covid consortium meeting #16 · progression. lancet study summary ... that cover the front and...
TRANSCRIPT
June 23rd, 2020
COVID Consortium Meeting #16
2
COVID Consortium Agenda: 6/23/20Agenda Item Presenter
Announcements / Updates
• CME: https://www.surveymonkey.com/r/COVIDCONSORTIUM
• Slides & Recording
• Meeting Cadence (Next Meeting: July 14)
Guy Dugan
COVID-19 Graph Guy Dugan
Reflection / First talk: Extreme Ownership. Jocko Willink
• https://www.youtube.com/watch?v=ljqra3BcqWM
Jocko Willink Ted
talk excerpt
What the Diamond Princess Cruise Outbreaks Reveal About COVID-1
• https://www.thelancet.com/journals/laninf/article/PIIS1473-3099(20)30364-9/fulltext
• https://www.nejm.org/doi/full/10.1056/NEJMc2013020
Janis Atkinson
PPE, AIIR, and COVID
• https://www.pnas.org/content/early/2020/06/10/2009637117
• https://royalsocietypublishing.org/doi/pdf/10.1098/rspa.2020.0376
Guy Dugan
Playbook updateNikki Hansra-
Godfrey
Publication reviews
• Tocilizumab as a Therapeutic Agent for Critically Ill Patients with SARS-CoV-2Dana Vais
Critical care drug taskforce update Sylvia Chen

3
Meeting Materials & Recording
• Slides and the link to the meeting recording will be
distributed following the meeting.
• This information will also be posted on the AMITA Health
COVID-19 site (top of page under same section as
physician townhall recordings).
CME Information
• For CME credit, please complete the form available at the
following link:
https://www.surveymonkey.com/r/COVIDCONSORTIUM
Reminders

4
Meeting Cadence and Upcoming
Physician Townhalls
In July, the COVID-19 Physician Townhall will begin alternating weeks with the
COVID Consortium. We invite you all to attend the Physician Townhalls during
off-weeks for updates on the system’s COVID-19 response.
Monday Tuesday Wednesday Thursday Friday
June22 23
COVID Consortium
24 25 26
Physician Townhall
July29 30 1 2 3
6 7 8 9 10
Physician Townhall
13 14
COVID Consortium
15 16 17
20 21 22 23 24
Physician Townhall
27 28
COVID Consortium
29 30 31
No meetings the week of July 4th

5
COVID-19 Graph

6
Reflection: Extreme Ownership. Jocko Willink

6 .23 .20
COVID Consortium Update

What the Diamond Princess Cruise outbreaks reveal about COVID-19

Overview
3711 passengers and crew; 712 COVID-19 RT-PCR Tested positive (spread easily to 19% of population) by end of quarantine (Feb 11 – Feb 25)
58% asymptomatic at the time of testing and most remained so!
All referred to various medical institutions designed for infectious disease by Japanese laws
Two studies have been published from this cohort:
Lancet June 12, 2020 Tabata et al.
NEJM June 12, 2020 Sakurai et al.

Unique situation
These are the first studies that included cohorts of asymptomatic individuals followed over time
Allows identification of risk factors for disease progression

Lancet Study Summary
104 participants, median age 64 years (25-93 years), 52% male, half with co-morbidities
All had blood tests and Chest CTs within 1-2 days of admission
Divided into three groups by presenting symptoms:
Asymptomatic
Severe: pneumonia (dyspnea, tachypnea, O2 sat <93%)
Mild: other symptoms
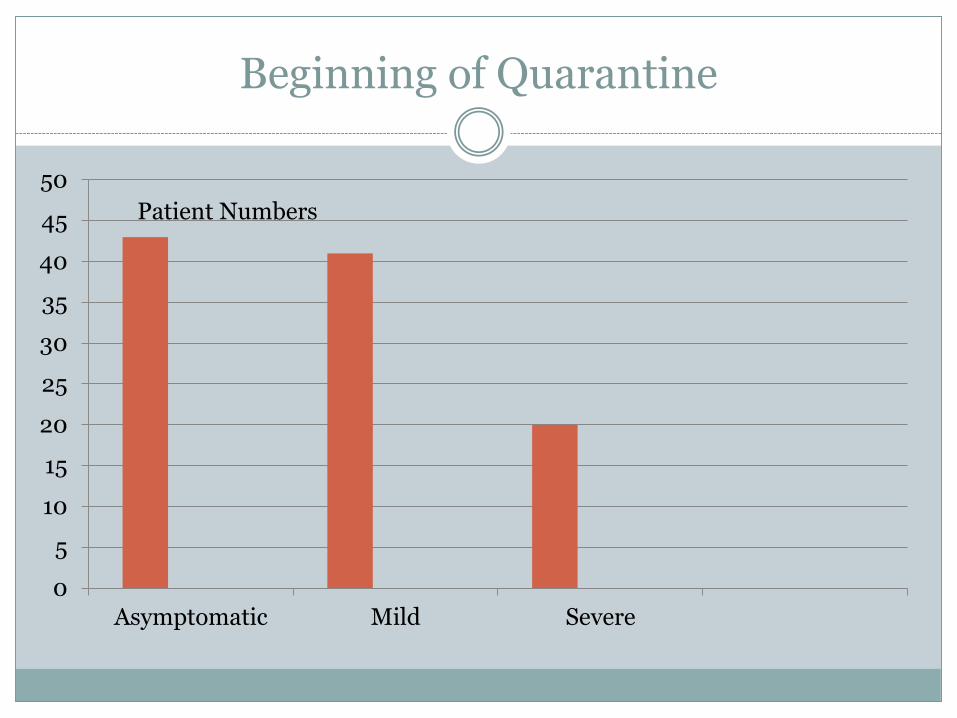
Beginning of Quarantine
0
5
10
15
20
25
30
35
40
45
50
Asymptomatic Mild Severe
Patient Numbers

End of Two week quarantine
0
5
10
15
20
25
30
35
40
45
50
Asymptomatic Mild Severe
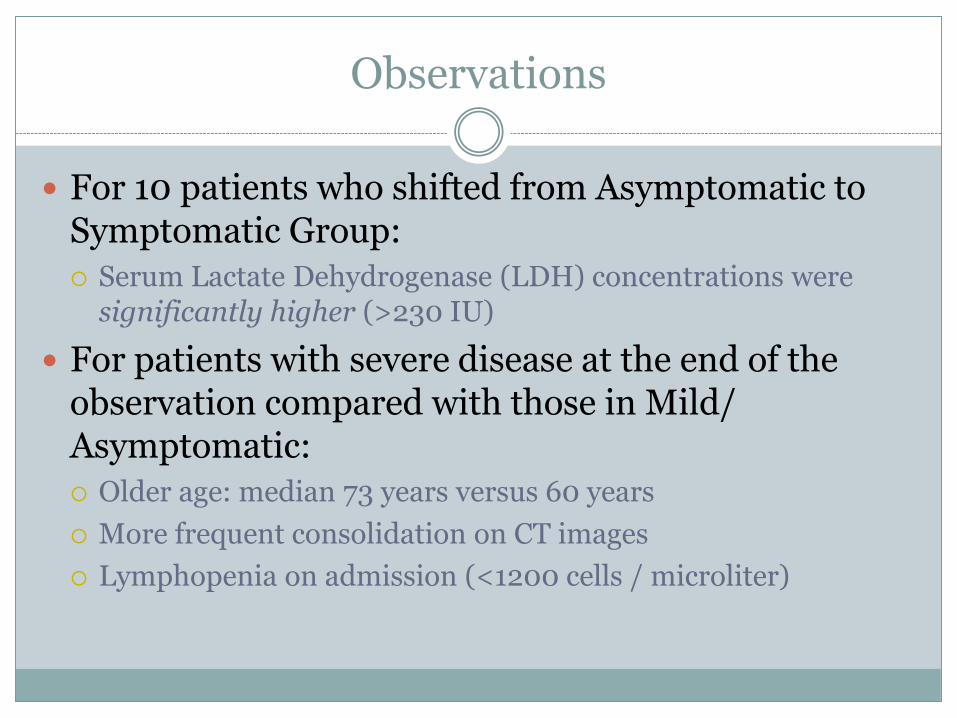
Observations
For 10 patients who shifted from Asymptomatic to Symptomatic Group:
Serum Lactate Dehydrogenase (LDH) concentrations were significantly higher (>230 IU)
For patients with severe disease at the end of the observation compared with those in Mild/Asymptomatic:
Older age: median 73 years versus 60 years
More frequent consolidation on CT images
Lymphopenia on admission (<1200 cells / microliter)

NEJM Study SummaryDiamond Princess
96 COVID+ individuals all asymptomatic (median age 59 years, range 9-77), 27 %with comorbities
11/96 eventually became symptomatic within 3-7 days
These patients interpreted as “pre-symptomatic”
The risk of being pre-symptomatic increased with increasing age
The time to resolution of infection increased with increasing age

Combined Data “Never Symptomatic”
Lancet Study (104 COVID-19 +patients) and NEJM study (96 COVID19+ patients) combined:
Only 15% of asymptomatic patients converted to symptomatic over the 2 week period in the two groups
85% of infected COVID-19+ asymptomatic individuals never developed symptoms during quarantine in these two cohorts


PPE AND SARS-COV-2GUY DUGAN

OUTLINE OF TALK
• Modes of viral transmission
• PPE based upon those modes
• Respiratory guidelines based upon transmission and PPE
• Role of control strategies in attenuating spread: E*p
• Predominate role of airborne spread and need for masks
• Scope of the challenge at AMITA
• Infections and deaths
• Inculcating good practice to ensure patient and staff protection

MODES OF VIRAL TRANSMISSION
Transmission Particle characteristics Transmission
Contact-Direct , Indirect Persons/Objects Self inoculation, fomites
Droplet >5 micons, < 17 min in air, < 1 m dispersion Cough, sneezing, talking deposition on mucous membranes and upper resp tract
Aerosol- Airborne < 5 microns, remains in air, > 1 m Long range transmission, inhalation of aerosols in with deposition along the resptract, including the lower airways

DROPLETS AND AEROSOLS: IT’S COMPLICATED
• Large droplets evaporate and become smaller
• Most activities create a very large variety of sizes: spectrum, not dichotomy
• Can’t distinguish between short distance aerosol transmission (I caught it while breathing a few feet away from you) and contact transmission (I touched the door handle and then rubbed my eye.)
• Assumes contact, droplet and biases the literature
DETERMINANTS OF SPREAD
• Temperature, humidity, microbial resistance to external physical and biological stresses, and solar ultraviolet (UV) radiation
• Size and number concentration of inhaled aerosols
• Stages of infection and varies between symptomatic and asymptomatic carriers
• Peak of infectiousness on or before the symptom onset
• Substantial asymptomatic transmission for SARS-CoV-2.

AEROSOL GENERATING PROCEDURES- AGP
• There is neither expert consensus, nor sufficient supporting data,
to create a definitive and comprehensive list of AGPs for
healthcare settings.
• due to limitations in available data on which procedures may
generate potentially infectious aerosols and
• the challenges in determining if reported transmissions during
AGPs are due to aerosols or other exposures.

COMMONLY REPORTED AGP- AIIR RECOMMENDED
• Sputum induction
• Cardiopulmonary resuscitation
• Endotracheal intubation and extubation
• Non-invasive ventilation (e.g., BiPAP, CPAP)- not clear
• Bronchoscopy
• Manual ventilation
• Uncertain whether aerosols generated from some procedures may be infectious, such as:
• nebulizer administration- aerosols or close contact
• high flow O2 delivery- better controlled with a mask
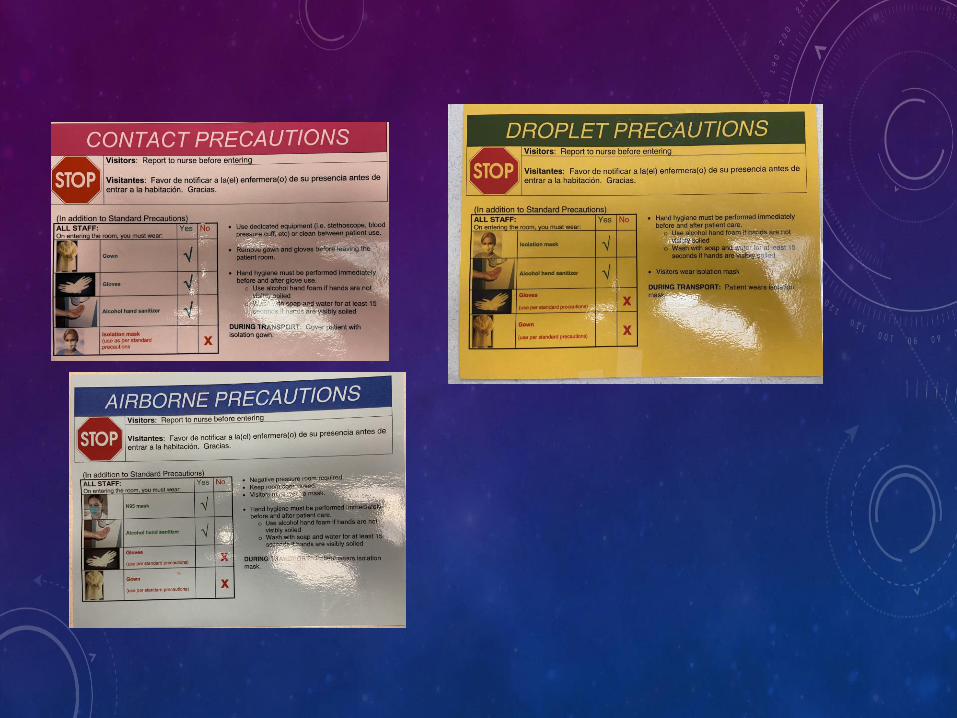

CDC PPE- PUI OR COVID 19
• Gloves
• Gown
• N95 or greater, or facemask if respirators are not available
• Eye protection- goggles or disposable face shield that cover the front and sides of the face.

HIGH-FLOW NASAL CANNULA FOR COVID-19 PATIENTS: LOW RISK FOR BIO-AEROSOL DISPERSIONEUROPEAN RESPIRATORY JOURNAL
LI J, FINK JB, EHRMANN S. HIGH-FLOW NASAL CANNULA FOR COVID-19 PATIENTS: LOW RISK OF BIO-AEROSOL DISPERSION. EUR RESPIR J 2020; 55: 2000892 [HTTPS://DOI.ORG/10.1183/13993003.00892-2020
40 L/min ~ 5.5 inches60 L/min~ 7.0 inches
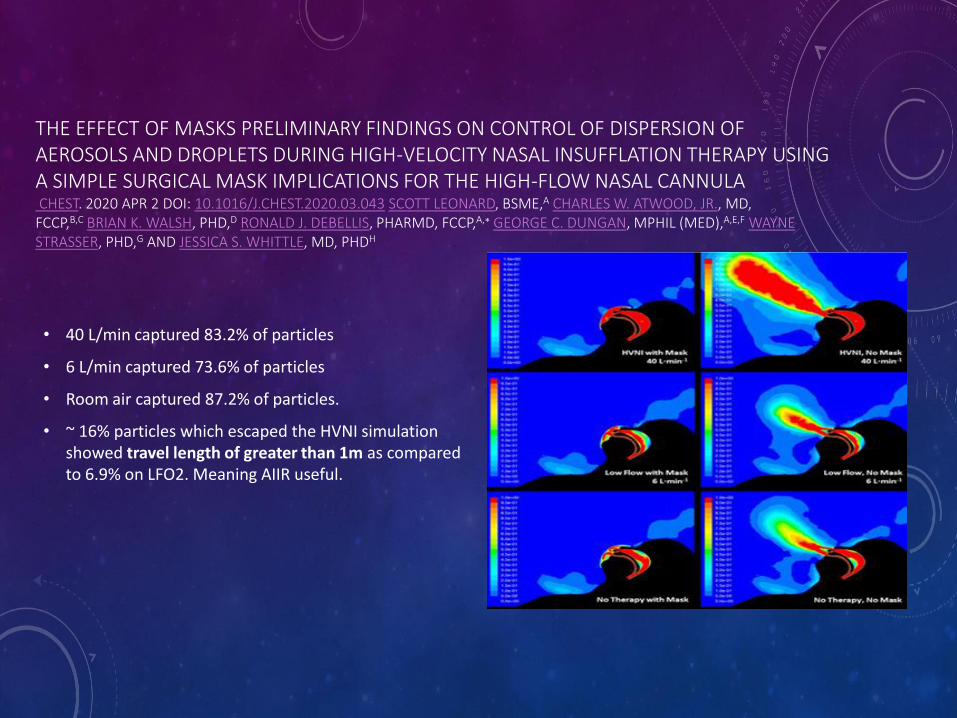
THE EFFECT OF MASKS PRELIMINARY FINDINGS ON CONTROL OF DISPERSION OF AEROSOLS AND DROPLETS DURING HIGH-VELOCITY NASAL INSUFFLATION THERAPY USING A SIMPLE SURGICAL MASK IMPLICATIONS FOR THE HIGH-FLOW NASAL CANNULACHEST. 2020 APR 2 DOI: 10.1016/J.CHEST.2020.03.043 SCOTT LEONARD, BSME,A CHARLES W. ATWOOD, JR., MD,
FCCP,B,C BRIAN K. WALSH, PHD,D RONALD J. DEBELLIS, PHARMD, FCCP,A,∗ GEORGE C. DUNGAN, MPHIL (MED),A,E,F WAYNE STRASSER, PHD,G AND JESSICA S. WHITTLE, MD, PHDH
• 40 L/min captured 83.2% of particles
• 6 L/min captured 73.6% of particles
• Room air captured 87.2% of particles.
• ~ 16% particles which escaped the HVNI simulation showed travel length of greater than 1m as compared to 6.9% on LFO2. Meaning AIIR useful.

NEJM VIDEO
• https://www.nejm.org/doi/10.1056/NEJMc2007800
AMITA RESPIRATORY GUIDELINES KELLI DEBERRY , ASHLEY BLACK, RAJ DESAI, DIANA DOEING, GUY DUGAN, PATTY GESSNER, NIKKI HANSRA,
OMAR HUSSEIN, MIKE KELLER, NAZISH KHAN, TOM MURPHY, IMRAN SHAIKH, NAWAID SHAKIR, SUNIL VARMA
• Airborne isolation for flow > 40 lpm
• Transfer to AIIR if available with preference given to those with difficulty wearing a mask
• Avoid venti masks due to increased aerosolization
• The data regarding NIPPV varies, but our recommendation is to use a viral filter and place these patients in an AIIR

How do we think about PPE and healthcare worker safety?
Hint: Mathematically

FLATTENING THE CURVE- THE VARIABLES OF CONTROL
E: exposure. Average number of people an infected person encounters
-Social distancing
p: probability of exposed becoming infected
-Mask, hand washing
The product of E and p is the Growth Rate
𝑁𝑑= (1 + 𝐸 ∗ 𝑝)𝑑∗ 𝑁0
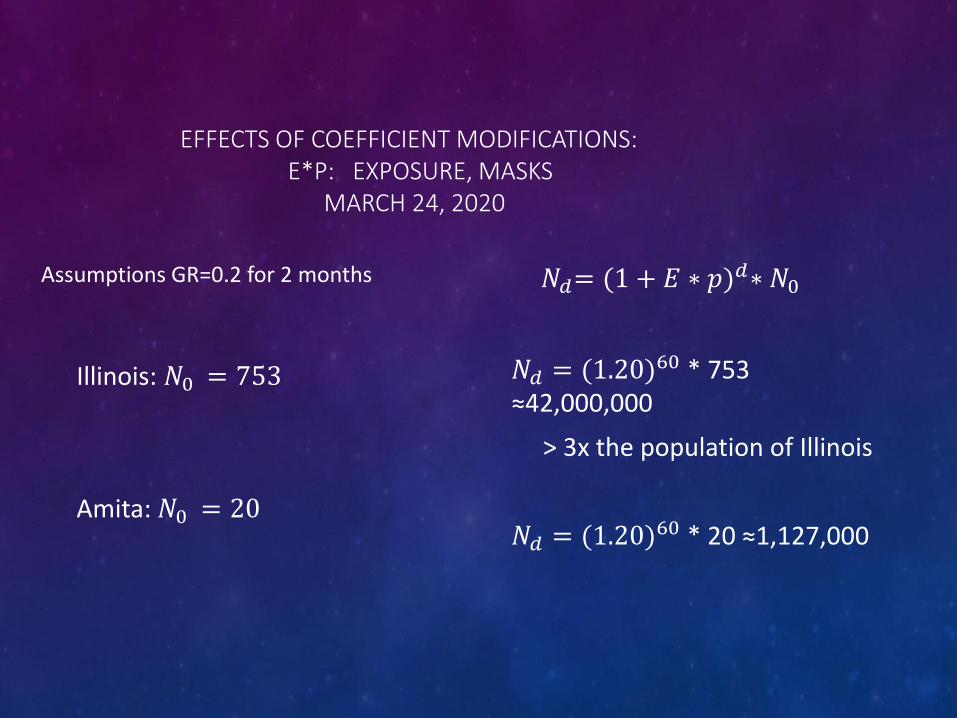
EFFECTS OF COEFFICIENT MODIFICATIONS:E*P: EXPOSURE, MASKS
MARCH 24, 2020
Assumptions GR=0.2 for 2 months
Illinois: 𝑁0 = 753
Amita: 𝑁0 = 20
𝑁𝑑= (1 + 𝐸 ∗ 𝑝)𝑑∗ 𝑁0
𝑁𝑑 = (1.20)60 * 753 ≈42,000,000
> 3x the population of Illinois
𝑁𝑑 = (1.20)60 * 20 ≈1,127,000
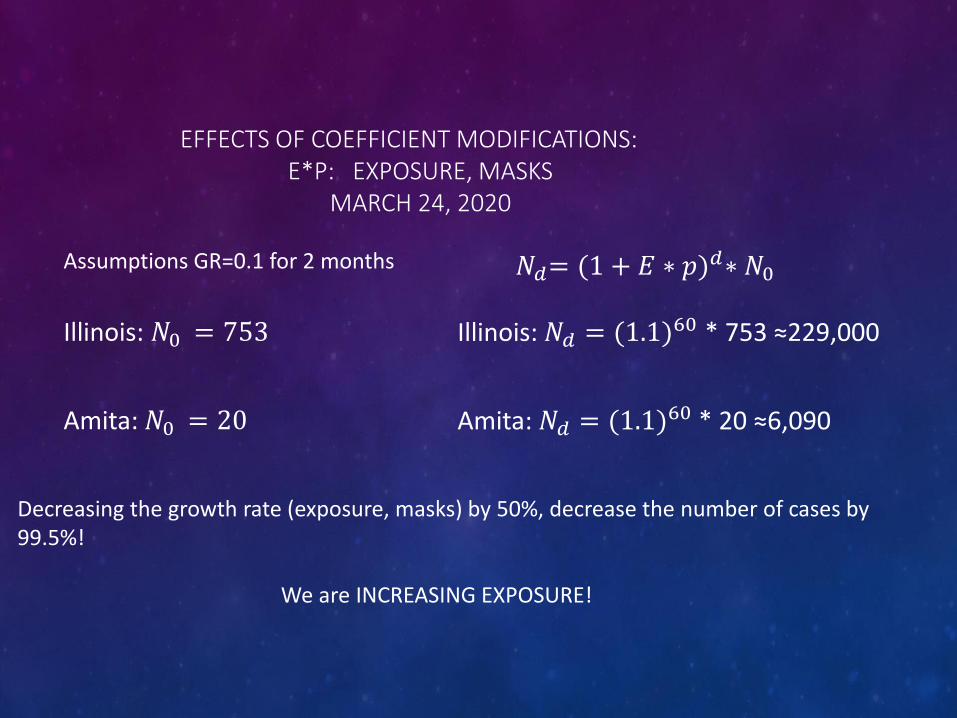
EFFECTS OF COEFFICIENT MODIFICATIONS: E*P: EXPOSURE, MASKS
MARCH 24, 2020
Assumptions GR=0.1 for 2 months
Illinois: 𝑁0 = 753
Amita: 𝑁0 = 20
𝑁𝑑= (1 + 𝐸 ∗ 𝑝)𝑑∗ 𝑁0
Illinois: 𝑁𝑑 = (1.1)60 * 753 ≈229,000
Amita: 𝑁𝑑 = (1.1)60 * 20 ≈6,090
Decreasing the growth rate (exposure, masks) by 50%, decrease the number of cases by 99.5%!
We are INCREASING EXPOSURE!
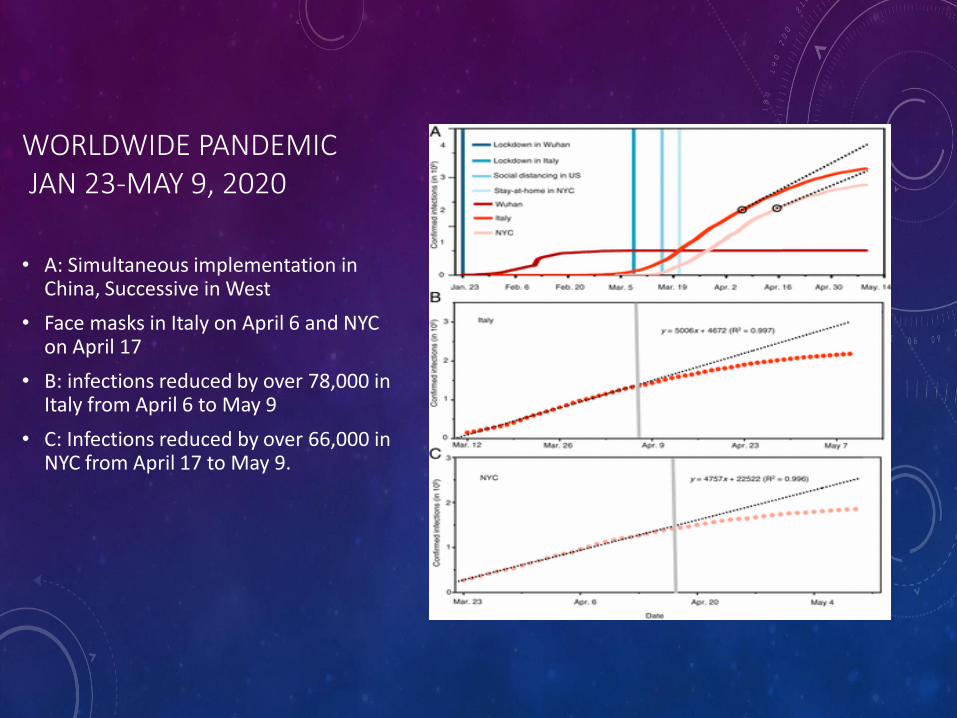
WORLDWIDE PANDEMICJAN 23-MAY 9, 2020
• A: Simultaneous implementation in China, Successive in West
• Face masks in Italy on April 6 and NYC on April 17
• B: infections reduced by over 78,000 in Italy from April 6 to May 9
• C: Infections reduced by over 66,000 in NYC from April 17 to May 9.

FACE COVERING IN ADDITION TO OTHER MEASURES
• Comparison of daily new cases between NYC and the United States (minus NYC) from 3/ 1 to 5/ 9 .
• Sharp increase in late March and early April.
• Slower increase in the number after the stay-at-home order (about 14 d in New York and shortly after April 3 in the United States)
• After April 3, the only difference is the face covering on April 17 in NYC which results in decreased infections
PROCEEDINGS OF THE NATIONAL ACADEMY OF SCIENCES PAPER CONCLUSIONS
• Airborne transmission is highly virulent and represents the dominant route of disease transmission which was not recognized by WHO and CDC
• The unrecognized importance of airborne virus transmission resulted in the propagation of the pandemic
• Face covering is critical to significantly reduce infections

FACE MASKS ARE IMPORTANTSUMMARY OF DATA
• Models of airflow
• Mathematics of attenuating exponentiated coefficient
• Analysis of the natural experiment in the global pandemic
AMITA PATIENT MASK COMPLIANCENON-SCIENTIFIC SURVEY
• Percentage of pts who are PUI/COVID+ who wear masks when HCP in room?
• 30% ~ 90% of the time
• Percentage of pts who are Not PUI/COVID- who wear masks when HCP in room?
• 20% ~90% of the time
• Significant infection risk exists

AMITA CHALLENGES
• 697 infected
• 5 deaths in AMITA staff:
• 1 environmental services while cleaning
• 1 nurse screener- with chronic illness
• 2 community from international travel
• 1 unclear-probably community

COVID + WORKERS AND DATE TAKEN OFF FROM WORK. THE THREE HIGHEST SPIKES INVOLVED EXPOSURES AT GLEN OAKS BEHAVIORAL HEALTH UNIT AND HFMC EXPOSURE. EXPOSURE AT SAMC AND THE FINAL HIGHEST PEAK IS ALEXIAN BROTHERS BEHAVIORAL HEALTH HOSPITAL.

SOCIAL VS. WORK RELATED EXPOSURE
33%
67%
COVID + WORKERS - SOCIAL VS. WORK RELATEDNESS
Social Work
0
50
100
150
200
250
300
350
400
Feb Mar Apr May Jun
Social vs Work Exposure by Month
Social Work

COVID + BY JOB TITLE
0 50 100 150 200 250
Analyst-Data-Quality
Asst-Office Operations
Dir-Medical Student Program
LPN
RCP
Technologist-Sonography
Transport
Lead Technologist-Echocardio
Resident
Therapist-Occupational
Nursing Leader
Therapist-Respiratory-Cert
RN-Behavior Health
Physician/APP/Resident
Tech-CPCT, Patient Care-Cert
RN
COVID + by Job Title

COVID + BY MINISTRY
0
10
20
30
40
50
60
70
COVID + Workers by Ministry

BARRIERS TO PATIENT MASKING
• New workflow patterns are difficult to engrain and need to be assisted by new educational paradigms
• Instruct all patients that that they need to help be responsible to help protect HCP by participating in putting on their own mask when someone enters the room
• Fliers in multiple languages

MASKING EDUCATION-BEGINS AT SITES OF ENTRY
• ED- 30% admissions
• Pre-surgical clinic
• Outpatient diagnostic areas
• AMITA Medical Group
• Tele-tracking
• Home health
• Nursing homes
AMITA PPE UPDATES FROM CDC, TJC
• Eye protection
• Bring two more bags

BATTLE PLANS
• Education of staff- Env Services, dietary, transport, nursing, physicians
• Develop strategies to enhance patient masking
• Establish education and protocols for appropriate cleaning with new supplies
• Continue to develop PPE conservation strategies
• Procure supplies for the next wave
• Ensure PPE is continued to be used appropriately for MRSA, ESBL
• Update isolation signs and playbook
• Continue to refine contact tracing strategies

CONCLUSIONS
• If you don’t like the mask, you’re gonna hate the ventilator.

When a team takes ownership of its problems, the problems get solved.
Jocko Willink
REFERENCES
• https://royalsocietypublishing.org/doi/10.1098/rspa.2020.0376?utm_campaign=wp_to_your_health&utm_medium=email&utm_source=newsletter&wpisrc=nl_tyh&wpmk=1&pwapi_token=eyJ0eXAiOiJKV1QiLCJhbGciOiJIUzI1NiJ9.eyJjb29raWVuYW1lIjoid3BfY3J0aWQiLCJpc3MiOiJDYXJ0YSIsImNvb2tpZXZhbHVlIjoiNTk2Yjk3NjZhZTdlOGE0NGU3ZGE0MDBmIiwidGFnIjoiNWVlMTQ0YjdmZTFmZjY1NGMyZjZmZDYzIiwidXJsIjoiaHR0cHM6Ly9yb3lhbHNvY2lldHlwdWJsaXNoaW5nLm9yZy9kb2kvMTAuMTA5OC9yc3BhLjIwMjAuMDM3Nj91dG1fY2FtcGFpZ249d3BfdG9feW91cl9oZWFsdGgmdXRtX21lZGl1bT1lbWFpbCZ1dG1fc291cmNlPW5ld3NsZXR0ZXImd3Bpc3JjPW5sX3R5aCZ3cG1rPTEifQ.1pa9a_i4v8OfKT1CDlutEXmT98f3yvPNx7_054cxlGw
• Who needs ppe https://www.cdc.gov/coronavirus/2019-ncov/hcp/using-ppe.html
• PPE guidelines https://www.cdc.gov/coronavirus/2019-ncov/hcp/infection-control.html

REFERENCES
• Healthcare ppe: https://www.cdc.gov/coronavirus/2019-ncov/hcp/infection-control-faq.html#asymptomatic
• Tran K, Cimon K, Severn M, Pessoa-Silva CL, Conly J (2012) Aerosol Generating Procedures and Risk of Transmission of Acute Respiratory Infections to Healthcare Workers: A Systematic Review. PLoS ONE 7(4); https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3338532/#!po=72.2222external iconexternal icon).
• https://web.archive.org/web/20200410151006/https://www.cdc.gov/coronavirus/2019-ncov/hcp/infection-control-recommendations.html?CDC_AA_refVal=https%3A%2F%2Fwww.cdc.gov%2Fcoronavirus%2F2019-ncov%2Finfection-control%2Fcontrol-recommendations.html summary on infection control
• https://aip.scitation.org/doi/10.1063/5.0015044#
• https://aip.scitation.org/doi/pdf/10.1063/5.0015044?download=true
• https://www.cdc.gov/infectioncontrol/pdf/guidelines/isolation-guidelines-H.pdf
• https://www.nejm.org/doi/full/10.1056/NEJMc2004973

REFERENCES
• https://apps.who.int/iris/bitstream/handle/10665/331498/WHO-2019-nCoV-IPCPPE_use-2020.2-eng.pdf how is covid spread
• https://www.nejm.org/doi/10.1056/NEJMc2007800 NEJM video
• https://first10em.com/aerosols-droplets-and-airborne-spread/
55
Playbook UpdateDana Vais
https://www.amitahealth.org/assets/documents/covid-19-
playbook/pulmonary-and-critical-care/amita-pulmonary-function-
testing-restart-recommendations-6.18.20_v18.pdf
Tocilizumab as a Therapeutic Agent for
Critically Ill Patients Infected with
SARSCoV-2
Russell M. Petrak MD, Nathan C. Skorodin PharmD, Nicholas W. Van Hise PharmD, BCPS,
Robert M. Fliegelman DO, Jonathan Pinsky MD, Vishal Didwania MD, Michael Anderson MD, Melina Diaz
MD, Kairav Shah MD, Vishnu V. Chundi MD, David W. Hines MD,
Brian P. Harting MD, Kamo Sidwha MD, Brian Yu MD, Paul Brune MD, Anjum Owaisi
MD, David Beezhold DO, Joseph Kent MD, Dana Vais MD, Alice Han MD, Neethi
Gowda MD, Nishi Sahgal MD, Jan Silverman DO, Jonathan Stake MD, Jenie
Nepomuceno MD, Renuka Heddurshetti MD

HIGHLIGHTS
● Tocilizumab administered early in the course of hospitalization for COVID 19
was associated with decreased mortality
● Fewer patients in the early dosing group required mechanical ventilation
● Mortality in intubated patients was 42.7%

RATIONALE
● COVID 19 spectrum includes:○ asymptomatic/minimally symptomatic ILI
○ mild/moderate disease: fever/cough/SOB/bilateral infiltrates +/- hypoxemia
○ severe/critical disease: rapidly worsening oxygenation/ARDS/MOSF; dysregulated
inflammatory reaction (high IL6 signature) driving the pathology
● Arresting this “cytokine storm” is thought to be key in reducing morbidity and
mortality
● Tocilizumab: IL6R antagonist approved in 2010; indicated for treatment of:○ rheumatoid arthritis
○ cytokine release syndrome (CRS) associated with CAR T therapy (provides rationale for the
treatment of severe COVID-19 disease)

STUDY SUMMARY
● Multi-center observational retrospective & concurrent study
● 145 hospitalized (24 hospitals, 4 states) patients with COVID 19 between
3/13/20-4/16/20, treated with tocilizumab
● Tocilizumab was prescribed at the discretion of the ID physician with
consideration of local hospital treatment protocols
● Inclusion criteria: all patients with confirmed COVID 19 (+SARS-CoV2 PCR)
treated with tocilizumab (157)
● Exclusion criteria: data not available for review (12)
● Data points collected: age, sex, race, date of admission, length of hospital stay
(LOS), mechanical ventilation, steroids, vasopressors, HQ+AZ, remdesivir
therapy; comorbidities; inflammatory markers (LDH, ferritin, CRP, D dimer)
● Disposition: discharged from the hospital, expired, or continued hospitalization

STUDY SUMMARY
● Tocilizumab timing of administration in relation to mechanical ventilation
(MV):○ Early group: before or no more than one day after MV
○ Late group: more than one day of mechanical ventilation
● Statistics: ○ descriptive for baseline patient characteristics, clinical variables, and outcomes
○ potential confounders: adjusted for by propensity scores (calculated from a regression model
with the dose timing (early vs late)as the outcome and baseline demographic and clinical
variables of each participant as predictor variables)
○ "inverse probability of treatment weights", or IPTW: to adjust for confounding variables
● multivariable regression models fit for each outcome, adjusting for baseline
patient demographic variables.
● Statistical significance for all methods was defined as a p-value ≤ 0.05



TREATMENT & OUTCOMES
● 123 (84.8%) patients received single dose; 135 received a dose of 400 mg
● 70 patients discharged, 41 expired, 34 remained in house
● Outcome MV: OR 1.21 per day for each day from admission to tocilizumab
● Outcome mortality: late dosing 17.8x more likely to expire than early dosing
(holding all other covariates constant 95% CI: [5.32, 74.55], p < 0.001)
● Patients on mechanical ventilation who received tocilizumab within several
days of admission or the day of intubation were more likely to be discharged
(p = <0.001)
● Mechanical ventilation was required in 56% of patients, with a mortality rate of
42.7%
● Non-intubated patients received the dose approximately one day earlier
than the age, sex, comorbidity matched, and ventilated counterparts


MECHANICALLY VENTILATED
MV discharged=30; expired=35
Timing of tocilizumab dose post MV: 1.1 days vs 4.1 days (p<0.001)
Race: African American 20% vs 45.7% (p 0.052)

Somers et al – Univ of Michigan; June 3

Tocilizumab Administered – Timeframe from Admission to Dose AdministrationN=245
AMITA hospitals tocilizumab use - May 2020

Tocilizumab Administered - Extubation Results – By Timeframe

Tocilizumab Administered –Survival to Discharge—Intubated vs Never Intubated(Only includes data for patients no longer admitted)

STUDY LIMITATIONS
● study was observational with no control group
● did not evaluate the relationship between IL-6 levels and tocilizumab efficacy
● did not formally evaluate any serious adverse drug reactions, like secondary
infections
● multiple therapeutic modalities implemented concurrently

STUDY STRENGTHS
● Largest cohort from a private practice setting
● Multi-center and multi-state
● Real life utilization of tocilizumab
● Using mechanical ventilation as a landmark in the disease severity and
progression
Critical Drug Task Force (CDTF):
Update on COVID-19 Treatment
Sylvia Chen, PharmD, BCPS – System Director, Clinical Pharmacy
June 23, 2020

73
Critical Drug Task ForceCOVID-19 Treatment Guideline Updates
• Hydroxychloroquine/
Chloroquine
• Remdesivir
• Tocilizumab
• Most recent AMITA
COVID-19 Treatment
Guidelines available
online at:
• https://www.amitahealth.org/covid-
19-amita/
74
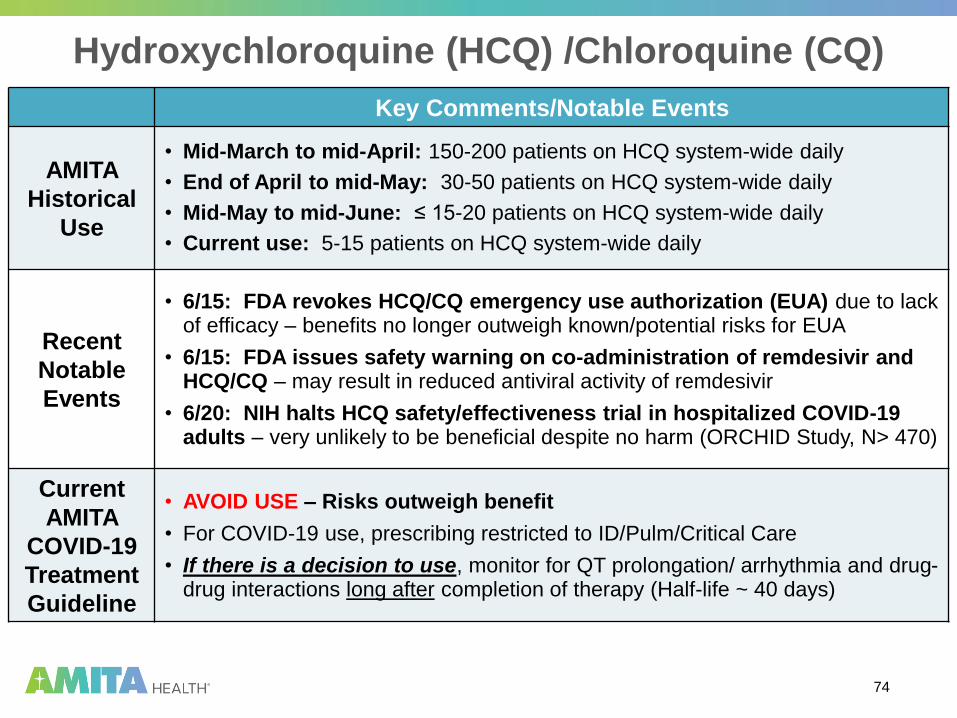
Hydroxychloroquine (HCQ) /Chloroquine (CQ)
Key Comments/Notable Events
AMITA
Historical
Use
• Mid-March to mid-April: 150-200 patients on HCQ system-wide daily
• End of April to mid-May: 30-50 patients on HCQ system-wide daily
• Mid-May to mid-June: ≤ 15-20 patients on HCQ system-wide daily
• Current use: 5-15 patients on HCQ system-wide daily
Recent
Notable
Events
• 6/15: FDA revokes HCQ/CQ emergency use authorization (EUA) due to lack of efficacy – benefits no longer outweigh known/potential risks for EUA
• 6/15: FDA issues safety warning on co-administration of remdesivir and HCQ/CQ – may result in reduced antiviral activity of remdesivir
• 6/20: NIH halts HCQ safety/effectiveness trial in hospitalized COVID-19 adults – very unlikely to be beneficial despite no harm (ORCHID Study, N> 470)
Current
AMITA
COVID-19
Treatment
Guideline
• AVOID USE – Risks outweigh benefit
• For COVID-19 use, prescribing restricted to ID/Pulm/Critical Care
• If there is a decision to use, monitor for QT prolongation/ arrhythmia and drug-drug interactions long after completion of therapy (Half-life ~ 40 days)

75
Tocilizumab (Actemra)
Key Comments/Notable Events
Recent
Clinical
Evidence
Potential
Mortality
Benefit
• Retrospective/concurrent multi-center study in COVID-19 patients
• Review of 145 patients who received tocilizumab: 64 not mechanically-ventilated (MV), 37 given “early” (within 1 day of MV), 44 given “late” (more than 24 hours after MV)
• Among the MV patients, a statistically significant mortality difference was seen based on timing of tocilizumab administration:
• Mortality of 13.5% (5/37 patients) if tocilizumab given within 24 hrs of MV
vs. 68.2% (30/44 patients) if tocilizumab given after 24 hours of MV
(p<0.001)
• No control group
• No evaluation of relationship between IL-6 levels and tocilizumab efficacy
• Authors’ conclusion: Our data strongly supports a mortality benefit of dosing tocilizumab early and within 1 day of intubation
Petrak RM, et al., Tocilizumab as a therapeutic agent for critically ill patients infected with
SARS-CoV-2 medRxiv. doi: https://doi.org/10.1101/2020.06.05.20122622
• Weigh risk vs. benefit

76
Tocilizumab – AMITA Use Criteria
• Based on the emerging data, clinical experience, as well as
provider feedback, inclusion/exclusion criteria adjusted to:
– INCLUSION Criteria
• Positive SARS-CoV-2 (including rapid test)
• No documented or suspected active bacterial, fungal, viral, or other infections (besides COVID-19)
– EXCLUSION Criteria
• Evidence of pancreatitis
• AST / ALT > 5 x ULN
• Neutrophils < 500 cells/mm3
• Platelets < 50,000 cells/mm3
• Complicated diverticulitis or intestinal perforation
• Anti-rejection immunosuppressive therapy
• Hospice status

77
Tocilizumab (Actemra)
Key Comments/Notable Events
AMITA
Historical
Use
• Mid-March to early-April: 47 doses (avg 3 doses daily) dispensed daily
• Mid-April to mid-May: 276 doses (avg 9 doses daily) dispensed daily
• Last half of May: avg 5 doses dispensed daily
• Current use: 0-1 dose dispensed daily
AMITA
COVID-19
Treatment
Guideline
from CDTF
• AVOID USE – Risks outweigh benefit
• For COVID-19, prescribing restricted to ID/Pulm/Critical Care
• If prescribed, dual provider agreement between ID and Pulm/Critical Care
is required
• Documentation of inclusion/exclusion criteria assessment and risk/benefit
discussion with patient/caregiver required – no more request form

78
Remdesivir – Status of Inventory & Patients
• IDPH memo on 6/17 – 202 more cases received in Illinois
– AMITA to receive 34 more cases (1360 vials = 226 more treatments)
– Overall total for AMITA = 168 cases (6720 vials = 1120 treatments)
• AMITA Inventory Status:
Treatment Courses
Received
Treatment Courses
Dispensed
Treatment Courses
Remaining
1120244
(22 treatment courses
were not completed)
885
79
Remdesivir – AMITA Use Criteria
• With sufficient inventory, further relaxation of remdesivir use
criteria:
• INCLUSION Criteria
– Hospitalized patient
– Positive SARS-CoV-2
– At least ONE of the following
respiratory criteria:• Rapidly worsening gas exchange
requiring doubling of oxygen
requirements in 12 hours OR
• SpO2 ≤ 94% on room air or
requiring supplemental oxygen
OR
• Respiratory failure on mechanical
ventilation for less than 72 hours
• EXCLUSION Criteria– Poor prognosis (unlikely to survive >
48 hours)
– Mechanical ventilation ≥ 72 hrs
– Severe renal impairment In patients
>28 days old: eGFR < 30 ml/min or
HD; if 7-28 days old, SCr ≥1 mg/dL)
– Severe liver impairment (ALT ≥ 5 x
ULN)
– Multi-organ failure or Vasopressor
support for >24 hours
– Hospice status

80
Remdesivir Daily Utilization: May 13 to June 21
New COVID-19 Positive Inpatients = ~ 15 per day
Remdesivir = ~ 3 per day

81
THANK YOU