critical care essentials for micu€¢ ambubag • iv access • drugs e))) • critical care...
TRANSCRIPT
John E Fitzgerald, MD
Professor of Medicine
UT Southwestern Medical Center
CRITICAL CARE ESSENTIALS

SHOCK
• State in which profound and widespread reduction of effective tissue perfusion leads to cellular injury
• Inability of cells to obtain or use O2 in sufficient quantity to meet their metabolic requirements
• Cellular dysfunction/organ failure in shock results from:
• Cellular ischemia
• Circulating/local inflammatory mediators
• Free radical injury

SHOCK
• Clinical consequences:
• Encephalopathy
• ARDS
• ATN, prerenal azotemia
• Ischemic hepatitis or intrahepatic cholestasis
• GI ischemia (stress gastritis, ileus, bacterial translocation, pancreatitis, acalculous cholecystitis)
• Myocardial ischemia/depression, arrythmias
• DIC, dilutional thrombocytopenia
• Immune depression (cellular/humoral, ¯ gut barrier function)

SHOCK• Is the cardiac output high or low?
• Low: narrow pulse pressure
• Cool extremities
• Is the heart too full or empty?
• JVD
• Edema
• S3
SHOCK• Distributive shock
• ê SVR
• é CO
• ê CVP
• ê PAOP
• é cvSVO2

SHOCK
• Distributive
• Peripheral maldistribution of blood flow to tissues
• Tissue malperfusion can persist despite normal or high CO
• Microcirculatory failure with impaired tissue oxygen extraction and impaired cellular utilization
• In septic shock, see ê density of perfused capillaries, “stopped flow” microvessels due to microvascular thrombosesand é leukocyte adhesion, and heterogeneous regional perfusion with precapillary shunting
• Warm extremities, ê DBP, é pulse pressure
• Sepsis, anaphylaxis, neurogenic (spinal) shock, thyroid storm, adrenal crisis
SEPSIS BUNDLE• Culture and begin antibiotics within first hour• Within 3 hours
• Measure lactate• BCx before antibiotics• Administer antibiotics• Administer 30 ml/kg crystalloid for hypotension or lactate ≥ 4
• Within 6 hours• Vasopressor for MAP ≥ 65• Measure CVP and ScvO2 (CVP > 8, ScvO2 > 70%)• Remeasure lactate
• PROCESS trial: using EGDT goals previously suggested made no difference

STEROIDS IN SEPTIC SHOCK• CORTICUS trial showed no survival benefit to steroids, but faster reversal of shock
• Increased incidence of new infections and hypernatremia
• Do not use steroids unless shock is refractory to adequate fluid resuscitation and use of pressors
• Do not need to do ACTH stimulation tests if refractory shock
• 2C evidence for HC 200 mg/d in refractory shock
SHOCK
• Hypovolemic
• Hemorrhage
• Dehydration
• GI fluid losses (diarrhea, vomiting)
• Urinary losses (diuretics, hyperglycemia, renal dysfunction)
• Loss of fluid to interstitium (é vascular permeability in sepsis/trauma), 3rd spacing (e.g., into abdomen in patients with portal HTN), critically low oncotic pressure in hypoalbuminemia
• Venodilation (sepsis, spinal injury, anaphylaxis, drugs/toxins)
SHOCK• Hypovolemic shock
• é SVR
• ê CO
• ê CVP
• ê PAOP
• ê cvSVO2

SHOCK
• Hypovolemic
• ê BP, ê pulse pressure
• Tachycardia
• Pale, cool, clammy, often mottled skin
• Flat neck veins and peripheral veins
• ê urine output

SHOCK
• Compensatory responses in hypovolemic shock
• Sympathetic stimulation
• Splanchnic vasoconstriction
• Blood flow to brain/heart relatively preserved in hypovolemic shock due to dominant autoregulatory control of those organ systems
• Compensatory mechanisms begin to fail with 20-25% acute blood volume loss (orthostasis, é SVR, é serum lactate)
• Hypotension occurs with ³ 40% acute loss

SHOCK• Cardiogenic shock
• é SVR
• ê CO
• é CVP
• é PA wedge pressure
• ê cvSVO2

SHOCK• Cardiogenic
• Hypotension, tachycardia, tachypnea
• Cool extremities
• Distended neck veins
• Wet crackles
• Heart murmur or gallop
• Lactic acidosis
• Peripheral edema
• Oliguria

SHOCK• Obstructive shock
• é SVR or PVR
• ê CO
• é CVP
• ê cvSVO2

SHOCK
• Obstructive
• ê Diastolic filling
• Tension pneumothorax
• Cardiac tamponade
• Gravid uterus compressing vena cava (roll pregnant shock patient to left lateral decubitus position)
• é Afterload
• Massive pulmonary embolism
• Aortic dissection

SHOCK
• One category of shock may dominate, but most cases involve elements of others
• Shock from any cause may result in decreased coronary perfusion pressure with resultant demand myocardial ischemia and dysfunction
• Even in hemorrhagic shock (a cause of pure hypovolemic shock), if resuscitation is not rapid, a series of cardiovascular and inflammatory mediator-driven events will occur driving further injury
• The shock state may not respond to volume and blood resuscitation alone (late phase of hemorrhagic shock), and pressors may be required despite restoration of the intravascular volume status

SHOCK
• Septic shock = classic distributive shock, but before resuscitation, a substantial hypovolemic component may exist due to venodilation and 3rd spacing (capillary leak), and there may be a cardiogenic component related to myocardial depression (TNF-a, IL-1)
• We think of septic shock patients being warm peripherally, but prior to fluid resuscitation, they are often cool because of this issue

SHOCK
• Cardiogenic shock typically manifests as high ventricular filling pressures, but patients with pump failure are often diuresedaggressively prior to the onset of actual shock (due to pulmonary or peripheral edema), and they may have a hypovolemic component
• If intravascular hypovolemia is suspected in cardiogenic shock, you still pressure bag IVFs and assess the clinical response, but use smaller aliquots like 100-200 cc
• May need PA catheter, inotropic support, IABP or PCI

VOLUME RESPONSIVENESS• CVP/PAWP not good at determining response to fluid challenge
• SVV or PPV can be measured from A line
• In mechanically ventilated patients on 8 ml/kg Vt, SVV > 10-13% predicts > 15% increase in CO after 500 ml fluid bolus (does not work in Afib or if spontaneously breathing or if have variable tidal volumes from breath to breath)
• IVC U/S collapse with respiration predicts volume response in septic patients on mechanical ventilation with Vt 8-10 ml/kg IBW
• Passive leg raise 30 degrees for 1 minute, if BP improves predicts +volume response
HEMORRHAGIC SHOCK• Ketamine preferred for intubating unstable head trauma and hypovolemic shock
• Raises sympathetic tone (é BP and HR)
• Benzodiazepines decrease associated nightmares

PRESSORS/INOTROPES
• Sympathomimetics
• Phosphodiesterase inhibitors
• Cardiac glycosides
• Vasopressin

DOPAMINE
• Typical dosing range 2-20 mcg/kg/min
• Vascular dopaminergic
• Dominates at < 4-5 mcg/kg/min
• Cardiac b1
• Dominates at 5-10 mcg/kg/min
• é CO due to é contractility (cardiac b1) and é venous tone and venous return (vascular a)
• Vascular a
• Prominent above 10 mcg/kg/min (é BP with smaller é in CO)

DOPAMINE• Vascular D2 receptors vasodilate renal, mesenteric, myocardial and
cerebrovascular beds
• Renal D1 receptors mediate mild natriuresis
• Renal dose dopamine may be useful for augmenting urine output in patients with renal insufficiency and volume overload requiring high doses of diuretics
• Renal dose dopamine does not improve/preserve renal function
NOREPINEPHRINE
• Inotropic effects (cardiac a and b1-adrenoreceptors)
• Peripheral vasoconstriction (vascular a)
• Most useful for septic/obstructive shock
• May ê forward flow in cardiogenic shock
• Only use for extremely brief periods in hemorrhagic shock pending volume infusion
NOREPINEPHRINE
• Usual dose 2-30 mcg/min
• More potent vasoconstriction compared to dopamine
• Somewhat lower effect on heart rate and contractility
• Preferred pressor in septic shock and obstructive shock due to PE
• Less arrythmogenic compared to dopamine
DOBUTAMINE• Increased myocardial contractility
• Cardiac a and b1 adrenoreceptors
• Weak arteriolar vasodilatation (ê afterload)
• b2 vascular relaxation > a constriction
• Vasoconstriction in venous bed (a effect may predominate in small capacitance vessels) causing é venous return
• Decreased filling pressures and greater é CO vs. dopamine
• é myocardial oxygen consumption (like dopamine)
• é myocardial perfusion (unlike dopamine)

DOBUTAMINE
• Usual dose 1-20 mcg/kg/min
• Useful in cardiogenic shock and cardiogenic pulmonary edema (é CO and ê ventricular filling pressures)
• May é BP in this setting
• May ê BP if myocardial damage is extensive (where vasodilatory properties dominate and CO cannot augment)
• May be useful in obstructive shock pending definitive intervention
EPINEPHRINE
• a, b1, b2
• Greater contractility é vs. other pressors
• First line for anaphylactic shock
• To support myocardial contractility post-CABG
• When other pressors/inotropes fail
• Usual dose 1-8 mcg/min

PHENYLEPHRINE
• Pure a agonist
• Peripheral vasoconstriction, weak é contractility
• Counteracts vasodilatory effects of anesthetics
• Useful in neurogenic (spinal) shock
• Useful in septic shock when HR high
• Risk = improved BP/HR numbers but actual worsening of organ ischemia
• Usual dose 20-200 mcg/min

MILRINONE
• Phosphodiesterase inhibitor (é cAMP)
• é myocardial contractility
• ê vascular tone (pulmonary vasodilator also)
• Useful in CHF, cardiogenic shock, post-CABG myocardial dysfunction
• Possible role in catecholamine-refractory septic shock
• Usual dose 37.5-75 mcg/kg/min
VASOPRESSIN
• Levels are significantly depressed in septic shock
• Profound pressor response in septic shock, but not in normals
• Other uses:
• Milrinone-induced shock in severe CHF
• Unstable brain dead organ donors
• Late-phase hemorrhagic shock
VASOPRESSIN
• Usual dose 0.01-0.04 mcg/min (max 0.1 mcg/min)
• Use only after hemodynamic stabilization attempted with standard agents
• At upper end of dosing, a subset of patients develop digital, mesenteric or myocardial ischemia
• In patients with vascular disease, even small doses may precipitate angina (may need nitroglycerin)

ARDS• Pneumonia is #1 cause, then sepsis of nonpulmonary origin, aspiration,
trauma
• Mortality much higher in sepsis and with advancing age
• Need bilateral opacities
• Mild ARDS = P/F ratio 200-300 with PEEP ≥ 5
• Moderate ARDS = P/F ratio ≤ 200 with PEEP ≥ 5
• Severe ARDS = P/F ratio ≤ 100 with PEEP ≥ 10
• For severe ARDS, opacities in at least 3 quadrants and Ve > 10 LPM or Crs < 40 ml/cm H2O
• ECHO to rule out CHF

LOW TIDAL VOLUME VENTILATION• Decreases mortality
• Decreases organ failures
• Increases unassisted breathing

CONSERVATIVE FLUID STRATEGY IN ARDS• Diurese if not hypotensive unless CVP < 4
• Dry patients were more likely to get off the ventilator (é vent and ICU free days)
• Less cardiovascular and CNS failures
• No increase in renal failures
• No difference in mortality
• Try to maintain patients on the dry side after the first 24 hours
CISATRACURIUM IN ARDS• For severe ARDS (P/F < 150, PEEP > 5, Vt 6-8 cc/kg), cisatracurium improved 90 day
survival (32% vs 41% placebo)

FAILED ARDS THERAPIES• Salbutamol
• Sivelastat
• Rosuvastatin
• Aerosolized surfactant
• Omega-3 fatty acids
• Steroids bad in ARDS if given after 2 weeks
• Could be beneficial earlier (day 7-13) in acute phase (trend toward ↓ mortality, mechanical vent days, MODS) but there are negatives including more neuromyopathy and reintubations
• Nobody received steroids in days 1-6
• Additional trials are needed to determine if steroids in days 1-13 is useful
HIGH PEEP VS LOW PEEP• No difference in survival when on low tidal volume ventilation taking all comers• ALVEOLI study showed improved oxygenation but no change in mortality or ventilator free
days• Reduced need for rescue therapies with higher PEEP• Higher PEEP was not harmful• May be some benefit to high PEEP in severe patients• Using esophageal pressure to titrate PEEP was associated with a trend toward lower
mortality in one study, better oxygenation and lung compliance at 72 hr• Using esophageal pressure to titrate PEEP results in higher PEEP in that group• This might be the best way to determine optimal PEEP• Other options are determining the lower inflection point (static compliance curve using
supersyringe method) or ARDSnet table for PEEP/FiO2

RECRUITING MANEUVERS IN ARDS• May improve refractory hypoxemia
• May reduce need for rescue therapies
• No change in mortality

PRONE POSITIONING• Useful for refractory hypoxemia, improves gas exchange
• Optimizes lung recruitment and V/Q matching
• Distributes stress and strain more homogeneously
• Only good for severe ARDS, not mild or moderate
• ê 28 and 90 day mortality with prone positioning in French trial
• More ventilator free days
• Use for patients with P/F < 100 on low Vt strategy (or at least < 150—another trial showed benefit there)
• Flip patient for 16 hour period or longer

LONG TERM ARDS OUTCOMES• Lung function returns to near normal
• Critical illness polyneuropathy in up to 70% of survivors with sepsis and ARDS or MOF
• Cognitive impairment
• Impaired return to work, ê productivity, PTSD, anxiety
• Poor nutritional status/weight gain
• Factors associated with improved function at 1 year
• Absence of steroid treatment
• Absence of illness acquired during ICU stay
• Rapid resolution o fMOF and lung injury
INHALED NITRIC OXIDE• Improves the PaO2 number (P/F ratio), lowers PAP, ê BAL IL-6 and IL-8, but no mortality
benefit in severe or less severe ARDS
• Very expensive
• Nebulized epoprostenol has similar effects but less expensive (data to support its use is pending)
IDEAL BODY WEIGHT CALCULATION• Male: (height in inches – 60)2.3 + 50 = kg• Female: (height in inches – 60)2.3 + 45.5 = kg• Initial setting on ventilator for ARDS 8 cc/kg, reduce to 6 cc/kg to keep Pplat < 30• Lower to 6 cc/kg for lung protection• Lung protective strategies
• ê organ failures• ê mortality• ê pulmonary infections• ê atelectasis• é unassisted breathing
• PEEP may worsen hypoxemia in unilateral lung disease, increase risk of barotrauma, reduce venous return and cardiac output
• Set high Vt alarm in pressure control mode to avoid overdistention in ARDS patients
DIFFICULT BAG MASK VENTILATION• MOANS
• Mask seal (facial hair, craniofacial problems)
• Obesity
• Age > 55
• No teeth
• Stiff

PREPARATION FOR INTUBATION• STOPMAID
• Suction• Tools• Oxygen• Positioning/plan• Monitors• Ambu bag• IV access• Drugs
• If preoxygenated, will have upwards of 8 minutes before sats drop below 90% in normals• 2-3 minutes in morbidly obese patients• Systemically ill or pulmonary shunt patients drop more quickly
INTUBATION MEDICATIONS• Lidocaine premedication good for asthma and elevated ICP (1.5 mg/kg IV 2-3 minutes prior)
• Fentanyl 3 mg/kg IV over 30-60 sec 3 minutes prior for elevated ICP or cardiovascular patients who may not tolerate an acute rise in BP with intubation attempt
• Ketamine associated with bronchodilation, good for “awake look”, respiratory drive preserved
• Midazolam out of favor: time to effect delayed, hypotension
• Etomidate: rapid onset, no hypotension, no analgesia
• Can get adrenal insufficiency, concerns with sepsis unjustified
• Propofol: rapid onset, hypotension, no analgesia
• Succinylcholine: lasts 6-10 minutes, 1-1.5 mg/kg
• Contraindicated in rhabdomyolysis, h/o malignant hyperthermia, muscular dystrophy, ALS, stroke > 72 hours, burns > 72 hours, hyperkalemia
• Rocuronium: 0.8-1.2 mg/kg, longer duration than sux
PROOF OF ETT PLACEMENT• Chest rise, auscultation, misting of tube are not sufficient
• CO2 color change: need > 5 breaths
• Waveform capnography = gold standard

MECHANICAL VENTILATION
• Goals
• Achieve adequate oxygenation/ventilation
• Decrease work of breathing
• Establish synchrony between patient and ventilator
• Avoid high inspiratory pressures

INITIATING MECHANICAL VENTILATION
• Choose mode with which you are most familiar, but become familiar with assist volume control, assist pressure control, PRVC (VC+) and PS/CPAP
• Initial FiO2 1.0, titrate for SpO2 92-94%
• VT 8 ml/kg usual for initiation
• VT 10-12 ml/kg for neuromuscular disease patients prone to atelectasis
• VT 6 ml/kg for ARDS (want plateau P < 30, so decrease VT further if necessary)
• Choose RR (VE), flow rate appropriate to clinical circumstances (e.g., patients with septic shock or severe metabolic acidosis will require higher minute volumes and inspiratory flows than patients intubated for airway protection)
• Use higher PEEP in patients with diffuse lung injury
• Wait 30 minutes after vent change to check ABG

MECHANICAL VENTILATION
• Ventilator Mode
• Program by which the ventilator interacts with the patient
• Determines relationship between possible types of breaths allowed by the ventilator and the inspiratory variables (trigger, limit, cycle)
• Cycling = changeover from inspiration to expiration, and depending on the mode selected may be determined by
• Elapsed time (pressure control ventilation)
• Delivered tidal volume (assist volume control ventilation)
• Predetermined decrement in flow (pressure support ventilation)
MECHANICAL VENTILATION
• Triggering = changeover from expiration to inspiration
• Pressure trigger
• Flow trigger
• Time (Controlled mandatory ventilation—patient cannot trigger)
• If sensitivity is too low, the ventilator may be triggered by patient motion, external compression, gastric suctioning, fluid moving within vent circuit, air leaks in the circuit or chest tube suction in the presence of a bronchopleural fistula
• If sensitivity too high, WOB increases

MECHANICAL VENTILATION MODES
• Assist Volume Control
• Volume-cycled ventilation (ventilator cycles when preset volume is delivered)
• Patient determines number of full mechanical breaths that are received (back-up rate = minimum number of breaths)
• Need to set a pressure limit (“pop-off” valve) to avoid potentially dangerous increases in airway pressure
• Pressure-limiting may result in significant hypoventilation

MECHANICAL VENTILATION MODES
• Assist Pressure Control
• Time cycled
• Ventilator maintains a constant pressure for a preset time interval (pressure limited strategy)
• Inspiratory flow is initially high then tapers as alveolar pressure rises
• Tidal volume not guaranteed (will é or ê with changes in airway resistance or thoracic compliance)
• Not recommended when lung mechanics may rapidly change
• The flow and volume variability from breath to breath may assist in improving patient ventilator synchrony provided that the set inspiratory time is close to what the patient actually wants (too short and the patient is still trying to inspire, too long and the patient gets an unwanted “plateau” with each breath)

MECHANICAL VENTILATION MODES
• Synchronized Intermittent Mandatory Ventilation (SIMV)
• Alternating pattern between fully supported and less supported breaths
• Back-up rate determines number of fully supported breaths
• If the patient triggers additional breaths, they get no support or pressure support depending on how the ventilator is set up
• Developed as a weaning mode and meant to keep the patient from developing atrophy of their bellows muscles during mechanical ventilation (but is clearly worse as a weaning strategy)
• Alternating pattern may be disturbing
• Patients not able to adjust neurologic output to respiratory muscles on breath-by-breath basis (so they end up working equally on both their PS and fully assisted breaths)
MECHANICAL VENTILATION MODES
• Pressure Support
• As patient inhales, ventilator adjusts flow to provide and maintain a preset inspiratory pressure
• Patient participates in selecting flow rate and VT
• No guaranteed minute volume or tidal volume
• Cannot use in patients with respiratory drive suppression
• Flow cycled
• Inspiration terminated when predetermined decrement in flow achieved (e.g., 25-30% of the peak flow seen at the beginning of that breath)
• Pressure-limited strategy
• Primarily a weaning mode, but can be used as a full support mode for patients with stable respiratory drive

MECHANICAL VENTILATION MODES
• Pressure Regulated Volume Control (called VC+ on the PB 840 vents)
• Variant of assist pressure control ventilation
• Pressure allowed to go up or down within preset limits to achieve desired VT
• Limits the disadvantage with pressure control ventilation of changing tidal volumes in response to changes in resistance/compliance, and also allows for flow variability (may be more comfortable than straight assist volume control)
MECHANICAL VENTILATION MODES
• BILEVEL
• Fluctuation between higher (PH) and lower (PL) pressures
• Set time spent at higher pressure (TH)
• Drop from PH to PL allows for CO2 elimination
• Spontaneous breaths allowed at both PH and PL
• Generally better patient synchrony vs other time-cycled vent modes
PEEP EFFECTS• Increased FRC and improved oxygenation
• Reduced cardiac output
• Overdistention
• Lung protection: reduced atelectrauma
• Help with triggering and improved expiratory flows in obstructive lung disease
• Improved cardiac performance in CHF

VAP PREVENTION• Hand washing
• HOB elevation 30-45° (low quality evidence)
• Chlorhexidine mouth care
• Daily spontaneous awakening and breathing trials to minimize vent/ICU time
• Delirium prevention, early mobility
• NIV in certain populations (COPD exacerbation, acute cardiogenic pulmonary edema, acute respiratory failure in immunocompromised host)
• Manage without sedation when possible
• Change vent circuit only if soiled or malfunctioning
• ETT with subglottic suction port if expect > 48-72 hours of mechanical ventilation

VENTILATOR INDUCED DIAPHRAGM DYSFUNCTION• Wasting and damage to the primary ventilator pump caused by unloading of the
respiratory muscles in the setting of mechanical ventilation• Decreased protein synthesis, oxidant stress, increased proteolysis leading to myofiber
atrophy, injury and remodeling, with decreased force generating capability and endurance• May begin after just 18-24 hours• Results in weaning failure• Must rule out other causes such as ongoing sepsis, shock, major malnutrition, electrolyte
distubances, neuromuscular disorders acquired in the ICU (CIP, CIM, prolonged NMB)• Should encourage persistent diaphragmatic activity (optimal level of effort not known)• Will neurally adjusted ventilatory assist (NAVA), adaptive support ventilation (ASV), and
proportional assist ventilation (PAV) offer advantages?• Daily use of electrical stimulation to prevent? Works to preserve LE muscle mass in ICU• Drugs targeting proteolytic pathways, antioxidants

STRATEGIES TO REDUCE NEED FOR MECHANICAL VENTILATION• Daily interruption of sedation (restart at ½ rate)
• Use small Vt 6 mg/kg IBW in ARDS
• Interruption of sedation before SBT
• Early PT/OT
• No use of sedatives in mechanical ventilation (analgesia only)
• Conservative fluid strategy in ALI
• Strategies to reduce VAP
• Use of NIV in acute exacerbation of COPD or acute cardiogenic edema
WHY FEAR THE ENDOTRACHEAL TUBE?• Early mortality 0.4%: mostly cardiac arrest from prolonged intubation procedure
• Late mortality related to VAP
• VAP mortality is 27% overall, and 43% with P. aeruginosa infections
• VAP adds 6-13 more ventilator days
• Direct blunt or penetrating trauma to the pharynx, larynx, esophagus, trachea, lips, teeth or tongue
• Aspiration of gastric contents, bronchospasm, hypoxic injury during prolonged intubation attempt, hypotension, pneumothorax
• Long term complications including laryngomalacia, tracheomalacia, tracheal stenosis
NONINVASIVE VENTILATION• Level I evidence supports use of NIV for these indications
• Exacerbations of COPD (best data for this)• pH < 7.35, PaCO2 > 45, RR > 25, respiratory distress• ê treatment failures• ê mortality• ê intubation• ê hospital LOS• Faster weaning from ventilator in intubated patients
• Acute cardiogenic pulmonary edema• CPAP and BIPAP ê need for mech vent, CPAP reduces mortality (BIPAP only trend)
• Hypoxemic respiratory failure in immunocompromised hosts• Preventing post-extubation respiratory failure in high risk patients (COPD, hypercapneic
patients, chronic CHF, patients with history of >1 failed extubation, stridor post-extubation)

CONTRAINDICATIONS TO NIV• Impending cardiac or respiratory arrest
• Inability to protect airway
• Altered mental status
• Nonrespiratory organ failure
• Facial surgery/trauma
• High aspiration risk
• Anticipated prolonged duration of mechanical ventilation

SEDATION IN ICU• RASS score target 0 to minus 2 (awaken to voice)
• Patients who are deeply sedated (RASS 4-5) have many more complications
• Benzodiazepines associated with higher rates of delirium
• Sleep in ICU
• ê nocturnal sleep time (vital signs, phlebotomy, noise, diagnostic tests, nrusinginterventions, light, medication administration, pain)
• é stage 1 and 2 sleep
• Reduced or absent deep sleep

VENTILATOR WEANING• Rapid shallow breathing index (RSBI)• Frequency/tidal volume (f/Vt) = most promising predictor of weaning success, but none is
more than moderately good• RSBI > 105: not weanable (NPV 0.95, but this hasn’t been confirmed in subsequent
studies)• RSBI 60-105 è continue SBT• RSBI < 60, can usually just extubate• 30 minute vs 120 minute SBT trial = no difference in outcomes• T piece or PS 5-6 cm H2O or CPAP alone (CPAP 0 or T piece may more closely simulate
WOB post-extubation compared to using PEEP and PS)• Reintubation rate 13-18%• é work of breathing = #1 cause of reintubation• Mortality is 28% in reintubated patients (odds ratio 5.2 for mortality)

WAKE UP AND BREATHE STRATEGY• ê days on ventilator
• ê ICU and hospital days
• é self extubations
• No significant difference if total reintubations
EARLY VS LATE TRACHEOSTOMY• Early trach 7-14 days
• Late trach > 14 days
• No difference in mortality, ICU days
• Duration of mechanical ventilation is lower with early tracheostomy (more successful weans) according to some, but not all studies
• No downside to doing it earlier apart from the surgical procedure itself
VENTILATOR WEANING
• Preparations for ventilator withdrawal should include:
• Adequate nocturnal rest with fully supported breathing
• Adequate nutrition
• Good circulatory reserve
• Avoidance of excessive intravascular volume
• Treatment of infection
• Appropriate body positioning
• Judicious sedation

VENTILATOR WEANING
• Impediments to successful weaning
• Obstipation
• Urinary retention
• Pleural effusions
• Gastric distention
• Uncontrolled pain
• Severe anemia
• Electrolyte imbalances
• Accumulation of sedative agents

VENTILATOR WEANING
• Sedation
• May accumulate due to excessive dosing
• continuous infusions
• clearance problems (storing drugs in fat
• Daily interruption of sedation with progressive dose reduction
• é ventilator-free days
• When given for lengthy periods, lingering sedative effects can persist for up to a week after the last dose
• Consider propofol or dexmedetomidine sedation when nearing possible extubation

VENTILATOR WEANING
• One of the main sources of weaning delay is failure of the physician to thinkthat the patient might be ready
• Weaning involves the use of three diagnostic tests
• Measurement of predictors
• A weaning trial
• An extubation trial
VENTILATOR WEANING
• Employ screening studies early
• Pimax to assess overall inspiratory muscle strength
• Dependent on patient motivation and cooperation
• Respiratory frequency-to-tidal volume ratio (f/VT)
• Measured during 1 minute of spontaneous breathing (no PS or CPAP)
• f/VT of 105 best discriminates between successful and unsuccessful weaning attempts
• RR > 38 also decreases probability of successful extubation

VENTILATOR WEANING
• Patients who pass the screening test should proceed to a SBT
• Once daily T-tube trial
• Multiple T-tube trials
• SIMV
• Pressure support
• Specificity of SBT unknown
• Would require an unethical experiment: extubating all patients who fail a weaning trial and counting number who require reintubation

VENTILATOR WEANING
• Approximately ½ of weaning failure patients develop an é PaCO2 of 10 mm Hg or more during the SBT
• Hypercapnia is uncommonly a consequence of decreased minute ventilation or respiratory drive during wean failure
• Hypercapnia results from rapid, shallow breathing with increased dead space ventilation
VENTILATOR WEANING
• Once daily T-tube trials
• 30-120 minutes
• If unsuccessful, rest on full support at least 24 hours, then repeat
• No form of weaning proven to be superior to this

VENTILATOR WEANING
• Pressure support
• 5-8 cm H2O commonly used to compensate for ETT and ventilator circuit resistance
• Note that if the upper airway is swollen due to several days of intubation, the WOB post-extubation is actually similar to breathing through the ETT without pressure support (AJRCCM 1998; 157: 23)

VENTILATOR WEANING
• Performing trials of SBT once a day is as effective as performing them several times a day (NEJM 1995; 332: 345)
• In patients not expected to pose particular difficulty with weaning, a half-hour trial of spontaneous breathing is as effective as a two hour trial (AJRCCM 1999; 159: 512)
• Weaning duration up to 3x longer with IMV vs spontaneous breathing trials (AJRCCM 1994; 150: 896, NEJM 1995; 332: 345)
VENTILATOR WEANING
• Certain patients may not tolerate abrupt transitions to spontaneous breathing
• Some advanced COPD patients
• Fragile cardiovascular status
• Neuromuscular weakness
• Psychological factors

VENTILATOR WEANING• Extubation
• After passing a SBT, physician must judge whether patient will be able to maintain a patent upper airway and handle secretions
• 10-15% of patients fail and require reintubation (mortality >6x higher among these patients—AJRCCM 1999; 159: 512)
• Post-extubation phase is crucial
• If UAO suspected, be prepared to manage it
• Check for audible air leak on 10-20 cm H20 PEEP or back on AC (not on 5/5)
• Exchange catheter, steroids, racemic epi nebs, heliox, difficult airway kit, bronchoscope
• Cough and deep breathing
• Adequate oxygenation, bronchodilatation
• Airstream hydration
• Maintain a clear central airway and mechanically efficient posture

TOXIDROMES• Cholinergic SLUDGE
• Salivation
• Lacrimation
• Urination
• Defecation
• GI upset
• Emesis
• May see bradycardia, confusion, miosis
TOXIDROMES• Anticholinergic
• Mad as a hatter (delirium)
• Blind as a bat (mydriasis, blurred vision)
• Red as a beet (flushing)
• Hot as a hare (fever)
• Dry as a bone (anhidrosis, dry mucous membranes)
• Tachycardia, thirst, urinary retention

DRUG OVERDOSE• Activated charcoal = best intervention for most orally ingested poisons• Best if given within an hour of ingestion• Can be used with cathartic (sorbitol)• Alcohols and ethylene glycol are not absorbed• Mall ionized chemicals are not well absorbed (metals like Li, iron, electrolytes, acids and alkali)• No definite indications for gastric lavage (contraindicated after acid/alkali ingestions)• Whole bowel irrigation to cleanse bowel for substances not absorbed by AC, sustained release
products and illicit drug packets• Alkaline diuresis for salicylates and barbiturates (Urine pH > 7)• Removed by HD: methanol, EG, ASA, Li, theophylline, amphetamines• Not removed by HD: digoxin, TCA, beta blockers, benzos, phenytoin• Hypotension usually due to venous pooling not myocardial depressionè give isotonic fluids
DRUG OVERDOSE• Acetaminophen toxicity
• AC within 1 hour of ingestion• NAC protocol x 17 doses (most effective within 8 hours)• Transplant center referral if pH < 7.3, Creatinine > 3.3, INR > 6.5, ≥ grade III
encephalopathy (somnolence, hyperreflexia)• Salicylate toxicity
• Tinnitus, respiratory alkalosis, metabolic acidosis (including lactate/ketoacids), noncardiogenic pulmonary edema, cerebral edema, neuroglycopenia (give dextrose), fever due to uncoupling of oxidative phosphorylation, hypovolemia (vomiting, hyperpnea, fever)
• Levels may not peak for 6-36 hours post-ingestion (bezoar, extended release prep, pylorospasm)
• HCO3 drip, alkalinize urine to pH 7.5-8 (must avoid hypokalemia to be effective)• HD indications: AMS, pulmonary or cerebral edema, renal insufficiency preventing
excretion, fluid overload prevents HCO3 administration, > 100 mg/dl in acute OD
DRUG OVERDOSE• Isopropyl alcohol
• Metabolized to acetone (can smell it on the breath)
• Ketonuria
• Osmolar gap but no metabolic acidosis
• Hemodialysis for severe intoxications

DRUG OVERDOSE• Methanol and ethylene glycol poisoning: antifreeze, windshield wiper fluid• Osmolar gap dissipates as alcohols are metabolized and anion gap increases• Pulmonary edema, hypotension, ataxia, seizure, coma• EG metabolized to oxalate (calcium glyoxalate causes renal failure—crystals seen on
Wood’s lamp)• Methanol metabolized to formic acid• Vision disturbance = clue to methanol• Ethanol and isopropyl alcohol cause an osmolar gap but are metabolized to CO2, H2O
and acetone (not an acid), so do not see an anion gap• Fomepizole must be given early if suspected (competes for alcohol dehydrogenase)• Indications for dialysis: visual impairment, renal failure, pulmonary edema, significant or
refractory acidosis, methanol or EG level > 25

DRUG OVERDOSE• Tricyclic antidepressants
• Sedation, coma, seizure, anticholinergic symptoms/signs (fever, flushing, delirium, mydriasis), conduction abnormalities (QT prolongation) with arrhythmia
• QRS >100 msec, R wave in AVR > 3 mm, S in I, AVL (watch for other factors that prolong repolarization: hypoxia, hypocalcemia, hypomagnesemia, hypercarbia, acidosis, drugs)
• HCO3 effective for treating/preventing seizures and arrhythmias (target pH 7.45-7.55)• Push 3 amps for QRS > 100, if narrows, then begin 250 cc/hr drip• May also use benzodiazepines for seizure (no phenytoin)• Hypertonic saline helpful if significant myocardial toxicity• Activated charcoal within 2 hours of ingestion unless ileus or sedated without an ETT:
multiple doses due to enterohepatic circulation• TCAs not dialyzable due to high degree of protein binding
DRUG OVERDOSE• SSRIs
• Nausea/vomiting, dizziness, CNS depression, arrhythmias (HCO3-responsive)
• Serotonin syndrome: agitation, BP fluctuation, fever, tachycardia, tremor, seizure, hyperreflexia, dilated pupils, akathisia, ocular clonus, clonus, diaphoresis
• Activated charcoal
• Cyproheptadine
• Benzodiazepines for sedation
• Beware of other drugs like MAOI, lithium, trazodone, linezolid

DRUG OVERDOSE• Lithium intoxication: nausea, vomiting, diarrhea, ataxia, confusion, agitation, tremors,
myoclonic jerks, seizures, prolonged neuropsychiatric symptoms may be seen (SILENT—syndrome of irreversible lithium effectuated neurotoxicity)
• 2.5-4.0 may be life threatening
• Decreased anion gap = clue
• Activated charcoal does not absorb, consider whole bowel irrigation
• Volume expansion
• Hemodialysis for renal failure or neurologic dysfunction, volume overload, level > 4.0 with acute ingestion or > 2.5 with chronic ingestion (more prone to toxic effects)
• Less chance for rebound with CRRT

DRUG OVERDOSE• Verapamil
• Hemodialysis not effective (protein bound)
• CaCl, glucagon, pacing, lipid emulsion
• Goal of glucagon is to improve BP not HR
• Beta blockers
• Hypotension due to negative inotropy not bradycardia
• IV isotonic fluids, glucagon for symptomatic hypotension or bradycardia
• Treat symptomatic bradycardia with atropine
• Treat seizures with benzodiazepines
• Pacing if refractory to glucagon, vasopressors, IV CaCl, lipid emulsion therapy
COMA• Differential Diagnosis
• Metabolic
• Overdose/poisoning
• Vascular disease
• Infection
• Seizure
• Initial Rx:
• Administer glucose, thiamine, naloxone if opioids suspected
• Assess for seizure, electrolyte disturbance, endocrine function, infection
• Neuroimaging

DELIRIUM• Hypoactive delirium or mixed more common than hyperactive
• Impaired attention, disorganized thinking, may hallucinate• Use CAM-ICU scoring system• Risk factors:
• Age• Acute illness• Sedatives (especially benzodiazepines)• Sleep deprivation• Use of restraints
• Treat pain, re-orientation, avoid sedatives, improve sleep-wake cycles, treat underlying derangements, early mobility (PT)
• Drugs: antipsychotics, a-2 agonist clonidine, dexmedetomidine

OSMOTIC DEMYELINATION SYNDROME• Paresis, dysarthria, dysphagia, coma
• Na always ≤ 120 and ≤ 115 in most cases
• Greatest risk is with Na ≤ 105, hypokalemia, alcoholism, malnutrition, liver disease, and chronic asymptomatic hyponatremia
• Patient types prone to rapid correction and overcorrection
• Normal saline in volume depleted patients
• Steroids in adrenally insufficient patients
• Use of vasopressin antagonists
• 3% saline recipients
PSEUDOTUMOR CEREBRI• Idiopathic intracranial hypertension
• Premenopausal women with papilledema
• Opening pressure > 250
• No etiology on brain imaging
• Treatment: acetazolamide, weight loss, low sodium diet
BRAIN DEATH• Specific criteria vary from state to state and are different in children
• Irreversible coma• Lack of brain stem reflexes• Presence of apnea• No motor response to pain
• Lack of complicating conditions (severe electrolyte/endocrine disturbances, hypotension, hypothermia, CNS depressants, paralytics)
• Two exams by different providers at least 3-6 hours apart• Preoxygenate before conducting apnea test
• Looking for PaCO2>60 mm Hg or 20 mm Hg rise with no respiratory effort• Not possible is marginal acid-base or needing high FiO2 or unstable BP• Nuclear perfusion scan, transcranial dopplers, EEG = ancillary confirmatory tests

STATUS EPILEPTICUS• ≥5 minutes of continuous seizure or ≥2 discrete seizure with incomplete recovery of
consciousness• DDx: epilepsy, stroke, head trauma, SAH, hypoxia, CNS infection (meningitis, encephalitis,
abscess), brain tumor, AVM, drug/ETOH withdrawal, hepatic encephalopathy, uremia, hyponatremia, hypoglycemia, hypocalcemia, hypomagnesemia, drugs (e.g., PCNs, imipenem, cefepime, quinolones, TCA, lithium, lidocaine, flumazenil), paraneoplastic/autoimmune encephalitis (anti-NDMA, Hashimoto’s)
• Prolonged seizure may result in neuronal death and may be an unrecognized cause of coma• Cognitive impairment may occur if >30-120 minutes• Check electrolytes, glucose, drug screen, give thiamine• Lorazepam repeated prn• 2nd line: fosphenytoin, valproate or keppra• 3rd line: propofol, phenobarbital/pentobarbital

NEUROMUSCULAR DISEASE• Guillain Barre
• GI illness like campylobacter may trigger
• Ascending weakness with ê/absent DTRs
• Need for ventilatory support in 10-30%
• May see facial/oropharyngeal weakness in 50%, oculomotor in 15%
• Paresthesias in hands/feet, but mild overall sensory abnormalities
• Dysautonomia in 70% (tachycardia, urinary retention, fluctuating BP, ileus, anhidrosis, arrythymias—often with suctioning)
• Elevated protein in CSF, normal WBC
• AIDP = most common form (AMAN, AMSAN are other variants)
NEUROMUSCULAR DISEASE• GBS signs of impending respiratory failure/need for intubation (avoid succinylcholine)
• FVC < 20 ml/kg• MIP < −30 cm H2O• MEP < +40 cm H2O
• GBS predictors of respiratory failure• Time of onset to admission < 7 days• Inability to cough• Inability to stand• Inability to lift elbows/head off bed• Elevated LFTs
• Steroids do not help• IVIG or PLEX

NEUROMUSCULAR DISEASE• Myasthenia gravis: fluctuating weakness in ocular, bulbar, limb and respiratory muscles• AChR or MuSK antibodies present in 90% with generalized disease• Decremental conduction with repetitive stimulation, edrophonium test• Muscle fatigue (worse late in day or after exercise)• Ptosis, diplopia• May see dysarthria, dysphagia, fatigable chewing• Drugs may worsen/unmask
• Aminoglycosides, clindamycin, fluoroquinolones, vancomycin, beta blockers, quinidine or procainamide, magnesium, hydroxychloroquine
• Consider intubation for VC < 5 ml/kg or MIP < −30 mm Hg• Pyridiostigmine (once improved, increased secretions during crisis), steroids,
immunomodulators, IVIG or PLEX

NEUROMUSCULAR DISEASE• Critical illness polyneuropathy: neurologic manifestation of SIRS
• Sensorimotor polyneuropathy with limb weakness/atrophy, êDTRs, êlight touch/PP, difficulty with vent weaning unrelated to cardiopulmonary causes
• Especially with ICU stays ≥ 2 weeks
• Sepsis (with MOF), poor glycemic control
• Critical illness myopathy
• Flaccid quadriparesis (proximal > distal), failure to wean, elevated CPK
• IV steroids major risk factor ( 1/3 or status asthmaticus and COPD in prospective trials)
• Paralytic drugs
• Hyperglycemia
• Hyperthyroidism

BACTERIAL MENINGITIS• Early antibiotics crucial immediately after stat cultures/LP
• If CT needed before the LP then give antibiotics first
• Dexamethasone 10 mg q6 x 4 days, first dose 15 minutes before antibiotics (most benefit in S. pneumoniae)è decreased mortality and improved neurological endpoints
• 2-50 year oldè vanc, ceftriaxone
• >50 year old, immunocompromised, diabeticè add ampicillin for listeria coverage
• If in setting of penetrating trauma, neurosurgery or CSF shunt use vanc + cefepime, ceftazidime or meropenem
• Lymphocytic meningitis with low glucose = TB until proven otherwise
• Meningococcus: purpura, younger patient, arthritis
HSV ENCEPHALITIS• Temporal lobe localization on MRI
• CSF PCR is gold standard (viral culture is poor)
• Rx: acyclovir
• If no red cells on LP can dismiss this
BRAIN ABSCESS• MR preferred imaging tool
• LP contraindicated
• Biopsy or aspiration for diagnosis
• Combined medical and surgical approach
• < 2.5 cm lesion or if multiple abscesses may just have medical therapy alone
• Steroids if cerebral edema/mass effect
STROKE• > 90% ischemic, 10% hemorrhagic• Initial work up: basic labs, coags, noncontrast head CT, NIH stroke scale, look for stroke mimics and
contraindications to lytics• Ensure adequate oxygenation and perfusion• Avoid overcorrecting HTN• Treat if BP > 220/120• If post thrombolysis then want BP < 185/110• DVT/GI prophylaxis• Avoid fever• Glycemic control important but avoid hypoglycemia• Time window for lytics is 4.5 hours• 6% have significant bleed with tPA• No benefit to hyperbaric O2, heparin, hypothermia or acute carotid surgery• Embolic strokes = 2nd most common etiology (can be multiple, max deficit at onset, anticoagulate once
certain there is no hemorrhagic conversion at 48 hours)• Do not anticoagulate infectious embolic strokes

HEMORRHAGIC STROKE• Intracerebral hemorrhage: chronic HTN, cocaine, tumor, anticoagulation• SBP < 160, reverse • Seizures more likely with hemorrhagic strokes (prophylax only if witnessed seizure)• For cerebellar hemorrhage, surgical intervention is most effective (> 3 cm posterior
fossa bleed, brainstem compression)• SAH: look for ECG changes, elevated cardiac enzymes, LV dysfunction (Takotsubo’s)
due to excess catecholamine release• Rebleeding in 10-15% in first 24 hours• Open clipping or endovascular coiling• Up to 70% have vasospasm with secondary morbidity (day 3-14)• Nimodipine reduces ischemia associated with vasospasm• HHH therapy (hypervolemia, hypertension, hemodilution) if spasm identified,
angioplasty, intra-arterial vasodilators

COMMON COMPLICATIONS OF STROKE• Pneumonia
• GI bleed
• CHF
• Cardiac arrest
• DVT/PE
• UTI
DELIRIUM TREMENS• Insomnia, tremulousness, anxiety, GI upset, headache, diaphoresis,
palpitations, agitation, tachycardia, hypertension, fever, disorientation 48-96 hours (up to 7 days)
• Seizure 12-48 hours after last drink: singular or flurry usually (do not use phenytoin, use benzos or phenobarb)
• Mortality up to 5%
• Alcoholic hallucinosis: no clouding of sensorium
• IVFs, thiamine, folate, quiet, dimly lit environment, NPO
• Benzodiazepines, propofol, phenobarbital
• Avoid haldol which lowers seizure threshold
WERNICKE’S ENCEPHALOPATHY• Encephalopathy (disorientation, indifference, may be agitated if concomitant
ETOH withdrawal), oculomotor dysfunction, ataxia, nystagmus, evidence of protein calorie malnutrition
• Blood thiamine level may not reflect brain level
• Check erythocyte thiamine transketolase level before and after thiamine

HYPERAMMONEMIA• Liver disease
• Medications (valproate)
• Seizure
• UTI with urease splitting organism (Proteus, Klebsiella, Pseudomonas, Staph)
• Hyperalimentation
• Inborn errors of metabolism
• Hypokalemia (increased renal ammoniagenesis)
SEROTONIN SYNDROME• Anxiety, agitated delirium, diaphoresis, tachycardia, fever, hypertension, vomiting,
diarrhea, tremor, muscle rigidity, akathisia, myoclonus, hyperreflexia, Babinski sign, clonus, slow rolling continuous eye movements (ocular clonus), dilated pupils, autonomic instability
• Seritonergic agents: amphetamines, cocaine, MDMA, levodopa, SSRIs, SNRIs, trazodone, TCAs, valproate, carbamazepine, dextromethorphan, fentanyl, lithium busiparone
• Avoid physical restraints: may lead to hyperthermia, lactic acidosis
• Sedate with benzodiazepines
• DDx may include NMS, anticholinergic toxicity, lithium poisoning, manic episode, drug intoxication

NEUROLOGIC COMPLICATIONS OF CANCER• Brain metastases
• Leptomeningeal carcinomatosis
• Cord compression syndrome
• Radiation effects
• Seizure
• Paraneoplastic (hyponatremia, hypercalcemia, encephalitis)
• Stroke from nonbacterial thrombotic endocarditis (sterile fibrin vegetations)
ACUTE PSYCHOSIS• Primary psychiatric disorder (schizophrenia/BPD)
• Substance or withdrawal induced
• Hyperthyroid or adrenal insufficiency
• Hepatic or uremic encephalopathy
• Infectious disease (HSV, HIV, syphilis)
• Anti-NMDA encephalitis, SLE cerebritis
• Seizure disorder
• B12 deficiency
• Check B12, VDRL, LFTs, TSH, drug screen, HIV, CTD serologies, heavy metal screen
STEMI• Revascularization in all STEMIs (including new LBBB) within 12 hours• PCI preferred with goal of 90 minutes door to balloon (120 min if transfer required)• If cannot meet that time frame then fibrinolysis within 30 minutes of arrival• PCI preferred in cardiogenic shock even if delayed or C/I to fibrinolysis (ICH, tumor, stroke
within 3 months, active bleeding, trauma, uncontrolled HTN)• Dual antiplatelet with ASA/clopidogrel recommended early• Give UFH (or enoxaparin or bivalrudin): can shut off after revascularization in cath lab• Fondaparinux contraindicated as sole anticoagulation due to ↑ catheter thrombosis after PCI• Beta blockade within 24 hours (po) unless CHF/heart block• IV beta blocker and NTG if hypertensive• ACEI within 24 h if EF ≤ 40% or anterior MI• Add aldosterone if already on ACEI• High intensity statin therapy
UNSTABLE ANGINA AND NSTEMI (ACS)• Chest pain at rest or é troponin without ST elevation or LBBB• Anticoagulation, ASA, beta blockade• NTG if persistent CP (do not give if patient takes sildenafil)• O2 if hypoxic• TIMI risk score ≥ 3 is high riskè invasive strategy (often for 2 also)
• Age > 65• 3 risk factors for CAD• Prior stenosis > 50%• ST ê on ECG• At least 2 anginal episodes in last 24 h• Elevated troponin• Use of ASA in prior 7 days
ACUTE CORONARY SYNDROME• Invasive strategy
• 4-48 h of admission• CABG for 2+ vessel disease and diabetics• PCI for single vessel disease or if too sick for surgery• Dual antiplatelet therapy if stent placed, otherwise long term ASA
• Conservative strategy (renal insufficiency tilts toward this)• Statin• Beta blockade• ACEI/ARB• ASA• PY12 inhibitor depending on risk/benefit of bleeding vs future events

TACHYARRYTHMIA• DC cardioversion always right answer for unstable patient with tachyarrythmia
• Narrow complex regular: 50-100 J synchronize
• Narrow complex irregular: 120-200 J
• Wide, regular: 100 J (VT or Aflutter with aberrancy)
• VT, stable with pulse: amiodarone or lidocaine, synch cardioversion 100 J
• Polymorphic VT: Mg or lidocaine, synch cardioversion 100 J
• Ventricular fibrillation: 200 J with biphasic defibrillator, Epi 1 mg or vasopressin 40 U, amio 300 mg if persistent
• If defibrillation not successful then CPR x 2 minutes before another attempt
• SVT: adenosine, vagal maneuvers
• AV blockade not recommended for WPW (amiodarone, procainamide)
TACHYARRYTHMIA• New tachyarrythmia with hemodynamic compromise è immediate synchronized
cardioversion
• If more stable, check 12-lead
• Hemodynamically stable monomorphic VT è amio bolus then infusion
• Most common side effect is hypotension (up to 25%)
• Indications for cardioversion
• Altered mental status
• Shock
• Angina
• Shortness of breath
TAMPONADE• Shock
• Chest pain, dyspnea, fatigue
• Elevated JVP, venous distention over forehead
• Peripheral edema
• Tachycardia
• >10 mm drop in SBP during inspiration
• Electrical alternans
• Diastolic collapse of the RA and RV
• Avoid positive pressure ventilation which may decrease preload further
CARDIAC ARREST• Out of hospital usually due to MI or arrhythmia (sometimes overdose, drowning, trauma)
• Survival to discharge 5-15%• Hypothermia indicated in VF/VT OHCA• Rapid IV cooling in the field led to more re-arrests• Maintain sats 95-98%, but hyperoxia may be bad• Consider cath for ST elevation or LBBB, trop > 5 and VF presentation
• In hospital arrest• 1/3 respiratory failure• 1/3 cardiac etiology• 1/3 MSOF• Survival to discharge 30% due to prompt CPR

THERAPEUTIC HYPOTHERMIA• 32-34 degrees x 12-24 hours post-arrest (start within 6 hours) then passive rewarming
• For neuroprotection not acute survival (+neuro outcomes in 55% vs 39% with usual care)
• Not proven for in-house arrests or non-Vfib arrests
• Untoward potential effects
• Coagulopathy (contraindicated if active bleeding or hemorrhagic stroke)
• Immune suppression (leukopenia, impaired migration/phagocytosis)
• Cold diuresis with electrolyte shifts (↓ K, Mg, PO4)
• Cardiovascular dysfunction
• Acid-base disturbances
• Hyperglycemia
AICD INDICATIONS• LVEF < 40% and nonsustained VT
• LVEF < 35% with NYHA II or III (NYHA IV are too sick and will not be benefitted)
• LVEF < 30% in ischemic cardiomyopathy
• If recent MI wait 40 days after revascularization before EF is determined
• If VF/VT in hospital > 48 h after MI or the patient presents with MI and cardiac arrest

AORTIC DISSECTION• Acute onset of pain (back/chest), pulse deficit, > 20 mm Hg BP differential, diastolic heart murmur (AI), focal
neuro deficits, syncope/hypotension, mediastinal widening
• Diagnosis: TEE or CT angiogram• Causes
• Hypertension• Connective tissue diseases (e.g., Marfan’s/Ehler’s Danlos syndrome)
• Pregnancy• Cocaine
• Bicuspid aortic valve or preexisting aneurysm• Vasculitis (Takayasu, Giant cell, syphilis, RA)
• Ascending dissection = 20% mortality, immediate surgical intervention
• Descending dissection < 10% mortality, IV beta blockers (HR < 60, BP < 120)• Some evidence for endovascular (vs surgical) repair with improved outcomes if there is evidence of end
organ ischemia
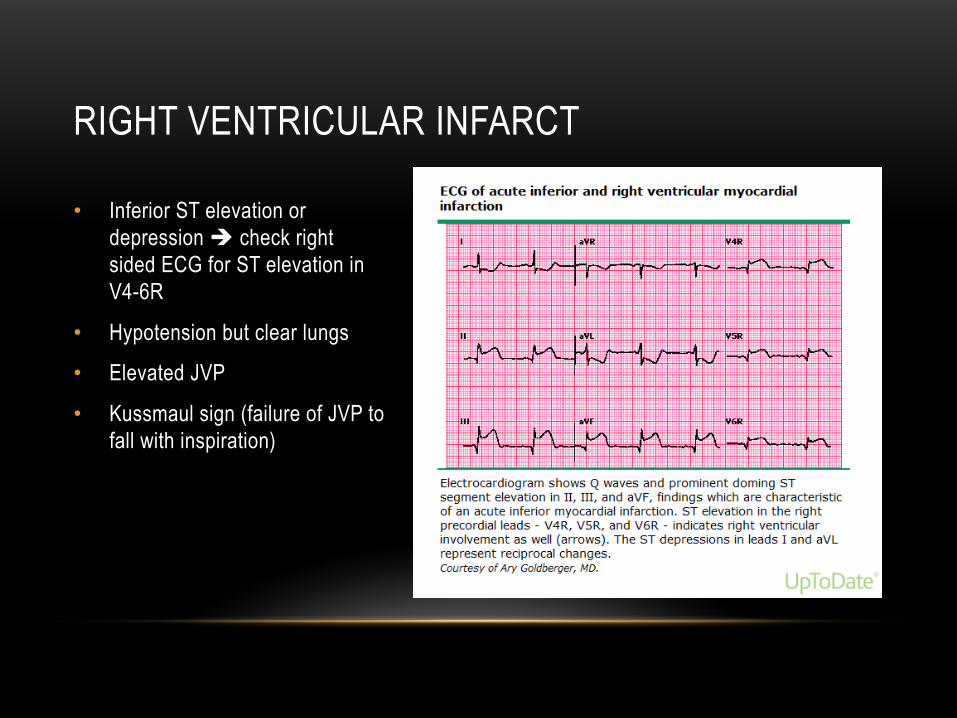
RIGHT VENTRICULAR INFARCT
• Inferior ST elevation or depression è check right sided ECG for ST elevation in V4-6R
• Hypotension but clear lungs
• Elevated JVP
• Kussmaul sign (failure of JVP to fall with inspiration)

PRINZMETAL ANGINA• Vasospastic angina
• Rest angina with ST elevation
• H/O migraines or Raynaud’s phenomenon
• ASA and beta blockers can precipitate!
• Intracoronary acetylcholine or hyperventilation may precipitate
• Smoking cessation, nitrates, calcium channel blocker

SUDDEN DEATH IN PATIENT UNDER 30 • Hypertrophic cardiomyopathy
• Rule out with ECHO
• Anomalous right coronary artery
• Young patient with CP, syncope with activity, ST elevations, ventricular tachycardia
• Check MRCA
STROKE RISK IN ATRIAL FIBRILLATION• Anticoagulation decreases stroke risk by 70% and improves mortaliy
• Dabigatran = direct thrombin inhibitor
• Lower rates of embolic and hemorrhagic strokes vs coumadin
• Rivaroxaban but not dabigatran may be reversed with PCC
TAKOTSUBO CARDIOMYOPATHY• Stress cardiomyopathy (consider when death in family, domestic abuse, catastrophic
medical diagnoses, natural disasters, major financial loss, severe acute illness like SAH)
• ST elevation (44%) and/or ST depressions or T wave inversions
• Modest elevated troponins
• Clean coronaries
• Signs of left heart failure
• Post-menopausal women after acute emotional stres
• Apical akinesis with hyperkinesis of the basal walls
• R/O ACS, cocaine-induced ACS, myocarditis and pheochromocytoma
MAT• Atrial distention
• COPD, CHF
• Hypokalemia, hypomagnesemia, beta agonists, chronic renal failure, poor oxygenation, acid-base imbalance
• May be due to triggered activity (like Torsades) and Mg repletion may help even with normal serum levels
• Treat with verapamil or beta blockers
PERICARDIAL EFFUSION• Idiopathic
• Malignancy
• Uremia
• Post myocardial infarction (Dressler’s)
• Infection (coxsackie, echovirus, TB, staph, fungal)
• Collagen vascular disease
• Hypothyroid
• Rare: FMF, IGG4-related disease, Whipple’s, GCA, GPA, Behcet’s, sarcoid, IBD)
HYPERTENSIVE EMERGENCY• SBP ≥ 180, DBP ≥ 120 with signs or symptoms of end organ damage
• Acute neurologic symptoms (HA, agitation, delirium, stupor, confusion, vision changes)
• Stroke
• Papilledema, flame hemorrhages
• N/V (increased ICP)
• CP or back pain (dissection or angina)
• SOB (pulmonary edema)
HYPERTENSIVE EMERGENCY• Check for cocaine, amphetamines or recent stopping of clonidine or beta blockers• Do not lower BP too quickly or too much except in acute dissection (want SBP 100-120 mm
Hg in 20 minutes)• Nicardipine has better safety profile with similar efficacy vs nitroprusside• Excessive drop in BP may cause stroke, MI, blindness• Hypertensive encephalopathy: 10-20% acute BP drop, 25% by 24 hours• Acute stroke: treat if BP ≥ 220/120, or 185/110 if lytic candidate• Cardiac emergency (acute heart failure): diuretics, nipride or NTG targeting 10-15%
(avoid drugs that increase cardiac work [hydralazine] or acutely decrease contractility [labetalol])
• Renal emergency: fenoldopam associated with temporary improvement in renal function• Cocaine/amphetamine OD: phentolamine or nipride• NTG causes venodilation > arterial, may see methemoglobinemia if > 24 hr use
COCAINE INDUCED MI• Do not give succinylcholine if intubating (plasma cholinesterase
metabolizes cocaine, and patients may also have rhabdomyolysis and develop hyperkalemia after succinylcholine)
• Use benzodiazepines for agitation
• Phentolamine (a blocker) for HTN
• No b blockers (unopposed a worsens coronary constriction)

ELEVATED CVP + SHOCK DIFFERENTIAL DX• Pulmonary embolism
• Acute MI
• Tension PTX
• Pericardial tamponade
PULMONARY EMBOLISM
• Obstruction of pulmonary arterial branches by material arising elsewhere in the body
• Venous thrombi
• Air
• Tumor
• Amniotic fluid
• Fat
• Necrotic bone marrow (sickle cell crisis)

PULMONARY EMBOLISM
• 65-90% of PEs arise from deep veins in the LEs
• May originate in pelvic veins, renal veins, UEs or right heart
• 50-80% of LE DVTs arise in calf veins and propagate proximally
• 20-30% of calf vein thrombi extend proximally if untreated
• Pulmonary emboli are usually multiple
• 10% of PEs cause pulmonary infarction (usually in patients with preexisting cardiopulmonary disease
• The majority of PEs are never diagnosed
PULMONARY EMBOLISM
• D-dimers
• Rapid ELISA test
• Elevated levels above 500 ng/ml seen in nearly all patients with PE
• Low levels help exclude PE (94% NPV), especially when paired with low pretest probability
• Use with caution in patients other than low-risk outpatients
• Specificity very low
• D-dimers also elevated in recent surgery, malignancy, trauma, severe infection, pregnancy, DIC, liver disease
PULMONARY EMBOLISM
• Causes of hypoxemia
• Altered V/Q ratios due to vascular obstruction, and the release of vasoactiveand bronchoactive substances
• Increased dead space
• Increased PVR due to mechanical obstruction and vasoconstriction due to hypoxia, neural reflexes and mediator released from activated platelets
• Atelectasis due to surfactant dysfunction distal to the embolus or splinting from pleuritic pain
• Impaired cardiac output with ¯ MVO2
• Intracardiac shunting through PFO

PULMONARY EMBOLISM
• Major risk factors
• Immobilization
• Surgery within the last three months
• Stroke
• Paresis/Paralysis
• History of venous thromboembolism
• Malignancy
• Central venous instrumentation within the last three months
• Chronic heart disease
• Additional risk factors in women may include obesity (BMI ≥29 kg/m2), heavy cigarette smoking (>25 cigarettes per day), estrogen therapy, and hypertension

PULMONARY EMBOLISM
• Conditions associated with thrombophilia
• Activated protein C resistance (Factor V Leiden mutation)
• APLA syndrome
• Prothrombin gene mutation 2021A
• Protein C or S deficiency
• Antithrombin III deficiency

PULMONARY EMBOLISM
• Symptoms • Dyspnea 73%• Pleuritic chest pain 44%• Leg pain 44%• Cough 34%• > 2 pillow orthopnea 28%• Wheezing 21%
• Signs• Tachypnea 54%• Tachycardia 24%• Rales 18%• ¯ breath sounds 18%• P2 15%• JVP 14%

PULMONARY EMBOLISM• Submassive: acute PE without hypotension but with either RV dysfunction or myocardial
necrosis (RV dilatation on CT/ECHO), é BNP, é troponin or ECG changes• Massive: sustained hypotension, pulseless or profound bradycardia• D-dimer helpful for ruling out PE in low to moderate risk patients• If high pretest probability then ignore the D-dimer• CT angio for Well’s score > 4• V/Q good if low probability and low clinical suspicion (no PE) or high probability and high
clinical suspicion ( PE)• Factors increasing risk of death in PE: massive PE, RV dysfunction, elevated
troponin/BNP, RV thrombus, coexisting DVT, hyponatremia, elevated lactate• Avoid volume induced RV overdistention• RV failure may lead to hypotension during intubation
PULMONARY EMBOLISM• LMWH or fondaparinux preferred over UFH
• IV UFH preferable for
• Persistent hypotension (massive PE)
• Increased bleeding risk (easier reversal)
• Thrombolysis being considered
• Renal failure
• Concern for SQ absorption (anasarca, morbid obesity)
• Dabigatran and rivaroxaban noninferior to standard Rx in stable patients (not for critically ill)
• HIT è argatroban or bivalrudin
PULMONARY EMBOLISM• Thrombolytics
• Improved pulmonary arterial hemodynamics, oxygenation and RV function at 24 hours• Probably improved survival in massive PE
• Major bleeding 13% vs 6% with heparin
• FFP, cryoppt, aprotinin for major lytic induced hemorrhage• Contraindications
• Ischemic stroke within 3 months• AVM
• Prior ICH• Active bleeding• Recent brain/spinal surgery
• Recent head trauma with fracture or brain injury• Known malignant intracranial lesion
• Bleeding diathesis

PULMONARY EMBOLISM• Massive PE = BP < 90 or 40 mm drop from baseline for > 15 minutes• Mortality with shock is 30-50%• Untreated PE mortality is 30% (mostly recurrent embolism)• 2-8% with treatment • RV dysfunction predicts increased PE related mortality• PE + DVT = increased mortality• NTproBNP > 600: 16x increased mortality in metanalysis• Elevated troponin: 9x increased mortality• Hyponatremia (especially < 130) associated with increased mortality• Massive PE is only clear indication for tPA• Submassive PE with elevated BNP/troponin, marked tachycardia, severe RV
dysfunction, residual DVT, high O2 requirements may be considered for lytics
PULMONARY EMBOLISM IN PREGNANCY• D-dimer not recommended
• Suspect PE and DVTè compression U/S of lower extremities first
• Note that clots often originate from compressed veins in abdomen/pelvis
• Suspect PE with no signs of DVT and normal CXRè V/Q scan
• Abnormal CXR or nondiagnostic V/Qè CT angio
• LMWH preferred for treatment and prevention of PE and DVT in pregnancy

STAPHYLOCOCCAL TOXIC SHOCK SYNDROME• Tampon use in menstruation, wound infections, mastitis, sinusitis, osteomyelitis, skin
lesions, burns, post-influenza pneumonia• TSST-1 exotoxin = superantigen capable of activating large numbers of T cells
simulaneously• Fever, hypotension, erythroderma (may be fleeting, desquamation after 1-2 weeks),
myalgias, weakness, GI symptoms, elevated CPK, encephalopathy• Need involvement of at least 3 organ systems: GI, muscle, mucous membranes
(hyperemia), renal, hepatic, hematologic (plt < 100K), CNS• Staph usually isolated from mucosal site or wound (only 5% BCx positive)• Vancomycin plus clindamycin, or Linezolid• Remove source• IVIG may help neutralize the toxin

GROUP A STREPTOCOCCAL TOXIC SHOCK• Shock and multiorgan failure, diffuse capillary leak
• Main distinguishing feature between GAS TSS and S. aureus TSS is that patients with GAS are bacteremic, while patients with Staph TSS usually have negative BCx
• May occur in setting of necrotizing fasciitis or myonecrosis
• Diagnosis of GAS TSS requires isolation of strep from a normally sterile site
• Rash like sunburn but involving palms/soles
• Mucosal involvement: conjunctival-scleral hemorrhage, hyperemia of oropharyngeal mucosa
• Clindamycin 900 mg IV q8 + carbapenem or Pip-tazo as empiric therapy
• Clindamycin + PCN G once diagnosis established
• IVIG may improve mortality
PNEUMONIA IN ICU• Pneumococcus is most common pathogen in pneumonia requiring ICU admission
• Pseudomonas risk: bronchiectasis, COPD, frequent antibiotic or glucocorticoid use, hospitalized
• MRSA risk: hospitalized, post-influenza, contact sports, IV drug use, prisoners
• CA-MRSA: more sensitive but more virulent, necrotizing pneumonia
NEUTROPENIC FEVER• T > 38 for > 1 hour or T > 38.3
• Noninfectious etiologies: engraftment, blood transfusions, drugs, cytokines
• 20-30% have documented infections
• First fever is rare to be fungal related
• Monotherapy with cefepime or carbapenem
• Add vancomycin if hypotensive, pneumonia, BCx + for GPC, SSSI or suspected catheter-related infection
• May add aminoglycoside or quinolone for unstable patients
• Add antifungal if febrile after 4-7 days of antibacterials with no fever source identified
• Echinocandins are drug of choice for candidemia in neutropenic patients
• If worried about mold, add voriconazole (DOC for invasive aspergillosis)

NEUTROPENIC FEVER• Bacteremia in 10-25%
• Most infections are GPC
• GNR infections are more severe
• May see fungi or viruses
• Lungs, abdomen, IV catheters, urine, skin = common sources
• Nodules or ulcers suggest fungi, NTM
• Vesicles suggest viruses
• Erythema gangrenosum suggests pseudomonas
• Check galactomannan, fungitell, C diff, respiratory viral DFA, LP if fever/HA/AMS

NECROTIZING SOFT TISSUE INFECTIONS• Systemic toxicity (hypotension, AKI, delirium)
• Pain out of proportion to exam findings
• Bullae, hemorrhage, sloughing
• Crepitus or wooden-hard feel
• Skin anesthesia (undermining of nerves going to the skin by deep tissue infection)
• Rapid progression despite antibiotics
• Group A strep or Staph aureus or polymicrobial (including anaerobes)
• Debridement
• Carbapenem or Zosyn + vancomycin and clindamycin (for toxin production)
COMMON CAUSES OF WBC>30K IN ICU• Clostridium difficile colitis
• Candidal sepsis
• Closed space infection (e.g., abscess/empyema/necrotic gallbladder/perforated viscus)

TYPHLITIS• Neutropenic enterocolitis
• Fever, abdominal pain (especially RLQ), neutropenia
• Check Abd CT with contrast
• DDx: cholangitis, cholecystitis, Ogilivie’s syndrome, CMV, C diff colitis
• Bowel rest, NG suction, IVFs, antibiotics (Vanc + Zosyn or ceftazidime + flagyl, or Vanc/Merrem), GCSF

ACUTE PANCREATITIS• Gallstones, alcohol, hypertriglyceridemia, post-ERCP, drugs, pregnancy, infections, vasculitis,
hypercalcemia, idiopathic• Can feed as pain/inflammatory markers ê if no ileus/N/V, enteral route preferred• No prophylactic antibiotics unless > 30% necrosis (no longer than 14 days)• Early necrosectomy (48-72 hr) a/w é mortality vs delayed (> 12 days)• Drain any abscess (but not acute peripancreatic fluid collections without walls)• 5-10 cc/kg/hr isotonic fluids initially (avoid LR if hypercalcemic)• Want HR < 120, MAP 65-85, UO > 0.5-1 cc/kg/hr, êBUN in first 24 hr• êUO may mean ATN or underresuscitation• Caution with high fluids after 48 hrs (respiratory failure, abdominal compartment syndrome—
monitor bladder pressures)• Hydromorphone or fentanyl analgesia• Avoid glucose > 200 mg/dl, may be associated with increased pancreatic infections

ACALCULOUS CHOLECYSTITIS• Post-operative patients, DM, EBV/CMV/HIV, candida infection, TB, TPN, chronic critical
illness, AML, BMT, CHF, sepsis, hypotension, vasculitis, ESRD, multiple transfusions, CPR, burns, major trauma
• Origin is biliary stasis and ischemia
• Consider in any critically ill/injured patient with sepsis or jaundice or unclear etiology
• GB wall thickening > 5 mm, pericholecystic fluid, Murphy’s sign, GB distention > 5 cm, mucosal sloughing, emphysematous cholecystitis, failure to opacify GB on HIDA scan (sens ~67%)
• Cholecystostomy tube with delayed cholecystectomy
• Failure to improve after C-tube may indicate gangrene or bile leakage or wrong Dx
• Amp-sulbactam or Pip-tazo or ceftriaxone/metronidazole or cipro/metronidazole or carbapenem monotherapy
CLOSTRIDIUM DIFFICILE• Prior antibiotics (esp FQs, clindamycin, cephalosporins, PCNs). Aminoglycosides do not cause• Age > 65• Use of PPI, H2B• Enteral TF• Recent hospitalization• Fever in 10-15%, WBC > 30K in 25% • Dx: PCR testing• Watch for toxic megacolon• Treatment
• Enteral vancomycin plus IV flagyl in critically ill (IV flagyl addition especially if there is an ileus, often with vancomycin retention enema)
• Surgical consult if WBC ≥ 20,000, lactate > 2.2, severe ileus• Some may need higher dose po vanc, vanc enemas or addition of fidaxomicin or rifaximin

UPPER GI BLEED• DDx: PUD, esophageal varices, PHG, UGI tumors, Dieulafoy lesion (aberrant submucosal
artery that erodes epithelium in absence of ulcer), Cameron lesion (erosion/ulcer within hiatal hernia), hemobilia, aortoenteric fistula
• Overall mortality for UGIB requiring transfusion = 10%• 2 large bore IVs• Restrictive transfusion strategies do not apply to acute bleeding• Target Hgb > 7 mg/dl unless acute MI, then 10 mg/dl• PPI reduces rebleeding risk in PUD but doesn’t stop acute bleeding• Therapeutic EGD with electrocautery, injection, clipping• Surgery and IR equally effective if endoscopy fails• Recent metaanalysis showed no difference in rebleeding, need for surgery or mortality
with continuous high dose PPI drip vs non-high dose oral or IV PPI (but drip still recommended)

UPPER GI BLEEDING• Variceal hemorrhage
• 50% stop bleeding spontaneously (vs 90% for other causes)• Rebleeding risk highest in first 72 hrs
• Age > 60, renal failure, large varices, hgb < 8 on admission, red wale, ascites• ~20% 30 day mortality for acute variceal hemorrhage• If survive first two weeks, 1 year survival is 50%• 20% cirrhotics with GIB infected at presentation and additional 50% will become infected
(UTI, SBP, pneumonia, primary bacteremia)• Antibiotics decrease infections and possibly mortality and rebleeding (ceftriaxone > FQ)• Target hgb 7 mg/dl, UO ≥ 50 cc/hr, avoid VO, correct coags (may not be able to with FFP,
?rfVIIa), monitor for ETOH withdrawal, give thiamine, watch K/PO4• Octreotide x 72 hrs (no mortality benefit)

ACUTE LIVER FAILURE• Acetaminophen, ischemia, pregnancy associated with better short term survival than DILI,
autoimmune or hep B• NAC for acetaminophen toxicity• If etiology not clear, give NAC (may be beneficial in non-acetaminophen ALF)• Antiviral therapy for hep B• TIPS or thrombolysis in Budd Chiari• Acyclovir in HSV• Steroids in autoimmune hepatitis• Forced diuresis and charcoal in mushroom poisoning, silibinin IV• Lactulose and rifaximin ê NH3 (unclear if that ê intracranial HTN risk)• ICP monitoring controversial, no improved outcomes in non-randomized trials• ICP > 25, osmotic therapy as bridge to transplant• MELD > 40 = 20% 3 month survival

ACUTE LIVER FAILURE• Vitamin K for all with coagulopathy in liver failure
• FFP does not reliably affect coagulation and may worsen cerebral edema
• Liver failure patients have increased bleeding risk (ê factor II, V, VII, IX, X XI, XIII, ê platelets)
• Also é thrombotic risk (ê protein C/S, AT levels, é factor VIII and vWF)
• Increased INR in liver patients does not protect from thrombosis
• Albumin with LVP è less hypotension and renal failure, ê mortality

SPONTANEOUS BACTERIAL PERITONITIS• > 250 PMNs
• E coli, K pneumoniae, Streptococcal sp
• SAAG > 1.1 g/dl = portal HTN
• Secondary bacterial peritonitis (perforation like PUD or nonperforation like perinephric abscess) in 1/20 cases of SBP
• Do not see surgical abdomen due to deparation of visceral/parietal surfaces
• WBC > 5-10K may suggest secondary cause
• Polymicrobial
VARICEAL HEMORRHAGE• Only 50% stop bleeding spontaneously vs 90% for other causes of UGIB
• Highest rebleeding risk in first 72 hours:
• Age > 60, renal failure, large varices, Hgb < 8 at admission, red wale sign, ascites
• Acute variceal bleed associated with 15-20% 30 day mortality
• Of those who survive the first two weeks, 50% will be dead at 1 year
• 20% of cirrhotics with GIB are infected at time of admission, and an additional 50% will become infected
• Prophylactic antibiotics reduce infections, mortality and rebleeding risk

HEPATIC ENCEPHALOPATHY RISK• GI bleed• Infection• Hypokalemia (causes increased renal ammoniagenesis)• Metabolic alkalosis• Renal failure• Hypovolemia• Hypoxia• Sedative use• Hypoglycemia• Constipation • Can use po vancomycin, metronidazole or rifaximin with lactulose if lactulose is
ineffective (must correct hypokalemia)
HYPERLEUKOCYTOSIS• Leukostasis: increased viscosity, plugs in microcirculation, endothelial damage
from cytokines, hemorrhage, diffuse interstitial or alveolar infiltrates
• SOB, hypoxia (with or without diffuse infiltrates), HA, dizziness, confusion, somnolence, ataxia, fever, DIC in up to 40%, spontaneous TLS in 10% (watch uric acid, K, PO4)
• Pulsox more accurate than ABG (O2 consumption in the syringe by WBCs)
• Fever common with or without infection
• Cytoreduction measures: chemotherapy, hydroxyurea, tyrosine kinase inhibitor, leukapheresis
• Leukapheresis when > 50K blasts when unable to do induction chemo and have symptoms
• Hydroxyurea can reduce WBC > 50% within 24-48 hours
PREGANCY AND CRITICAL CARE• Pre-eclampsia: HTN, edema, proteinuria after 20 weeks (can occur post-partum)
• Most severe complication is HELLP syndrome• Eclampsia is defined by seizures• Treatment = delivery of the fetus and placenta, BP control (hydralazine or methyldopa),
magnesium• Amniotic fluid embolism
• Abrupt onset of severe dyspnea, hypoxemia, cardiovascular collapse, altered mental status or seizure most often after delivery
• Supportive treatment• Risk of failed extubation 4-6x greater in pregnant patient• Normal PaCO2 30-32 near term• Maintain PaO2 > 80 mm Hg in pregnant patients to ensure fetal oxygenation• Phenylephrine is pressor of choice in pregnancy

HYPOTHERMIA• Mild 32-35°: confusion, impaired judgment, paradoxical undressing
• Moderate 28-32°: ê HR/CO, hypoventilation, stupor, arrhythmias (hypothermic heart is very sensitive to movement), muscle rigidity
• Severe < 28°: obtunded, appear dead, high risk of VF, pulmonary edema, oliguria, hypotension, bradycardia
• Passive external rewarming for mild hypothermia
• Active external rewarming (bear hugger, warming blankets) for moderate-severe hypothermia (risk of recirculating cold blood so limit warming to the trunk)
• Active core rewarming with warm IVFs, lavage, venovenous ECMO for severe hypothermia or nonperfusing rhythm
MALNUTRITION• > 40% of hospitalized patients are malnourished on admission
• é mortality, LOS, risk of infection, ê wound healing
• 25 kcal/kg/d, 1.2-1.5 g/kg/d protein
• TPN associated with worse outcomes such as new infections, longer mechanical ventilation, longer hospital stay
• Enteral nutrition is associated with aspiration/VAP risk, but overall less infections vs TPN
• Some evidence that early enteral feeding within 48 hrs may have better survival
• Trophic feeds in ARDS as good as full rate (no change in mortality or ventilator free days and better sugar control)
• Omega 3 FA in ARDS: study stopped early for futility

THROMBOCYTOPENIA IN ICU• Sepsis is the most common cause in medical patients who are not bleeding (though
usually not severe)• Drug-induced {antiepileptics, antibiotics (linezolid, piperacillin, TMP-SMX, vancomycin,
rifampin), H2 blockers, anti-plt drugs, HIT}• Hemodilution• Blood loss• DIC: MAHA, tissue ischemia and bleeding, é PT/PTT, ê fibrinogen, é D-dimer/FDPs in
setting of sepsis, trauma, malignancy, pregnancy• ITP• TTP/HUS: MAHA, ê plt, AKI, AMS/seizure, fever
• Associations: bloody diarrhea (E. coli), quinine, chemo, pregnancy, SLE• PLEX ASAP, don’t wait for ADAMSTS13

HEPARIN INDUCED THROMBOCYTOPENIA• Type II HIT occurs 5-10 days after starting heparin (unless previous exposure)
• > 50% reduction in count between 5-10 days
• Thrombosis or necrotic skin lesions
• Anticoagulate whether or not thrombosis identified
• Argatroban preferred in renal disease
• Bivalirudin preferred for cardiac surgery patient
• Fondaparinux alternative

MALIGNANT HYPERTHERMIA• Succinylcholine, halothane, isoflurane, sevoflurane
• 1/100,000 anesthetics
• Muscular rigidity (begins in masseter) then generalized (despite NMB)
• Hypercarbia (rise in ETCO2), tachycardia, metabolic acidosis, hyperkalemia, rhabdo
• Temperature elevation happens later
• Discontinue triggering agent
• Increase Ve
• Dantrolene
• Treat hyperkalemia as needed, watch HCO3, CPK

STEVENS JOHNSON SYNDROME AND TOXIC EPIDERMAL NECROLYSIS• Severe mucocutaneous reactions to medications, especially allopurinol, sulfa drugs,
carbamazepine, phenytoin• SJS < 10% BSA• TEN > 30% BSA• SCORTEN ≥ 2 =ICU/BURN UNIT• Stop offending drug• Wound care/sterile handling• IVFs/nutritional support• Room temp 30-32˚• Ocular/vaginal care• IVIG controversial• Steroids controversial
Independent prognosis factors WeightAge ≥40 years 1Malignancy* Yes 1Body surface area detached ≥10 percent 1
Tachycardia ≥120/min 1Serum urea >10 mmol/L 1Serum glucose >14 mmol/L 1Serum bicarbonate <20 mmol/L 1SCORTEN# 7
ANGIOEDEMA• Swelling of face, lips, tongue, larynx, bowels
• Mast cell/IgE mediated: foods, insect stings
• Urticaria, pruritus, bronchospasm, hypotension
• Epinephrine (if anaphylaxis), aggressive IVFs, O2, albuterol, diphenhydramine, ranitidine, methylprednisolone
• Bradykinin-mediated: hereditary, acquired C1-inhibitor deficiency, ACEI
• No urticaria or pruritus or bronchospasm
• Acquired C1-inhibitor deficiency: older, lymphoproliferative disorder, ê C4 level (C4 = substrate for C1 esterase)
• Hereditary: family history of swelling or recurrent abdominal pain, ê C4 level
ANGIOEDEMA• H/O preceding (often milder) episodes is common with ACEI-induced angioedema
• Bradykinin is inactivated by ACE
• Risk factors for ACEI-induced angioedema: age > 65, smoking, ASA or NSAIDs, female, seasonal allergies, African descent
• Antihistamines, glucocorticoids and epinephrine are of little benefit (small number of studies suggest antihistamines may help some in ACEI-induced angioedema, and intubated patients were extubated earlier if treated with antihistamines in one trial)
• Icatibant: bradykinin receptor antagonist
• FFP: contains ACE
• C1 inhibitor concentrate (Cinryze)

LACTIC ACIDOSIS• Type A:
• Inadequate oxygen delivery (hypoperfusion or hypoxemia)
• Type B:
• Malignancy
• Alcohol
• Short gut syndrome (D-lactate)
• Drugs (metformin, ativan, propofol, albuterol)
• Nutritional deficiency (thiamine)

THYROID STORM• Triggers include surgery, trauma, iodine, infection, amiodarone, parturition
• Fever > 103• Tachycardia, atrial fibrillation• Agitation• Tremulous• Congestive heart failure• Psychotic• Diarrhea
• Treatment: beta blockers, thionamides (stop synthesis), iodine solution to block release, lithium may block release, steroids decrease T4èT3 conversion and promote vasomotor stability, bile acid sequestrants to reduce enterohepatic recycling of thyroid hormones, cooling measures, acetaminophen

SICKLE CELL ACUTE CHEST SYNDROME• Pulmonary infiltrate with fever/respiratory symptoms (DDx = PE, ACS, pneumonia)• Infection, fat/necrotic bone marrow embolism, microvascular occlusion• Transfusion goal hgb 10• Simple transfusion for Hgb < 5 (Hgb S level close to 30% can be achieved with this alone)• Empiric antibiotics (can’t reliably distinguish from pneumonia without ACS)• Supplemental O2, incentive spirometry, avoid hypovolemia• Partial exchange transfusion (erythrocytapheresis) for:
• Progression of ACS despite simple transfusion • Severe hypoxemia (≥ 4 lpm O2 requirement)• Multilobar disease• Previous history of severe ACS
• Hydroxyurea decreases risk of ACS by 40%

ICU OUTCOMES IN CANCER PATIENTS• Patients with organ failure with a new cancer diagnosis have comparable outcome to non-
oncology patients if they do not require mechanical ventilation
• If mechanical ventilation is needed there is a 5% two month survival rate
ANTIHYPERTENSIVES AND SURGERY• Want to continue antihypertensives, especially beta blockers, prior to surgery
• Increased perioperative complications are seen with beta blocker withdrawal (e.g., Afib)
• Want to stop ACEI and ARBs, however, as they may cause refractory hypotension when combined with inhalational anesthetics

PHEOCHROMOCYTOMA• Triad: episodic HA, sweating, tachycardia (most don’t have all)
• Sustained or paroxysmal HTN, may see orthostasis and hypotension
• Urinary (24 hr urine)/plasma metanephrines and catecholamines
• Abdominal/pelvic CT/MRI, MIBG scintigraphy if negative and suspicion remains
• Most sporadic, 40% genetic (MEN2, Von Hippel Lindau, NF1)
• Phentolamine is drug of choice in hypertensive emergency due to pheo
• Phenoxybenzamine pre-op to control BP/arrhythmia
• High sodium diet (catecholamine induced volume contraction and alpha blockade)
• Beta blockers only after adequate alpha blockade achieved
• Laparoscopic adrenalectomy

HYPOGLYCEMIA IN THE ICU• May lead to seizures, brain damage (global injury or focal neurological deficits), cardiac
arrythmias• Independent risk factor for death in some studies• Drugs (insulin, oral hypoglycemics)• Sepsis• Hepatic failure• Renal failure (decrease renal gluconeogenesis)• Malnutrition• Adrenal insufficiency• Mechanical ventilation, diabetes mellitus and severity of illness are also independent risk
factors• Intensive insulin therapy with target 80-100 mg/dl leads to é mortality and hypoglycemia• Target 140-180 mg/dl• Glucagon is not effective in malnourished critically ill patients

TUMOR LYSIS SYNDROME• K, PO4, nucleic acids released
• Uric acid derived from nucleic acids causes AKI (ppt in renal tubules, renal vasoconstiction, inflammation)
• Ca-PO4 > 60 = risk for CaPO4 ppt in renal tubules
• N/V/D, anorexia, lethargy, hematuria, CHF, dysrhythmias, seizure, cramps, tetany, syncope
• IV hydration and diuresis, allopurinol, rasburicase, alkalinize urine
• Dialysis if hyperuricemia persists and urine output is low
• Chance of renal recovery is good if HD started early
• Rasburicase C/I in G6PD deficiency (methemoglobinemia)
ISSUES WITH SEDATIVES/PARALYTICS• Dexmedetamidine: bradycardia
• Propofol: hypertriglyceridemia, pancreatitis, Propofol infusion syndrome
• Etomidate: does not affect BP, associated with adrenal insufficiency
• Ketamine: increased BP/HR, dissociative analgesia
• Fentanyl: skeletal muscle rigidity with high bolus dose
• Non-depolarizing paralytics associated with histamine release/bronchospasm, prolonged weakness in setting of aminoglycosides or steroids
• Cisatracurium has least issues with hemodynamics and clearance

ECMO• If compared to lung protective vent strategy, ECMO does not help a lot
• Good result in H1N1 study
• Need randomized controlled trials
• May try in refractory hypoxemia cases after paralysis, prone ventilation and conservative fluid strategy
INCREASED RISK OF DEATH IN ASTHMA• Prior h/o severe exacerbations/intubation
• > 2 admissions/year
• Using > 2 SABA canisters/month
• Poor perceivers of asthma activity
• Low socioeconomic status
• Illicit drug use
• Comorbid cardiac or chronic lung disease or psychiatric disease

DIFFERENTIAL DIAGNOSIS OF STATUS ASTHMATICUS• Congestive heart failure• Myocardial infarction• Pulmonary embolism• Vocal cord dysfunction• Upper airway obstruction• Tracheobronchomalacia• Anaphylaxis• Endobronchial lesion• COPD• Bronchiolitis• Acute bronchitis/pneumonia

STATUS ASTHMATICUS• Hyperinflation: distended alveoli compress capillaries leading to é dead space, flattened
diaphragm creates mechanical disadvantage with é WOB, é intrathoracic pressure causes ê venous return and stroke volume
• Watch UO and BP to make sure CO is ok, if low bolus fluids
• Continuous nebulization of albuterol may lead to improvement at first and then development of lactic acidosis (may need to stop SABA)
• Mg improves FEV1 in severe exacerbations who fail to respond to conventional treatment after 1 hour, ê intubations and hospitalizations
• Heliox 70:30 or 80:20 beneficial in severe airflow obstruction
• NIV: small trials showed improved lung function and decreased need for hospitalization
• May be considered in cooperative patients prior to intubation

STATUS ASTHMATICUS• Altered mental status or loss of pulsus paradoxus = sign of fatigue→ consider intubation
• Avoid severe hyperinflation on ventilator (PIP < 50-55 cm H2O, Plat P < 30)• Lowering respiratory rate is most effective means to ê autoPEEP• Vt 6-8 cc/kg IBW
• Higher flow rates (but not too high)• Episodic disconnect from ventilator
• Permissive hypercapnia reduces mortality• Caution in elevated ICP, pregnancy, myocardial ischemia
• Deep sedation may be necessary (suppress resp drive so patient doesn’t overbreathe)• Ketamine bronchodilates but does not suppress drive• Usually propofol, opioids, benzodiazepines
• If sedation ineffective è paralyze but interrupt q4-6 hours to prevent accumulation• Risk of myopathy
• Improved synchrony, ê O2 consumption and CO2 production, ↓ barotrauma
PNEUMOTHORAX• < 2-3 cm from apex: administer oxygen and repeat CXR in several hours
• If >3 cm: aspirate with IV catheter ± chest tube
• If unstable: decompression then chest tube
• If on mechanical ventilation place chest tube
• Small bore chest tubes as effective as large bore
• If recurrent: VATS pleurodesis
• U/S more sensitive than CXR to detect PTX
• Confirms PTX : lung point
• Suggests PTX: absence of lung sliding, no seashore (barcode) sign
• Excludes PTX: lung sliding, B-lines, seashore sign (normal)

PLEURAL EFFUSION• Serum-pleural fluid albumin < 2 increases specificity for an exudate (92%) over just one of
the three Light’s criteria
• Pleural/serum protein > 0.5
• Pleural/serum LD > 0.6
• Pleural LDH > 2/3 ULN
• Complicated pleural effusion
• Gross pus
• + culture
• + gram stain
• pH < 7.2
• A-F level, loculations, thickened pleura

PLEURAL EFFUSION• Small tubes are as effective as large tubes for complicated effusions
• tPA and DNAse reduce need for surgical referral and hospital LOS
• Esophageal rupture: high amylase in fluid, food particles
• TG > 110 mg/dl = chylothorax (lymphoma, thoracic duct injury, LAM)
• Hemothorax
• Fluid HCT: blood ≥ 0.5
• Large bore 36 Fr CT
• Surgery if > 1.5L or persistent drainage 3 ml/kg/h

ACUTE KIDNEY INJURY IN ICU• > 50% AKI in ICU = acute tubular necrosis
• Ischemia, sepsis, vascular surgery, toxic injury (drugs, contrast dye, heme pigments)
• Major drugs: aminoglycosides, PCNs, vancomycin, acyclovir, NSAIDs, amphotericin, foscarnet, tenofavir
• 50% aggregate mortality for patients requiring RRT
• ATN: granular (muddy brown) and epithelial casts
• Prerenal: normal or hyaline casts
• Glomerulonephritis: RBCs (dysmorphic), RBC casts, WBCs
• Acute interstitial nephritis: WBC casts, proteinuria
• Urinary obstruction: hematuria
• Rhabdomyolysis: pigmented casts

ACUTE TUBULAR NECROSIS• Decreases in GFR are not always accompanied by decreases in UO
• There is no difference in mortality between oliguric and nonoliguric renal failure
• There is no benefit to furosemide use early or late in renal failure
• Furosemide does not delay the need for renal replacement therapy

RENAL REPLACEMENT THERAPY INDICATIONS• Encephalopathy
• Seizures
• Pericarditis
• Intractable GI symptoms
• Refractory hyperkalemia, acidosis
• Diuretic resistant volume overload

RENAL REPLACEMENT THERAPY IN ICU• Late initiation at higher BUN concentrations associated with é risk of death
• Early RRT within 48 hours associated with improved renal recovery and ICU LOS and a trend toward mortality benefit
• Intermittent HD associated with more volume overload vs continuous
• Dialysis dose 35 vs 20 mg/kg/h (intensive vs less intensive) had no effect on mortality
• Preference for CRRT in hypotension, severe sepsis, severe volume overload, liver failure, ARDS, tumor lysis
• Less hemodyamic instability with CRRT vs iHD but no difference in mortality
• 10-30% require continued dialysis after discharge
INTRADIALYTIC HYPOTENSION• SBP drop > 20 or MAP > 10• Risks: older age, longer dialysis vintage, DM, lower predialysis BP, Hispanic, large BMI• Systemic infection• Arrythmias, pericaridial tamponade or MI• Air embolism• Reaction to dialyzer membrane (chest or back pain and signs of allergic rxn like hives,
sneezing, flushing)• Rapid or excessive ultrafiltration• Rapid reduction in plasma osmolality• Autonomic neuropathy (especially in long standing DM)• Vagal symptoms: yawning, sighing, hoarseness• Antihypertensive meds given before HD• Eating during HD: PVR drops 20-120 minutes later

DELIRIUM IN CKD• Uremic encephalopathy
• Seizure
• Drugs (impaired excretion)
• Star fruit ingestion
• Dialysis disequilibrium syndrome
• Hemodynamic instability
• Cerebrovascular disease
• Thiamine deficiency
• ETOH withdrawal
HYPONATREMIA• CHF, cirrhosis
• SIADH: CNS disturbances (CVA, hemorrhage, infection, trauma, psychosis), malignancies (especially small cell Ca), drugs (carbamazepine, SSRI), pulmonary disease, HIV
• Primary polydipsia
• Hypothyroidism
• Adrenal insufficiency
• HCTZ
• Volume depletion
• Low solute/protein intake
HYPONATREMIA• Una < 10 + hypokalemia = likely hypovolemic hyponatremia (decreased
po intake, GI losses, diuretics)
• With SIADH UNa > 20-40 Meq/L
• Urine osmolarity > 100 indicates impaired ability to dilute the urine (but in advanced renal impairment the minimum urine Osm rises to 200-250 despite ADH suppression)
• Low urine Na and low urine Osm: primary polydipsia, beer potomania

SEVERE HYPONATREMIA• Emergency treatment for seizures or obtundation or in ACUTE hyponatremia
with even mild symptoms
• Goal is 4-6 Meq correction within several hours, but not > 8 Meq in 24 hours
• Monitor Na q2 during emergency treatment
• Do not correct more than 0.5-1.0 Meq/hr or 8 Meq over 24 hours
• 0.9% normal saline = 154 Meq
• 3% saline = 513 Meq
HYPOKALEMIA• K 2.5-3: weakness, constipation/ileus
• K < 2.5: muscle necrosis/rhabdomyolysis, weakness
• K < 2.0: ascending paralysis, respiratory impairment
• Every 1 Meq/L drop ~ 200-400 Meq loss
• Maximum rate of infusion is 20 Meq/h for most patients (up to 40 Meq/h for immediately life threatening hypokalemia)
• Do not add to D5 solution: stimulates insulin which drives K into cells
• Cardiac arrhythmias, heart block, bradycardia, prominent U waves
• Increased renal ammoniagenesis
• Do not give insulin in DKA until the serum K > 3.3
REFEEDING SYNDROME• Anorexia nervosa, cancer patients undergoing chemotherapy, malnourished elderly,
homeless or alcoholic patients (especially when weight < 70% IBW)
• Hypophosphatemia, hypokalemia, hypomagnesemia, vitamin (e.g., thiamine) deficiencies, CHF, peripheral edema
• Bradycardia expected in anorexia nervosa (HR >70 may = harbinger of cardiac compromise)
• CHF due to impaired contractility, Na/fluid retention, thiamine deficiency may contribute
• Arrhythmias
• Respiratory muscle weakness, myalgia, tetany, rhabdomyolysis
• Hemolysis also occurs with serum phosphate < 1.0
• Wernicke’s encephalopathy: encephalopathy, oculomotor dysfunction, ataxia
CENTRAL VENOUS CATHETERS• Do not routinely replace CVC
• Do not remove CVC or PICC because of fever alone
• Do not use guidewire exchanges routinely for nontunneled catheters, and never when catheter infection is suspected
• Use guidewire to replace a nonfunctioning nontunneled catheter if no evidence of infection is present
• Treat 10-14 days after catheter removal for CLASBI (day 1 = first negative BCx)
• For persistent bacteremia > 72 hours after catheter removal è 4-6 weeks of antibiotics

HYPOTHERMIA• ê HR, CO, hypoventilation, CNS depression, reduced renal blood flow, loss of
shivering, paradoxical undressing, Afib, junctional bradycardia
• Hypothermic heart is sensitive to movement
• Hypothyroid, adrenal insufficiency, sepsis, malnutrition, thiamine deficiency, alcohol, hypoglycemia
• Esophageal probe best to track rewarming
• Do not use bladder temps as this lags behind core temps
POLYCYTHEMIA• Hypoxemia
• Diuretic induced hemoconcentration
• Renal cell Ca, HCC, pheochromocytoma may increase erythropoeitin
• Polycythemia vera: splenomegaly, thrombocytosis, thrombotic or bleeding complications, aquagenic pruritus, HA/paresthesias, leukoerythroblastic smear (tear drops, immature WBCs)
KETOACIDOSIS• Diabetes
• Starvation
• Alcohol
DKA TRIGGERS• Noncompliance or under treatment with insulin
• New onset diabetes (20-25%)
• Infection (30-40%)
• Cerebrovascular accident
• Myocardial infarction
• Acute pancreatitis
• Cocaine, methamphetamines
• Thiazides, atypical antipsychotics

DIABETIC KETOACIDOSIS• Severe DKA: pH < 7, bOHB > 8, stupor, coma (if serum osm not > 320 look for other causes of AMS)
• bOHB:acetoacetate ratio may exceed 10:1, so may have false negative urine ketone (nitroprusside) test
• Abdominal pain is associated with the severity of acidosis (86% report this when HCO3 ≤ 5): delayed gastric emptying, ileus, pancreatitis, stress gastritis
• Amylase and lipase may be elevated in DKA (15-25%) without clinical or radiographic evidence of pancreatitis (use imaging for diagnosis of pancreatitis)
• If WBC > 25K consider infection as cause (as opposed to DKA related stress response)• If pH 6.9-7.14 HCO3 treatment does not change mortality or morbidity (only use for pH < 6.9)
• Check for hyperlipidemia• Average K deficit > 300 Meq
• If serum K < 3.3, hold insulin• Can begin adding potassium to replacement fluids in DKA when level < 5.3
• If PO4 < 1 may see cardiac dysfunction, arrhythmias, respiratory depression, hemolysis or rhabdomyolysis
RHABDOMYOLYSIS• Trauma, muscle compression, exertional rhabdo, electrolyte disorders, drugs,
venoms, cocaine/amphetamines, infections, inflammatory myopathies, endocrine disorders (thyroid, pheo)
• AKI risk when CPK > 5000
• Saline 1-2 L initially
• Want high UO (200-300 cc/hr) to wash out tubular casts unless volume overloaded
• Alkalinize urine pH > 6.5: may diminish renal toxicity of heme by reducing pigment precipitation with intratubular cast formation, decreasing release of iron from myoglobin which triggers vasoconstriction, and reducing uric acid precipitation
CHRONIC HYPERCAPNEIC RESPIRATORY FAILURE• COPD
• Obesity hypoventilation syndrome
• Hypothyroidism
• Respiratory muscle weakness due to neuromuscular disease (muscular dystrophy, myasthenia gravis, polymyositis, ALS, polio, Guillain Barre)
• Severe restrictive lung disease (kyphoscoliosis or fibrosis)
• CNS events/disease: CVA, encephalitis, C-spine/brainstem pathology)
• Severe hypophosphatemia, hypokalemia hypermagnesemia