craniovertebral junction anomalies
TRANSCRIPT

CRANIOVERTEBRALJUNCTION
CRANIOVERTEBRAL JUNCTION
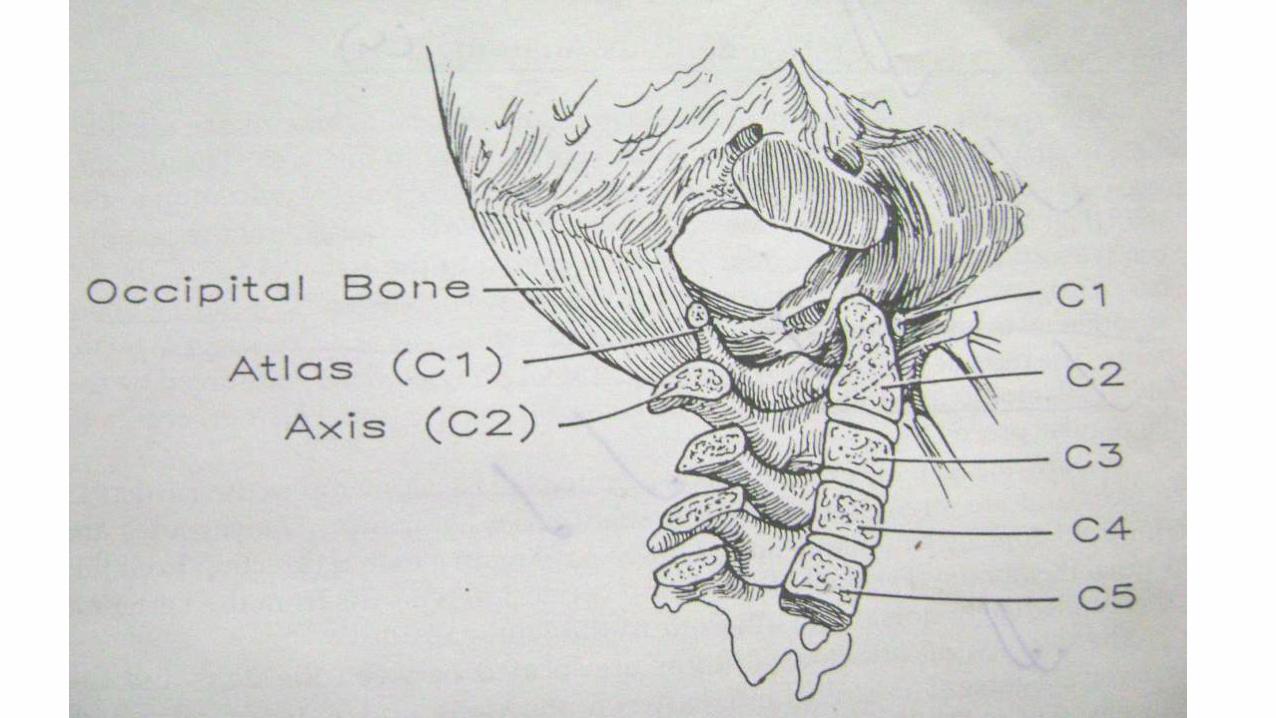
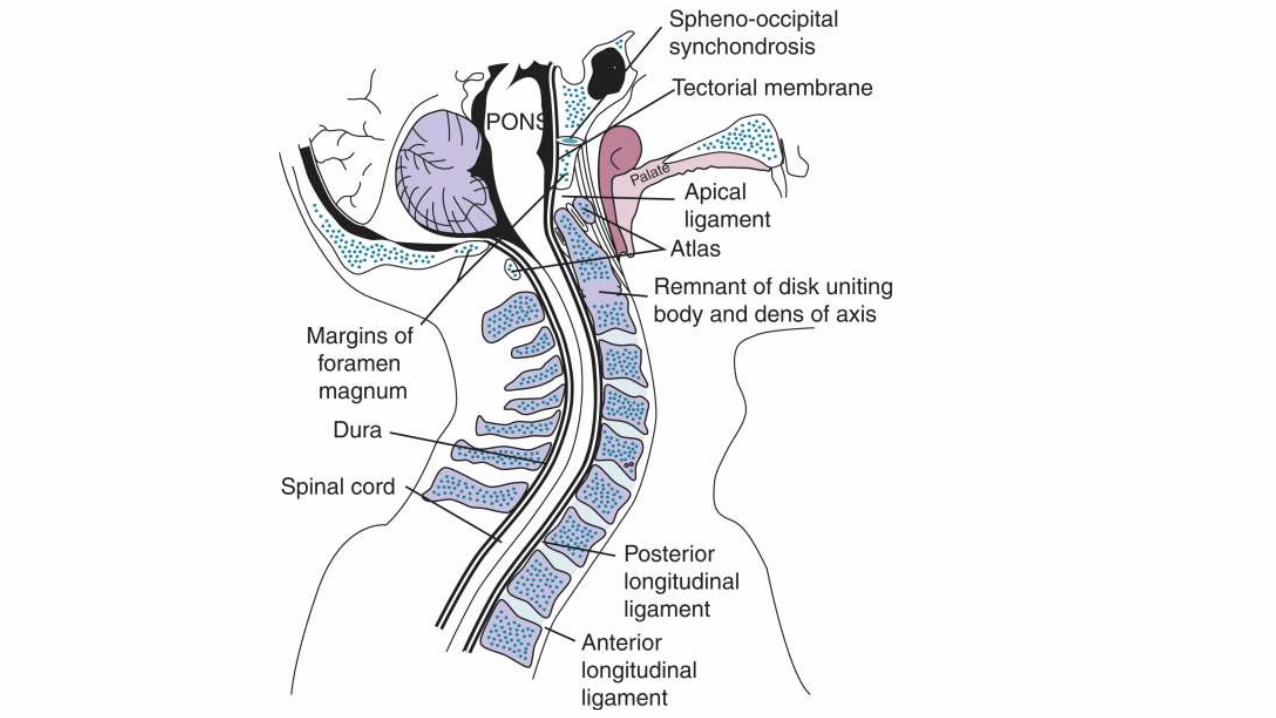
• The craniovertebral (or craniocervical) junction(CVJ) is a collective term that refers to the occiput(posterior skull base), atlas, axis, and supporting ligaments.
• It is a transition zone b/w a mobile cranium & spinal column.
• It encloses the soft tissue structures of the cervicomedullaryjunction (medulla, spinal cord, and lower cranial nerves).
Contents
• Embyology
• Anatomy of CV junction
• Classification of CV Anomalies
• Anatomical and radiological aspects
• Specific anomalies – AA dislocation, Dens dysplasia, KFS
• ACM, Syrinx
• Clinical features
• Management
EMBRYOLOGY & DEVELOPMENT OF THE CVJ
• Development of the cartilaginous cranium & the adjacent structures begins during the early weeks of intrauterine life.
• 2ndGestational week: Mesoderm cells condense in the midline to form notochordal process.
• 3rdGestational week:
-notochordal process invaginates in b/w ecto& endoderm to form notochord.
-dorsal ectoderm thickens to form neural groove which folds, fuses, & becomes neural tube.
EMBRYOLOGY & DEVELOPMENT OF THE CVJ
Between 3rd& 5thweek:
• -part of mesoderm which lies on either side of notochord (Paraxial mesoderm) gives rise to somites(Segmentation).
• -total 42 somites form at 4thweek.
• -ventromedial portion of somite is k/a sclerotome which forms the vertebral bodies.
• -each sclerotome differentiates into a cranial, loosely arranged portion and a caudal compact portion by a fissure k/a “Fissure of von Ebner”
EMBRYOLOGY & DEVELOPMENT OF THE CVJ
• Mesenchymal cells of the fissure condense around the notochord to form the intervertebral disc.
• Notochord disappears at the vertebral bodies, but persist as nucleus pulposus at disc.
• The first four sclerotomes do not follow this course & fuse to form the occipital bone.
• This membraneous stage is formed by stages of chondrification & ossification.
• Out of 4 occipital sclerotomes the first 2 form basiocciput, the III Jugular tubercles and the IV (Proatlas) form parts of foramen magnum, atlas and axis
APPLICATIONS
• Dysplasia of the occipital segments may flatten the clivus-platybasia.
• When the basiocciput and rim of foramen magnum are underdeveloped, the odontoid and arch of atlas may invaginate- Basilar invagination.
• The proatlas may develop into separate vertebrae -Occipital vertebra, hypochondral bow of proatlas may persist to gain attachment to the atlas, clivusor even to the apical segment of the dens -responsible for anterior cervicomedullarycompression

APPLICATIONS
• If the posterior segment of the proatlas fails to fuse with the atlas, a rare anomaly termed bipartite articular facets occurs, may result in horizontal instability of the OA joint.
• Bicornuate dens : dens body may fail to fuse in utero resulting in a V-shaped cleft found radiographically at birth , rare in adults.
• Failure of segmentation b/w the axis & the 3rd cervical vertebra involves both the ant. & the post. vertebral segments, associated with other anomalies like Klippel–Feil syndrome.
ANATOMY OF CVJ (ARTICULAR)
• Upper surfaces of C1 lateral masses are cup-like or concave which fit into the ball & socket configuration, united by articular capsules surr. the AO joint & by the ant. & post. AO membranes.
4 synovial joints b/w atlas & axis –
• 2 median –front & back of dens (Pivot variety)
• 2 lateral –b/w opposing articular facets (Plane variety)
• Each joint has its own capsule & synovial cavity.
ANATOMY OF CVJ(LIGAMENTOUS)
Principal stabilizing ligaments of C1 -
• -Transverse atlantal ligament
• -Alar ligaments
Secondary stabilizing ligaments of CVJ are more elastic & weaker than the primary ligaments.
• -Apical ligament
• -Anterior & posterior A-O membranes
• -Tectorial membrane
• -Ligamentum flavum
• -Capsular ligaments
ANATOMY OF CVJ (MUSCLES)
• Muscles have only a minor role related to CVJ stabilization & do not limit the movements of the joints.
• Their principal function is one of initiating & maintaining movement at the CVJ.
ANATOMY OF CVJ (MUSCLES)
• Muscles have only a minor role related to CVJ stabilization & do not limit the movements of the joints.
• Their principal function is one of initiating & maintaining movement at the CVJ.
ANATOMY OF CVJ (NEURAL)
• Neural structures related to CVJ are –
• Caudal portion of brainstem (Medulla)
• Cerebellum
• Fourth ventricle
• Rostral part of spinal cord
• Lower cranial & upper cervical nerves
• In cerebellum, only the tonsils, biventral lobules & the lower part of the vermis (nodule, uvula & pyramid) are related to CVJ.
• Biventrallobule is located above the lateral part of FM & the tonsils lie above the posterior edge.
ANATOMY OF CVJ (NEURAL)
• CRANIAL NERVES :
• Lower four cranial N. are closely related to CVJ.
• 9th& 10thcranial N arise from the medulla in the groove b/w the inferior olivary nucleus & the inferior cerebellarpeduncle.
• 9th& 10thN are separated by a dural sheath which separate these nerves as they penetrate the dura to enter the jugular foramen.
• The accessory N is the only cranial N that passes through the FM.
ANATOMY OF CVJ (NEURAL)
• SPINAL NERVE ROOTS:
• The C1, C2, and C3 nerves, distal to the ganglion, divide into dorsal and ventral rami.
• The first cervical nerve located just below the foramen magnum.
• The C1 ventral root (SUBOCCIPITAL NERVE) is composed of four to eight rootlets that joined and coursed laterally and supplies the rectuscapitislateralis.
ANATOMY OF CVJ (LYMPHATICS)
• The lymphatic drainage of the O-A-A joints is primarily into the retropharyngeal LN & then into the deep cervical chain.
• These LN’s also drain the nasopharynx & hence retrograde infection may affect the synovial lining of the CVJ complex with resultant neck stiffness & instability.
ANATOMY OF CVJ (ARTERIAL)
The major arteries related to CVJ are :-
• Vertebral arteries
• Posteroinferior cerebellar arteries (PICA)
• Meningeal branches of the vertebral
• External and internal carotid arteries.
ANATOMY OF CVJ (VENOUS)
The venous structures in the region of the FM are divided into three groups:
• Extradural veins(extraspinal& intraspinalpart)
• Intradural (neural) veins, &
• Dural venous sinuses( superior petrosal, marginal & occipital)
The three groups anastomose through bridging and emissary veins.
Classification
I. Bony AnomaliesA. Major Anomalies
1. Platybasia
2. Occipitalization
3. Basilar Invagination
4. Dens Dysplasia
5. Atlanto- axial dis.
B. Minor Anomalies1. Dysplasia of Atlas2. Dysplasia of
occipital condyles, clivus, etc.
II. Soft Tissue anomalies1. Arnold-Chiari Malformation2. Syringomyelia/ Syringobulbia
INVESTIGATIONS
• The investigations which are invaluable in the diagnosis of cranio-vertebral anomalies are enlisted below:-
1) X Rays
• Antero-posterior view
• Lateral view
• Open mouth view
2) Stress X-Rays
3) Tomogram
4) Myelogram
5) Ventriculogram
6) Angiography
7) CT Scan
X-RAYS
• Conventional antero-posterior and lateral views will reveal the presence and type of cranio-vertebral anomaly.
• It will show whether the odontoid is present or absent and also the integrity of the rings of atlas and axis.
• Block vertebrae and occipitalisation of atlas are also visualised.
• The open mouth view shows hypoplastic odontoid, osodontoideum or ossiculum terminale with clarity.
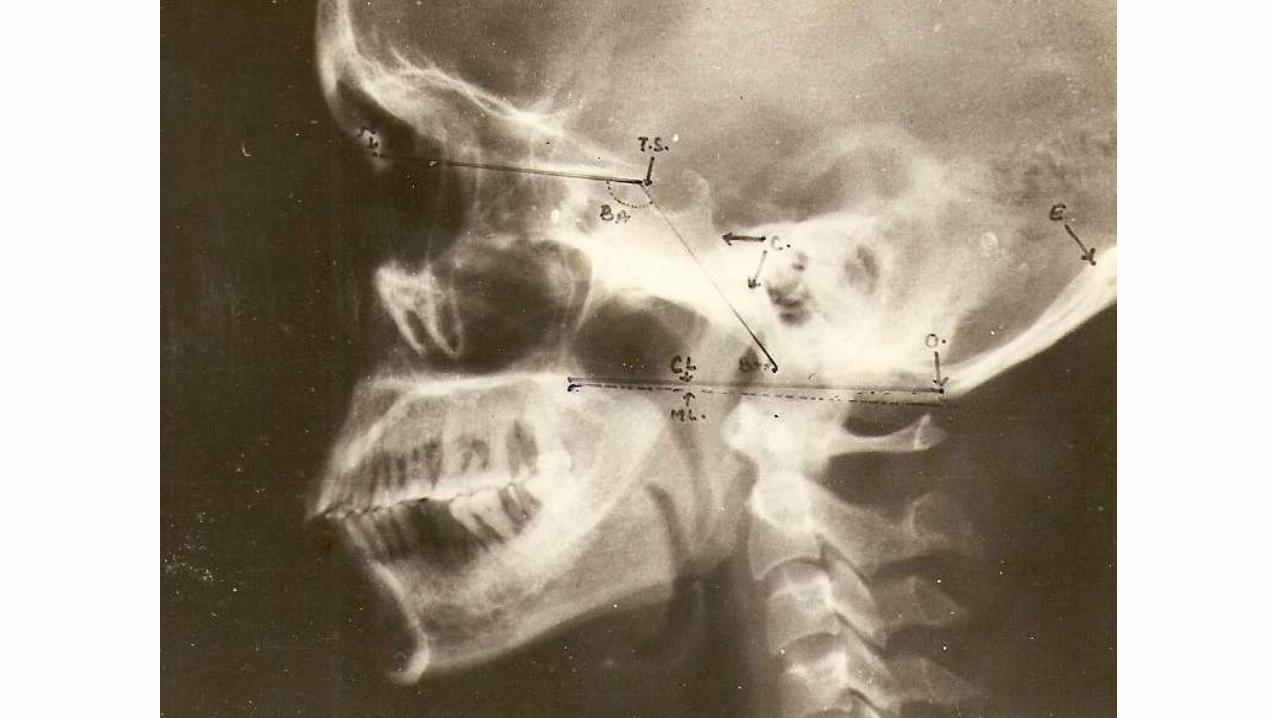
LATERAL CRANIOMETRY
• determine basilar invagination, which is an upward movement of the base of the skull in the region of the foramen magnum.
• It is measured by the intracranial extension of the tip of the odontoid process.
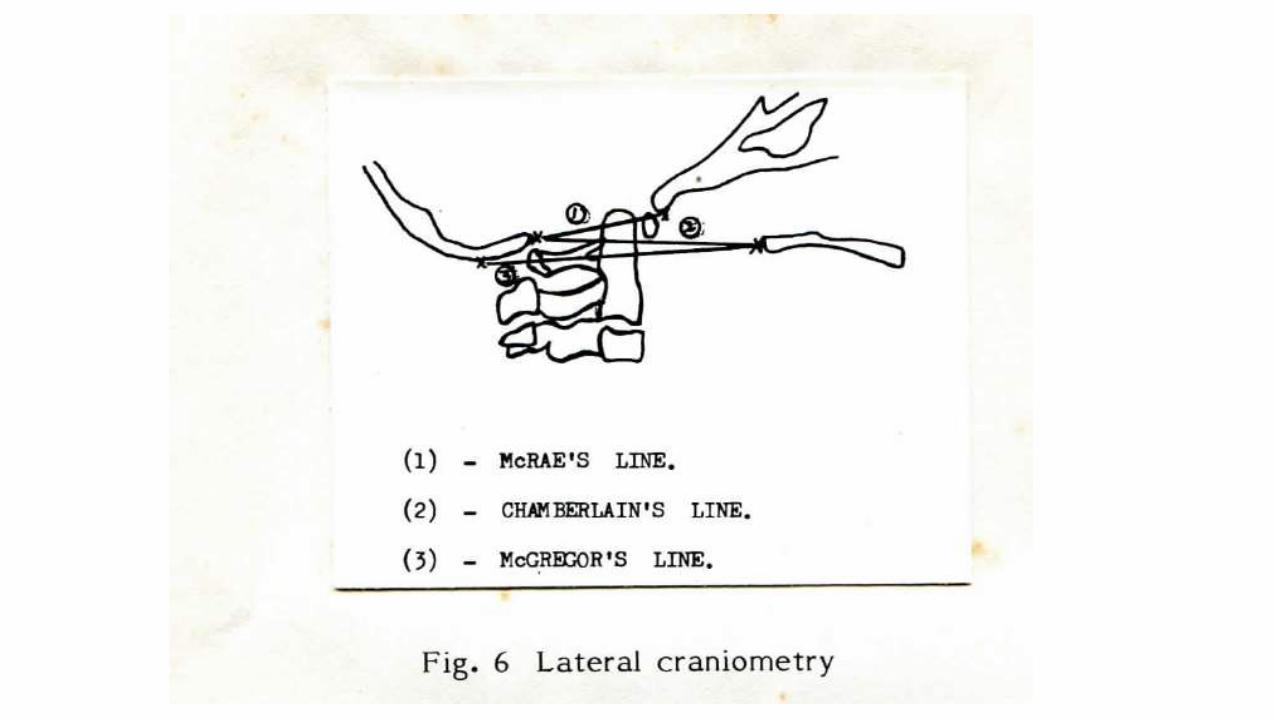
• Chamberlain's line (1939) is drawn from the posterior lip of the foramen magnum to the dorsal margin of the hard palate.
• Intracranial projection of up to one third of the length of the odontoid is normal.
• McGregor's line (1948) is drawn from the upper surface of the posterior edge of the hard palate to the most caudal point of the occipital curve of the skull.
• The tip of the odontoid normally does not extend more than 4.5 mm above this line.

• McRae's line (1953) defines the opening of the foramen magnum.
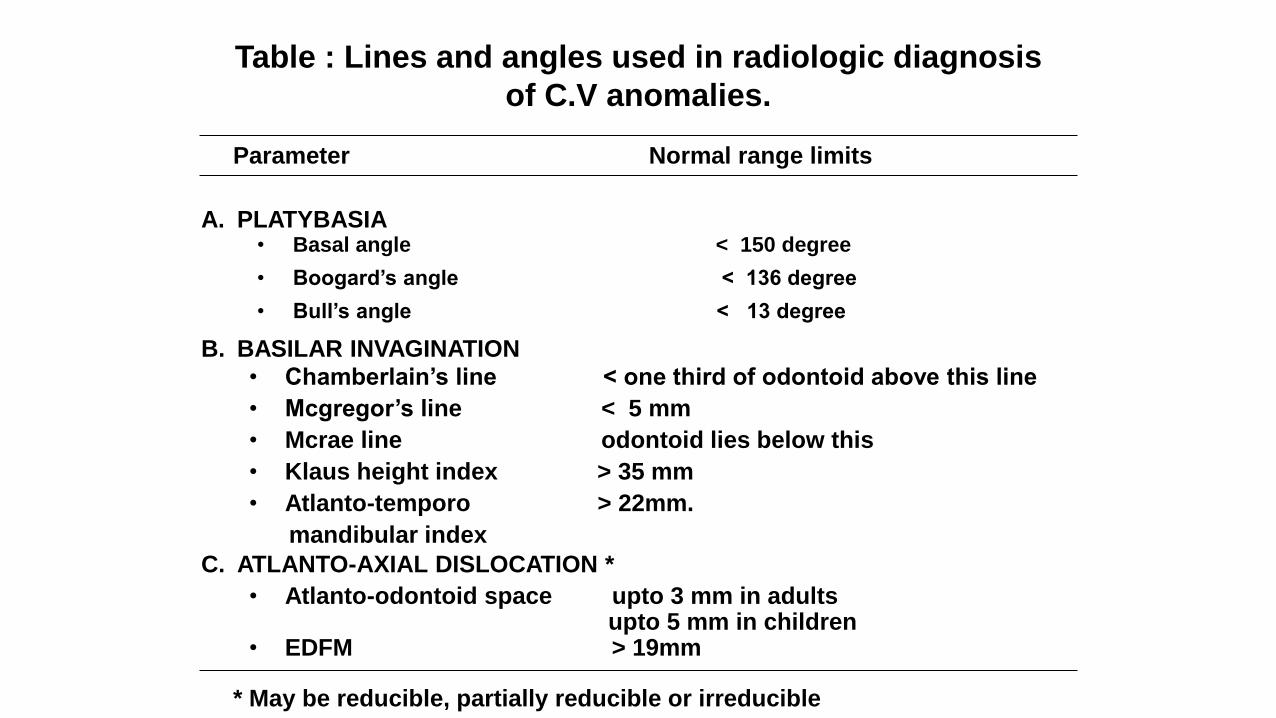
Table : Lines and angles used in radiologic diagnosis
of C.V anomalies.
Parameter Normal range limits
A. PLATYBASIA
B. BASILAR INVAGINATION
C. ATLANTO-AXIAL DISLOCATION *
• Basal angle < 150 degree
• Boogard’s angle < 136 degree
• Bull’s angle < 13 degree
• Chamberlain’s line < one third of odontoid above this line
• Mcgregor’s line < 5 mm
• Mcrae line odontoid lies below this
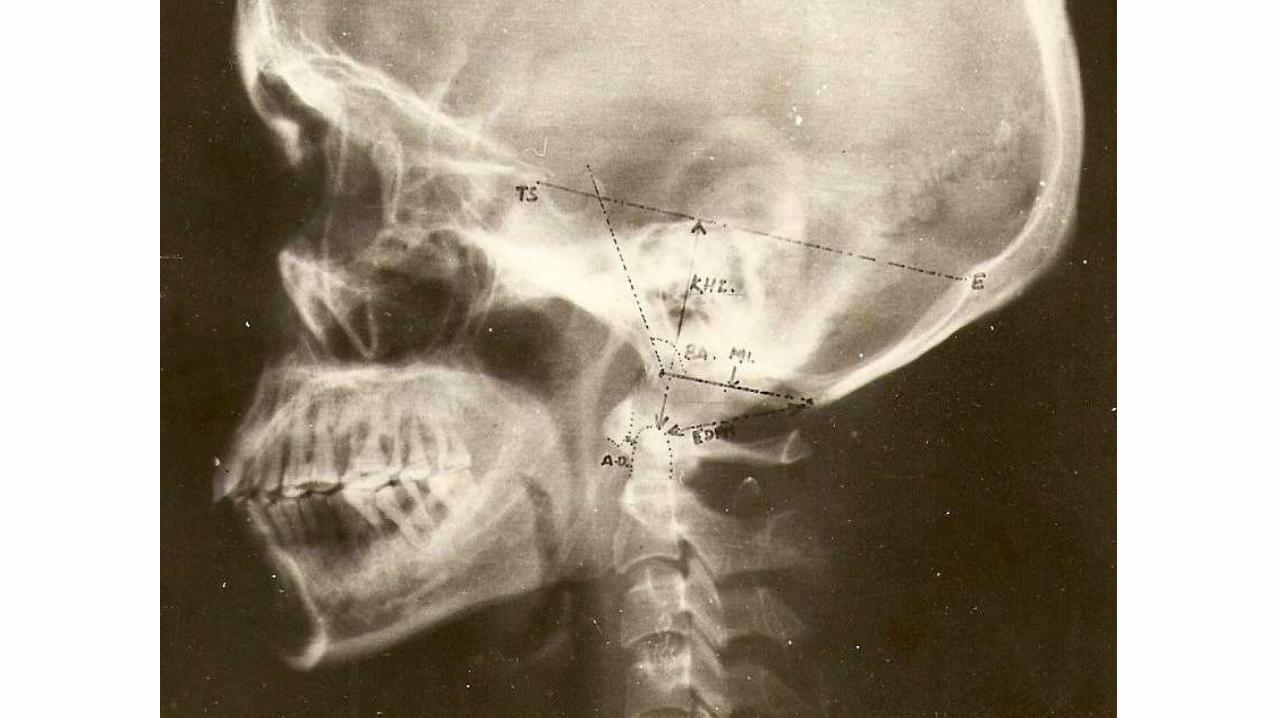
• Klaus height index > 35 mm
• Atlanto-temporo > 22mm.
mandibular index
• Atlanto-odontoid space upto 3 mm in adultsupto 5 mm in children
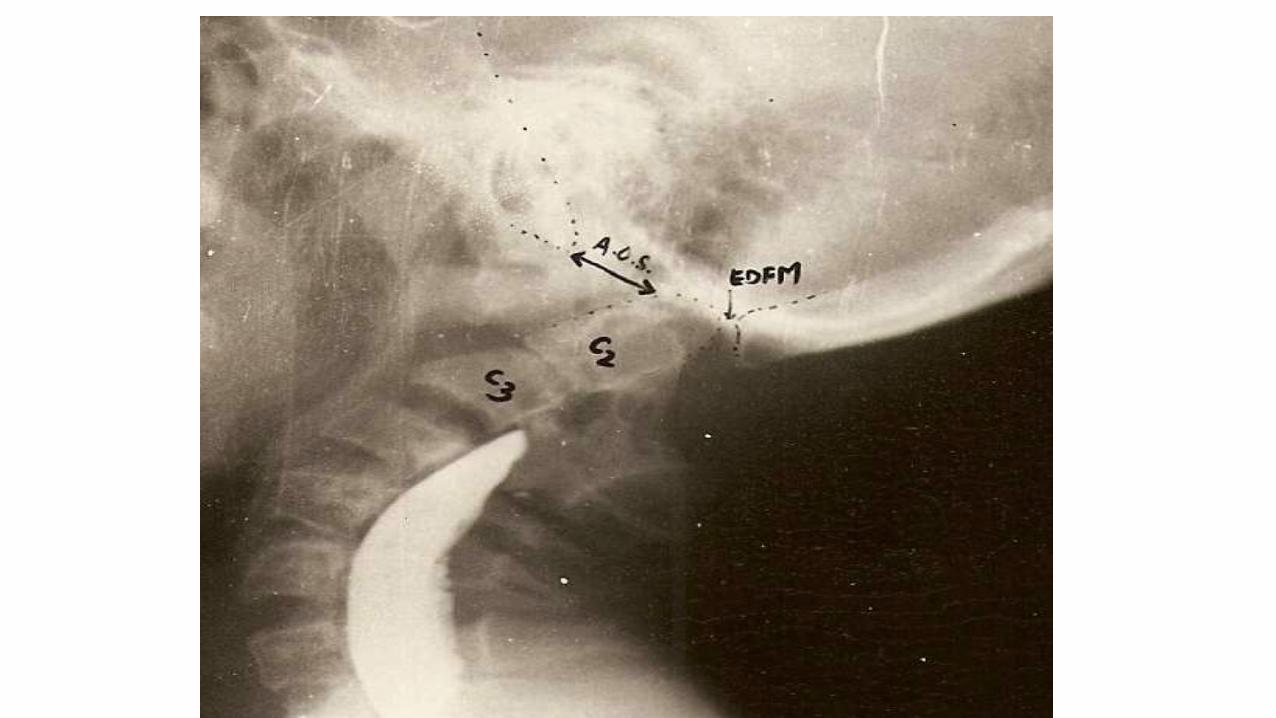
• EDFM > 19mm
* May be reducible, partially reducible or irreducible
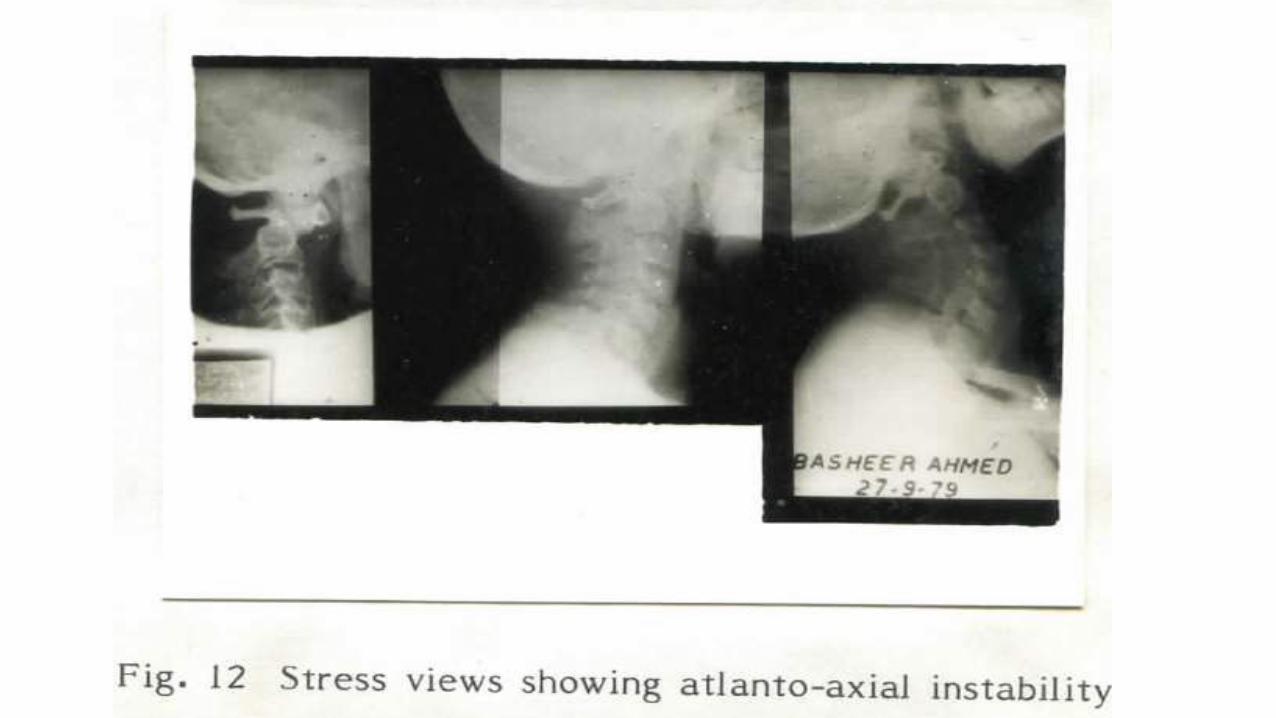
STRESS X-RAYS
• These are the lateral views of the cervical spine in flexion and extension.
• These are absolutely essential to determine the presence of atlanto-axial instability and cord compression.
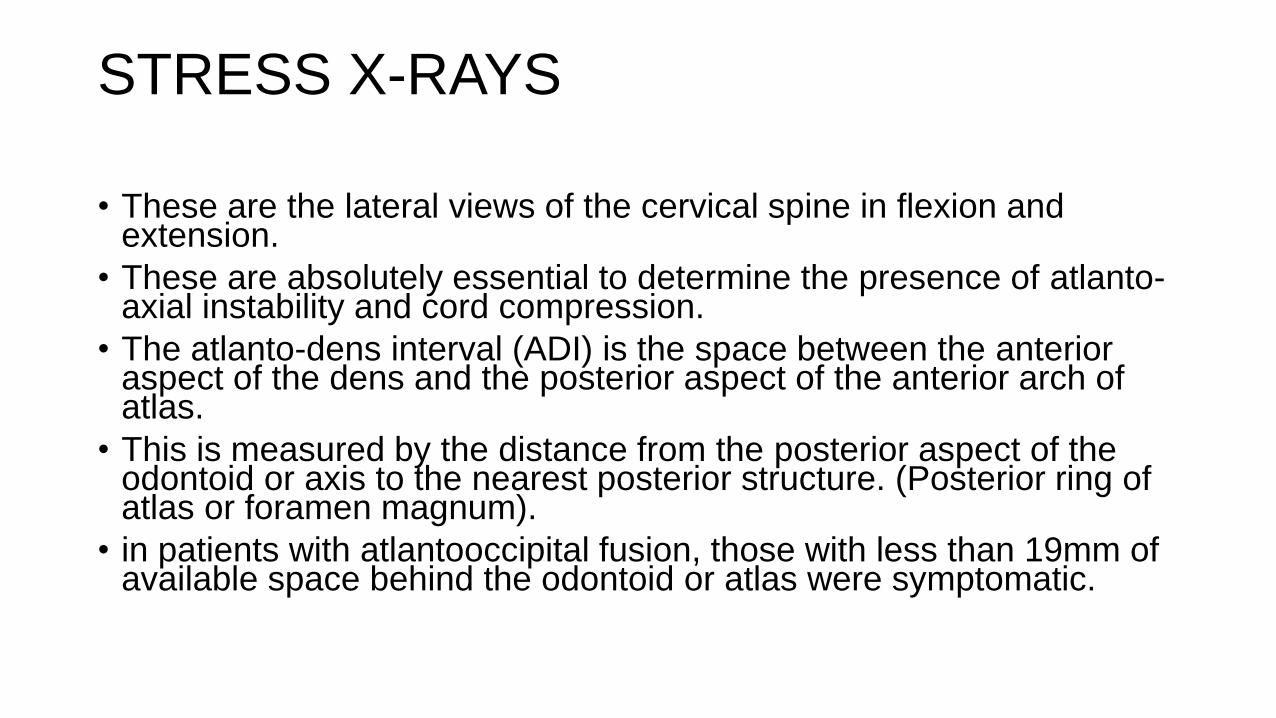
• The atlanto-dens interval (ADI) is the space between the anterior aspect of the dens and the posterior aspect of the anterior arch of atlas.
• This is measured by the distance from the posterior aspect of the odontoid or axis to the nearest posterior structure. (Posterior ring of atlas or foramen magnum).
• in patients with atlantooccipital fusion, those with less than 19mm of available space behind the odontoid or atlas were symptomatic.
TOMOGRAM
• Antero-posterior and lateral tomograms are indicated when routine
• views are not satisfactory in demonstrating the anomaly.
• Anomalies like hypoplastic odontoid, occipitalisation of atlas are clearly visualised.
MYELOGRAPHY
• Before the advent of CT scan, contrast myelography was useful in demonstrating and localising space occupying lesions and congenital malformations in the cervical canal and cistern.
• Contrast medium may be an oily or water soluble medium.
• The use of Metrizamide enables the level of maximum cord compression to be demonstrated and gives an idea of the necessity or not of decompression before stabilisation is performed.
VENTRICULOGRAPHY AND ANGIOGRAPHY
• Air ventriculography was performed in earlier days to determine the element of internal hydrocephalus due to long standing compression at the cranio-vertebral junction.
• Surgically remediable soft tissue lesions at the upper cervical level have been revealed by angiography and it was performed in earlier days during the investigation of posterior fossa anamoly.
COMPUTERISED TOMOGRAPHY SCAN
• provides valuable information as to the presence of
• (a) cord compression
• (b) neural anomalies
• (c) internal hydrocephalus
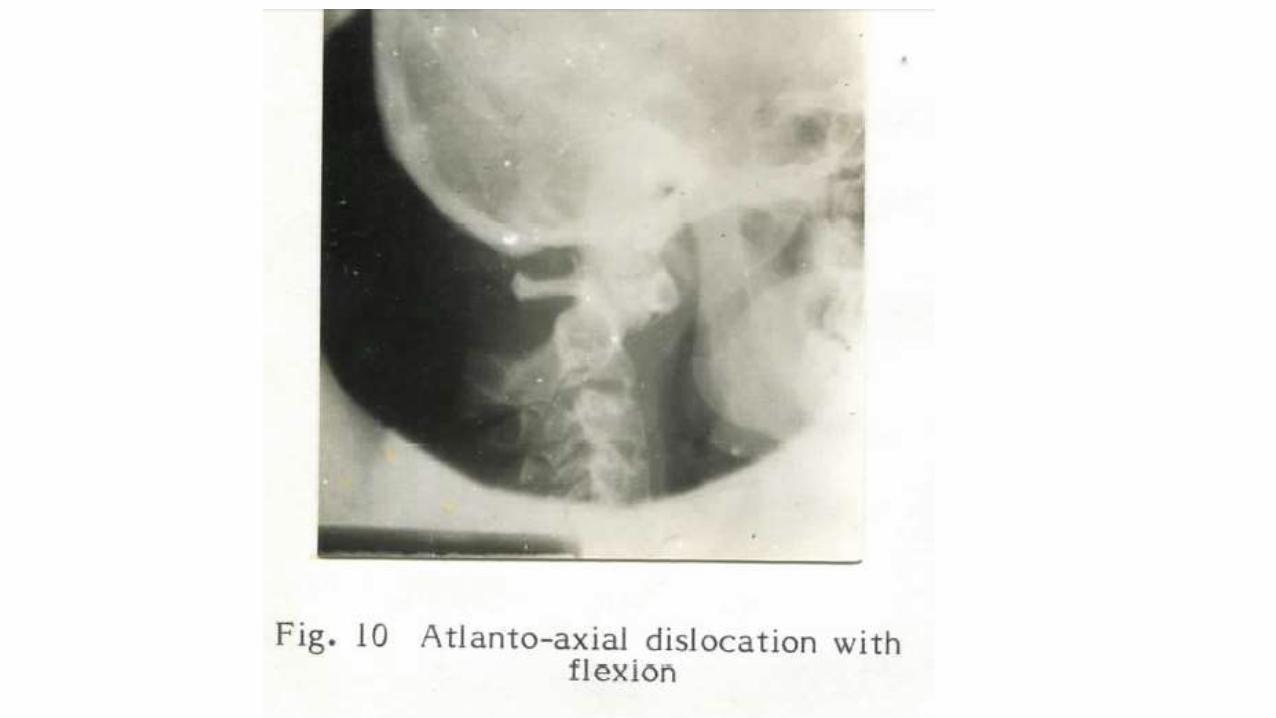
Atlanto-Axial Dislocation
–Traumatic
–Spontaneous (Hyperemic)
–Congenital

Wadia Classification (1973)
• Group 1- associated with occipitalization & frequent fusion of C2,C3
• Group 2- Associated with Dens Dysplasia- frequently totally reducible
• Group 3- No Congenital Bony abnormality
Types of dens dysplasia
• Type 1 (Os odontoideum) separate odontoid process
• Type 2 (Ossiculum terminale) failure of fusion of .
apical segment with its base
• Type 3 – Agenesis of odontoid base & apical segment .
. lies separately.
• Type 4 – Agenesis of odontoid apical segment
• Type 5 –Total agenesis of odontoid process.

Klippel- Feil Syndrome
• 1912
• Maurice Klippel and Andre Feil
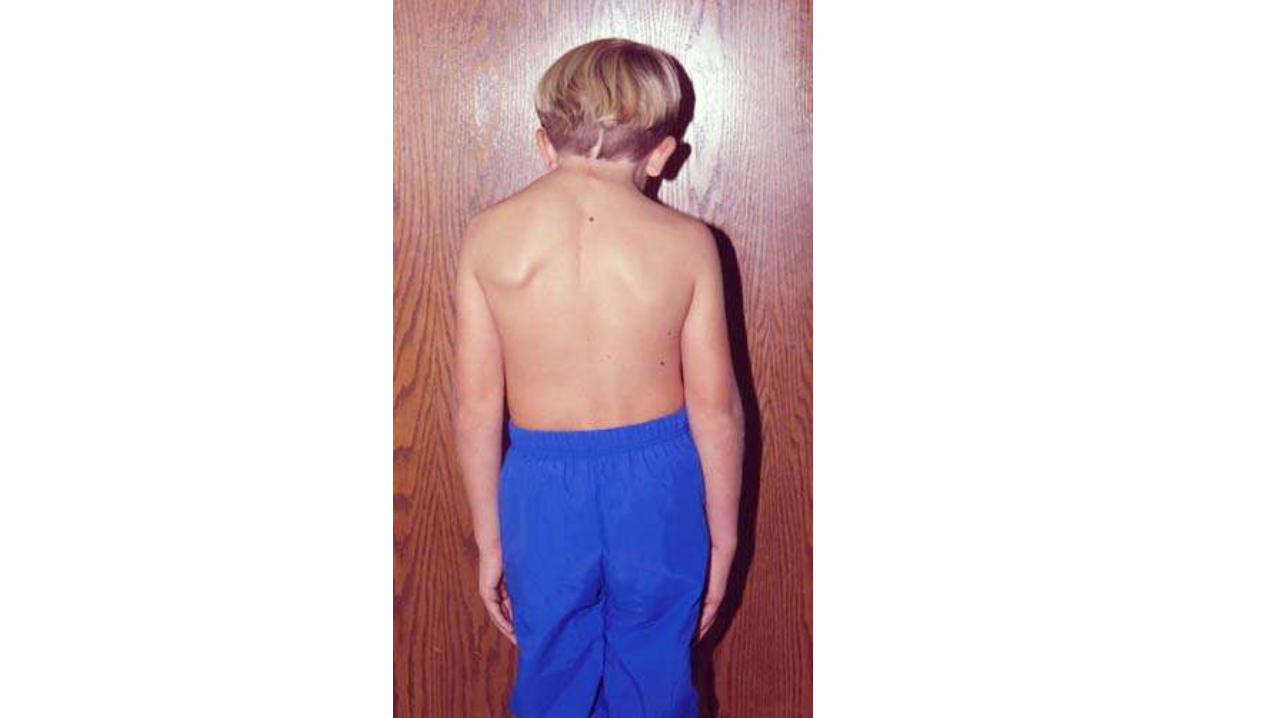
• described patients who had a short, webbed neck; decreased range of motion (ROM) in the cervical spine; and a low hairline
Klippel- Feil Syndrome
• Type 1- Massive fusion of cervical and often upper thoracic vertebra. Associated with short neck, low hairline and restricted neck movements
• Type 2- associated with fusion of several cervical vertebra
• Type 3 – associated with fusion of 2 cervical vertebra.



Arnold-Chiari Malformation
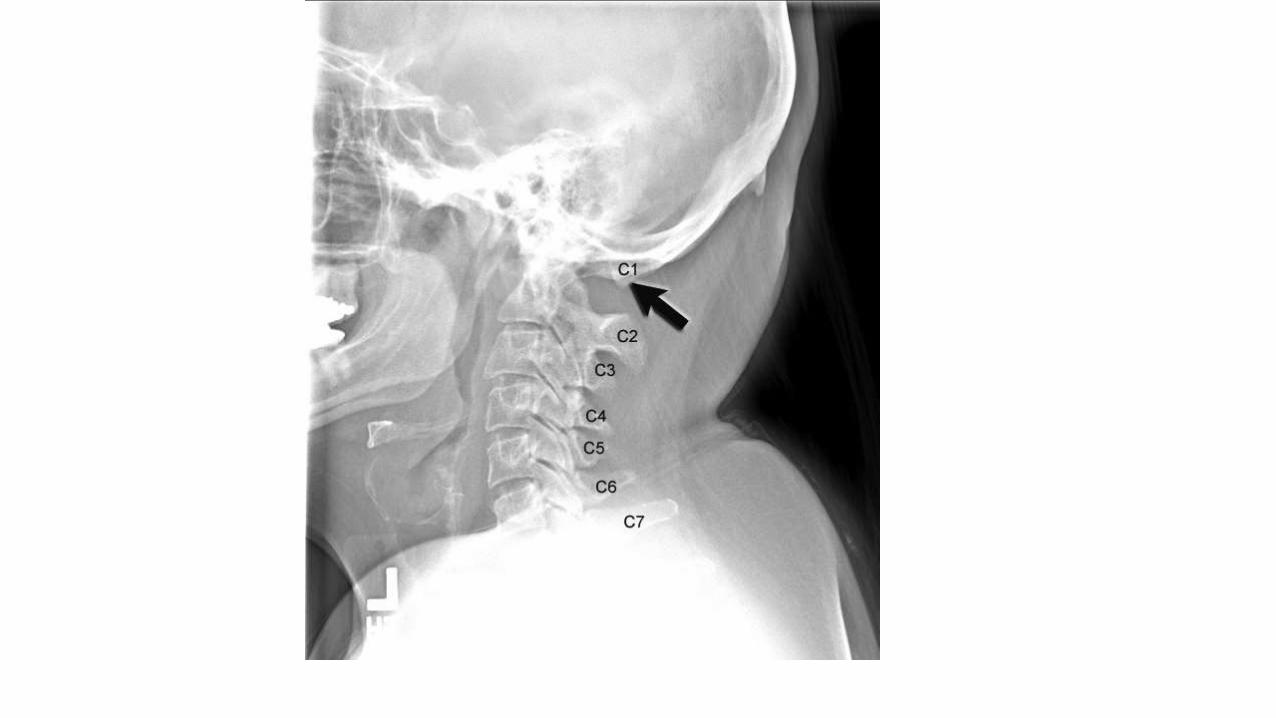
• Type 1- Chiari type I malformation is the most common and the least severe of the spectrum, often diagnosed in adulthood.
• Its hallmark is caudal displacement of peglike cerebellar tonsils below the level of the foramen magnum, a phenomenon variably referred to as congenital tonsillar herniation, tonsillar ectopia, or tonsillar descent.
• The resultant impaction of the foramen magnum, compression of the cervicomedullary junction by the ectopic tonsils, and interruption of normal flow of cerebrospinal fluid (CSF) through the region produce the clinical syndrome.
• Chiari type II malformation is less common and more severe, almost invariably associated with myelomeningocele.
• Because of its greater severity, it becomes symptomatic in infancy or early childhood.
• Its hallmark is caudal displacement of lower brainstem (medulla, pons, 4th ventricle) through the foramen magnum.
• Symptoms arise from dysfunction of brainstem and lower cranial nerves.
• Chiari type III and IV malformations are exceedingly rare and generally incompatible with life .
• The type III malformation refers to herniation of cerebellum into a high cervical myelomeningocele, whereas type IV refers to cerebellar agenesis.
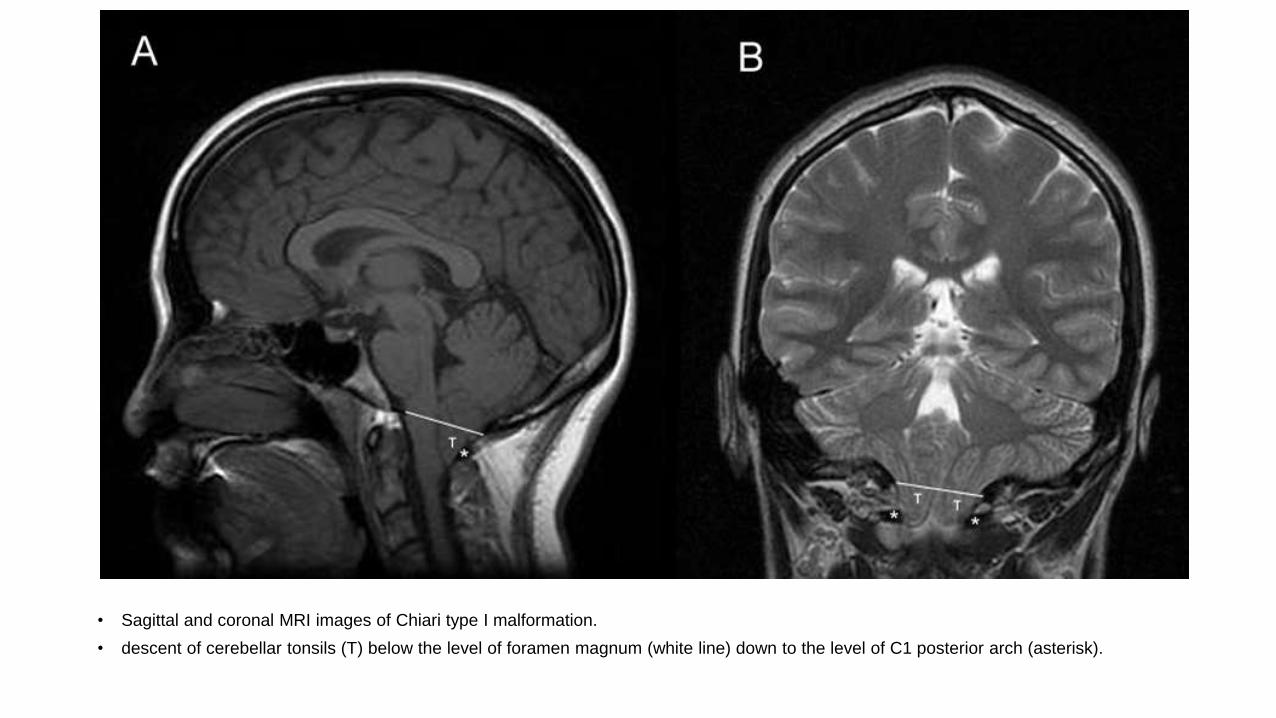
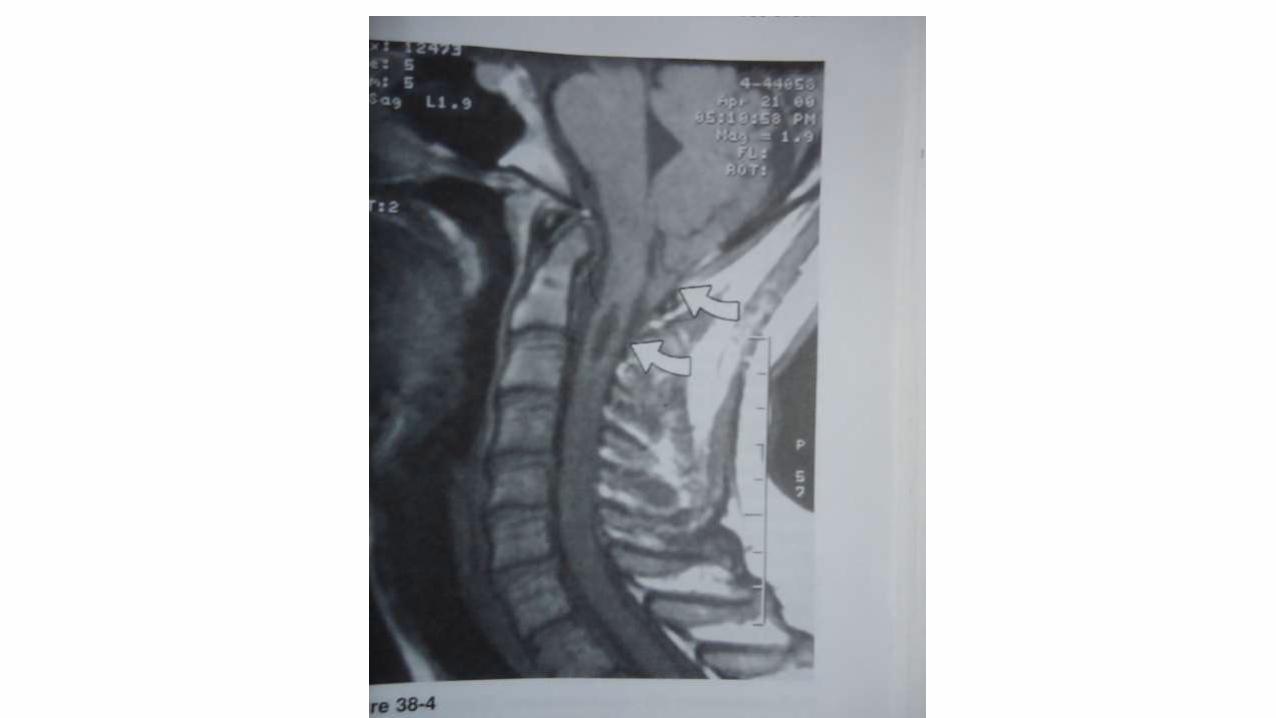
• Sagittal and coronal MRI images of Chiari type I malformation.
• descent of cerebellar tonsils (T) below the level of foramen magnum (white line) down to the level of C1 posterior arch (asterisk).

• crowding of foramen magnum by the ectopic cerebellar tonsils (T) and the medulla (M, absence of cerebrospinal fluid.

Syringomyelia/ Syringobulbia
Progressive degenerative/ developmental disorder of the spinal cord, characterized clinically by brachial amyotrophy, suspended dissociative sensory loss, and pathologically by cavitation in the central region of the spinal cord.
90% cases associated with ACM type I.
Syringobulbia: the lower brainstem equivalent of syringomyelia, usually co-exists
Types I: Syrinx with obstn of the foramen magnum
Type II: Syrinx without obstn of the foramen magnum
Type III: Syrinx with other diseases of the spinal cord
Type IV: Pure hydromyelia
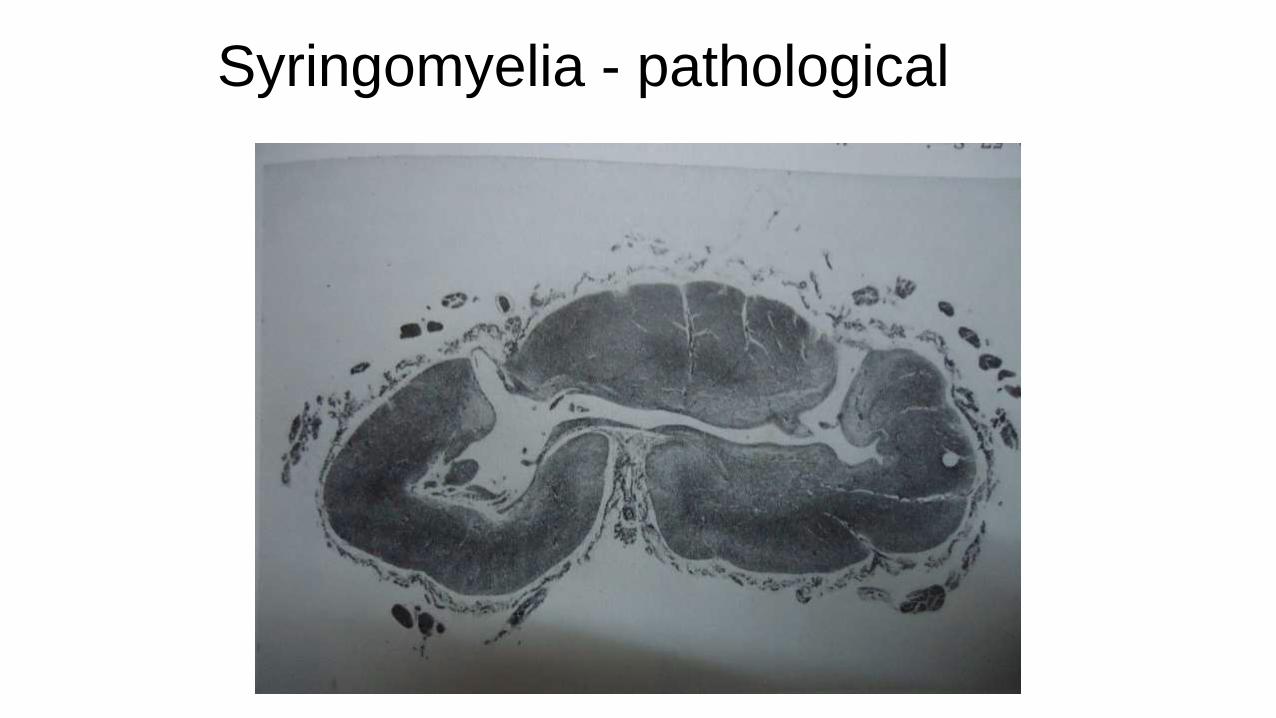
Syringomyelia - pathological

Syringomyelia -clinical
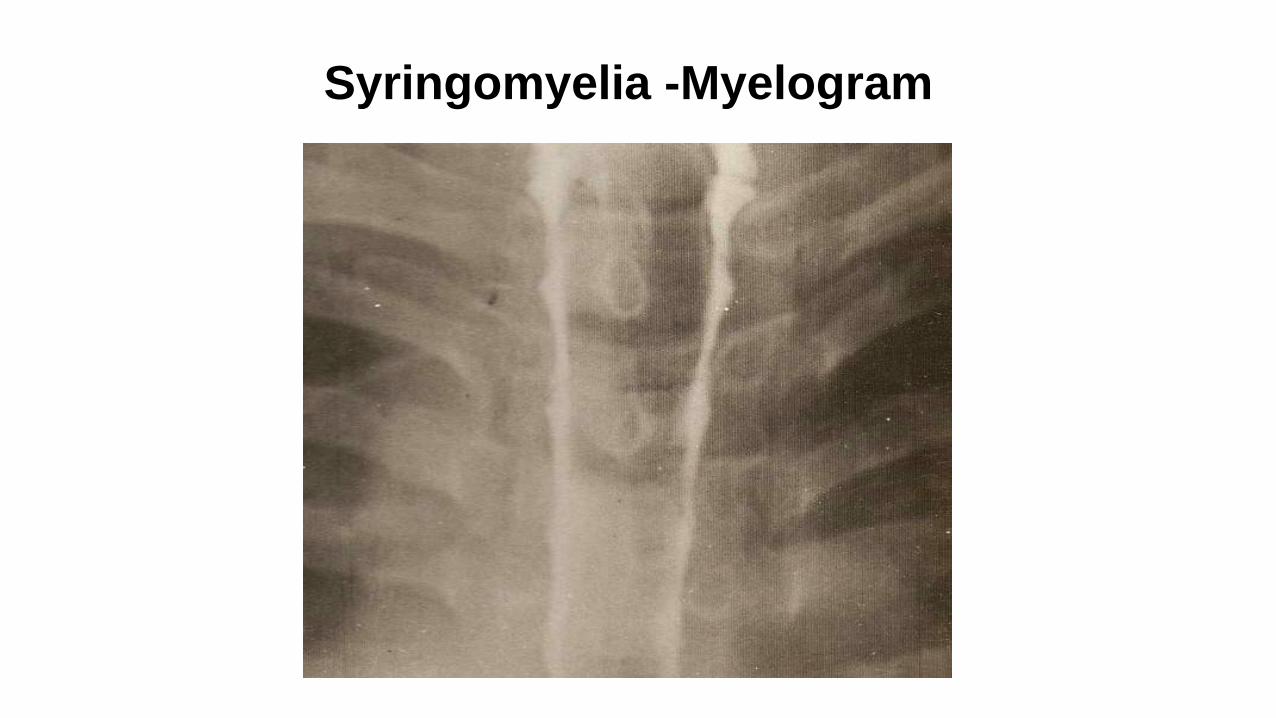
Syringomyelia -Myelogram

Syringomyelia - MRI
Cervical canal stenosis in CV anomalies
• Foramen Magnum: 25-30mm
• C1 25-30mm
• C2 20-25mm
• C3-C7 ≥ 14mm
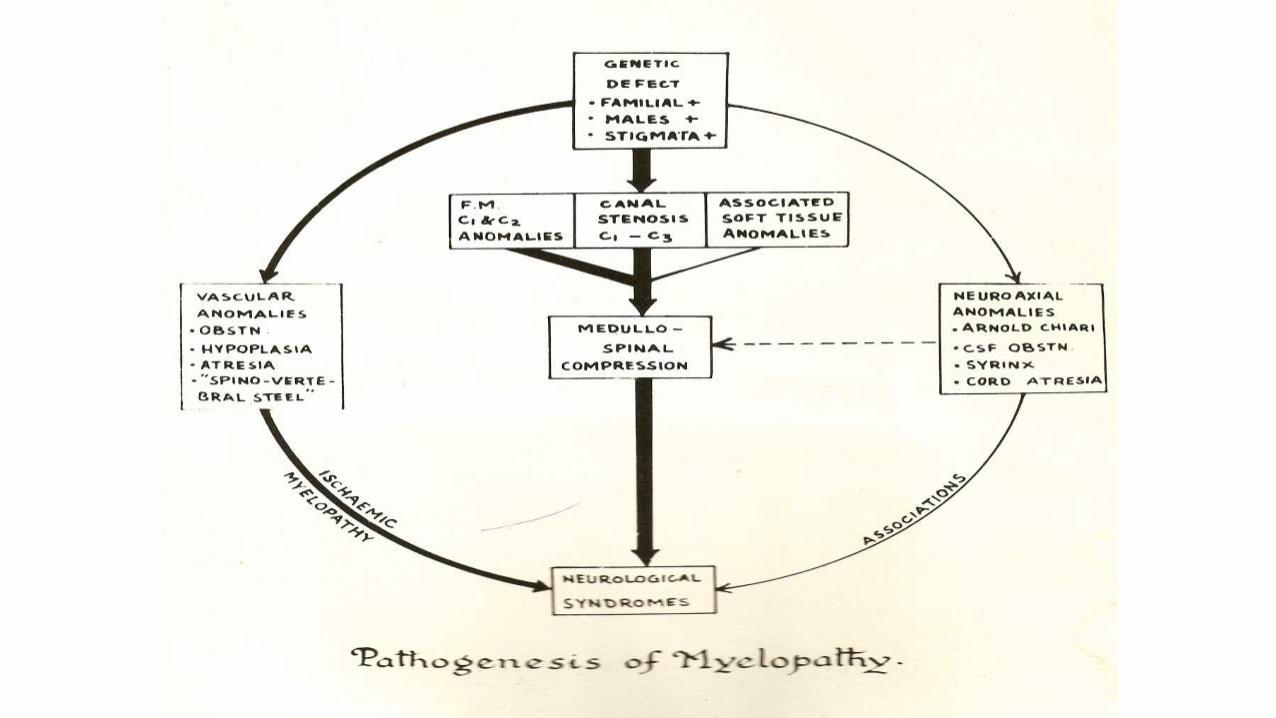
Clinical manifestations of CV anomalies
• Age
• Sex
• Familial occurrence
• Precipitating factors
• Onset
Presenting Features
A. Cervical symptoms and signs
B. Myelopathic Features- long tract involvement and wasting
C. CN involvement- IX, X,XI,XII,V, AND rarely VIII,VII
D. Cerebellar symptoms/signs- Nystagmus, Ataxia, intention tremor, dysarthria
E. Transient Attack of V-B insufficiency
F. Features of Raised ICT- usually seen in Pts. Having basilar impresssion and/or ACM
1. Short neck, low hairline, restricted neck movements are frequently seen in KF anomaly, Occipitalization, and basilar invagination
2. Transient Attacks of VB insufficiency are usually encountered in Pts. With A-A dislocation.
3. Several bony and soft tissue anomalies often co-exist
4. Neurological deficit is usually produced by A-A dislocation, Basilar Invagination, ACM and Syringomyelia / Syringobulbia
Treatment of CV anomalies
1. Treatment of A-A dislocationa) Conservative treatment- For patients having only cervical symptoms
or transient VB insufficiency with or without mild neurological deficit maybe initially managed conservatively using –
1. Cervical Collar
2. Head- Halter Traction- if there is associated myelopathicfeatures
b) Surgical Management

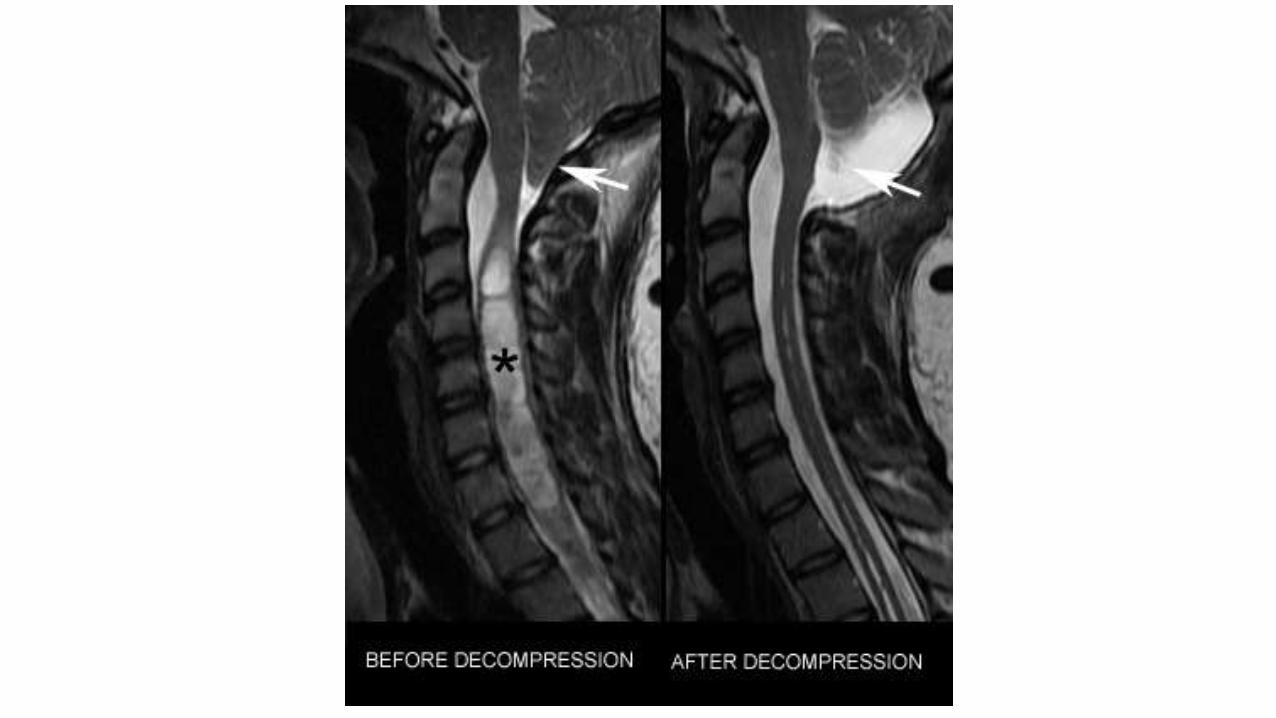
Treatment of Basilar Invagination and ACM
A. Conservative management
B. Surgical treatmentA. Upper cervical laminectomy and enlargement of
Foramen Magnum

References
• Goel A, Shah A. Reversal of longstanding musculoskeletal changes in basilar invagination after surgical decompression and stabilization. J Neurosurg Spine 2009;10:220-7.
• Apley’s Textbook of Orthopaedics
• A Textbook of Neuroanatomy GARTNER
• HARRISONS’S Textbook Of Internal Medicine
• Dr. Vincent Thamburaj
THANK YOU