crystal-induced arthritis gerald f. falasca, m.d. johnson city, tn march 27, 2012 “all the pearls...
TRANSCRIPT

Crystal-Induced Crystal-Induced ArthritisArthritis
Gerald F. Falasca, M.D.
Johnson City, TN
March 27, 2012March 27, 2012
“All the Pearls in 50 Minutes”

The risk factors for gout were known to the
ancients.

Ben Franklin (1706 -1790)
"Be temperate in wine, in eating, girls, and sloth, or the Gout will seize you and plague you…"
-- Franklin

MAJOR ARTHRITOGENIC CRYSTALS
• Monosodium urate
• Calcium pyrophosphate dihydratte
• Hydroxyapatite
• Corticosteroid esters
• Calcium oxalate

MAJOR ARTHRITOGENIC CRYSTALS
• Monosodium urate
• Calcium pyrophosphate dihydratte
• Hydroxyapatite• Corticosteroid esters• Calcium oxalate

Risk Factors for Gout• Underexcretors (80%)• Male gender• Postmenopausal females• Obesity, metabolic synd.• Ethanol• Renal insufficiency• Plumbism• Medications (see separate)• Dehydration/low flow• Filipino ancestry• Fructose ingestion• Uromodulin kidney dis.
• Overproducers (20%)• Ethanol• High cell turnover states
(psoriasis, myeloprolif. disorders)
• Excessive purine ingestion• PRPP overactivity (x-linked)• HGPRT underactivity (x-
linked)• Beta aldolase deficiency• Sarcoidosis• B12 deficiency• Down syndrome• Glycogen storage dis. 3, 5, 7• Fever, post-op state

Risk Factors for Gout
• Obesity, metabolic syndrome
• Ethanol
• Diuretics
• Fructose ingestion
• Excessive purine ingestion

Hyperuricemia and Gout
• Dairy consumption is protective.
• Estrogen protective (suppresses URAT1, the proximal renal tubule epithelial cell anion exchanger ).
• Beer much worse than wine.

Overproducers
• 15-20% of gouty patients are overproducers.
• Distinguished by 24 hour uric acid excretion:– > 800 mg/d on regular diet.– > 600 mg/d on purine-free diet.

Drugs Associated with Hyperuricemia
• Diuretics (loop and thiazide types)
• Low-dose aspirin• Cyclosporine,
tacrolimus• Ethanol• Ethambutol• Pyrazinamide• Ritonavir,
darunavir, didanosine
• Levodopa
• Nicotinic acid, niacin
• Pancreatic enzymes• Rituximab• Basiliximab• Teriparatide• Filgrastim• Sildenafil• Diazoxide• Cytotoxic
chemotherapy

Drugs Associated with Hyperuricemia
• Diuretics (loop and thiazide types)
• Low-dose aspirin• Cyclosporine,
tacrolimus• Ethanol• Ethambutol• Pyrazinamide• Ritonavir,
darunavir, didanosine
• Levodopa
• Nicotinic acid, niacin
• Pancreatic enzymes• Rituximab• Basiliximab• Teriparatide• Filgrastim• Sildenafil• Diazoxide• Cytotoxic
chemotherapy
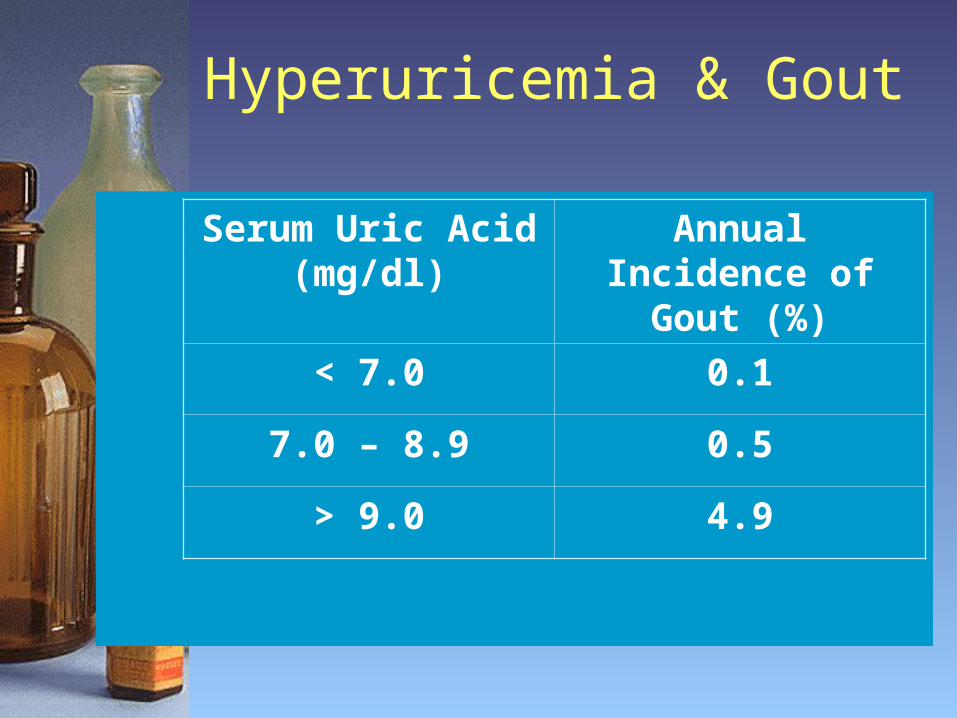
Hyperuricemia & Gout
Serum Uric Acid (mg/dl)
Annual Incidence of Gout (%)
< 7.0 0.1
7.0 – 8.9 0.5
> 9.0 4.9

Hyperuricemia and Gout
• Hyperuricemia (>7.0 mg/dl) in 5% - 8% of male population.
• Most (about ⅔) are forever asymptomatic.
• 80% of gouty patients have uric acid < 9 mg/dl.
• Above 10 mg/dl, risk rises rapidly.• Gout is the most common cause of
monarthritis in middle-aged and elderly men (8% yearly prevalence).

Who Almost Never Gets Gout?
• Pre-pubertal children
• Pre-menopausal women
• Look for enzyme defects in these patients.
• Look for familial kidney disease

Provocative Factors“Adding Insult to Injury”
• Ethanol• Cessation of
ethanol• Purine
overindulgence• Surgery• Trauma
• Overexercise• Fasting• Fever

The Fructose Connection
• Fructose raises uric acid levels in minutes.
• Biggest source of fructose: high fructose corn syrup.
• Sucrose does not seem to raise uric acid.

Link to Cardiovascular Dis.
• In experimental models, hyperuricemia causes:– Hypertension– Reduced perfusion– Endothelial dysfunction– Renal dysfunction
• Reversible with hypouricemics

Frequent Clinical Associations with Gout
• Hypertension
• Diabetes
• Hyperlipidemia
• Obesity
• Ethanol – the fuel

Gout & Kidney Disease
• Stones - Uric acid and calcium
• Urate nephropathy - chronic interstitial disease, not well defined.
• Uric acid nephropathy – acute tubular deposition of uric acid, with renal failure, not seen in gout.

Uromodulin-associated kidney disease
AKA: • Familial medullary cystic kidney
disease, type 2.
• Familial juvenile hyperuricemic nephropathy.
• Uromodulin storage disease.

Uromodulin (cont’d)
• Uromodulin (Tamm-Horsfall protein) accumulates in the thick ascending portion of Loop of Henle.
• Reduced excretion of uric acid.
• No renal deposition of urates.
• Autosomal dominant.

A Typical Attack of Gout
• Lasts several days to several weeks.
• May spread from joint to joint.
• Often accompanied by fever, leukocytosis.
• Gets worse as the years go on.
• Pain appears last, disappears first.
• Petite attacks occur (lasting hours).


Causes of Podagra
• MSU
• CPPD
• Hydroxyapatite
• Septic
• Psoriatic, Reiter’s
• Rheumatoid










Radiographic Hallmarks of Gout
• Overhanging edges
• Punched out lesions with sclerotic borders.
• Preservation of joint space (till late)
• Degenerative changes



The “Double Contour Sign” of Gout. Filippucci E, Grassi W Department of Rheumatology, University of Ancona, Italy


The Three Phases of Gout Treatment
• Treat acute attack
• Prevent new attacks
• Reduce uric acid level (sometimes)

Phase 1 - Termination
• NSAID
• Colchcine
• Intra-articular steroids
• Systemic steroids
• IL-1 inhibitors

NSAIDs
• Treatment of choice in otherwise healthy patient.
• Avoid in renal insufficiency and in peptic ulcer disease.
• Avoid salicylates (these cause swings in serum uric acid).

Intra-Articular Steroids
• One or a few joints.
• Not useful for polyarticular or soft-tissue gout.
• Make sure infection not present.

Oral Colchicine
• 1.2 mg followed by 0.6 mg 2 hrs later.
• Loading dose same in renal insufficiency.
• Maintenance (preventive) dose 0.6 mg qd or bid.
• 0.3 mg 2-3 times per week in dialysis patients (preventive).

Systemic Steroids
• Polyarticular attacks or fever.
• Longstanding attacks (>3-5 days).
• Need divided doses.
• Taper over 7-10 days.
• Start prophylactic agent (colchicine) as soon as possible.

Anakinra (Off-Label)
• Effective for acute attack in studies.
• Best in pts who cannot take steroids or colchcine.
• Expensive but 1 week of treatment may be affordable.
• Not for preventive use.• Other interleukin-1 inhibitors
currently in trials (rilonacept & canakinumab)
Adjunctive Measures
• Rest
• Ice
• Elevation
• Analgesics
• Anti-motility agents (if using colchicine or indomethacin)
• Continue hypouricemic agent if patient has been taking it.

Phase 2 - Preventive Therapy
• Colchicine or NSAID.• Always use when beginning a
hypouricemic drug.• Continue several weeks to years
(depending on tophi, serum uric acid).
• Always use before surgery in previously gouty patient.

Phase 3 - Hypouricemic Therapy
• Not every patient needs it.
• May not need it in:– Very elderly– Non-compliant– Infrequent attacks and no tophi
• May exacerbate attacks early on

Goals of Hypouricemic Treatment
• Aim for serum uric acid under 6, preferably near 5 for some chronic gouty patients.
• But remember:– allopurinol toxicity more likely with
higher dose.–More likely with renal insufficiency.

Hypouricemic Agents
• Allopurinol
• Febuxostat
• Probenecid
• Pegloticase
• Losartan (off-label)
• High-dose salicylates (off-label)
• Vitamin C (off-label)

Hypouricemic Therapy
• Don’t start hypouricemic agent during acute attack.
• Use probenecid first; it’s safer.
• Don’t use probenecid if:– overproducer– creat clearance < 35-50 ml/min.– history of kidney stones.

Reasons for Hypouricemic Treatment Failure
• Need lower uric acid levels than “normal.”
• Non-compliance.
• Renal insufficiency.
• Rapid dissolution of tophi.• Rapid elimination of oxypurinol
(may occur with combined allopurinol and probenecid).

Asymptomatic Hyperuricemia
• Don’t treat it (this advice may change in future)
• Exception: Patients getting chemotherapy for leukemia, lymphoma.

Major Toxicities of Allopurinol
• Increased gout attacks early on (use prophylaxis)
• Rash (may be severe)
• Stevens-Johnson syndrome
• Vasculitis
• Hepatitis
• Renal failure (interstitial nephritis)
• Bone marrow suppression

Allopurinol Hypersensitivity Syndrome
• Fever• Rash• Renal Failure
• Hepatic injury• Leukocytosis• Eosinophilia (the
tipoff!)
• May be fatal. Hard to treat.
• Serious reactions to allopurinol reported
in 1 of 260 patients. Arthritis Rheum 29:82, 1986

Treatment of Stonesin Gouty Patients
• Allopurinol– calcium and uric acid stones
• Potassium citrate– calcium and uric acid stones– direct inhibitor of nucleation
• Fluids!

Treatment of Stonesin Gouty Patients
• Allopurinol– calcium and uric acid stones
• Potassium citrate – calcium and uric acid stones– direct inhibitor of nucleation
• Fluids!

Febuxostat
• Non-xanthine inhibitor of XO and XD.
• Better tolerated than allopurinol.
• Lower uric acid levels than allopurinol (53% vs. 21% met target of 6.0 mg/dl).
• Better dissolution of tophi.

Tophus ReductionMean Reduction in Tophus Area
Becker MA. N Engl J Med. 2005 Dec 8;353(23):2450-61. Febuxostat compared with allopurinol in patients with hyperuricemia and gout.
Group % Area Reduction P Value
Feb 80 mg 83 P = .08 (NS)
Feb 120 mg 66 P = 0.16 (NS)
Allop 300mg 50
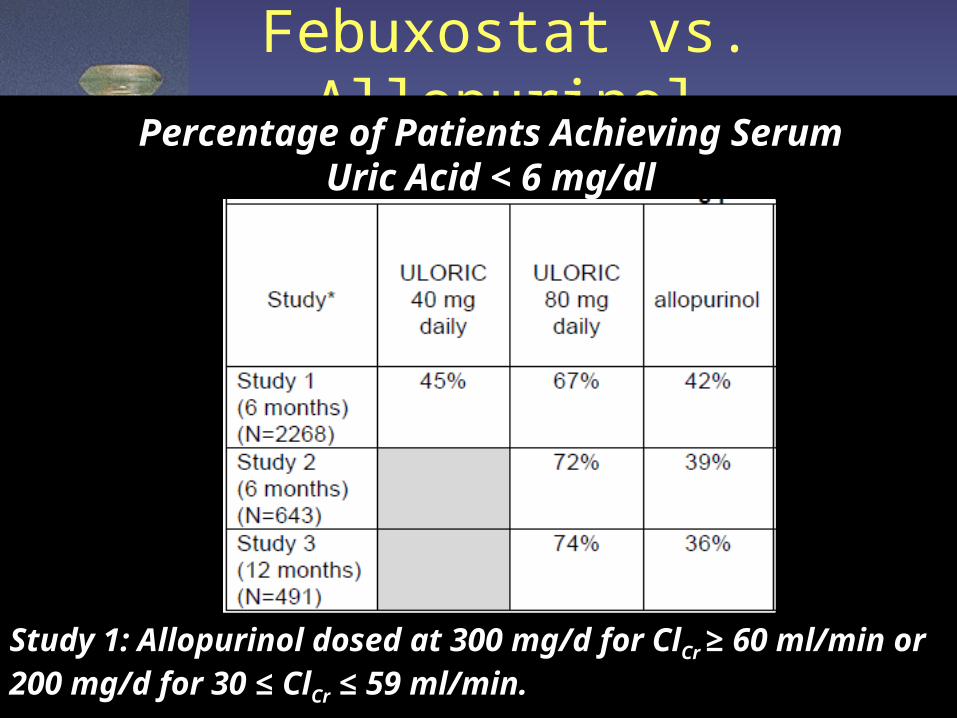
Febuxostat vs. AllopurinolPercentage of Patients Achieving Serum
Uric Acid < 6 mg/dl
Study 1: Allopurinol dosed at 300 mg/d for ClCr ≥ 60 ml/min or 200 mg/d for 30 ≤ ClCr ≤ 59 ml/min.

Febuxostat
• Adverse Reactions– Nausea– Gout flare (must be on prophylaxis!)– Elevated ALT, AST (3% > 3xULN)– Elevated CRP– Rash– Elevated CK

Febuxostat: Best Use
• Allopurinol failures
• Renal insufficiency
• Tophaceous gout

Allopurinol & Febuxostat Drug Interactions
• Life threatening interaction with azathioprine, 6-mercaptopurine.– Reduce dose of purine analogue by
approximately 2/3.
• Theophylline
• Other interactions also

Pegloticase
• For refractory chronic gout• Dissolves tophi in weeks to
months• Problems:– Anaphylaxis– Antibody formation– Not in G6PD defic.– $$$$

This is chronic refractory
gout!

Resistant Hyperuricemia?
• Try febuxostat 40 mg BID instead of 80 mg qd (off-label use).
• Short half-life supports this dosing.
• Currently in clinical trials

Losartan & Vit C (Off-Label)
• Lowers uric acid 0.3 – 1.3 mg/dl (dose range 25 – 200 mg/d).
• Uricosuric mechanism.• Useful when 24 hour uric acid is < 800
mg/d.• Maintain good hydration.• Effect is not seen with other ARBs.• Also consider fenofibrate (quite good
actually) and atorvastatin (both off-label).
• Don’t forget vitamin C (500 mg BID)


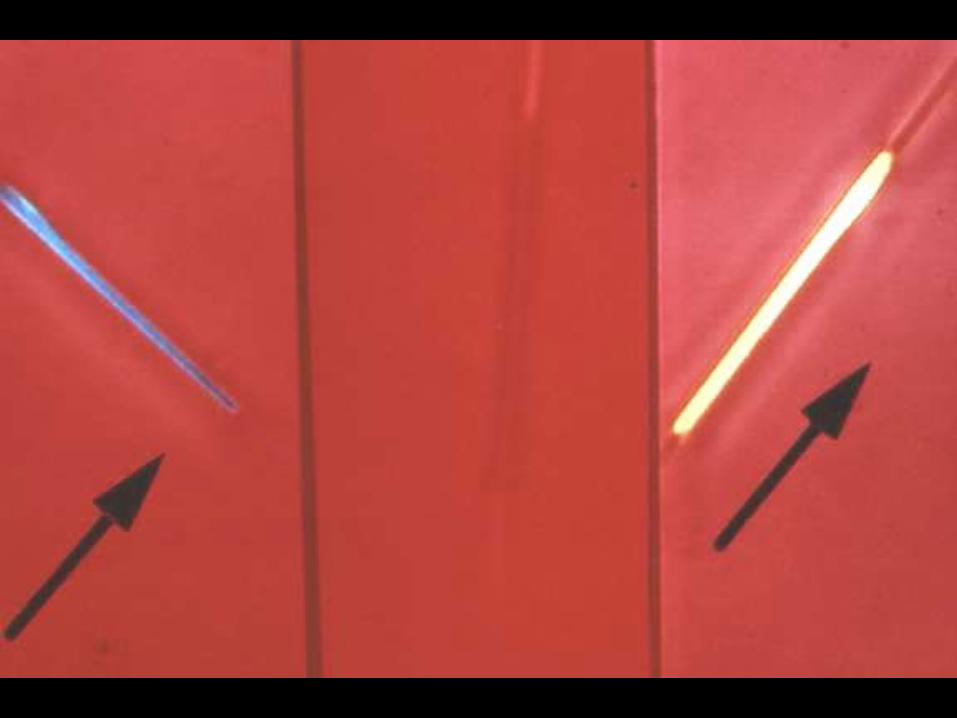

Gout
Yellow
Negative (when parallel)
G Y N
Synovial Fluid in Gout
• May be cloudy or clear.
• Inspect for tophaceous deposits.
• WBC – 2000 – 50,000 or more…
• Glucose normal.
• Between attacks, may have free crystals.
• Don’t forget to culture it.

Send Synovial Fluid for:
• Cell count Lavendar top• Crystals Green top• Culture Red top, no preserv.• Glucose Red top
• Protein, pH, complement – not helpful

Reasons MSU Crystals May Not Be Seen
• Needle in crystal-less sac.
• Ultramicroscopic size (need EM).
• Spherules.
• Settled out.
• Lack of time to search.
• Lack of experience.

On to Pseudogout!

Gout vs. Pseudogout
• Gout– hallux, ankle, knee, hand– younger, male
• Pseudogout– knee, wrist, ankle– older, female
• Almost any joint can be affected by either disease!






Screening Films to Getin Pseudogout Patient
•Knees
• Pelvis
•Hands

CPPD Deposition
• Wrist: triangular ligament
• Pelvis: symphysis pubis
• Knee: menisci
• Also: annulus fibrosis, articular capsules, bursae, ligaments, tendons

Clinical Associations with Psuedogout
• Aging• Previous joint
surgery• Previous joint
trauma• Familial types• Gout• Amyloidosis
• Hyperpara• Hemochromatosis• Hypomagnesemia• Familial hypocalciuric
hypercalcemia• Hypophosphatasia• Wilson’s disease• Ochronosis

Pseudo-DJD Pattern of CPPD
• 50% of CPPD patients.
• Wrists, MCPs, elbows, shoulders, knees. Note difference from usual DJD pattern.
• Heberden’s or Bouchard’s frequently found.
• May be acute or chronic.

Treatment of Acute Psuedogout
• Aspiration (more important than in gout!)
• Rest
• Intra-articular steroids
• NSAIDs
• Systemic steroids
• Colchicine?
• IL-1 Inhibitors?

Pseudogout Prevention
• Colchicine
• NSAID
• Magnesium?
• There’s no allopurinol for pseudogout (unfortunately).

The Basic (Non-Acidic) Calcium Phosphates
• Hydroxyapatite
• Calcium carbonate
• Octacalcium phosphate
• Tricalcium phosphate (whitlockite)
• Hydroxyapatite is non-birefringent.

Syndromes Associated with Hydroxyapatite
• Acute monoarthritis (pseudopseudogout)
• Acute calcific tendinitis, bursitis
• Scleroderma, dermatomyositis
• Heterotopic calcification
• Milwaukee shoulder
• Crowned Dens Synd.

Acute Apatite Monoarthritis
(Pseudopseudogout)• Is usually a peri-arthritis.
• Intense inflammation (looks septic)
• Synovial fluid often non-inflammatory.
• Often causes podagra (especially in younger women).
• Look for the telltale calcifications on radiographs.






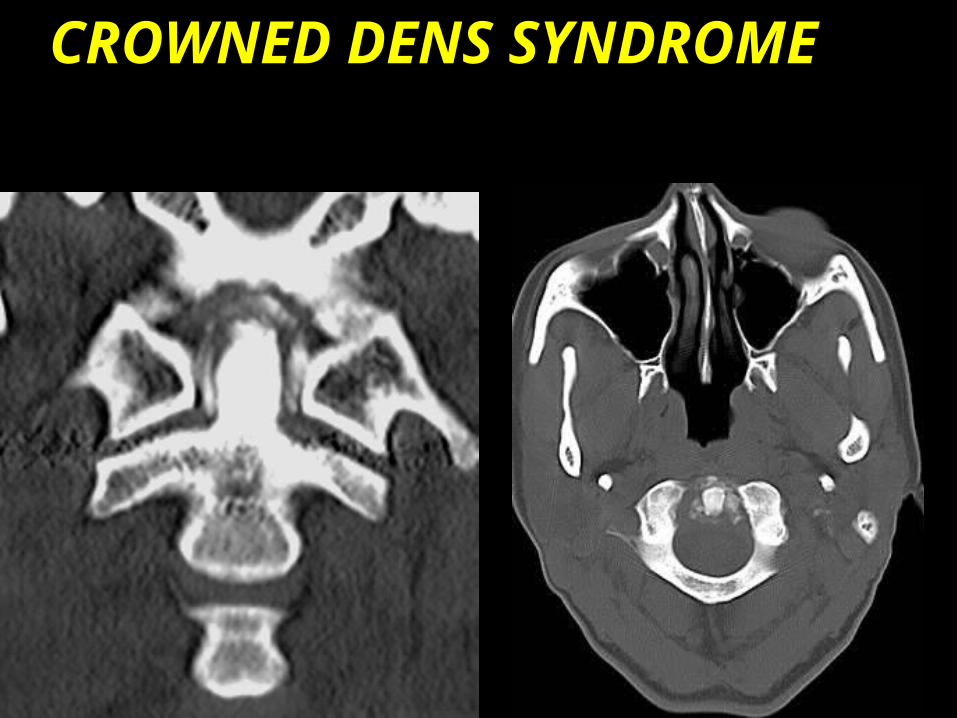
CROWNED DENS SYNDROME

Crowned Dens Synd
• Headache
• Pain with head rotation
• Shoulder myalgias
• Very elevated sed rate


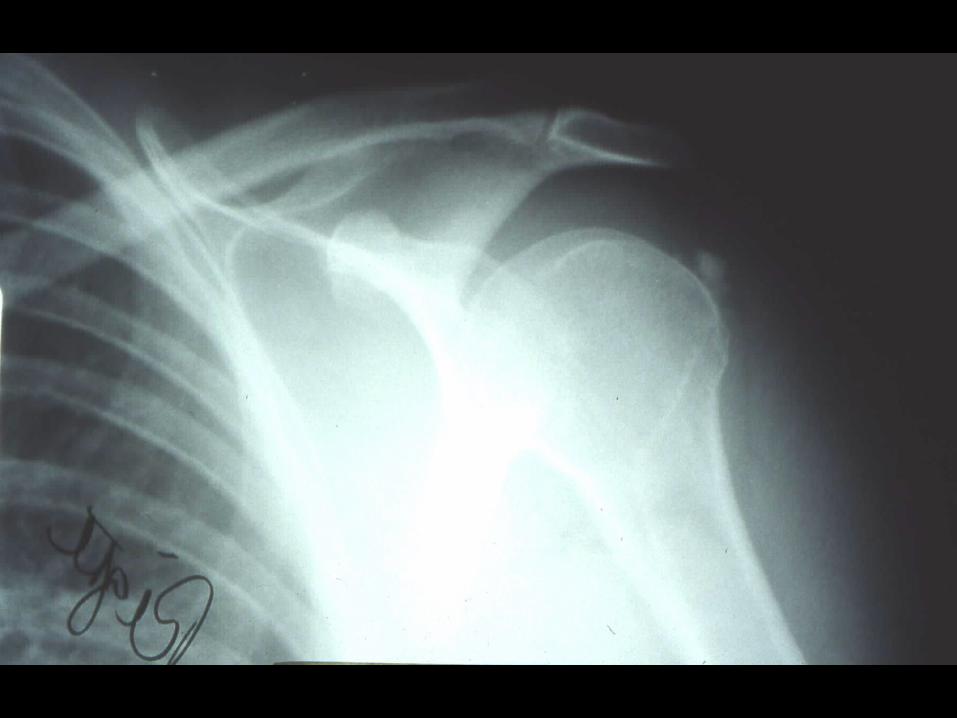
Milwaukee Shoulder
• Severe, destructive shoulder arthropathy.
• Seen in elderly females with DJD of shoulder.
• High-riding humeral head on radiographs (large rotator cuff tear).
• Non-inflammatory fluid with BCP crystals.


Steroid Crystal Arthritis
• Iatrogenic crystal arthritis.• Starts several hours after intra-
articular steroid injection.• Septic arthritis usually takes
longer. • Usually short-lived.• Ice it; may drain it, but don’t
operate on it.


Take Home Msgs
• Always give prophylaxis (colchicine or NSAID) before reducing uric acid.
• Longer courses of prednisone in divided doses for severe gout.
• Consider anakinra for acute treatment in some cases.
• Febuxostat is more effective than allopurinol in renal insufficiency.

Take Home Msgs
• The “crowned dens” is a cause of severe headaches, and a mimicker of PMR/GCA.
• Pseudopseudogout mimicks gout in young persons.
• CPPDD is associated with destructive osteoarthritis; consider methotrexate.

THE END