critical concepts nicu brian m. barkemeyer, md lsuhsc division of neonatology 2011-12
TRANSCRIPT
Critical ConceptsNICU
Brian M. Barkemeyer, MDLSUHSC Division of Neonatology
2011-12
At birth
• 100% of infants need someone present dedicated to the infant and capable of initial steps in neonatal resuscitation
• 10% of infants require some level of resuscitation at birth
• 1% of infants require major resuscitation
“Golden hour”
• At no other time in one’s life will necessary critical concepts in resuscitation have a potential lifelong impact– Appropriate interventions (or the lack thereof)
can make the difference between life or death, or normal life vs. life of disability
Preparation
• NRP - Neonatal Resuscitation Program– Evidence-based, standardized program jointly
sponsored by American Academy of Pediatrics and American Heart Association
• Proper equipment• Knowledge– In most cases, the need for neonatal
resuscitation is predictable– But not always!
Risk Factors Predictive ofNeed for Neonatal Resuscitation
• Maternal illness– Hypertension– Diabetes– Infection
• Prematurity• Post-maturity• Multiple gestation• Maternal bleeding• Maternal drug abuse• No prenatal care
• Fetal distress• Abnormal fetal position• Abnormal labor• Fetal anomalies• Macrosomia• IUGR• Placental abnormalities• Meconium-stained
amniotic fluid
Transition toExtrauterine Life
• Fluid-filled alveoli to air-filled alveoli• Circulatory changes– Decreased pulmonary vascular resistance
resulting in increased pulmonary blood flow and cessation of flow through foramen ovale and ductus arteriosus
– Cessation of flow to placenta resulting in increased systemic vascular resistance
Lack of Appropriate Resuscitation
• Interrupts normal transition to extrauterine life
• Hypoxia• Respiratory and metabolic acidosis• Ischemia
• Potential for death or long term adverse outcome
Three Basic Questions
• Term infant?• Breathing/crying at birth?• Normal tone at birth?
• If the answer to these three questions is yes, infant doesn’t need resuscitation, but does deserve initial steps
Initial Steps
• Drying• Warming• Stimulation• Positioning• Clear airway
• Necessary for all newborns!
Warming
• Appropriate room temperature• Rapid drying to avoid evaporative heat loss• Remove wet towels• Mother – skin to skin• Radiant heat warmer• Blankets, cap
• Premature infants and IUGR infants at highest risk for hypothermia
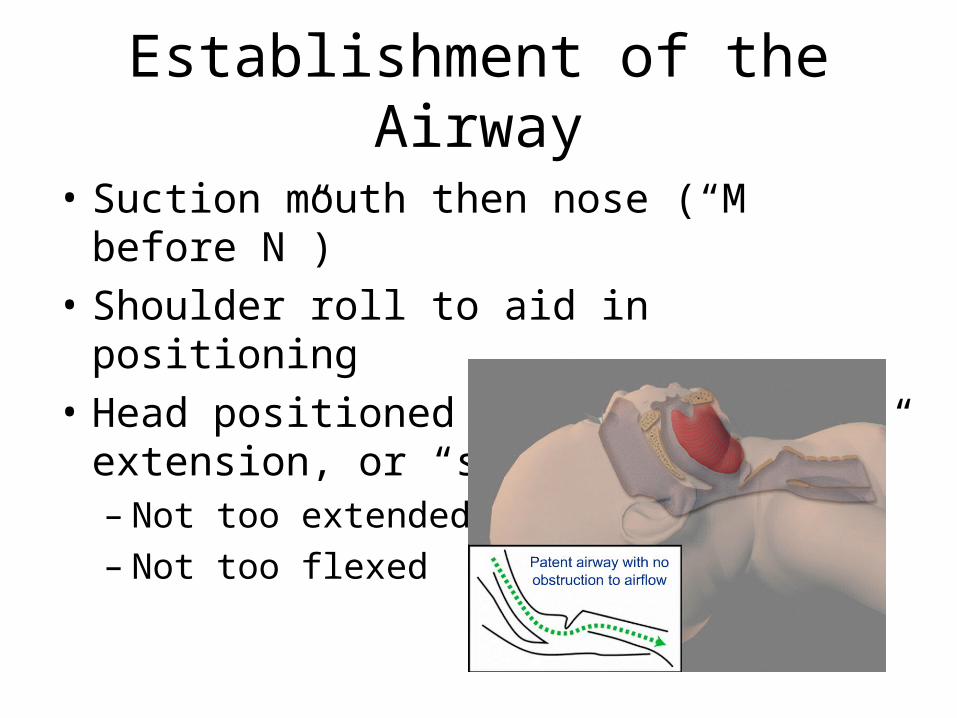
Establishment of the Airway
• Suction mouth then nose (“M before N”)• Shoulder roll to aid in positioning• Head positioned in slight extension, or
“sniffing position”– Not too extended– Not too flexed
ABC’s
• Airway– Suction secretions, assess for anomalies
• Breathing– Stimulate respiratory effort
• Tactile• Bag-mask positive pressure ventilation (PPV)
• Circulation– Assess heart rate
• Chest compressions if PPV ineffective at restoring heart rate
Skills to Learn
• Neonatal assessment• Use of bulb suction• Administration of positive pressure ventilation
by bag-mask• Intubation and assistance with intubation• Chest compressions
Assessment/Reassessment:Sequential steps in resuscitation
• Initial steps [30 seconds]
• PPV [30 seconds]
• Chest compressions [30 seconds]
• Medications [30 seconds]
Neonatal Assessment
• Respirations– Normal rate and depth, good chest movement
• Heart rate– Normal > 100– Count for 6 seconds, multiply x 10
• Color– Pink lips and trunk– Acrocyanosis vs. central cyanosis
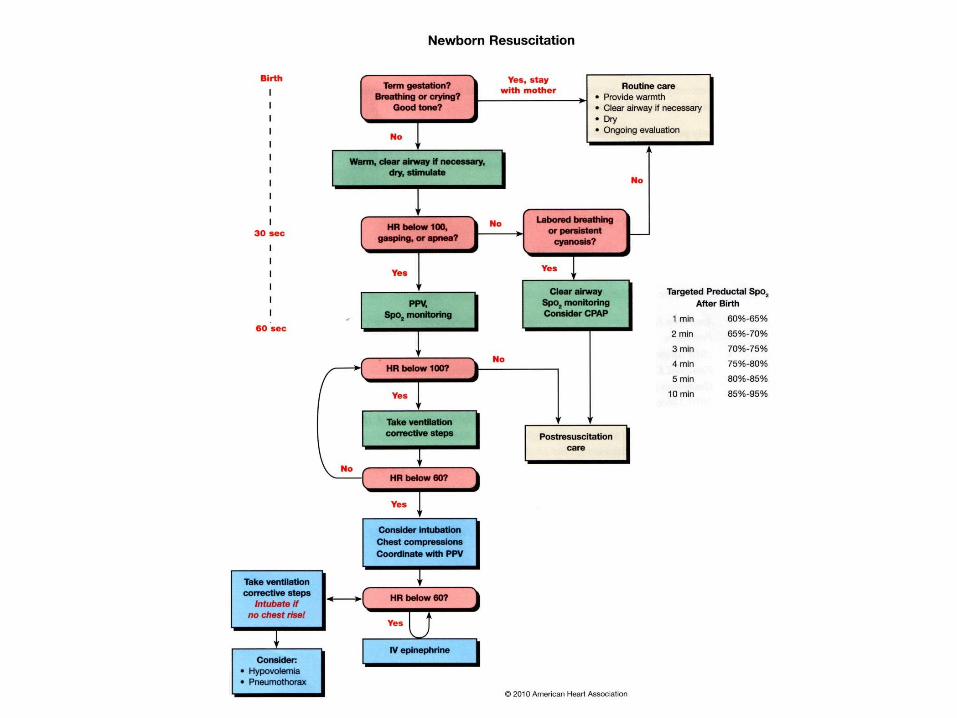
Indications for PPV
• If after initial steps in resuscitation [30 sec], assessment reveals– Apnea– Gasping respirations– Heart rate < 100
Indications for Chest Compressions
• If after initial steps in resuscitation [30 sec] and effective PPV [30 sec], assessment reveals– Heart rate < 60
Indications for Epinephrine
• Heart rate persists < 60 after– Initial steps [30 seconds]– PPV [30 seconds]– Chest compressions [30 seconds]
• Dosage given IV (UVC preferred), or endotracheal (higher dose given)
Indications for Volume Administration
• History of blood loss at delivery suggesting hypovolemia
AND
• Infant appears to be in shock (pallor, poor perfusion, failure to respond appropriately to resuscitation efforts)
• IV, 10-20 mL/kg, Normal saline, Ringer’s lactate, or O- blood
Meconium-stained Amniotic Fluid
• 15% of deliveries; at risk for meconium aspiration syndrome
• Suctioning of upper airway and trachea in infants who are not vigorous may help prevent meconium aspiration syndrome– Vigorous defined by• Heart rate > 100• Normal respiratory effort• Normal tone
Positive Pressure Ventilation
• Appropriate size mask and bag• Self-inflating vs. flow-inflating bag• Forming a good seal with mask• Achieve adequate chest rise• 40-60 breaths per minute
• When done appropriately, PPV should result in improvement in heart rate and color
Ineffective PPV
• Reposition mask on face• Reposition head• Suction upper airway• Ventilate with mouth open• Increase ventilatory pressure• Replace bag• Endotracheal intubation
Self-inflating bag
Flow-inflating bag
Chest Compressions
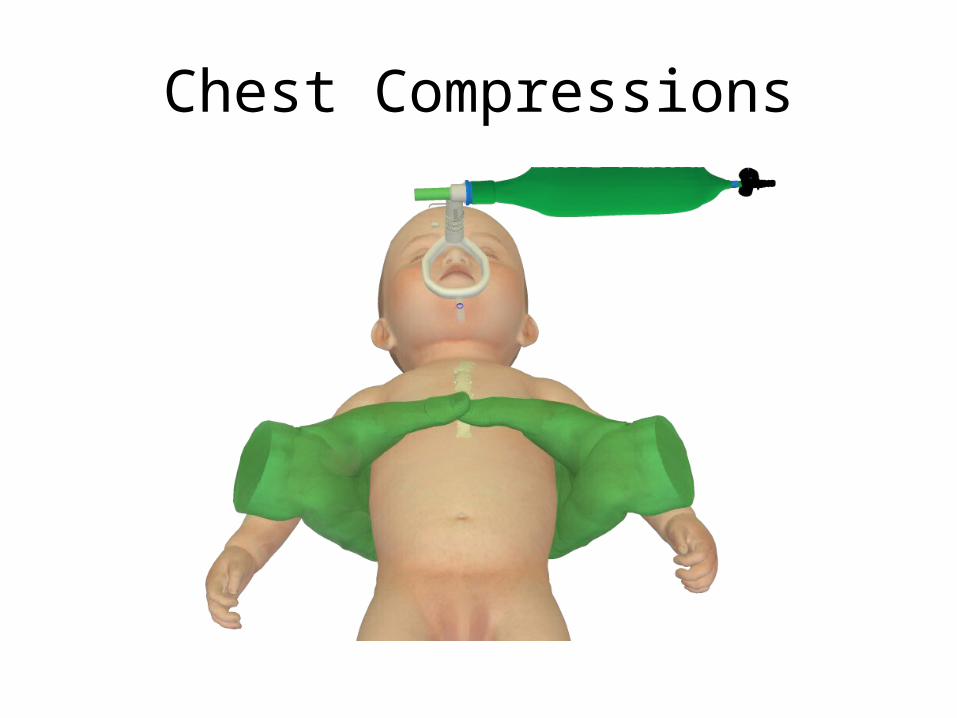
• Should be coordinated with PPV• 2 thumb method preferred• Compression of sternum 1/3 depth of AP
diameter of chest
• 120 events per minute (compressions and respirations combined)
• “One and two and three and breathe”
Chest Compressions
Endotracheal Intubation
• ET tube size similar to size of patient’s little finger
• < 28 wks, < 1000 g = 2.5 ETT• 28-34 wks, 1000-2000 g = 3.0 ETT• 34-38 wks, 2000-3000 g = 3.5 ETT• 38-42 wks, > 3000 g = 4.0 ETT
• Insertion depth– “Tip to lip” measurement = weight in kg plus 6• 2 kg patient should have ETT secure at 8 cm mark at lip
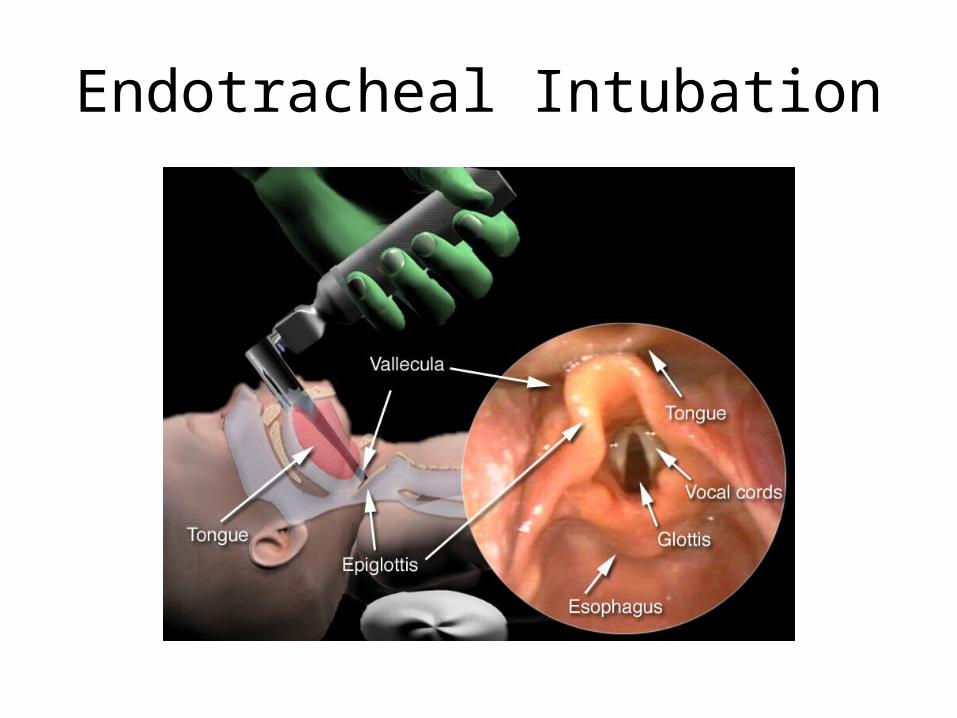
Endotracheal Intubation
Unique Aspects of Endotracheal Intubation in Infants
• Narrowest part of airway is subglottic area• Uncuffed ET tubes typically utilized• Increased airway resistance associated with
more narrow airway diameter• Relative lack of structural support for neonatal
airway
Unique Anatomic Challenges
• Choanal atresia– Endotracheal intubation may be required
• Pierre-Robin sequence– Prone positioning– NG tube into posterior pharynx
• Congenital diaphragmatic hernia– Endotracheal intubation– Gastric decompression
Key Points
• Appropriate resuscitation requires a rapid series of assessments, interventions, and reassessments
• All infants deserve basic steps of resuscitation– Drying, warming, positioning, clear airway
• Prompt initiation of respiratory support with positive pressure ventilation by bag-mask is the key to successful resuscitation of most infants