craniosynostosis: implementation and validation of a new ... · protocols for their application in...
TRANSCRIPT
CentralBringing Excellence in Open Access
JSM Pediatric Neurology
Cite this article: Blanco-Lobato P, Vazquez JL, Pombar MA, Salgado-Barreira A, Fernandez-Lorenzo JR, et al. (2017) Craniosynostosis: Implementation and Validation of a New Optimized Low-Dose Multidetector CT Protocol for Skull Assessment. JSM Pediatr Neurol 1(2): 1007.
*Corresponding authorPatricia Blanco-Lobato, Departamento de Radiodiagnóstico, Complejo Hospitalario Universitario de Vigo, Hospital Alvaro Cunqueiro, Estrutura Organizativa de Xestión Integrada de Vigo, Estrada de Clara Campoamor, 341, 36312 Vigo, Pontevedra, Spain, Email:
Submitted: 29 April 2017
Accepted: 21 June 2017
Published: 23 June 2017
Copyright© 2017 Blanco-Lobato et al.
OPEN ACCESS
Keywords•Multidetector computed tomography•Low dose•Image quality•Craniosynostosis•Child
Research Article
Craniosynostosis: Implementation and Validation of a New Optimized Low-Dose Multidetector CT Protocol for Skull AssessmentPatricia Blanco-Lobato1*, Jose L. Vazquez1, Miguel A. Pombar2, Angel Salgado-Barreira3, Jose R. Fernandez-Lorenzo4, and Juan M. Vieito1
1Department of Radiology, Complejo Hospitalario Universitario de Vigo, Spain2Department of Radiophysics, Complejo Hospitalario Universitario de Santiago de Compostela, Spain3Department of Research Support, Complejo Hospitalario Universitario de Vigo, Spain4Department of Pediatrics, Complejo Hospitalario Universitario de Vigo, Spain
Abstract
Objectives: Given the particular sensitivity of children to ionizing radiation it is considered essential the continuous development of low-dose optimized CT protocols for their application in the pediatric population.
We present the implementation and validation of an optimized low-dose multidetector CT protocol for the evaluation of cranial deformity in children.
Study design: A prospective study of 102 CT exams performed in 93 pediatric patients. We applied a self-developed 64-multidetector CT low-dose protocol designed for the study of the skull. Dose indicators used were: computed tomography dose index volume (CTDIvol), dose-length product (DLP) and effective dose (E). For statistical analysis the Kruskal-Wallis test was used. Additional lifetime cancer risk estimate was also calculated.
Results: Diagnostic accuracy of the studies was considered good. Mean dose values obtained were: CTDIvol 1.9 mGy, DLP 32.4 mGy•cm and E 0.36 mSv in the 0-1 year-old group and CTDIvol 2.1 mGy, DLP 38.5 mGy•cm and E 0.26 mSv in the 1-5 years-old group. Additional lifetime cancer risk was negligible.
Conclusion: This study validates low-dose multidetector CT as an excellent tool for the evaluation of the pediatric skull and may well be considered as the initial diagnostic technique for the study of cranial deformities in clinically selected patients.
ABBREVIATIONSAEC: Automatic Exposure Control; ALARA: As Low As
Reasonably Achievable; CTDIvol: Computed Tomography Dose Index; DLP: Volume Dose-Length Product; E: Effective dose; MDCT: Multidetector Computed Tomography; NI: Noise Index; DICOM: Digital Imaging and Communication in Medicine
INTRODUCTIONSince its application into clinical practice in 1974, the use of
CT as a diagnostic imaging technique has grown both substantial and rapidly, reaching at the present time around 70 million of CT scans performed each year in the United States of America [1]. Remarkably, the largest increase has been in the diagnosis of pediatric disorders; with up to 7 million CT exams performed annually, a quarter of which are head CT studies [1-4].
Its main disadvantage is the use of ionizing radiation,
comprising relatively high doses compared to conventional radiography. In fact, although CT exams represent only a small percentage of all radiological examinations, some authors reports that its dose accounts for up to 70% of medically induced radiation exposure to the general population. Moreover, radiation is accumulative and around 30% of patients who have had a CT study will have a second or more CT scans in the future [2].
Parallel to the increasing use of CT grows the preoccupation about the associated risk of radiation-induced harm. Radiation dose is of concern in the general population and specifically in children. Within this context, it is considered essential to develop dose-reduced optimized CT protocols for their application in the general population, and especially in children. Following the ALARA (As Low As Reasonably Achievable) radiation protection principle, the radiation dose required to produce a diagnostic quality exam may be significantly reduced in many if not in most studies [5-7]. This is particularly true for those targeted to the

CentralBringing Excellence in Open Access
Blanco-Lobato et al. (2017)Email:
JSM Pediatr Neurol 1(2): 1007 (2017) 2/7
study of the bony skull, for which there is no alternative imaging technique with the same diagnostic accuracy.
Cranial deformity currently represents the main cause for pediatric neurosurgical consultation in western countries [8,9]. This deformity is mainly due to benign plagiocephaly and less often, but with potential serious implications, it may be due to craniosynostosis or other bony lesions. Clinical recognition and accurate diagnosis are key for proper management [10-12]. Referring physicians may, in selected patients, require a CT to support diagnosis and management.
We present the implementation and validation of a self-developed optimized low-dose multidetector CT (MDCT) protocol for the evaluation of the skull in children.
MATERIALS AND METHODSOur research ethics committee approved this prospective
single-institution study. Over a 42-month period (from August 2010 to February 2014), a total of 102 CT studies in 93 pediatric patients (68 boys, 25 girls) were performed. The age range was from 3 days to 6.5 years, with a mean age of 7 months. Inclusion criteria were children with cranial deformities referred for CT imaging, mainly plagiocephaly versus craniosynostosis, head bumps, skull surgeries follow-up and also diastatic fractures at risk of developing leptomeningeal cysts. No patients were excluded from the study. Their parents or legal guardians were informed and consent was obtained.
All examinations were performed with a 64-MDCT (LightSpeed VCT XT; General Electric Healthcare, Milwaukee, WI, USA). We used a self-developed CT low-dose protocol designed for the study of the skull uniformly applied to all patients [13]. Following the acquisition of a lateral topogram, an eye bismuth shield was placed and a single unenhanced helical acquisition was obtained. Technical parameters included: 80 kVp tube voltage, 50-150 mA range, 23.22 noise index (NI), 1.25 mm acquisition width, 0.625 mm interval, 40 mm total collimation width, 0.4 s rotation time, 0.984 pitch, 39.37 mm table feed per rotation, 98.4 mm/s table speed. A 16 cm FOV was used. Automatic exposure control (AEC) over the z-axis (Auto-mA, GE Healthcare) was enabled. The CT scan time duration was similar to conventional protocols. Reconstruction algorithms included bone and soft tissue. All studies were reviewed and processed, by two pediatric radiologists, on the workstation (General Electric Advantage Workstation Volume Share 2 version 4.4 software) that allows all viewing needs to globally evaluate them. For the assessment of the skull (bones and sutures), the 2004 European guidelines for multislice CT recommendations for pediatric craniofacial malformations were again taken as a reference [13,15]. These guidelines image quality criteria include: visualization (organ and structures to be visualized in the study) and critical reproduction (anatomical detail that should be clearly defined). We, once more, included a criterion of critical reproduction of the three-dimensional reconstruction of the skull [13]. Meeting image quality criteria was evaluated with a “yes” or a “no”. The diagnostic accuracy of the studies was assessed using a 3-point graded scale (1–good; 2–adequate; 3–inadequate). Orderly routine visualization of images consisted of: 1, evaluation of intracranial structures with 5-mm-thick images
reconstructed with soft tissue algorithm in brain window, at least in the axial plane; 2, evaluation of bones and sutures with 1–2 mm images reconstructed with bone algorithm in bone window settings and mean interpretation mode, at least in the axial plane; 3, MIP evaluation of thin (2–3 mm) and thick (5–50 mm) bone algorithm reconstructed images; 4, global evaluation of the skull (bones and sutures) in three-dimensional volume-rendered soft tissue algorithm reconstructed images. If necessary, it is possible to use the scan data (DICOM) with free software to produce 3D printed models for surgical planning.
The following dose indicators were used: computed tomography dose index volume (CTDIvol [mGy]), dose-length product (DLP [mGy·cm]) and effective dose (E [mSv]). The CT console displays the CTDIvol and DLP values [14]. CTDIvol and DLP are CT-specific dose descriptors that do not allow for comparisons with radiation exposure from other sources, e.g., projection radiography, nuclear medicine or natural background radiation. The only common denominator to achieve this goal is E. With E, the organ doses from a partial irradiation of the body are converted into an equivalent uniform dose to the entire body thus permitting different types of radiological examination to be directly compared [15,16]. E was obtained multiplying DLP by a conversion factor (k) adjusted to the region of body (head) and age (<1 year, k=0.011; 1–5 years, k=0.0067; 5–10, k=0.004 and >10 years, k=0.0032) [17].
Additional lifetime risk estimate of cancer from the CT examination was obtained using two online calculators: the one provided by the American Society of Radiologic Technologists (www.xrayrisk.com/index.php) and the University of Washington CT Effective Dose and Risk Estimator (http://faculty.washington.edu/aalessio/doserisk2/) [18,19]. These tools provide an estimate based on patient age and gender using the current, albeit incomplete, understanding of risk from ionizing radiation [19]. For statistical analysis of the data, we distributed the patients into three age groups: <1 year, 1-5 years and 5-10 years, according to the age range defined by k used in the calculation of E. We additionally divided the patients in two groups (<2 years and >2 years) in order to compare our results to recent publications [20,21].
The data are shown as the mean ± standard deviation, as frequency or as percentages where appropriate. For continuous variables, normality was assessed with the Kolmogorov-Smirnov test. The differences between age groups in continuous variables (CTDIvol, DLP and E) were analyzed using the Kruskal-Wallis test. All analyses were performed using SPSS 15.0 for Windows (SPSS Inc., Chicago, IL), and a value of P<0.05 was considered statistically significant.
RESULTSA total of 102 CT scans were performed in 93 pediatric
patients (85 patients with a single study, 7 patients with 2 studies and 1 patient with 3 studies). The majority of the exams were focused to the study of the skull, with merely two exams including both the skull and face, always at the request of the neurosurgeon. All studies were well tolerated. No complications occurred in any of the patients.
The studies were demanded, in decreasing order, from the
CentralBringing Excellence in Open Access
Blanco-Lobato et al. (2017)Email:
JSM Pediatr Neurol 1(2): 1007 (2017) 3/7
Department of Neurosurgery (52%), Pediatrics (42%) and Rehabilitation (6%). The most common clinical indication for CT requisition, by far, was to evaluate cranial deformities, mainly to differentiate significant deformational plagiocephaly from craniosynostosis, less frequently head bumps, skull surgeries follow-up and for the study of potential development of post-fracture leptomeningeal cysts. 79 out of the 102 CT scans were initial diagnostic CT studies and 23 were control exams. Of these 23 control exams, 4 patients had a CT scan performed prior to this CT study. Findings on initial diagnostic CT studies included: 40 parieto-occipital plagiocephaly (50.6%), 5 sagittal suture synostosis (6.33%), 5 cephalohematomas (6.33%), 4 metopic suture synostosis (5.1%), 2 bifid craniums (2.5%), and one of the following: universal craniosynostosis, bilateral coronal suture synostosis, unilateral coronal suture synostosis, dolichocephaly without sutural synostosis, dermoid cyst, enlarged bilateral parietal foramina, sinus pericranii, eosinophilic granuloma and a incidental linear cranial fracture (1.27% each). 14 studies were considered normal (17.7%). Four patients were syndromic; three of them had a disorder of suture closure (one Crouzon syndrome patient with bilateral coronal synostosis, a second patient with Muenke syndrome and a unilateral coronal synostosis and a third one with metopic suture synostosis and genetic diagnosis pending) and, finally, a fourth patient with deletion 5q14-q15 presenting dolichocephaly without synostosis. Out of the 23 control exams, 4 were follow-up studies (1 craniosynostosis and 3 diastatic fractures at risk of becoming growing skull fractures) while 19 were postoperative controls (13 surgically corrected craniosynostosis, 1 eosinophilic granuloma, 3 dermoid cysts and 2 leptomeningeal cyst).
This low dose protocol is tailored to study the cranium and does not allow accurate evaluation of intracranial structures due to image noise. However, it was possible to grossly visualize findings such as benign enlargement of the subarachnoid spaces, one patient with severe cerebral atrophy and universal craniosynostosis, and even an area of encephalomalacia, confirmed by MRI, in a patient with bifid cranium.
The diagnostic accuracy of the studies was concordantly considered good in 100 out of 102 (98%). The quality of the exams is shown with the following examples: posterior plagiocephaly, sagittal sutural synostosis, unilateral and bilateral coronal synostosis, metopic synostosis, universal synostosis, postoperative CT scan of a repaired sagittal synostosis, bilateral calcified parietal cephalohematomas and a bifid cranium (Figures 1-9). Only two studies were considered inadequate for diagnosis and it was necessary to repeat them. This was because of patient motion during the acquisition and not due to technical factors or limitations of the low-dose CT protocol technique.
The dosimetric values achieved with this low-dose protocol and their distribution per age groups are shown in Table 1. The mean dose values obtained in children up to 1 year of age were: CTDIvol 1.9 mGy, DLP 32.4 mGy·cm and E 0.36 mSv. The 2004 European guidelines for multislice CT recommended dosimetric reference levels for head CT in this age group scans are: CTDIvol 31 mGy, DLP 333 mGy·cm and E 2.6 mSv [14]. This translates into a 7-16 times mean dose reduction. The minimum values attained in this age group were CTDIvol 1.05 mGy, DLP 15.5 mGy·cm and E 0.17 mSv. In other words, up to a maximum of 30 times dose reduction. The guidelines next study group refers to children between the ages of 4 and 6 years with the following recommended dose values: CTDIvol 47 mGy, DLP 374 mGy·cm and E 1.8 mSv [14]. In our study, the comparable 1-5 years-old group mean values obtained were: CTDIvol 2.1 mGy, DLP 38.5 mGy·cm and E 0.26 mSv. This translates into a 7-22 times mean dose reduction. The minimum values achieved in this age group were CTDIvol 1.7 mGy, DLP 29.1 mGy·cm and E 0.2 mSv. In other words, up to a maximum of 28 times dose reduction in regards to the same guidelines.
Additional lifetime cancer risk achieved a value below two decimals on both calculators. Therefore, a figure close to 0, a significant value compared with the calculated value of 0.04 from the references levels standard head CT protocol [13,14].
DISCUSSIONImaging studies are required to characterize syndromic
Table 1: Distribution of dosimetric values (CTDIvol, DLP and E) per age groups.
Age groups n Mean SD Min. Max. p-value
CTDIvol(mGy)
o-1 years 70 1,90 0,42 1,05 3,12
0,0081-5 years 27 2,10 0,35 1,70 3,00
5-10 years 5 2,30 0,31 2,10 2,90
Total 102 2,00 0,41 1,05 3,10
DLP(mGy.cm)
o-1 years 70 32,40 8,60 15,50 61,9
0,0011-5 years 27 38,50 7,50 29,10 59,10
5-10 years 5 43,00 5,40 36,90 51,00
Total 102 34,60 8,80 15,50 61,90
E(mSv)
o-1 years 70 0,36 0,09 0,17 0,68
<0,0011-5 years 27 0,26 0,05 0,20 0,40
5-10 years 5 0,17 0,02 0,15 0,20
Total 102 0,32 0,10 0,15 0,65

CentralBringing Excellence in Open Access
Blanco-Lobato et al. (2017)Email:
JSM Pediatr Neurol 1(2): 1007 (2017) 4/7
Figure 1 Right parieto-occipital positional plagiocephaly in a 10-month-old boy. Cranial CT: (a) axial 2-mm thick bone algorithm image in bone window and (b) axial thick MIP reconstruction image.
Figure 2 Dolichocephaly due to sagittal synostosis in a 4-day-old boy. Cranial CT: (a) coronal MPR and (b) axial 2-mm thick bone algorithm images in bone window; (c) axial thick MIP and (d) three-dimensional reconstruction superolateral view.
Figure 3 Right unilateral coronal synostosis in a 4-month-old girl. Cranial CT: (a) axial thick MIP and (b) three-dimensional reconstruction frontal superior view.
Figure 4 Bilateral coronal synostosis in a 4-day-old boy. Cranial CT: (a) coronal thick MIP and (b) three-dimensional reconstruction frontal view. Incidentally noted a bregmatic bone.
Figure 5 Trigonocephaly due to metopic synostosis in a 21-month-old boy. Cranial CT: (a) axial thick MIP and (b) three-dimensional reconstruction superior view.
Figure 6 Universal synostosis due to parenchymal atrophy in a 5-month-old boy. Cranial CT: Cranial CT: (a) axial thick MIP reconstruction image, (b) axial 5-mm thick image in brain window, note the parenchymal atrophy, (c) three-dimensional reconstruction superior and posterolateral views.
CentralBringing Excellence in Open Access
Blanco-Lobato et al. (2017)Email:
JSM Pediatr Neurol 1(2): 1007 (2017) 5/7
craniosynostosis and, more commonly, for the evaluation of children with significant or worsening cranial deformity that may be due to plagiocephaly versus craniosynostosis and even other skull lesions such as cephalohematoma. Imaging studies are fundamental, in clinically selected patients, to confirm the suspected diagnosis, for therapy planning (conservative or surgical) and postoperative follow-up. Plain radiographs have their inherent limitations, being particularly inaccurate in children under 3 months of age due to the low mineralization of the cranium [11,12,22]. MDCT with its isotropic volumetric data sets and post-processing capabilities is an excellent, if not the best, tool to evaluate the skull [12,20,23-28]. Therefore, and following the ALARA principle, optimization of CT studies for evaluation of the skull is in order. Firstly, we developed an optimized a low-dose cranial CT protocol for the study of the bony calvarium in children imaged for head deformity [13]. In the current study, we present the implementation and validation of the attained protocol uniformly applied to a large group of pediatric patients. A substantial dose reduction was accomplished while maintaining an acceptable diagnostic image quality, not only by the radiologists standards but with high overall clinician’s satisfaction with both the studies image quality and diagnostic utility, along the lines of recently published work [1]. In keeping with the ALARA principle, decision was made to perform focused head CT studies in the majority of patients (98%), reserving the lengthier craniofacial CT for a minority of patients, always at the clinical judgment of the referring physician. A focused head CT is sufficient for the evaluation of most of these patients and spares them from the extra facial irradiation.
Significantly reduced dosages, as mentioned in the Results section, were achieved. In this regard, a recent publication refers to their cranial CT full and low-dose protocols with a 64-MDCT scanner of the same make and model of ours. In their more optimized group (quarter-dose) they report a mean CTDIvol of 5.86 mGy in the <2 years group and 8.86 mGy in the >2 years group [20]. In an editorial commentary, in the same journal issue, Mody and Slovis claim a CTDIvol of 2.3 mGy and 2.5 mGy for these age groups [21]. In our study, we obtained lesser values with a mean CTDIvol of 1.93 mGy for the <2 years group and 2.3 mGy for the >2 years group. Also mentioned in the last two referred reports, the downside of these low-dose CT protocols is the limited soft-tissue evaluation. Our low-dose protocol is intended for the study of the bones and sutures, nevertheless and as previously mentioned in the Results section; it allows gross evaluation of intracranial structures such as size and shape of the ventricular system, brain parenchyma, midline deviation and extracerebral spaces. A minority of patients, such as children with syndromic synostosis and others requiring parenchymal evaluation should undergo complementary preoperative MRI and MR venography. This combined approach achieves considerable radiation reduction to this vulnerable population [20,21] and is probably more cost-efficient. Given that the few pediatric head MDCT reference levels published involve the assessment of intracranial structures and require a low NI with significantly higher dose values [14,29], we would suggest that future pediatric MDCT guidelines should include a separate category of low-dose MDCT for the study of the pediatric skull.
The overall lifetime risk of developing an invasive cancer is
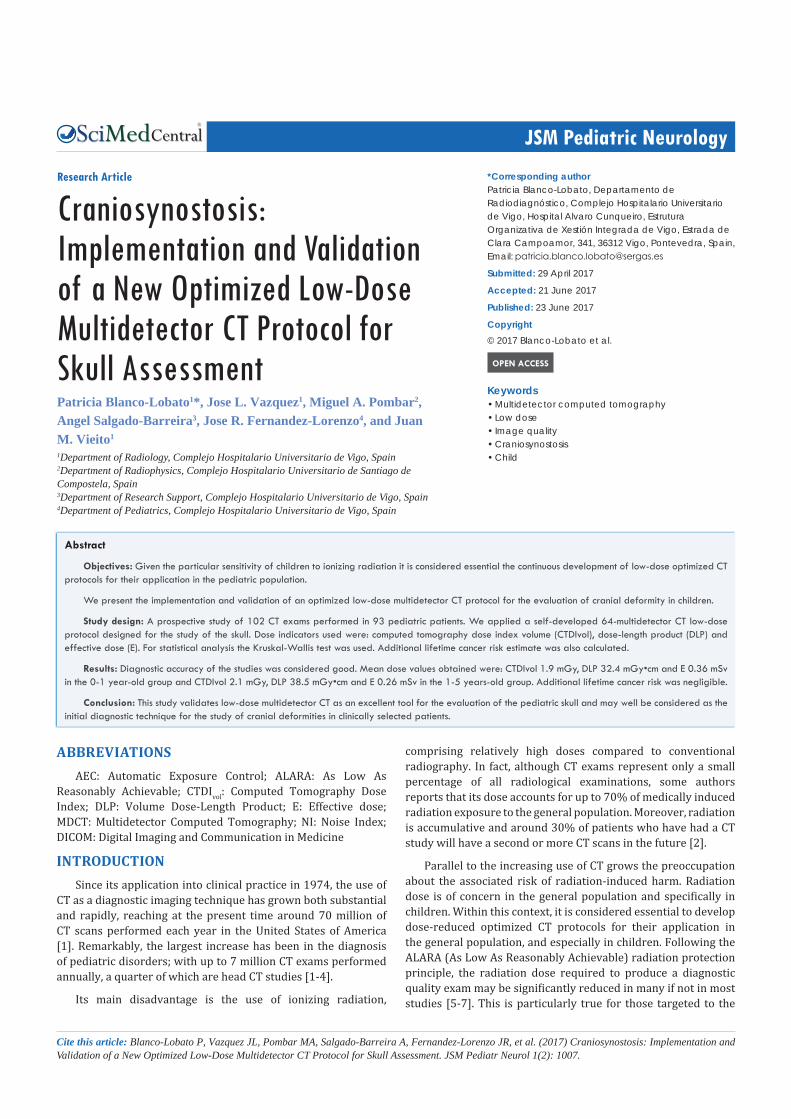
Figure 7 Sagittal synostosis in a 9-month-old boy and postoperative CT scan. Cranial CT: (a) and (b) axial thick MIP reconstruction images, (c) and (d) three-dimensional reconstruction posterolateral views.
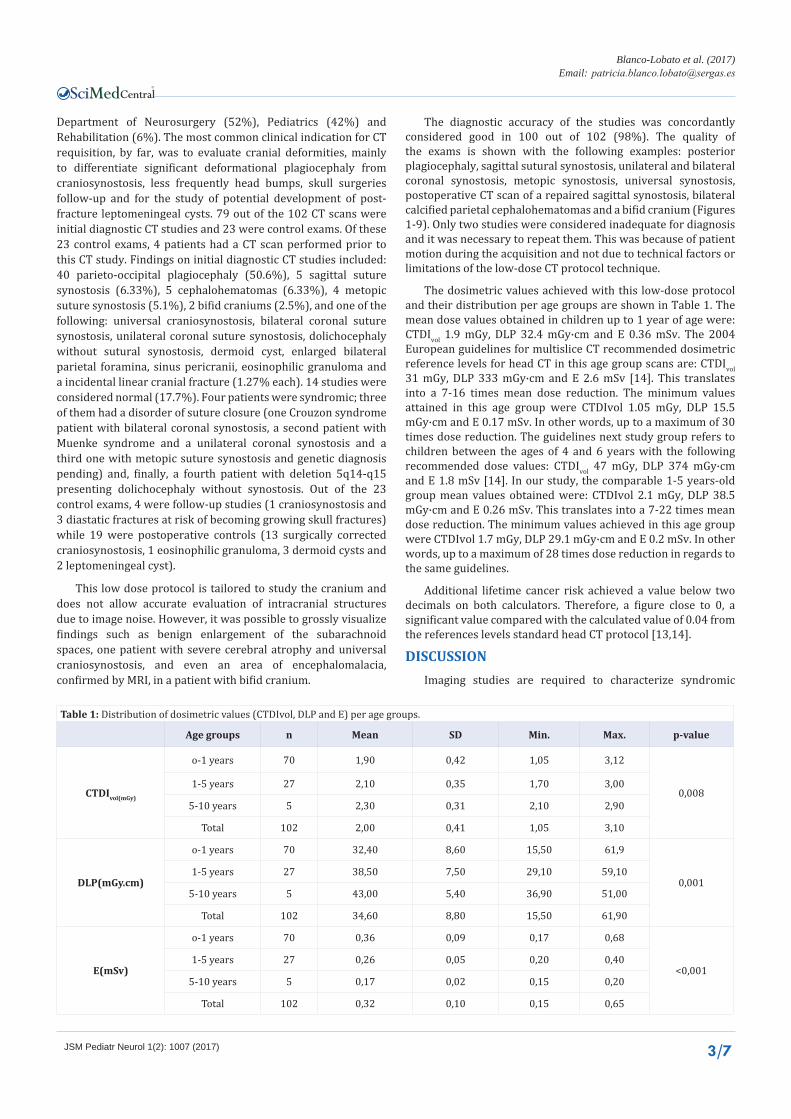
Figure 8 Bilateral parietal calcified cephalohematoma in a 3-month-old boy. Cranial CT: (a) coronal MPR 2-mm thick bone algorithm image in bone window and (b) three-dimensional reconstruction posterolateral view.
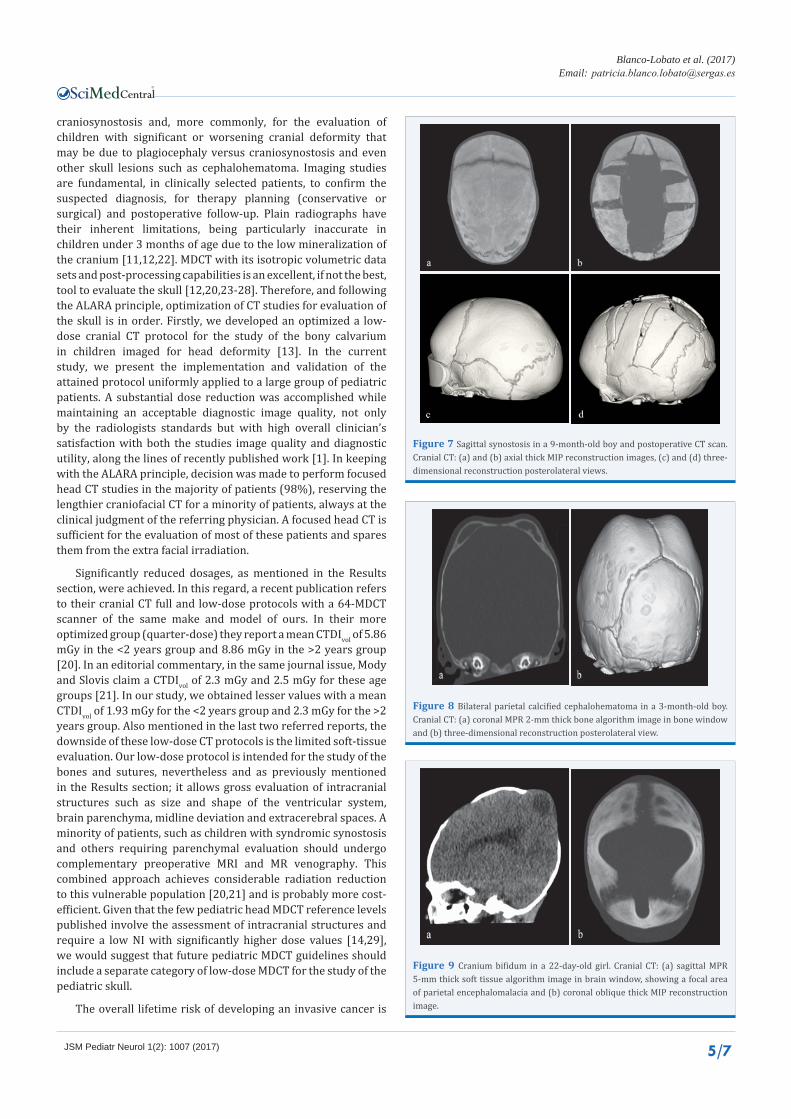
Figure 9 Cranium bifidum in a 22-day-old girl. Cranial CT: (a) sagittal MPR 5-mm thick soft tissue algorithm image in brain window, showing a focal area of parietal encephalomalacia and (b) coronal oblique thick MIP reconstruction image.

CentralBringing Excellence in Open Access
Blanco-Lobato et al. (2017)Email:
JSM Pediatr Neurol 1(2): 1007 (2017) 6/7
37.5% for women and 44.9% for men. These figures are averages; they do not take into consideration individual risk factors such as lifestyle or genetics. The majority of cancers occur later in life and the average lifetime risk of dying from cancer is 25%. These rough estimates of cancer risk are derived from interpolation of factors described in the BEIR VII report [18,19,30]. Regarding cancer risk estimate, in the present study the specific organ risk includes the brain and the proportional part of the bone with the bone marrow. In neonates and young children 25-30% of the active bone marrow is present in the skull, whereby in adults is only 5-10%. Recent studies have shown a three-fold increased risk of leukemia and brain tumors in children exposed to head CT scan with cumulative doses of 50-60 mGy [31]. Furthermore, other studies conclude that even intellectual development may be adversely affected in the infant brain exposed to ionizing radiation doses greater than 100 mGy [32]. Therefore, high priority should be given to dose-reduction measures for head CT in infants [33]. In this regard, in the present study the mean dose for a single CT exam were: 1.9 mGy for the children under 1 year of age and 2.1 mGy for the 1-5 year-old group. The additional cancer risk from every single CT study calculated in our exams was close to 0.
This CT protocol may be easily adapted to other MDCT makes and models [13]. Application of newer hardware and software dose reduction improvements such as adaptive collimation, iterative reconstructions, axial volumetric data acquisition, lower kVp, improved beam filters and software upgrades, etc. will translate in even greater dose savings [13,34].
The main limitation of our study is that all exams were performed with our low-dose head CT protocol. We did not perform a simultaneous low-dose and standard head CT in the same patient. This would have allowed comparison between the two protocols of image quality criteria and critical reproduction, including the three-dimensional reconstruction, at the cost of additional radiation for our pediatric patients, completely unacceptable by current standards.
CONCLUSIONThis study validates a simple, adaptive, easy to use, low-
dose MDCT protocol for the evaluation of the pediatric skull with good diagnostic quality. Low-dose MDCT is useful and may even obviate the need for plain radiographs, in clinically selected patients, for the study of skull deformities.
REFERENCES1. Morton RP, Reynol RM, Ramakrishna R, Levitt MR, Hopper RA, Lee
a, et al. Low-dose head computed tomography in children: a single institutional experience in pediatric radiation risk reduction. J Neurosurg Pediatrics. 2013; 12: 406-410.
2. Shah NB, Platt SL. ALARA: is there a cause for alarm? Reducing radiation risks from computed tomography scanning in children. Curr Opin Pediatr. 2008; 20: 243-247.
3. Didier RA, Kuang AA, Schwartz DL, Selden NR, Stevens DM, Bardo DME. Decreasing the effective radiation dose in pediatric craniofacial CT by changing head position. Pediatr Radiol. 2010; 40: 1910-1917.
4. Strauss KJ, Goske MJ, Kaste SC, Bulas D, Frush DP, Butler P, et al. Image gently: ten steps you can take to optimize image quality and lower CT dose for pediatric patients. AJR Am J Roentgenol. 2010; 194: 868-873.
5. Mulkens T, Salgado R, Bellinck P. Dose optimization and reduction in CT of the brain and head and neck region. In: Tack D, Kalra MK, Gevenois PL, editors. Radiation dose from multidetector CT, 2nd ed. Berlin Heildelberg: Springer-Verlag. 2012; 281-306.
6. Smith AB, Dillon WP, Lau BC, Gould R, Verdun FR, Lopez EB, et al. Radiation dose reduction strategy for CT protocols: successful implementation in neuroradiology section. Radiology. 2008; 247: 499-506.
7. Udayasankar UK, Braithwaite K, Arvaniti M, Tudorascu D, Small WC, Little S, et al. Low-dose nonenhanced head CT protocol for follow-up evaluation of children with ventriculoperitoneal shunt: reduction of radiation and effect on image quality. AJNR Am J Neuroradiol. 2008; 29: 802-806.
8. Robinson S, Proctor M. Diagnosis and management of deformational plagiocephaly. J Neurosurg Pediatr. 2009; 3: 284-295.
9. Esparza J, Hinojosa J, Munoz MJ, Romance A, Garcia-Recuero I, Munoz. Positional plagiocephaly. Diagnosis and treatment. Neurocirugia (Astur). 2007; 18: 457-467.
10. Kirmi O, Lo SJ, Johnson D, Anslow P. Craniosynostosis: a radiological and surgical perspective. Semin Ultrasound CT MR. 2009; 30: 492-512.
11. Fernbach SK. Craniosynostosis 1998: concepts and controversies. Pediatr Radiol. 1998; 28: 722-728.
12. Pattisapu JV, Gegg CA, Olavarria G, Johnson KK, Ruiz RL, Costello BJ. Craniosynostosis: diagnosis and surgical management. Atlas Oral Maxillofac Surg Clin North Am. 2010; 18: 77-91.
13. Vazquez JL, Pombar MA, Pumar JM, del Campo VM. Optimised low-dose multidetector CT protocol for children with cranial deformity. Eur Radiol. 2013; 23: 2279-2287.
14. Bongartz G, Golding SJ, Jurik AG, Leonardi M, van Meerten EvP, Geleijns J, et al. European guidelines for multislice computed tomography. European Commission 2004; Contract number FIGM-CT2000-20078-CT-TIP.
15. Nagel HD. CT parameters that influence the radiation dose. In: Tack D, Gevenois PA, eds. Radiation dose from adult and pediatric multidetector computed tomography. Berlin: Springer. 2007; 51-79.
16. Huda W, Ogden KM. Computing effective doses to pediatric patients undergoing body CT examinations. Pediatr Radiol. 2008; 38: 415-423.
17. Valentin J. Managing patient dose in multi-detector computed tomography (MDCT). ICRP Publication 102. Ann ICRP. 2007; 37: 1-79.
18. Hanley M, Koonce JD, Bradshaw ML. www.X- rayRisk.com: an online calculator for cancer risk. J Am Coll Radiol. 2009; 6: 475-476.
19. Alessio AM, Phillips GS. A pediatric CT dose and risk estimator. Pediatr Radiol. 2010; 40: 1816-1821.
20. Badve CA, Mallikarjunappa MK, Iyer RS, Ishak GE, Khanna. Craniosynostosis: imaging review and primer on computed tomography. Pediatr Radiol. 2013; 43: 728-742.
21. Mody SS, Slovis TL. Craniosynostosis—another look. Pediatr Radiol. 2013; 43: 657-658.
22. Kirks DR, Griscom NT. Practical pediatric imaging: diagnostic radiology of infants and children. 3rd edn. Philadelphia: Lippincott- Raven; 1998.
23. Kotrikova B, Krempien R, Freier K, Muhling J. Diagnostic imaging in the management of craniosynostoses. Eur Radiol. 2007; 17: 1968-1978.
24. Benson ML, Oliverio PJ, Yue NC, Zinreich SJ. Primary craniosynostosis: imaging features. AJR Am J Roentgenol. 1996; 166: 697-703.

CentralBringing Excellence in Open Access
Blanco-Lobato et al. (2017)Email:
JSM Pediatr Neurol 1(2): 1007 (2017) 7/7
Blanco-Lobato P, Vazquez JL, Pombar MA, Salgado-Barreira A, Fernandez-Lorenzo JR, et al. (2017) Craniosynostosis: Implementation and Validation of a New Optimized Low-Dose Multidetector CT Protocol for Skull Assessment. JSM Pediatr Neurol 1(2): 1007.
Cite this article
25. Medina LS, Richardson RR, Crone K. Children with suspected craniosynostosis: a cost-effectiveness analysis of diagnostic strategies. AJR Am J Roentgenol. 2002; 179: 215-221.
26. Pilgram TK, Vannier MW, Hildebolt CF, Marsh JL, McAlister WH, Shackelford GD, et al. Craniosynostosis: image quality, confidence, and correctness in diagnosis. Radiology. 1989; 173: 675-679.
27. Vannier MW, Hildebolt CF, Marsh JL, Pilgram TK, McAlister WH, Shackelford GD, et al. Craniosynostosis: diagnostic value of three-dimensional CT reconstruction. Radiology. 1989; 173: 669-673.
28. Álvarez Zallo N, Sanchez-Carpintero R. 3D-CT in the diagnosis of craniosynostosis. Ann Pediatr (Barc). 2010; 72: 355-356.
29. Brisse H. Guide des Procédures Radiologiques SFR / INRS Scanographie Pédiatrique. 2006.
30. National Research Council. Health Risks from Exposure to Low Levels of Ionizing Radiation: BEIR VII Phase 2. Washington DC: The National Academies Press. 2006.
31. Pearce MS, Salotti JA, Little MP, McHugh K, Lee C, Kim KP, et al. Radiation exposure from CT scans in childhood and subsequent risk of leukaemia and brain tumours: a retrospective cohort study. Lancet. 2012; 380: 499-505.
32. Hall P, Adami HO, Trichopoulos D, Pedersen NL, Lagiou P, Ekborn A, et al. Effect of low doses of ionising radiation in infancy on cognitive function in adulthood: Swedish population based cohort study. BMJ. 2004; 328: 19-21.
33. Fearon T, Vucich J. Normalized pediatric organ-absorbed doses from CT examinations. AJR Am J Roentgenol. 1987; 148: 171-174.
34. Erns CW, Hulstaert TL, Belsack D, Buls N, Van Gompel G, Nieboer KH, et al. Dedicated sub 0.1 mSv 3DCT using MBIR in children with suspected craniosynostosis: quality assessment. Eur Radiol. 2016; 26: 892-899.