cure cure (oasis-4) clopidogrel in unstable angina to prevent recurrent ischemic events
TRANSCRIPT

CURECURE (OASIS-4)Clopidogrel in Unstable
Angina to preventRecurrent ischemic Events
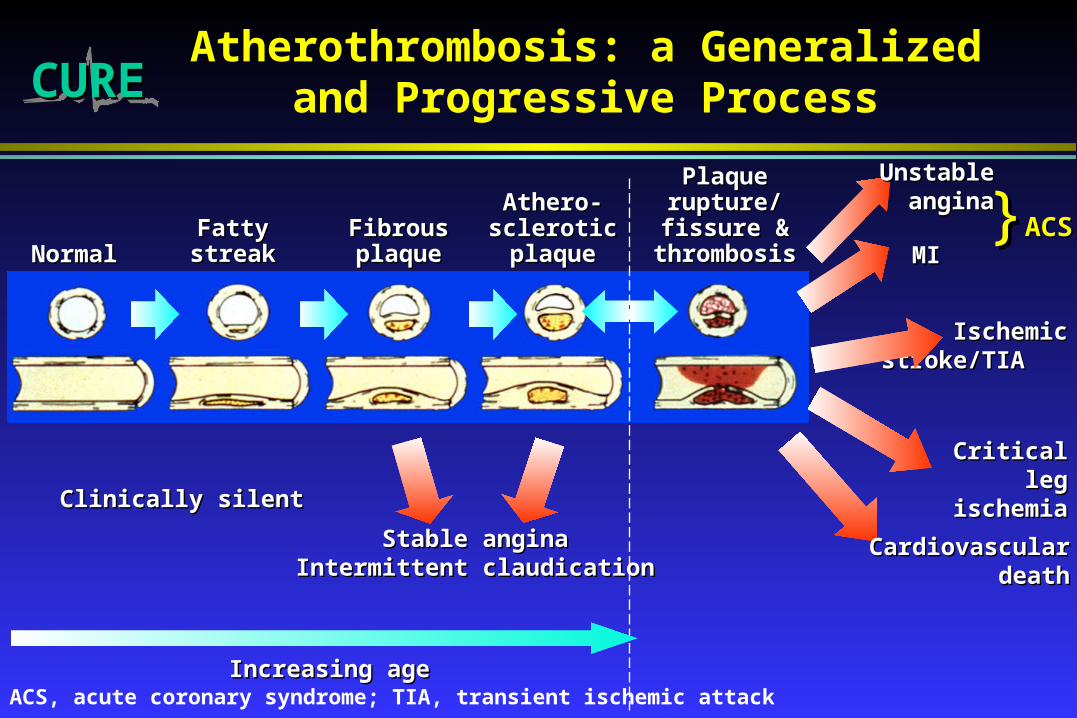
CURECUREAtherothrombosis: a Generalized and
Progressive Process
NormalNormalFattyFattystreakstreak
FibrousFibrousplaqueplaque
Athero-Athero-scleroticscleroticplaqueplaque
PlaquePlaquerupture/rupture/fissure &fissure &
thrombosisthrombosis MIMI
IschemicIschemicstroke/TIA stroke/TIA
Critical leg Critical leg ischemiaischemia
Clinically silentClinically silent
CardiovascularCardiovasculardeathdeath
Increasing ageIncreasing age
Stable anginaStable anginaIntermittent claudicationIntermittent claudication
UnstableUnstableanginaangina}}ACSACS
ACS, acute coronary syndrome; TIA, transient ischemic attack

CURECURE
Based on data from the Atherosclerotic Risk in Communities study (ARIC) of the National Heart, Lung, and Blood Institute, 1987–94. Includes Americans hospitalized with definite or probable MI or fatal CHD, not including silent MIs.
American Heart Association, 2001, Heart and Stroke Statistical Update
Epidemiology of MI and Angina
in the USA • Single largest cause of death
– 459 000 deaths in the USA in 1998
– 1 in every 5 deaths
• Incidence
– 1 100 000 Americans will have a new or recurrent coronary attack each year. Over 40% of people who experience a coronary attack in a given year will die of it in the same year
– 400 000 new cases of stable angina and about 150 000 new cases of unstable angina per year
• Prevalence
– 12 400 000 with a history of MI, angina, or both

CURECUREHospitalizations in the USA
Due to ACS
Acute Coronary SyndromesAcute Coronary Syndromes
1.5 million hospital admissions per year1.5 million hospital admissions per year
Unstable anginaUnstable angina Myocardial infarctionMyocardial infarction(Q-wave and non-Q-wave)(Q-wave and non-Q-wave)
Cairns J et al Cairns J et al Can J CardiolCan J Cardiol 1996;12:1279–1292 1996;12:1279–1292
750 000 admissions750 000 admissions 750 000 admissions750 000 admissions
CURECURE
Théroux P et al Circulation 1998; 97:1195–1206
The Role of Antiplatelet Therapy in Unstable Angina and Non-Q-wave MI
• Atherothrombosis is a generalized disease affecting the coronary, cerebral and peripheral circulations
• Unstable angina/non-Q-wave MI is one of the classic examples of the progression of atherothrombotic disease
• Platelets play a key role in thrombus formation associated with rupture of an unstable atherosclerotic plaque
• Angioscopic findings show that unstable angina is due to the formation of a platelet-rich thrombus
• Consequently, antiplatelet therapy is recognized as the foundation of long-term management
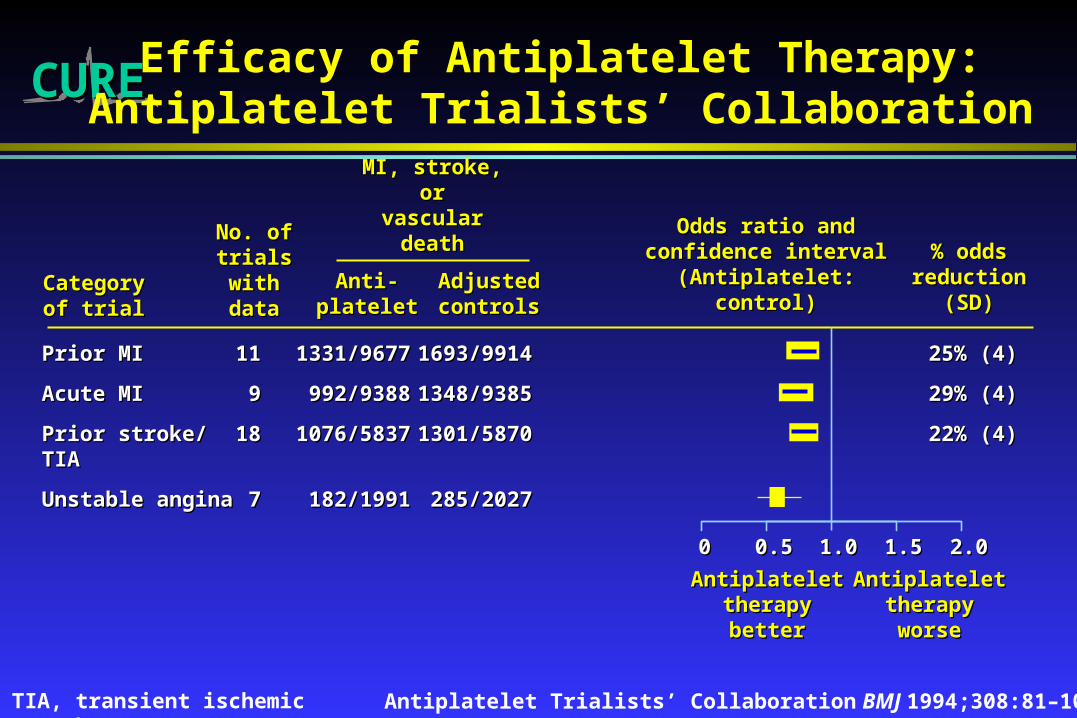
CURECURE Efficacy of Antiplatelet Therapy:Antiplatelet Trialists’ Collaboration
Antiplatelet Trialists’ Collaboration BMJ 1994;308:81–106
Prior MIPrior MI 1111 1331/96771331/9677 1693/99141693/9914 25% (4)25% (4)
Acute MIAcute MI 99 992/9388992/9388 1348/93851348/9385 29% (4)29% (4)
Prior stroke/Prior stroke/ 1818 1076/58371076/5837 1301/58701301/5870 22% (4)22% (4)TIATIA
Unstable angina Unstable angina 77 182/1991182/1991 285/2027285/2027
CategoryCategoryof trialof trial
No. ofNo. oftrialstrialswithwithdatadata
Anti-Anti-plateletplatelet
AdjustedAdjustedcontrolscontrols
Odds ratio andOdds ratio andconfidence intervalconfidence interval
(Antiplatelet:(Antiplatelet:control)control)
% odds% oddsreductionreduction
(SD)(SD)
MI, stroke, orMI, stroke, orvascular deathvascular death
00 0.50.5 1.01.0 1.51.5 2.02.0
AntiplateletAntiplatelettherapytherapybetterbetter
AntiplateletAntiplatelettherapytherapyworseworse
TIA, transient ischemic attack
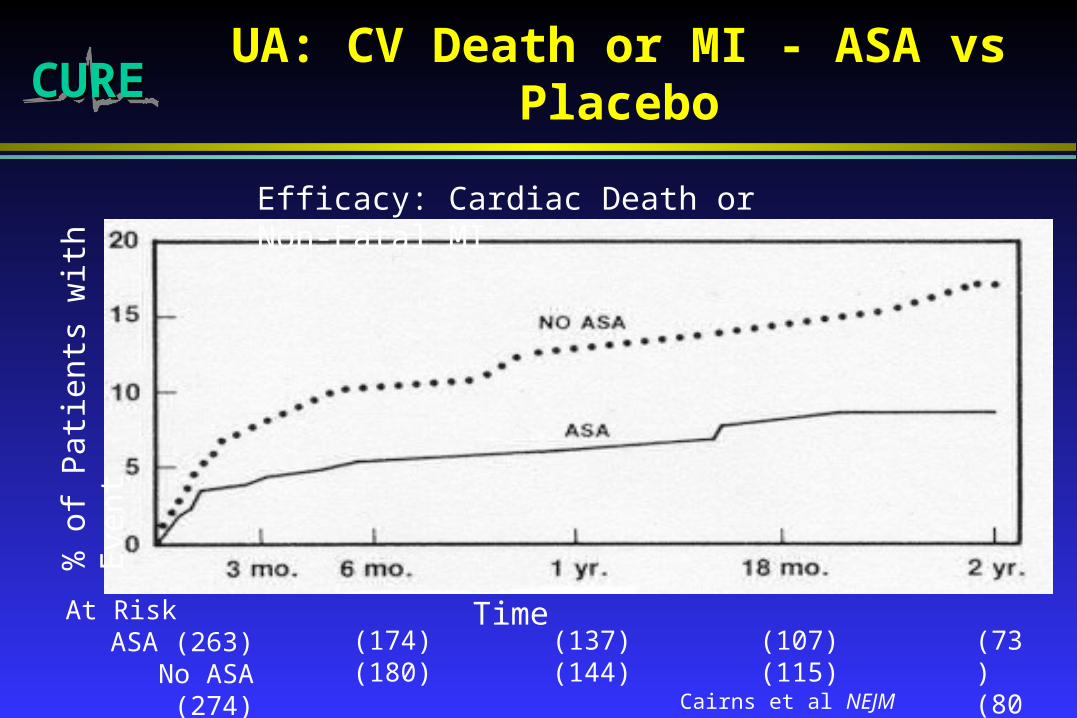
CURECURE UA: CV Death or MI - ASA vs Placebo%
of
Pat
ient
s w
ith E
vent
Cairns et al NEJM 1985;313:1369-1375
Efficacy: Cardiac Death or Non-Fatal MI
At RiskASA (263)
No ASA (274)(174)(180)
(137)(144)
(107)(115)
(73)(80)
Time
CURECURE The Role of an ADP Receptor Antagonist
• Clopidogrel is an advanced ADP receptor antagonist and inhibits platelet aggregation by antagonizing the effects of ADP
• Clopidogrel is indicated for the reduction of atherothrombotic events in patients with a history of stroke, MI or peripheral arterial disease.
• Clopidogrel is at least as safe as ASA• Combining clopidogrel with ASA may potentially lead to
greater benefit
Jarvis B et al Drugs 2000;60:347–377Antiplatelet Trialists’ Collaboration BMJ 1999;308:81–106CAPRIE Steering Committee Lancet 1996:348:1329–1339

CURECUREComplementary Mode of Action between
Clopidogrel and ASA
COX, cyclooxygenase; ADP, adenosine diphosphate; TxACOX, cyclooxygenase; ADP, adenosine diphosphate; TxA2, 2, thromboxane Athromboxane A2 2
Schafer AI Am J Med 1996;101:199–209
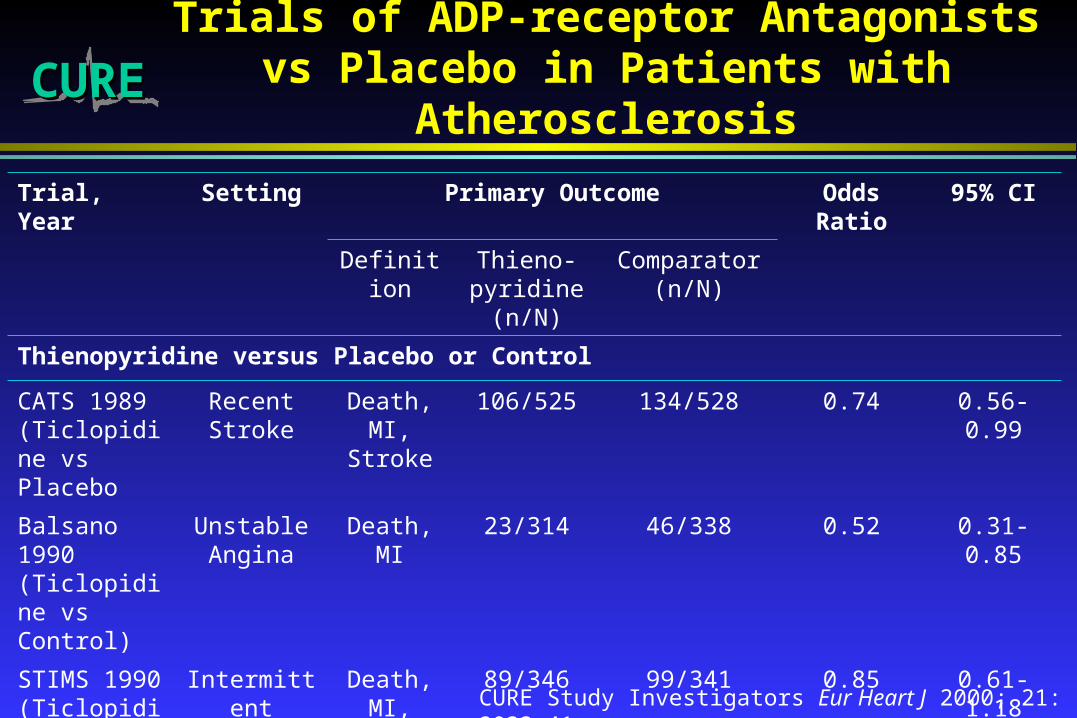
CURECURETrials of ADP-receptor Antagonists vs
Placebo in Patients with Atherosclerosis
Trial, Year Setting Primary Outcome Odds Ratio 95% CI
Definition Thieno-pyridine
(n/N)
Comparator (n/N)
Thienopyridine versus Placebo or Control
CATS 1989 (Ticlopidine vs Placebo
Recent Stroke
Death, MI,
Stroke
106/525 134/528 0.74 0.56-0.99
Balsano 1990 (Ticlopidine vs Control)
Unstable Angina
Death, MI 23/314 46/338 0.52 0.31-0.85
STIMS 1990 (Ticlopidine vs Placebo)
Intermittent Claudication
Death, MI,
Stroke
89/346 99/341 0.85 0.61-1.18
TOTAL 218/1185 279/1207 0.73 0.60-0.90CURE Study Investigators Eur Heart J 2000; 21: 2033-41.

CURECURE Trials of ADP-receptor Antagonists vs ASA
in Patients with Atherosclerosis
Trial, Year Setting Primary Outcome Odds Ratio 95% CI
Definition Thieno-pyridine
(n/N)
Comparator (n/N)
Thienopyridine versus ASA
TASS, 1989 (Ticlopidine vs ASA)
Cerebral Ischemia
Death, Stroke
306/1529 349/1540 0.85 0.82-0.97
CAPRIE, 1996 (Clopidogrel vs ASA)
Recent Stroke,
Previous MI or PVD
Death, MI,
Stroke
939/9599 1021/9586 0.91 0.83-1.00
TOTAL 1245/11128 1370/11126 0.90 0.83-0.97
CURE Study Investigators Eur Heart J 2000; 21: 2033-41.
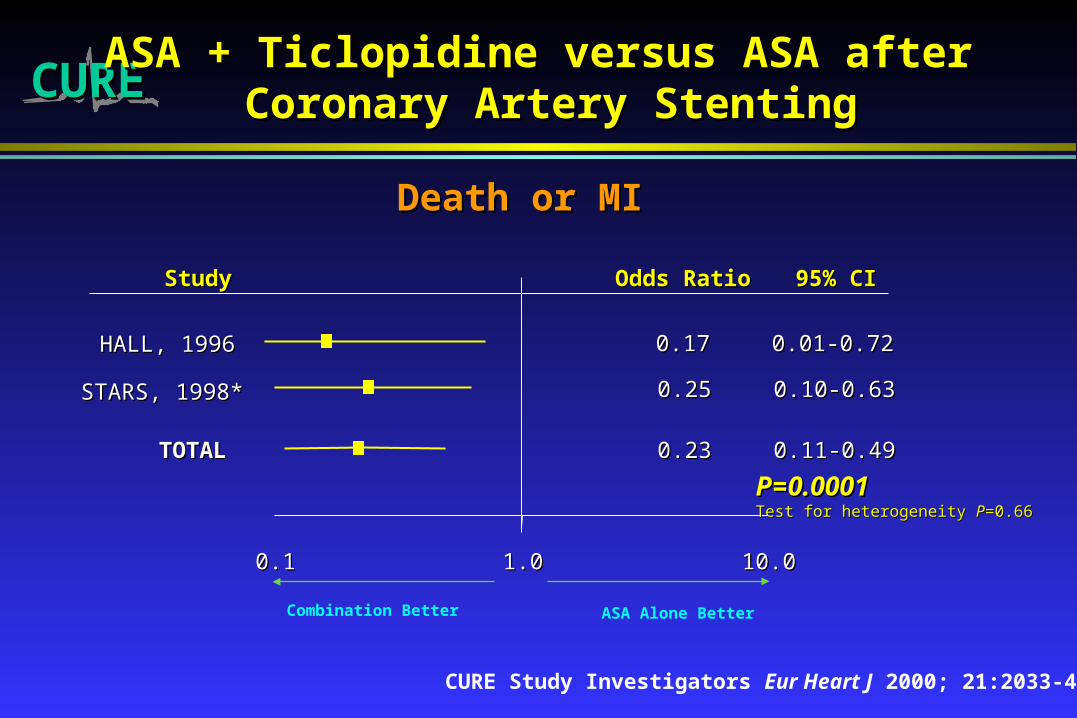
CURECURE
StudyStudy
HALL, 1996HALL, 1996
STARS, 1998*STARS, 1998*
TOTALTOTAL
0.10.1 1.01.0 10.010.0
Odds RatioOdds Ratio 95% CI95% CI
0.170.17 0.01-0.720.01-0.72
0.250.25 0.10-0.630.10-0.63
0.230.23 0.11-0.490.11-0.49
PP==0.00010.0001Test for heterogeneity Test for heterogeneity PP=0.66=0.66
ASA + Ticlopidine versus ASA after ASA + Ticlopidine versus ASA after Coronary Artery StentingCoronary Artery Stenting
Death or MIDeath or MI
CURE Study Investigators Eur Heart J 2000; 21:2033-41
Combination Better ASA Alone Better

StudyStudy
ISAR, 1996ISAR, 1996
MATTIS, 1998MATTIS, 1998
TOTALTOTAL
0.10.1 1.01.0 10.010.0
Odds RatioOdds Ratio 95% CI95% CI
0.310.31 0.11-0.910.11-0.91
0.610.61 0.26-1.430.26-1.43
0.510.51 0.33-0.780.33-0.78
P=0.002P=0.002Test for heterogeneity Test for heterogeneity PP=0.51=0.51
ASA + Ticlopidine vs ASA + Oral ASA + Ticlopidine vs ASA + Oral Anticoagulation after StentingAnticoagulation after Stenting
FANTASTIC, 1998FANTASTIC, 1998 0.660.66 0.33-1.300.33-1.30
STARS, 1998STARS, 1998 0.320.32 0.11-0.910.11-0.91
Death or MIDeath or MI
Combination Better ASA Alone Better
CURE Study Investigators Eur Heart J 2000; 21:2033-41
CURECURE

CURECUREEffect of Clopidogrel Alone or in Combination
with ASA on Thrombus Formation: Animal Model
-100
-80
-60
-40
-20
0
0 5 10 15 20 25 30 35 40 45 50
Time (min)
Clopidogrel + ASA (10 + 10 mg/kg)
Clopidogrel (10 mg/kg)
ASA (10 mg/kg) Placebo
Herbert JM et al Thromb Haemost 1998;80:512–518
Blood flow(% decrease)
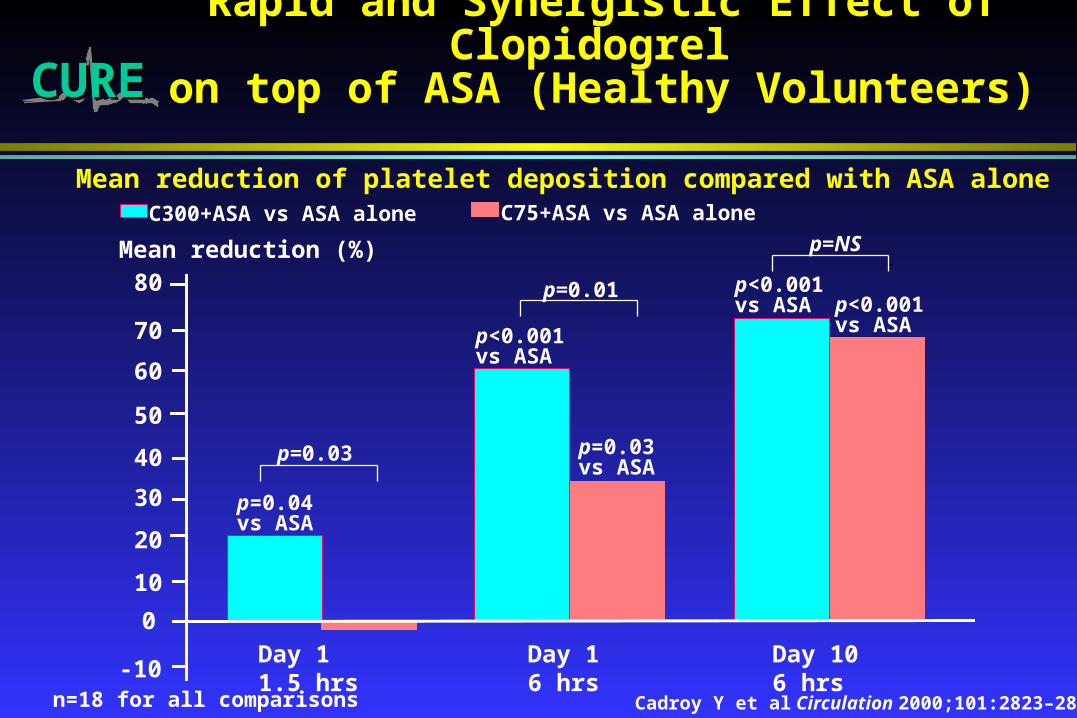
CURECURERapid and Synergistic Effect of Clopidogrel
on top of ASA (Healthy Volunteers)
Mean reduction of platelet deposition compared with ASA alone
Cadroy Y et al Circulation 2000;101:2823–2828
C75+ASA vs ASA aloneC300+ASA vs ASA alone
-10
0
10
20
30
40
50
60
70
80
Day 1 1.5 hrs
Day 1 6 hrs
Day 10 6 hrs
Mean reduction (%)
p=0.03vs ASA
p<0.001vs ASA
p=0.04vs ASA
p<0.001vs ASA
p<0.001vs ASA
p=0.03
p=0.01
p=NS
n=18 for all comparisons
CURECURE
•Randomized, double-blind, parallel group, clinical trial of clopidogrel vs placebo in patients with ACS
•All patients receive ASA (75-325 mg)
•International trial (28 countries)
•12,562 patients (482 Hospitals)
•Central randomization
•3-12 month Rx and follow-up
•Main outcomes: -CV death/MI, stroke
-Above + refractory ischemia
Study Design

CURECURE Study Objectives
To evaluate if clopidogrel is superior to placebo in preventing
a) CV death, MI, stroke (Primary at 0.045)
b) Above and refractory ischemia (Co-primary at 0.01)
CURECURE Inclusion Criteria
• Ischemic symptoms, suspected to represent UA or MI without ST segment elevation
• Randomized within 24 hours of onset of CP
• and ECG evidence of ischemia at inclusion or already elevated cardiac enzymes or Troponin I or T to at least 2 x ULN*
* Prior to June 1999, pts > 60 yrs with normal ECG allowed
Revised July, 1999
CURECURE Outcome Definitions (1/2)
CV Death: Excludes clear non-CV deaths
MI: Two of three usual criteria (CP, ECG or enzyme changes)
Stroke: Neurological deficit 24 hrs (CT/MRI encouraged)
Refractory Ischemia: Inhosp*: recurrent ischemia on max med Rx + ECG changes + intervention 1 day
After discharge: Rehosp for UA with ECG changes
Severe Ischemia*: Changes similar to in hospital Refractory Ischema, but no intervention
Recurrent Angina*: All other ischemic CP in hospital

CURECURE Outcome Definitions (2/2)
Major Bleeds: Significantly disabling, intraocular (vision loss), or transfusion of 2 units
Classified as Life Threatening if:
Hb > 5g/dl, hypotension needing IV inotropes, surgery to stop bleeding, symptomatic ICH or transfusion or 4 units of blood
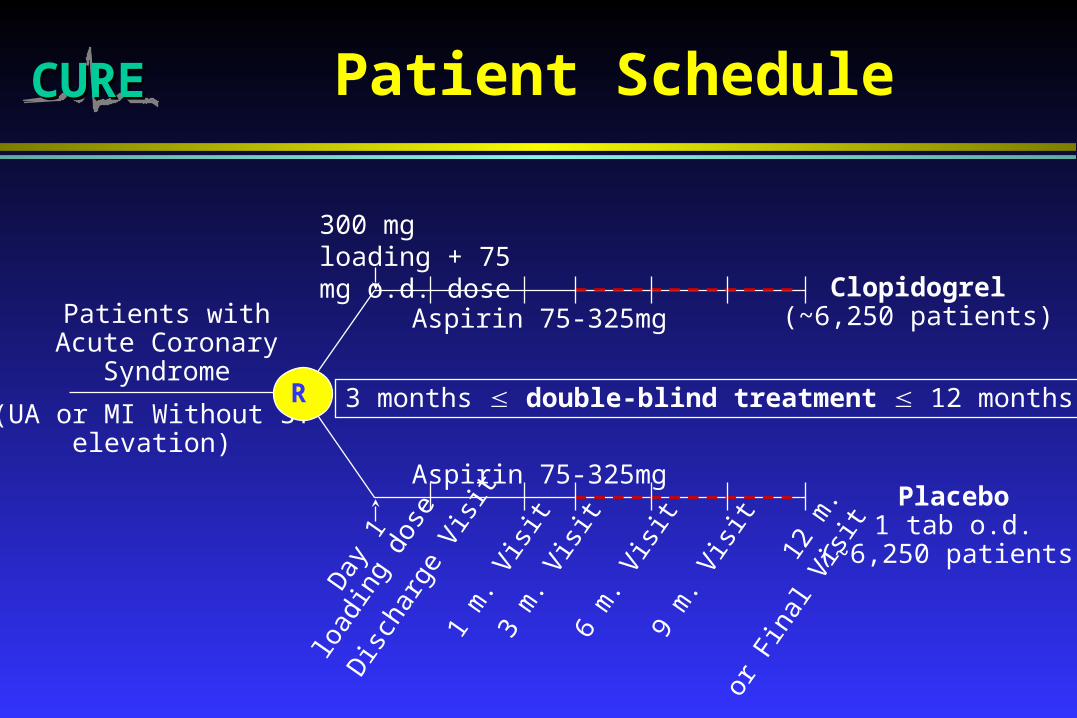
CURECURE Patient Schedule
3 months double-blind treatment 12 months
Aspirin 75-325mg
Clopidogrel(~6,250 patients)
Placebo1 tab o.d.
(~6,250 patients)
Aspirin 75-325mgD
ay 1
6 m
. Vis
it9
m. V
isit
12 m
.
or F
inal
Vis
it
3 m
. Vis
it
Dis
char
ge V
isit
1 m
. Vis
it
Patients withAcute Coronary
Syndrome
(UA or MI Without STelevation)
R
load
ing
dose
300 mg loading + 75 mg o.d. dose

CURECURESample Size (12,500) and
Power Calculations
Main Endpoints Control Event Rate
80% Power
90% Power
CV Death/MI/Stroke 10% 14.7% 16.9%
=0.045 (two-sided) 12% 13.3% 15.3%
Above + Refractory ischemia
14% 14.6% 16.4%
=0.01 (two-sided) 16% 13.6% 15.3%

2463
1110831
5036
3122
CURE: 12,562 from 482 centres in 28 countries

CURECURE Baseline Characteristics (1)
Placebo Clopidogrel
N=6303
%
N=6259
%
Male 61.7 61.3
Female 38.3 38.7
Unstable Angina 74.9 74.9
MI w/o ST Elevation 25.1 25.1
Abnormal ECG 93.9 93.7
Elevated enzymes/marker 25.3 25.3

CURECURE Baseline Characteristics (2)
Placebo Clopidogrel
N=6303
Mean (SD)
N=6259
Mean (SD)
Age 64.2 (11.3) 64.2 (11.3)
Heart rate 73.0 (14.6) 73.2 (14.8)
Systolic BP 134.1 (22.0) 134.4 (22.5)
Symptom onset to randomization (hrs) 14.1 (7.1) 14.2 (7.2)

CURECUREMedications After Randomization
in Hospital
Placebo Clopidogrel
% %
IV Heparin 46.9 46.0
LMW Heparin 56.0 56.1
Beta-blocker 78.4 78.7
Any CCB 36.0 36.0
ACE-I 49.9 50.9
Lipid-lowering 47.0 46.3

CURECURETemporary Interruptions by
Procedure
Any Procedure
(PTCA + CABG + Other Surgery)Plac Clop
With procedure
No. pts 2430 2359
% interruptions (84%) (84%)
Without procedure
No. pts 3873 3900
% interruptions (21%) (23%)

CURECURE ASA at Each Visit
Placebo
N = 6303
Clopidogrel
N = 6259
% on ASA Median Dose % on ASA Median Dose
Pre-Rand 65.6 150 66.6 150
Since-Rand 99.8 150 99.8 150
1-Month 94.1 150 94.0 150
3-Month 96.2 150 96.0 150
6-Month 95.8 125 95.4 125
9-Month 94.7 100 94.6 100

CURECURE Outcomes 1 /2
Plac Clop
% % RR CI p
# Patients 6303 6259
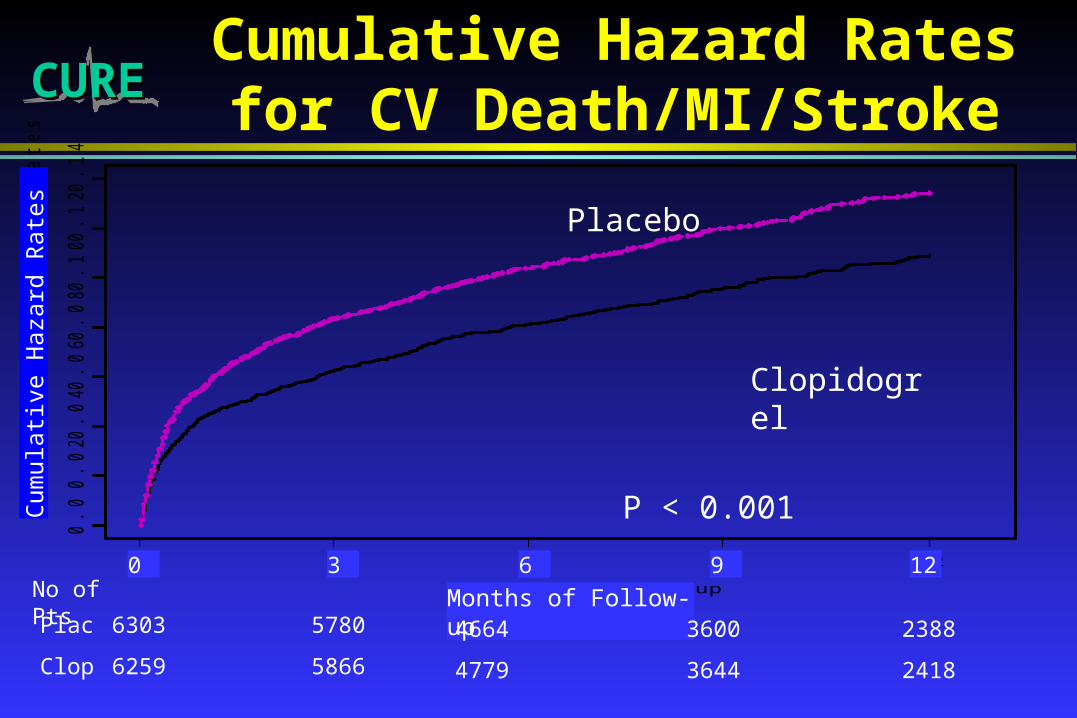
1st Co-Primary 11.41 9.30 0.80 0.72-0.90 < 0.001
•CV Death 5.47 5.08 0.93 0.79-1.08
•MI 6.65 5.18 0.77 0.67-0.89
•Stroke 1.38 1.20 0.86 0.63-1.18
Non CV death 0.71 0.66 0.91 0.60-1.39
CURECURE
Months of Follow-up
Cu
mu
lative
Ha
za
rd R
ate
s
0.0
0.0
20
.04
0.0
60
.08
0.1
00
.12
0.1
4
0 3 6 9 12
Cumulative Hazard Rates for CV Death/MI/Stroke
P < 0.001
Clopidogrel
Placebo
Cum
ulat
ive
Haz
ard
Rat
es
Months of Follow-up0 3 6 9 12
6303
6259
5780
5866
4664
4779
3600
3644
2388
2418
Plac
Clop
No of Pts

CURECURE
Days of Follow-up
Cu
mu
lative
Ha
za
rd R
ate
s
0.0
0.0
10
.02
0.0
30
.04
0.0
50
.06
0 10 20 30
Cumulative Hazard Rates for CV Death/MI/Stroke up to 30 Days
P = 0.003
Clopidogrel
Placebo
Cum
ulat
ive
Haz
ard
Rat
es
Days of Follow-up0 10 20 30
6303
6259
6108
6103
5998
6035
5957
5984
No. Plac
No. Clop
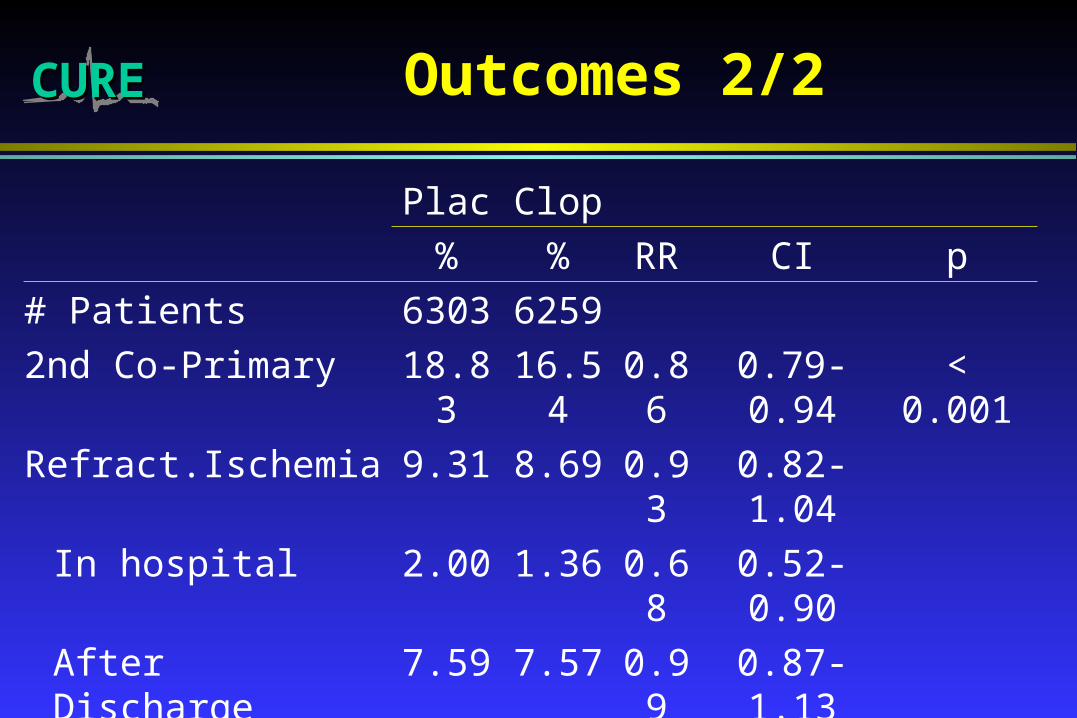
CURECURE Outcomes 2/2
Plac Clop
% % RR CI p
# Patients 6303 6259
2nd Co-Primary 18.83 16.54 0.86 0.79-0.94 < 0.001
Refract.Ischemia 9.31 8.69 0.93 0.82-1.04
In hospital 2.00 1.36 0.68 0.52-0.90
After Discharge 7.59 7.57 0.99 0.87-1.13
Severe Ischemia 5.03 3.80 0.75 0.63-0.89 < 0.001
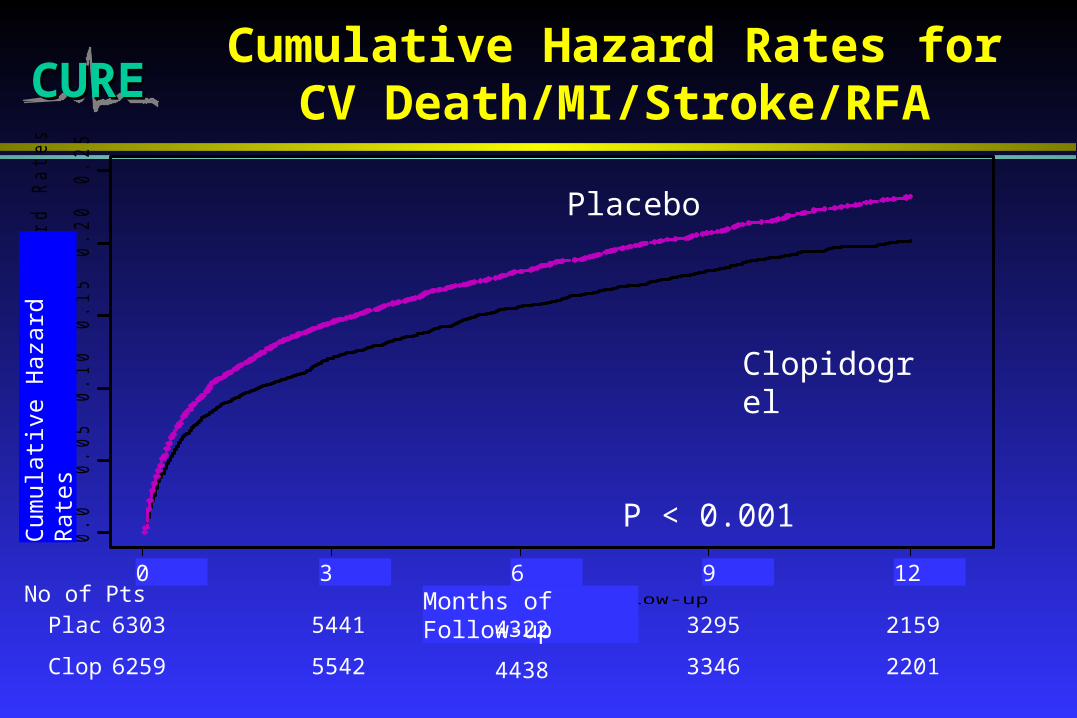
CURECURECumulative Hazard Rates for CV
Death/MI/Stroke/RFA
Months of Follow-up
Cu
mu
lative
Ha
za
rd R
ate
s
0.0
0.0
50
.10
0.1
50
.20
0.2
5
0 3 6 9 12
P < 0.001
Clopidogrel
Placebo
Cum
ulat
ive
Haz
ard
Rat
es
Months of Follow-up0 3 6 9 12
6303
6259
5441
5542
4322
4438
3295
3346
2159
2201
Plac
Clop
No of Pts
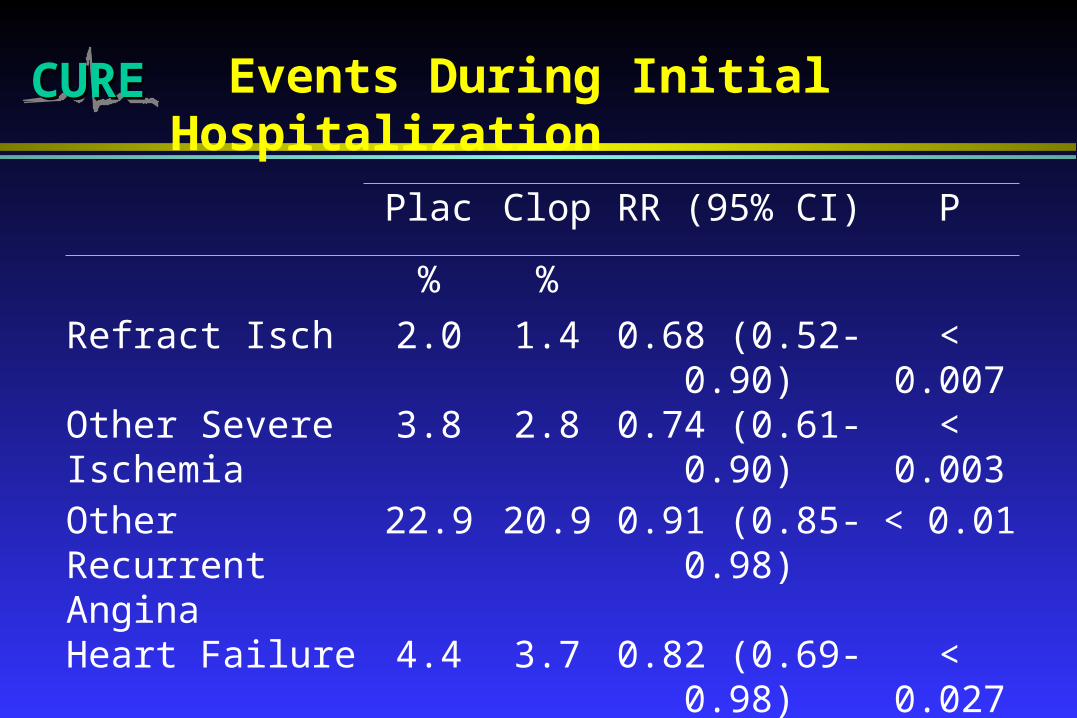
CURECURE Events During Initial Hospitalization
Plac Clop RR (95% CI) P
% %
Refract Isch 2.0 1.4 0.68 (0.52-0.90) < 0.007
Other Severe Ischemia
3.8 2.8 0.74 (0.61-0.90) < 0.003
Other Recurrent Angina
22.9 20.9 0.91 (0.85-0.98) < 0.01
Heart Failure 4.4 3.7 0.82 (0.69-0.98) < 0.027

CURECURE CV Death/MI/Stroke in Subgroups: (1)
Subgroup
2N Placebo%
Clopidogrel%
RR CI
• Major ST Dev 6275 14.3 11.5 0.79 0.69-0.91
Others 6287 8.6 7.0 0.81 0.68-0.97
• With Enzyme
Elevation 3176 13.0 10.7 0.81 0.66-0.99
Without Enzyme
Elevation 9386 10.9 8.8 0.80 0.70-0.91
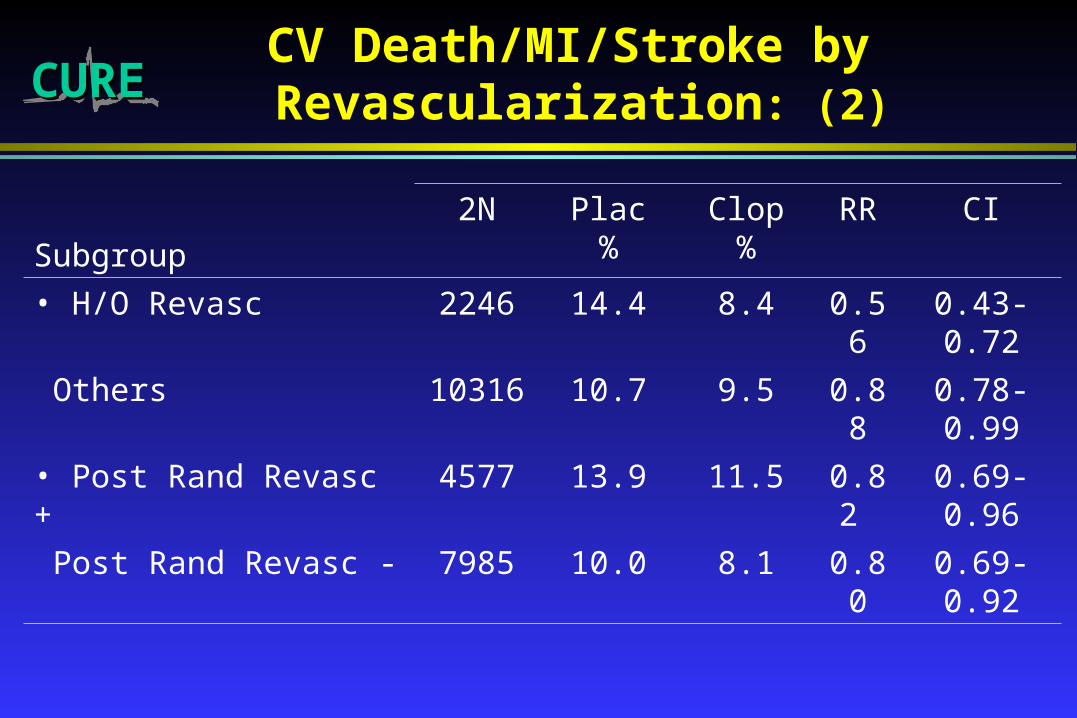
CURECURECV Death/MI/Stroke by Revascularization: (2)
Subgroup
2N Plac%
Clop%
RR CI
• H/O Revasc 2246 14.4 8.4 0.56 0.43-0.72
Others 10316 10.7 9.5 0.88 0.78-0.99
• Post Rand Revasc + 4577 13.9 11.5 0.82 0.69-0.96
Post Rand Revasc - 7985 10.0 8.1 0.80 0.69-0.92
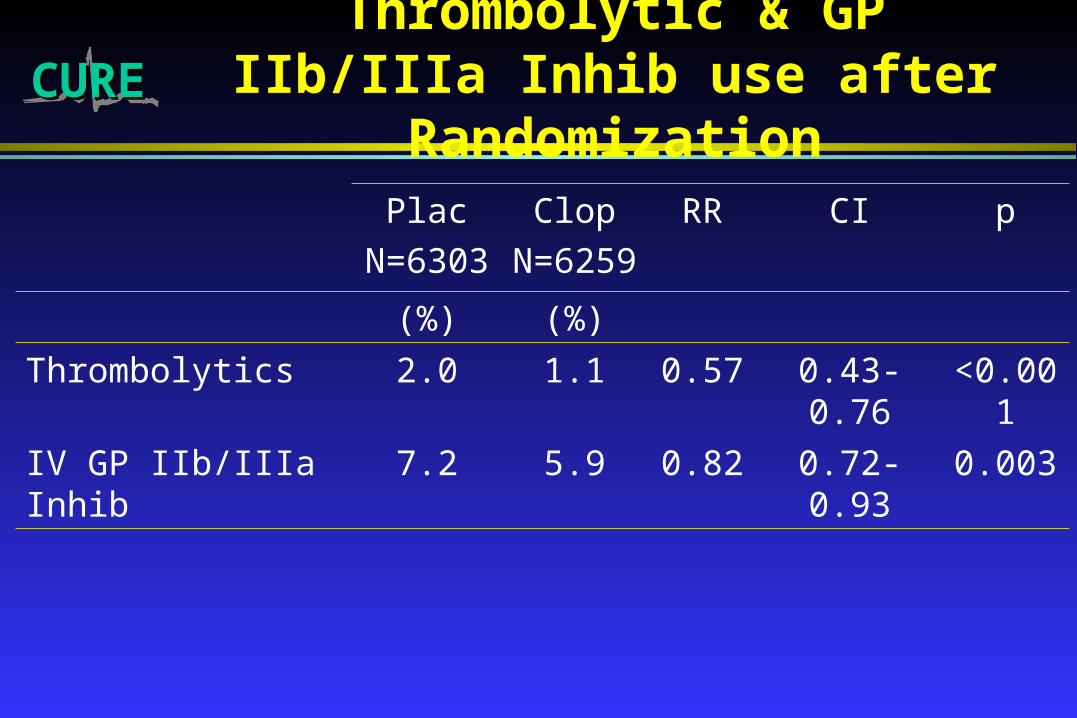
CURECUREThrombolytic & GP IIb/IIIa Inhib
use after Randomization
Plac
N=6303
Clop
N=6259
RR CI p
(%) (%)
Thrombolytics 2.0 1.1 0.57 0.43-0.76 <0.001
IV GP IIb/IIIa Inhib 7.2 5.9 0.82 0.72-0.93 0.003
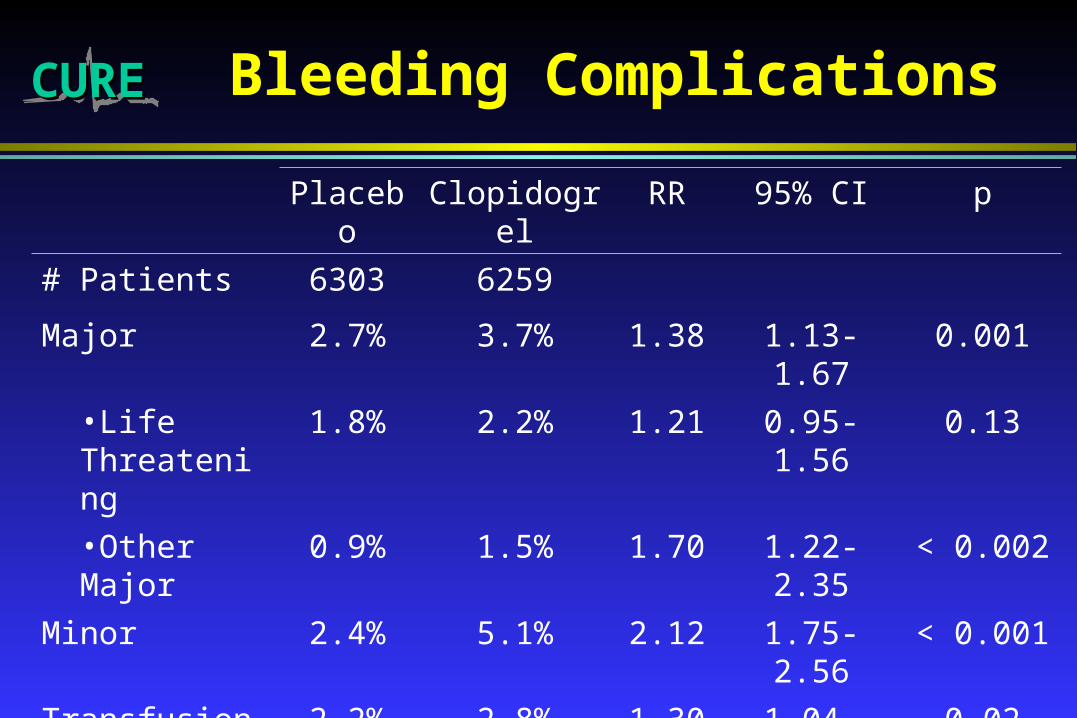
CURECURE Bleeding Complications
Placebo Clopidogrel RR 95% CI p
# Patients 6303 6259
Major 2.7% 3.7% 1.38 1.13-1.67 0.001
•Life Threatening
1.8% 2.2% 1.21 0.95-1.56 0.13
•Other Major 0.9% 1.5% 1.70 1.22-2.35 < 0.002
Minor 2.4% 5.1% 2.12 1.75-2.56 < 0.001
Transfusion (2+Units)
2.2% 2.8% 1.30 1.04-1.62 0.02
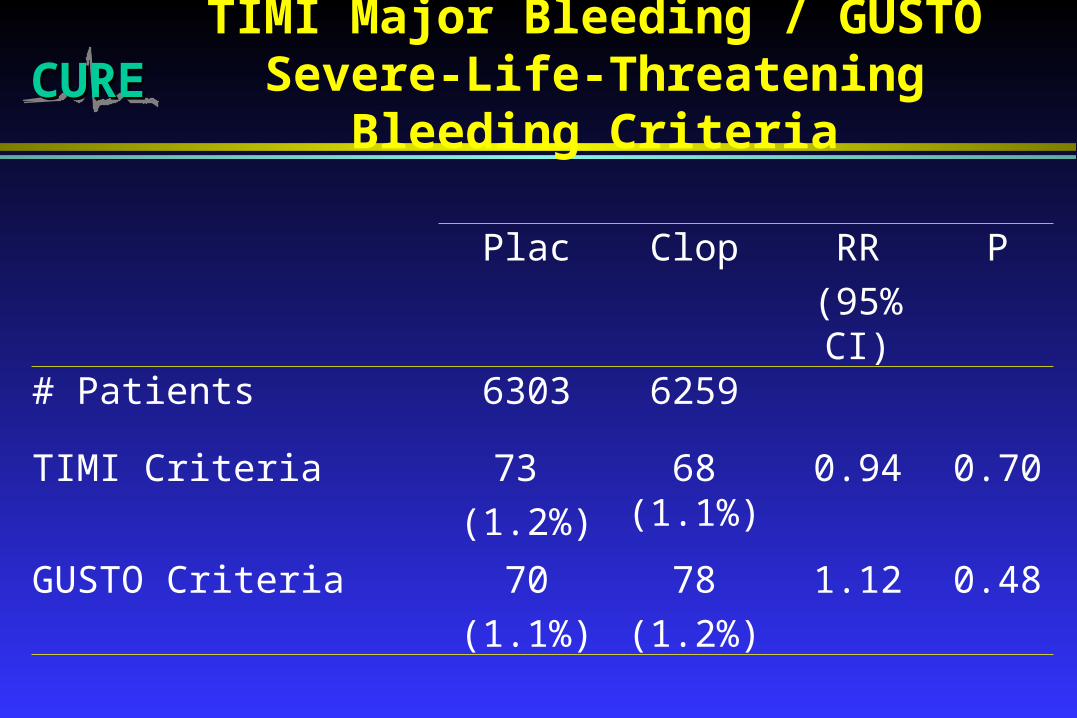
CURECURETIMI Major Bleeding / GUSTO Severe-
Life-Threatening Bleeding Criteria
Plac Clop RR
(95% CI)
P
# Patients 6303 6259
TIMI Criteria 73
(1.2%)
68 (1.1%)
0.94 0.70
GUSTO Criteria 70
(1.1%)
78
(1.2%)
1.12 0.48

CURECUREMajor/Life-Threatening Bleeds within 7
Days of CABG Surgery
Plac Clop RR p
Stopped < 5 days prior to CABG
N = 476 N = 436
Pts with Maj/LT Bleeds 6.3% 9.6% 1.53 0.06
Stopped > 5 days prior to CABG
N = 454 N = 456
Pts with Maj/LT Bleeds 5.3% 4.4% 0.83 0.53

CURECUREThrombocytopenia and
Neutropenia
Plac Clop
# Rand 6303 6259
Thrombocytopenia 28 (0.44%) 26 (0.42%)
Neutropenia 5 (0.1%) 8 (0.13%)
CURECURE Conclusions
Clopidogrel significantly reduces the risk of:
a) CV Death, MI, Stroke by about one-fifth (p < 0.001)
b) CV Death, MI, Stroke, and Refractory Ischemia by about one-sixth (p < 0.001)
c) Early revascularization, severe and recurrent ischemia and heart failure by about one-fifth to one-quarter in hospital
There is a small (absolute 1%) significant excess of major, but not life threatening, bleeds
CURECURE Clinical Implications
Clopidogrel is beneficial both early and long term in patients with ACS, with a small excess in bleeds. The benefits are consistently observed in various subgroups examined and in addition to other established therapies.
Treating 1000 patients for 9 months prevents about 27 major events in 23 patients at a cost of 4 life threatening bleeds (+ 2 other transfusions).
CURECURE Public Health Implications
USA: 1.5 million MI per year 0.5 mill non-fatal non-Q MI
1.5 million UA pts per year
Potential eligible for clopidogrel is about 2 millionMajor vascular events (CV death/MI/Stroke) reduced from about
250,000 to 200,000 (i.e. 12.5% to 10%) at one year.
If patients are treated longer (e.g. 3 yrs)500,000 reduced to 400,000 (i.e. 25% to 20%)
Therefore 50,000 to 100,000 individuals will avoid a major vascular eventin the USA per year
Global impact: if one-fifth of eligible pts receive clopidogrel, 250,000–500,000 individuals could benefit