPP Coronary Perfusion Pressure• Deploy To implement and position
for readiness• DowntimeNumber of minutes from onset
of sudden cardiac arrest to initiation of
resuscitation efforts
Key Terms and Abbreviations• Duty cycle The time is takes to
complete one cycle• ECC Emergency Cardiovascular
Care• LDB Load-distributing band• ROSC Return of Spontaneous
Circulation• SCA Sudden Cardiac Arrest• VF Ventricular Fibrillation
Circulation is Critical for Survival
• Provides oxygen to preserve vital organ function
• Converts non-shockable rhythms (asystole, PEA) to shockable ones (VF, VT)– More than half of all arrests involve non-
shockable rhythms

Presenting Rhythms in SCARecent studies show that VF or VT
is the initial rhythm less than 50% of the time
Peberdy MA et al. Resuscitation. 2003;58:297-308.Kaye W et al. JAMA. 2002:39(5),Suppl A.Cobb L et al. JAMA. 2002;288(23):3008-3013.
25%
41%
75%59%
0%
20%
40%
60%
80%
100%
120%
Hospital EMS
% o
f C
ard
iac
Arr
es
ts
VF/VT PEA/Asystole

• Why are they non-shockable more than half the time?– EMS
• Long response times
– Hospital• Some drugs (e.g., calcium channel blockers and beta
blockers) significantly shorten the time in which a person is in VF
Presenting Rhythms in SCA

Right Atrial Pressure
(RAP)
Aortic Pressure
(AP)
Coronary Perfusion Pressure
CPP = AP minus RAPCPP = AP minus RAP
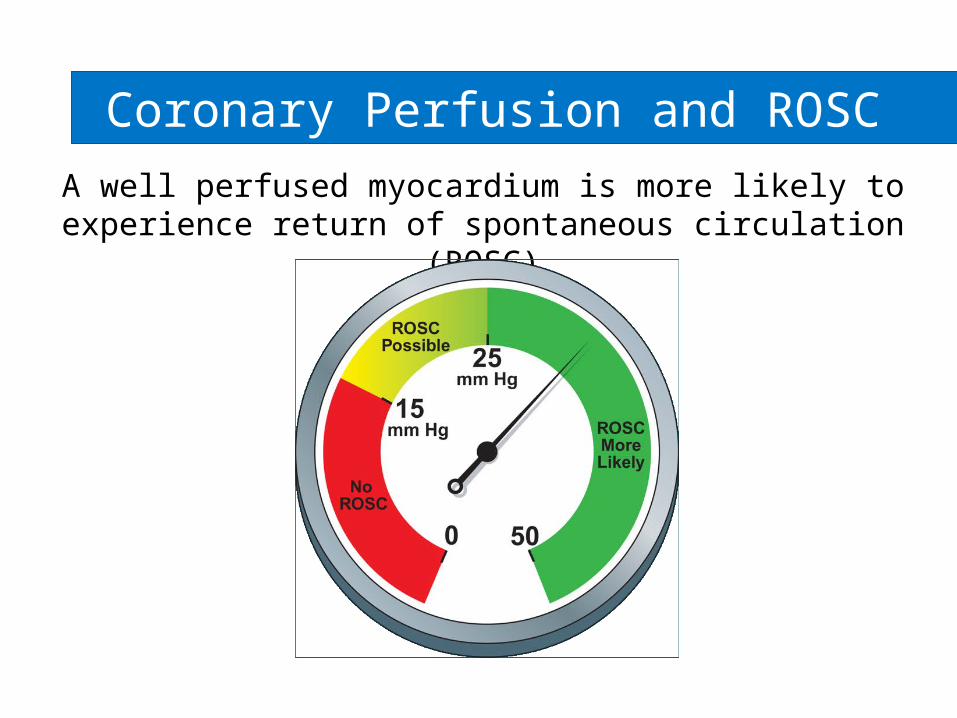
Coronary Perfusion and ROSC
A well perfused myocardium is more likely to experience return of spontaneous circulation (ROSC)
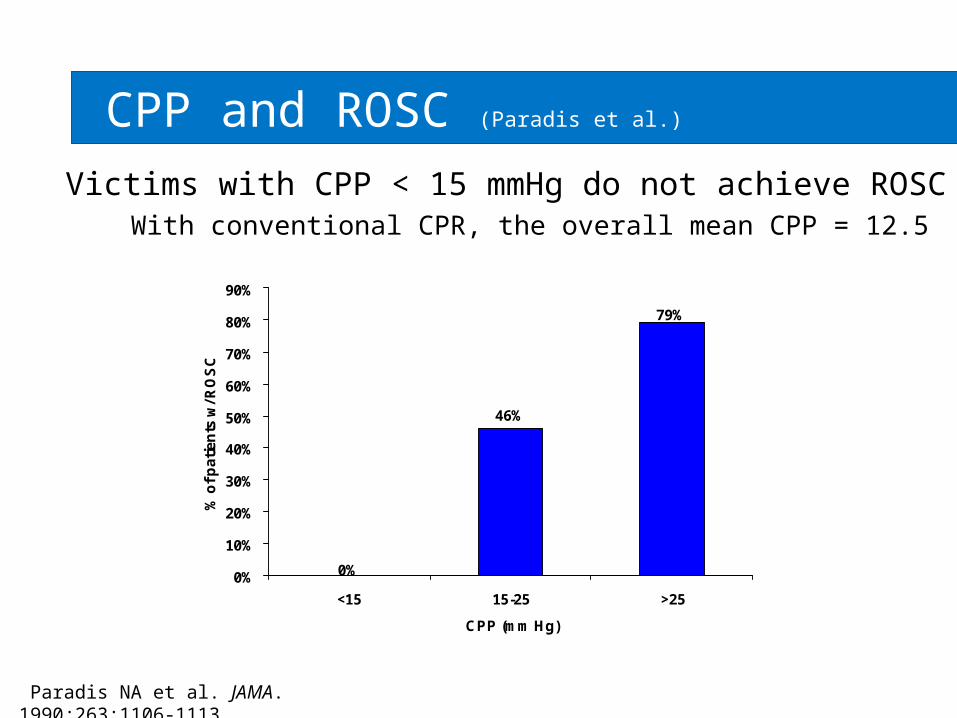
CPP and ROSC (Paradis et al.)
46%
0%
79%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
<15 15-25 >25
CPP (mm Hg)
% o
f p
ati
en
ts w
/ RO
SC
Paradis NA et al. JAMA. 1990;263:1106-1113.
Victims with CPP < 15 mmHg do not achieve ROSCWith conventional CPR, the overall mean CPP = 12.5
AHA Guidelines 2005: CPR
“Simply put: …push hard, push fast, allow full chest recoil, minimize interruptions in
compressions…”
Circulation. 2005;112:IV-206.
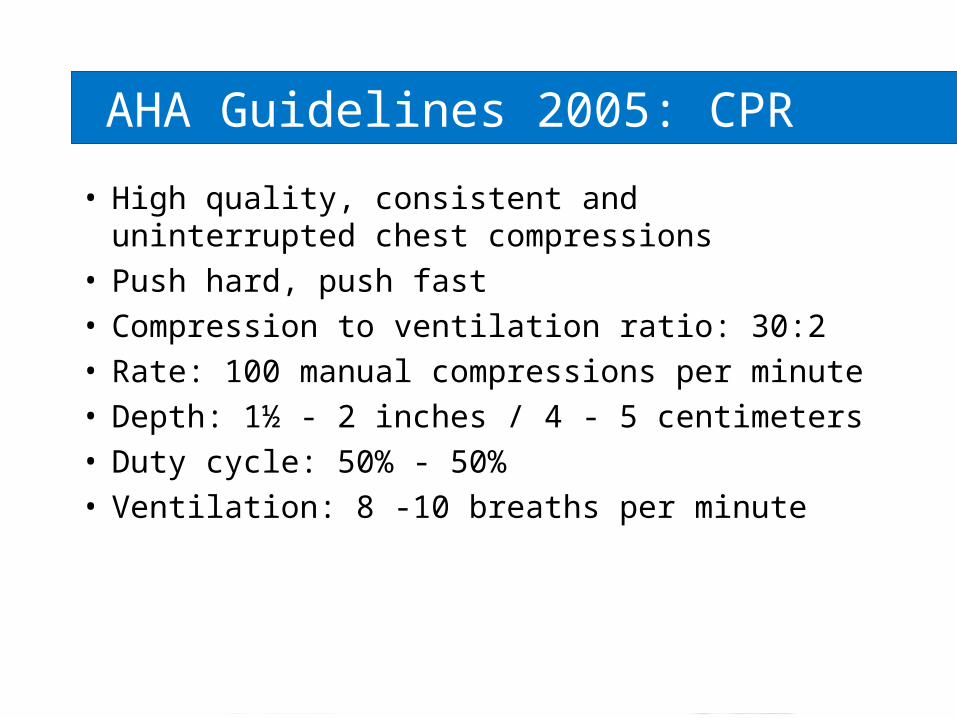
AHA Guidelines 2005: CPR
• High quality, consistent and uninterrupted chest compressions
• Push hard, push fast• Compression to ventilation ratio: 30:2• Rate: 100 manual compressions per
minute• Depth: 1½ - 2 inches / 4 - 5 centimeters• Duty cycle: 50% - 50%• Ventilation: 8 -10 breaths per minute

CPR Challenges
• Poor quality– Inconsistent rate, depth, duty cycle
• Harmful interruptions– Required due to clinician fatigue, patient
transport
• Inadequate cerebral and coronary perfusion
• Ineffective defibrillation support

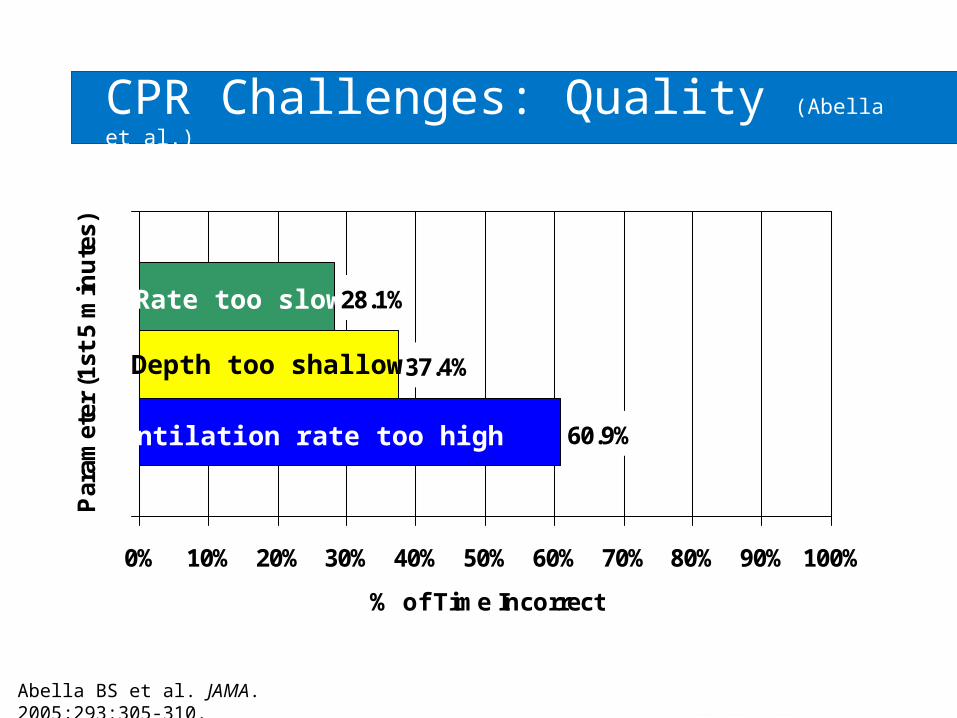
CPR Challenges: Quality (Abella et al.)
Abella BS et al. JAMA. 2005;293:305-310.
• “…quality of multiple parameters of CPR was inconsistent and often did not meet published guideline recommendations….”
Parameter (1st 5 minutes)
Criteria% of Time Incorrect
Rate too slow < 90/min
28.1%
Depth too shallow < 1.5 in 37.4%
Ventilation rate too high > 20/min
60.9%
CPR Challenges: Quality (Abella et al.)
60.9%
37.4%
28.1%
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
Par
amet
er (
1st
5 m
inu
tes)
% of Time Incorrect
Rate too slow
Depth too shallow
Ventilation rate too high
Abella BS et al. JAMA. 2005;293:305-310.
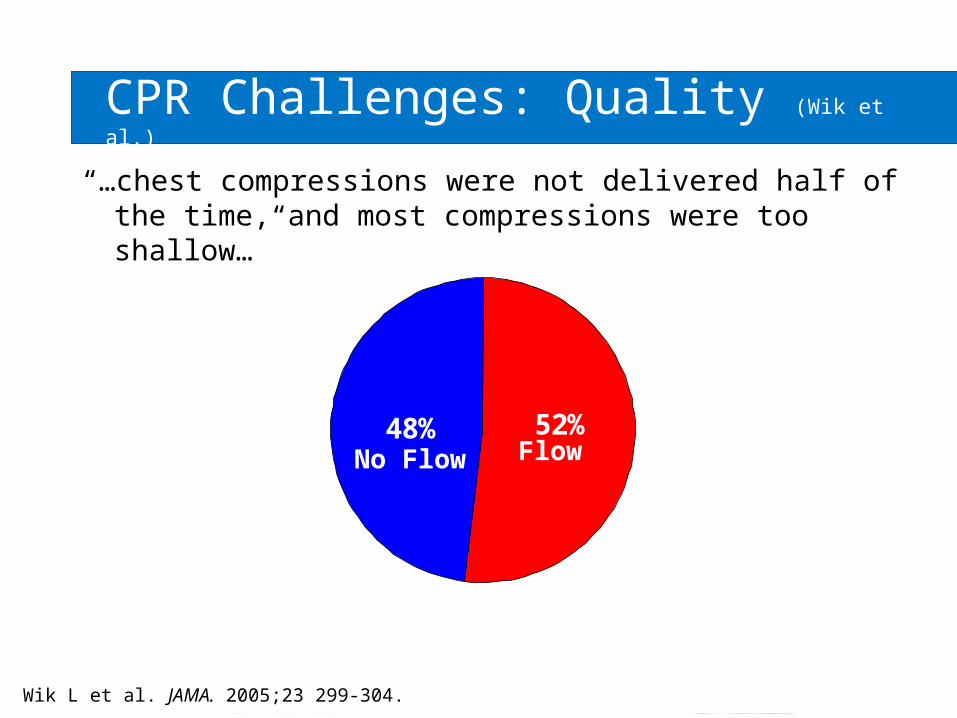
CPR Challenges: Quality (Wik et al.)
“…chest compressions were not delivered half of the time, and most compressions were too shallow…”
52%48%
Wik L et al. JAMA. 2005;23 299-304.
FlowNo Flow

CPR Challenges: Quality
• CPR feedback to rescuers can help improve CPR quality– Elkadi et al.
• Pre-hospital Emergency Care. 2005;8:81-82.
– Handley et al.• Resuscitation. 2003;57:57-62.

Aufderheide TP et al. Circulation. 2004;109:1960-1965.
Mean ventilation rate: 30/minute ± 3.2
first group: 37/minute ± 4 after retraining: 22/minute ± 3
16 seconds
v v v v v v v v v v
CPR Challenges: HyperventilationHyperventilation induces hypotension

Future of CPR Quality Study
International consortium for data collection
Oslo, Norway Vienna, Austria London, UK
Stockholm, Sweden Chicago, USA
Phase I: Collect baseline data on CPR qualityPhase II: Implement feedback system to monitor and improve
CPR performance
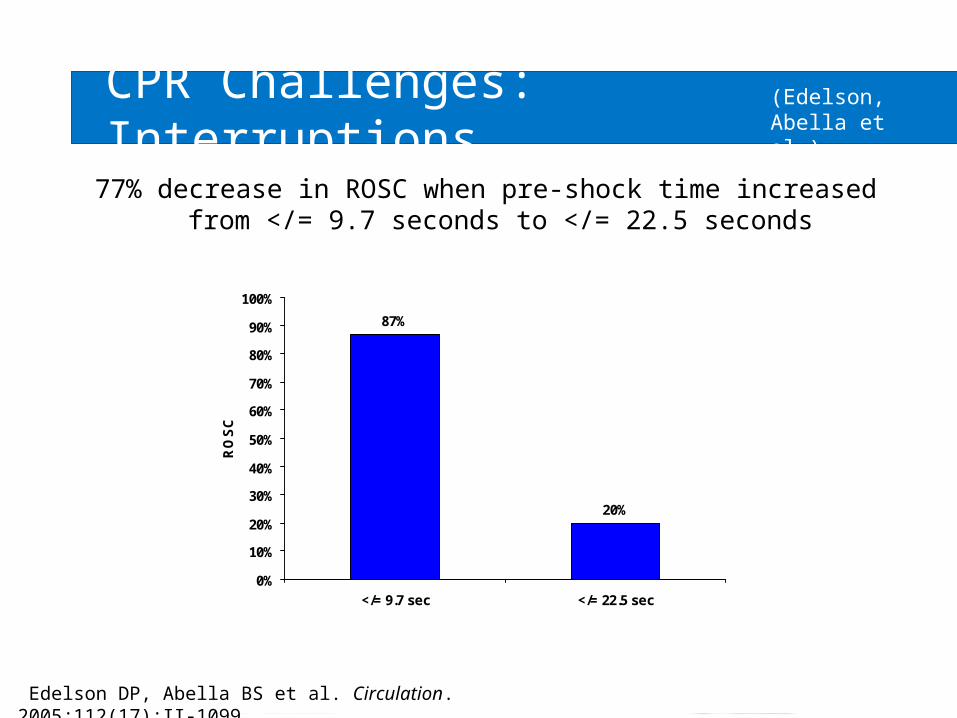
CPR Challenges: Interruptions
77% decrease in ROSC when pre-shock time increased from </= 9.7 seconds to </= 22.5 seconds
Edelson et al. Circulation. 2005;112(17)II-1099
87%
20%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
</= 9.7 sec </= 22.5 sec
RO
SC
Edelson DP, Abella BS et al. Circulation. 2005;112(17):II-1099.
(Edelson,Abella et al.)
CPR Challenges: Interruptions (Kern et al.)
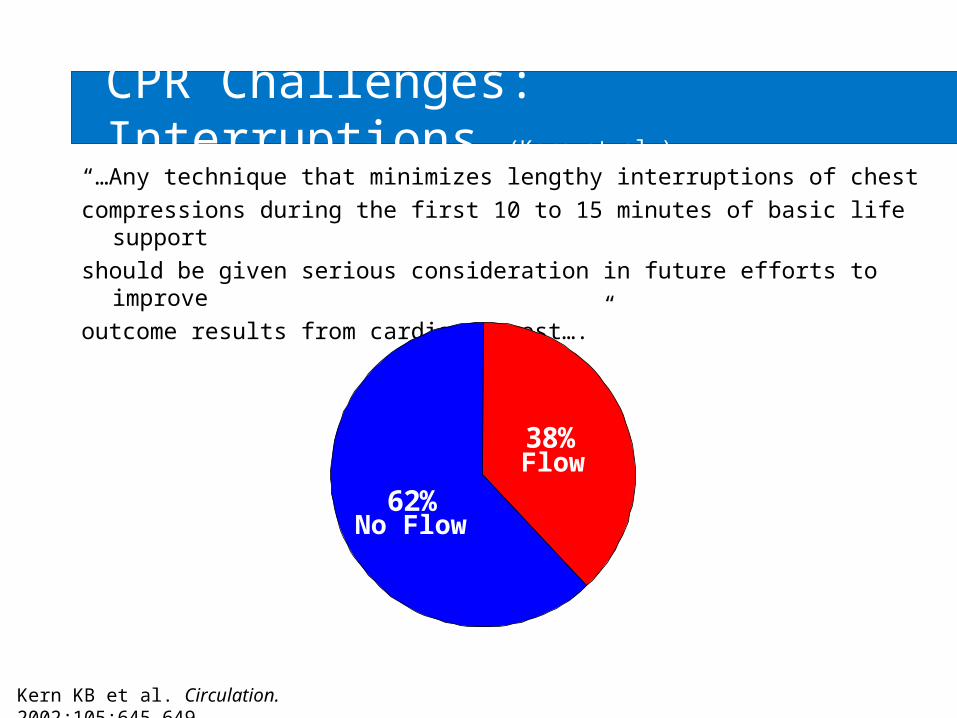
“…Any technique that minimizes lengthy interruptions of chestcompressions during the first 10 to 15 minutes of basic life
supportshould be given serious consideration in future efforts to
improveoutcome results from cardiac arrest….”
38%
62%
Kern KB et al. Circulation. 2002;105:645-649.
Flow
No Flow
Berg et al, 2001
Blo
od
pre
ssu
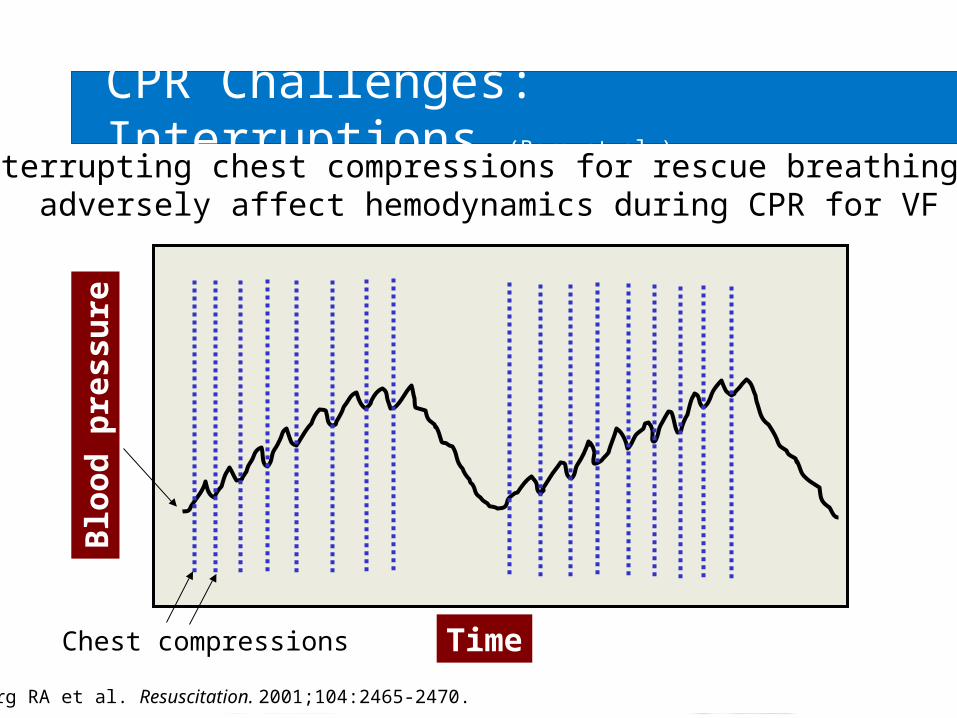
reCPR Challenges: Interruptions (Berg et al.)
Time
Berg RA et al. Resuscitation. 2001;104:2465-2470.
Interrupting chest compressions for rescue breathing canadversely affect hemodynamics during CPR for VF
Chest compressions

CPR Challenges: Perfusion (Kern)
Manual CPR provides minimal blood flow to the heart and brain
30% - 40% of normal flow10% - 20% of normal flow
Kern KB Bailliere’s Clinical Anaesthesiology. 2000;14(3):591-609.

CPR Challenges: Defibrillation Support
After ~4 minutes of VF, the myocardium is nearly depleted of ATP*, a vital energy source needed for successful defibrillation
*Adenosine triphosphate (ATP), which breaks down into adenosine diphosphate (ADP).
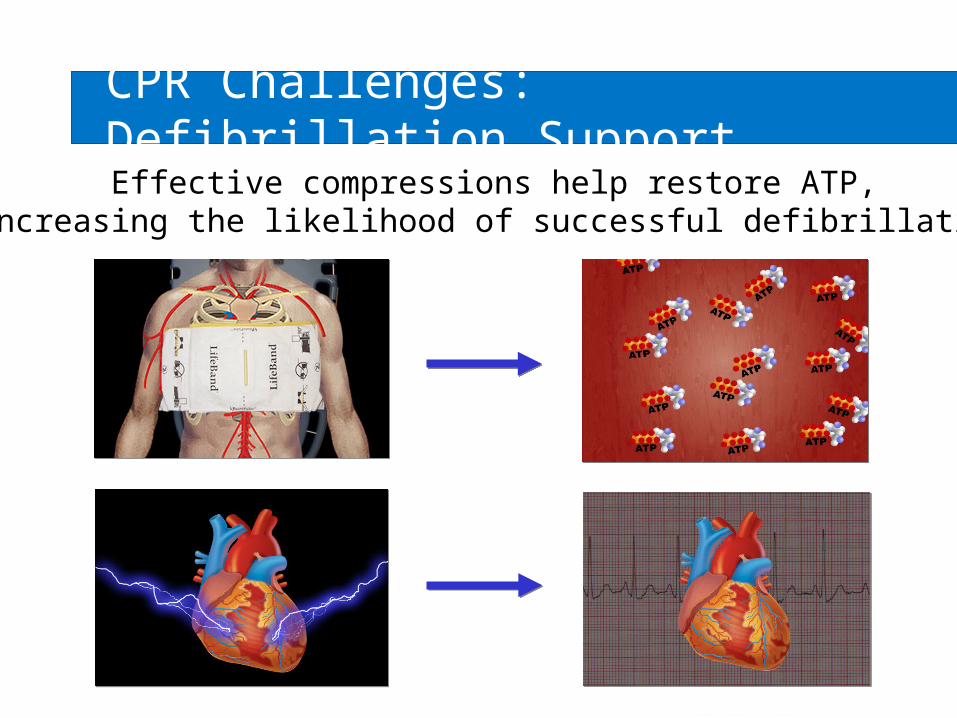
Effective compressions help restore ATP,increasing the likelihood of successful defibrillation
CPR Challenges: Defibrillation Support

Defibrillation is most effective during the first few minutes after cardiac arrest
Engdahl J et al. Resuscitation. 2002;52(3):235-245.Guidelines for CPR and ECC. Circulation. 2000;102(suppl I):I-23.
Defibrillation most effective Circulation
enhances outcome
CPR Challenges: Defibrillation Support

“LDB*-CPR may be considered for use by properly trained personnel as an
adjunct to CPR for patients with cardiac arrest in the out-of-hospital or in-hospital setting (Class IIb).”
AHA Guidelines 2005: LDB CPR
*Load-distributing band.
Circulation. 2005;112:IV-59.
AutoPulse® LDB CPR

AutoPulse LDB CPR• What is the AutoPulse?
– The world’s only load-distributing band chest compression device
• What does the AutoPulse do?– Compressions that humans can’t
possibly do
• What does the AutoPulse do for the SCA patient?– Moves more blood, more
effectively, to the heart and brain– Offers the promise of better
outcomes
Summary of LDB CPR Benefits
• Improved blood flow
• Functions as an “additional person”
• Fast, easy and intuitive to start-up and use
• Clinician safety

Improved Blood flow
• To the brain• To the coronary arteries • Consistent, uninterrupted
compressions• Thoracic and cardiac compression

Dual Function
Compresses onlythe heart
Compresses theentire chest
Cardiac Pump Thoracic Pump
Compresses onlythe heart
Compresses muchof the chest
Compressesmainly the heart
Compresses theentire chest
Functions as an “Additional Person”
• Clinicians are free to perform other critical tasks
• Eliminates clinician fatigue
• Extremely simple user interface
• Automatically “sizes the patient,” calculating…– Size– Shape– Compliance/resistance
• Helps to “organize” or “calm” the code situation
Fast, Easy and Intuitive
Clinician Safety
• No risk of being injured while attempting to do manual compressions during chaotic codes and/or patient transport
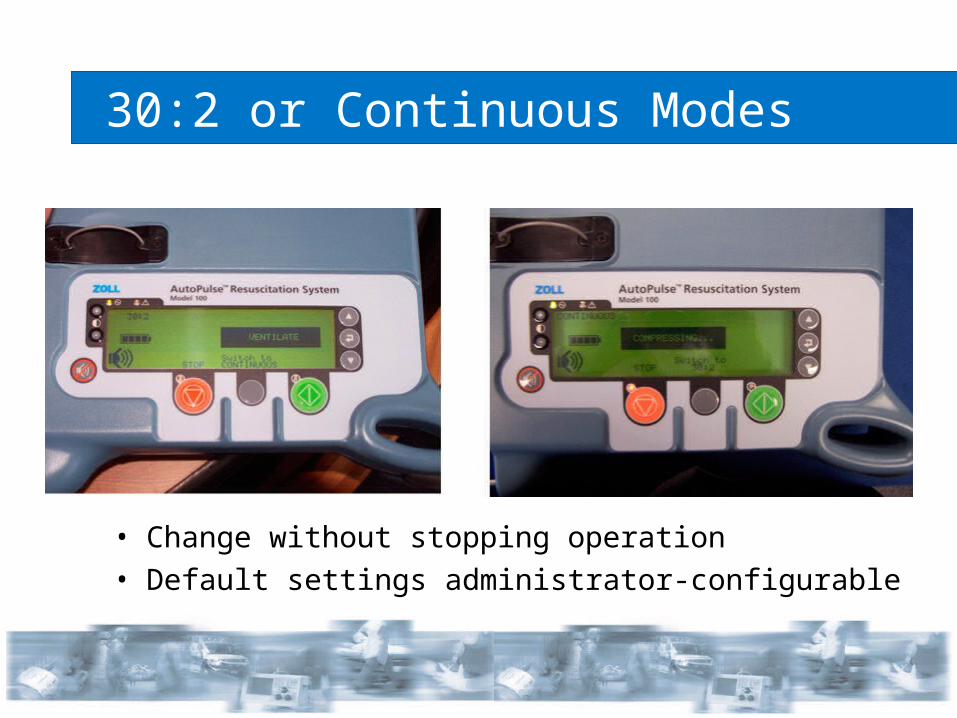
30:2 or Continuous Modes
• Change without stopping operation• Default settings administrator-configurable

Battery Operated
• Minimum 30 minutes of continuous compressions
• Maximum 4¼ hours recharge time

Easily Transportable
Transporter for HospitalsCarry Case for EMS

• Conducted by Halperin et al. @ Johns Hopkins• 20 16-kg pigs induced with VF for one minute• Treated with conventional CPR (“The Thumper”) or
the AutoPulse• Two arms of study
– “BLS” scenario – no epinephrine– “ALS” scenario – with epinephrine
• Regional flow measured with neutron-activated microspheres
Animal Hemodynamics Study (Halperin et al.)

AutoPulse produced pre-arrest levels ofblood flow to the heart and brain
(ACLS protocol – with epinephrine)
Animal Hemodynamics Study (Halperin et al.)
29% 31%
127% 129%
0%
20%
40%
60%
80%
100%
120%
140%
Heart (Myocardium*) Brain (Cerebrum**)
% o
f P
re-a
rres
t B
loo
d F
low
Conventional CPR AutoPulse
Halperin HR et al. JACC. 2004;44(11):2214-20.
*p<0.02**p<0.003

• Conducted by Ikeno et al. @ Stanford• Objective was to evaluate the ability of
AutoPulse’s improved hemodynamics to affect survival
• Used a clinically relevant cardiac arrest model:– 8 min down – 4 min BLS – 4 min ALS
• End-points were ROSC, 24-hour survival and neurologic status at 24-hours
• CPR treatment was randomized to AutoPulse or conventional CPR (“The Thumper”)
Animal Survival Study (Ikeno et al.)
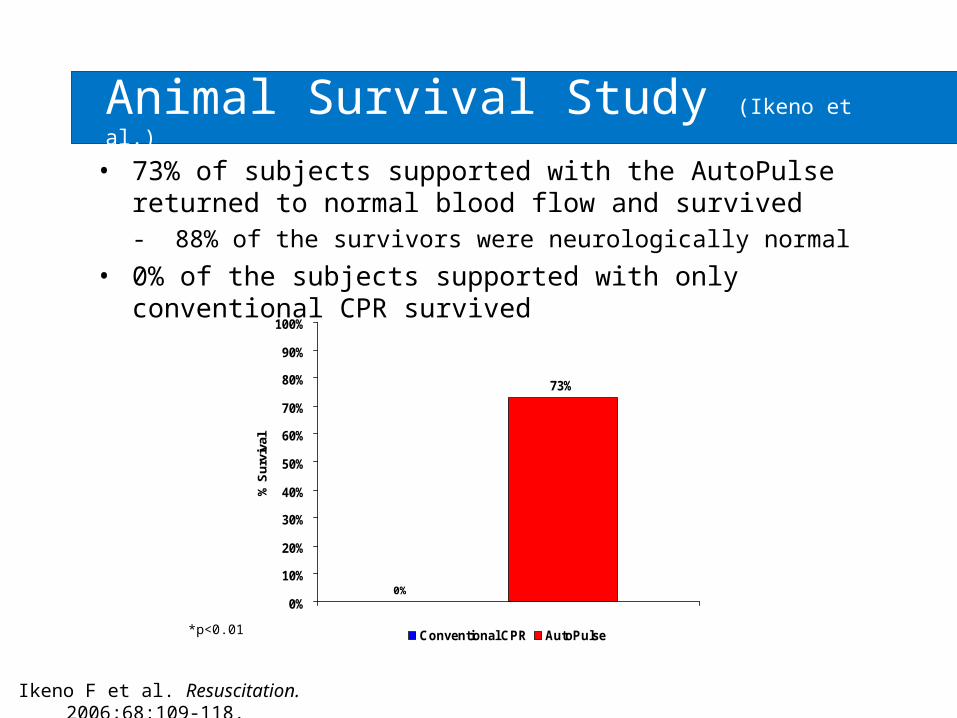
• 73% of subjects supported with the AutoPulse returned to normal blood flow and survived - 88% of the survivors were neurologically normal
• 0% of the subjects supported with only conventional CPR survived
Ikeno F et al. Resuscitation. 2006;68:109-118.
0
73%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
% S
urv
ival
Conventional CPR AutoPulse
Animal Survival Study (Ikeno et al.)
0%
*p<0.01
• Conducted by Timerman et al. in Sao Paolo, Brazil• 16 terminally ill subjects who experienced in-hospital
cardiac arrest• Study initiated after at least 10 minutes of failed ACLS
support• AutoPulse and manual compressions were alternated for
90 seconds each• Catheters were placed in the thoracic aorta and right
atrium to measure CPP and peak aortic pressure• Average time between arrest and the start of
experiment was 30 (+/-5) minutes
Human Hemodynamics Study (Timerman et al.)

AutoPulse-generated Coronary Perfusion Pressure (CPP)was 33% better than manual CPR
Human Hemodynamics Study (Timerman et al.)
Timerman S et al. Resuscitation. 2004;61:273-280.
15
20
0
5
10
15
20
25C
oro
na
ry P
erf
us
ion
Pre
ss
ure
(C
PP
) m
mH
g
Manual CPR AutoPulse
*p=0.015
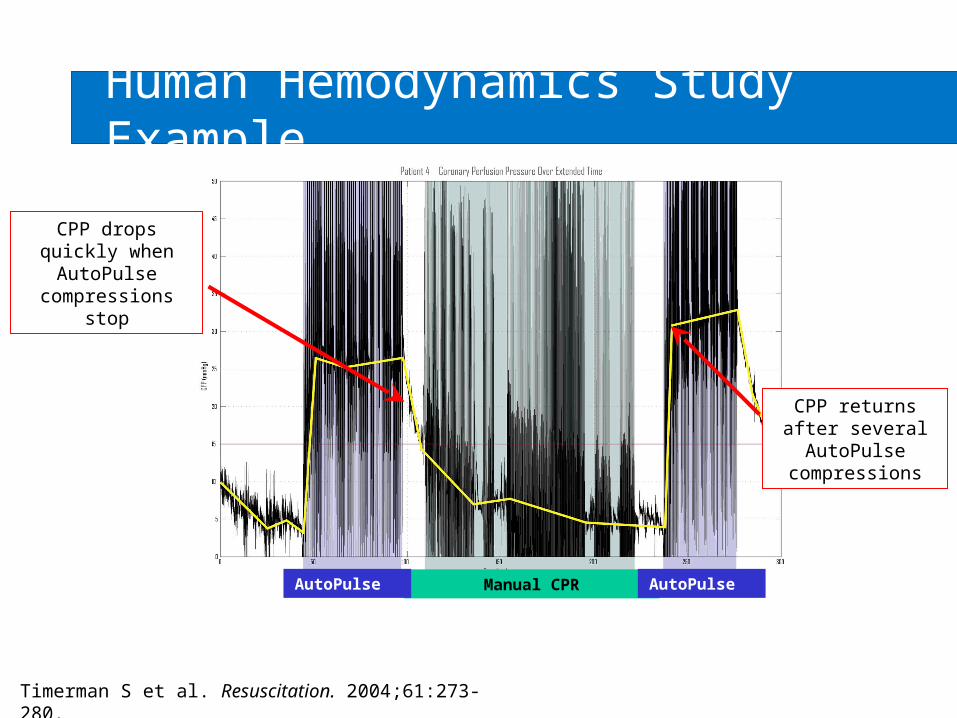
CPP drops quickly when AutoPulse
compressions stop
Manual CPR
CPP returns after several AutoPulse
compressions
AutoPulse AutoPulse
Human Hemodynamics Study Example
Timerman S et al. Resuscitation. 2004;61:273-280.
• Conducted by Casner et al. in San Francisco, CA• Compared the rate of delivery of 162 patients in
ROSC sustained to the ED– 93 patients treated with manual CPR– 69 patients treated with the AutoPulse
• Increased sustained ROSC rate was most pronounced when the initial presenting rhythm was asystole or PEA
Human Short-term Survival Study (Casner et al.)
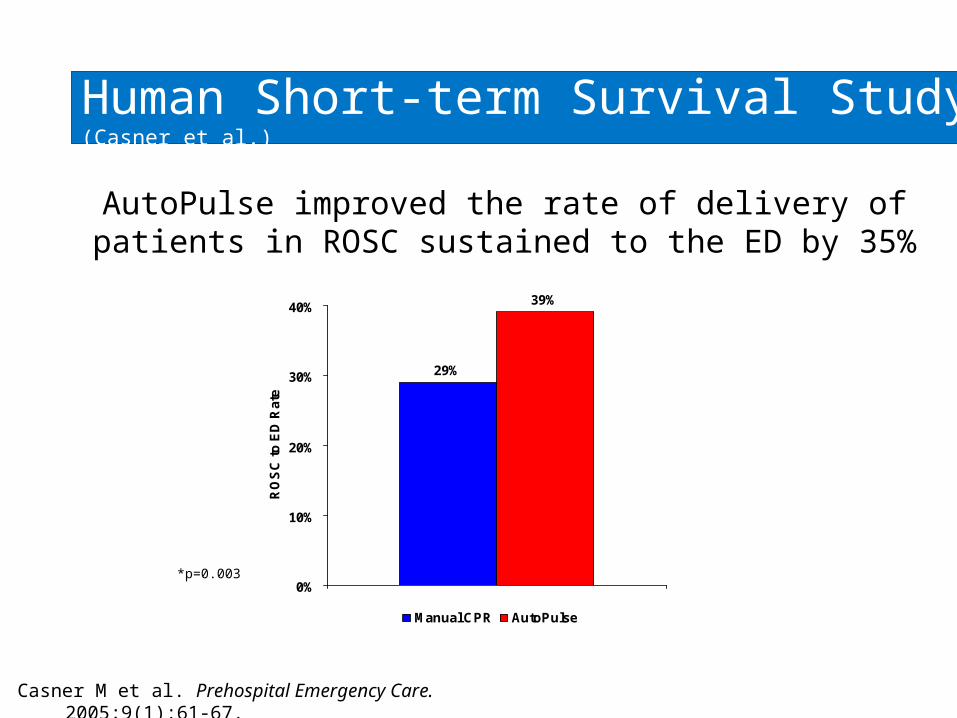
AutoPulse improved the rate of delivery of patients in ROSC sustained to the ED by 35%
Human Short-term Survival Study (Casner et al.)
Casner M et al. Prehospital Emergency Care. 2005;9(1):61-67.
*p=0.003
29%
39%
0%
10%
20%
30%
40%
RO
SC
to
ED
Ra
te
Manual CPR AutoPulse

• Conducted by Swanson et al. in Volusia County, FL• Compared the rate of delivery of 523 patients in
ROSC sustained to the ED– 405 patients treated with manual CPR– 118 patients treated with the AutoPulse
• Increased sustained ROSC rate was most pronounced when the initial presenting rhythm was asystole or PEA
Human Short-term Survival Study (Swanson et al.)

AutoPulse improved the rate of delivery of patients in ROSC sustained to the ED by 53%
Human Short-term Survival Study (Swanson et al.)
Swanson M et al. Circulation. 2005;112(17):II-106.
*p=0.02
19%
29%
0%
10%
20%
30%R
OS
C t
o E
D R
ate
Manual CPR AutoPulse

• Conducted by Ornato et al. in Richmond, VA• Compared survival rates in 783 patients
– 499 patients treated with manual CPR– 284 patients treated with the AutoPulse
• 235% improvement in survival to discharge• 88% improvement in survival to hospital admission• 71% improvement in field ROSC
(Ong, Ornatoet al.)
Human Long-term Survival Study

AutoPulse improved survival to hospital discharge by 235%
(Ong, Ornatoet al.)
Ong ME, Ornato J et al. JAMA. 2006;295(22):2629-2637.
2.9%
9.7%
0%
5%
10%%
Su
rviv
al
Manual CPR AutoPulse
*p=0.0001
Human Long-term Survival Study

• Clinical evidence support AutoPulse benefits– Animal study (Halperin et al.) shows blood
pressure equivalent to pre-arrest levels– Animal study (Ikeno et al.) shows blood pressure
equivalent to normal and neurologically intact survival
– Human study (Timerman et al.) shows improved blood pressure
– 2 human studies (Swanson et al. and Casner et al.) show improved short-term survival
– Human study (Ong, Ornato et al.) shows improved short and long-term survival
Research Synopsis
Disclosure Policy
It is the policy of Saint Louis University School of Medicine to insure balance,independence, objectivity and scientific rigor in its continuing medical education program. Faculty and planning committee participating in the planning and presentation of these activities are required to disclose to the audiences prior to the activity the following:
– Existence of any significant financial or other relationship with the manufacturer of any commercial product or provider of any commercial service discussed.
– Their intention to discuss a product that is not labeled for the use under discussion.
– Their intention to discuss preliminary research data.
Saint Louis University has reviewed this activity’s disclosures and resolved all identified conflicts of interest, if applicable.

Validation of Content Statement
Saint Louis University School of Medicine follows the policy of the Accreditation Council for Continuing Medical Education (ACCME) regarding validation of clinical content for CME activities, which requires accredited sponsors to insure that: – All recommendations involving clinical medicine are based on
evidence that is accepted within the profession of medicine as adequate justification for their indications and contraindications in the care of patients.
– All scientific research referred to, reported or used in CME in support or justification of a patient care recommendation conforms to the generally accepted standards of experimental design, data collection and analysis.