curitiba trial custodiol vs ringer - società italiana di ... · curitiba trial custodiol vs ringer...
TRANSCRIPT

CURITIBA TRIAL Custodiol VS Ringer
Qual è il miglior substrato per la protezione renale durante la chirurgia aperta per aneurisma
dell’aorta toracoaddominale?
Yamume TshombaUniversità Vita-Salute at Scientific Institute San Raffaele in Milano, Italy
Head of Department Professor Roberto Chiesa
Bologna, 24 Ottobre 2017

Disclosures
Yamume Tshomba
I have the following potential conflicts of interest to report:
Institutional research grant from Dr. Frantz Köhler Chemie GmbH (Bensheim - DE)Travel support from Dr. Frantz Köhler Chemie GmbH (Bensheim - DE)
NOReceipt of honorariaParticipation in a company sponsored speakers' bureauEmployment in industryShareholder in a healthcare companyOwner of a healthcare company
Disclosures
Yamume Tshomba
I have the following potential conflicts of interest to report:
Off-label discussion of the use of Custodiol for “in-vivo” renal perfusion

Background: Open Repair

TAAA Open Repair
Focusing On Renal Function

Acute Tubular NecrosisSuprarenal Clamping: increase of baseline Scr x 1.5 >70%
What Cells Are involved?

PROXIMAL TUBULE
67%
HENLE LOOP20%
COLLECTING DUCT3%
DISTAL TUBULE7%
Proximal Tubule: ↑ Na+ Reabsorption
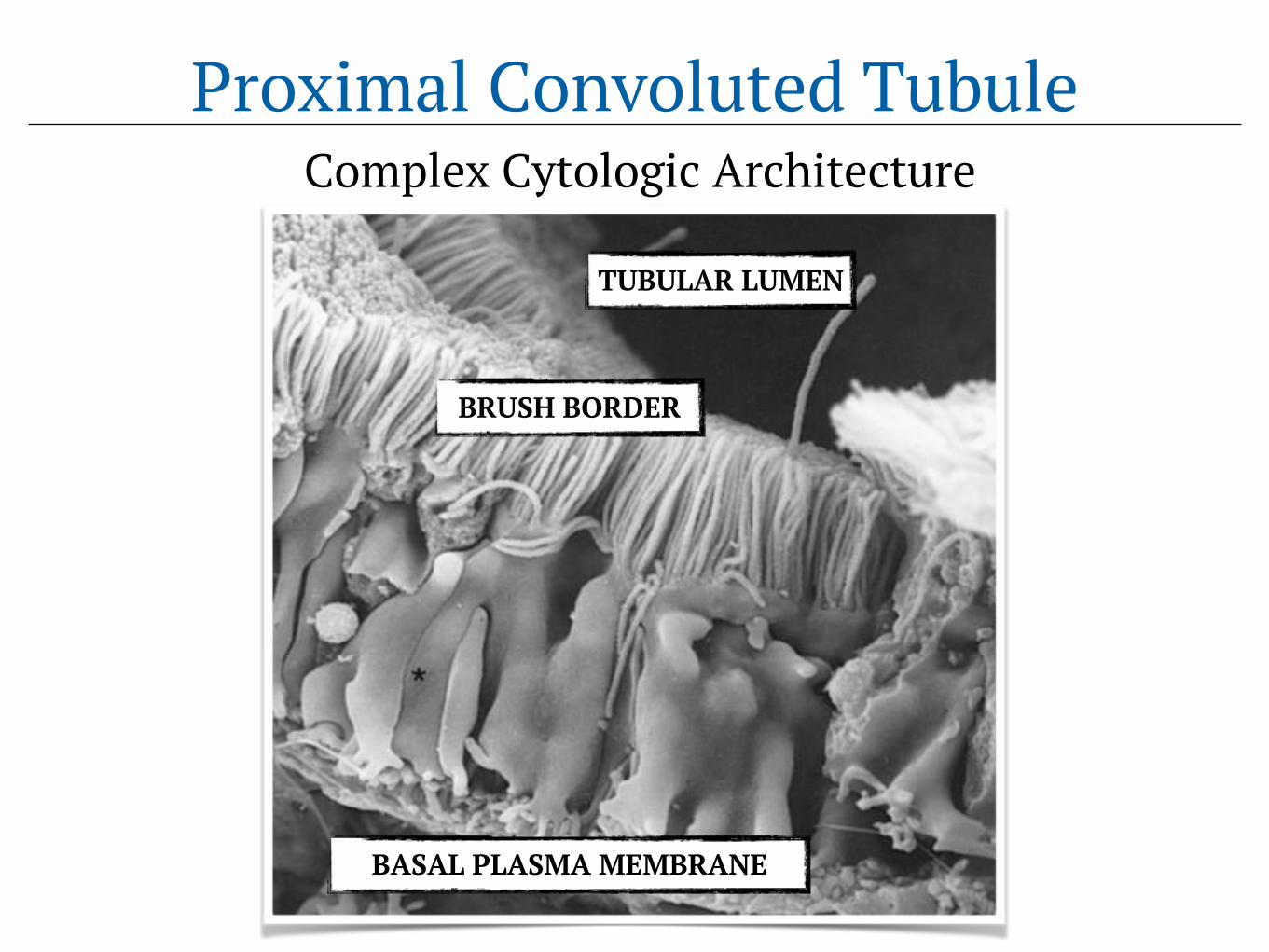
Proximal Convoluted TubuleComplex Cytologic Architecture
TUBULAR LUMEN
BRUSH BORDER
BASAL PLASMA MEMBRANE

TUBULAR LUMEN
BRUSH BORDER
PERITUBULAR CAPILLARY
High Oxidative Metabolic ActivityProximal Convoluted Tubule

How Can We Protect Kidney in OR?

Crucial Step: Cold Crystalloid Perfusion
H. J. Bretschneider (1922-1993)S. Ringer (1835-1910)
OSR Crystalloyd PerfusionRINGER… until 2009 CUSTODIOL… since 2009
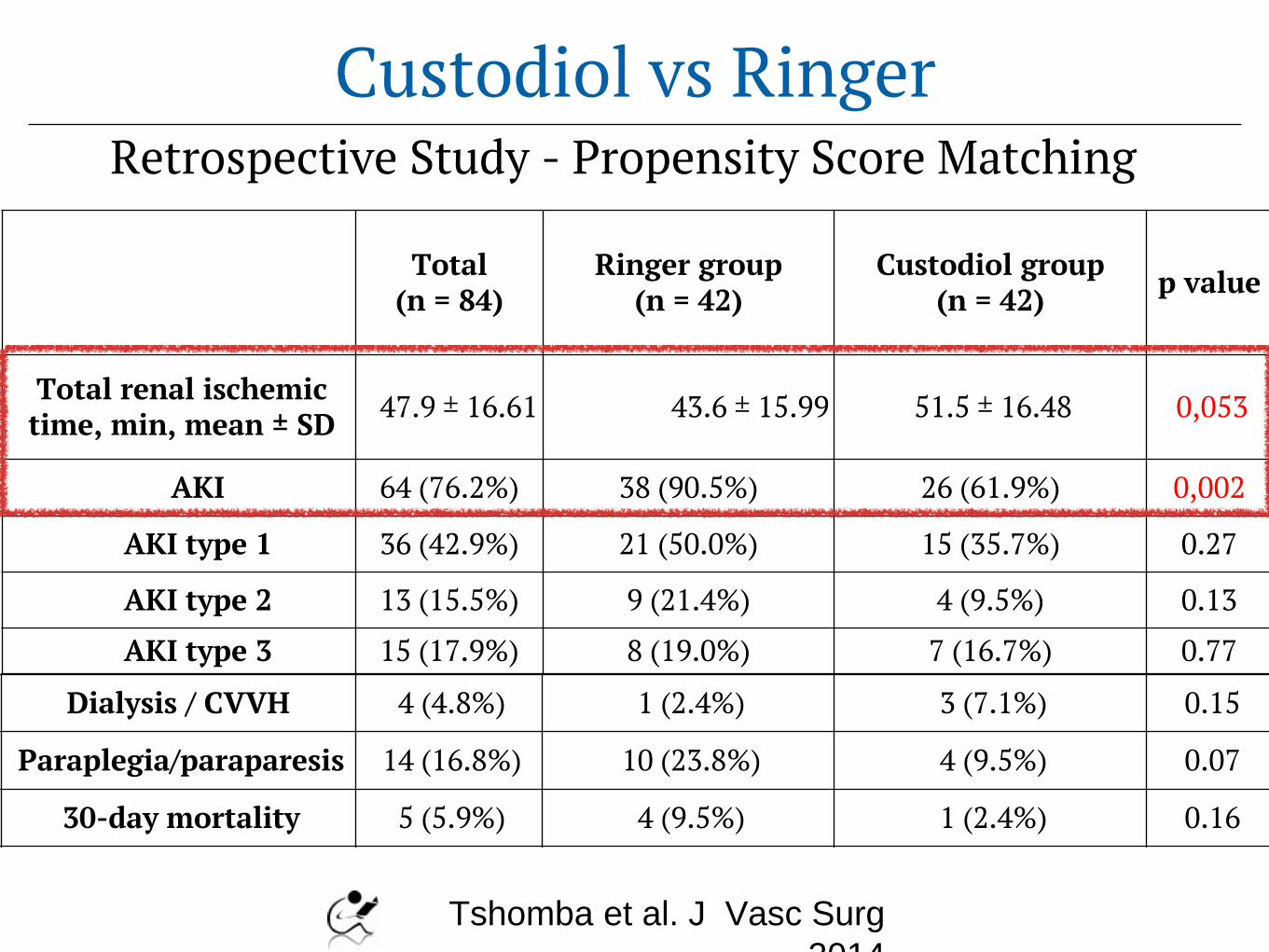
Total (n = 84)
Ringer group (n = 42)
Custodiol group (n = 42) p value
Total renal ischemic time, min, mean ± SD 47.9 ± 16.61 43.6 ± 15.99 51.5 ± 16.48 0,053
AKI 64 (76.2%) 38 (90.5%) 26 (61.9%) 0,002
AKI type 1 36 (42.9%) 21 (50.0%) 15 (35.7%) 0.27
AKI type 2 13 (15.5%) 9 (21.4%) 4 (9.5%) 0.13
AKI type 3 15 (17.9%) 8 (19.0%) 7 (16.7%) 0.77
Dialysis / CVVH 4 (4.8%) 1 (2.4%) 3 (7.1%) 0.15
Paraplegia/paraparesis 14 (16.8%) 10 (23.8%) 4 (9.5%) 0.07
30-day mortality 5 (5.9%) 4 (9.5%) 1 (2.4%) 0.16
Tshomba et al. J Vasc Surg
2014
Retrospective Study - Propensity Score MatchingCustodiol vs Ringer

Study Drawbacks
• Retrospective in nature • Temporal bias / Learning curve• Biomarkers of subclinical renal injuries?

ClinicalTrials.gov Identifier: NCT 02327611
CURITIBA TRIAL
Prospective, Randomized & Double-blinded Non-Inferiority Trial (Off-label Use)

CURITIBA TRIAL
CUstodiol versus RInger:whaT Is the Best Agent?

CURITIBA TRIAL
- Spontaneous Study- Independent Design Process- PI’s Data Property- External Provider
- Randomization- Data collection and cleaning- Statistical analysis
- Obtained funding: YT
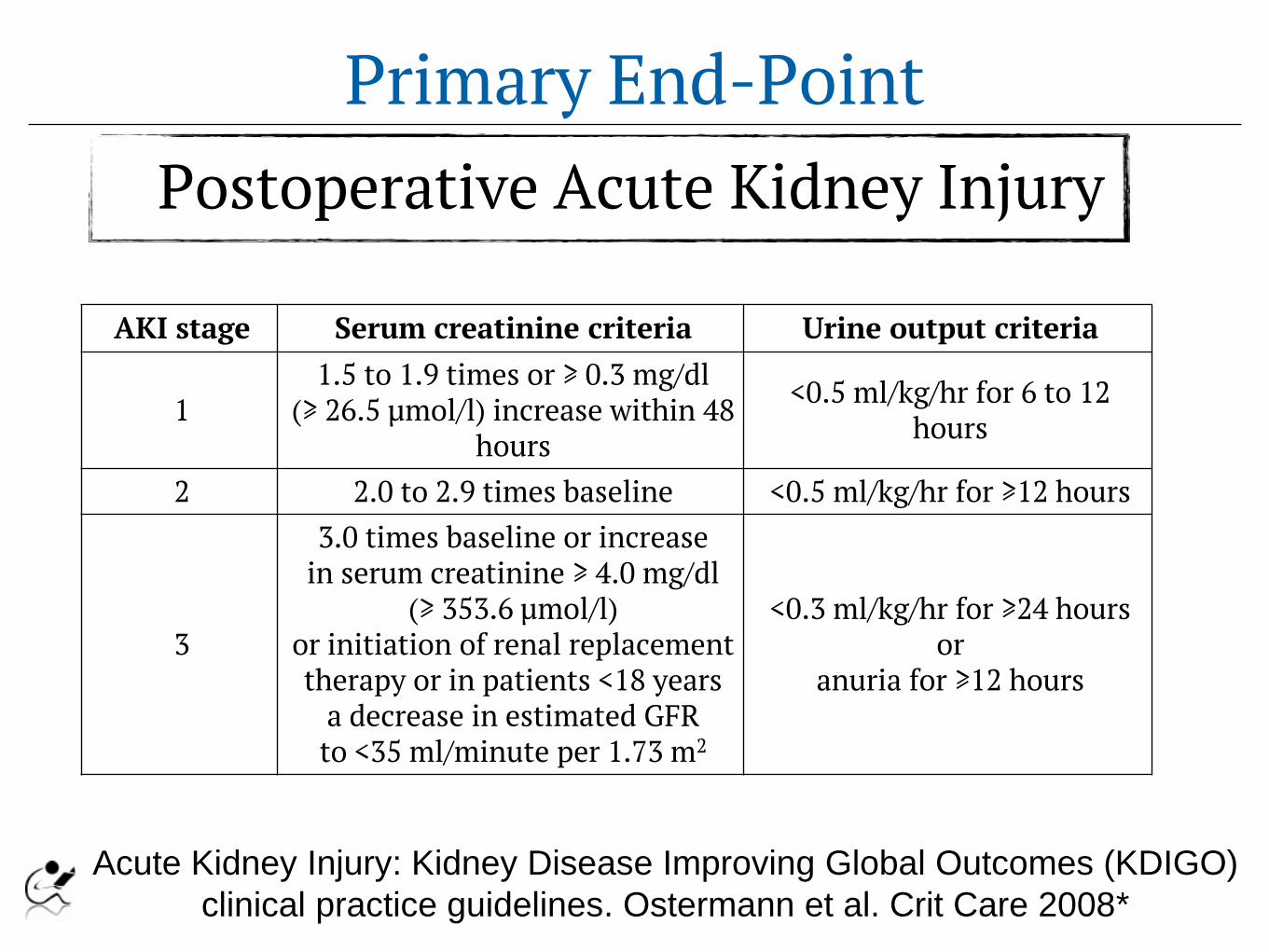
Primary End-PointPostoperative Acute Kidney Injury
Acute Kidney Injury: Kidney Disease Improving Global Outcomes (KDIGO)
clinical practice guidelines. Ostermann et al. Crit Care 2008*
AKI stage Serum creatinine criteria Urine output criteria
11.5 to 1.9 times or ≥ 0.3 mg/dl
(≥ 26.5 µmol/l) increase within 48 hours
<0.5 ml/kg/hr for 6 to 12 hours
2 2.0 to 2.9 times baseline <0.5 ml/kg/hr for ≥12 hours
3
3.0 times baseline or increase in serum creatinine ≥ 4.0 mg/dl
(≥ 353.6 µmol/l) or initiation of renal replacement therapy or in patients <18 years
a decrease in estimated GFR to <35 ml/minute per 1.73 m2
<0.3 ml/kg/hr for ≥24 hours or
anuria for ≥12 hours
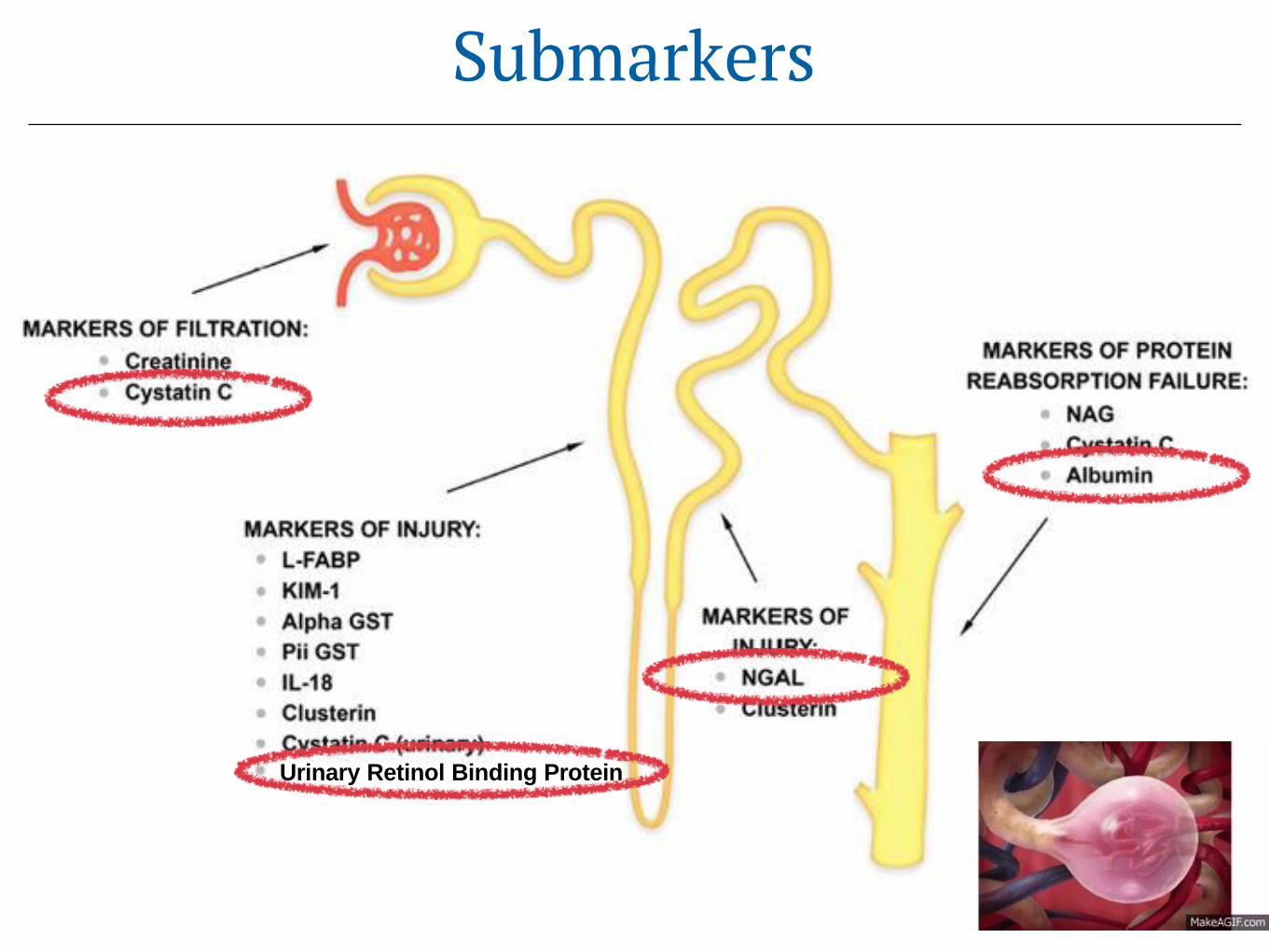
Submarkers
Urinary Retinol Binding Protein

Flow Of Study Patients

Excluded in OR (n=1)- Change in extent (n=1)
Did not receive allocated perfusion for distal suprarenal clamping
Assessed for eligibility (n=113)
Enrolled (n=96)
Randomized (n=90)
Allocated to Custodiol renal perfusion (n=45) Allocated to Ringer renal perfusion (n=45)
Received allocated perfusion (n=44) Received allocated perfusion (n=44)
Excluded (n=6)- Medical decision (n=5)- Consent withdrawn (n=1)
Excluded in OR (n=1)- Change in extent (n=1)
Did not receive allocated perfusion for distal suprarenal clamping
- Lost to follow up (n=2)[Intraoperative death]
Analysed (n=42) Analysed (n=44)
Randomized (ITT population)
Prescreening
Screening
Efficacy Analysis(PP population)
Allocation
Follow up
Excluded (n=17)- Refused to partecipate (n=12)- Not meeting inclusion criteria (n=5)
- Emergency procedures (n=4) - Age > 18 yrs (n=1)
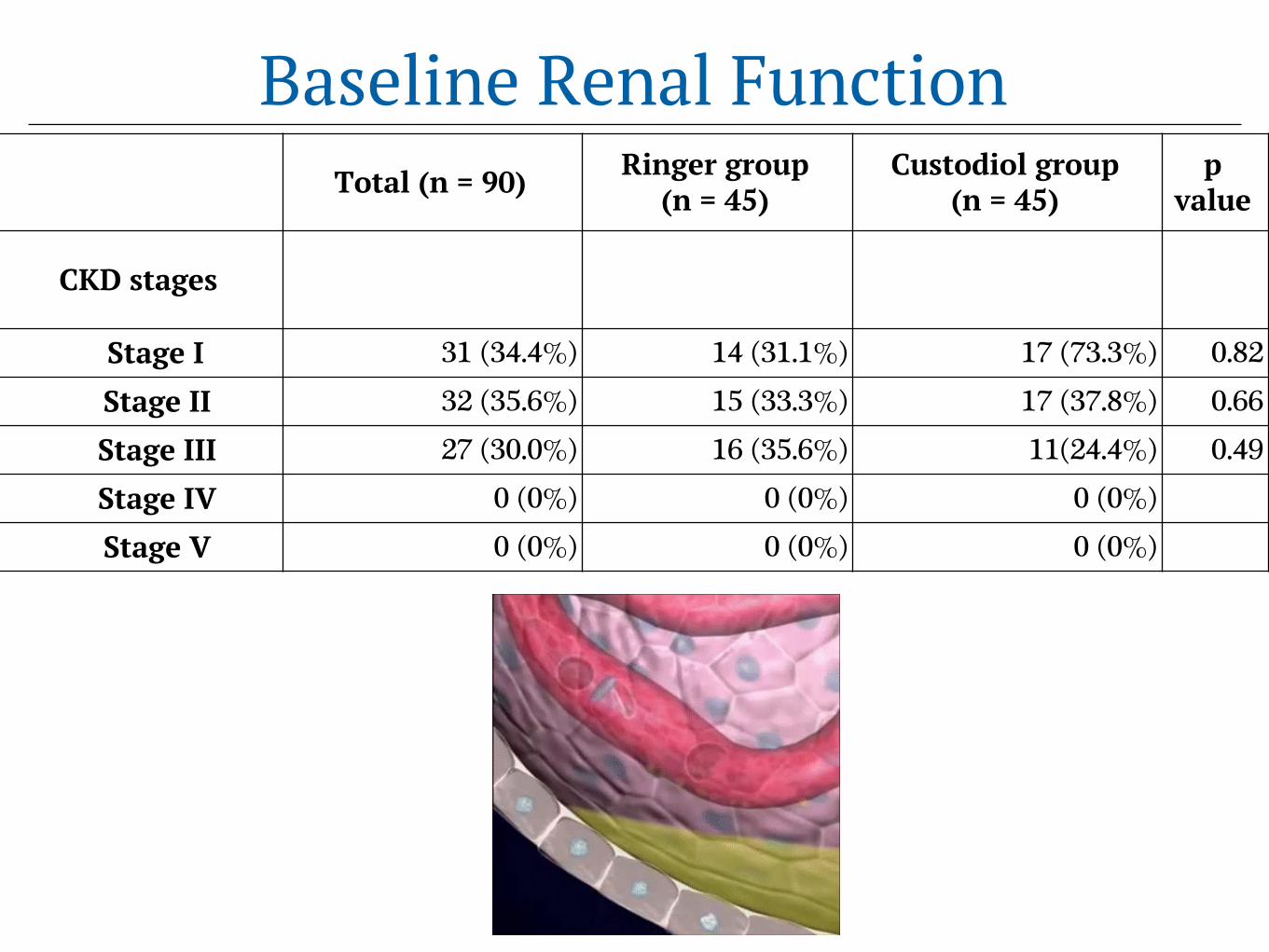
Baseline Renal FunctionTotal (n = 90) Ringer group
(n = 45)Custodiol group
(n = 45)p
value
CKD stages
Stage I 31 (34.4%) 14 (31.1%) 17 (73.3%) 0.82
Stage II 32 (35.6%) 15 (33.3%) 17 (37.8%) 0.66
Stage III 27 (30.0%) 16 (35.6%) 11(24.4%) 0.49
Stage IV 0 (0%) 0 (0%) 0 (0%)
Stage V 0 (0%) 0 (0%) 0 (0%)

Intraoperative DetailsTotal
(n = 90)Ringer group
(n = 45)Custodiol group
(n = 45) p value
Overall Operative Time, min, mean ± SD 288.3 ± 66.3 265.6 ± 68.1 298.6 ± 72.7 0.21
Overall Clamping Time, min, mean ± SD 49.0 ± 19.2 50.3 ± 19.1 48.5 ± 20.2 0.15
Visceral Selective Perfusion Time, min, mean ± SD 26.6 ± 10.42 25.7 ± 17.01 27.9 ± 7.6 0.12
Total renal ischemic time, min, mean ± SD 49.7 ± 12.8 46.6 ± 16.7 51.7 ± 19.8 0.08
Isothermic renal distal perfusional time, min 22.2 ± 11.1 24.4 ± 10.2 20.9 ± 14.4 0.07
Cold renal perfusional time, min 23.1 ± 12.4 24.7 ± 13.3 22.5 ± 8.2 0.31
Total renal perfusional volume, ml, mean ± SD 401.4±77.3 388.7±77.3 413.9±77.1 0.57
Urine output during operation, ml, mean ± SD 3834.7 ± 2245.3 3873.6 ± 2245.3 3791.1± 2220.0 0.62

Results

Total (n = 90)
Ringer group (n = 45)
Custodiol group (n = 45) p value
Peak serum creatinine, mg/dL, mean ± SD 1.9 ± 1.1 1.9 ± 1.0 1.9 ± 1.2 0,21
Minimum peak of eGFR, mean ± SD 46.4 ± 25.0 46.5 ± 24.3 46.0 ± 26.2 0,18
AKI 56 (62.2%) 34 (75.6%) 22 (48.9%) 0,008
AKI type 1 29 (32.2%) 18 (40.0%) 11 (24.4%) 0,08
AKI type 2 13 (14.4%) 6 (13.3%) 7 (15.5%) 0,38
AKI type 3 14 (15.5%) 10 (22.2%) 4 (8.8%) 0,07
Dialysis / CVVH 7 (7.7%) 6 (13.3%) 1 (2.2%) 0,06Paraplegia/Paraparesis 6 (6.6%) 4 (8.8%) 2 (4.4%) 0,24
30-day mortality 7 (7.8%) 5 (11.1%) 2 (4.4%) 0,16
Short-Term OutcomesIntention To Treat Analysis

Submarkers
POSTOPERATIVE VALUES
CUSTODIOL GROUP
RINGER GROUP P
U-Albumin (mg/L) Range 0-15
12.6 (6.5-50.1)
14.9 (4.5-43.4) 0.94
U-RBP (mg/L) Range 20-50
5720 (228-13700)
2510 (321-15000) 0.86
U-NGAL (𝜇g/L) Range < 133
33.5 (11-94.2)
26 (9-82) 0.54
S-Cystatin C (mg/L)Range 0.53-0.95
1.305 (1.1-1.64)
1.42 (1.1-1.63) 0.64
Blood / Urine Collection (PO d 3-6)

Excluded in OR (n=1)- Change in extent (n=1)
Did not receive allocated perfusion for distal suprarenal clamping
Randomized (n=90)
Allocated to Custodiol renal perfusion (n=45) Allocated to Ringer renal perfusion (n=45)
Received allocated perfusion (n=44) Received allocated perfusion (n=44)
Excluded in OR (n=1)- Change in extent (n=1)
Did not receive allocated perfusion for distal suprarenal clamping
Randomized (ITT population)
Allocation
Per Protocol Analysis
Chi-square without Yates correction: P= .0128
Extent AKI NO AKI Total
Custodiol 23 (52.3%) 21 (47.7%) 44
Ringer 34 (77.3%) 10 (22.7%) 44
Total 57 (64.7%) 31 (35.2%) 88
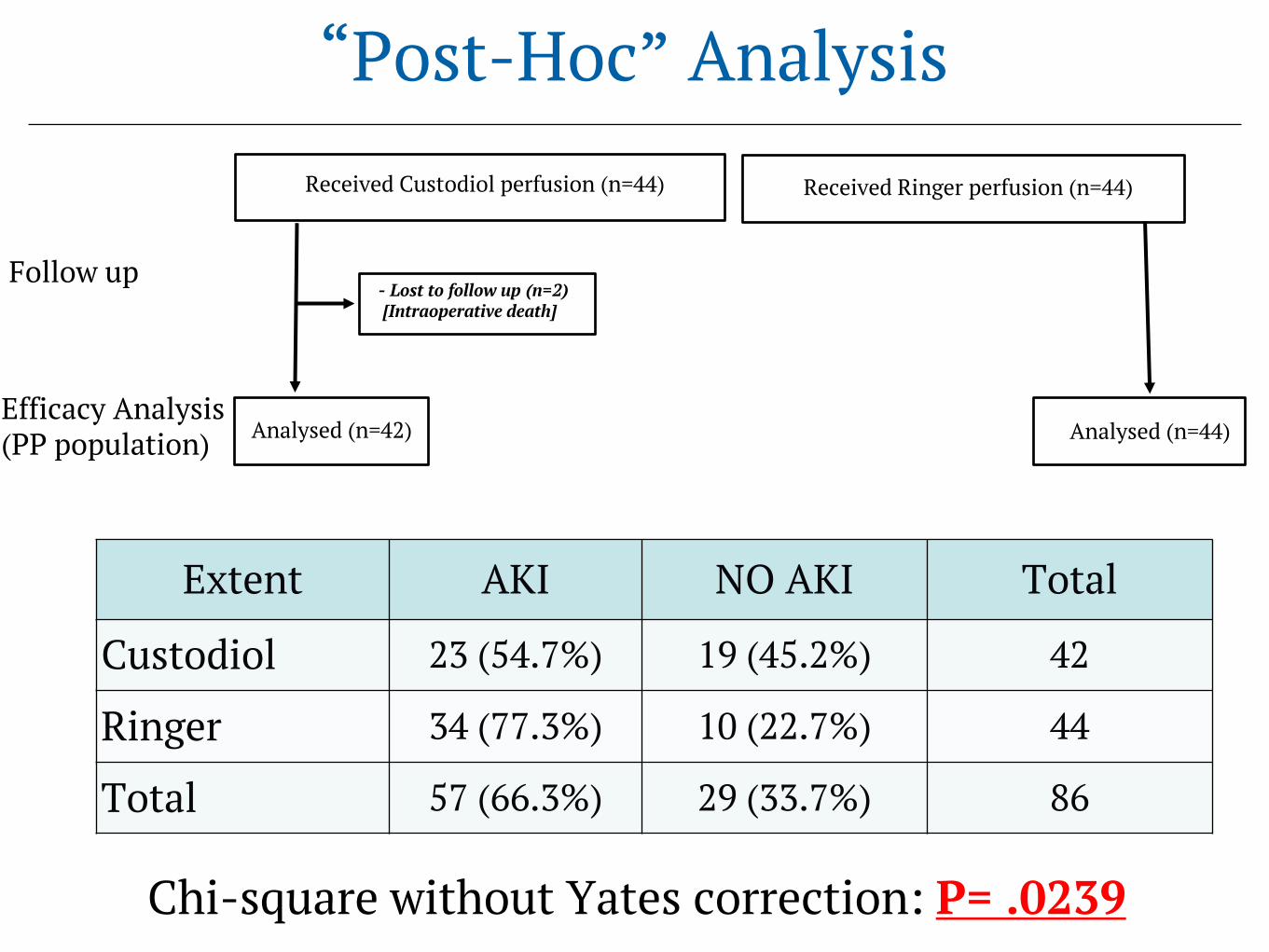
Received Custodiol perfusion (n=44) Received Ringer perfusion (n=44)
- Lost to follow up (n=2)[Intraoperative death]
Analysed (n=42) Analysed (n=44)Efficacy Analysis(PP population)
Follow up
“Post-Hoc” Analysis
Chi-square without Yates correction: P= .0239
Extent AKI NO AKI Total
Custodiol 23 (54.7%) 19 (45.2%) 42
Ringer 34 (77.3%) 10 (22.7%) 44
Total 57 (66.3%) 29 (33.7%) 86
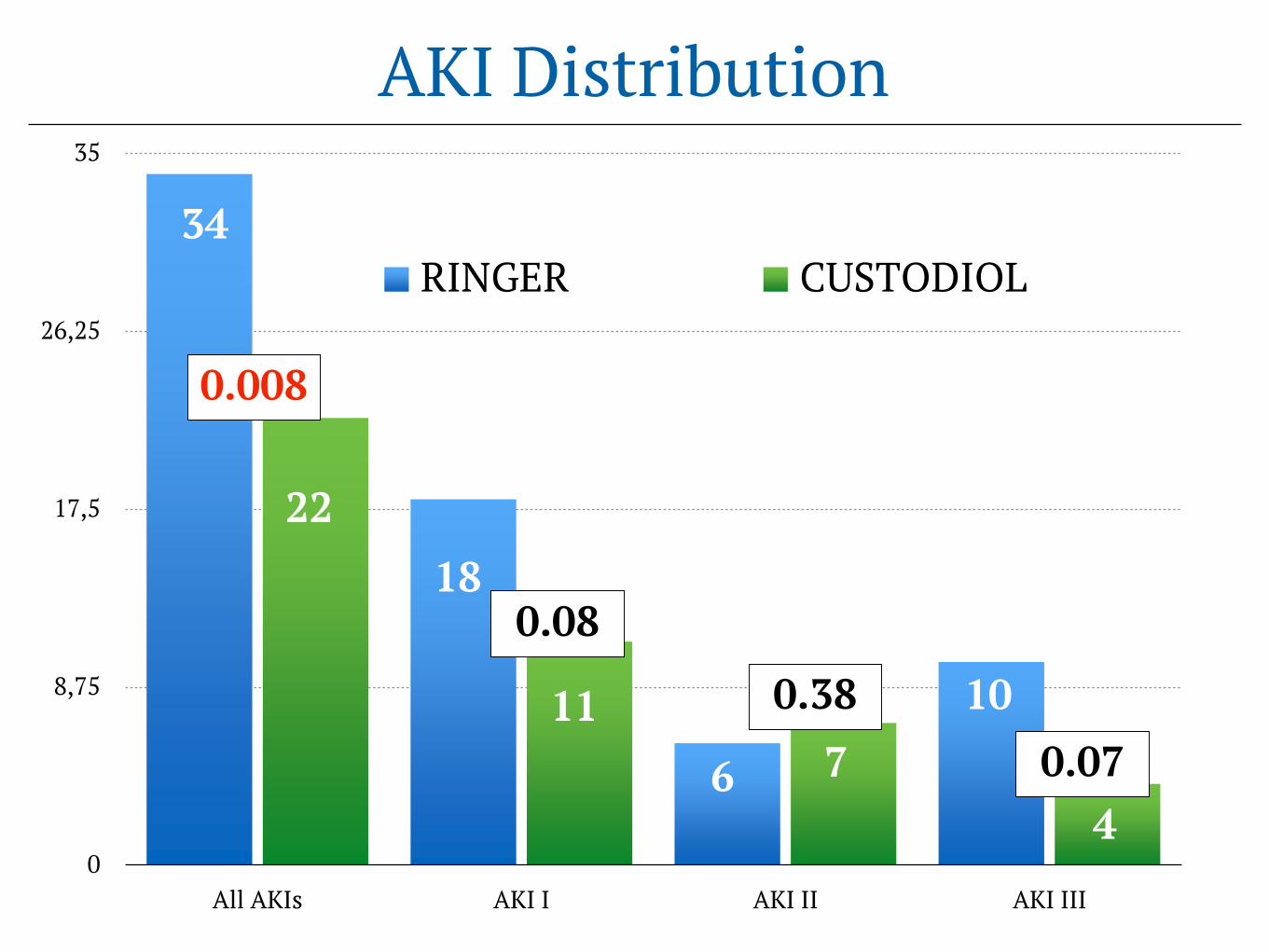
0
8,75
17,5
26,25
35
All AKIs AKI I AKI II AKI III
RINGER CUSTODIOL
AKI Distribution
0.008
0.08
0.380.076
2218
11
34
710
4

Multivariate AnalysisMultivariate cut-off 0.05
(Significant variables at Univariate: ASA 2 & Custodiol)
OR IC 95% P value
Renal perfusion with Custodiol solution 4.12 1.90-8.93 0,0001
Multivariate cut-off 0.1: (Significant variables at Univariate: Hb, HCT, ASA 2 & Custodiol)
OR IC 95% P value
Renal perfusion with Custodiol solution 4.12 1.90-8.93 0,0001
Multivariate cut-off 0.2 (Significant variables at Univariate: CABG, Aortic Surgery, Prostatic K, Hb, HCT, ASA 2 & Custodiol)
OR IC 95% P value
Renal perfusion with Custodiol solution 3.6 1.66-7.92 0,001
Renal Custodiol Perfusion In TAAA
- Safe, simple use, effective in renal cooling
- Not increased submarkers of filtration impairment
- Not increased submarkers of tubular injury
- Significantly reduced AKI compared to Ringer
READY FOR ON LABEL USE?


Enrolled (n=96)
Randomized (n=90)
Allocated to Custodiol renal perfusion (n=45) Allocated to Ringer renal perfusion (n=45)
Excluded (n=6)- Medical decision (n=5)- Consent withdrawn (n=1)
Randomized (ITT population)
Allocation
Chi-square without Yates correction: P= .008
Extent AKI NO AKI Total
Custodiol 23 (51%) 22 (49%) 45
Ringer 34 (75.6%) 11 (24.4%) 45
Total 57 (63.3%) 33 (36.7%) 90
Intention To Treat Analysis

LAST 511 TAAA n
1.5 to 1.9 times
baseline
2.0 to 2.9 times
baseline
3.0 times
baselineTot
Type I 103 33 (32%) 18 (17%) 15 (14%) 66 (64%)
Type II 148 56 (38%) 19 (13%) 16 (11%) 91 (61%)
Type III 136 42 (31%) 20 (15%) 22 (16%) 84 (61%)
Type IV 124 65 (52%) 32 (26%) 26 (21%) 123 (99%)
Total 511 196 (38%) 89 (17%) 79 (15%) 364 (71%)
Serum Creatinine Criteria Postoperative ChangesChiesa’s series 1993-2017: 1024 TAAAs