critical nutrition
TRANSCRIPT

Latest Evidence on Nutrition in the ICU: Latest Evidence on Nutrition in the ICU: Will it Change Existing Guidelines?Will it Change Existing Guidelines?
Rupinder Dhaliwal, RD
Clinical Evaluation Research Unit
Critical Care Nutrition
Kingston ON, Canada
1

Outline of Session
New RCTs in area of critical care nutrition (adult)
Updated analyses of Canadian Guidelines
Impact on evidentiary basis
1

Conflict of interest
Co-author of Canadian Clinical Practice Guidelines
1

Canadian CPGs
1
1980-2003 n > 200 RCTs 34 topics 17 recommendations
JPEN 2003

www.criticalcarenutrition.com
2005 update2005 update20072007 updateupdate2009 update 2009 update

Development of Guidelines
Validity Homogeneity
SafetyFeasibility
Cost
evidence integration of values+
practiceguidelines
1

Inclusion Criteria
Updated to 2011• Randomized controlled trials• Critically ill patients (not elective surgery)• Clinical Outcomes• EMBASE, Medline, Cinhal, reference lists

Topic # RCTs 2009 # new RCTs
Early vs. delayed 14 2
Target dose EN 2 2
Fish Oils/Borage Oils 5 4
Protein/peptides 4 1
Fibre 6 1
Small Bowel vs. Feeding 11 5
Protocols/GRVs 3 2
Probiotics 12 7
Supplemental PN 5 5
PN Type of lipids 5 4
PN Glutamine 17 8
Antioxidants 16 5
PN Selenium 11 5
New RCTs* per Topic (n =51)
* from 2009-2011

Probiotics
1

Probiotics
2009 Recommendation
There are insufficient data to make a recommendation on the use of Prebiotics/Probiotics/Synbiotics in critically ill patients
1
Knight 2009Barraud 2010Morrow 2010Frohmader 2010Ferrie 2011Sharma 2011Tan 2011
New RCTs = 7

Probiotics: effect on infections (n =11)
2009 update : RR 0.89 [0.68, 1.17] p = 0.4
Petrof et al in submission Critical Care 2012
Lower quality studies > effect vs. higher quality studies
p = 0.03

Probiotics: effect on VAP (n = 7)
Petrof et al in submission Critical Care 2012

Probiotics: effect on ICU mortality (n = 6)
Petrof et al in submission Critical Care 2012
2009 update : RR 0.74 [0.50, 1.09] p = 0.12

Probiotics with new RCTs
stronger signal for reduction in infections– higher quality studies do NOT show a reduction in
infections
significant reduction in VAP still trend towards reduction in ICU mortality
1

Arginine
2009 Recommendation
Based on 22 studies, we recommend arginine and other
select nutrients not be used for critically ill patients
no effect on mortalityno effect on infections
1

Drover et al Am Coll Surg 2011
significant reduction in infections p <0.0001 significant shorter HLOS p <0.0001

Enteral Fish Oils* ?
(Product enhanced with fish oils +borage oils + antioxidants)*
1

Enteral Fish Oils(Product enhanced with fish oils +borage oils + antioxidants)
2009 Recommendation
Based on 5 studies, we recommend the use of
enteral formula with fish oils, borage oils, and
antioxidants in patients with ALI/ARDS
New RCTs = 4New RCTs = 4

Multicenter, RCT, 14 ICUs in Brazil
N = 200, early stages of sepsis (no organ failures; within 36 hrs from onset of sepsis).
Fish oil/borage oil/antioxidant vs. standard polymeric X 7 days
Outcomes:
• Evolution to more severe forms of sepsis (severe sepsis or septic shock
• 28 day all-cause mortality, organ failure development, hyper/hypoglycemic events, insulin use, hospital stay, ICU stay
Pontes-Arruda Crit Care 2011;15:R144
PREVENTION VS. TREATMENT
11 Spanish ICUs 89 patients with diagnosis of Sepsis on admission Randomized to:
• Fish Oil/Borage Oil formula OR• Standard polymeric formula
Outcomes: new organ dysfunction
Grau-Carmona Clin Nutr 2011

Clinical Outcomes
Grau-Carmona Clin Nutr 2011
Fish Oils: Trend towards lower SOFA scores (NS)

Timing of FeedingTiming of Feeding
SSUUPPPPLLEEMMEENNTT
““Early Early Full”Full”Fast ramp upFast ramp up
““Early Early Trophic”Trophic”(10 ml/hr)(10 ml/hr)
N-3 + GLA +N-3 + GLA +AntioxidantsAntioxidants(Module delivered (Module delivered as as bolusbolus bid) bid)
ControlControlStandard ENStandard EN(480 cal/ 20 g pro)(480 cal/ 20 g pro)
n = 250 n = 250
n = 250 n = 250
NIH NHLBI

OMEGA: 60-Day MortalityOMEGA: 60-Day Mortality
P=0.05P=0.14P=0.14
Rice et al JAMA Oct 2011

89 patients from 5 centres in US
Mechanically ventilated patients with Acute lung injury (ALI)
Randomized to (separate from EN):• BOLUS fish oils 7.5 mls q 6 hrs, 9.75g EPA & 6.75 gm DHA/day OR• placebo i.e. normal saline X 14 days
EN or PN as per MDs discretion
Stapleton CCM 2011
Fish Oils ONLYBolus
Separate from EN
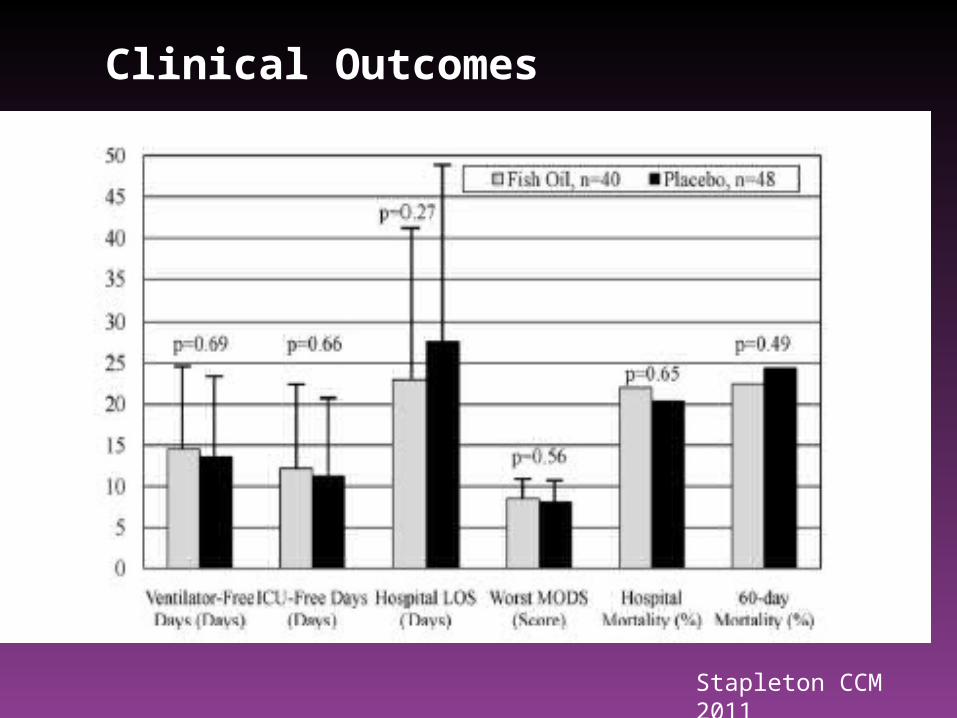
Clinical Outcomes
Stapleton CCM 2011
……..Because of different study design, difficult to combine with other studies of continuous administration in moderately well fed patients…..
Cook, Heyland JAMA Oct 2011

Fish Oils: Effect on mortality (n = 7)
2009: RR 0.67, 95% CI 0.51, 0.97, p = 0.003
No effect , statistical heterogeneity!
INTERSEPT data not included

Fish oils: effect on mortality removing bolus RCTs
1

EN fish oils: with new RCTs
Effect on mortality disappears when bolus studies are included
clinical heterogeneity-studies using bolus fish oils are methodologically different
- one RCT does not have GLA, antioxidants
statistical heterogeneity with the addition of the bolus studies

Parenteral Fish Oils
IV lipid
emulsion
1

Type of Lipids (PN)
2009 Recommendation
There are insufficient data to make a recommendation
on the type of lipids to be used in critically ill patients
receiving parenteral nutrition
IV lipid
emulsion
Fish Oil containing vs LCT/MCT or LCTOlive Oil containing vs LCT/MCT or LCTLCT + MCT vs LCTLCT vs LCT
New RCTs = 4New RCTs = 4

N = 25 septic pts
PN + Fish Oil vs. PN + soybean oil
p = 0.004
Barbosa Crit Care 2010

Wang Inflammation 2009
N = 56 patients with SAP, China
PN with Fish Oils (+ LCT) vs PN (LCT) X 5 days
Fish Oils improved plasma IL-10 levels, decreased HLA= anti-inflammatory
No effect on clinical outcomes

N= 28 patients with Severe Sepsis, Taiwan
Supplementation with Fish Oils 100 mls/day X 5 d vs. Placebo (saline)
Reduction in APACHE 3 score:• improved more in Fish oil group Days 3, 5 & 7 (p =0.03-0.004)
Khor Asian J Surg 2011

Procalcitonin levels
Procalcitonin levels are a marker of inflammatory response
No difference in hospital or length of stay between the groups
Khor Asian J Surg 2011

N = 61 patients with ARDS, India
Supplementation with Fish Oils + EN vs. EN alone X 14 days
Oxygenation •P/F ratio: no differences• worsening in P/F ratio: higher in control group (p=0.0004)
Mortality: trend towards lower in Fish Oil group (p = 0.10)
Ventilation, ICU LOS: no difference
Gupta Ind J Crit Care Med 2011
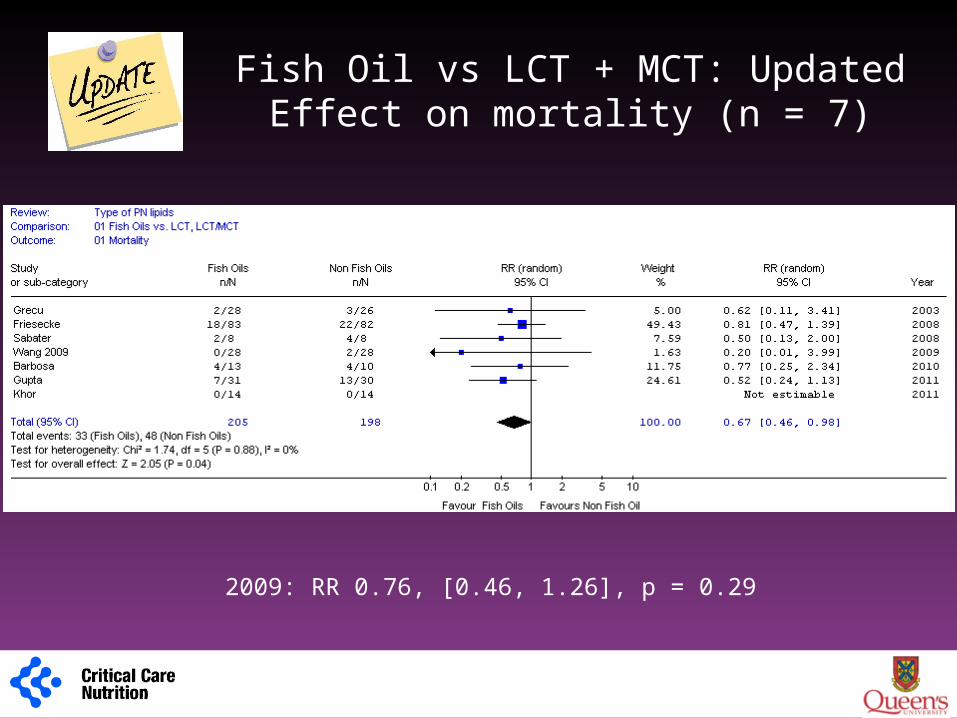
Fish Oil vs LCT + MCT: Updated Effect on mortality (n = 7)
2009: RR 0.76, [0.46, 1.26], p = 0.29
1

Fish Oil vs LCT or LCT + MCT: Effect on infections (n = 3)
2009: RR 0.77 [0.39, 1.49], p = 0.43
1

PN lipids: with new RCTs
Other lipids: no changes fish oils: studies with different designs
2 studies of lipids in PN 2 studies of supplemental fish oils
fish oils: signal for reduction in mortality fish oils: still no effect on infections
1

Glutamine supplementation?
1

EN Glutamine
2009 Recommendation
Based on 2 level 1 and 7 level 2 studies, enteral glutamine
should be considered in burn and trauma patients. There
are insufficient data to support the routine use of enteral
glutamine in other critically ill patients
Chinese Chinese RCTsRCTs
New RCTs = 2New RCTs = 2
PN Glutamine2009 Recommendation
Based on 17 studies, when parenteral nutrition is prescribed to critically ill patients, parenteral supplementation with glutamine, where available, is strongly recommended. There are insufficient data to generate recommendations for intravenous glutamine in critically ill patients receiving enteral nutrition
Grau 2011Grau 2011Andrews 2011Andrews 2011Wernerman 2011Wernerman 2011Eroglu 2009Eroglu 2009Perez Barcena 2010Perez Barcena 2010+ possibly 3 Chinese RCTs+ possibly 3 Chinese RCTs
New RCTs = 5New RCTs = 5

• 10 centres in Scotland • 502 Patients expected to be in ICU for at least 48h and required PN
meet at least half their requirements• Randomized 2.6 days after admission to ICU• Trial PN isocaloric and isonitrogenous, given for up to 7 days
unless died or stopped PN» Glutamine 20g/d» Selenium 500μg/d» Both» Neither
• Median duration of study PN was 4-5 days
Andrews BMJ 2011:342

The SIGNET Trial – RESULTSThe SIGNET Trial – RESULTS
Effect of GlutamineEffect of Glutamine
No significant differences
Confirmed infections within 14 daysMortality
No significant differences

• Right patient population?– Only about half getting PN at time of randomization
• Timing of intervention?– Started too late (2.6 days plus time to get PN running)
• Inadequate exposure to intervention?– Too small of dose– Too short of duration (4-5 days)
The SIGNET Trial – The SIGNET Trial – QuestionsQuestions!!

Multicenter trial in Spain
127 patients with APACHE II score >12 and requiring PN for 5–9 days
Standard PN vs. Supplemented with 0.5 g/kg/d of Ala-Gln dipeptide
Enrolled patients received only 5-6 days of PN
Grau CCM 2011; 39

P=0.10 P=0.03Grau CCM 2011; 39

413 Patients given nutrition by EN and/or PN route
Within 72 hrs of ICU admission
Supplemented as IV L-Ala-Glutamine, 0.283 g/kg/day administered separate from PN vs. placebo (saline)
Primary endpoint SOFA; infections not recorded
No effect on SOFA
Wernerman Acta Anesthesiology 2011

Wernerman Acta Anesthesiology 2011
PN glutamine group: lower mortality PP p = 0.046ITT p = 0.098

Ahmet Eroglu Anesthesia Anal 2009
Critical Care 2010

PN GLN: mortality revised (n = 20)
2009 RR 0.71 [0.55, 0.52] p = 0.008

PN GLN: infections revised (n = 12)
2009 RR 0.76 (0.62, 0.93) p = 0.008

less effect on mortality, still a trend less effect on infections, still significant
PN GLN with new RCTs
1

Awaiting results

The REDOXS© Study REducing Deaths due to OXidative Stress
The REDOXS© StudyREducing Deaths from OXidative Stress
Study ChairDr. Daren Heyland
Enrolment completed, n =1200Results expected Summer 2011

Antioxidant supplementationParenteral Selenium
1

Supplemental Antioxidant Nutrients
2009 Recommendation:Based on 16 studies, the use of supplemental vitamins and trace
elements should be considered
Parenteral Selenium2009 Recommendation:
There are insufficient data to make a recommendation regarding IV/PN selenium supplementation, alone or in combination with other antioxidants, in critically ill patients
New RCTs = 5 New RCTs = 5

• Randomized, open-label, single-centre clinical trial
• 150 patients with SIRS/sepsis and a SOFA score of >5
•
• Patients in the Se group received 1,000 ug on day 1 followed by 500 ug/day on days 2–14
• Administered daily over 30 mins
• Patients in both groups received a standard Se dose (75 ug/day)
Lower mortality in patients with a higher APACHE p =0.10

Phase II study building on previous dosing work
35 Patients with SIRS and APACHE II >15
Randomized within 24 hrs of admission Received either placebo or IV Se as a
bolus-loading dose of 2,000 ug followed by continuous infusion of 1,600 ug/ day for 10 days.
Lower VAP (p =0.04) Lower SOFA at day 10 (p=0.01)

The SIGNET Trial – RESULTSThe SIGNET Trial – RESULTS
Effect of SeleniumEffect of Selenium
No significant differences
Confirmed infections within 14 days
P=0.12 P=0.02
Mortality

AOX combined mortality, n =20
2009 0.76 RR [0.64, 0.91], p = 0.002
Manazares et al in submission 2012

AOX combined Infections, n=10
2009 RR 0.94 [0.75, 1.17], p = 0.56
Manazares et al in submission 2012


still significant effect on reduction on mortality stronger reduction on infections reduction stronger signal in sicker patients selenium associated with a trend towards lower mortality
& infections
Antioxidants with new RCTs
1

Conclusion
• Many recent RCTs in area of critical care nutrition • Careful review of the articles is recommended• Recommendations for following not expected to change:
– Arginine– EN glutamine– PN glutamine– IV fish oils
• Recommendations for following may be upgraded:
Probiotics and AOX• Recommendations for the following pending discussion
– EN Fish Oils
• Other Societies for critical care: harmonize the evidence
