coxhealth crsou 11172017 handout - cox college applicable law or appropriate for a given member s...
TRANSCRIPT

Card
iovascula
r M
ark
et
Update
2017
Card
iova
scula
r R
oundta
ble
Pre
pare
d f
or:
Cox H
ealth
11/1
7/2
017
Stu
art
Cla
rkM
anag
ing D
irecto
rcla
rks@
advis
ory
.com
LEGAL CAVEAT
Advisory Board is a division of The Advisory Board Company. Advisory Board has made efforts to verify the accuracy of the information it provides to members. This report relies on data obtained from many sources, however, and Advisory Board cannot guarantee the accuracy of the information provided or any analysis based thereon. In addition, Advisory Board is not in the business of giving legal, medical, accounting, or other professional advice, and its reports should not be construed as professional advice. In particular, members should not rely on any legal commentary in this report as a basis for action, or assume that any tactics described herein would be permittedby applicable law or appropriate for a given member�s situation. Members are advised to consult with appropriate professionals concerning legal, medical, tax, or accounting issues, before implementing any of these tactics. Neither Advisory Board nor its officers, directors, trustees, employees, and agents shall be liable for any claims, liabilities, or expenses relating to (a) any errors or omissions in this report, whether caused by Advisory Board or any of its employees or agents, or sources or other third parties,(b) any recommendation or graded ranking by Advisory Board, or (c) failure of member and its employees and agents to abide by the terms set forth herein.
The Advisory Board Company and the �A� logo are registered trademarks of The Advisory Board Company in the United States and other countries. Members are not permitted to use these trademarks, or any other trademark, product name, service name, trade name, and logo of Advisory Board without prior written consent of Advisory Board. All other trademarks, product names, service names, trade names, and logos used within these pages are the property of their respective holders. Use of other company trademarks, product names, service names, trade names, and logos or images of the same does not necessarily constitute (a) an endorsement by such company of Advisory Board and its products and services, or (b) an endorsement of the company or its products or services by Advisory Board. Advisory Board is not affiliated with any such company.
©2017 Advisory Board � All Rights Reserved � advisory.com � 35421A
IMPORTANT: Please read the following.
Advisory Board has prepared this report for the exclusive use of its members. Each member acknowledges and agrees that this report and the information contained herein (collectively, the �Report�) are confidential and proprietaryto Advisory Board. By accepting delivery of this Report, each member agrees to abide by the terms as stated herein, including the following:
1. Advisory Board owns all right, title, and interest in and to this Report. Except as stated herein, no right, license, permission, or interest of any kind in this Report is intended to be given, transferred to, or acquired by a member. Each member is authorized to use this Report only to the extent expressly authorized herein.
2. Each member shall not sell, license, republish, or post online or otherwise this Report, in part or in whole. Each member shall not disseminate or permit the use of, and shall take reasonable precautions to prevent such dissemination or use of, this Report by (a) any of its employees and agents (except as stated below), or(b) any third party.
3. Each member may make this Report available solely to those of its employees and agents who (a) are registered for the workshop or membership program ofwhich this Report is a part, (b) require access to this Report in order to learn from the information described herein, and(c) agree not to disclose this Report to other employees or agents or any third party. Each member shall use, and shall ensure that its employees and agents use, this Report for its internal use only. Each member may make a limited number of copies, solely as adequate for use by its employees and agents in accordance with the terms herein.
4. Each member shall not remove from this Report any confidential markings, copyright notices, and/or other similar indicia herein.
5. Each member is responsible for any breach of its obligations as stated herein by any of its employees or agents.
6. If a member is unwilling to abide by anyof the foregoing obligations, then such member shall promptly return this Report and all copies thereof to Advisory Board.
Cardiovascular Market Update 2017
Cardiovascular Roundtable
Prepared for: Cox Health11/17/2017
Stuart ClarkManaging [email protected]
©2017 Advisory Board � All Rights Reserved � advisory.com � 35421A
ROAD MAP6
The Next Wave of Health Reform 1
2 5 Market Realities Impacting CV Programs
3 Defining a No-Regrets Strategy
©2017 Advisory Board � All Rights Reserved � advisory.com � 35421A
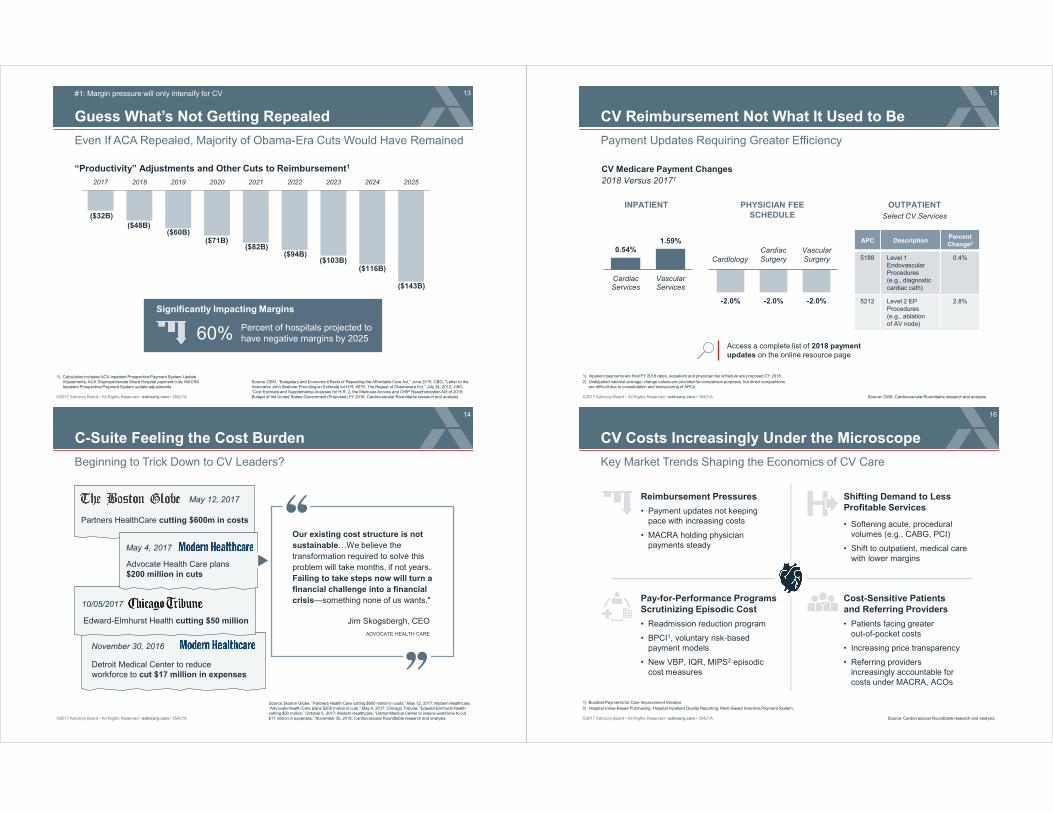
7
What a Year It�s Been
2017 a Roller Coaster Year in Health Care Policy
Source: Cardiovascular Roundtable research and analysis.
1) American Health Care Act of 2017; Better Care Reconciliation Act; Obamacare Repeal and Reconciliation Act.
2) Episode Payment Models.
3) Department of Health and Human Services.
January 20
President Trump sworn in, makes health care top priority on Day 1
� July 25-28: Senate votes down AHCA, BCRA, ORRA1
� September 26: Senate cancels vote on Cassidy-Graham
Key Milestones in 2017 Health Care Agenda
New President of the United States
Attempts to Repeal, Replace the ACA Begin
Cardiac Bundles Cancelled
August 15
CMS issues proposal to cancel mandatory CABG, AMI EPMs2
New HHS3
Secretary
October 4
Eric Hargan announced as acting HHS Secretary following resignation of Tom Price
©2017 Advisory Board � All Rights Reserved � advisory.com � 35421A
8
Health Care Squarely in the Hands of the GOP
Congress, Executive Branch, and Most States Now in Republican Control
Source: Cardiovascular Roundtable research and analysis.
33/50Republican Governors
32/50Republican-Led Legislatures
52/100Senate Republicans
241/435House Republicans
Four Key Principles Guiding GOP Reform Efforts
Promote Transparency of Cost and Quality
Reduce Federal Entitlement Spending
Embrace Free Markets and Consumer Choice
Use free-markets to promote private sector competition in payer, provider markets
Focus more aggressively on reducing federal health care spending
Mandate greater consumer choice at the point-of-care, coverage through improved transparency
Reduce federal role in health care; provide states more autonomy to make decisions, cut spending
Devolve Health Policy Control to States

©2017 Advisory Board � All Rights Reserved � advisory.com � 35421A
9
What�s Next for Health Care Reform?
Future of Repeal Legislation Unclear
Source: Nather, D. and Baker, S. �Axios Vitals,� Axios, Aug. 1, 2017; Davis, S. and Montanaro, D. �McCain Votes No, Dealing Potential Death Blow to Republican Health Care Efforts,� NPR, July 27, 2017; Health Care Advisory Board interviews and analysis.
Legislative Agenda Shifting�For Now
�We haven't given up on changing the American health care system. We're [just] not going to be able to do that this week.�
Senate Majority Leader Mitch McConnell (R-KY),
Senate Briefing, September 26th
1 2 3
Renew Effort for FY2019
Refocus on Bipartisan Health Reform
Incorporate Health Care into Tax Reform
Three Potential Legislative Paths Forward
"With a process that gives more attention and time, we will repeal and replace Obamacare... It's not a matter of if, only a matter of when."
Senator Lindsey Graham (R-SC),
Senate Briefing, September 26th
©2017 Advisory Board � All Rights Reserved � advisory.com � 35421A
10
Election Raising Questions About the Future of Risk
Despite Uncertainty, Payment Reform Likely to Remain in Some Form
Source: Verma S, �Medicare and Medicaid Need Innovation,� The Wall Street Journal,
September 19, 2017, www.wsj.com; Cardiovascular Roundtable interviews and analysis.
1) Centers for Medicare and Medicaid Innovation.
2) Medicare Access and CHIP Re-Authorization Act.
Key Questions from CV Leaders
How will the new administration impact MACRA2 implementation?
Will the new administration migrate away from payment transformation?
How will CMS prioritize value-based initiatives moving forward?
What is the future of CMMI1 and care transformation programs (e.g., ACOs)?
Many Reasons to Bet on the Future of Payment and Care Delivery Reform
Strong bipartisan support for the concept of payment reform
Near-unanimous bipartisan support for MACRA legislation
CMS Administrator Seema Vermahas confirmed continued support for value-based care
Current administration committed to testing new models to deliver and pay for health care through CMMI
©2017 Advisory Board � All Rights Reserved � advisory.com � 35421A
11
5 Market Realities Impacting CV Programs
Source: Cardiovascular Roundtable research and analysis.
#1
#2
#3
#4
#5
Margin pressure will only intensify for CV
CV is not just increasingly an outpatient business, but an ambulatory business
MACRA is changing physician payment as well as how hospital�s should align with physicians
As referring providers become more accountable for population health, CV will be expected to play a bigger role
The shift to risk is not abating�more CV payment will be tied to cross-continuum cost and quality in the future
©2017 Advisory Board � All Rights Reserved � advisory.com � 35421A
ROAD MAP12
The Next Wave of Health Reform 1
2 5 Market Realities Impacting CV Programs
3 Defining a No-Regrets Strategy
©2017 Advisory Board � All Rights Reserved � advisory.com � 35421A
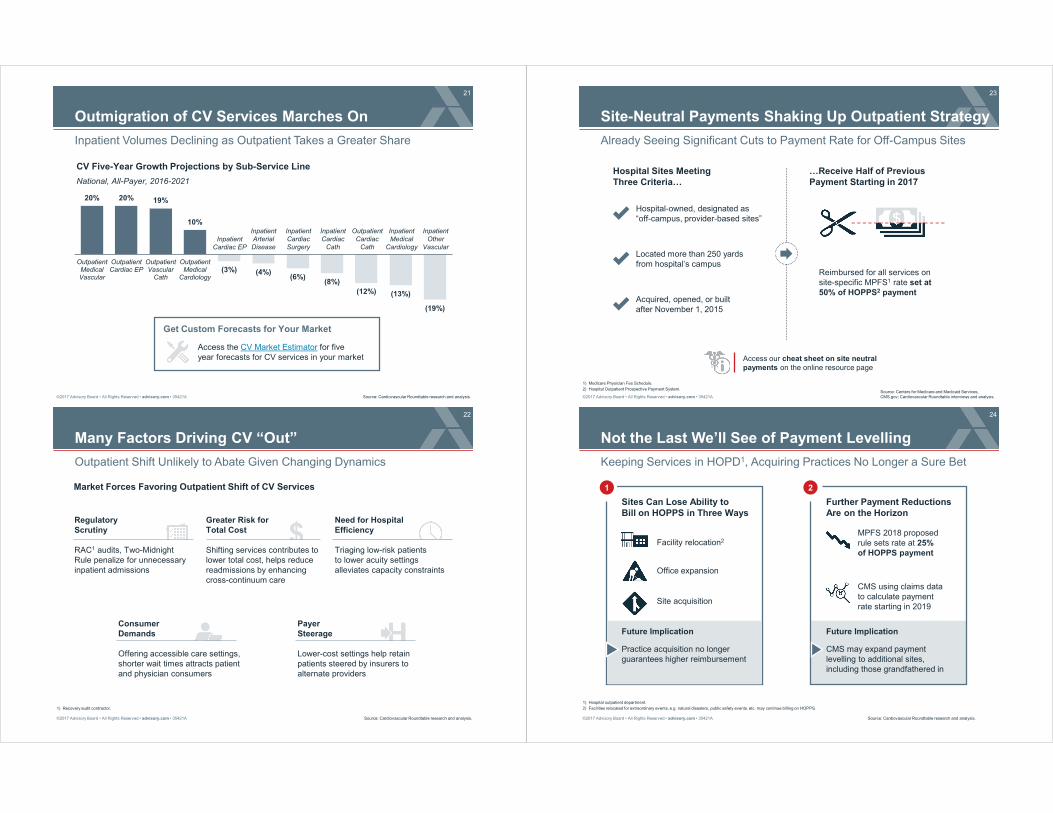
13
Guess What�s Not Getting Repealed
Even If ACA Repealed, Majority of Obama-Era Cuts Would Have Remained
#1: Margin pressure will only intensify for CV
Source: CBO, �Budgetary and Economic Effects of Repealing the Affordable Care Act,� June 2015; CBO, �Letter to the Honorable John Boehner Providing an Estimate for H.R. 6079, The Repeal of Obamacare Act,� July 24, 2012; CBO, �Cost Estimate and Supplemental Analyses for H.R. 2, the Medicare Access and CHIP Reauthorization Act of 2015; Budget of the United States Government (Proposed) FY 2016; Cardiovascular Roundtable research and analysis.
1) Calculation includes ACA Inpatient Prospective Payment System Update Adjustments; ACA Disproportionate Share Hospital payment cuts; MACRA Inpatient Prospective Payment System update adjustments.
�Productivity� Adjustments and Other Cuts to Reimbursement1
2017 2018 2019 2020 2021 2022 2023 2024 2025
($32B)
($48B)($60B)
($71B)($82B)
($94B)($103B)
($116B)
($143B)
60%
Significantly Impacting Margins
Percent of hospitals projected to have negative margins by 2025
©2017 Advisory Board � All Rights Reserved � advisory.com � 35421A
14
C-Suite Feeling the Cost Burden
Beginning to Trick Down to CV Leaders?
Source: Boston Globe, �Partners Health Care cutting $600 million in costs,� May 12, 2017; Modern Healthcare, �Advocate Health Care plans $200 million in cuts,� May 4, 2017; Chicago Tribune, �Edward-Elmhurst Health cutting $50 million,� October 5, 2017; Modern Healthcare, �Detroit Medical Center to reduce workforce to cut $17 million in expenses,� November 30, 2016; Cardiovascular Roundtable research and analysis.
Partners HealthCare cutting $600m in costs
May 12, 2017
Jim Skogsbergh, CEO
ADVOCATE HEALTH CARE
Our existing cost structure is not
sustainable�We believe the
transformation required to solve this
problem will take months, if not years.
Failing to take steps now will turn a
financial challenge into a financial
crisis�something none of us wants."
Detroit Medical Center to reduce workforce to cut $17 million in expenses
November 30, 2016
Edward-Elmhurst Health cutting $50 million
10/05/2017
Advocate Health Care plans $200 million in cuts
May 4, 2017
©2017 Advisory Board � All Rights Reserved � advisory.com � 35421A
15
CV Reimbursement Not What It Used to Be
Payment Updates Requiring Greater Efficiency
Source: CMS; Cardiovascular Roundtable research and analysis.
1) Inpatient payments are final FY 2018 rates; outpatient and physician fee schedule are proposed CY 2018.
2) Unadjusted national average; change values are provided for comparison purposes, but direct comparisons are difficult due to consolidation and restructuring of APCs.
0.54%1.59%
CardiacServices
VascularServices
CV Medicare Payment Changes
2018 Versus 20171
INPATIENT OUTPATIENTPHYSICIAN FEE SCHEDULE
Access a complete list of 2018 paymentupdates on the online resource page
-2.0% -2.0% -2.0%
Cardiology
Cardiac
Surgery
Vascular
Surgery
Select CV Services
APC DescriptionPercent Change2
5188 Level 1 Endovascular Procedures (e.g., diagnostic cardiac cath)
0.4%
5212 Level 2 EP Procedures (e.g., ablation of AV node)
2.8%
©2017 Advisory Board � All Rights Reserved � advisory.com � 35421A
16
CV Costs Increasingly Under the Microscope
Key Market Trends Shaping the Economics of CV Care
Source: Cardiovascular Roundtable research and analysis.
1) Bundled Payments for Care Improvement Initiative.
2) Hospital Value-Based Purchasing; Hospital Inpatient Quality Reporting; Merit-Based Incentive Payment System.
Reimbursement Pressures
� Payment updates not keeping pace with increasing costs
� MACRA holding physician payments steady
� Readmission reduction program
� BPCI1, voluntary risk-based payment models
� New VBP, IQR, MIPS2 episodic cost measures
Pay-for-Performance Programs Scrutinizing Episodic Cost
Shifting Demand to Less Profitable Services
� Softening acute, procedural volumes (e.g., CABG, PCI)
� Shift to outpatient, medical care with lower margins
Cost-Sensitive Patients and Referring Providers
� Patients facing greater out-of-pocket costs
� Increasing price transparency
� Referring providers increasingly accountable for costs under MACRA, ACOs

©2017 Advisory Board � All Rights Reserved � advisory.com � 35421A
17
No Relief in Sight
CV Demographics Increasing Cost of Care Moving Forward
Source: American Heart Association, �Cardiovascular Disease: A Costly Burden for America�Projections Through 2035� (2017); Cardiovascular Roundtable research and analysis.
Cost of CV Disease in United States
Drivers Impacting the Rising Cost of CV Care Delivery
Increase in staffing costs
Investment in more complex, expensive technologies
Increasingly chronic, comorbid patient population
2016
$555 billion
2035
$1.1 trillion
©2017 Advisory Board � All Rights Reserved � advisory.com � 35421A
18
Carving Out a Role in Institution Efforts
Clear Opportunity for CV to Support Targeted Cost Reduction Initiatives
Source: Cardiovascular Roundtable research and analysis.
Savings
Potential
Difficulty
HighLow
Low
High
� Reallocate acute care services across system
� Rightsize excess inpatient capacity
Minimize Unwarranted Care Variation
Restructure Fixed Cost & Assets
Reduce Labor and Supply Costs
� Develop a foundation for implementing care standards
� Eliminate quality shortfalls that increase cost per case
� Update labor staffing models
� Ensure value of supply contracting arrangements
Focus of C-Suite, health system executives
More within CV�s realm of control
©2017 Advisory Board � All Rights Reserved � advisory.com � 35421A
19
ROUNDTABLE RESOURCESStrategies for Success
CV Guideline Compendium
Building the High-Value CV Care Team
Playbook for Reducing CV Care Variation
Practicing Top-of-License CV Care
Build long-term strategies to reduce
programs costs, not just focusing on
quick wins
Build a lean provider team across settings
and services that engages each team
member in high-value care tasks
Develop care standards for areas where
care variation is contributing to high clinical
and operational costs and poor outcomes
Prioritize CV Cost Reduction
1
Ensure Top-of-License Care Delivery
2
Reduce Variation in Care Delivery
3
Source: Cardiovascular Roundtable interviews and analysis.
Playbook for CV Episodic Cost Management
CV Margin Management Resource Center (coming soon)
©2017 Advisory Board � All Rights Reserved � advisory.com � 35421A
20
The Future of Ambulatory Care?
Drones Delivering AEDs in Rural Sweden Save Critical Time
#2: CV is not just increasingly an outpatient business, but an ambulatory business
Source: Columbus C, �Could Drones Help Save People in Cardiac Arrest?� NPR Health Shots, June 13, 2017, http://www.npr.org/; Cardiovascular Roundtable research and analysis.
�Could Drones Help Save
People in Cardiac Arrest?�
Drones delivering automated external defibrillators (AEDs) to cardiac arrest victims in rural Sweden
Andre
as C
laesson/F
lyP
uls
e/N
PR
Reduced Dispatch Time
3 minutes 3 secondsvs.
©2017 Advisory Board � All Rights Reserved � advisory.com � 35421A
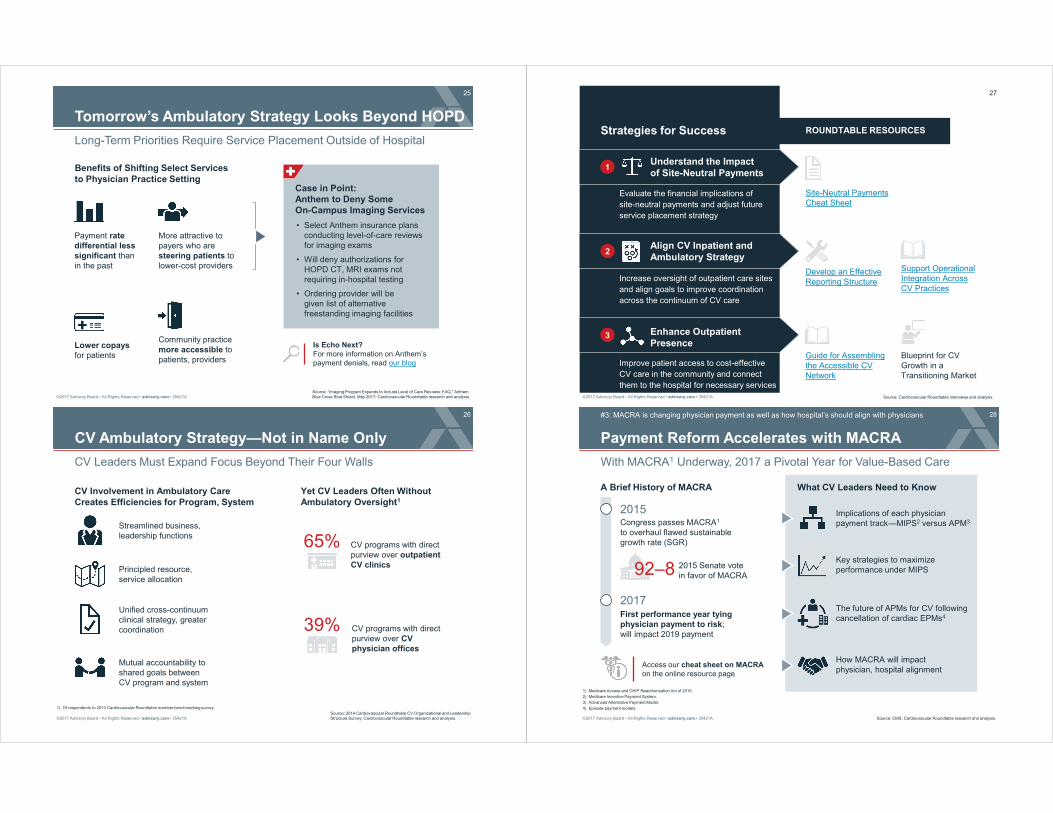
21
Outmigration of CV Services Marches On
Inpatient Volumes Declining as Outpatient Takes a Greater Share
Source: Cardiovascular Roundtable research and analysis.
CV Five-Year Growth Projections by Sub-Service Line
National, All-Payer, 2016-2021
20% 20% 19%
10%
(3%) (4%)(6%)
(8%)
(12%) (13%)
(19%)
OutpatientMedicalVascular
OutpatientCardiac EP
OutpatientVascular
Cath
OutpatientMedical
Cardiology
Inpatient
Arterial
Disease
Inpatient
Cardiac
Surgery
Inpatient
Cardiac
Cath
Outpatient
Cardiac
Cath
Inpatient
Medical
Cardiology
Inpatient
Other
Vascular
Inpatient
Cardiac EP
Get Custom Forecasts for Your Market
Access the CV Market Estimator for five year forecasts for CV services in your market
©2017 Advisory Board � All Rights Reserved � advisory.com � 35421A
22
Many Factors Driving CV �Out�
Outpatient Shift Unlikely to Abate Given Changing Dynamics
Source: Cardiovascular Roundtable research and analysis.
1) Recovery audit contractor.
Greater Risk forTotal Cost
Shifting services contributes to lower total cost, helps reduce readmissions by enhancing cross-continuum care
Market Forces Favoring Outpatient Shift of CV Services
RegulatoryScrutiny
RAC1 audits, Two-Midnight Rule penalize for unnecessary inpatient admissions
Need for HospitalEfficiency
Triaging low-risk patients to lower acuity settings alleviates capacity constraints
Payer Steerage
Lower-cost settings help retain patients steered by insurers to alternate providers
Consumer Demands
Offering accessible care settings, shorter wait times attracts patient and physician consumers
©2017 Advisory Board � All Rights Reserved � advisory.com � 35421A
23
Site-Neutral Payments Shaking Up Outpatient Strategy
Already Seeing Significant Cuts to Payment Rate for Off-Campus Sites
Source: Centers for Medicare and Medicaid Services, CMS.gov; Cardiovascular Roundtable interviews and analysis.
1) Medicare Physician Fee Schedule.
2) Hospital Outpatient Prospective Payment System.
Access our cheat sheet on site neutral payments on the online resource page
Hospital Sites Meeting Three Criteria�
�Receive Half of Previous
Payment Starting in 2017
Reimbursed for all services on site-specific MPFS1 rate set at 50% of HOPPS2 payment
Hospital-owned, designated as �off-campus, provider-based sites�
Located more than 250 yards from hospital�s campus
Acquired, opened, or built after November 1, 2015
©2017 Advisory Board � All Rights Reserved � advisory.com � 35421A
24
Not the Last We�ll See of Payment Levelling
Keeping Services in HOPD1, Acquiring Practices No Longer a Sure Bet
Source: Cardiovascular Roundtable research and analysis.
1) Hospital outpatient department.
2) Facilities relocated for extraordinary events, e.g. natural disasters, public safety events, etc. may continue billing on HOPPS.
1
Site acquisition
Facility relocation2
Office expansion
Practice acquisition no longer guarantees higher reimbursement
Future Implication
Sites Can Lose Ability to Bill on HOPPS in Three Ways
2
CMS using claims data to calculate payment rate starting in 2019
MPFS 2018 proposed rule sets rate at 25% of HOPPS payment
CMS may expand payment levelling to additional sites, including those grandfathered in
Future Implication
Further Payment ReductionsAre on the Horizon
©2017 Advisory Board � All Rights Reserved � advisory.com � 35421A
25
Tomorrow�s Ambulatory Strategy Looks Beyond HOPD
Long-Term Priorities Require Service Placement Outside of Hospital
Source: �Imaging Program Expands to Include Level of Care Reviews: FAQ,� Anthem Blue Cross Blue Shield, May 2017; Cardiovascular Roundtable research and analysis.
Lower copays for patients
Payment rate differential less significant than in the past
Community practice more accessible to patients, providers
More attractive to payers who are steering patients to lower-cost providers
Benefits of Shifting Select Services to Physician Practice Setting
Case in Point: Anthem to Deny SomeOn-Campus Imaging Services
� Select Anthem insurance plans conducting level-of-care reviews for imaging exams
� Will deny authorizations for HOPD CT, MRI exams not requiring in-hospital testing
� Ordering provider will be given list of alternative freestanding imaging facilities
Is Echo Next?For more information on Anthem�s payment denials, read our blog
©2017 Advisory Board � All Rights Reserved � advisory.com � 35421A
26
CV Ambulatory Strategy�Not in Name Only
CV Leaders Must Expand Focus Beyond Their Four Walls
Source: 2014 Cardiovascular Roundtable CV Organizational and Leadership Structure Survey; Cardiovascular Roundtable research and analysis.
1) Of respondents to 2014 Cardiovascular Roundtable member benchmarking survey.
CV Involvement in Ambulatory Care Creates Efficiencies for Program, System
Principled resource, service allocation
Streamlined business, leadership functions
Unified cross-continuum clinical strategy, greater coordination
Mutual accountability to shared goals between CV program and system
Yet CV Leaders Often Without Ambulatory Oversight1
39% CV programs with direct purview over CV physician offices
65% CV programs with direct purview over outpatient CV clinics
©2017 Advisory Board � All Rights Reserved � advisory.com � 35421A
27
ROUNDTABLE RESOURCESStrategies for Success
Evaluate the financial implications of
site-neutral payments and adjust future
service placement strategy
Increase oversight of outpatient care sites
and align goals to improve coordination
across the continuum of CV care
Improve patient access to cost-effective
CV care in the community and connect
them to the hospital for necessary services
Understand the Impact of Site-Neutral Payments
1
Align CV Inpatient and Ambulatory Strategy
2
Enhance OutpatientPresence
3
Source: Cardiovascular Roundtable interviews and analysis.
Site-Neutral PaymentsCheat Sheet
Develop an Effective Reporting Structure
Support Operational Integration Across CV Practices
Guide for Assembling the Accessible CV Network
Blueprint for CV Growth in a Transitioning Market
©2017 Advisory Board � All Rights Reserved � advisory.com � 35421A
28
Payment Reform Accelerates with MACRA
With MACRA1 Underway, 2017 a Pivotal Year for Value-Based Care
#3: MACRA is changing physician payment as well as how hospital�s should align with physicians
Source: CMS; Cardiovascular Roundtable research and analysis.
1) Medicare Access and CHIP Reauthorization Act of 2015.
2) Medicare Incentive Payment System.
3) Advanced Alternative Payment Model.
4) Episode payment models.
A Brief History of MACRA
92�8 2015 Senate vote in favor of MACRA
2015Congress passes MACRA1
to overhaul flawed sustainable growth rate (SGR)
2017First performance year tying physician payment to risk; will impact 2019 payment
Access our cheat sheet on MACRAon the online resource page
What CV Leaders Need to Know
Key strategies to maximize performance under MIPS
Implications of each physician payment track�MIPS2 versus APM3
The future of APMs for CV following cancellation of cardiac EPMs4
How MACRA will impact physician, hospital alignment
©2017 Advisory Board � All Rights Reserved � advisory.com � 35421A
29
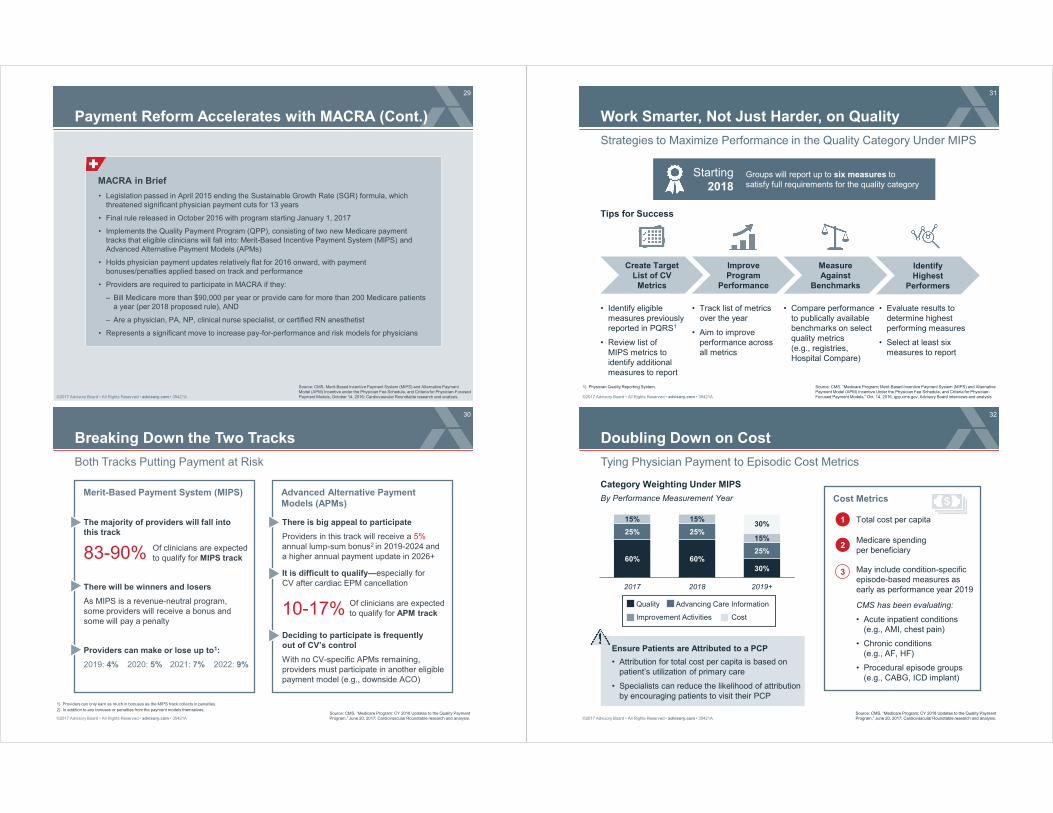
Payment Reform Accelerates with MACRA (Cont.)
Source: CMS, Merit-Based Incentive Payment System (MIPS) and Alternative Payment Model (APM) Incentive under the Physician Fee Schedule, and Criteria for Physician-Focused Payment Models, October 14, 2016; Cardiovascular Roundtable research and analysis.
MACRA in Brief
� Legislation passed in April 2015 ending the Sustainable Growth Rate (SGR) formula, which threatened significant physician payment cuts for 13 years
� Final rule released in October 2016 with program starting January 1, 2017
� Implements the Quality Payment Program (QPP), consisting of two new Medicare payment tracks that eligible clinicians will fall into: Merit-Based Incentive Payment System (MIPS) and Advanced Alternative Payment Models (APMs)
� Holds physician payment updates relatively flat for 2016 onward, with payment bonuses/penalties applied based on track and performance
� Providers are required to participate in MACRA if they:
� Bill Medicare more than $90,000 per year or provide care for more than 200 Medicare patients a year (per 2018 proposed rule), AND
� Are a physician, PA, NP, clinical nurse specialist, or certified RN anesthetist
� Represents a significant move to increase pay-for-performance and risk models for physicians
©2017 Advisory Board � All Rights Reserved � advisory.com � 35421A
30
Breaking Down the Two Tracks
Both Tracks Putting Payment at Risk
Source: CMS, �Medicare Program: CY 2018 Updates to the Quality Payment Program,� June 20, 2017; Cardiovascular Roundtable research and analysis.
1) Providers can only earn as much in bonuses as the MIPS track collects in penalties.
2) In addition to any bonuses or penalties from the payment models themselves.
Merit-Based Payment System (MIPS) Advanced Alternative Payment Models (APMs)
The majority of providers will fall into this track
83-90%
10-17%
Of clinicians are expected to qualify for MIPS track
Of clinicians are expected to qualify for APM track
There will be winners and losers
As MIPS is a revenue-neutral program, some providers will receive a bonus and some will pay a penalty
2020: 5% 2021: 7% 2022: 9%
Providers can make or lose up to1:
2019: 4%
It is difficult to qualify�especially for CV after cardiac EPM cancellation
There is big appeal to participate
Providers in this track will receive a 5% annual lump-sum bonus2 in 2019-2024 and a higher annual payment update in 2026+
Deciding to participate is frequently out of CV�s control
With no CV-specific APMs remaining, providers must participate in another eligible payment model (e.g., downside ACO)
©2017 Advisory Board � All Rights Reserved � advisory.com � 35421A
31
Work Smarter, Not Just Harder, on Quality
Strategies to Maximize Performance in the Quality Category Under MIPS
Source: CMS, �Medicare Program; Merit-Based Incentive Payment System (MIPS) and Alternative Payment Model (APM) Incentive Under the Physician Fee Schedule, and Criteria for Physician-Focused Payment Models,� Oct. 14, 2016, qpp.cms.gov. Advisory Board interviews and analysis
1) Physician Quality Reporting System.
� Track list of metrics over the year
� Aim to improve performance across all metrics
Improve Program
Performance
Measure Against
Benchmarks
Identify Highest
Performers
Create Target List of CV
Metrics
� Identify eligible measures previously reported in PQRS1
� Review list of MIPS metrics to identify additional measures to report
� Evaluate results to determine highest performing measures
� Select at least six measures to report
� Compare performance to publically available benchmarks on select quality metrics (e.g., registries, Hospital Compare)
Starting2018
Groups will report up to six measures to satisfy full requirements for the quality category
Tips for Success
©2017 Advisory Board � All Rights Reserved � advisory.com � 35421A
32
Doubling Down on Cost
Tying Physician Payment to Episodic Cost Metrics
Category Weighting Under MIPS
60% 60%
30%
25% 25%
25%
15% 15%
15%
30%
2017 2018 2019+
Source: CMS, �Medicare Program: CY 2018 Updates to the Quality Payment Program,� June 20, 2017; Cardiovascular Roundtable research and analysis.
Quality Advancing Care Information
Improvement Activities Cost
By Performance Measurement Year Cost Metrics
1
2
3
Total cost per capita
Medicare spending per beneficiary
May include condition-specific episode-based measures as early as performance year 2019
CMS has been evaluating:
� Acute inpatient conditions (e.g., AMI, chest pain)
� Chronic conditions (e.g., AF, HF)
� Procedural episode groups (e.g., CABG, ICD implant)
Ensure Patients are Attributed to a PCP
� Attribution for total cost per capita is based on patient�s utilization of primary care
� Specialists can reduce the likelihood of attribution by encouraging patients to visit their PCP

©2017 Advisory Board � All Rights Reserved � advisory.com � 35421A
33
APMs Not Primed for CV
Majority of Existing Qualifying Models Out of CV Leaders� Control
Source: CMS, �2018 Updates to the Quality Payment Program,� (2017); HHS, �Secretary�s Response to the ACS-Brandeis Advanced APM,� September 7, 2017, available at www.innovation.gov; Cardiovascular Roundtable research and analysis.
But New APMs on the Horizon May Be Positive Signs for CV
Voluntary CMS CV BundlesTo be developed for 2018
Forthcoming voluntary risk-based payment model for select CV conditions, services
Medicare AdvantageTo become eligible for APM
track starting in 2021
Private Payer Models
Example: ACS-Brandeis APMIncludes CABG, valve surgery, and HF, recently approved for limited testing
Responsible entity can be a group of physicians rather than a hospital
Even providers selected for cardiac EPMs may have had difficulty meeting the thresholds to qualify for APM track
� Receive 25% of Medicare payments through APM or,
� See 20% of Medicare patients through APM
Majority of APMs centered around primary care (e.g., ACOs)
Even if participating in an APM, programs still have to meet high payment, volume thresholds
Limitations of APM Models for CV
©2017 Advisory Board � All Rights Reserved � advisory.com � 35421A
34
An Environment Ripe for Partnership
MACRA Will Drive�and Require�Hospital-Physician Alignment
Source: Medical Group Management Association 2017 Cost and Revenue Survey; Cardiovascular Roundtable research and analysis.
$15,128IT operating expenses per FTE physician at a physician-owned CV practice
Improve performance under MIPS
Offload reporting burden
Stabilize practice economics
Case in Point: IT Expense
Think Strategically About Alignment
Hospitals employing physicians will be accountable for physician performance under MIPS
Programs may restructure physician incentive models to incorporate metrics impacting performance under MACRA
Physicians Will Increasingly Look to Employment To�
Health Systems Should�
Consider opportunities to scale physician network to support new or existing risk contracts
©2017 Advisory Board � All Rights Reserved � advisory.com � 35421A
35
ROUNDTABLE RESOURCESStrategies for Success
Design Effective CV Physician Compensation Models
Educate physicians and CV leaders on
the implications of MACRA and how to
be successful
Be selective in employing physicians as
hospitals will be financially accountable
for employed physician performance
under MIPS
Structure physician compensation
models to include metrics that align
with those you are at-risk for under
MACRA
Learn MoreAbout MACRA
1
Carefully Evaluate YourPhysician Alignment Strategy
2
Redesign Incentives to Align with New Metrics of Success
3
Source: Cardiovascular Roundtable interviews and analysis.
MACRA Cheat Sheet
MACRA: What the 2018 Proposed Rule Means for Providers
MIPS measures picklist at qpp.cms.gov
Advancing CV Hospital-Specialist Alignment
©2017 Advisory Board � All Rights Reserved � advisory.com � 35421A
36
A New Prescription for� Food?
Geisinger�s Fresh Food Pharmacy Aims to Improve Health, Reduce Costs
#4: As referring providers become more accountable for population health, CV will be expected to play a bigger role
Source: Aubrey A, �Fresh Food By Prescription: This Health Care Firm is Trimming Costs� And Waistlines,� NPR: The Salt, May 8, 2017; Geisinger Health System, �An RX for Good Health: Geisinger Launches Fresh Food Pharmacy,� PR Newswire, November 10, 2016; Cardiovascular Roundtable research and analysis.
Geisinger�s Fresh Food Pharmacy Program
� Program measuring the impact of healthy food, education for diabetes patients
� Provides free, fresh food weekly in addition to nutrition counselling, meal preparation lessons
Early Program Successes
Per-patient reduction in hemoglobin A1C points
Estimated per-patient savings from program3 $24K
Big
Fis
hD
esig
n/N
PR

©2017 Advisory Board � All Rights Reserved � advisory.com � 35421A
37
Primary Care at Center of Population Health Efforts
Seeing Continued Interest in ACOs, but CV Often Left On the Sidelines
Source: CMS, available at: data.cms.gov; Advisory Board, �Where the ACOs are�, available at: advisory.com; Cardiovascular Roundtable interviews and analysis.
.
220
353 404
474 525
2013 2014 2015 2016 2017
Yet CV Leaders Rarely Involved in ACO Decisions
ACO Participation Continues to Grow
Total ACO Participants, by Performance Year
VP Heart & Vascular Services
Large Hospital in the Midwest
Our physicians are assigned to an ACO on the contract, but as far as our involvement? I�d say minimal at best.�
Director of CV Services
AMC in the Northeast
We�ve received a global view and know the goals of the ACO, but we haven�t quite
formulated our strategies to function as one in CV.�
©2017 Advisory Board � All Rights Reserved � advisory.com � 35421A
38
Risks of Non-Action Too Great to Ignore
Accountable PCPs1 Changing Referral Patterns to CV Specialists
Source: Cardiovascular Roundtable research and analysis.
1) Primary care providers.
2) Pseudonym.
3) Aortic stenosis.
Potential Consequences for CV Due to Care Redesign Initiatives
ACO PCPs hesitant to refer patients for high-cost specialty services
Patients referred later in disease progression, with more acute needs
CV program locked out of referral network if not demonstrating high-value care
An Extreme Example: Curie Hospital2
� Large CV program with robust structural heart program
� Hospital-employed PCPs joined ACO, started referring fewer valve patients due to fear patients would receive expensive treatments (e.g., TAVR)
� Structural heart program sees volume decline, threatens stability
� Patients with AS3 referred too late in disease progression
PCPs Acting as Gatekeeper for High-End CV Care
©2017 Advisory Board � All Rights Reserved � advisory.com � 35421A
39
Positioning CV to Succeed Under Care Redesign
Programs Must Demonstrate Value to Secure Continued Referrals
Source: Cardiovascular Roundtable research and analysis.
Secure Referrer Trust
Strengthen referring physician alignment by demonstrating positive outcomes and appropriate utilization
Improve Patient Access
Ensure timely, convenient referrals and appointments in accessible care settings
Provide Quality Care at Low Cost
Deliver high-quality, low-cost care to demonstrate high-value CV care delivery
Imperatives for Success Under Care Redesign Initiatives
Market to Providers Based on Value
Emphasize quality of care, appropriate utilization, and cost reduction efforts to attract referring PCPs
©2017 Advisory Board � All Rights Reserved � advisory.com � 35421A
40
A New Role for CV in Population Health
Million Hearts Initiative Puts Primary Prevention in the Spotlight
Source: CMS, �Million Hearts,� https://innovation.cms.gov/; HHS, �Million Hearts,� https://millionhearts.hhs.gov/; �Million Hearts: Meaningful Progress 2012-2016�; Ritchey M, et al., �Million Hearts: Description of the National Surveillance and Modeling Methodology Used to Monitor the Number of Cardiovascular Events Prevented During 2012-2016,� J. Am Heart Assoc, 6, no. 5 (2017): e006021; Cardiovascular Roundtable research and analysis.
1) Defined as heart attacks, strokes, and other CVD-related ED encounter or hospitalization with a primary ICD9 or death code.
2) Million Hearts program estimate, based on available data for prior years.
3) Cardiovascular disease.
4) Transient ischemic attack.
5) Fee-for-service.
500KCV events1 prevented between 2012 and 20162
� CMS initiative launched in 2011
� Goal to prevent one million heart attacks and strokes
� Provides guidance on CV primary prevention efforts
Million Hearts Initiative
3.3MMedicare FFS5
beneficiaries
20KHealth care practitioners
Expected Program Reach by 2021
� Million Hearts CVD3 Risk Reduction Model launched in 2016
� 516 organizations selected to participate
� Participants receive a stipend for managing patients at high-risk of CVD who have not yet had a heart attack, stroke, or TIA4
New Model Tying Payment to Prevention
Successfully Preventing CV Events
©2017 Advisory Board � All Rights Reserved � advisory.com � 35421A
41
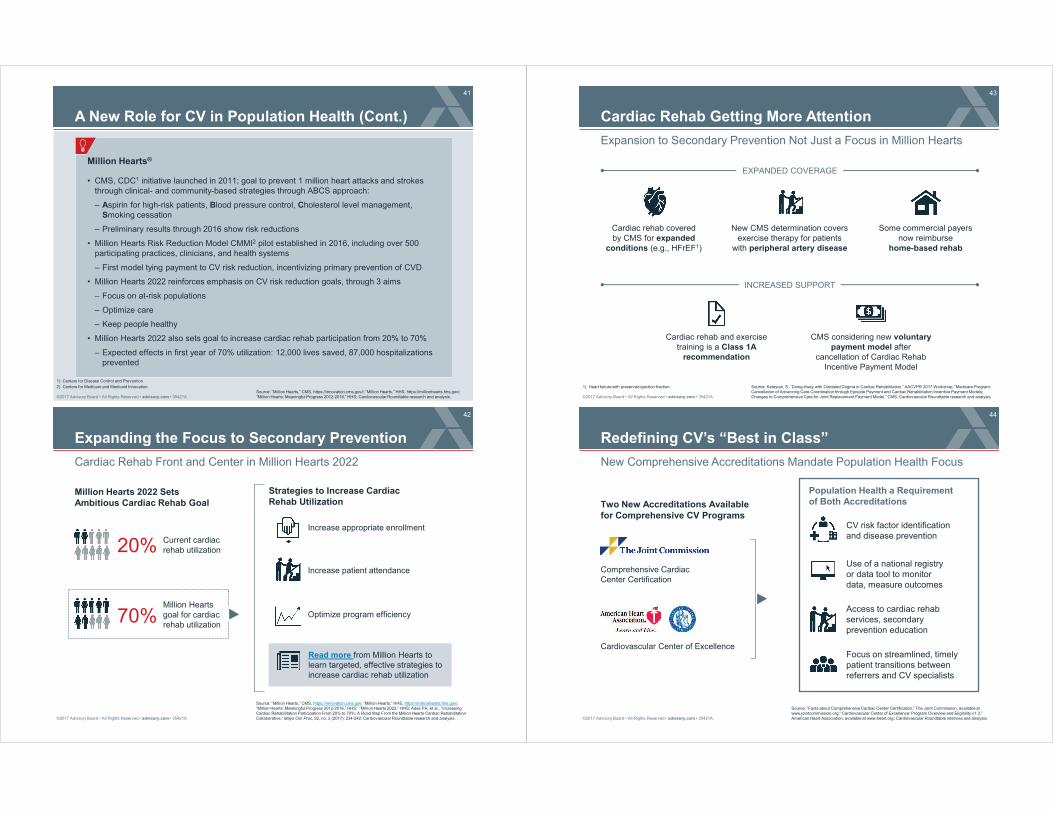
A New Role for CV in Population Health (Cont.)
Source: �Million Hearts,� CMS, https://innovation.cms.gov/l; �Million Hearts,� HHS, https://millionhearts.hhs.gov/; �Million Hearts: Meaningful Progress 2012-2016,� HHS; Cardiovascular Roundtable research and analysis.
1) Centers for Disease Control and Prevention.
2) Centers for Medicare and Medicaid Innovation.
Million Hearts®
� CMS, CDC1 initiative launched in 2011; goal to prevent 1 million heart attacks and strokes through clinical- and community-based strategies through ABCS approach:
� Aspirin for high-risk patients, Blood pressure control, Cholesterol level management, Smoking cessation
� Preliminary results through 2016 show risk reductions
� Million Hearts Risk Reduction Model CMMI2 pilot established in 2016, including over 500 participating practices, clinicians, and health systems
� First model tying payment to CV risk reduction, incentivizing primary prevention of CVD
� Million Hearts 2022 reinforces emphasis on CV risk reduction goals, through 3 aims
� Focus on at-risk populations
� Optimize care
� Keep people healthy
� Million Hearts 2022 also sets goal to increase cardiac rehab participation from 20% to 70%
� Expected effects in first year of 70% utilization: 12,000 lives saved, 87,000 hospitalizations prevented
©2017 Advisory Board � All Rights Reserved � advisory.com � 35421A
42
Expanding the Focus to Secondary Prevention
Cardiac Rehab Front and Center in Million Hearts 2022
Source: �Million Hearts,� CMS, https://innovation.cms.gov; �Million Hearts,� HHS, https://millionhearts.hhs.gov/; �Million Hearts: Meaningful Progress 2012-2016,� HHS; �Million Hearts 2022,� HHS; Ades PA, et al., �Increasing Cardiac Rehabilitation Participation From 20% to 70%: A Road Map From the Million Hearts Cardiac Rehabilitation Collaborative,� Mayo Clin Proc, 92, no. 2 (2017): 234-242; Cardiovascular Roundtable research and analysis.
Million Hearts 2022 Sets Ambitious Cardiac Rehab Goal
20%
70%
Current cardiac rehab utilization
Million Hearts goal for cardiac rehab utilization
Increase appropriate enrollment
Increase patient attendance
Optimize program efficiency
Strategies to Increase Cardiac Rehab Utilization
Read more from Million Hearts to learn targeted, effective strategies to increase cardiac rehab utilization
©2017 Advisory Board � All Rights Reserved � advisory.com � 35421A
43
Cardiac Rehab Getting More Attention
Expansion to Secondary Prevention Not Just a Focus in Million Hearts
Source: Keteyian, S, �Doing Away with Outdated Dogma in Cardiac Rehabilitation,� AACVPR 2017 Workshop; �Medicare Program: Cancellation of Advancing Care Coordination through Episode Payment and Cardiac Rehabilitation Incentive Payment Models; Changes to Comprehensive Care for Joint Replacement Payment Model,� CMS; Cardiovascular Roundtable research and analysis.
1) Heart failure with preserved ejection fraction.
INCREASED SUPPORT
EXPANDED COVERAGE
Cardiac rehab covered by CMS for expanded
conditions (e.g., HFrEF1)
New CMS determination covers exercise therapy for patients
with peripheral artery disease
Some commercial payers now reimburse
home-based rehab
Cardiac rehab and exercise training is a Class 1A
recommendation
CMS considering new voluntary payment model after
cancellation of Cardiac Rehab Incentive Payment Model
©2017 Advisory Board � All Rights Reserved � advisory.com � 35421A
44
Redefining CV�s �Best in Class�
New Comprehensive Accreditations Mandate Population Health Focus
Source: �Facts about Comprehensive Cardiac Center Certification,� The Joint Commission, available at www.jointcommission.org; �Cardiovascular Center of Excellence: Program Overview and Eligibility v1.3,� American Heart Association, available at www.heart.org; Cardiovascular Roundtable intervies and analysis.
Population Health a Requirement of Both Accreditations
Use of a national registry or data tool to monitor data, measure outcomes
CV risk factor identification and disease prevention
Access to cardiac rehab services, secondary prevention education
Focus on streamlined, timely patient transitions between referrers and CV specialists
Two New Accreditations Available for Comprehensive CV Programs
Cardiovascular Center of Excellence
Comprehensive Cardiac Center Certification
©2017 Advisory Board � All Rights Reserved � advisory.com � 35421A
45
ROUNDTABLE RESOURCESStrategies for Success
Enhancing CV Specialist Partnerships with Primary Care
Give PCPs guidance and tools to help
them identify and refer CV patients
earlier in disease progression
Develop profitable, effective cardiac,
PAD, and pulmonary rehab and make
sure patients are referred and attend
Tailor cross-continuum care management
services to patients based on risk
Help PCPs IdentifyCV Patients
1
Increase Utilization of CV Rehab Programs
2
Improve Care Management for High-Risk Patients
3
Source: Cardiovascular Roundtable interviews and analysis.
CV Referral Guideline Compendium
Tactics for Sustainable Pulmonary Rehab Program Development
Blueprint for CV Care Management
Cardiac Rehab: Strategies for Success webconference (December 2018)
©2017 Advisory Board � All Rights Reserved � advisory.com � 35421A
46
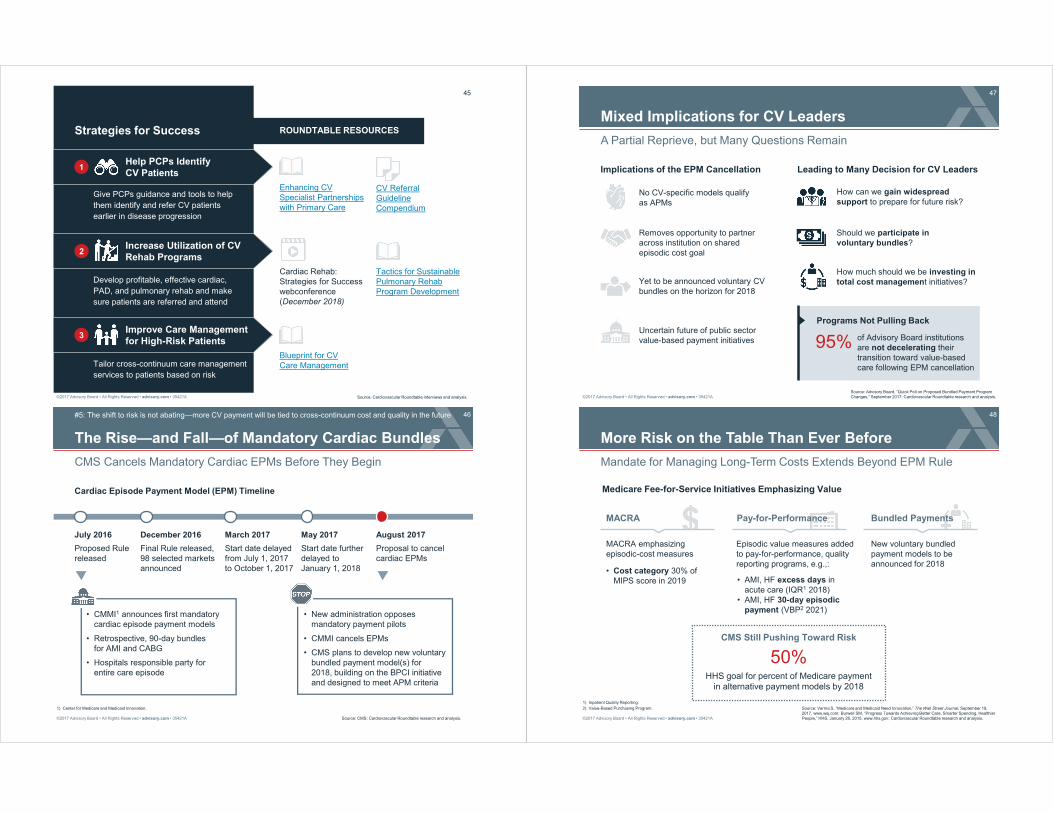
The Rise�and Fall�of Mandatory Cardiac Bundles
CMS Cancels Mandatory Cardiac EPMs Before They Begin
#5: The shift to risk is not abating�more CV payment will be tied to cross-continuum cost and quality in the future
Source: CMS; Cardiovascular Roundtable research and analysis.
1) Center for Medicare and Medicaid Innovation.
� New administration opposes mandatory payment pilots
� CMMI cancels EPMs
� CMS plans to develop new voluntary bundled payment model(s) for2018, building on the BPCI initiative and designed to meet APM criteria
July 2016
Cardiac Episode Payment Model (EPM) Timeline
December 2016 August 2017March 2017 May 2017
� CMMI1 announces first mandatory cardiac episode payment models
� Retrospective, 90-day bundles for AMI and CABG
� Hospitals responsible party for entire care episode
Proposed Rulereleased
Final Rule released, 98 selected markets announced
Start date delayed from July 1, 2017 to October 1, 2017
Start date further delayed to January 1, 2018
Proposal to cancel cardiac EPMs
©2017 Advisory Board � All Rights Reserved � advisory.com � 35421A
47
Mixed Implications for CV Leaders
A Partial Reprieve, but Many Questions Remain
Source: Advisory Board, �Quick Poll on Proposed Bundled Payment Program Changes,� September 2017; Cardiovascular Roundtable research and analysis.
No CV-specific models qualify as APMs
Yet to be announced voluntary CV bundles on the horizon for 2018
Removes opportunity to partner across institution on shared episodic cost goal
Uncertain future of public sector value-based payment initiatives
How can we gain widespread support to prepare for future risk?
Should we participate in voluntary bundles?
How much should we be investing in total cost management initiatives?
Implications of the EPM Cancellation Leading to Many Decision for CV Leaders
Programs Not Pulling Back
95% of Advisory Board institutions are not decelerating their transition toward value-based care following EPM cancellation
©2017 Advisory Board � All Rights Reserved � advisory.com � 35421A
48
More Risk on the Table Than Ever Before
Mandate for Managing Long-Term Costs Extends Beyond EPM Rule
Source: Verma S, �Medicare and Medicaid Need Innovation,� The Wall Street Journal, September 19, 2017, www.wsj.com; Burwell SM, �Progress Towards Achieving Better Care, Smarter Spending, Healthier People,� HHS, January 26, 2015, www.hhs.gov; Cardiovascular Roundtable research and analysis.
1) Inpatient Quality Reporting.
2) Value-Based Purchasing Program.
Medicare Fee-for-Service Initiatives Emphasizing Value
� Cost category 30% of MIPS score in 2019 � AMI, HF excess days in
acute care (IQR1 2018)� AMI, HF 30-day episodic
payment (VBP2 2021)
Alternative Payment Models
MACRA emphasizing episodic-cost measures
Episodic value measures added to pay-for-performance, quality reporting programs, e.g.,:
New voluntary bundled payment models to be announced for 2018
50%HHS goal for percent of Medicare payment
in alternative payment models by 2018
CMS Still Pushing Toward Risk
MACRA Pay-for-Performance Bundled Payments

©2017 Advisory Board � All Rights Reserved � advisory.com � 35421A
49
Private Sector Spurring More Innovation
Risk-Based Payment Models Not Losing Steam for Private Payers
Source: Health Care Transformation Task Force, �Health Care Transformation Task Force Urges Incoming Administration and Congress to Continue Drive for Value-Based Payments,� December 6, 2016, available on www.hcttf.org; Cardiovascular Roundtable research and analysis.
1) Smarter Management And Resource use for Today�s complex cardiac Care.
2) Medicaid-led, multi-payer, multi-part payment model.
Percent of payments to be tied to risk-based payment models by 2020
Commitment from Health Care Transformation Task Force
Sample Private Sector Payment Innovations Impacting CV
The SMARTCare1 program has proposed a bundled payment for diagnosis and treatment of stable ischemic heart disease
Horizon Blue Cross Blue Shield of New Jersey�s Episodes of Care program includes HF and CABG episode payments
Arkansas Health Care Payment Improvement Initiative2 includes HF and CABG episode payments
75%
©2017 Advisory Board � All Rights Reserved � advisory.com � 35421A
50
Medicare Advantage Increasing Its Reach
Private Models Testing Payment Innovation in Medicare
Source: CMS; CBO, �March 2015 Medicare Baseline,� March 9, 2015, available at www.cbo.gov; Cardiovascular Roundtable research and analysis.
MA1 Continues to Grow
Enrollment in Millions, Percentage
of Total Medicare Population
5.6M(13%)
16.8M(31%)
202520152005
30.0M40%
CMS testing Medicare Advantage Value-Based Insurance Design (VBID)Model for enrollees in select states with defined chronic conditions2
Medicare Advantage will count as a MACRA APM starting in 2021
Implications on CV Programs
More capitation
Tying more payment to cost, quality
1) Medicare Advantage.
2) Including diabetes, CHF, past stroke, hypertension, COPD, CAD.
Focus on closing care gaps
©2017 Advisory Board � All Rights Reserved � advisory.com � 35421A
51
ROUNDTABLE RESOURCESStrategies for Success
Playbook for CV Episodic Cost Management
Identify where you have the greatest
opportunity to reduce costs across the
continuum as both public and private
payers increase scrutiny
Provide high-quality cross-continuum care
to attract patients, providers, and payers
and reduce unnecessary utilization
1
Improve Quality of Care
2
3
Source: Cardiovascular Roundtable interviews and analysis.
CV Playbook for Avoidable Costs
Playbook for Reducing CV Care Variation
Learn More About 2018 Medicare Updates
Reduce EpisodicCare Costs
Medicare Payment Update Final Rule for Hospital Inpatient Payments for FY 2018
Medicare Payment Update Final Rule for Hospital Outpatient Payments for CY 2018
CV Readmission Reduction Toolkits
Understand what metrics your program
will be measured against in Medicare
pay-for-performance programs
©2017 Advisory Board � All Rights Reserved � advisory.com � 35421A
52
5 Market Realities Impacting CV Programs
Source: Cardiovascular Roundtable research and analysis.
#1
#2
#3
#4
#5
Margin pressure will only intensify for CV
CV is not just increasingly an outpatient business, but an ambulatory business
MACRA is changing physician payment as well as how hospital�s should align with physicians
As referring providers become more accountable for population health, CV will be expected to play a bigger role
The shift to risk is not abating�more CV payment will be tied to cross-continuum cost and quality in the future
©2017 Advisory Board � All Rights Reserved � advisory.com � 35421A
ROAD MAP53
The Next Wave of Health Reform 1
2 5 Market Realities Impacting CV Programs
3 Defining a No-Regrets Strategy
©2017 Advisory Board � All Rights Reserved � advisory.com � 35421A
54
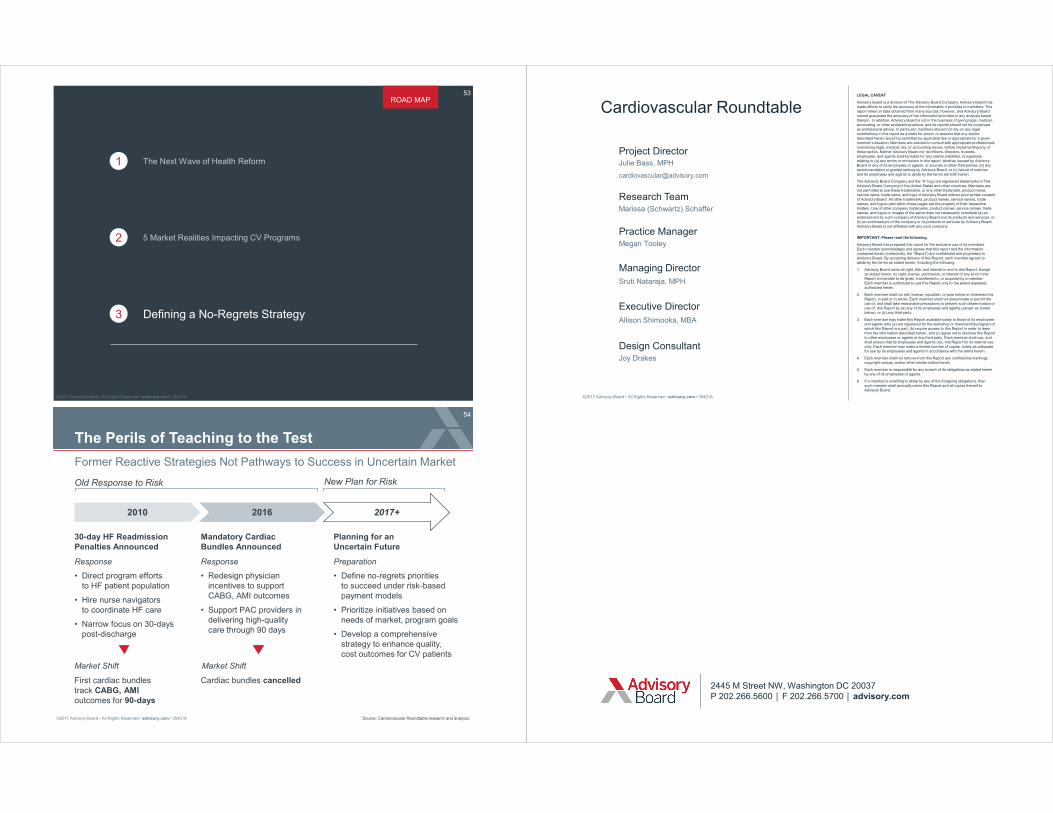
The Perils of Teaching to the Test
Former Reactive Strategies Not Pathways to Success in Uncertain Market
Source: Cardiovascular Roundtable research and analysis.
2010 2016 2017+
30-day HF Readmission Penalties Announced
Response
Cardiac bundles cancelled
Preparation
� Define no-regrets priorities to succeed under risk-based payment models
� Prioritize initiatives based on needs of market, program goals
� Develop a comprehensive strategy to enhance quality, cost outcomes for CV patients
Old Response to Risk New Plan for Risk
� Direct program efforts to HF patient population
� Hire nurse navigators to coordinate HF care
� Narrow focus on 30-days post-discharge
Mandatory Cardiac Bundles Announced
Response
� Redesign physician incentives to support CABG, AMI outcomes
� Support PAC providers in delivering high-quality care through 90 days
First cardiac bundles track CABG, AMI outcomes for 90-days
Planning for an Uncertain Future
Market Shift Market Shift
©2017 Advisory Board � All Rights Reserved � advisory.com � 35421A
LEGAL CAVEAT
Advisory Board is a division of The Advisory Board Company. Advisory Board has made efforts to verify the accuracy of the information it provides to members. This report relies on data obtained from many sources, however, and Advisory Board cannot guarantee the accuracy of the information provided or any analysis based thereon. In addition, Advisory Board is not in the business of giving legal, medical, accounting, or other professional advice, and its reports should not be construedas professional advice. In particular, members should not rely on any legal commentary in this report as a basis for action, or assume that any tactics described herein would be permitted by applicable law or appropriate for a given member�s situation. Members are advised to consult with appropriate professionals concerning legal, medical, tax, or accounting issues, before implementing any of these tactics. Neither Advisory Board nor its officers, directors, trustees, employees, and agents shall be liable for any claims, liabilities, or expenses relating to (a) any errors or omissions in this report, whether caused by Advisory Board or any of its employees or agents, or sources or other third parties, (b) any recommendation or graded ranking by Advisory Board, or (c) failure of memberand its employees and agents to abide by the terms set forth herein.
The Advisory Board Company and the �A� logo are registered trademarks of The Advisory Board Company in the United States and other countries. Members are not permitted to use these trademarks, or any other trademark, product name, service name, trade name, and logo of Advisory Board without prior written consent of Advisory Board. All other trademarks, product names, service names, trade names, and logos used within these pages are the property of their respective holders. Use of other company trademarks, product names, service names, trade names, and logos or images of the same does not necessarily constitute (a) an endorsement by such company of Advisory Board and its products and services, or (b) an endorsement of the company or its products or services by Advisory Board. Advisory Board is not affiliated with any such company.
IMPORTANT: Please read the following.
Advisory Board has prepared this report for the exclusive use of its members.Each member acknowledges and agrees that this report and the information contained herein (collectively, the �Report�) are confidential and proprietary to Advisory Board. By accepting delivery of this Report, each member agrees toabide by the terms as stated herein, including the following:
1. Advisory Board owns all right, title, and interest in and to this Report. Except as stated herein, no right, license, permission, or interest of any kind in this Report is intended to be given, transferred to, or acquired by a member.Each member is authorized to use this Report only to the extent expressly authorized herein.
2. Each member shall not sell, license, republish, or post online or otherwise this Report, in part or in whole. Each member shall not disseminate or permit the use of, and shall take reasonable precautions to prevent such dissemination or use of, this Report by (a) any of its employees and agents (except as stated below), or (b) any third party.
3. Each member may make this Report available solely to those of its employees and agents who (a) are registered for the workshop or membership program of which this Report is a part, (b) require access to this Report in order to learn from the information described herein, and (c) agree not to disclose this Report to other employees or agents or any third party. Each member shall use, and shall ensure that its employees and agents use, this Report for its internal use only. Each member may make a limited number of copies, solely as adequate for use by its employees and agents in accordance with the terms herein.
4. Each member shall not remove from this Report any confidential markings, copyright notices, and/or other similar indicia herein.
5. Each member is responsible for any breach of its obligations as stated herein by any of its employees or agents.
6. If a member is unwilling to abide by any of the foregoing obligations, thensuch member shall promptly return this Report and all copies thereof to Advisory Board.
Cardiovascular Roundtable
Project DirectorJulie Bass, MPH
Research TeamMarissa (Schwartz) Schaffer
Practice ManagerMegan Tooley
Design ConsultantJoy Drakes
Sruti Nataraja, MPH
Managing Director
Allison Shimooka, MBA
Executive Director
2445 M Street NW, Washington DC 20037P 202.266.5600 ! F 202.266.5700 ! advisory.com