current guideline for af treatment - 대한내과학회 guideline for af treatment young keun on,...
TRANSCRIPT
Current Guideline for AF Treatment
Young Keun On, MD, PhD, FHRS
Samsung Medical Center
Sungkyunkwan University School of Medicine
Case 1
• 59 year-old lady
• Sudden palpitation and breathlessness for 12 hours
• Remote onset 2 months ago
• Palpitation persisted for 1~2 hours
• HTN (-), DM (-)
Echocardiography
• LVEF 67% LVESD/EDD 30/53 mm
• LA 42 mm LAVI 22 ml/m2
• IVSd 10 mm, LVPWd 10 mm
• Normal LV and RV
• Valve : normal
• Great vessel : normal

What treatment strategy would you choose?
1. Rate control strategy
2. Rate control strategy with anticoagulation
3. Rhythm control strategy
4. Rhythm control strategy with anticoagulation
5. Anticoagulation only

Classification
First detected AF
Permanent AF
(irreversible)
Persistent AF
(Not self- terminating)
> 7 days
Paroxysmal AF
(Self- terminating)
≤ 7 days (most <24hr)
Recurrent : two or more episode
Longstanding persistent AF: continuous AF of greater than one-year duration

Diseases associated with AF
• Valvular Heart Disease : Rheumatic mitral disease
• Non-valvular HD : CAD, HTN
• Hyperthyroidism
• Pulmonary thromboembolism

Rhythm control for AF
• Pharmacologic treatment
• DC cardioversion
• RFCA (radiofrequency catheter ablation)
• Maze operation

Vaughan Williams Classification
of Antiarrhythmic Drug Actions
Type IA (block the sodium channel with intermediate recovery time)
Disopyramide, Procainamide, Quinidine
Type IB (block the sodium channel with rapid recovery time)
Lidocaine, Mexiletine
Type IC (block the sodium channel with slow recovery time)
Flecainide, Moricizine, Propafenone
Type II Beta-blockers (e.g., propranolol)
Type III (prolongation of the cardiac action potential)
Amiodarone, Bretylium, Dofetilide, Ibutilide, Sotalol
Type IV
Calcium-channel antagonists (e.g., verapamil and diltiazem)

2014 AHA/ACC/HRS AF guideline
Rhythm Control in AF


After Medication of Propafenone 300 mg bid

Atrial Fibrillation
• The most common cardiac arrhythmia.
• Confers a 5-fold risk of stroke.
• The rate of ischemic stroke among patients with AF
averages 5% per year.
• One of five (20%) of all strokes is attributed to AF.
• The risk of death from AF-related stroke is doubled.

Treatment strategy of AF
• Prevention of thromboembolism
: Antithrombotic therapy
• Rhythm control
• Rate control
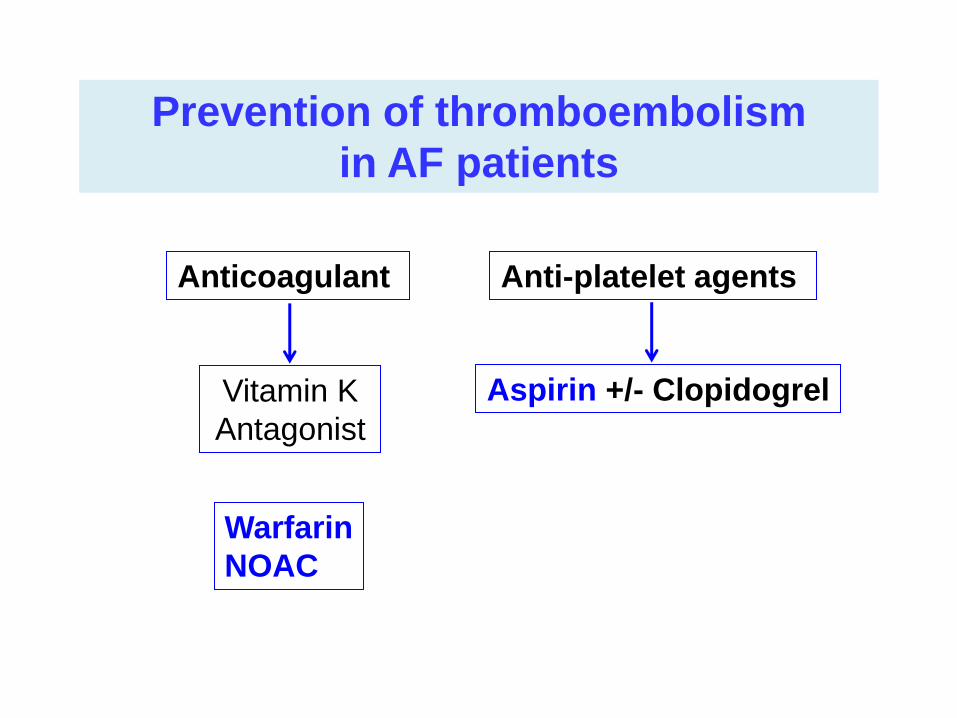
Prevention of thromboembolism
in AF patients
Vitamin K
Antagonist
Warfarin
NOAC
Anticoagulant Anti-platelet agents
Aspirin +/- Clopidogrel
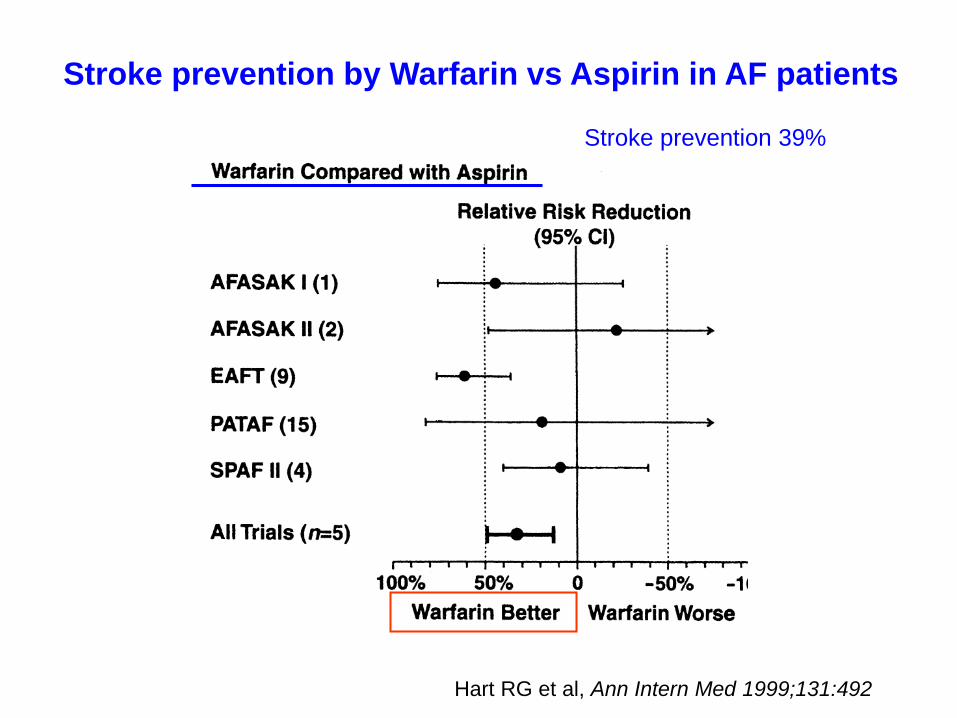
Hart RG et al, Ann Intern Med 1999;131:492
Stroke prevention by Warfarin vs Aspirin in AF patients
Stroke prevention 39%

Stroke and ICH by INR in AF patients
Hylek EM et al, N Engl J Med 1996;335:540
INR

CHA2DS2VASc score and stroke rate
Camm AJ, et al. Eur Heart J 2010
Risk factors
• CHF (1)
• HT (1)
• ≥ 75 yrs old (2)
• DM (1)
• Previous stroke, TIA,
Thromboembolism (2)
• Vascular disease (1)
• 65~74 yrs old (1)
• Female (1) 0
2
4
6
8
10
12
14
16
0 1 2 3 4 5 6 7 8 9
Annual stroke rate

Pisters R, et al, Chest 2010
HAS-BLED bleeding risk score
Bleeding risk score
• Hypertension (1)
• Abnormal renal function (1)
• Abnormal liver function (1)
• Stroke (1)
• Bleeding (1)
• Labile INRs (1)
• Elderly > 65 yrs old (1)
• Drugs (1)
• Alcohol (1)
• Hypertension: systolic blood pressure >160 mmHg
• Abnormal kidney function: the presence of chronic dialysis or renal transplantation or serum creatinine ≥200 mol/L.
• Abnormal liver function: chronic hepatic disease (e.g. cirrhosis) or bilirubin >2 x upper limit of normal in association with aspartate aminotransferase/alanine aminotransferase/alkaline phosphatase >3 x upper limit normal).
• Bleeding : previous bleeding history and/or predisposition to bleeding, e.g. bleeding diathesis, anemia, etc.
• Labile INRs : unstable/high INRs or poor time in therapeutic range (e.g. <60%)
• Drugs/alcohol use : concomitant use of drugs, such as antiplatelet agents, non-steroidal anti-inflammatory drugs, or alcohol abuse
Bleeding risk score
• Elderly > 65 yrs old (1)
• Stroke (1)
• Hypertension (1)
• Abnormal renal function (1)
• Abnormal liver function (1)
• Bleeding (1)
• Labile INRs (1)
• Drugs (1)
• Alcohol (1)
CHA2DS2VASc score vs HAS-BLED score
Stroke risk factors
• ≥ 75 yrs old (2)
• Previous stroke, TIA,
Thromboembolism (2)
• CHF (1)
• HTN (1)
• DM (1)
• Vascular disease (1)
• 65~74 yrs old (1)
• Female (1)
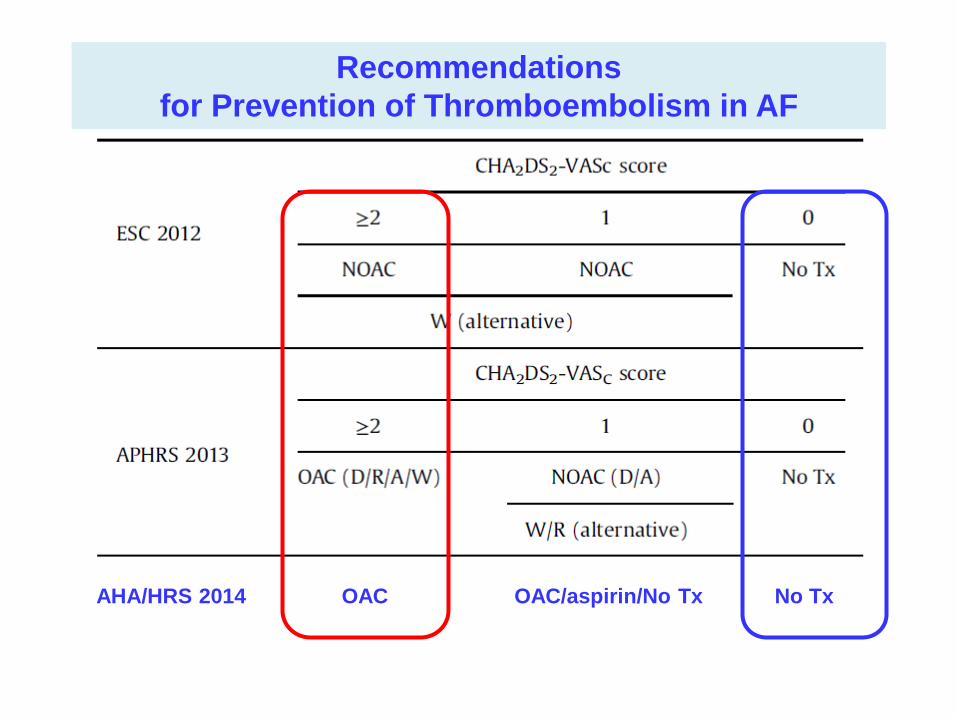
Recommendations
for Prevention of Thromboembolism in AF
AHA/HRS 2014 OAC OAC/aspirin/No Tx No Tx

Case 1 CHA2DS2VASc score : 1 → 0 • Female (1) ; lone AF
HAS-BLED score : 0

What treatment strategy would you choose?
1. Rate control strategy
2. Rate control strategy with anticoagulation
3. Rhythm control strategy
4. Rhythm control strategy with anticoagulation
5. Anticoagulation only

Case 2
• 60 year-old gentleman
• Palpitation with chest discomfort, dizziness
• Drug refractory recurrent paroxysmal to persistent AF
• Medication Hx : propafenone, flecainide, sotalol
• Hypertension (+) with medication for 2 years


Echocardiography
• Normal LV cavity size & systolic function
• Normal LV wall thickness
• No regional wall motion abnormality
• LVEF: 68% LVIDs/LVIDd: 27/48mm
• LA: 40mm LAVI: 25.7ml/m2
• IVSd : 9mm LVPWd: 10mm
• E: 0.89m/s e`: 0.164m/s E/e`: 5.43
• Ao: 27mm DT: 119.0msec

CHA2DS2VASc score : 1 • HTN
HAS-BLED score : 1
• HTN
What treatment strategy would you choose?
1. Rate control strategy
2. Rate control strategy with anticoagulation
3. Rhythm control strategy
4. Rhythm control strategy with anticoagulation
5. Anticoagulation only
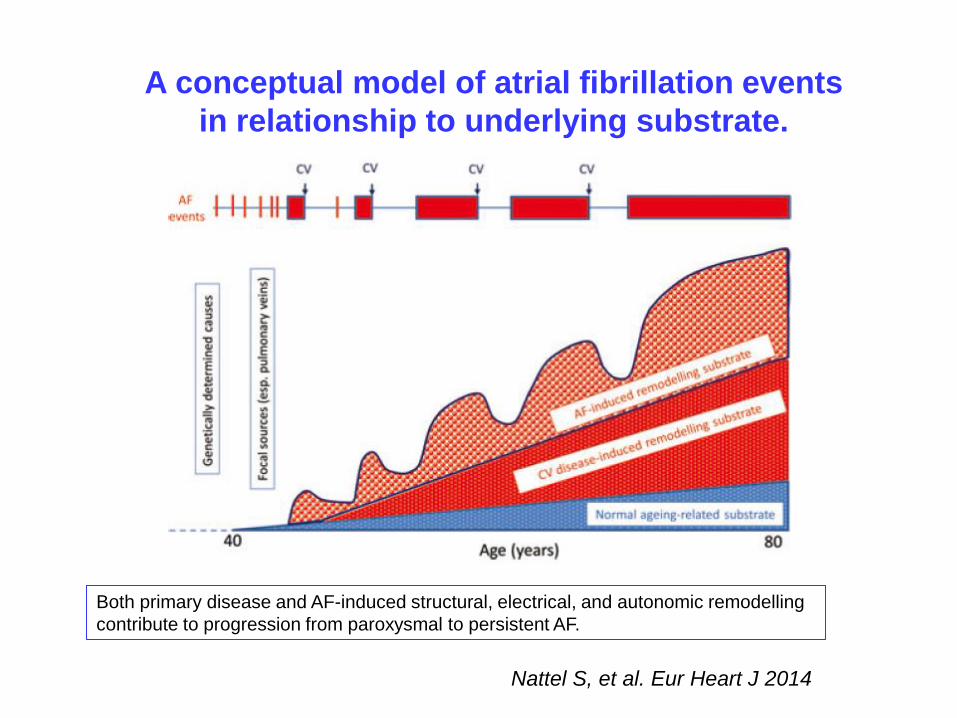
Nattel S, et al. Eur Heart J 2014
A conceptual model of atrial fibrillation events
in relationship to underlying substrate.
Both primary disease and AF-induced structural, electrical, and autonomic remodelling
contribute to progression from paroxysmal to persistent AF.
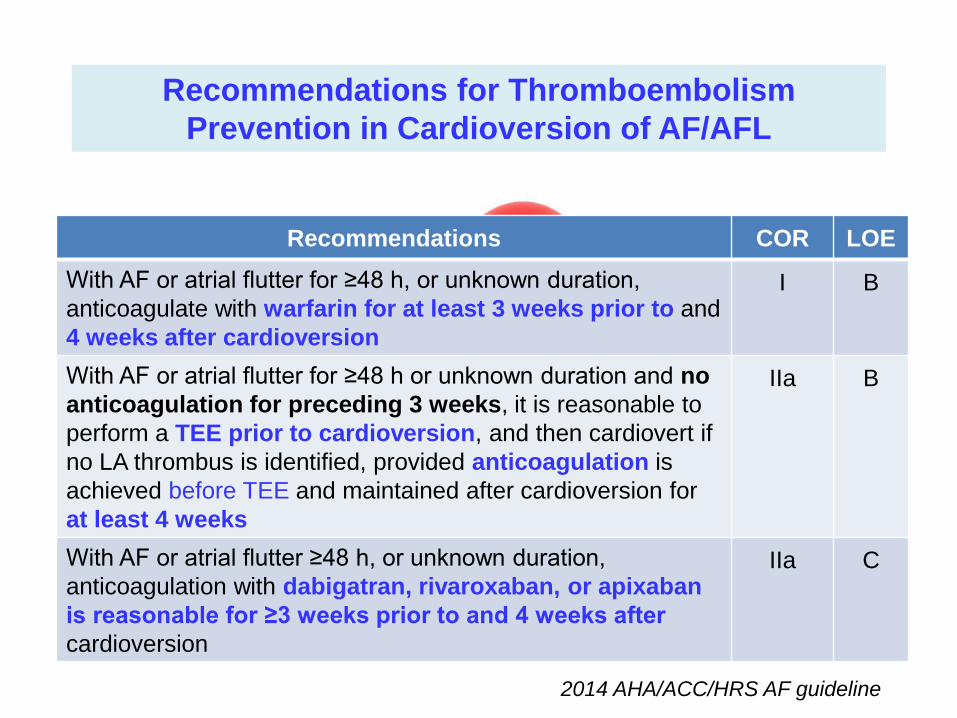
Recommendations for Thromboembolism
Prevention in Cardioversion of AF/AFL
Recommendations COR LOE
With AF or atrial flutter for ≥48 h, or unknown duration,
anticoagulate with warfarin for at least 3 weeks prior to and
4 weeks after cardioversion
I B
Recommendations COR LOE
With AF or atrial flutter for ≥48 h, or unknown duration,
anticoagulate with warfarin for at least 3 weeks prior to and
4 weeks after cardioversion
I B
With AF or atrial flutter for ≥48 h or unknown duration and no
anticoagulation for preceding 3 weeks, it is reasonable to
perform a TEE prior to cardioversion, and then cardiovert if
no LA thrombus is identified, provided anticoagulation is
achieved before TEE and maintained after cardioversion for
at least 4 weeks
IIa B
With AF or atrial flutter ≥48 h, or unknown duration,
anticoagulation with dabigatran, rivaroxaban, or apixaban
is reasonable for ≥3 weeks prior to and 4 weeks after
cardioversion
IIa C
2014 AHA/ACC/HRS AF guideline

Recurrence of Atrial Fibrillation patients
after DC cardioversion

What treatment strategy would you choose?
1. Rate control strategy
2. Rate control strategy with anticoagulation
3. Rhythm control strategy
4. Rhythm control strategy with anticoagulation
5. Anticoagulation only
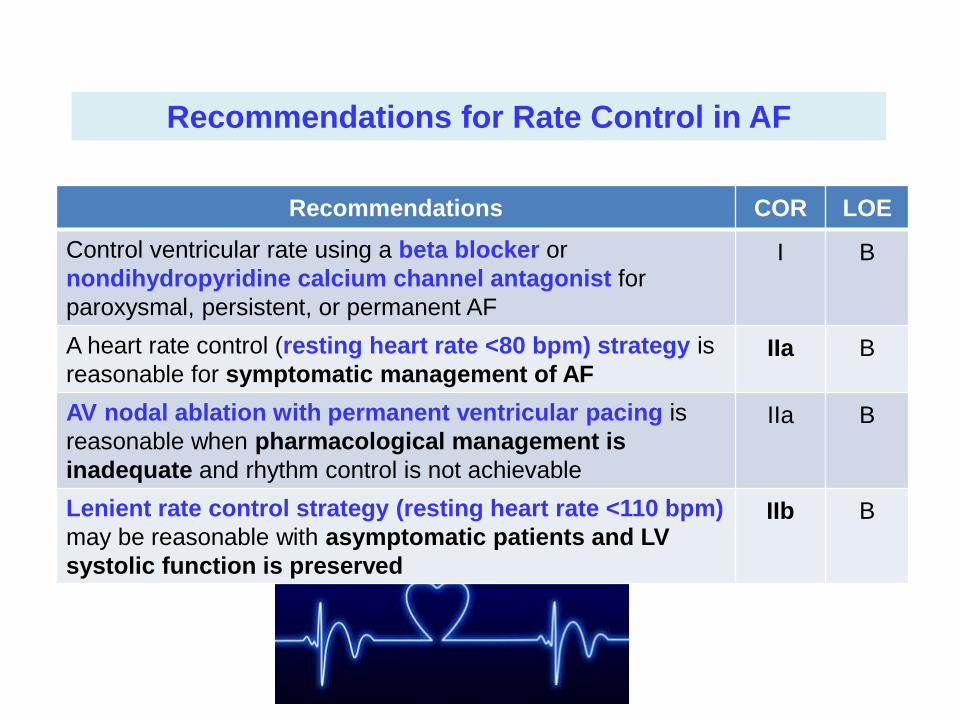
Recommendations for Rate Control in AF
Recommendations COR LOE
Control ventricular rate using a beta blocker or
nondihydropyridine calcium channel antagonist for
paroxysmal, persistent, or permanent AF
I B
A heart rate control (resting heart rate <80 bpm) strategy is
reasonable for symptomatic management of AF IIa B
AV nodal ablation with permanent ventricular pacing is
reasonable when pharmacological management is
inadequate and rhythm control is not achievable
IIa B
Lenient rate control strategy (resting heart rate <110 bpm)
may be reasonable with asymptomatic patients and LV
systolic function is preserved
IIb B

Radiofrequency Catheter Ablation (RFCA)
Radiofrequency lesion in human ventricular myocardium
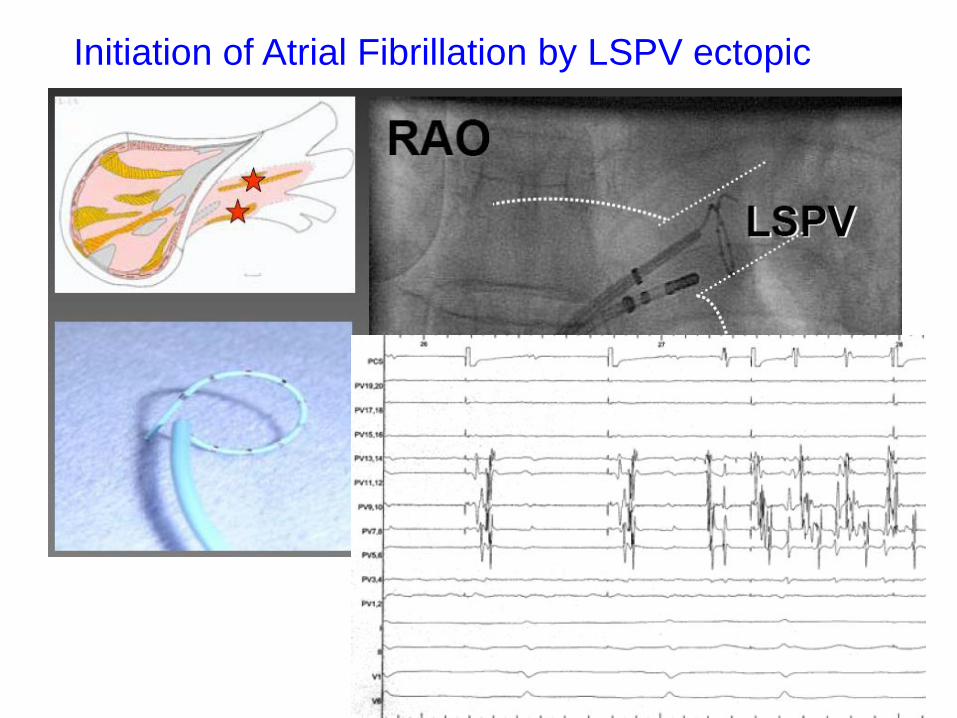
Initiation of Atrial Fibrillation by LSPV ectopic


PAC & induction of AF
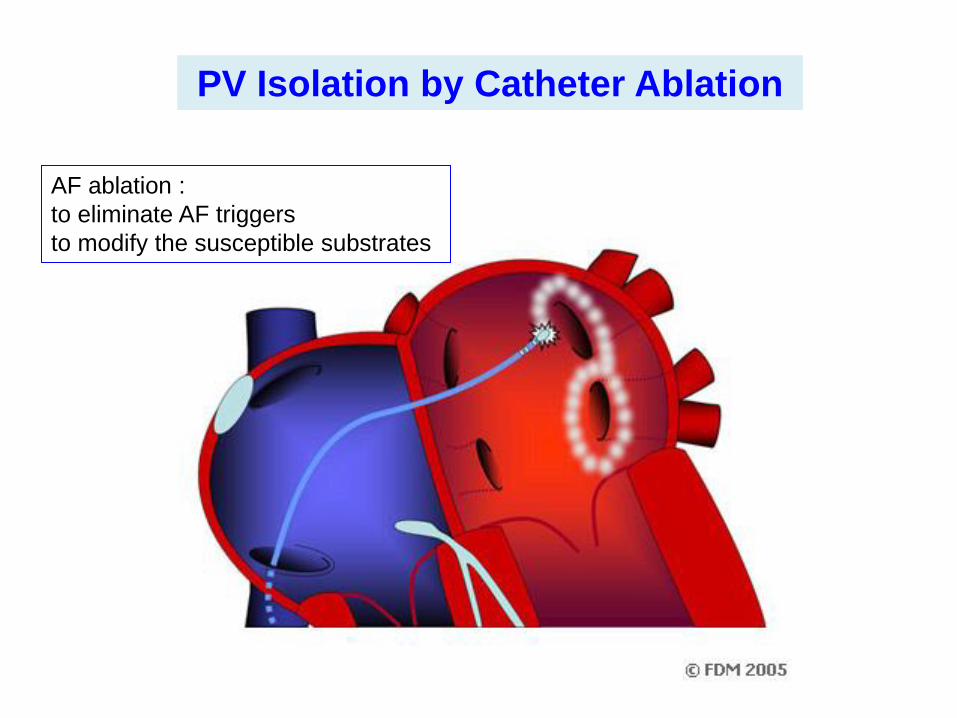
AF ablation :
to eliminate AF triggers
to modify the susceptible substrates
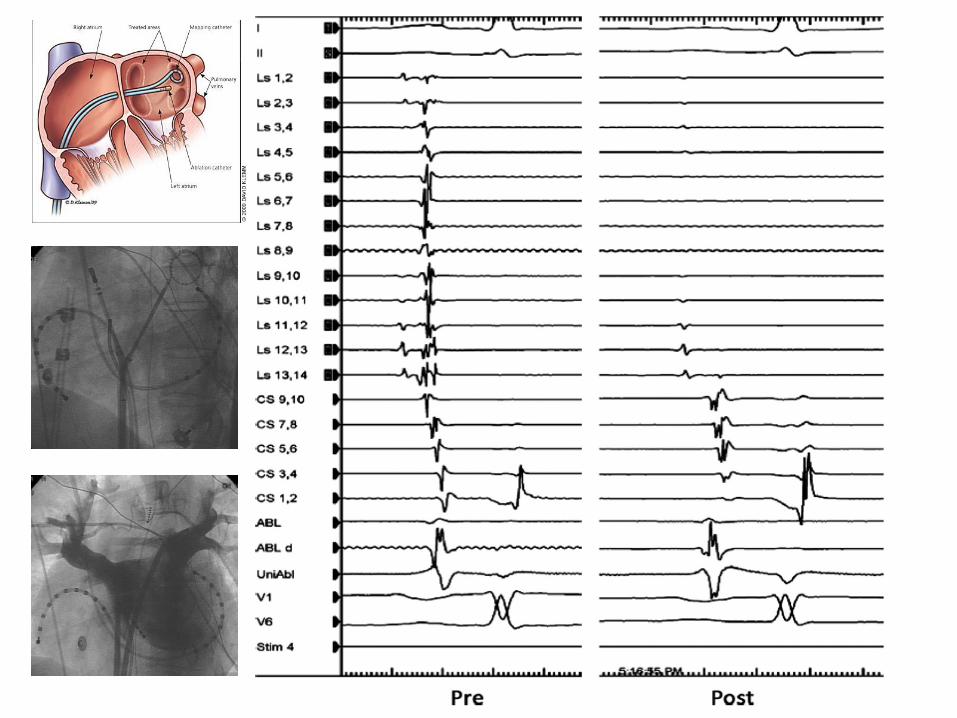
PV Isolation by Catheter Ablation

Three dimensional map of the LA and PV
Radiofrequency lesions
CT angiography
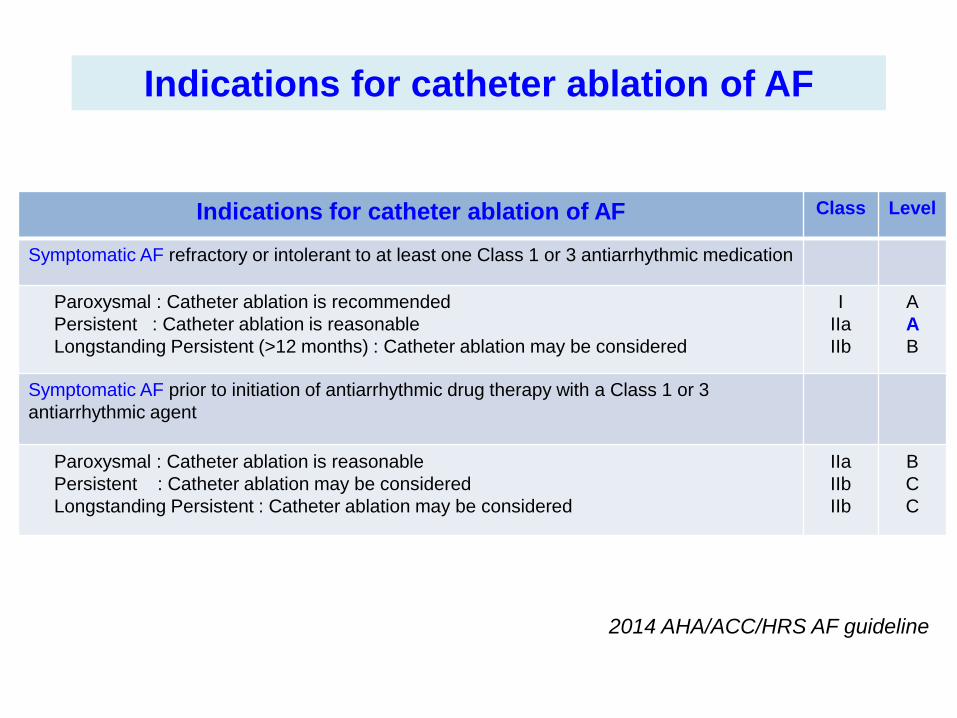
Indications for catheter ablation of AF
Indications for catheter ablation of AF Class Level
Symptomatic AF refractory or intolerant to at least one Class 1 or 3 antiarrhythmic medication
Paroxysmal : Catheter ablation is recommended
Persistent : Catheter ablation is reasonable
Longstanding Persistent (>12 months) : Catheter ablation may be considered
I
IIa
IIb
A
A
B
Symptomatic AF prior to initiation of antiarrhythmic drug therapy with a Class 1 or 3
antiarrhythmic agent
Paroxysmal : Catheter ablation is reasonable
Persistent : Catheter ablation may be considered
Longstanding Persistent : Catheter ablation may be considered
IIa
IIb
IIb
B
C
C
2014 AHA/ACC/HRS AF guideline
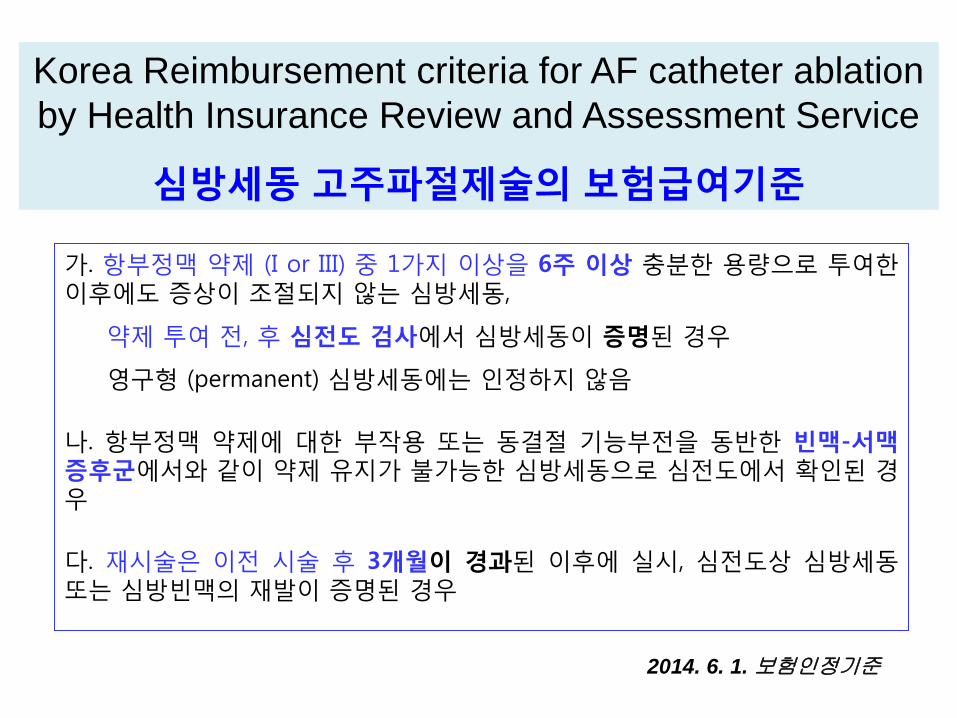
가. 항부정맥 약제 (I or III) 중 1가지 이상을 6주 이상 충분한 용량으로 투여한 이후에도 증상이 조절되지 않는 심방세동,
약제 투여 전, 후 심전도 검사에서 심방세동이 증명된 경우
영구형 (permanent) 심방세동에는 인정하지 않음
나. 항부정맥 약제에 대한 부작용 또는 동결절 기능부전을 동반한 빈맥-서맥 증후군에서와 같이 약제 유지가 불가능한 심방세동으로 심전도에서 확인된 경우
다. 재시술은 이전 시술 후 3개월이 경과된 이후에 실시, 심전도상 심방세동 또는 심방빈맥의 재발이 증명된 경우
Korea Reimbursement criteria for AF catheter ablation
by Health Insurance Review and Assessment Service
심방세동 고주파절제술의 보험급여기준
2014. 6. 1. 보험인정기준

Case 3
• 68 year-old gentleman
• Frequent dizziness with palpitation
• No functional decline
• Hypertension (+), DM (+)
• Medication of HTN and DM

1초
Tachycardia Bradycardia syndrome

CHA2DS2VASc score : 3
• Age 68 yrs
• HTN
• DM
HAS-BLED score : 2
• Age 68 yrs
• HTN
What treatment strategy would you choose?
1. Rate control strategy with anticoagulation
2. Rhythm control strategy
3. Rhythm control strategy with anticoagulation
4. Anticoagulation only
5. Pacemaker
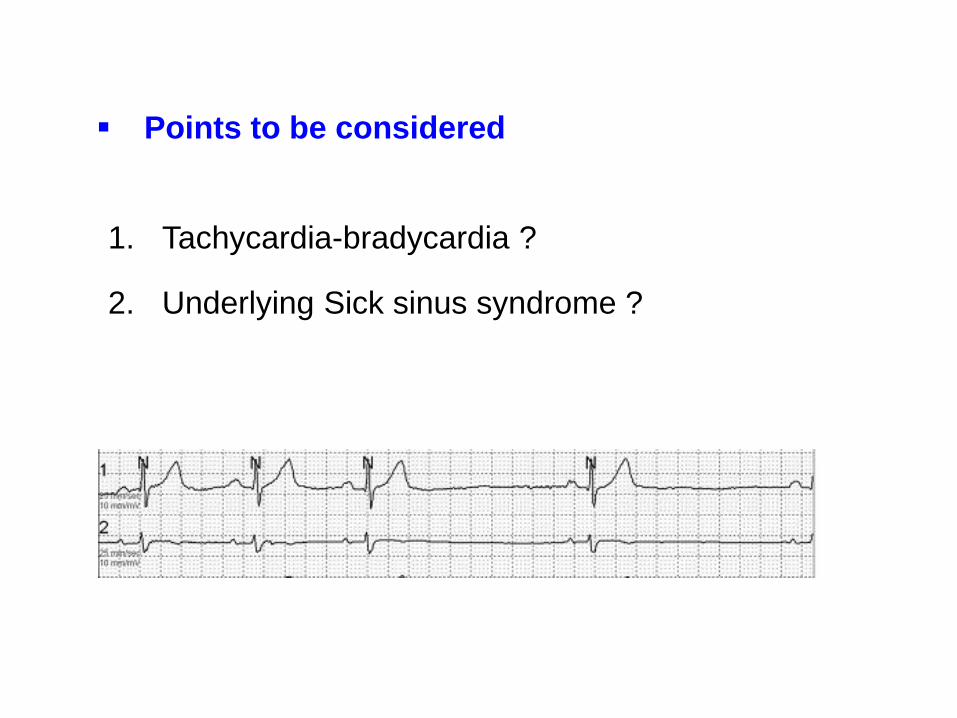
Points to be considered
1. Tachycardia-bradycardia ?
2. Underlying Sick sinus syndrome ?

What treatment strategy would you choose?
1. Rate control strategy with anticoagulation
2. Rhythm control strategy
3. Rhythm control strategy with anticoagulation
4. Anticoagulation only
5. Pacemaker

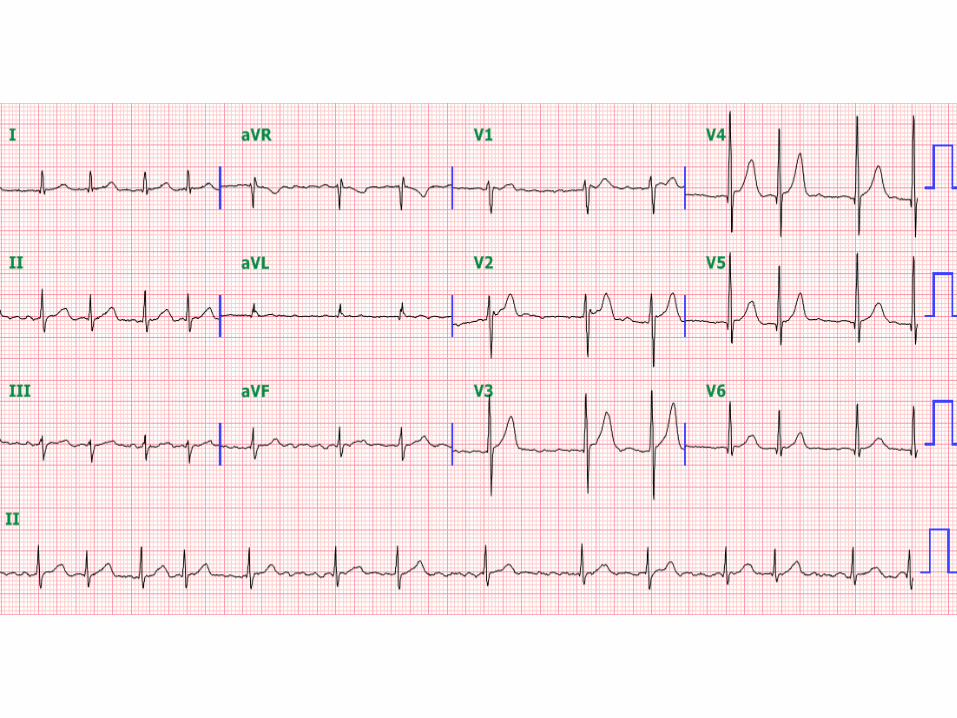
Case 4
• 65 year-old lady
• No specific symptom
• Detection of AF in ECG during routine health check up
• No functional decline
• Medication of beta blocker
• No underlying heart and other problem

Echocardiography
• LVEF 58% LVESD/EDD 33/51 mm
• LA 58 mm LAVI 45 ml/m2
• IVSd 10 mm, LVPWd 10 mm
• Normal LV and RV
• Valve : normal
• Great vessel : normal

What treatment strategy would you choose?
1. Rate control strategy
2. Rate control strategy with anticoagulation
3. Rhythm control strategy
4. Rhythm control strategy with anticoagulation
5. Anticoagulation only

Case 4 CHA2DS2VASc score : 2 • 65 years old (1)
• Female (1)
HAS-BLED score : 1
• 65 years old (1)

• Not an ideal candidate for AF ablation
: The patient has a more advanced form of AF.
There is little to be gained from a symptom perspective
AF ablation should not be performed for solely “curative”
purposes.
The predominant arrhythmia mechanism shifts from a focal
“trigger” in paroxysmal AF, to a reliance on an abnormal
anatomic substrate capable of arrhythmia self-perpetuation.
What treatment strategy would you choose?
1. Rate control strategy
2. Rate control strategy with anticoagulation
3. Rhythm control strategy
4. Rhythm control strategy with anticoagulation
5. Anticoagulation only
Summary
• The rate of ischemic stroke among patients with AF averages 5% per year.
• CHA2DS2-VASc score recommended to assess stroke risk.
• With prior stroke, TIA, or CHA2DS2-VASc score ≥ 2, oral anticoagulants
recommended. Warfarin or NOAC
• With nonvalvular AF and CHA2DS2-VASc score of 0, it is reasonable to
omit antithrombotic therapy.
• With AF or atrial flutter for ≥48 h, or unknown duration, anticoagulate with
warfarin for at least 3 weeks prior to and 4 weeks after cardioversion.
• Catheter ablation of AF : symptomatic AF refractory or intolerant to
antiarrhythmic medication