current clinical practice - scbtmr.org · • gland confined vs. extraglandular (t2 vs. t3) ... ca...
TRANSCRIPT
1
Prostate MRProstate MR
Harvard Medical School
BBETH ETH IISRAEL SRAEL DDEACONESSEACONESSMMEDICAL EDICAL CCENTERENTER
Neil M. Rofsky, MD
•• DIGITAL RECTAL EXAMINATIONDIGITAL RECTAL EXAMINATION•• PSA PSA ( ~ 20% False negative)( ~ 20% False negative)
•• BIOPSY BIOPSY (18(18--25% False negative)25% False negative)•• Each specimen = 1/10,000 of the gland volumeEach specimen = 1/10,000 of the gland volume•• Gleason grading (tumor Gleason grading (tumor ‘‘severityseverity’’) ) ––
•• has variabilityhas variability•• 2 largest areas of cancer tissue2 largest areas of cancer tissue
Current Clinical PracticeCurrent Clinical Practice
Imaging to AddressImaging to AddressClinical ChallengesClinical Challenges
•• Need reliable staging Need reliable staging →→ Treatment OptionsTreatment Options•• Gland confined vs. Gland confined vs. extraglandularextraglandular (T2 vs. T3)(T2 vs. T3)
•• Rising PSA Rising PSA •• Repeat Negative Repeat Negative BiospyBiospy•• S/P S/P TxTx
•• Most men will have it, relatively few will die from itMost men will have it, relatively few will die from it•• How can we identify the How can we identify the ““bad actorsbad actors””??•• How do we monitor watchful waiting/active surveillance?How do we monitor watchful waiting/active surveillance?
MR Imaging EvaluationsMR Imaging Evaluations•• T2WIT2WI
•• Straight forwardStraight forward•• False +False +‘‘s s
•• DCEDCE•• ↑↑‘‘ss detectiondetection•• Requires softwareRequires software
•• DiffusionDiffusion•• Improve detection and specificityImprove detection and specificity
•• MR SpectroscopyMR Spectroscopy•• Difficult to perform Difficult to perform
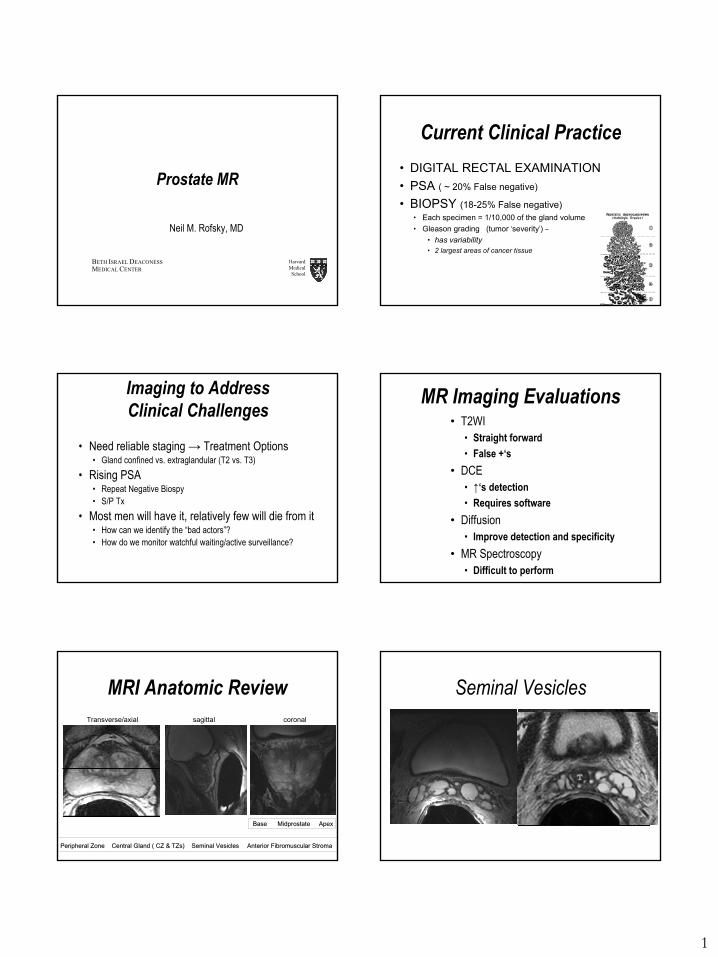
Peripheral Zone Peripheral Zone Central Gland ( CZ & TZs) Central Gland ( CZ & TZs) Seminal Vesicles Seminal Vesicles Anterior Anterior FibromuscularFibromuscular StromaStroma
BaseBase MidprostateMidprostate ApexApex
Transverse/axial sagittal coronal
MRI Anatomic ReviewMRI Anatomic Review Seminal VesiclesSeminal Vesicles
2
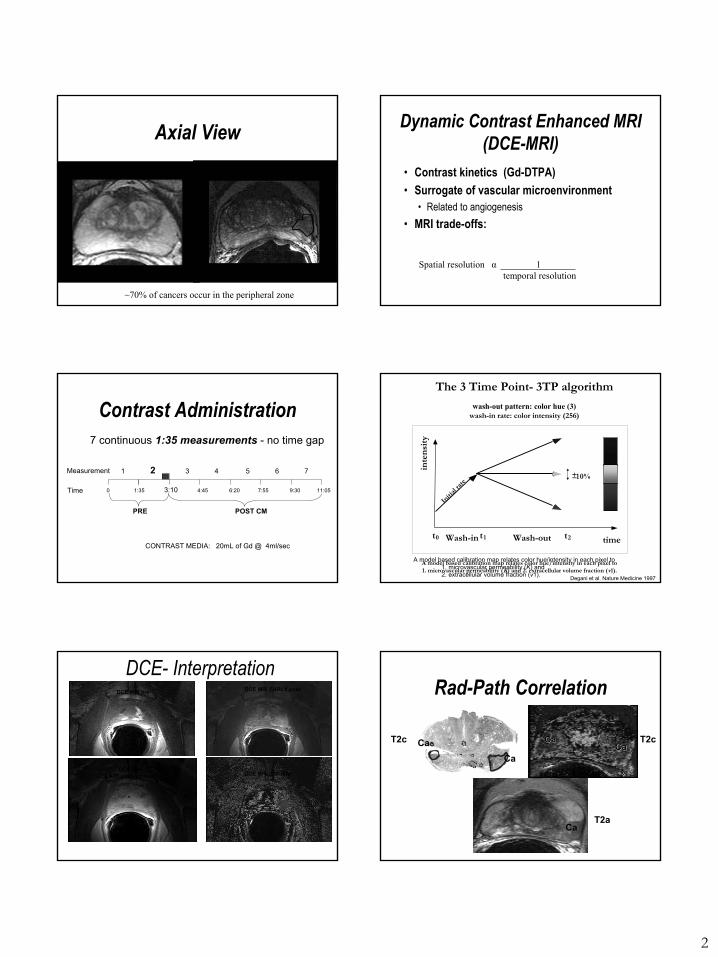
Axial ViewAxial View
~70% of cancers occur in the peripheral zone
Dynamic Contrast Enhanced MRI Dynamic Contrast Enhanced MRI (DCE(DCE--MRI)MRI)
•• Contrast kinetics (Contrast kinetics (GdGd--DTPA)DTPA)•• Surrogate of vascular microenvironmentSurrogate of vascular microenvironment
•• Related to angiogenesisRelated to angiogenesis•• MRI tradeMRI trade--offs:offs:
Spatial resolution α 1temporal resolution
7 continuous 1:35 measurements1:35 measurements - no time gap
Measurement 1 2 3 4 5 6 7
Time
CONTRAST MEDIA: 20mL of Gd @ 4ml/sec
0 1:35 3:10 4:45 6:20 7:55 9:30 11:05
PRE POST CM
Contrast AdministrationContrast AdministrationThe 3 Time PointThe 3 Time Point-- 3TP algorithm3TP algorithm
wash-out pattern: color hue (3)wash-in rate: color intensity (256)
t0
±10%
t1 t2Wash-in Wash-out
inte
nsi
ty
Initi
al ra
te
time
A model based calibration map relates color hue/intensity in each pixel to 1. microvascular permeability (K) and 2. extracellular volume fraction (v1).
A model based calibration map relates color hue/intensity in eacA model based calibration map relates color hue/intensity in each pixel to h pixel to 1. microvascular permeability (1. microvascular permeability (KK) and ) and 2. extracellular volume fraction (2. extracellular volume fraction (vv1). 1). Degani et al. Nature Medicine 1997Degani et al. Nature Medicine 1997
DCE MRI 3TP-MAPDCE MRI
LATE post contrast
DCE MRI EARLY postDCE MRI pre
DCEDCE-- InterpretationInterpretation
CaCaCaCaCa
Ca
CaT2a
RadRad--Path CorrelationPath Correlation
T2cT2c

3
% Staging Accuracy in 32 Patients w/ path correlation: Comparison of T2W, DCE and Combined Data Sets
Note.—All data are percentages. For AUC, numbers in ( )s are 95% CIs.
† Improvement vs. T2W MR images for reader 2 (P = .042).
Bloch, et al Radiology. 2007 Oct; 245:176-85.
3T 3T endoendo--rectal MRIrectal MRIof the Prostateof the Prostate
700700µµ x 500x 500µµ x 1.5 mmx 1.5 mm
3TP
3TP
HR T2-W MRI
Bloch, et al., Acad Radiol 2004
Higher Resolution for Finer DetailsHigher Resolution for Finer Details
-Smaller tumors
-Better visualization of relevant anatomy
MRI Impacting Clinical PracticeMRI Impacting Clinical Practice
•• Identify a target for Identify a target for bxbx•• ↑↑ PSA, no PSA, no dxdx•• ↑↑ PSA, PSA, s/ps/p txtx
•• Assist in watchful waitingAssist in watchful waiting
61 61 y.oy.o. man, a husband & father . man, a husband & father Rising PSARising PSA3 3 negneg bxbx rounds (~60 rounds (~60 negneg cores!)cores!)
US images rarely reveal a successful target
Virtual 18 core Virtual 18 core bxbx (one slice!!)(one slice!!)

4
Efficacy Study:Efficacy Study:MR ‘prompted’ MR ‘prompted’ bxbx procedureprocedure
1) Systematic Bx
2) Bx ‘targeted’ to uniqueMR findings
MR RESULTS: +; anterior
BX RESULTS (2 weeks after MR)Cores: 12 Systematic: all NEG
1/6 MR prompted POS (Gleason 3+4)18 total
CONCORDANCE: + Anterior
76 76 y.oy.o; PSA = 31, 3 prior ; PSA = 31, 3 prior negneg bxbx roundsrounds2.5 x 1.6 cm
Value of MR to prompt or guide Value of MR to prompt or guide bxbx•• Increased +Increased +bxbx yieldyield
•• In patients with prior In patients with prior negneg bxbx•• Compared to Compared to ‘‘saturation saturation bxbx’’•• Success with a variety of MR approachesSuccess with a variety of MR approaches
•• Relevant cancers detectedRelevant cancers detected•• 77% with Gleason 4 component77% with Gleason 4 component
•• Most found anterior and apicalMost found anterior and apical•• Less commonly sampledLess commonly sampled•• More difficult areasMore difficult areas
Correlation of Gleason Score and Tumor Size with High Resolution 3T Magnetic Resonance Image-Detected Prostate
CancerElizabeth M Genega 2 , B. Nicolas Bloch 1, Robin Elliott 2,
William Dewolf 3, Yineng Fu 2, Martin Sanda 3, John Tomaszewski 4, Andrew Wagner 3 , Neil M. Rofsky 1,
1Department of Radiology, Beth Israel Deaconess Medical Center and Harvard Medical School, Boston.2Department of Pathology, Beth Israel Deaconess Medical Center and Harvard Medical School, Boston. 3Department of Urology, Beth Israel Deaconess Medical Center and Harvard Medical School, Boston. 4Department of Pathology, University of Pennsylvania
Harvard Medical
School
PurposePurpose
To compare prostate cancer detected To compare prostate cancer detected and missed by MRI with whole mount and missed by MRI with whole mount prepared radical prostatectomy prepared radical prostatectomy specimens.specimens.To assess the histological features To assess the histological features associated with each group.associated with each group. Cancerous histology indicated by ‘black’Cancerous histology indicated by ‘black’

5
Results of Detailed Results of Detailed MRI/Path Correlation: MRMRI/Path Correlation: MR--
Most MR negative PCA foci are:Most MR negative PCA foci are:GS 6 (87%) GS 6 (87%) ≤≤7mm (97%)7mm (97%)Sparse TumorsSparse Tumors: Few tumor glands : Few tumor glands infiltrating between benign glandsinfiltrating between benign glands
Cancer indicated by ‘black’Cancer indicated by ‘black’ Subtraction Early – late T2 weighted image
MRI/Path Correlation: MRI/Path Correlation: 1of 2 tumors detected (both GS 3+4)1of 2 tumors detected (both GS 3+4)
Undetected3.5mmHisto ‘D’
Detected
8mm
Histo ‘B’
56yo w/ 56yo w/ ↑↑ PSA (prior to MRI = 27.7)PSA (prior to MRI = 27.7)3 prior NEG bx session; 3 prior NEG bx session; 63 cores prior to MRI 63 cores prior to MRI 3 months between 33 months between 3rdrd bx and MRIbx and MRI
T2T2--W W
DCEMRI color mapcolor map
Gleason 4+341mm
Histo ‘A’
RadRad--Path: ConclusionsPath: Conclusions
High resolution T2W and DCE 3T ecMR High resolution T2W and DCE 3T ecMR may be useful for guiding patient may be useful for guiding patient management, including:management, including:
a) Prea) Pre--biopsy detection / guidance of unusually located tumors biopsy detection / guidance of unusually located tumors b) Facilitates F/u b) Facilitates F/u
i) Locally treated cancers (esp. when the tumor is i) Locally treated cancers (esp. when the tumor is >7mm>7mm))ii) Active surveillanceii) Active surveillance
Active SurveillanceActive Surveillance•• Low grade, low volume tumorLow grade, low volume tumor•• No No txtx, No adverse effects, No adverse effects•• Survival rates no differentSurvival rates no different
•• Careful Careful f/uf/u is essential!!is essential!!•• Intent to treat if aggressive features emergeIntent to treat if aggressive features emerge
Case 1 Case 1
•• 49 49 yoyo African American Man African American Man
•• No urinary symptoms; sexually active, singleNo urinary symptoms; sexually active, single
•• PSA 4.5, Normal prostate examPSA 4.5, Normal prostate exam
•• Biopsy Biopsy –– Gleason 6 in less than 20Gleason 6 in less than 20--30% of 2 cores 30% of 2 cores (12 total biopsy cores)(12 total biopsy cores)
6
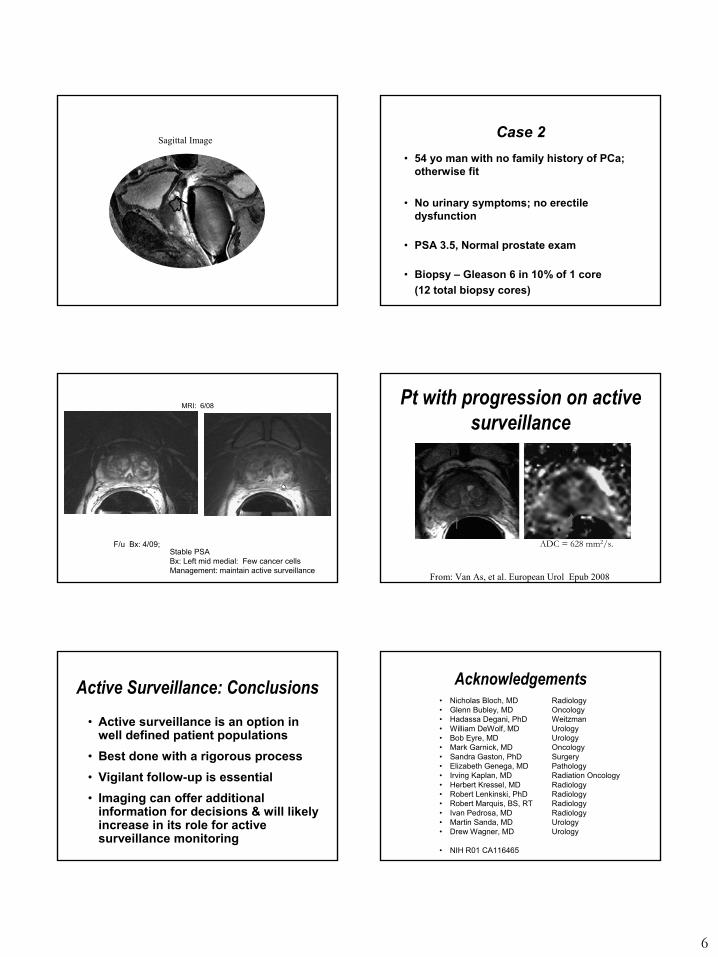
NLNL Sagittal Image Case 2 Case 2 •• 54 54 yoyo man with no family history of man with no family history of PCaPCa; ;
otherwise fitotherwise fit
•• No urinary symptoms; no erectile No urinary symptoms; no erectile dysfunctiondysfunction
•• PSA 3.5, Normal prostate examPSA 3.5, Normal prostate exam
•• Biopsy Biopsy –– Gleason 6 in 10% of 1 core Gleason 6 in 10% of 1 core (12 total biopsy cores)(12 total biopsy cores)
MRI: 6/08
F/u F/u BxBx: 4/09; : 4/09; Stable PSAStable PSABxBx: : Left mid medial: Few cancer cellsLeft mid medial: Few cancer cellsManagement: maintain active surveillanceManagement: maintain active surveillance
Pt with progression on active Pt with progression on active surveillancesurveillance
T2WI Diffusion MAP
ADC = 628 mm2/s.
From: Van As, et al. European Urol Epub 2008
Active Surveillance: ConclusionsActive Surveillance: Conclusions•• Active surveillance is an option in Active surveillance is an option in
well defined patient populationswell defined patient populations•• Best done with a rigorous processBest done with a rigorous process•• Vigilant followVigilant follow--up is essentialup is essential•• Imaging can offer additional Imaging can offer additional
information for decisions & will likely information for decisions & will likely increase in its role for active increase in its role for active surveillance monitoringsurveillance monitoring
AcknowledgementsAcknowledgements•• Nicholas Bloch, MDNicholas Bloch, MD RadiologyRadiology•• Glenn Glenn BubleyBubley, MD, MD OncologyOncology•• HadassaHadassa DeganiDegani, PhD, PhD WeitzmanWeitzman•• William William DeWolfDeWolf, MD, MD UrologyUrology•• Bob Eyre, MDBob Eyre, MD UrologyUrology•• Mark Mark GarnickGarnick, MD, MD OncologyOncology•• Sandra Gaston, PhDSandra Gaston, PhD SurgerySurgery•• Elizabeth Elizabeth GenegaGenega, MD, MD PathologyPathology•• Irving Kaplan, MDIrving Kaplan, MD Radiation OncologyRadiation Oncology•• Herbert Herbert KresselKressel, MD, MD RadiologyRadiology•• Robert Robert LenkinskiLenkinski, PhD, PhD RadiologyRadiology•• Robert Marquis, BS, RTRobert Marquis, BS, RT RadiologyRadiology•• Ivan Ivan PedrosaPedrosa, MD, MD RadiologyRadiology•• Martin Martin SandaSanda, MD, MD UrologyUrology•• Drew Wagner, MDDrew Wagner, MD UrologyUrology
•• NIH R01 CA116465NIH R01 CA116465