critical care in pregnancy - swedish
TRANSCRIPT
Critical Care in PregnancyErica Foster, MD
OB Fellow

Overview
• Physiologic changes in pregnancy
• Causes of critical illness in pregnancy
• Recognition and initial management
• Transferring critically ill patients



Physiology of pregnancy
• Cardiovascular System• HR ↑15-20 BPM
• Stroke volume ↑
• Cardiac output ↑40%
• Plasma volume ↑40-50%
• Erythrocyte volume ↑20%
• Arterial blood pressure ↓10-15mmHg
• SVR ↓

Physiology of pregnancy
• Respiratory • RR (breaths/min) ↑
• Tidal volume (mL) ↑
• Minute ventilation (mL/min) ↑
• Oxygen consumption ↑20-30%
• Maternal pH 7.40-7.45
• Serum bicarb ↓18-21 mEq/L
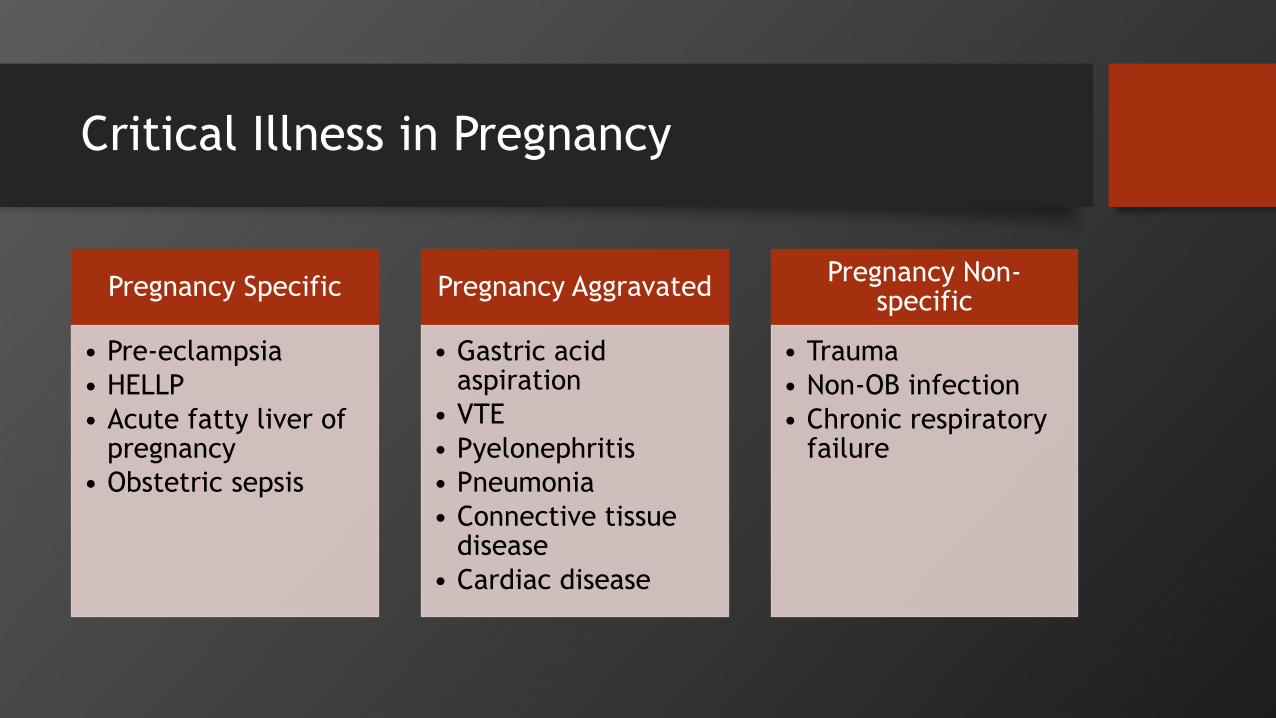
Critical Illness in Pregnancy
Pregnancy Specific
• Pre-eclampsia
• HELLP
• Acute fatty liver of pregnancy
• Obstetric sepsis
Pregnancy Aggravated
• Gastric acid aspiration
• VTE
• Pyelonephritis
• Pneumonia
• Connective tissue disease
• Cardiac disease
Pregnancy Non-specific
• Trauma
• Non-OB infection
• Chronic respiratory failure
Principles of critical care in pregnancy
• Maternal stabilization
• Determine gestational age
• Remember physiology
• Don’t withhold diagnostic imaging
• Consider steroids
• Fetal monitoring
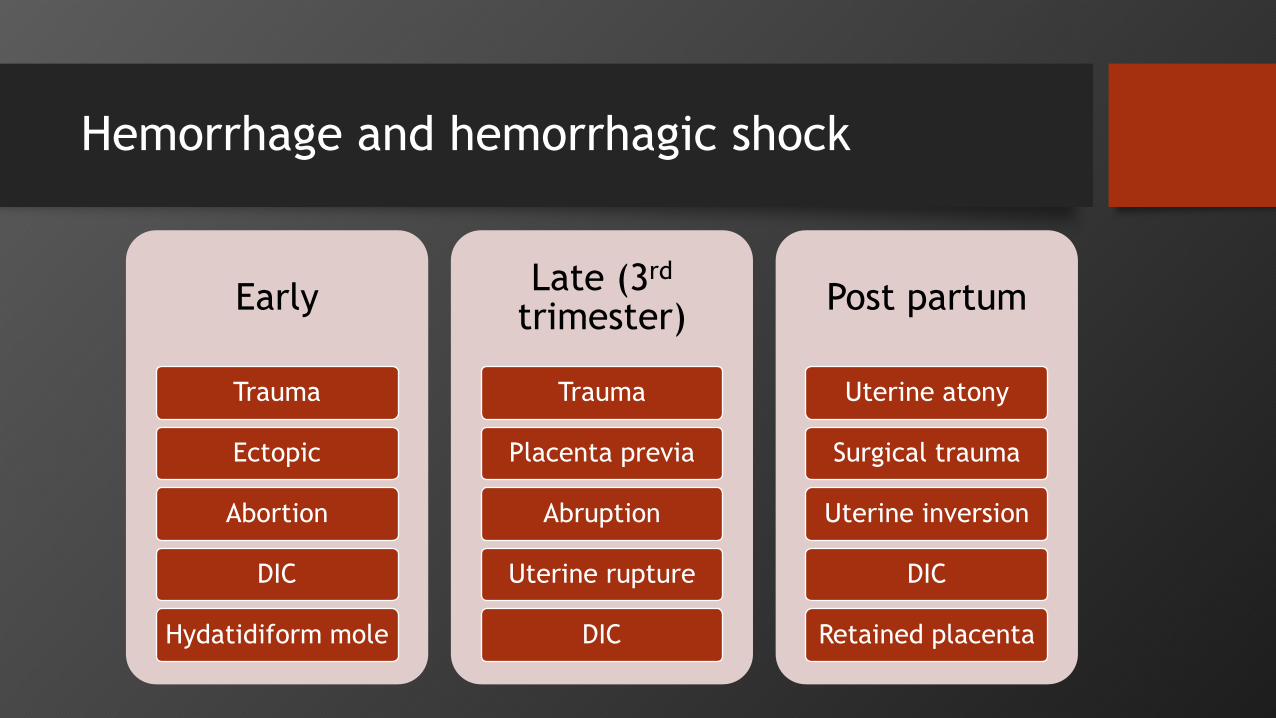
Hemorrhage and hemorrhagic shock
Early
Trauma
Ectopic
Abortion
DIC
Hydatidiform mole
Late (3rd
trimester)
Trauma
Placenta previa
Abruption
Uterine rupture
DIC
Post partum
Uterine atony
Surgical trauma
Uterine inversion
DIC
Retained placenta

Hemorrhage and hemorrhagic shock
Hemorrhage
Class
Acute Blood Loss (mL) Lost (%) Physiologic Adaptation
1 1000 10-15 Dizziness, palpitations, minimal BP change
2 1500 25-30 Tachycardia, tachypnea, sweating, weakness,
narrowed pulse pressure
3 2000 30-35 Significant tachycardia and tachypnea,
restlessness, pallor, cool extremities,
hypotension
4 >2500 >40 Cardiogenic shock, air hunger, oliguria, anuria

Hemorrhage and hemorrhagic shock
• Assessment• Hgb/Hct, plt, coags (pt, ptt, fibrinogen), potassium, ical
• EBL
• Initial Management• Replacement begins with appropriate fluid resuscitation (warmed crystalloid
3:1 ratio)
• Blood components
• Drug therapy
• Balloon tamponade, surgical intervention, IR embolization
• Complications

Trauma
• Types of injury• MVC (48%), falls (25%), assault/IPV (17%)
• Maternal trauma is a major health disparity
• Maternal trauma is the leading cause of non OB maternal death
• Complications of trauma• Maternal and/or fetal death• Preterm birth, low birthweight• Placental abruption• Fetomaternal hemorrhage• Uterine rupture • Direct fetal injury

Trauma
• Initial Management • Primary survey (ABCDE+F)
• Secondary survey
• Immobilize C spine
• Clear any obstruction/secretion
• Consider advanced airwayA -Airway
• Check rate/effort
• Supplemental O2B - Breathing
• Assess pulse and BP
• Establish IV accessC- Circulation
• GCS
• Neuro examD - Disability
• Inspect entire body for injury
• Provide warm blanket!
E - Expose patient
• CEFM for at least 4-6 hour if viable pregnancyF - Assess
fetus

Management algorithm for trauma in pregnancy
- Cardiac arrest
- Unresponsive
- Loss of airway/respiratory arrest
-BP<80/40 or HR <50 or >140
- If fetus viable, FHR<110 or >160
- ABCDE
- Consult trauma team, notify NICU
- Supplemental O2
- Displace Uterus if >20 wk
- IV Access (2 PIVs)
- Labs: CBC, Coags, T&S, KB
- Viable fetus FHR via doppler
- Toco (esp if concerned about abruption)
- Fetal US +/- BPP
- Consider other labs – chem, UA, Utox
- Radiologic assessment/peritoneal lavage/FAST exam
Maternal injury greater than minor bruising, lacerations or
contusion
- Consider trauma team consult
- IV access
- Labs: CBC, coags, type and screen KB
- Viable fetus: monitor 4+ hours
- Toco (esp if concern for abruption)
- Brief fetal assessment
- No lab eval required
- No radiologic imaging required
- Patient counseled on s/sxs of abruption
PRESENT ABSENT
PRESENT ABSENT
ASSESS MATERNAL STATUS
ADVANCED LIFE SUPPORT
ONCE PATIENT IS STABLE

Hypertensive emergencies
• Severe Pre-Eclampsia/Eclampsia, HELLP Syndrome
• Hypertensive emergencies• Hypertensive encephalopathy
• Acute left ventricular failure
• Acute aortic arch dissection
• Ischemia of retina

Hypertensive emergencies
• Initial management• IV access, infusion of NS
• Continuous BP monitoring, volume status, urinary output, ECG reading, mental status
• CEFM
• BP lowering therapy with goal to reduce MAP <25%, small reduction in first 60 minutes, work towards systolic level 155-160mmHg/100-110mmHg
• Magnesium sulfate (for pre-eclampsia/eclampsia)
Sepsis and Septic Shock
• Sepsis: Life threatening organ dysfunction caused by an abnormal host response to an infection
• Septic shock: Sepsis with hypotension requiring vasopressor therapy and serum lactate >2 mmol/L

Sepsis and Septic Shock
Jones, A., Trzeciak, S., The Sequential Organ Failure Assessment score for predicting
outcome in patients with severe sepsis and evidence of hypoperfusion at the time of
emergency department presentation. Critical Care Medicine 2009; 37(5): 1649-54.
Sepsis and Septic Shock
• Initial management • Broad spectrum antibiotics (*within 1 hour)
• Crystalloid fluid (30mL/kg)
• Blood product as needed
• Vasopressors and inotropes
• Removal of infections source
• Ventilation support
• Delivery as indicated

Amniotic fluid embolism
• Rare – 1/13,000-1/50,000
• During labor or immediately post partum
• Assessment • Shortness of breath
• AMS
• Cardiorespiratory collapse/cardiac arrest
• Management• Supportive
• Anticipate ARDS, DIC
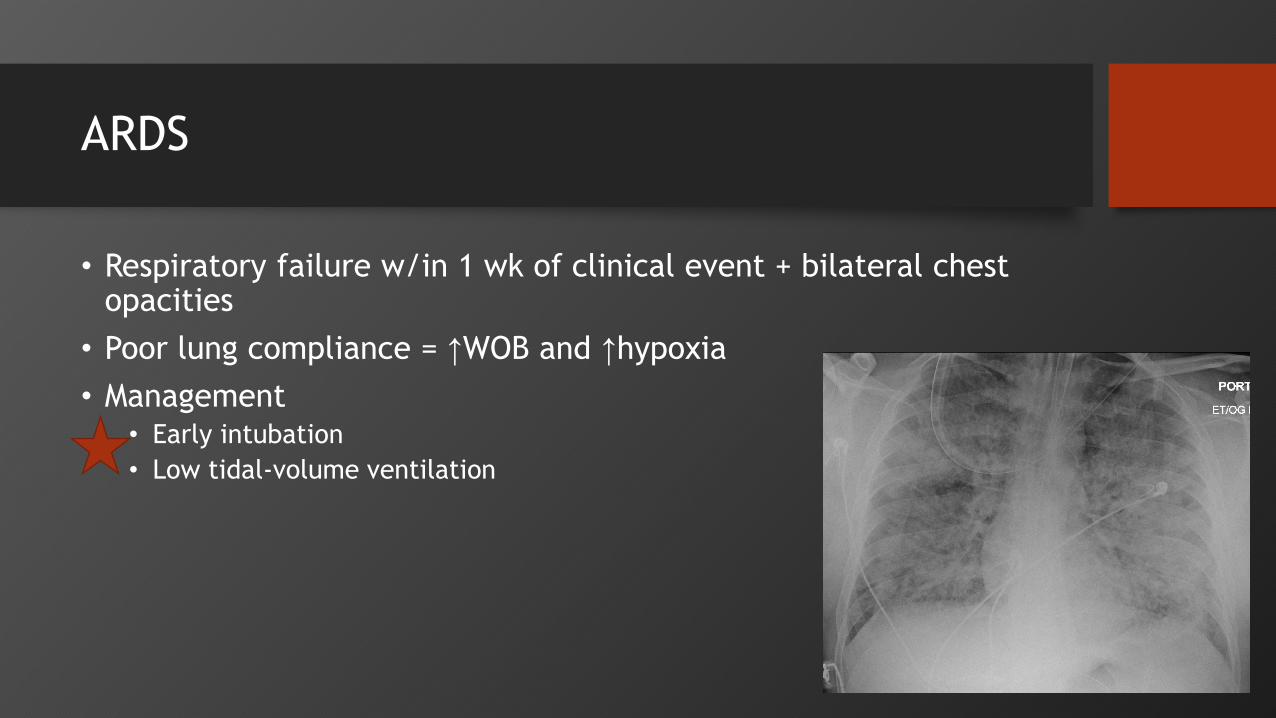
ARDS
• Respiratory failure w/in 1 wk of clinical event + bilateral chest opacities
• Poor lung compliance = ↑WOB and ↑hypoxia
• Management• Early intubation
• Low tidal-volume ventilation
Transferring Patients
• Need to facilitate access to higher level of care
• Consideration should be given to transport as soon as need is identified
• Maternal status must be stabilized prior to transport
• Monitoring

Cardiac Arrest
• Tilt/uterine displacement
• Chest compressions
• Remove monitors prior to delivering shocks
• Otherwise same ratio compressions to breaths, respiratory support, breaths, defibrillation
Resuscitative hysterotomy
• Recommended with uterine size >20wk
• Preparations should begin if no ROSC in first few minutes
• 74 third trimester cases• 45% died
• 45% survived without obvious sequelae
• 10% survived with significant sequelae
Review
Hemorrhage
- Fluid
resuscitation
- Blood product
HTN Emergency
- BP Lowering
medication goal
reduce MAP by
25%
Sepsis
- Broad spectrum abx
- Fluid resuscitation
30ml/kg
AFE
- Support (ACLS)
- Anticipate DIC,
ARDS
ARDS
- Early intubation
with lung
protective
ventilation
Trauma
- Primary survey
(ABCDE+F
- Secondary
survey
References
• American College of Obstetricians and Gynecologists. Critical Care in Pregnancy. ACOG Practice Bulletin No. 211. Obstetrics Gynecology 2019 133(5)
• Beckett VA, Knight M, Sharpe P. The CAPS Study: incidence, management and outcomes of cardiac arrest in pregnancy in the UK: a prospective, descriptive study. BJOG 2017;124:1374-81.
• Foley, Michael R., Strong, Thomas H., Garite, Thomas J. Obstetric Intensive Care Manual, Fifth Edition. 2018.
• Jones, A., Trzeciak, S., The Sequential Organ Failure Assessment score for predicting outcome in patients with severe sepsis and evidence of hypoperfusion at the time of emergency department presentation. Critical Care Medicine 2009; 37(5): 1649-54.
• Mendez-Figueroa, H., Dahlke, JD., Vrees, RA., Rouse, DJ. Trauma in Pregnancy: An updated systematic review. Am J Obstet Gynecol. 2013; 209(1):1-10