culture magazine - march 1981
TRANSCRIPT
·1
I 1 , ,
OXOID
Published as a service 10 microbiology by Oxoid Limiled
Vol2 No 1 March 1981
Anaerobes in Clinical Microbiology Ian Phillips, MA, MD., M.R.C.P., M.R.C. Path., Department of Microbiology, St Thomas'Hospital Medical School , London
During the past decade Ihe clinical spectrum of anaerobic in fection has been redefined, inilially largely by workers in the USA ' but later with con tribut ions from Britain,2·3 after many years of neglect. However, even as it was defined it changed. The infections lollowing large-bowel surgery which received most attention are now much less common because 01 the effectiveness 01 prophylactic measures, while on the other hand pseudomembranous colitis has been added with the recognition of the aetrological role 01 C/. diffiCi/e .In addition there have been Important discoveries in the field of antimicrobial sensitivity, and Important changes. lncreflsed clinical interest has placed a considerable burden on the diagnostic laboraloryin which cumbersome time-consuming techniques are usually inappropriate and rapid diagnosis is olten a higher goal than accurate taxonomy.
CLINICAL MANIFESTATIONS OF ANAEROBIC INFECTION
Anaerobic infections present in three general clinical patterns. The first,distinctlyuncommon,is a group 01 highly characteristic syndromes associated with clostridial intoxications. The second, also uncommon, is a group of progressive gangrenes of skin and subcutaneous tissues associated with ill-defined mixtures of anaerobes and aerobes the synergistic gangrenes. Thi rd,and much more common but unti I recently least associated with anaerobes, are the pyogenic inlections. both acute and chronic, which may be complicaled bybacteraemia and metastatic spread of infection.
Clostridial intoxications Tetanus, botulism, gas gangrene and C/. pertringens lood poisoning are all well known syndromes.3 Each is diagnosed primarily on clinical grounds and the role olthe laboratory is largely confi rmatory. However, pseudomembranous col it is has only been recognised relatively recen tly. Usually the pallent has received an antibiotic, most often clindamycin though almost all other antibiotics may be involved , and presents with profuse diarrhoea and sometimes abdominal distension and pain. The clinical diagnosis is
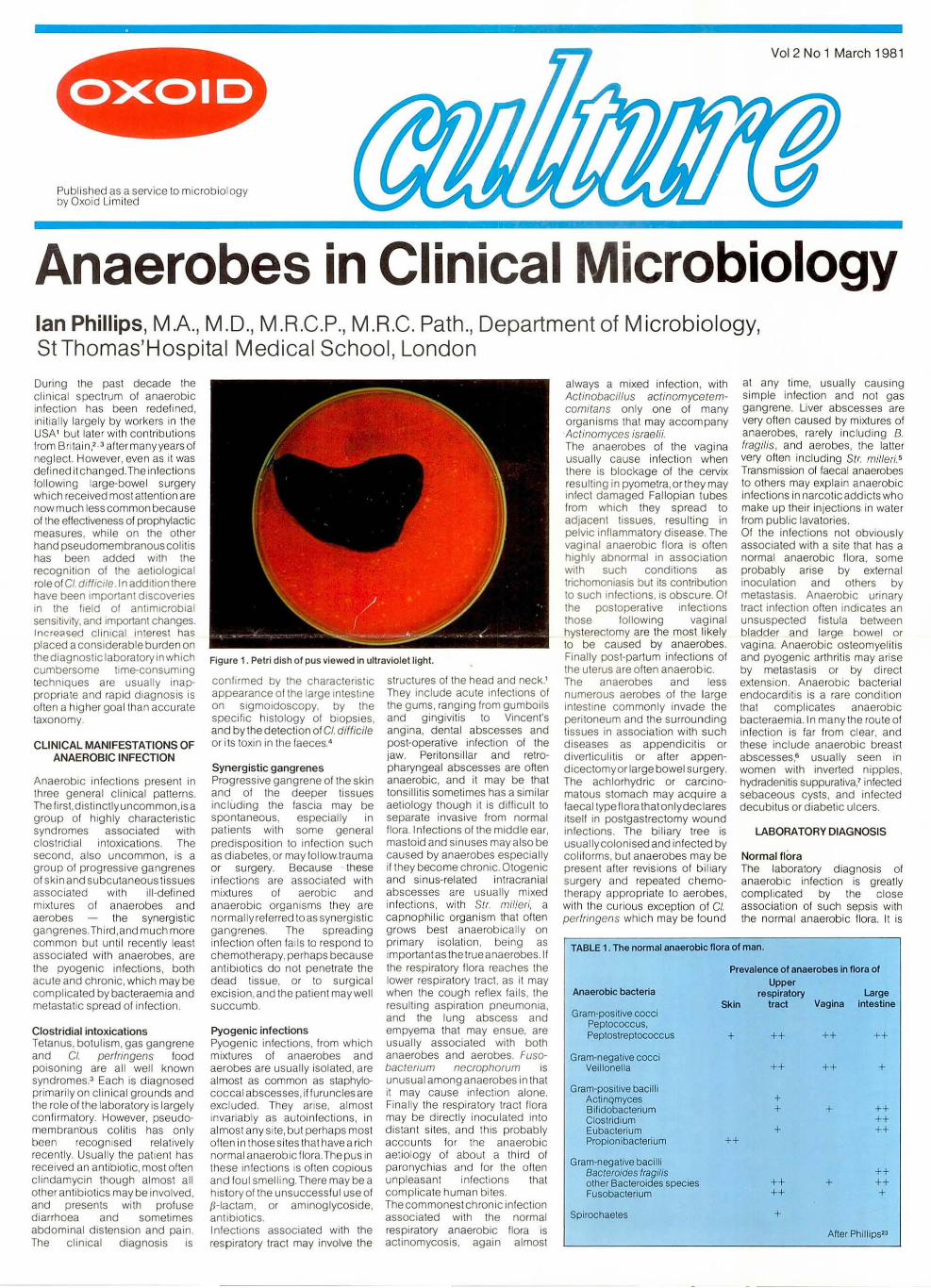
Figure 1 . Petri dish of pus viewed in ultraviolet light.
confirmed by the characteristiC appearance of the large intestine on sigmoidoscopy. by the specilic hislOlogy 01 biopsies. and by the detection 01 C/. diffici/e or its toxin in the faeces."
Synergistic gangrenes Progressive gangrene of the skin and 01 the deeper tissues including the fascia may be spontaneous, especially in patients with some general predisposition to infection such as diabetes, or may follow trauma or surgery. Because these infections are associated with mixtures of aerobic and anaerobic organisms they are normally referred toas synergistic gangrenes. The spreading infection often fails to respond to chemotherapy. perhaps because antibiotics do not penetrate the dead tissue, or to surgical exciSion, and the patient may well succumb.
Pyogenic infections Pyogenic inlections. Irom which mixtures of anaerobes and aerobes are usually isolated, are almost as common as staphylococcal abscesses, if furuncles are excluded. They anse. almost invariably as autoinfections, in almost any si te. but perhaps most often in those sites that havea rich normal anaerobic flora. The pus in these in fections is oiten copious and loul smelling. There may be a history 01 the unsuccesslul use 01 p-Iaclam. or aminoglycoside. antibiotics. I nlections associated with the respiratory tract may involve the
structures 01 the head and neck.' They include acute inlections 01 the gums. rang ing lrom gumboils and gingivitis to Vincent's angina, dental abscesses and post-operative infection of the jaw. Peritonsillar and retropharyngeal abscesses are olten anaerobic. and it may be that tonsi ll itis sometimes has a similar aetiology though it is difficult to separate invasive from normal flora. Infections of the middle ear, mastoid and sinuses mayalso be caused by anaerobes especially if they become chronic. Otogenic and sinus-related intracranial abscesses are usually mixed infections , wi th Str. millen', a capnophilic organism that olten grows best anaerobically on primary isolation . being as important as the true anaer~bes.lf the respi ratory Ilora reaches the lower respiratory tracl, as it may when the cough reflex lails. the resulting aspiration pneumonia, and the lung abscess and empyema that may ensue, are usually associated with both anaerobes and aerobes. Fusobacterium necrophorum is unusual among anaerobes in that it may cause infection alone. Finally Ihe respi ratory tract flora may be directly inoculated in to distant sites. and this probably accounts for the anaerobic aetiotogy of about a third 01 paronychias and lor the olten unpleasant infections that complicate human bites. The commonest chronic infection associated with the normal respiratory anaerobic flora is actinomycosis, again almost
always a mixed infection, with Actinobacillus actinomycetemcomitans only one of many organisms that may accompany Actinomyces israelii. The anaerobes of the vagina usual ly cause infection when there is blockage 01 the cervix resulting in pyometra. or they may inlect damaged Fallopian lubes lrom which they spread to adjacent tissues, resulting in pelviC inflammatory disease. The vaginal anaerobic flora is often highly abnormal in association with such conditions as trichomoniaSIS but its contribution to such infections, is obscure. Of the postoperative infections those following vaginal hysterectomy are the most likely to be caused by anaerobes. Finally post-partum in lections 01 the uterus are often anaerobic. The anaerobes and less numerous aerobes of the large in testine commonly invade the peritoneum and the surrounding tissues in association with such diseases as appendiCitis or diverticulitis or alter appendicectomyor large bowel surgery. The achlorhydric or carcinomatous stomach may acquire a laecaltypeflora that onlydeclares itself in postgastrectomy wound infections. The biliary tree is usually colonised and inlected by coli forms, but anaerobes may be present after revisions of biliary surgery and repeated chemotherapy appropriate 10 aerobes. wi th the curious exception 01 C/. pertringens which may be lound
at any time. usually causing simple infection and not gas gangrene. Liver abscesses are very olten ca used by mixtu res 01 anaerobes, rarely includ ing B. Iragi/is. and aerobes. the laller very often includ ing Slr. milleri.5 Transmission of faecal anaerobes to others may explain anaerobic infections in narcotic add icts who make up their injections in water from publ ic lavatories. 01 the inlections not obviously associated wi th a site that has a normal anaerobic flora, some probably arise by external inoculation and others by metastasis. Anaerobic urinary tract infection often indicates an unsuspected fistula between bladder and large bowel or vagi na. Anaerobic osteomyel it is and pyogenic arthritis may arise by metastasis or by direct extension. Anaerobic bacterial endocarditis is a rare condition that complicates anaerobic bacteraemia.ln many the route of in fection is fa r from clear, and these include anaerobic breast abscesses,s usually seen in women with inverted nipples, hydradenitis suppurativa! inlected sebaceous cys ts, and infected decubi tus or diabetic ulcers.
LABORATORY DtAGNOSIS
Normal flora The laboratory d iagnosis 01 anaerobic in fection is greatly compl icated by the c lose assoc iation 01 such sepsis with the normal anaerobic flora. I t is
TABLE 1. The normal anaerobic flora of man.
Anaerobic bacteria
Gram-positive cocci Peptococcus, Peptostreptococcus
Gram-negative cocci Veillonella
Gram-positive bacilli ActinQmyces Bifidobacterium Clostridium Eubacterium Propionibacterium
Gram-negative bacilli Bacteroides fragilis other Bacteroides species Fusobacterium
Spirochaetes
Prevalence of anaerobes in flora of Upper
respiratory Large Skin tract Vagina intestine
+
++
++
++
+ +
+
++ ++
+
++
++
+
+
++
+
++ ++ ++
++ ++ +
After Phillips23

difficult to take a sample that is known to be uncontaminated with saliva, faeces or vaginal sec retions, orwith anaerobes from the skin. Interpretation of culture results demands a knowledge of the flora found in these sites, summarised in Table 1. This lis t includes almoslall the anaerobes associafed with the three types o f anaerobic infection. It also
even by sophisticated methods. 1\ is imperative that all specimens for anaerobic bacteriological investigation should be submitted to the laboratory and processed as quickly as possible and pro tected from oxygen. Where the laboratory and the clinical department are in the same insWution these two requi rements are easily attained. Pus should be
TABLE 2. Recovery of anaerobes from samples of pus.
Macroscopic examination. Pus that is brownish rather than creamy is often anaerobic. A foul smell, dillerent from that of faeces to the trained nose, almost invariably means anaerobes. Brillant red fluorescence in ultraviolet Iight(Fig. 1) is almost always associated with the presence of B. melaninogeniGus which is present
Number of isolates '/r
on immediate after 4-6h Irom after 24h from culture CO2 bottle Stuart's swab CO2 bottle Stuart's swab
transport transport medium medium
Isolates 111 111 109 96 106 106 67 showing
minor decrease 3 11 40 17 25 36 major decrease 0 0 3 2 0 16 total loss 0 2 15 5 5 44
"Bacteroides 42 (incI.B. fragilis 12); Fusobacterium 18; non-spOring bacilli 6: Clostridium 13 (incLel. perfringens 6); anaerobic Gram-positive cocci 32.
includes many organisms that are taxonomically III-defined, and many that can be isolated only with great difficulty, or not at all by present fechniques. These difficult organisms, including the "extremely oxygen-sensitive" or "EOS" group appear, on present evidence, not to be associated with disease in man. Not injrequenlly, organisms that are rare or present in small numbers in the normal flora are more important in injection. Such organisms include F. necrophorum, CI. difficile and A. israelii. However, B. tragilis is much less numerous in the faecal flora than Its predominance In gut-associated infection would suggest. This appears to be associated with the fac t that B. tragifis is often capsulated whereas o ther bacteroides are not.e
Specimens The most common specimen submitted to the laboratory for the diagnosis of anerob ic infection is pus. With care thiS can often be collec ted with minimal contamination by normal flora, though this may involve the use of invasive techniques such as transtracheal or trans pleural aspiration in the case of the lower respiratory tract or laparoscopy in the caseof intraabdominal sepSis. Sometimes infected tissue samples are submitted, such as bone, necrotic muscle or skin. These too may be collected relatively free from contamination with normal flora. Finally, blood can usually be collected aseptically, though occasionally skin anaerobes such as P. aenes or anaerobic diphtheroids may contaminate samples. Superticial samples from the respiratory tract such as nasal , mouth orthroatswabs,expectorated sputum, specimens admixed with faeces, and vaginal secretions, yield cu lture resu lts that can be di ff icult or impossible to interpret.
aspirated and submitted either in the syringe or in a plain universal container which should be filled if possible: under these conditions even fastidious anaerobes will survive for some hours.9 Swabs should be avoided if possible, but if this is the only means of submitting a sample, Stuart's transport medium will ensure their surviva l for some hours.9 Table 2 shows some of the resul ts of qua ntitative studies on anaerobes in pus maintained under such condi tions. Other means of transport are avai lable and shou Id be considered if the laboratory is distant from the patient. They range in sophistication from commercial presentations of Stuart's or Amies' systems, gassed-out specimen tubes, and containers with simple oxygenremoving systems, to systems that take the anaerobic culture sys tem to the patien t' s bedside on a specially adapted "golf-buggy". If detailed anaerobic bacteriology is requi red there is no substitute for culture of the specimen immediately upon ils receipt in the laboratory, though a good specimen as defined above will probably yield as good a range of anaerobes after an overnight delay. The question of refrigeration is difficult. It is clear that some anaerobes do not tolerate it, buton the other hand the more robust organisms, including the aerobes tend to increase without it, perhaps giving a false impression of theircontribution to the infective process.
Rapid presumptive diagnosis Good clinical care demands a rapid diagnosis. The isolation and identification of anaerobes takes several days or even weeks, but fortunately a number of investigations enable an immediate differentiation of anaerobic (or mixed) infection from aerobic in fection to be made, especially when pus is submitted to the laboratory.'o
TABLE 3. Relationship between fluorescence of pus in ultraviolet light and isolation of anaerobes.
Fluorescence in ultraviolet light positive negative
Anaerobes
isolated 119 259
not isolated o
197
After Phillips, Taylor and Eykyn 'O
Adapted from Gargan and Phillips!!
Figure 2. Gram stained film of pus from anaerobic infection.
in a substantial minority of specimens (Table 3).
Gram-stained film . A film, not contaminated by secretions containing normal flora, but containing pus cells and a mixture of Gram-positive and Gramnegative cocci and bacilli is almost always an indication of anaerobic infection (Fig. 2). Sometimes the Gram-negative bacilli will have a characteristic fusiform or pleomorphic morphology. Gram-negative bacilli may be missed , and Gram-positive cocci over-emphasised , resulting in a half-hearted examination of cultures. The characteristic morphology of actinomyces is usually obvious in actinomycosis, provided one realises that they may resemble chains of cocci rather than branching bacilli (Fig. 3). CI. perfringens is usually all too obvious in wound exudat8' from gas gangrene, in which there are often few pus cells.
Immunofluorescence. There is little experience of thiS technique in Britain but reagents are now available for the detection of B. tragilis and 8. mefaninogenicus. Many who have used them find them valuable. Gas-liquid chromatography, Biochemists demand extraction and derivatisation of the characteristic short-chain fatty acids present in
• y \-
Figure 3. Gram stained film: actinomycosis.
Figure 4. Gas·liquid chromatograph of unextracted, underivatised pus from anaerobic infection.
anaerobic pus. We have found that the injection of unextracted, underivatised pus into a column packed with Chromosorb 101 and held at 20QoC gives reliable chromatograms(Fig. 4) with in minutes of the receipt of the specimen.lO The method may also be used for the early detection of certain anaerobes in blood cultures. Unfortunately, the eqUipment required for this investigation is expensive. Some results of the use of gas-liquid chromatography are shown in Table 4.
whole and 2.5% lysed (by freezing and thawing) horse blood, which we have used with a non-selective horse blood agar plate. Table 5 shows results of the application of its use. This simple, inexpensive medium enables us to detect the haemolysis of CI. perfringens, promotes black pigmentation among bacteroides, and inhibits most coliforms and some anaerobes. Another pass ibi I ity is a medium containing nalidixic acid in place oj neomycin.1S Other simple media are described in the Wadsworth Anaerobic Bacteriology Manual.'3 An efficient anaerobic chamber is essential for the isolation of all but a few anaerobes.'3.16 We have examined a number of efficient systems including a variety of anaerobic jars and gas replacement systems but lind that our needs are best met by a converted pressure cooker with a palladium catalyst, filled from a cylinder with a mixture of carbon dioxide (10%), hydrogen (t 0%), and nitrogen (80%) - again an inexpensive and safe solution to a
TABLE 4. Relationship of results of gas-liquid chromatography to culture.
Gas liquid chromatOgraphy Culture for anaerobes positive negative
positive 276 30
Confirmation of diagnosis Culture. Theultimateconfirmation of the presence of anaerobes in a specimen is their isolation on culture media. Solid media are far preferable to liquid media unless enrichment of a particular organism is required, such as that of heat-resistant Cf. perfrinr:;ens or of CI. difficile for which p-cresol may be added to a liquid medium. '2
The major problems in the isolation of anaerobes arise from the profusion of species: it is not unusual to find up to a dozen anaerobic or facultative organisms. ' Fortunately the clinical situation does not often demand complete speciation, and reports such as "A heavy
negative 52
136
problem.9 Anaerobic tents, cabinets and workstations are not necessary for the isolation of even quite fastidious species: a laboratory that is able to isolate B. melaninogenicus regularly from a simple anaerobic jar has little cause for concern. An easy check on the efficiency of any anaerobiC system is if a culture of Ps. aeruginosa fails to grow on a minimal medium such as Simmon's citrate agar.9
A final requirement is patience. Fastidious anaerobes seem to be at their most vulnerable during the phases of growth befor~ macroscopic colon ies appear. An advantage of an anaerobic cabinet containing an incubator is the possibility of examination o(
TABLE 5. Com mom anaerobes from 450 cases of anaerobic infection
Bacteroides B. fragilis 200 Peptostreptococcus anaerobius 83
asaccharolyticus 169 sp 34 thetaiotaomicron 58 ovatus 22 Peptococcus prevotii 71 vulgatus 15 asaccharolyticus 31 bivius 14 sp 42 melaninogenicus 14 Unidentified Gram·positive cocci 76 oraNs 12 other 26 Eubacterium /imosum 13
unidentified 59 other 6 total 589 sp 17
Fusobacterium Propionibacterium 1 F. nuc/eatum 44 Actinomyces israeli; 1
necrophorum 10 other 2 other 5
unidentified 35 Bifidobacteria 3 lotal 94
Clostridium perfringens 43 8 Veillonella other 32
Selenomonas sp 41
Adapted Irom Phillips, Taylor and Eykyn10
growth of mIxed anaerobes" are usually to be encouraged in routine work. Many selective media are available," ' " but it is likely that the average clinical laboratory will be able to use only one or two. We have developed a medium'o consisting of Brain Heart Infusion agar (Oxoid CM 375) containing 0.05% cysteine, 1 % vitamin Khaemin, 0.5% yeast extract and neomycin (1 00 mg/litre),plus 7.5%
culture plates Without removing them from their protective anaerobic environment. The identification of all but a few anaerobes is difiicult,14 but as has already been pointed out, is seldom necessary for clinical purposes. The prod uction of black pigmented colonies is characteristic of certain bacteroides, the commonest of which in clinical material is B. asaccharofyticus, probably somewhat easier to

isolate than the H melanmogenicus subspecies. However, other bacteroides such as B. bivius and B. ora/is may produce pigmented colonies, although seldom of a good rich black. Gram-staining allows organisms to be allocated totheirmaindivisions.This maybe aided by the disc determination of their sensitivity to kanamycin (1000 I'g), colistin (10 I'g), vancomycin (5 I'g) and penicillin (2 units) and occasionally olher agents,13 and by the demonstration that the organism fails to grow in 10% CO2 in air. Penicillin-resistant Gram-negative bacilli are usually, but not invariably B. tragilis. Blackpigmented, penicillin-resistant Gram-negative bacilli are usually the subspecies o f B. mefaninogenicus rather than B. asaccharolyticus. Peptococci may be distinguished from peptostreptococci by their resistance to novobiocin.17
If further identification is required, the use of the API or other similar systems, linked with gas-liquid chromatography of cultures in peptone-yeast-glucose medium,lO , 13, 14 will lead to the identification of biochemically active and robust species suCh as many of the bacteroides. More complex investigation tends to lead, especially in inexperienced hands, into a morass of variable reactions and confused taxonomy.
Serology. Infection with anaerobes gives rise to a specific antibody response. It has been suggested that this may be a good means of diagnosing deep anaerobic infections. Preliminary resu lts are encouraging.
Antimicrobial susceptibility The anlimicrobial sensitivity of anaerobes from any individual patient is often finally known when treatment has been given forsome days, and seldom contributes to the initial choice. This is determined, in part at least, from cumulative knowledge of what species are likely to beassociated with a given syndrome or site of
TABLE 6 . Activity of clindamycin, cefoxitin, metronidazole and tetracycline on anaerobes isolated from clinical samples, St. Thomas' Hospital.
%of isolates sensitive to
clindamycin (M IC < 1 mg/litre)
cefoxilin metronidazole tetracycline
Bacteroides spp. B. melaninogenicus Fusobacterium spp. C/ostndium perfringens Clostridium spp. Anaerobic Gram+ cocci Anaerobic Gram+ bacilli
infection and what is their likely sensitivity to ant ibiotics. It is thus the role of laboratories that specialise in anaerobic bacteriology to identify clinical isolates as far as possible, to determine the antimicrobial susceptibility patterns for each species, and fa make these results available to others in their vicinity, taking account of geographical variations. A rough guide to antimicrobial susceptibili ty can be obtained by disc testing, though there are many pitfalls.13 . 18 For example an isolate of B. Iragilis may appear resistant to metronidazole because the inoculum was too heavy, because the atmosphere was not fully anaerobic, or because the metronidazole had been inactivated by light. Erythromycin in particular is affected by even loca l variations in pH. Appropriate agents to be tested include penicillin (or ampicillin), clindamycin, erythromycin, chloramphenicol. tetracycline, cefoxitin and metronidazole. M ICs can be determined most readily by the use of a solid medium such as DST (Oxoid CM261) containing lysed horse blood " In (he IJSA, WilkinsChalgren agar has been advocated.JJ However, whatever method is used, a control organism such as B. (ragilis NCTC9343 of known sensitivity, should be included. Table 6 shows results for recent clinical isolates from SI. Thomas' Hospital, London, for some of these agents. Resistance is recognised for all the useful agents, but except in the
(MIC < 4mg/li tre) (M IC < 16mg/litre) (M IC < 8mgtlitre)
98 100 90
100 77 98 94
90 100
83 100
40 87 94
case of tetracycline, is rare in Britain as Table 6 shows. It is disturbing, however, that the resistance is p lasmld mediated and thus transferab le in many cases. 19
TREATMENT In most anaerobic infections surgery is almost always an important part of therapy, and sometimes it alone is sufficien t. Of the agents most often used metronidazole is probably most effective, and most free of unwanted effects.20 There is little evidence that its action on DNA is likely to be harmful to man.21 Clindamycin isalsoeifective,22 but is used less than formerly because of the problem of pseudomembranous colitis. Cefoxitin has not yet received sufficient clinical investigation for a decision on its relative meri ts to be made with confidence. Ch loramphenicol is particularly useful for infections of the central neNOUS system, as it crosses the blood-brain barrier well , and attacks aerobes as well as anaerobes. Some organisms, notably the toxigenic clostridia, are penicillin-sensitive, and benzylpenicillin remains the antibiotic of choice in tetanus, and gas-gangrene though not for CI. difficile infections.
CONCLUSION As the clinician's interest in anaerobic infection has increased, laboratories have risen to the new challenge. It is within the capacity of any laboratOlY to ensu re that
tOO 80 97 100 96 96
lOa 95 97 80 93 80 86 88
After Phillips23
provided good specimens are received, the simple diagnosis "anaerobic infection p resent or absent" can be made w ith some confidence, and w ith sufficien t rapidity to help even the initial management of the patient. If the microbiologist combines these simple measu res w ith a knowledge of which particular organisms are likely to be associa ted with a particular cl inical syndrome and what is thei r likely antimicrobial susceptibility and the likely effect of antibacterials, he is li kely to be able to make an important contribution to patient management.
References 1. Finegold, S.M. (1977). Anaerobic
Bacteria in Human Disease. Charles Thomas, Springfield.
2. Phillips, I. and Sussman, M. (1974). Infection With non-spore-formmg anaerobic bacteria. Churchill livingstone, Edinburgh, London, New York.
3. Willis, A.T. (1979). AnaerobiC bacteflofogy:clinical and laboratory practice. 3rd edn, Butterworth, London.
4. Keighley, MRB. (t 979). In: Strachan, C.J.L.and Wise, R.(eds). Surgical SepsIs. Academic Press, London.
5. Bateman, N.T., Eykyn, S.J. and Phillips. I. (1975). Lancel, 1,657-659.
6. Leach, R.D., Eykyn, S.J., Phillips, I. and Corrin, B. (1979). Lancet, 1, 35-37.
Clostridium Difficile Agar Base and Supplement
The combination of fhe base medium (CM601) and the selective supplement(SR96) is deSigned to improve the isolation and recognition of C I. difficile.
Blaser Campylobacter Supplement CODESR98
A new Campylobacter supplement from CDC Atlanta which adds the selective virtues of amphotericin and cephalothin to the Skirrow formulation (SR69).
7. Leach, R.D., Eykyn,S.J., Phillips, I., Corrin, B. and Taylor, E. (1979). Brit. Med. J, 3, 5-7.
8. Kasper, o.l. (1976).J Infect. Dis., 133,79-87.
9. Gargan, RA. and Phillips, I. (1979). Med. Lab. Sci .. 36, 159-169.
10. Phillips, I., Taylor, E. and Eykyn S. (1980).lnlection, 8.suppI2,S 155-S158.
11. Werner, H., Schaal, K.P., Collee, J.G. and Marge1, W.(eds). (1980). Diagnosis and Therapy of Anaerobic Infections, Infection, 6, suppl2.
12. Larsen, H.E., Price, A.B., Honour, P. and Borriello, SP. (1978). Lancel, 1, t 063-1 066.
13.Sutter, V.l., Ci tron, o.M. and Finegold,S,M.(1980). Wadsworth Anaerobic Bacteriology Manual, 3rd edn. C.v. MosbyCo, SI Louis, Toronto, London.
14. Holdeman, L.V. and Moore, W.E.C. (t 978). VPI Anaerobe Laboratory Manual, 4th edn. Vi rginia Polytechnic Institute, Blacksburg, Virginia.
15.Wren, MWD.1(978). Med. Lab. Sci .. 35,371-378.
16.Collee, J.G. (1980). Infection, 8 , suppI 2,SI50-S152.
17.Wren, M.w.D., Eldon, C.P. and Dakin, G.H. (1977). J Clm. Palh .. 30,620-622.
18. Phillips, I. and Warren C. (1978), In: Reeves, O.S., Phillips, I., Williams, J.D. and Wise, R. (eds). Laboratory Methods in Antimicrobial Chemotherapy. Churchill Livingstone, Edinburgh, London, New York.
19. Tally, F.P.,Snydman,o.R.,Shimell, M.J. and Goldin, B.R. (1979). Metronidazole. Royal Society of MediCine International Con· gress and Symposium Series No. 18. Academic Press, London.
20. Eykyn, SJ. and Phillips. I. (1976). Brit. Med. J, 2,1418-1421
21.Phillips, I. and Collier, J. (eds). (1979). Metronidazole. Royal Socie\yof Medicine International Congress and Symposium Series No. 18. Academic Press, London.
22.Phillips, I. (1980). J. Antimlcrob. Chemother., in press.
23 Phillips, I. (1980). Annales de I'lnstitut Pasteur de Lille, in press.
I'
I I
I , ,
- ---
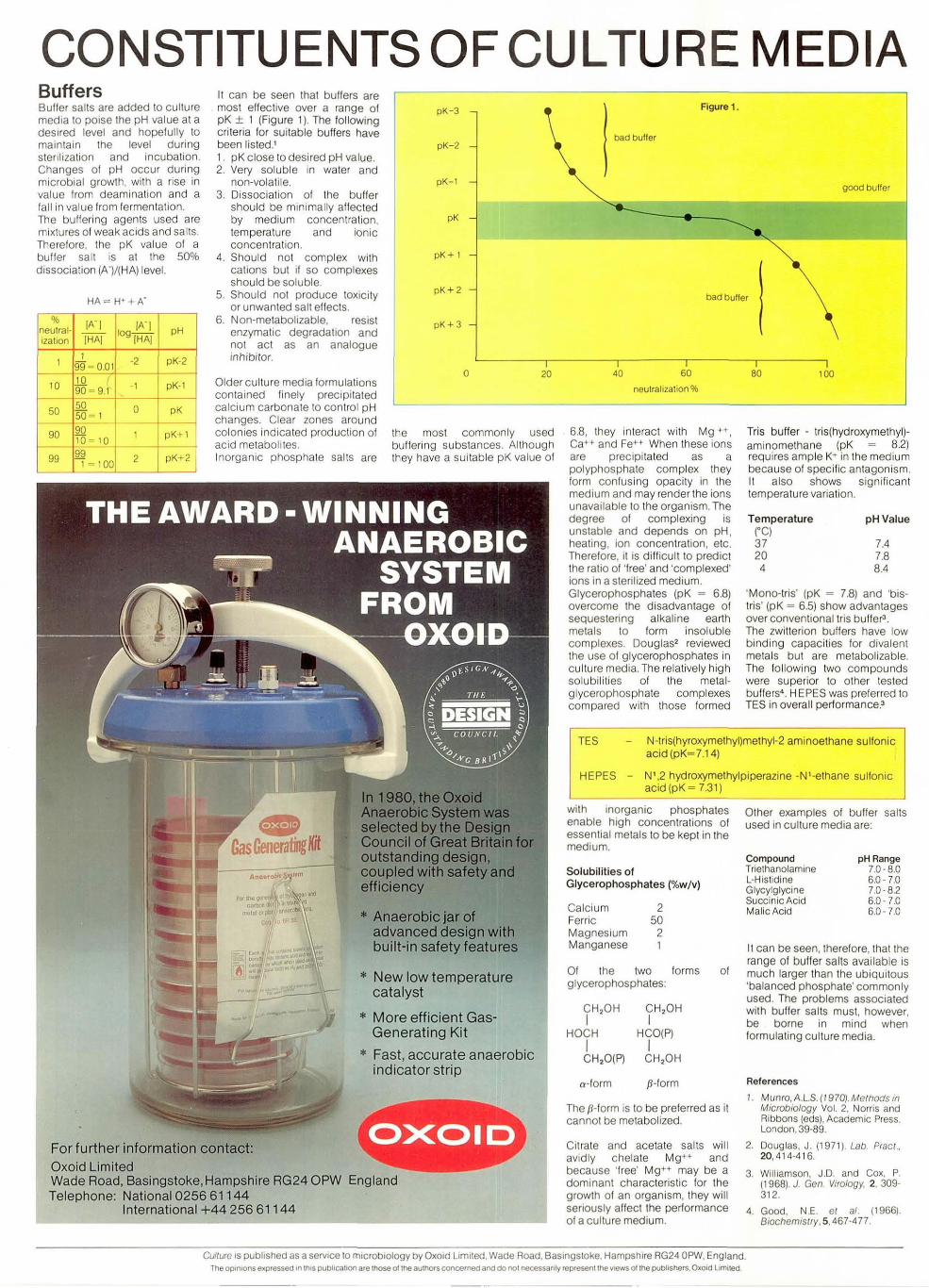
CONSTITUENTS OF CULTURE MEDIA Buffers Buller sails are added 10 cullure media 10 poise Ihe pH value al a desired level and hopefully to maintain the level during sterilization and incubation. Changes of pH occur during microbial growth, with a rise in value from deamination and a fall in value from fermentation. The bullering agents used are mixtures of weak acids and sal ts. Therefore, the pK value of a buller salt is at the 50% dissociation (A-)/(HA) level.
% lA- I lA-I neutral-IHAI
I091HAI
pH iza llon
I I
99 ~ 0 .0 1 -2 pK-2
10 10 .r 90 - 9.1 -1 pK-l
50 50 0 pK 50 - 1
It can be seen that bullers are most effective over a range of pK ± 1 (Figure 1). The following criteria for suitable buffers have been listed.' 1. pK close to desired pH value. 2. Very soluble in water and
non-volatile. 3. Dissociation of the bu ller
should be minimally allected by medium concentration, temperature and ionic concentration.
4. Should not complex with cations but if so complexes should be soluble.
5. Should not produce toxici ty or unwanted salt effects.
6. Non-metabofizable, resist enzymatic degradation and not act as an analogue inhibitor.
pK-3
pK-2
pK-l
pK
pK+ 1
pK + 2
pK+ 3
o 20
90 90 10 - 10
99 99 1- 100
1 pK+l
2 pK+2
Older culture media formulations contained finely precipitated calcium carbonate to control pH changes. Clear zones around colonies indicated production of acid metabolites. Inorganic phosphate sails are
the most commonly used bufferrng substances. Although they have a suitable pK value of
... Anaerobic jar of advanced design with built-in safety features
* New low temperature catalyst
* More efficient Gas-Generating Kit
* Fast, accurate anaerobic indicator strip
For further information contact: Oxoid Limited Wade Road, Basingstoke,Hampshire RG24 OPW England Telephone: National 0256 61144
International +44 256 61144
Figure 1.
bad buller
good buffer
bad buffer
40 60
neutralization %
6.8, they interact with Mg ++, Ca++ and Fe++ When these ions are precipita ted as a polyphosphate complex they form confusing opacity in the medium and may render the ions unavailable to the organism. The degree of complexing is unstable and depends on pH , healing, ion concentration, etc. Therefore, it is difficult to predict the ratio of 'free' and 'compfexed' ions in a sterilized medium. Glycerophosphates (pK ~ 6.8) overcome the disadvantage of sequestering alkaline earth metals to form insoluble complexes. Douglas2 reviewed the use of glycerophosphates in culture media. The relatively high solubilities of the metal-glycerophosphate complexes compared with those formed
80 100
Tris buffer - tri s(hydroxymethyl)aminomethane (pK 8.2) requires ample K+ in the medium because of specific antagonism. It also shows significant temperature variation.
Temperature (OCI 37 20 4
pH Vafue
7.4 7.8 8.4
'Mono-tris' (pK ~ 7.8) and 'bistris' (pK ~ 6.5) show advantages over conventional tris buffer3 .
The zwitterion buffers have low binding capacities for divalent metals but are metabolizable. The foll owing two compounds were superior to other tes ted buffers'. H EPES was preferred to TES in overall pertormance.'
TES N-tris(hyroxymethyl)melhyl-2 aminoethane sulfonic acid (pK~7.14)
HEPES - N' ,2 hydroxymethylpiperazine -N'-ethane sulfonic acid (pK ~ 7.31)
with inorganic phosphates enable high concentrations of essential metals 10 be kept in the medium.
Sofubilities of Glycerophosphates (%w /v)
Calcium 2 Ferric 50 Magnesium 2 Manganese 1
Of the two forms glycerophosphates:
CH,OH I
CH,OH I
HOCH HCO(P) I I CH,O(P) CH,OH
a-form p-form
of
The p-form is to be preferred as it cannot be metabolized.
Citrate and acetate salts will avidly chelate Mg++ and because 'free' Mg++ may be a dominant characteristic lor the growth of an organism, they will seriously affect the pertormance of a culture medium.
Other examples of buffer salts used in culture media are:
Compound Triethanolamine L-Histidine Glycylglycine Succinic Acid Malic Acid
pH Range 7.0-8.0 6.0 -7.0 7.0 -82 6.0- 7.0 6.0 - 7.0
It can be seen, therefore, that the range of bulfer salts available is much larger than the ubiquitous 'balanced phosphate' commonly used. The problems associated with buffer salts must, however, be borne in mind when formulating culture media.
References
1. Munro, A.L.s. (1970}. Mefhods in Microbiology Vol. 2, Norris and Ribbons (eds), Academic Press. London,39-89.
2. Douglas, J. (1971). Lab. Pracl .. 20,414-416.
3. Williamson, J.D. and Cox, P. (1968). J. Geo. Vlfo/ogy, 2, 309-312.
4. Good, N.E. et at. (1966). Biochemistry, S, 467-477 .
Culture is published as a service 10 microbiology by Oxoid Limited. Wade Road, Basingsloke, Hampshire RG24 OPW. England. The opInIons e~pressed In thIS pubhcallOO are those ot the authors concerned and do not necessarIly represent the VIews ollhe publishers. Oxold Limited