current conceptson the relationship between pulpal and periodontal diseases
TRANSCRIPT

_____________________________98 TMJ 2008, Vol. 58, No. 1 - 2
REVIEW ARTICLES
abstract
Received for publication: Feb. 22, 2008. Revised: May 19, 2008.
rEZUMat
1 Department of Anatomy and Embryology, 2 Department of Endodontology, Faculty of Dental Medicine, Carol Davila University of Medicine and Pharmacy, Bucharest, Romania, 3 Department of Periodontology, Faculty of Dental Medicine, Victor Babes University of Medicine and Pharmacy, Timisoara, Romania, 4 Department of Oral Rehabilitation, Faculty of Dental Medicine, Carol Davila University of Medicine and Pharmacy, Bucharest, Romania, 5 Department of Orthodontics, Faculty of Dental Medicine, Victor Babes University of Medicine and Pharmacy, Timisoara, Romania
Correspondence to:Andreea Didilescu, 2 Iovita Str., Bl. P24, Apt. 32, Bucharest, Tel. + 40-722-536-798 Email: [email protected]
INtrODUctION The dental pulp is closely connected with the
periodontal ligament through the apical foramina, accessory canals and dentinal tubules. Due to this relationship, pulp diseases may influence periodontal health and vice versa, and the periodontal infection may affect the pulp integrity. It is estimated that pulpal and periodontal problems are responsible for more than 50% of tooth mortality.1
cUrrENt cONcEPts ON tHE rELatIONsHIP bEtWEEN PULPaL aND PErIODONtaL DIsEasEs
Andreea Didilescu1, Radita Iliescu2, Darian Rusu3, Alexandru Andrei Iliescu4, Alexandru Ogodescu5, Emilia Ogodescu5, Stefan Stratul3
Combined endodontic-periodontal lesions represent a real challenge in the daily practice, both for the endodontist and periodontologist. The simultaneous existence in the same tooth of pulpal problems and inflammatory periodontal disease can complicate the diagnosis and the treatment of the affected tooth. This type of pathology represents a special situation in dentistry due to the complexity of anatomy and physiology of the pulp and periodontium. In this review, current topics relating to etiology, pathways of dissemination and clinical concepts in combined endo-periodontal lesions are summarized. The poor prognosis of these affections recommends an interdisciplinary approach with a good collaboration between specialists in endodontology, periodontology and microbiology.Key Words: pulp infection, periodontal infection, bacterial migration
Leziunile combinate endo-parodontale reprezint\ o adevarat\ provocare n practica medicala curent\, att pentru specialistul n endodon]ie, ct [i pentru cel n parodontologie. Existen]a simultan\ a problemelor pulpare [i parodontale la acela[i dinte poate complica diagnosticul [i tratamentul planificat pentru dintele respectiv. Acest tip de patologie reprezint\ o situa]ie special\ datorit\ complexit\]ii anatomiei [i fiziologiei pulpare [i parodontale. Lucrarea prezent\ [i propune s\ revizuiasc\ informa]iile din literatura de specialitate despre etiologie, c\i de diseminare [i aspecte clinice n leziunile endo-parodontale. Prognosticul rezervat al acestor afec]iuni recomand\ o abordare interdisciplinar\, cu o bun\ colaborare ntre speciali[tii n endodon]ie, parodontologie [i microbiologie.Cuvinte cheie: infec]ie pulpar\, infec]ie parodontal\, migrare bacterian\
Simon et al. (1972) have classified the lesions based on the primary source of infection, as follows:2
1. Primary endodontic lesions;2. Primary endodontic lesions with secondary
periodontal involvement;3. Primary periodontal lesions;4. Primary periodontal lesions with secondary
endodontic involvement;5. True combined lesions.In addition, Belk and Gutmann (1990) proposed
a sixth group of lesions - concomitant pulpal and periodontal lesions.3
EtIOLOGY
It has been demonstrated that the primary etiologic agent in periodontitis is bacterial plaque adhering to the teeth and other hard surfaces in the oral cavity. The pulp may be affected by the invasion of bacteria or their toxins, or by a direct trauma during the restorative therapy.4,5
Several factors make it difficult to establish a correct etiology of the combined endo-periodontal lesions.

_____________________________Andreea Didilescu et al 99
First, the pulpal pain may occur either in a primary endodontic lesion or in a primary periodontal lesion with secondary endodontic involvement. In the last situation, the periodontal symptoms may be masked by the pulpal symptoms. Second, the tests used for the diagnosis of endo-periodontal lesions, such as vitality tests and radiographic examinations, may lead to an incorrect or incomplete diagnosis.
MIcrObIOLOGY
The literature contains few descriptions of the periodontal-endodontic lesion microbiology. The profiles of the periodontal pathogens in simultaneous pulpal and periodontal disease associated with the same tooth, were investigated by Rupf et al.6 The periodontal pathogens displayed comparable profiles in pulpo-periapical lesions, except in progressive adult periodontitis. Kobayashi et al. concluded that the periodontal pocket in teeth with advanced periodontitis may be a possible source of root canal infections.7
The microbiology of endodontic infectionsRoot canal infections are mixed and semispecific
infections with a great predominance of obligate and facultative anaerobic bacteria. However, only a small group is commonly isolated from infected dental pulp cavities. The relative proportion of strict anaerobic bacteria to facultative aerobic bacteria increases with the time, and so does the total number of bacteria.8-12 According to recent reports, it is presumed that over 700 bacterial species inhabit the oral cavity and more than half of these cannot be cultivated.13,14 Specific combinations of bacteria can be found in the root canal and they can contribute to ecological shifts of the flora by different mechanisms of interaction.15
Bacteria may not only reside in the main canal, but they also invade the dentinal tubules, making them act as a reservoir for future dental and systemic infections.16,17 Porphyromonas gingivalis, Tannerella forsythensis and Fusobacterium nucleatum are associated with extraradicular biofilm formation and refractory periapical chronic periodontitis.18 The presence of T. forsythensis, P. gingivalis and Treponema denticola was demonstrated in root canal samples collected from patients with carious lesions, necrotic pulp and radiographic evidence of periradicular bone loss.19 T. denticola was highly associated with symptomatic endodontic infections and periapical bone resorption, whereas Enterococcus faecalis was associated with asymptomatic chronic apical periodontitis and secondary endodontic infections in
endodontic failures.20 Black-pigmented bacteria have been isolated from acute abscesses of dental origin, suggesting an active role in the pathogenesis of acute symptoms.21-23
The microbiology of periodontal infectionsThe periodontal infection is caused by
microorganisms colonizing the tooth surface at supra or subgingival level. Living, dying and dead bacteria and their metabolic byproducts form a resistant biofilm by attaching to the tooth, to the epithelial cells and to the underlying exposed tissues.24 The onset of the infectious periodontal disease depends on the simultaneous occurrence of a number of factors for initiation and progression, such as the virulence of periodontal pathogens, the local environment and the host defense mechanisms. It is already documented that approximately 15 host genes are involved in the onset and progression of the periodontal disease in humans.25
Different studies used various criteria such as the association between the pathogens and the disease, the elimination or decrease of species and the parallel remission of disease due to specific treatment, the host response, the virulence factors, associated different bacteria with different periodontal pathoses.26-30 Actinobacillus actinomycetemcomitans, P. gingivalis, T. forsythensis, Prevotella intermedia, F. nucleatum, Campylobacter rectus, Eikenella corrodens, Peptostreptococcus micros and Eubacterium are the best studied periodontal pathogens.31 However, their proportion in the dental biofilm and their virulence may differ among individuals with periodontal disease.32
PatHWaYs OF DIssEMINatION
Both endodontic and periodontal diseases are caused by mixed anaerobic infections. Bacteria and their inflammatory by-products can penetrate through the pathways connecting the periodontium and the pulp. Kerns and Glickman described six groups of normal and pathological pathways:33 (Fig. 1)
1. The apical foramen may be the most significant direct route of communication between the pulp and the periodontium. The apical foramina represent also a portal of entry towards the pulp from deep periodontal pockets. Pulp infection extends into the periapical tissues causing a local inflammatory response, followed by alveolar bone and sometimes by focal root resorptions.34
2. Lateral and accessory canals appear mainly in the apical area and in the furcation area of molars.
_____________________________100 TMJ 2008, Vol. 58, No. 1 - 2
Figure 1. The normal pathways of communication between the endodontium and the periodontium (1 -the apical foramen, 2, 3 - lateral and accessory canals, 4 - dentinal tubules).
They have been suggested to be direct pathways between the pulp and the periodontium and contain connective tissue and blood vessels that connect the circulatory systems of the two tissues.33 The presence of patent accessory canals is a potential pathway for the spread of bacteria and toxic substances from the pulp, resulting in an inflammatory process within the periodontal ligament.34
3. Dentinal tubules contain odontoblastic processes that extend from the odontoblasts to the dentin-enamel junction or the dentin-cementum junction. Fluid may flow through patent dentinal tubules. In absence of an intact enamel or cementum covering, the pulp may be considered exposed to the oral environment. The number of dentinal tubules per square millimetre varies from 8,000 to 57,000 and the diameter ranges from 0.5 μm in the peripheral dentin to 3-4 μm near the pulp. The permeability of root dentin depends upon dentin thickness, the number of tubules/mm2, and the diameter and patency of the tubules.35
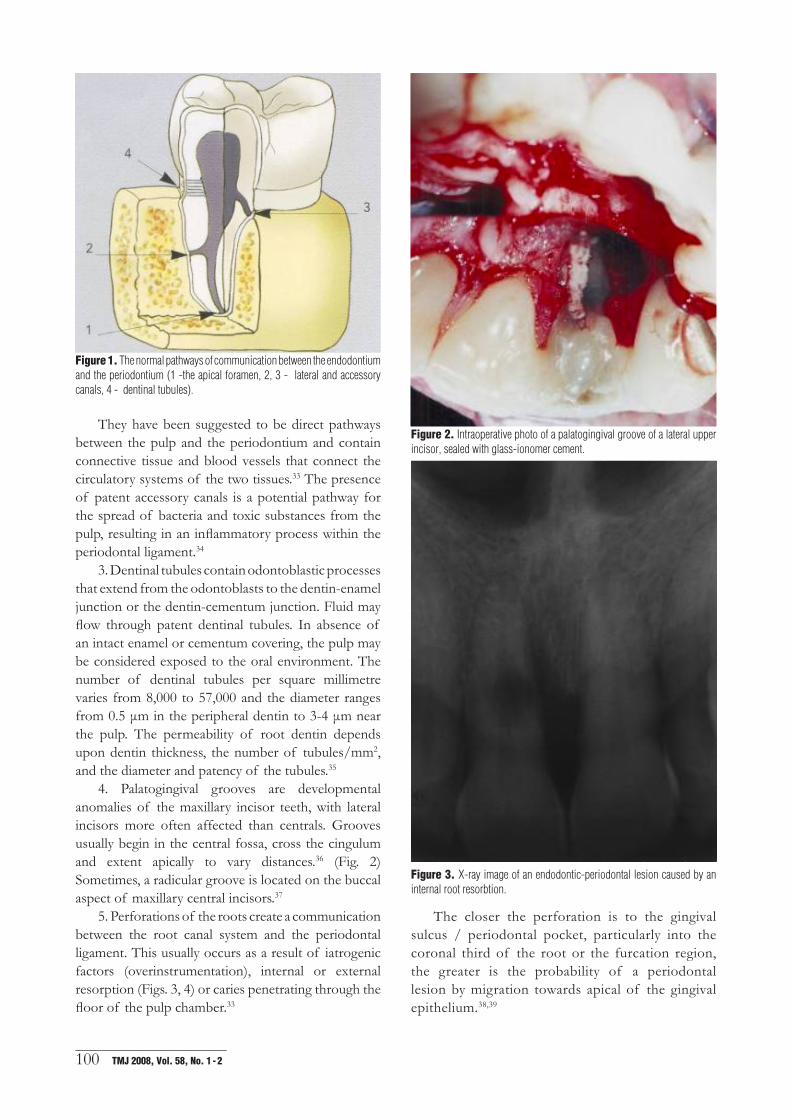
4. Palatogingival grooves are developmental anomalies of the maxillary incisor teeth, with lateral incisors more often affected than centrals. Grooves usually begin in the central fossa, cross the cingulum and extent apically to vary distances.36 (Fig. 2) Sometimes, a radicular groove is located on the buccal aspect of maxillary central incisors.37
5. Perforations of the roots create a communication between the root canal system and the periodontal ligament. This usually occurs as a result of iatrogenic factors (overinstrumentation), internal or external resorption (Figs. 3, 4) or caries penetrating through the floor of the pulp chamber.33
Figure 2. Intraoperative photo of a palatogingival groove of a lateral upper incisor, sealed with glass-ionomer cement.
Figure 3. X-ray image of an endodontic-periodontal lesion caused by an internal root resorbtion.
The closer the perforation is to the gingival sulcus / periodontal pocket, particularly into the coronal third of the root or the furcation region, the greater is the probability of a periodontal lesion by migration towards apical of the gingival epithelium.38,39

_____________________________Andreea Didilescu et al 101
Figure 5. Endodontic-periodontal lesion with primary endodontic lesions and secondary periodontal involvement of 16. Initial (A) and after re-entry (B) X-ray of the upper first molar. Intra-operatory image of the initial periodontal defect (C) and the re-entry image after the 6 months (D).
endodontic origin of this condition, due most probably to the second mesio-buccal canal, very often ignored during the endodontic therapy. (Fig. 5)
Figure 4. Pre-operatory image of the same lesion while measuring the initial pocket depth.
6. Vertical root fractures occur accidentally. A periapical lesion often forms, which may have the radiographical appearance of a pulpal related lesion. A way of communication between root canal and periodontium is created, giving possibility to bacteria and their by-products to invade the surrounding periodontal ligament.34,39
cLINIcaL cONcEPts
Primary endodontic lesions with secondary periodontal involvement
A causal relationship between root canal infection and periodontal disease requires a patent route to the periodontium, an infected root canal system and sufficient virulence of the pulpal bacteria to promote marginal periodontitis.40 In the absence of treatment, the pulpal infection will continue, leading to destruction of the periapical alveolar bone and progressing into the area of furcation. Due to drainage through the gingival sulcus and accumulation of plaque in the purulent pocket, periodontal disease progresses and the further apical migration of the attachment may occur.33 Extensive pulpal infection spreading through patent lateral canals or dentinal tubules in the absence of an intact cementum may alter the periodontium, too.40 Radiographs show evidence of both pulpal and periodontal disease.
A typical situation: the upper first molar displays signs of periodontal disease with loss of attachment of mesio-buccal root. Radiographic examination reveals the presence of periapical and periodontal radiolucency, and a complete obturation of three canals. Usually, in this case, the symptoms are misinterpreted and the diagnosis is of localized periodontitis; consequently, the applied treatment consists of scaling and root-planning, associated with local antiseptics and irrigations with clorhexidine. Healing does not occur because of the
A
B
C
D

_____________________________102 TMJ 2008, Vol. 58, No. 1 - 2
Therefore, the correct diagnosis is of primary endodontic lesion with secondary periodontal involvement.
Primary endodontic lesions with secondary periodontal involvement may also be the results of iatrogenic factors, such as root perforations, root fracture or misplacement of posts during coronal restorations.34
Figure 6. Primary periodontal lesions with secondary endodontic involvement lesion. Initial x-ray of the defect (A) and initial probing of the PD (B). Intra-operatory aspect of the bone (C). Six months after x-ray (D) with the root canal treatment completed and the bone defect filled.
Primary periodontal lesions with secondary endodontic involvement
The effect of periodontitis on the healthy pulp has been reported in several studies.41,42 Periodontal disease can affect the pulp through dentinal tubules, lateral canals or apical foramina. Lateral canals and dentinal tubules may be also infected through a temporary opening to the oral environment during surgical flap procedures. When the pulp is affected, the patient reports acute pain and clinical signs of pulpal inflammation. Radiographically, these lesions may be indistinguishable from the primary endodontic lesions with secondary periodontal involvement.33 (Fig. 6)
True combined lesionsPulpal and periodontal diseases may occur
independently and concomitantly in and around the same tooth. A necrotic pulp or a failing endodontic treatment, plaque, calculus and periodontitis are present in varying degrees.33 True combined endo-periodontal lesions present radiographic evidence of bone loss surrounding a substantial area of the root. Periodontal probing reveals a pocket extending to the apical region of the tooth. However, a fully documented diagnosis of a true combined lesion is hard to establish.
Concomitant pulpal and periodontal lesionsIn this case, periodontal and pulpal diseases
coexist, but with different etiology. Radiographically, the endodontic lesion and a noncommunicating periodontal pocket are observed.33
cONcLUsIONs
The tooth anatomy and the etiology of endodontic-periodontal lesions offers a strong base for establishing a correct diagnosis. Due to the complexity of these affections, an interdisciplinary approach with a good collaboration between endodontists, periodontologists and microbiologists, is recommended.
rEFErENcEs
1. Chen SY, Wang HL, Glickman GN. The influence of endodontic treatment upon periodontal wound healing. J Clin Periodontol 1997;24:449-56.
2. Simon JH, Glick DH, Frank AL. The relationship of endodontic-periodontic lesions. J Periodontol 1972;43(4):202-8.
3. Belk CE, Gutmann JL. Perspectives, controversies, and directives on pulpal-periodontal relationship. J Canadian Dent Assoc 1990;56:1013-7.
4. Zach L, Cohen G. Pulp response to externally applied heat. Oral Surg Oral Med Oral Pathol 1965;19:515-30.
5. Trowbridge HO. Pathogenesis of pulpitis resulting from dental caries. J Endod 1981;7:52-60.
A
B
C
D

_____________________________Andreea Didilescu et al 103
6. Rupf S, Kannengieber S, Merte K, et al. Comparison of profiles of key periodontal pathogens in periodontium and endodontium. Endod Dent Traumatol 2000;16(6):269-75.
7. Kobayashi T, Hayashi A, Yoshikawa R, et al. The microbial flora from root canals and periodontal pockets of non-vital teeth associated with advanced periodontitis. Int Endod J 1990;23(2):100-6.
8. Sundqvist G. Ecology of the root canal flora. J Endod. 1992;18(9):427-30.
9. Baumgartner JC. Endodontic microbiology. In: Walton RE, Torabinejad M, editors. Principles and practice of endodontics. 3rd ed. Philapdelphia: Saunders Co.; 2002. p. 282-93.
10. Siqueira JF Jr. Endodontic infections: concepts, paradigms, and perspectives. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2002;94(3):281-93.
11. Siqueira JF Jr, Rôças IN, Souto R, et al. Actinomyces species, streptococci, and Enterococcus faecalis in primary root canal infections. J Endod 2002;28(3):168-72.
12. Baumgartner JC, Hutter JW, Siqueira JF. Endodontic Microbiology and Treatment of Infections. In: Cohen S, Hargreaves KM, editors. Pathways of the pulp, 9th ed. St. Louis: Mosby Inc, 2006, p. 580-607.
13. Socransky SS, Haffajee AD. Periodontal microbial ecology. Periodontol 2005;38(1):135-87.
14. Sakamoto M, Umeda M, Benno Y. Molecular analysis of human oral microbiota. J Periodontal Res 2005;40(3):277-85.
15. Peters LB, Wesselink PR, van Winkelhoff AJ. Combinations of bacterial species in endodontic infections. Int Endod J 2002;35(8):698-702.
16. Oguntebi BR. Dentine tubule infection and endodontic therapy implications. Int Endod J 1994;27(4):218-22.
17. Matsuo T, Shirakami T, Ozaki K, et al. An immunohistological study of the localization of bacteria invading root pulpal walls of teeth with periapical lesions. J Endod 2003;29(3):194-200.
18. Noguchi N, Noiri Y, Narimatsu M, et al. Identification and localization of extraradicular biofilm-forming bacteria associated with refractory endodontic pathogens. Appl Environ Microbiol 2005;71(12):8738-43.
19. Siqueira JF, Rocas IN, Souto R, at al. Checkerboard DNA-DNA hybridization analysis of endodontic infections. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2000;89:744-8.
20. Foschi F, Cavrini F, Montebugnoli L et al. Detection of bacteria in endodontic samples by polymerase chain reaction assays and association with defined clinical signs in Italian patients. Oral Microbiol Immunol 2005;20:289-95.
21. Yoshida M, Fukushima H, Yamamoto K et al. Correlation between clinical symptoms and microorganisms isolated from root canals of teeth with periapical pathosis. J Endod 1987;13:24-8.
22. Hashioka K, Yamasaki M, Nakane A et al. The relationship between clinical symptoms and anaerobic bacteria from infected root canals. J Endod 1992;18:558-661.
23. Siqueira JF Jr, Rocas IN, Oliveira JC et al. Molecular detection of black-pigmented bacteria in infections of endodontic origin. J Endod 2001;9:563-6.
24. Costerton JW, Stewart PS, Greenberg EP. Bacterial biofilms: a common cause of persistent infections. Science 1999;284:1318-22.
25. Kinane DF, Hart TC. Genes and gene polymorphism associated with periodontal disease. Crit Rev Oral Biol Med 2003;14(6):430-49.
26. Darveau RP, Belton CM, Reife RA, et al. Local chemokine paralysis, a novel pathogenic mechanism for Porphyromonas gingivalis. Infect Immun 1998;66:1660-5.
27. Lamont RJ, Jenkinson HF. Life below the gum line: pathogenic mechanisms of Porphyromonas gingivalis. Microbiol Mol Biol Rev 1998;62:1244-63.
28. Kolenbrander PE. Oral microbial communities: biofilms, interactions, and genetic systems. Annu Rev Microbiol 2000;54:413-37.
29. Potempa J, Banbula A, Travis J. Role of bacterial proteinases in matrix destruction and modulation of host responses. Periodontol 2000;24:153-92.
30. Ximénez-Fyvie LA, Haffajee AD, Socransky SS. Microbial composition of supra- and subginigival plaque in subjects with adult periodontitis. J Clin Periodontol 2000;27:722-32.
31. Socransky SS, Haffajee AD. Microbiology of periodontal disease. In: Lindhe J, Karring T, Lang NP, editors. Clinical Periodontology and Implant Dentistry, 4th Ed. Copenhagen: Blackwell Munksgaard; 2003, p. 106-49.
32. Haffajee AD, Bogren A, Hasturk H, et al. Subgingival microbiota of chronic periodontitis subjects from different geographic locations. J Clin Periodontol 2004;31(11):996-1002.
33. Kerns DG, Glickman GN. Endodontic and periodontal interrelationships. In: Cohen S and Hargreaves KM, Eds. Pathways of the Pulp, 9th Ed. St. Louis: Mosby Inc, 2006, p. 650-67.
34. Rotstein I, Simon JHS. Diagnosis, prognosis and decision-making in the treatment of combined periodontal-endodontic lesions. Periodontol 2004; 34(1):165-203.
35. Pashley D. Pulpodentin complex. In: Hargreaves KM, Goodis HE, editors. Seltzer and Bender’s Dental Pulp, 4th Ed. Carol Stream: Quintessence, 2002, p. 63-93.
36. Nanba K, Ito K. Palatal radicular multigrooves associated with severe periodontal defects in maxillary central incisors. J Clin Periodontol 2001;28(4):372-5.
37. Kerezoudis NP, Siskos GJ, Tsatsas V. Bilateral buccal radicular groove in maxillary incisors: case report. Int Endod J 2003;36(12):898-906.
38. Basten CH-J, Ammons WF Jr, Persson R. Long-term evaluation of root resected molars: a retrospective study. Int J Periodontics Restorative Dent 1996;16:206.
39. Meng HX. Periodontic-Endodontic Lesions. Ann Periodontol 1999;4(1): 84-90.
40. Rutherford RB. Interrelationship of Pulpal and Periodontal Diseases. In: Hargreaves KM, Goodis HE, Eds. Seltzer and Bender’s Dental Pulp, 4th Ed. Carol Stream: Quintessence, 2002, p. 411-24.
41. Bergenholtz G, Lindhe J. Effect of experimentally induced marginal periodontitis and periodontal scaling on the dental pulp. J Clin Periodontol 1978;5:59-73.