current management of community-acquired pneumonia a review
TRANSCRIPT
Current Management ofCommunity-acquired Pneumonia
A review
Mark Woodhead
Honorary Clinical Professor of Respiratory Medicine

• Background• Diagnosis• Severity assessment• Treatment – antibiotics• Treatment – flu• Treatment – Steroids• Treatment - NIV• Response to treatment• Safe Discharge


3.87. Pneumonia continues to place a huge burden on the NHS – improving our response will help to relieve the pressure, particularly during winter. • Community-acquired pneumonia is a
leading cause of admission to hospital, despite being avoidable in many cases.
• Pneumonia also disproportionally affects older people, with incidence doubling for those aged 85-95 compared with 65-69.
• For every degree drop in temperature below five degrees Celsius, there is a 10.5% increase in primary care respiratory consultations and a 0.8% increase in respiratory admissions.
• Acute pneumonia admissions have risen by 35% since 2013 with stays in hospitals getting shorter, indicating admission may not have always been essential.

www.nice.org.uk/guidance/cg191

• Background• Diagnosis• Severity assessment• Treatment – antibiotics• Treatment – flu• Treatment – Steroids• Treatment - NIV• Response to treatment• Safe Discharge

75 year old male
2 days fever and rigorsCough, purulent sputumRight pleuritic chest painCrackles and
bronchial breathing right lung

85 year old female
Residential homeGeneral deterioration 1/52BreathlessNew confusionBibasal crackles

77 year old male
Diabetes, Ischaemic HDCough and dyspnoeaBibasal crackles
?CAP, ?LVF

85 year old female
Residential homeGeneral deterioration 1/52BreathlessNew confusionBibasal crackles
CRP 110, WCC 8.4
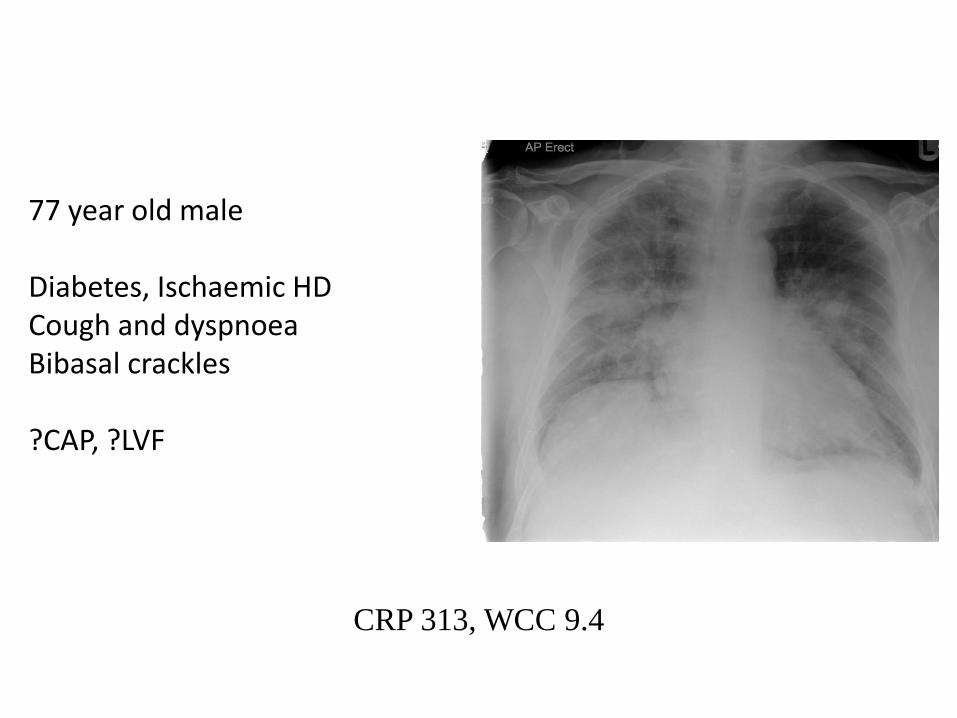
CRP 313, WCC 9.4
77 year old male
Diabetes, Ischaemic HDCough and dyspnoeaBibasal crackles
?CAP, ?LVF

CRP 313, WCC 9.4
(D-dimer, BNP and Troponin may all rise in CAP)
77 year old male
Diabetes, Ischaemic HDCough and dyspnoeaBibasal crackles
?CAP, ?LVF

Upchurch et al Chest 2017
Aug 9. pii: S0012-3692(17)31392-2. doi: 10.1016/j.chest.2017.07.035
• hospital length of stay,
• ICU admission,
• mechanical ventilation, and
• shock,
were similar between groups
• In-hospital death was rare in both the CT-only and
pneumonia on CXR groups (0% vs 2%).
CT CAP

• Background• Diagnosis• Severity assessment• Treatment – antibiotics• Treatment – flu• Treatment – Steroids• Treatment - NIV• Response to treatment• Safe Discharge

Severity Assessment
Prognostic value – predicts mortality
Assists in
• Place of care home/hospital/ICU
• Intensity of investigation
• Antibiotic therapy
• What to tell patient / family

11.7
23.4
0
5
10
15
20
25
Direct Delayed
Outcome related to ICU Transfer Mode
28-day mortality %
Renaud et al Crit Care Med 2009;37:2867-2874
Direct = straight from EDDelayed = within 3 days of admission
Severity Assessment

Mortality (%) related to CURB-65 score
0
5
10
15
20
25
30
35
0 or 1 Two 3 or more
CURB-65 score
CRB65
ATS/IDSA
1.5%
mortality
9.2%
Lim et al Thorax 2003;58:377-382, Fine et al NEJM 1997;336:243-250
1.5%
9.2%
22%

Severity assessment in hospital
• Use clinical judgement in conjunction with the CURB65 score to guide the management of community-acquired pneumonia, as follows:
• consider home-based care for patients with a CURB65 score of 0 or 1• consider hospital-based care for patients with a CURB65 score of 2 or
more• consider intensive care assessment for patients with a CURB65 score of 3
or more.[Based on prognostic cohort studies of moderate to very low quality with a large number of patients, and the experience and opinion of the GDG]
• Stratify patients presenting with community-acquired pneumonia into those with low-, moderate- or high-severity disease. The grade of severity will usually correspond to the risk of death.
[Based on the experience and opinion of the GDG]
www.nice.org.uk/guidance/cg191

Low intermediate High Low intermediate High
CRB65 CURB65
Pneumonia Patient Distribution by Mortality Risk Score
Lim et al Thorax 2003;58:377-382
n = 718
1.2% 8.1% 31% 1.5% 9.2% 22%
**

Low intermediate High Low intermediate High
CRB65 CURB65
Antibiotic Choice by Mortality Risk Score
Lim et al Thorax 2003;58:377-382
n = 718
1.2% 8.1% 31% 1.5% 9.2% 22%
**
AmoxicillinB-lactam + macrolideB-lactam + macrolide

• Background• Diagnosis• Severity assessment• Treatment – antibiotics• Treatment – flu• Treatment – Steroids• Treatment - NIV• Response to treatment• Safe Discharge

• Offer a 5-day course of a single antibiotic to patients with low-severity community-acquired pneumonia.
• Consider amoxicillin in preference to a macrolide or a tetracycline.
www.nice.org.uk/guidance/cg191

• Offer a 5-day course of a single antibiotic to patients with low-severity community-acquired pneumonia.
• Consider amoxicillin in preference to a macrolide or a tetracycline.
• Consider dual antibiotic therapy with amoxicillin and a macrolide for patients with moderate-severity community-acquired pneumonia.
• Consider dual antibiotic therapy with a beta-lactamase stable beta-lactam and a macrolide for patients with high-severity community-acquired pneumonia.
www.nice.org.uk/guidance/cg191

Horita et al Respirology 2016;21:1193-1200
FavoursBL + ML
FavoursBL alone
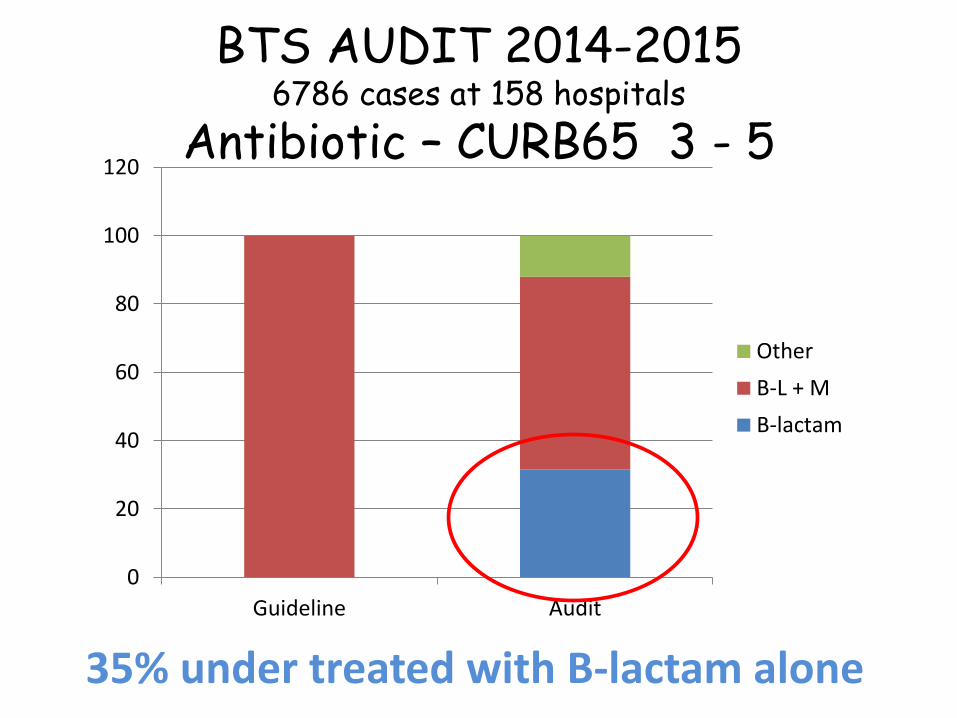
BTS AUDIT 2014-20156786 cases at 158 hospitals
Antibiotic – CURB65 3 - 5
0
20
40
60
80
100
120
Guideline Audit
Other
B-L + M
B-lactam
35% under treated with B-lactam alone

Timely diagnosis and treatment
• Put in place processes to allow diagnosis (including X-rays) and treatment of community-acquired pneumonia within 4 hours of presentation to hospital.
• Offer antibiotic therapy as soon as possible after diagnosis, and certainly within 4 hours to all patients with community-acquired pneumonia who are admitted to hospital.
[Based on observational cohort studies of low to very low quality with a large number of patients]
www.nice.org.uk/guidance/cg191

Time to first antibiotic (hours)
first antibiotic dose within 4 h of admission was associated
with a 16% lower adjusted 30-day IP
mortality compared with later antibiotic administration
Time to First Antibiotic
Daniel P, et al. Thorax 2016 Jun;71(6):568-70
< 4 4-8 8-12 >12
n = 23,315

16
17
18
19
20
2009 2010 2011 2012 2014
0
20
40
60
80
2009 2010 2011 2012 2014
%
30-day mortality
CURB-65 3 - 5
Antibiotic within 4 hours
OR (AOR) for mortality from 2009 (reference) to 2014
AOR 0.86 (95% CI 0.68 to 1.08)
p for trend=0.004
24,187 cases in 218 hospitals
Daniel P, et al. Thorax 2016;71:1061–1063
24
26
28
30
32
2009 2010 2011 2012 2014

• Offer a 5-day course of a single antibiotic to patients with low-severity community-acquired pneumonia.
• Consider amoxicillin in preference to a macrolide or a tetracycline.
www.nice.org.uk/guidance/cg191

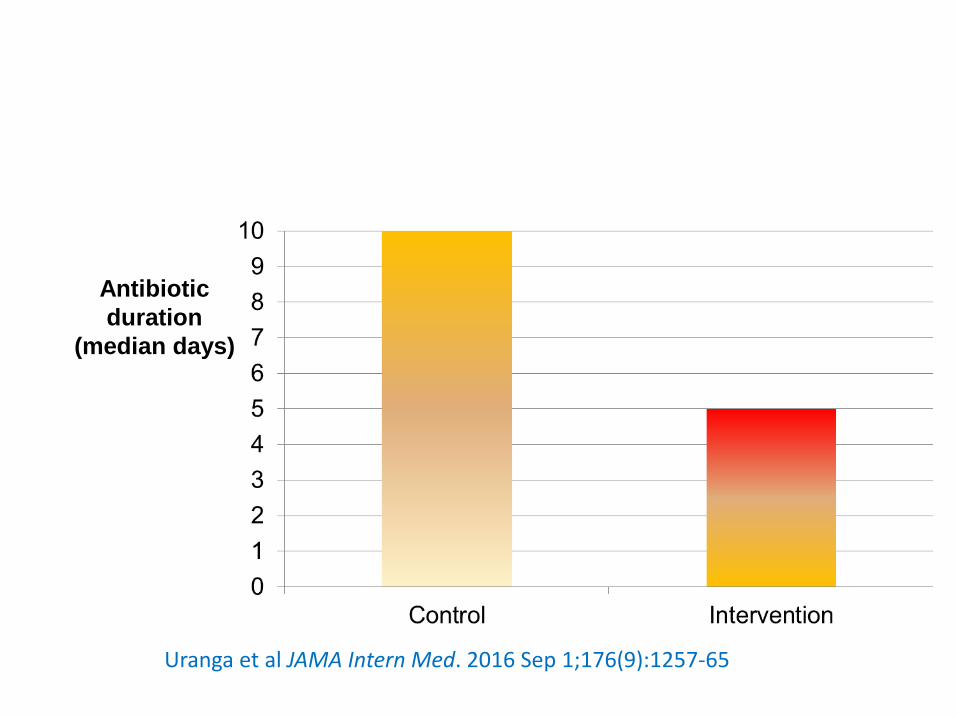
• Multicentre, non-inferiority randomized clinical trial • Hospitalized patients diagnosed as having CAP 4 teaching hospitals in Spain
control group duration of antibiotics was determined by physicians as usual in clinical practice.
Uranga et al JAMA Intern Med. 2016 Sep 1;176(9):1257-65
Usual Antibiotic
intervention group
treated with antibiotics for minimum 5 days,
stopped at this point if temperature was ≤ 37.8°C
for 48 hours and ≤ than 1 clinical instability,
Admission Day 5
Randomised
Antibiotic
duration
(median days)
Uranga et al JAMA Intern Med. 2016 Sep 1;176(9):1257-65

Antibiotic
duration
(median days)
Uranga et al JAMA Intern Med. 2016 Sep 1;176(9):1257-65
n 150 162 p
30-day mortality (%) 2.2 2.1 NS
Day 10 clinical success(%) 48.6 56.3 .18
Day 30 clinical success(%) 88.6 91.9 .33
Day 10 Mean symptom score 18.6 17.9 .69

Low-severity community-acquired pneumonia
• Offer a 5-day course of a single antibiotic to patients with low-severity community-acquired pneumonia.
[Based on moderate to very low quality evidence from randomised controlled trials, a cost analysis with limitations, and the experience and opinion of the GDG]
Moderate- and high-severity community-acquired pneumonia
• Consider a 7- to 10-day course of antibiotic therapy for patients with moderate- or high-severity community-acquired pneumonia.
[Based on the experience and opinion of the GDG]
www.nice.org.uk/guidance/cg191

• Background• Diagnosis• Severity assessment• Treatment – antibiotics• Treatment – flu• Treatment – Steroids• Treatment - NIV• Response to treatment• Safe Discharge

Oseltamivir and zanamivir cause small reductions in the time to first alleviation of influenza symptoms in adults. The use of oseltamivir increases the risk of nausea, vomiting, psychiatric events in adults and vomiting in children.
Oseltamivir has no protective effect on mortality among patients with 2009A/H1N1 influenza.
Prophylaxis with either NI may reduce symptomatic influenza in individuals and inhouseholds.
The balance between benefits and harms should be considered when making decisions about use of NIs for either prophylaxis or treatment of influenza.
Heneghan CJ, et al Health Technol Assess 2016;20(42)

Compared with no treatment, neuraminidase inhibitor treatment (irrespective of timing) was associated with a reduction in mortality risk (adjusted odds ratio [OR] 0·81; 95% CI 0·70–0·93; p=0·0024).
Compared with later treatment, early treatment (within 2 days of symptom onset) was associated with a reduction in mortality risk (adjusted OR 0·48; 95% CI 0·41–0·56; p<0·0001).
There was an increase in the mortality hazard rate with each day’s delay ininitiation of treatment up to day 5 as compared with treatment initiated within 2 days of symptom onset (adjusted hazard ratio [HR 1·23] [95% CI 1·18–1·28]; p<0·0001 for the increasing HR with each day’s delay)
Muthuri et al Lancet Respir Med 2014;2: 395–404

Neuraminidase Inhibitors for Influenza
High quality evidence suggests they are ineffective……….
in the mainly young, fit and healthy
Low quality evidence suggests benefit……….
in more severely ill cases

• Background• Diagnosis• Severity assessment• Treatment – antibiotics• Treatment – flu• Treatment – Steroids• Treatment - NIV• Response to treatment• Safe Discharge


Meta-analyses
Salluh 2010
Nie 2012
Siemieniuk 2015
Horita 2015
Chen 2015
Marti 2015
Wan 2016
Bi 2016
Wu 2018
Briel 2018
Original Studies
Wagner 1955
Bennett 1963
Klastersky 1971
McHardy 1972
Marik 1993
Confalonieri 2005
El Ghamrawy 2006
Mikami 2007
Snijders 2010
Fernandez-Serano 2011
Meijvis 2011
Sabry 2011
Nafae 2013
Blum 2015
Torres 2015
Steroid Treatment for CAP

Two New RCTs in Sepsis…..

Among patients with septic shock undergoing mechanical
ventilation, a continuous infusion of hydrocortisone did not
result in lower 90-day mortality than placebo
35% of 3698 cases had pulmonary infection
Mortality 28%
Venkatesh et al N Engl J Med 2018;378:797-808
….90-day all-cause mortality was lower among those
who received hydrocortisone plus fludrocortisone than
among those who received placebo
59% of 1240 cases had pulmonary infection
Mortality 45%
Annane et al N Engl J Med 2018;378:378:809-818
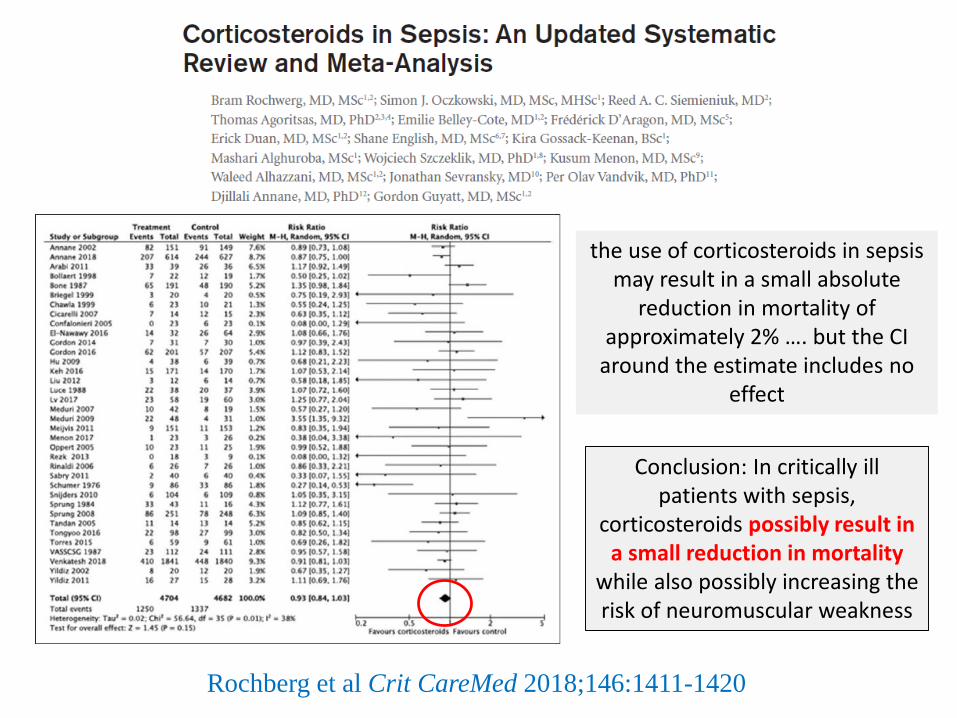
Rochberg et al Crit CareMed 2018;146:1411-1420
Conclusion: In critically ill patients with sepsis,
corticosteroids possibly result in a small reduction in mortality
while also possibly increasing the risk of neuromuscular weakness
the use of corticosteroids in sepsis may result in a small absolute
reduction in mortality of approximately 2% …. but the CI
around the estimate includes no effect

Our panel make a weak recommendation to give corticosteroids to people with all types
and severity of sepsis, based on new evidence.
Because we are not certain that they are beneficial, it is also reasonable not to prescribe
them.
Patients’ values and preferences may guide this decision-making process.
Lamontagne et al Brit Med J 2018; 362:k3284 doi: 10.1136/bmj.k3284

0
10
20
30
40
50
60
70
80
90
100
No Sepsis
Sepsis
Sepsis in Community-acquired Pneumonia
Prospectively collected cohort of 6874 adult CAP cases
Sepsis present if QSOFA ≥ 2
Ranzani et al Am J Respir Crit Care Med Vol 196, Iss 10, pp 1287–1297
%

• Background• Diagnosis• Severity assessment• Treatment – antibiotics• Treatment – flu• Treatment – Steroids• Treatment - NIV• Response to treatment• Safe Discharge
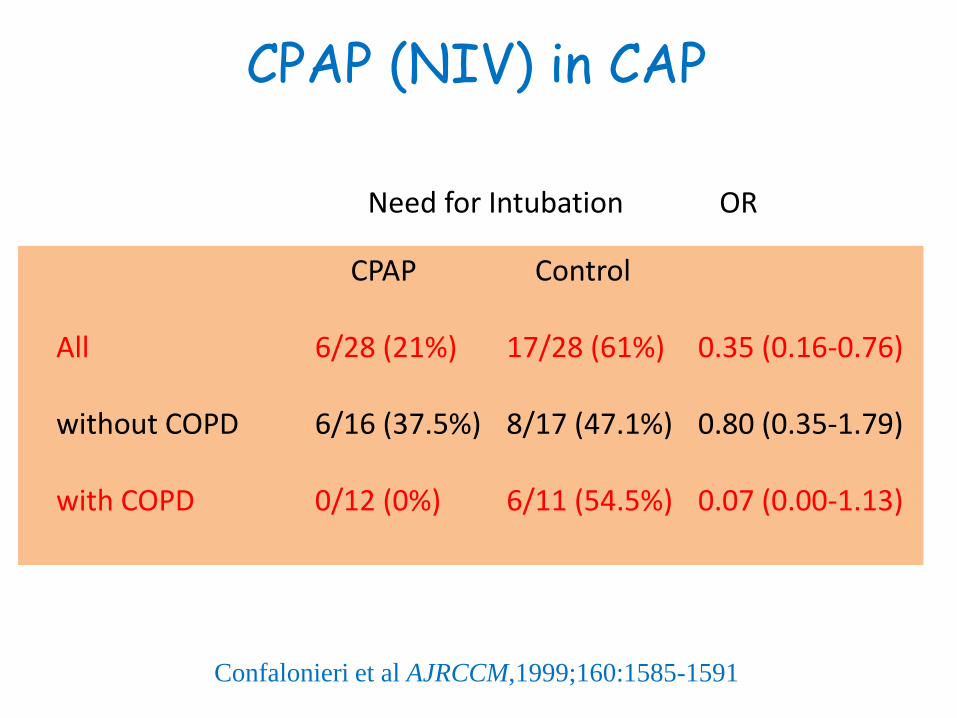
CPAP (NIV) in CAP
Confalonieri et al AJRCCM,1999;160:1585-1591
CPAP Control
All 6/28 (21%) 17/28 (61%) 0.35 (0.16-0.76)
without COPD 6/16 (37.5%) 8/17 (47.1%) 0.80 (0.35-1.79)
with COPD 0/12 (0%) 6/11 (54.5%) 0.07 (0.00-1.13)
Need for Intubation OR

• Background• Diagnosis• Severity assessment• Treatment – antibiotics• Treatment – flu• Treatment – Steroids• Treatment - NIV• Response to treatment• Safe Discharge

A CRP that fails to fall by 50% or more within 4 days of admission is
independently associated with
increased 30 day mortality (OR 24.5; 6.4-93.4), P .0001;
mechanical ventilation and/or inotropic support (OR 7.1; 2.8-17.8), P .0001
and complicated pneumonia (OR 15.4; 6.32-37.6), P .0001.
REPEAT CRP WITHIN 4 DAYS OF ADMISSION
Chalmers et al Am J Med 2008;121:219-225
0
5
10
15
20
25
30 d mortality AV / inotropes complications
Day 4 CRP decreased by >49%
Day 4 CRP decreased by < 50%
%

Monitoring in hospital
• Consider measuring a baseline C-reactive protein concentration in patients with community-acquired pneumonia on admission to hospital, and repeat the test if clinical progress is uncertain after 48 to 72 hours.
[Based on low to very low quality observational cohort studies, and the experience and opinion of the GDG]
www.nice.org.uk/guidance/cg191

3.87. Pneumonia continues to place a huge burden on the NHS – improving our response will help to relieve the pressure, particularly during winter. • Community-acquired pneumonia is a
leading cause of admission to hospital, despite being avoidable in many cases.
• Pneumonia also disproportionally affects older people, with incidence doubling for those aged 85-95 compared with 65-69.
• For every degree drop in temperature below five degrees Celsius, there is a 10.5% increase in primary care respiratory consultations and a 0.8% increase in respiratory admissions.
• Acute pneumonia admissions have risen by 35% since 2013 with stays in hospitals getting shorter, indicating admission may not have always been essential.

36
38
40
42
44
46
48
2009 2010 2011 2012 2014
3.87. Pneumonia continues to place a huge burden on the NHS – improving our response will help to relieve the pressure, particularly during winter. • Community-acquired pneumonia is a
leading cause of admission to hospital, despite being avoidable in many cases.
• Pneumonia also disproportionally affects older people, with incidence doubling for those aged 85-95 compared with 65-69.
• For every degree drop in temperature below five degrees Celsius, there is a 10.5% increase in primary care respiratory consultations and a 0.8% increase in respiratory admissions.
• Acute pneumonia admissions have risen by 35% since 2013 with stays in hospitals getting shorter, indicating admission may not have always been essential.
CURB-65 0 - 1
Daniel P, et al. Thorax 2016;71:1061–1063
CURB-65 3 - 5
24
26
28
30
32
2009 2010 2011 2012 2014

• Background• Diagnosis• Severity assessment• Treatment – antibiotics• Treatment – flu• Treatment – Steroids• Treatment - NIV• Response to treatment• Safe Discharge

3.87. Pneumonia continues to place a huge burden on the NHS – improving our response will help to relieve the pressure, particularly during winter.
• Consistent use and application of risk scoring for deteriorating patients may reduce avoidable admissions to hospital.
• Patients identified with community acquired pneumonia in emergency departments will be supported to be cared for safely out of hospital by receiving nurse-led supported discharge services, as set out in Chapter One.

Instabilities
Temp > 37.8
Resp Rate > 24/min
Heart Rate > 100/min
SBP ≤ 90
SaO2 < 90%
Altered mental status
Can’t maintain oral intake
PREDICTION OF SAFE HOSPITAL DISCHARGE IN CAP
N = 680
130 (19%) 1 instability
at discharge
0
10
20
30
40
50
60
Mor
talit
y
Rea
dmission
s
Major
Eve
nts
not B
TN
0 1 2
No of
instabilities
Halm et al Arch Int Med 2002;162:1278-1284

Safe discharge from hospital
• Do not routinely discharge patients with community-acquired pneumonia if in the past 24 hours they have had 2 or more of the following findings:• temperature higher than 37.5°C• respiratory rate 24 breaths per minute or more• heart rate over 100 beats per minute• systolic blood pressure 90 mmHg or less• oxygen saturation under 90% on room air• abnormal mental status• inability to eat without assistance.
• Consider delaying discharge if their temperature is higher than 37.5°C.[Based on evidence from moderate to very low quality prognostic cohort studies at low risk of bias]
www.nice.org.uk/guidance/cg191

• CRP may help if diagnosis uncertain• Severity assessment by clinical judgement + CURB65• Amoxicillin for non-severe• B-lactam + macrolide for moderate or severe• 5 days adequate for non-severe• Neuraminidase inhibitors in seasonal flu outbreak• Steroids at best minimal effect• NIV in place of safety• Repeat CRP if uncertain clinical response• Don’t discharge if >1 instability marker present
Current Management ofCommunity-acquired Pneumonia
A review