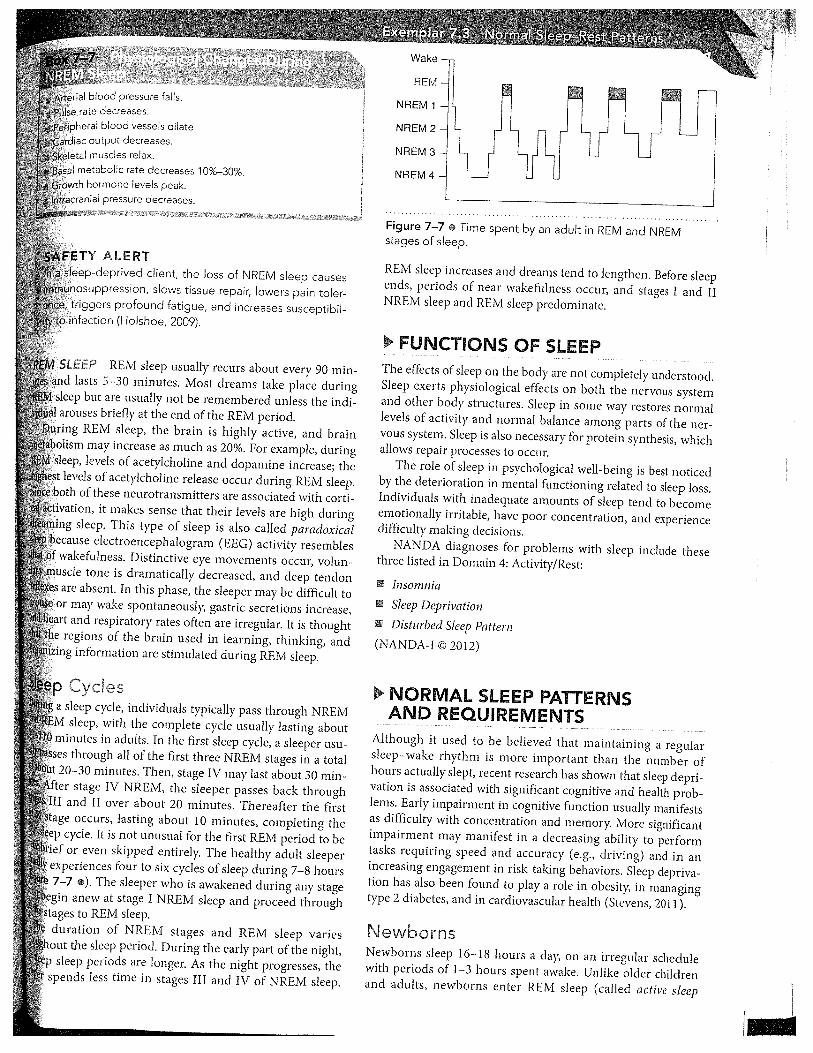
curriculum concepts handbook
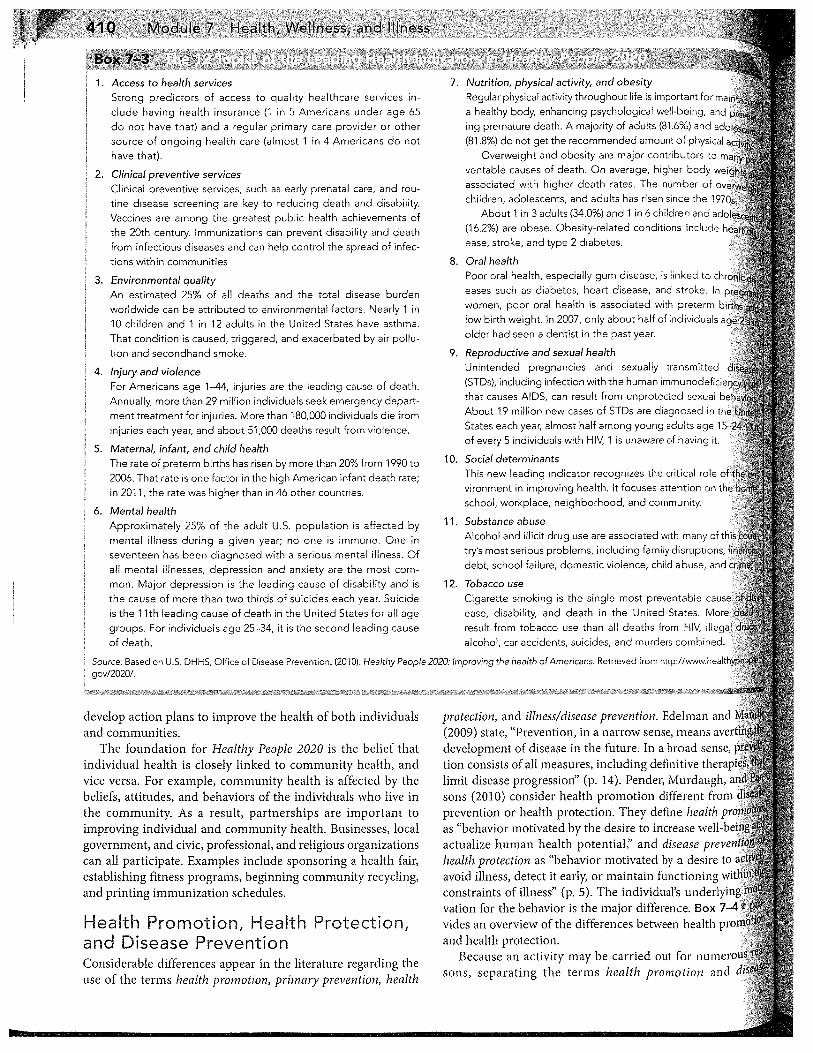
TRANSCRIPT
College of Nursing
The Curriculum Concepts handbook is made in accordance with the University of Manitoba’s Fair Dealing Policy for use by students enrolled in the course of study for which it was made. The handbook may also include copyright-protected material pursuant to permissions granted by the copyright holder. Any reproduction or other use of this material is strictly forbidden.
CURRICULUM CONCEPTS
A Handbook
Health & Illness
Client & Context
Professional Foundation
Page | 2
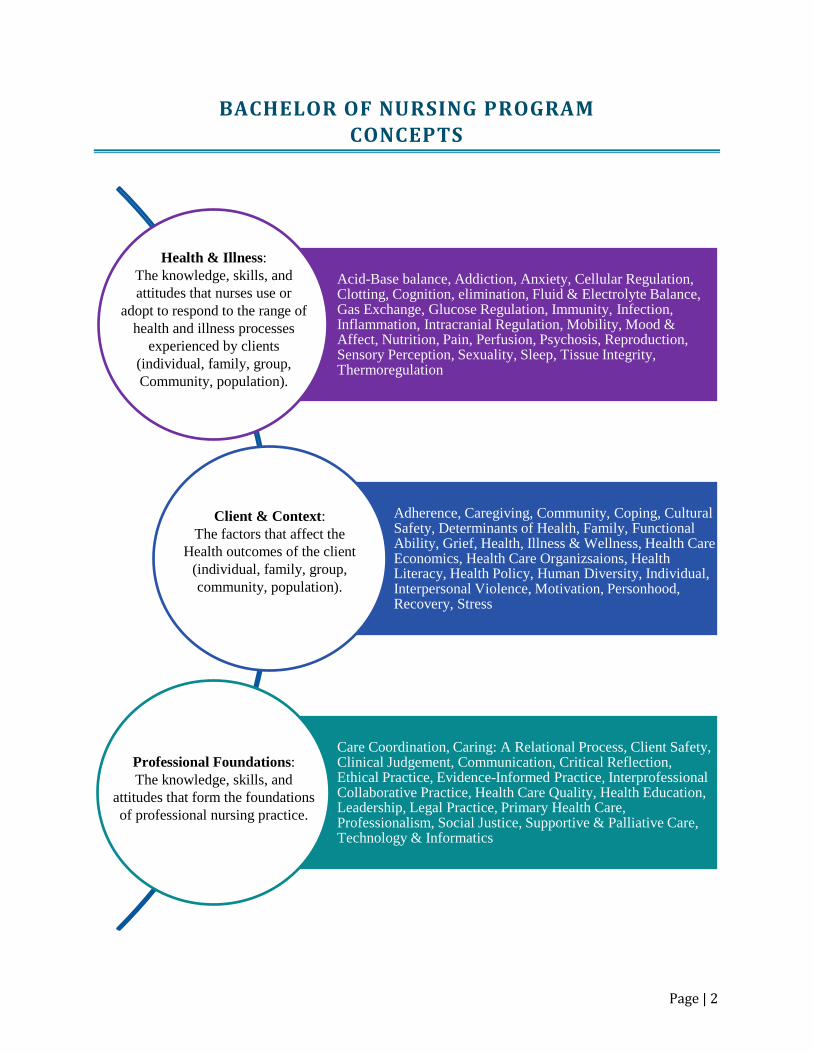
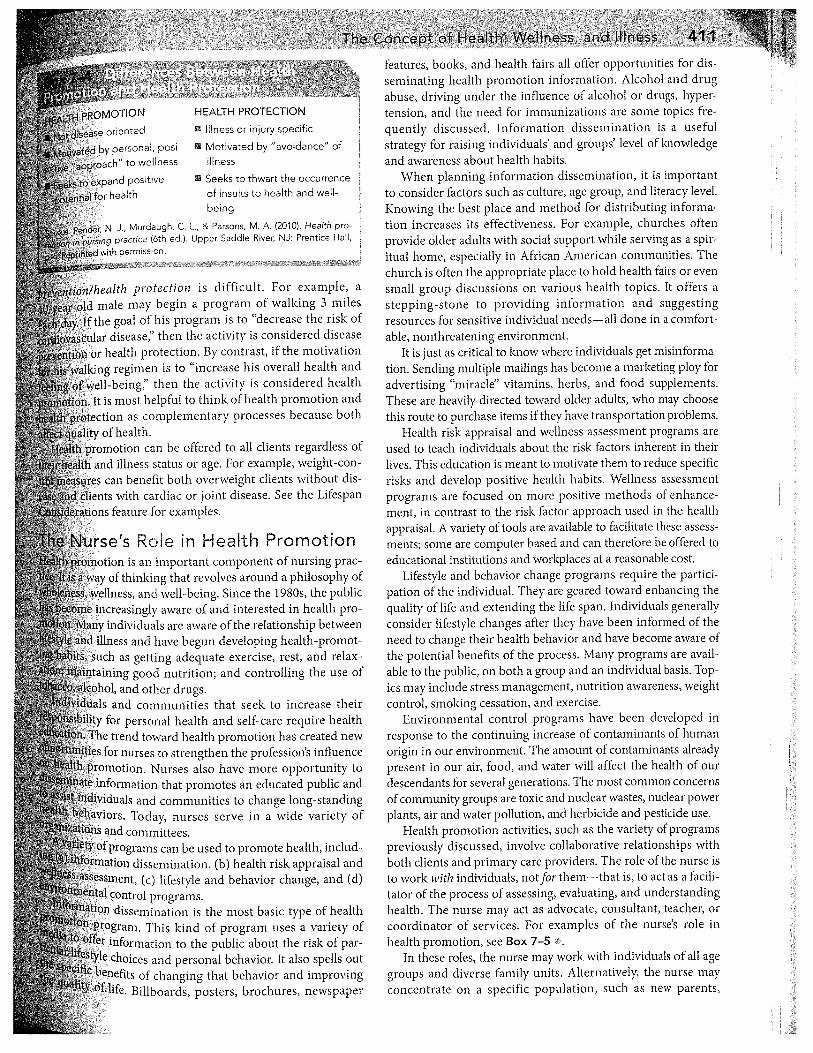
BACHELOR OF NURSING PROGRAM CONCEPTS
Acid-Base balance, Addiction, Anxiety, Cellular Regulation, Clotting, Cognition, elimination, Fluid & Electrolyte Balance, Gas Exchange, Glucose Regulation, Immunity, Infection, Inflammation, Intracranial Regulation, Mobility, Mood & Affect, Nutrition, Pain, Perfusion, Psychosis, Reproduction, Sensory Perception, Sexuality, Sleep, Tissue Integrity, Thermoregulation
Adherence, Caregiving, Community, Coping, Cultural Safety, Determinants of Health, Family, Functional Ability, Grief, Health, Illness & Wellness, Health Care Economics, Health Care Organizsaions, Health Literacy, Health Policy, Human Diversity, Individual, Interpersonal Violence, Motivation, Personhood, Recovery, Stress
Care Coordination, Caring: A Relational Process, Client Safety, Clinical Judgement, Communication, Critical Reflection, Ethical Practice, Evidence-Informed Practice, Interprofessional Collaborative Practice, Health Care Quality, Health Education, Leadership, Legal Practice, Primary Health Care, Professionalism, Social Justice, Supportive & Palliative Care, Technology & Informatics
Health & Illness: The knowledge, skills, and attitudes that nurses use or
adopt to respond to the range of health and illness processes
experienced by clients (individual, family, group, Community, population).
Client & Context: The factors that affect the
Health outcomes of the client (individual, family, group, community, population).
Professional Foundations: The knowledge, skills, and
attitudes that form the foundations of professional nursing practice.
Page | 3
HEALTH AND ILLNESS The knowledge, skills and attitudes that nurses use or adopt to respond to the range of health and illness processes experienced by clients (individual, family, group, community, population).
Resources from Giddens Acid-Base Balance Addiction Anxiety Cellular Regulation Clotting Cognition Elimination Fluid & Electrolyte Balance Gas Exchange Glucose Regulation Immunity Infection Inflammation Intracranial Regulation Mobility Mood and Affect Nutrition Pain Perfusion Psychosis Reproduction Sensory Perception Sexuality Sleep Tissue Integrity Thermoregulation
Page | 4
CLIENT AND CONTEXT The factors that affect the health outcomes of the client (individual, family, group, community, population).
Resources from Giddens Adherence Caregiving Coping Family (see Giddens: Family Dynamics) Functional Ability Individual (see Giddens: Development) Interpersonal Violence (see Giddens: Safety) Motivation Stress
Resources from Other Sources Cultural Safety National Aboriginal Health Organization (2006). Fact sheet: Cultural safety. Retrieved from
http://www.naho.ca/documents/naho/english/Culturalsafetyfactsheet.pdf Determinants of Health Reutter, L., & Kuschner, K. (2014). Health and wellness. In P. Potter, & A. Perry (Eds.), Canadian
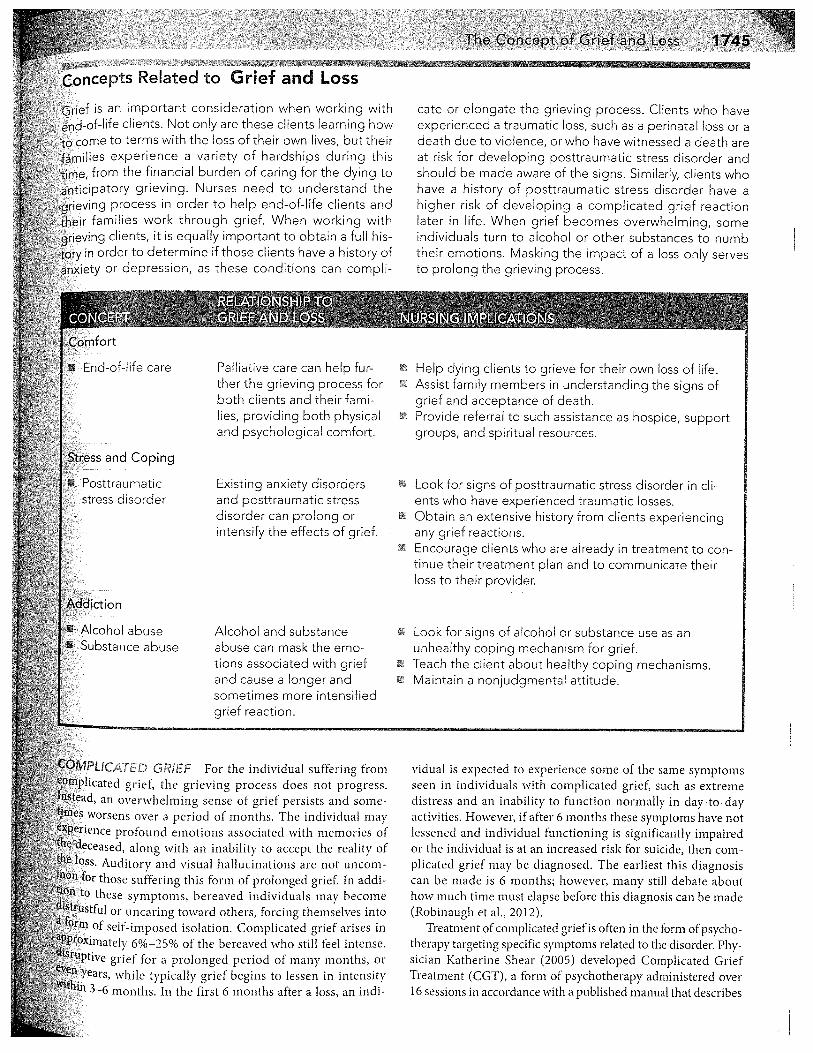
fundamentals of nursing (5th ed.) (pp. 1-14). Toronto: Elsevier Canada. Students have this textbook, so the chapter is not reproduced here. Grief: Pearson, (2015). Grief and loss. Nursing: A concept-based approach to learning, Vol. 2 (pp. 1741-
1773). Upper Saddle River, NJ: Pearson
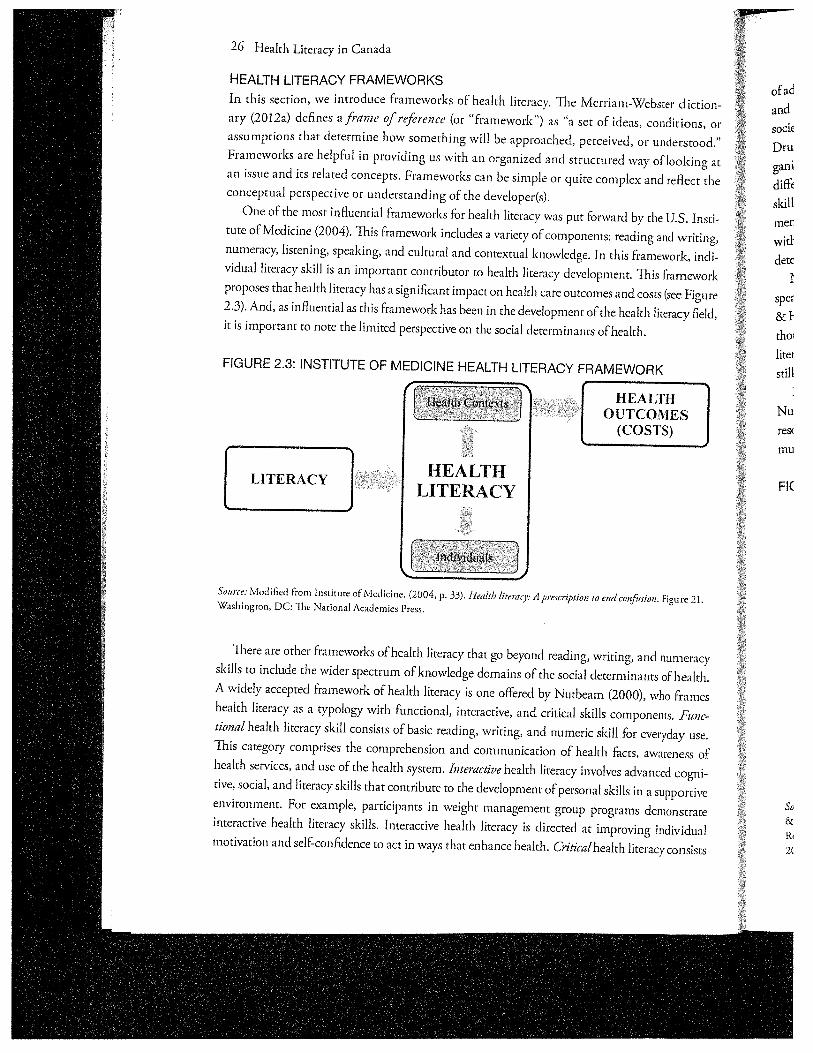
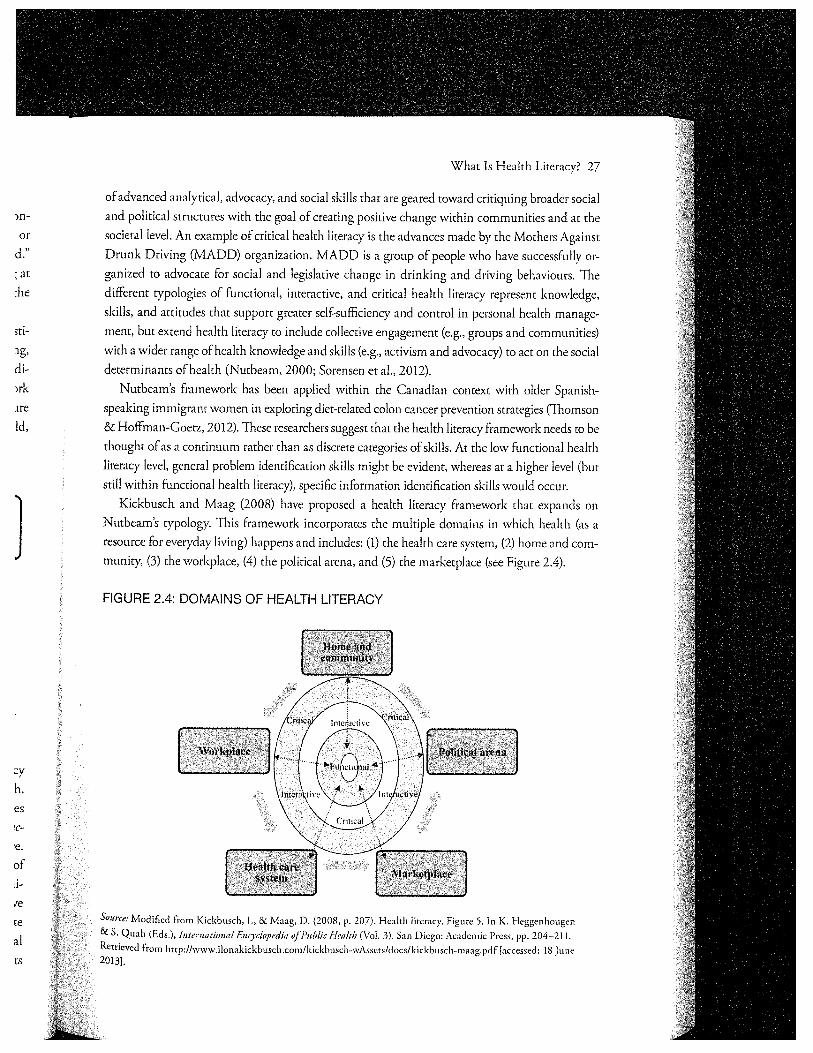
Health Literacy: Hoffman-Goetz, L., Donelle, L, & Ahmed, R. (2014). What is health literacy? Health literacy in
Canada: A primer for students. Toronto, ON: Canadian Scholars Press, pp. 15-38. Human Diversity North Carolina Concept-Based Learning Editorial Board (2011). Diversity. In Nursing: A Concept-
Based Approach to Learning. Upper Saddle River, New Jersey: Pearson, pp. 397-407. Recovery: Brennaman, L., & Lobo, M. (2011). Recovery from serious mental illness: A concept analysis. Issues
in mental health nursing, 32, p. 654-663. Retrieved from:
http://web.a.ebscohost.com.uml.idm.oclc.org/ehost/detail/detail?vid=5&sid=5a57c24a-9015-
Page | 5
48b1-a2bf1d09cdbbe5d6%40sessionmgr4009&hid=4206&bdata=JnNpdGU9ZWhvc3QtbGl2ZQ%3d%3d#AN=65552957&db=a9h
Resources Developed by the College of Nursing
Community Health Care Economics Health Care Organizations Health Policy Personhood

Page | 6
PERSONHOOD
MCKAY, M., ASHCROFT, T., GUSE, L., HARWOOD, R., & JENSEN, F.
Personhood is a complex concept that straddles diverse and conflicting religious, ethical and legal opinions and arguments. Conceptions of personhood are also deeply influenced by cultural beliefs. Even within Western culture, complex philosophical, theological, ethical and legal debates have resulted in a range of definitions of personhood. Understanding the concept of Personhood is important because the designation of the status of person upon a living entity “confers status, respect, and moral worth” (Ohlin, 2005, p. 211). The most straightforward definition of personhood is the state of being an individual who possesses human characteristics or traits. Dewing (2008), for example, defines personhood as the attributes possessed by human beings that make them persons. Naffine (2004) defines a person as a “separate and distinct being who bears rights and duties” (p. 119). However, there is no consensus regarding how personhood should be defined. DEFINITION(S) Kitwood (1997) defines personhood as “a standing or status that is bestowed upon one human being, by others, in the context of relationship and social being. It implies recognition, respect and trust” (p. 8). This definition, which creates a relationship between the person and another, often a caregiver, provides an appropriate starting point for professional nurses to explore this complex concept.
SCOPE, TYPE OR CATEGORY(S) Scholarly literature on the subject of personhood identifies a number of types of persons, including: “partial persons (children), potential persons (fetuses and embryos), past persons (brain-dead patients), almost persons (animals), irrational persons (persons living with, for example, multiple personality disorder), and group persons (corporations and nation-states)” (Ohlin, 2005, p. 213). In the case of professional health care practice, personhood is an attribute of human beings. Therefore, for the purposes of professional nursing practice, the scope of the concept of personhood is humans, and would not consider the personhood of animals, corporations or nation-states. ATTRIBUTES Many attributes have been used to define or describe personhood. Although controversial, the most fundamental attribute of personhood is being human; that is a member of the species Homo sapiens. However, for reasons which will be discussed later in this document, simply being human has rarely been accepted, either historically or currently, as the sole attribute of personhood. A number of other attributes have been proposed. These attributes tend to fall into two general categories: cognitive and relational. The attributes of personhood are culturally contingent in that they represent predominately Western thinking about the idea of personhood. As well, they emerge out of an intellectual (Cartesian) tradition that separates the mind and body and views the
Page | 7
mind and spirit as more human than the body (Dewing, 2008). Within this tradition, the attributes of personhood include the actual possession of or the potential to possess cognitive and relational capacities such as those listed below. Cognitive • Consciousness/self-consciousness/self-
awareness (Buron, 2008; Ohlin, 2005; Quintan, 1973; Taylor, 1985, Warren, 1973)
• Morality (Naffine, 2004; Quintan, 1973) • Rationality/Reasoning (Flynn & Arstein-
Kerslake, 2014; Naffine, 2004; Quintan, 1973; Warren, 1973)
• Agency (Harre, 1998; Flynn & Arstein-Kerslake, 2014; Kitwood & Bredin, 1992; Ohlin, 2005; Quintan, 1973; Taylor, 1985, Warren, 1973)
• Possessing rights and responsibilities (Naffine, 2004; Taylor, 1985)
• A sense of personal distinctiveness and continuity (Harre, 1998)
• Achievement of full potential (Maslow, 1970; Rogers, 1980)
• Capacity to communicate (Warren, 1973) Relational • Social relationships (Kitwood & Bredin,
1992; Quintan, 1973) THEORY It is beyond the scope of this document to explore all definitions of personhood or to fully explore the assumptions underlying these definitions. Rather, this concept analysis seeks to create an awareness of selected theories of personhood because these approaches may inform professional nursing practice and the manner in which nurses engage with clients in the health care setting.
Personhood as an inherent attribute of humans The earliest definitions of personhood come out of the Judeo-Christian beliefs about humans as a special creation of God. Because humans (Homo sapiens) were believed to have been made in the image of God, only humans could be persons (Harvard Law Review Editors, 2001; Holdron, 2013; Sullivan, 2001). This approach to the idea of personhood asserts that personhood begins at conception and ends with death (Sullivan, 2001, White, 2013). During the Enlightenment (18th century), and the emergence of secular society, this once unquestioned belief came under increasing scrutiny. Darwin’s assertion that differences between the species were differences of degree, not kind, further eroded the belief that personhood is exclusively an attribute of humans (Holdron, 2013). It can no longer be assumed to be the predominant way of conceptualizing personhood. Personhood as cognitive or relational capacity Theories of personhood as capacity are socially constructed (Harvard Law Review Editors, 2001; Kadlac, 2010; Roháĕ, 2010). They are therefore contested, evolving, and limited to the specific society defining personhood for their purposes. The shift from the idea of personhood as an essential state of all humans conferred by a higher being to a contingent state defined by society (and not necessarily confined to humans) has accelerated over the past fifty years. The destabilization of the idea of personhood as an inherent attribute of all humans can be attributed to many social

Page | 8
developments, including a shift in bioethics from a religious to a secular discipline (Sullivan, 2001), the emergence of cognition as the defining attribute of personhood (Farah & Heberlein, 2007; Flynn & Arstein-Kerslake, 2014), debates about abortion (Cox, 2011; Saurette & Gordon, 2013; Sullivan, 2001), increased uncertainty about when life actually begins and ends (Farah & Heberlein, 2007; Perry, 2001; Sullivan, 2001), the rise of modern medical technologies (Farah & Heberlein, 2007; Sullivan, 2001), and the animal rights movement (Holdron, 2013; Sullivan, 2001). Capacity-based conceptualizations of personhood specify the attributes associated with being a person (Farah & Heberlein, 2007; Kadlac, 2010, Perry, 2011; Redwin, 2006). Although there is no consensus about the attributes proposed by a variety of philosophers and ethicists, they can be divided into two major categories: cognitive and relational. Overwhelmingly, cognitive attributes are posited as being essential to the state of being a person. Unfortunately, the attributes-based approach to the concept of personhood has created two problems. The first, which will not be further considered in this document, is that there may be non-human species that could, by virtue of their intelligence, ability to communicate, and capacity to have relationships with others (including humans), be defined as persons (Holdron, 2013). The second is that there may be humans who could not, because of significant temporary or permanent impairment of their cognitive or relational capacity, be defined as persons (Harvard Law Review Editors, 2001; Naffine, 2003). Arneil (2009), for example, asserts that the advent of capacity-based definitions
of personhood has eroded the personhood of the disabled, who were historically defined as persons by virtue of their being human and therefore made in the image of God. Other writers have argued that the same problem exists for the mentally ill (Redwin, 2006) and the profoundly cognitively impaired (Silvers & Francis, 2009). Recognizing that personhood is a product of social relationships, Silvers and Francis (2009) argue that being born cognitively impaired is analogous to a social stillbirth. Further, because the disabled, the mentally ill and the profoundly cognitively impaired are frequently relegated to the margins of society, conceptions of their personhood, or lack thereof, are constructed by those in positions of power without regard for their needs, preferences or opinions (Silvers & Francis, 2009). In response to the problems associated with attributes-based conceptualizations of personhood, some theorists have proposed that there is a social obligation on the part of those who are recognized as persons to act on behalf of those whose personhood may be viewed as uncertain. For example, in the case of those living with dementia, Thomas Kitwood asserts that the provision of care that sustains the value and dignity of those who no longer have the capacity for conscious experience is an important component of health care (Perry, 2011). In this conceptualization of personhood, the onus rests with the caregiver to uphold the personhood of those who once, but no longer, fulfill the cognitive and relational attributes associated with personhood. The relationships among the person, the family and the caregiver are complex and can sustain or diminish personhood (Smebye & Kirkevold, 2013). Sometimes, through
Page | 9
families and their knowledge of the person’s past experiences, preferences and values, caregivers can more specifically address needs that cannot be expressed by the person (Palmer, 2013). Kitwood believed that the personhood of these individuals is supported when the caregiver is present and available to the person living with dementia. Examples of caregiver “positive person work” include: warmth, relaxed pace, respect, acknowledgement of the person and collaboration. Personhood is undermined when individualized needs and rights are not considered. Specifically, Kitwood (1997) stated that personhood is undermined by “malignant social psychology” - caregiver behaviours that are not necessarily intended with malice but which have “become unchallenged and an interwoven part of care” (p. 24). Examples include caregiver behaviours of intimidation, outpacing, infantilization and mockery toward persons living with dementia. On the other hand, personhood is promoted with “positive person work”. Kitwood identified five psychological needs that are based in cultural values and overlap in the central need for love (p. 81). These are: comfort (to feel strong and able to persevere in the face of lost abilities); attachment (to feel connected with others in the face of uncertainty); inclusion (to feel accepted as they are within a social group); occupation (to feel involved with others in a significant way); and identity (to feel recognized as having a history and as being a unique person) (pp. 81-84).
Personhood as legal status Legal definitions of personhood differ from those previously discussed because they are generally conceived to be limited to those who have legal rights and responsibilities (Naffine, 2003). These rights and responsibilities are conferred by the political system and enshrined in the laws of the society within which the individual lives. Personhood as a legal status is intimately linked with the idea of citizenship (Baron, 2015). It is also assumed by most scholars to be essential to the process of making a human rights claim (Flynn & Arstein-Kerslake, 2014; Ohlin, 2005). In other words, one cannot assert one’s human rights or one’s rights as a person unless one is protected as a person under the law. The law is inconsistent in its determination of who is a person, and legal decisions are often based on the theory that best supports the desired outcome (Harvard Law Review Editors, 2001). Further, legal decisions not only reflect social beliefs and values about personhood, they also shape beliefs and values by creating definitions and expectations that guide future policy development and actions. A careful examination of the history of citizenship rights, both in Canada and elsewhere, reveals several troubling facts. First, the history of citizenship uncovers a long-standing fundamental rift between the idea of personhood as an inherent attribute of humans and the idea of personhood under the law. Throughout history, many groups have been legally excluded from the rights associated with citizenship. Slavery, which has been described as a social death because it denies the personhood of those so defined

Page | 10
(Rawls, 1971), continues to be legal in some societies to this day. Extending the rights of citizenship to those initially excluded from these rights has been a long struggle. For example, in Canada, Aboriginal peoples living under the jurisdiction of the Indian Act were not given the right to vote until 1960. With respect to women, Naffine (2003; 2004) asserts that legal persons have always been sexed (adult) male. Many of the challenges that women have encountered in their efforts to attain the full rights and responsibilities of citizenship have been an outcome of the gendered nature of legal definitions of personhood. For example, under the British North America (BNA) Act (1867), Canadian women did not have the right to vote in provincial and federal elections. Manitoba became the first province to extend the franchise to women in 1916. By 1927, with the exception of Aboriginal women and women living in Quebec, most Canadian women had the right to vote in federal and provincial elections. The right for women to hold political office has also been contested within Canadian law. In 1928, in response to a petition from ‘The Famous Five’ (Emily Murphy, Irene Parlby, Nellie Mooney McClung, Louise McKinney and Henrietta Muir Edwards), the Supreme Court of Canada ruled that women did not have the right to be appointed to Senate because they were not defined as persons under the BNA Act. This ruling was overturned by the Privy Council of England in 1929 (Bright, 1998). Children are also excluded from certain legal rights, including the right to vote and, except in exceptional circumstances, the right of consent. Their exclusion from the full rights of personhood have been based primarily on the judgement that they do not yet have the
cognitive capacity to make informed and autonomous decisions (McGillivray, 2011). The right to consent and to make other decisions with legal implications has also been withheld from disabled persons and persons living with significant cognitive impairment. In 2006, renewed attention to the legal rights of these groups followed the release of the United Nations’ Convention on the Rights or Persons with Disabilities (Flynn & Arstein-Kerslake, 2014). In the future, statutory removal of an individual’s legal capacity (personhood) through mechanisms such as guardianship may be no longer permitted under international human rights law. Academics and care providers are currently exploring avenues, such as supported decision-making, to ensure that the affected individual participates to the fullest extent possible and that their desires are upheld when important and potentially life-altering decisions must be made (Flynn & Arstein-Kerslake, 2014). In Canada, the rights of citizens are enshrined in the Canadian Charter of Rights and Freedoms, which protects the fundamental freedoms, democratic rights, legal rights, equality rights and language rights of all citizens (Government of Canada, 2015). Extending the rights of citizenship to those initially excluded from these rights has been a long struggle and Canada’s record in recognizing the personhood of those who live within its borders has been mixed. Today, Canada is one of the few countries that does not explicitly withhold the right to vote from those living with cognitive impairment. On the other hand, prisoners were not given the right to vote until 2002. The personhood of Canadians and their rights of citizenship

Page | 11
continue to be contingent and are shaped by those in positions of political power. CONTEXT TO NURSING AND HEALTH CARE Personhood is an important concept in nursing and health care because it has been identified as a fundamental component to person-centred care (Brooker, 2004; Hunter et al., 2013). As Kitwood and others have argued, every individual has the right to dignity and the right to individualized health care that is respectful of their needs and wishes. Personhood shapes nursing and health care in many ways. First, it influences the nature of the nurse’s interaction with individual clients. The way people understand and relate to each other influences our understanding of personhood and whether we see the other as a person. Personhood has been identified as a fundamental component of client-centred care (Hunter et al., 2013) and therapeutic relationships. Effective communication promotes therapeutic relationships, but communicating with older adults who are living with dementia and with the cognitively impaired can be challenging. Out of his concern for the dignity and personhood of individuals living with dementia, Kitwood (1997) developed the “Enriched Model of Dementia Care” which proposed that neurological impairment, health and physical fitness, biography/life story, personality and social psychology all affect how a person living with dementia acts, feels and thinks (p. 15). Specific strategies for communication
that promote engagement and support personhood (Jootun & McGhee, 2011) are an integral part of professional nursing practice. Second, legal personhood is fundamental to informed consent and who may provide consent for treatment. Health care providers must act within the constraints set out in law and within the ethical codes set out by their profession when making decisions about an individual client’s health care plan. Finally, ideas about personhood also shape the nature of health care, since the question of whether or not all human beings can be seen to be persons has a direct effect on the kind of health care that might be available to them. For example, debates about the personhood of the fetus and the legality of abortion have pre-occupied the legal and health care systems for many decades. More recently, attention has turned to the issues of euthanasia and physician-assisted suicides. Both of these issues current exist on the margins of contemporary society’s willingness to allow individuals to make autonomous decisions about matters related to life and death. Other issues that relate to the concept of personhood and legal rights include the rights of children and those living with significant cognitive impairment to make decisions about their health care. The right of parents to make decisions about withholding treatment or providing specific treatments for their children is also controversial.
In addition, society has historically denied some individuals and groups the status of personhood. This has influenced how they are treated by society which, in turn, may affect their health status.
Page | 12
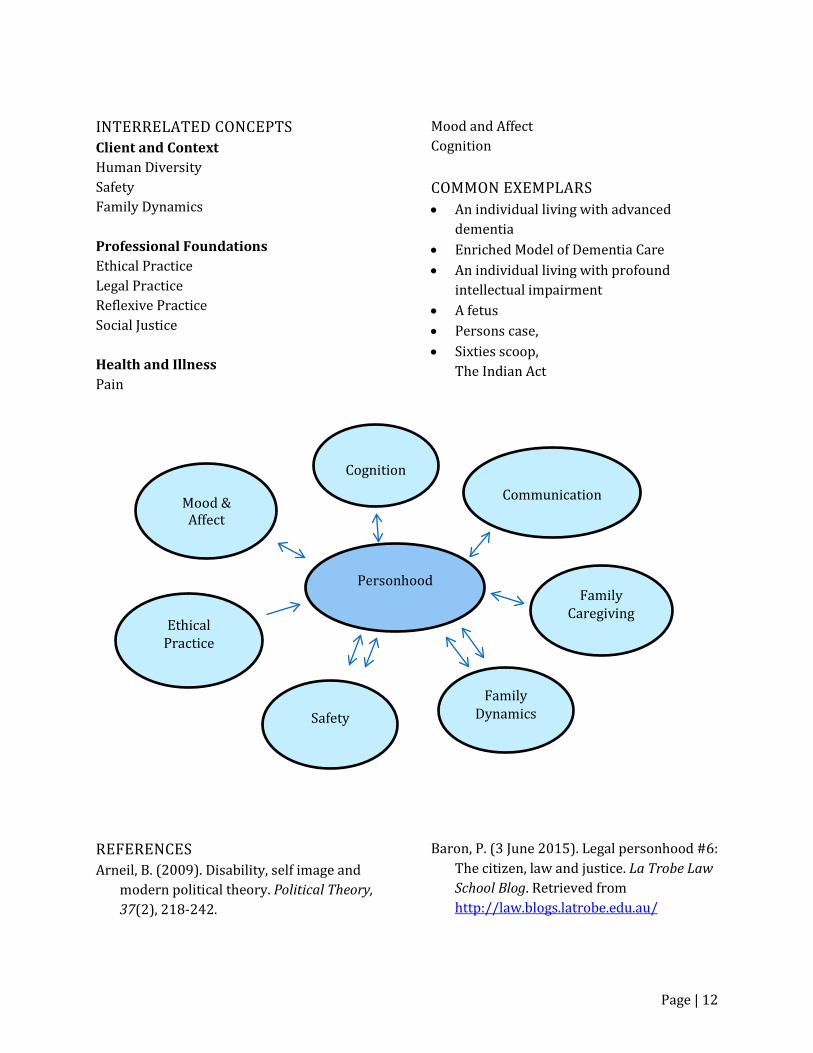
INTERRELATED CONCEPTS Client and Context Human Diversity Safety Family Dynamics Professional Foundations Ethical Practice Legal Practice Reflexive Practice Social Justice Health and Illness Pain
Mood and Affect Cognition COMMON EXEMPLARS • An individual living with advanced
dementia • Enriched Model of Dementia Care • An individual living with profound
intellectual impairment • A fetus • Persons case, • Sixties scoop,
The Indian Act
REFERENCES Arneil, B. (2009). Disability, self image and
modern political theory. Political Theory, 37(2), 218-242.
Baron, P. (3 June 2015). Legal personhood #6: The citizen, law and justice. La Trobe Law School Blog. Retrieved from http://law.blogs.latrobe.edu.au/
Personhood
Communication
Cognition
Family Dynamics Safety
Mood & Affect
Ethical Practice
Family Caregiving
Page | 13
Bright, D. (1998). The other woman: Lizzie Cyr and the origins of the “Persons Case.” Canadian Journal of Law & Society, 13(2), 99-115.
Brooker, D. (2004). What is person-centred
care in dementia? Reviews in Clinical Gerontology, 13 (3), 215-222.
Buron, B. (2008). Levels of personhood: A
model for dementia care. Geriatric Nursing, 29(5), 324-332.
Cox, D. R.A. (2011). The problems with
utilitarian conceptions of personhood in the abortion debate. Journal of Medical Ethics, 37(5), 318-320.
Dewing, J. (2008). Personhood and dementia:
Revisiting Tom Kitwood’s ideas. International Journal of Older People Nursing, 3(1), 3-13.
Farah, M.J., & Heberlein, A.S. (2007).
Personhood and neuroscience: Naturalizing or nihilating? The American Journal of Bioethics, 7(1), 37-48.
Flynn, E., & Arstein-Kerslake. (2014).
Legislating personhood: Realising the right to support in exercising legal capacity. International Journal of Law, 10(1), 81-104.
Government of Canada. (2015). Rights and
freedoms in Canada. Retrieved from http://www.justice.gc.ca/eng/csj-sjc/just/06.html
Harre, R. (1998). The singular self: An
introduction to the psychology of personhood. London, UK: Sage Publications.
Harvard Law Review Editors. (2001). What we talk about when we talk about persons: The language of a legal fiction. Harvard Law Review, 114(6), 1745-1768.
Holdron, C. (2013). The case for legal
personhood for nonhuman animals and the elimination of their status as property in Canada (unpublished master’s thesis). University of Toronto, Toronto, Canada.
Hunter, P. V., Hadjistavropoulos, T., Smythe,
W. E., Malloy, D. C., Kaasalainen, S., & Williams, J. (2013). The Personhood in Dementia Questionnaire (PDQ): Establishing an association between beliefs about personhood and health providers' approaches to person-centred care. Journal of Aging Studies, 27(3), 276-287.
Jootun, D., & McGhee, G. (2011). Effective
communication with people who have dementia. Nursing Standard, 25(25), 42-46.
Kadlac, A. (2010). Humanizing personhood.
Ethical Theory and Moral Practice, 13(4), 421-437.
Kitwood, T. (1997). Dementia reconsidered:
The person comes first. Philadelphia, PA: Open University Press.
Kitwood, T., & Bredin, K. (1992). Person to
person: A guide to the care of those with failing mental powers (2nd ed.). Loughton, Essex: Gale Centre.
Maslow, A. (1970). Motivation and
personality, (revised ed.). New York: Harper & Row.
Page | 14
McGillivray, A. (2011). Children’s rights, paternal power and fiduciary duty: From Roman law to the Supreme Court of Canada. International Journal of Children’s Rights, 19, 21-54.
Naffine, N. (2003). Who are law’s persons?
From Cheshire cats to responsible subjects. The Modern Law Review, 66, 346-367.
Naffine, M. (2004). Our legal lives as men,
women and persons. Legal Studies 21(4), 621-642.
Palmer, J.L. (2013). Preserving personhood of
individuals with advanced dementia: Lessons from family caregivers. Geriatric Nursing, 34, 224-229.
Quintan, A. (1973). The nature of things.
London, UK: Routledge. Ohlin, J. (2005). Is the concept of the person
necessary for human rights? Cornell Law Faculty Publications. Paper 434. Retrieved from http://scholarship.law.cornell.edu/facpub/434
Perry, D.W. (c. 2011). Ethics and personhood:
Some issues in contemporary neurological science and technology. . Retrieved from http://www.scu.edu/ethics/publications/submitted/Perry/personhood.html
Rawls, J. (1971). A Theory of Justice.
Cambridge, MA: Harvard University Press. Redwin, R. (2006). An alternative view of
personhood. The Australian and New
Zealand Journal of Psychiatry, 40(6-7), 608.
Rogers, C. (1980). A way of being. Boston:
Houghton Mifflin. Roháĕ, D. (2010). Knight, Habermas and
Rawls on freedom, personhood and constitutional choice. The European Journal of the History of Economic Thought, 19(1), 23-43.
Saurette, P., & Gordon, K. (2013). Arguing
abortion: The new anti-abortion discourse in Canada. Canadian Journal of Political Science 46(1), 157-185.
Smebye, K.L., & Kirkevold, M. (2013). The
influence of relationships on personhood in dementia care: A qualitative hermeneutic study. BMC Nursing, 12 (29), 1-13.
Silvers, A., & Francis, L. (2009). Thinking
about the good: Reconfiguring liberal metaphysics (or not) for people with cognitive disabilities. Metaphilosophy, 40(3-4), 475-498.
Sullivan, D.M. (2001). A thirty-year
perspective on personhood: How has the debate changed? Ethics and Medicine, 17(3), 177-186.
Taylor, C. (1985). The concept of a person.
Philosophical Papers. Volume 1. Cambridge, UK: Cambridge University Press.
Warren, M. (1973). On the moral and legal
status of abortion. The Monist, 57(1), 43-61.
Page | 15
White, F. (2013). Personhood: An essential characteristic of the human species. The Linacre Quarterly, 80(1), 74-97.
OTHER SOURCES Adkins, L. (2005). The new economy,
property and personhood. Theory, Culture & Society, 22(1), 111.
Alzheimer Europe. (2013). Personhood: Other
ethical principles. Retrieved from http://www.alzheimer-
europe.org/Ethics/Definitions-and-approaches/Other-ethical-principles/Personhood
Blain, S., & McKeever, P. (2011). Revealing
personhood through biomusic of individuals without communicative interaction ability. Augmentative and Alternative Communication, 27(1), 1-4.
Casella, E., & Croucher, K. (2011). Beyond
human: The materiality of personhood. Feminist Theory, 12(2), 209-218.
Hymer, J., & Leuven, K. (1999). Not a modest
proposal: Peter Singer and the definition of person. Ethical Perspectives, 6(2), 126-138.
Ikäheimo, H., & Laitinen, A. (2007).
Dimensions of personhood. Journal of Consciousness Studies, 14(5-6), 6-16.
Landers, M., & McCarthy, G. (2010). A
conceptual model of nursing: A Model of personhood for Irish nursing. Nursing Science Quarterly: Theory, Research and Practice, 23(4), 343-348.
McCance, T., McCormack, B., & Dewing, J.
(2011). An exploration of person-centred
in practice. The Online Journal of Issues in Nursing, 16(2), no page numbers.
McCarthy, G., & Landers, M. (2010). A
conceptual model of nursing: A model of personhood for Irish Nursing, Nursing Science Quarterly, 23(4), 343-347,
Mulder, N. (2011). The crux is the skin:
Reflections on Southeast Asian personhood. Journal of Current Southeast Asian Affairs, 30(1), 95.
Naffine, N. (2011). Review essay: Liberating
the legal person. Canadian Journal of Law and Society, 26(1), 193-203.
Nolan, M. T., & Mock, V. (2004). A conceptual
framework for end-of-life care: A reconsideration of factors influencing the integrity of the human person. Journal of Professional Nursing, 20(6), 351-360.
Nussbaum, M. (2007). Frontiers of justice:
Disability, nationality, species membership. India: Oxford University Press.
Palmer, J. (2013). Preserving personhood of
individuals with advanced dementia: Lessons from family caregivers. Geriatric Nursing, 34, 224-229.
Plaxton, M., & Lardy, H. (2010). Prisoner
disenfranchisement: Four judicial approaches. Berkeley Journal of International Law, 28(1), 101-141.
Ruddick, S. (2007). At the horizons of the
subject: Neo-liberalism, neo-conservatisms and the rights of the child part one: From ‘knowing’ fetus to ‘confused’ child. Gender, Place & Culture, 14(5), 513-527.

Page | 16
Ruddick, S. (2007). At the horizons of the subject: Neo-liberalism, neo-conservatisms and the rights of the child
part two: Parent, caregiver, state. Gender, Place & Culture, 14(6), 627-640.









Page | 105
PROFESSIONAL FOUNDATIONS
The knowledge, skills and attitudes that form the foundations of professional nursing practice.
Resources from Giddens Care Coordination Client Safety (see Giddens, Safety) Clinical Judgment Communication Ethical Practice (see Giddens, Ethics Evidence Informed Practice (see Giddents: Safety) Health Care Quality Health Education (see Giddens, Patient Education) Leadership Legal Practice Professionalism Supportive and Palliative Care (see Giddens, Palliation) Technology and Informatics
Resources from Other Sources Primary Health Care Smith, D. Van Herk, K., and Rahaman, Z. (2012). Primary Health Care. In Stamler, L., & Yiu, L. (eds.)
Community health nursing: A Canadian perspective. Toronto, ON: Pearson, pp. 109-123.
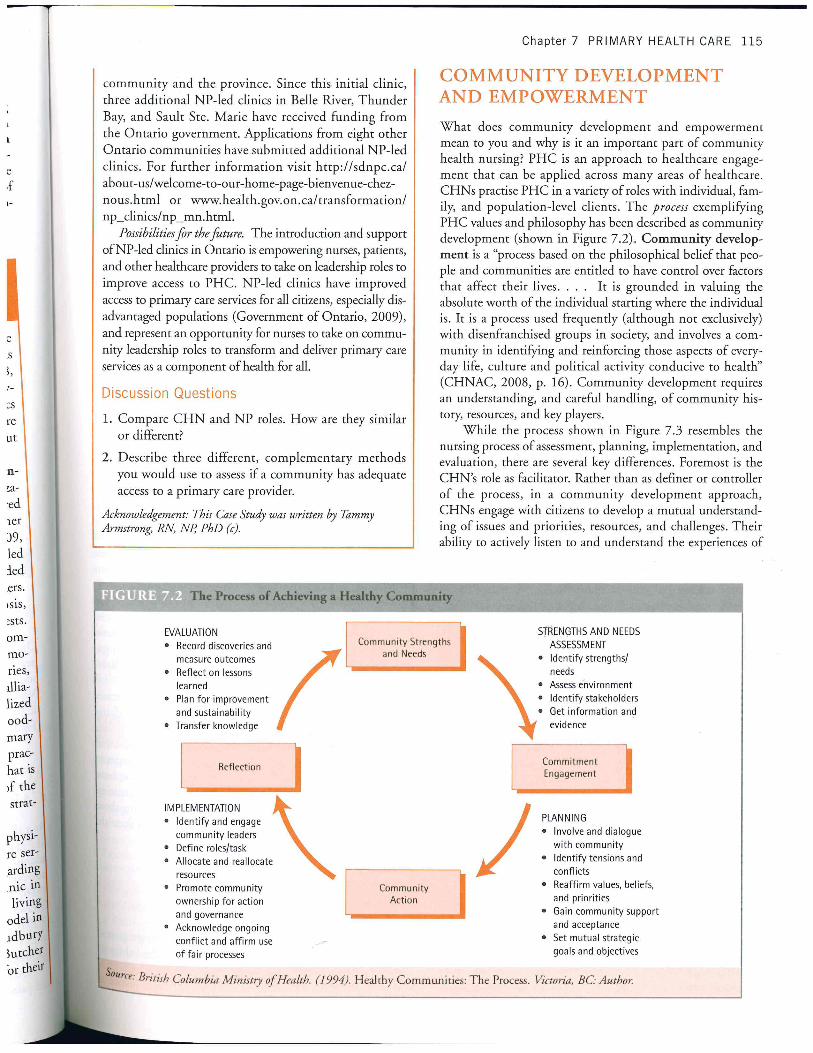
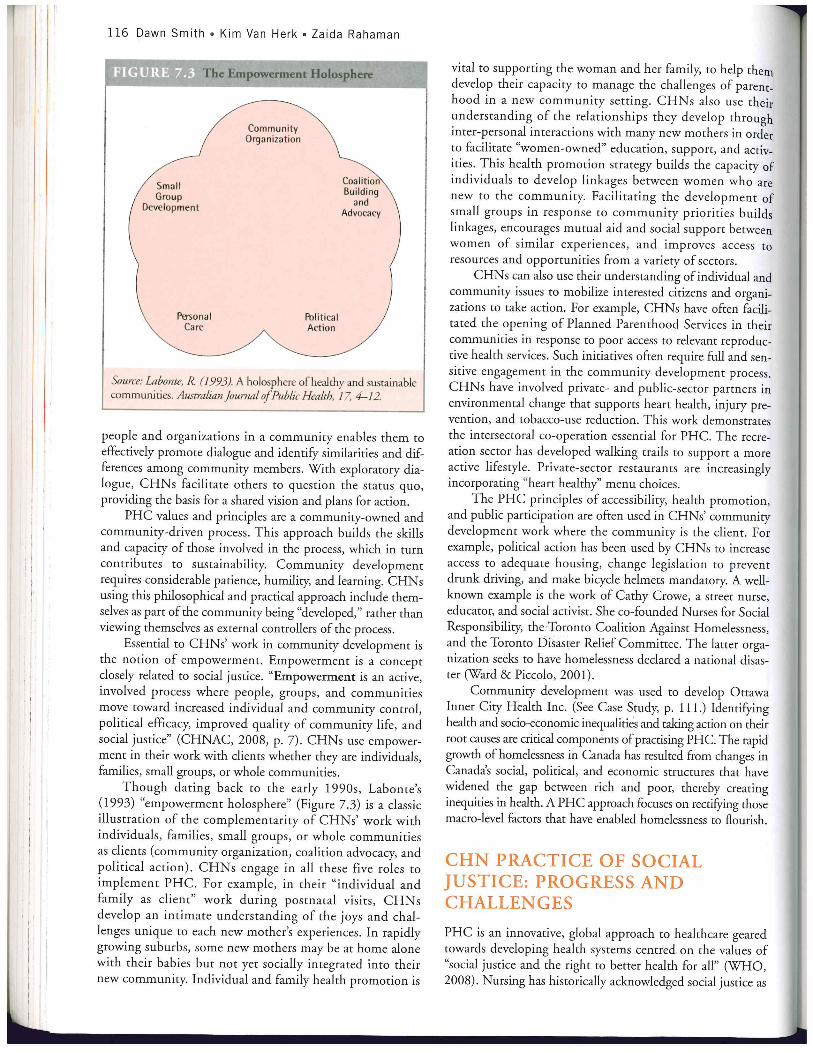
Resources Developed by the College of Nursing Caring: A Relational Process Critical Reflection Interprofessional Collaborative Practice Social Justice
Page | 106
CARING: A RELATIONAL PROCESS
MCKAY, M., ASCHROFT, T., & SEGUIRE, M.
Caring is consistently identified as a fundamental and essential characteristic of professional nursing. Indeed, caring is often used to distinguish medical practice from nursing practice. Yet there is little consensus about how caring in nursing practice should be defined, and even less consensus about whether it can be learned, measured or consistently integrated into nursing practice settings. The centrality of caring in professional nursing practice is contested and controversial. In fact, caring has been identified as the fundamental paradox within professional nursing. American historian Susan Reverby has argued that, while caring individuals are often attracted to nursing, the ‘duty to care’ has operated throughout the profession’s history to disempower nurses, to subordinate them to physicians and to sustain the perception that nursing is women’s work (Reverby, 1987). Martha Rogers, an influential nursing theorist, argued that identifying nursing with caring rather than scientific knowledge undermined the advancement of nursing knowledge and contributed to the anti-intellectualism that she perceived as pervasive within the profession (Smith, 2013). More recent scholarship in the conceptualization of caring has endeavored to move beyond the dichotomies of science/sentiment to create linkages between the art and science of nursing (Nelson & Gordon, 2006; Watson, 2012). Exploration of the rich body of literature on caring as an
integral component of professional nursing practice challenges both new and experienced practitioners to define and re-define caring as a complex and multi-dimensional concept that both underlies and shapes professional nursing practice. DEFINITION Caring is defined as “an interpersonal process that is characterized by expert nursing, interpersonal sensitivity and intimate relationships” (Fingeld-Connett, 2007, p. 198). It is a relational process that involves the nurse’s intentional extension of the self to another to provide physical, emotional, and spiritual comfort and support in response to the human aspect of the health and illness experience. (Boykin and Schoenhofer , 2001b; Kapborg & Berterö, 2003; Pavlish & Ceronsky, 2009). SCOPE, TYPE OR CATEGORY(S) Caring can be conceptualized as a continuum with the complete absence of caring at one end and the complete presence of caring at the other. The absence of caring is characterized by hurried, mechanical, task-oriented, emotionally detached and/or non-competent nursing interventions. The presence of caring is characterized by evidence-based nursing interventions that are responsive to the physical, emotional, psychological and spiritual needs of the client and the client’s family. ATTRIBUTES Brilowsky & Wendler (2005) proposed five attributes of caring in professional nursing.

Page | 107
These are: relationship, action, attitude, acceptance and variability. The first, relationship, occurs when the nurse is motivated to respond to an identified client need. Relationships are characterized by trust, intimacy, and responsibility; and are created through personal qualities such as openness, sincerity, love, and patience (p. 643). The second attribute, action, occurs in response to the identified client needs. Caring actions include nursing care, touch, presence, and competence (Brilowsky & Wendler, 2005, p. 644). Within the context of professional nursing practice, action includes moral and ethical dimensions. The individual providing nursing care within the caring relationship is responsible for ensuring that their actions are informed by current evidence and knowledge (Brilowsky & Wendler, 2005, p. 643). The third attribute of caring identified by Brilowsky & Wendler (2005) is attitude. Caring is accomplished through a particular way of acting, which includes (amongst other characteristics) a positive attitude and a work style that integrates visible evidence of concern and compassion for others, reflective self-knowledge, ethical values and courage (Brilowsky & Wendler, 2005, p. 644). Acceptance, the fourth attribute of caring proposed by Brilowsky & Wendler (2005), involves the belief that all human beings are worthy of dignity and respect (p. 645). The fifth attribute, variability, describes a process by which caring behaviours are shaped by the unique circumstances of each encounter between the nurse and client. The capacity of the nurse to modify caring interventions increases over time and is learned with
experience (Brilowsky & Wendler, 2005, p. 645). Finfgeld-Connett (2007) proposed three attributes of caring: expert nursing, interpersonal sensitivity, and intimate relationships. Many elements of these three attributes echo and amplify those identified by Brilowsky & Wendler (2005). In analyzing the attribute of expert nursing, Finfgeld-Connett (2007) emphasizes the importance of expert nursing knowledge and skills, but also argues that expert nursing involves advocacy and empowering clients to care for themselves. Interpersonal sensitivity includes elements congruent with those included in Brilowsky & Wendler’s (2005) attributes of attitude, acceptance and variability. However, Finfgeld-Connett explicitly includes the identification and consideration of cultural differences as an important element of interpersonal sensitivity. Finfgeld-Connett’s (2007) third attribute, intimate relationships, is similar to Brilowsky & Wendler’s (2005) attribute of relationship. However, Finfgeld-Connett (2007) argues that caring relationships are extended to the client’s family. She further argues that there are cultural variations in caring relationships that shape their nature and enactment (Finfgeld-Connett, 2007, p. 200). THEORY Rolfe (2008) argues that there is no shared understanding of what is meant by the term caring. In his analysis of the literature, he argues that the term is used in at least four ways: 1) a generic term for nursing practice; 2) a specific term for a particular type of practice (e.g. comfort care); 3) an emotional state (caring about); and 4) both caring for and caring about (p. 146).

Page | 108
The lack of a consistent definition of what is meant by caring in nursing is reflected in the many conceptualizations of caring found in the literature. Most theories of caring incorporate an analysis of the relational process of caring, which involves the human act of being present with and attuned to the client’s experience of illness and their need for nursing care. Some theories incorporate the emotional and behavioural attributes of the nurse, including professionalism. The ethical dimensions of the caring relationship, including honesty, are incorporated into some theories of caring. Less frequently, the nurse’s knowledge and skill are integrated into theoretical approaches to caring in nursing practice. A number of theorists have explored caring and caring in nursing. Milton Mayeroff, a philosopher, proposed a definition and theory of caring that has profoundly influenced the development of nursing theories about caring. Mayeroff conceptualized caring as the act of enabling ‘the other’ to grow while fully acknowledging their agency and personhood (Smith, 2013). He identified eight components of caring: 1) knowing, 2) alternating rhythm, 3) hope, 4) trust, 5) courage, 6) humility, 7) patience, and 8) honesty (Mayeroff, 1971). The cognitive (knowledge) dimensions of caring are incorporated in the components of knowing and alternating rhythm. The latter dimension is described by Mayeroff as the capacity to move between narrow and wide points of view to gain a fuller understanding of ‘the other’ (Smith, 2013). In his writings, Myeroff dismissed the notion that knowledge was not an integral component of a caring relationship:
To care for someone, I must know many things. I must know, for example, who the other is, what his powers and limitations are, what his needs are, and what is conducive to his growth. I must know how to respond to his needs and what my own powers and limitations are. (Myeroff, 1971, p. 13)
Attributes of the care-giver incorporated into Mayeroff’s theory include hope, trust, courage, humility and patience. The ethical dimensions of caring are incorporated in the dimension of honesty. Simone Roach, a Canadian nurse, theorist and ethicist proposed six elements of caring: compassion, competence, confidence, conscience, commitment and comportment (Roach, 2002). Roach argues that caring is the “human mode of being” (2002, p. 28). She further proposed that caring is achieved through relationships with others and by valuing others. As is the case with Myeroff, Roach’s theoretical approach to caring incorporates the knowledge and skills (competence), attributes (compassion, confidence, commitment, comportment) of the nurse, and the ethical dimensions (conscience) of the caring relationship. Like Myeroff, Roach argues that knowledge is an essential component of the caring relationship. Caring in nursing practice can be fully achieved only when the nurse possesses the knowledge and skills required for their work:
Caring is professionalized in nursing and in other helping professions through affirmation of
Page | 109
caring as the human mode of being, and through development of the capacity to care through the acquisition of skills – cognitive, affective, technical, administrative – required for the fulfillment of prescribed roles. (Roach, 2001, p. 39).
Jean Watson, a nursing theorist, has long proposed a theoretical approach to caring that reframes caring as a science. In so doing, Watson argues that the traditional scientific (medical) paradigm does not adequately support an understanding of “the phenomena of human caring in nursing” (Watson, 2012, p. 26). In particular, Watson argues that scientific approaches to knowledge development and knowing are detached from human experiences and “neutral in regard to human values” (Watson, 2013, p. 145). The development of a mature capacity to explore the science of caring would balance science with humanism, and would support the nursing’s efforts to develop a scientific heritage that supports the art and science of nursing. The 10 carative factors specified in Watson’s theory are: 1) humanistic-altruistic system of values, 2) faith-hope, 3) sensitivity to self and others, 4) helping-trusting, human care relationship, 5) expressing positive and negative feelings, 6) creative problem-solving, caring process, 7) transpersonal teaching-learning, 8) supportive, protective, and/or corrective mental, physical, societal and spiritual environment, 9) human needs assistance; and 10) existential-phenomenological-spiritual forces (Watson, 2012; Watson, 2013). When compared to Myeroff and Roach, Watson’s theory of Human Caring Science lacks the cognitive dimension that the other
theorists specified was an essential component of the caring relationship. When knowledge is discussed at all, it is within the context of knowledge development in the science of caring. CONTEXT TO NURSING AND HEALTH CARE Caring is a fundamental component of professional nursing practice. It inspires, validates and sustains nursing practice and contributes to the nurse’s ability to achieve the full scope of professional nursing practice. Caring is often conceptualized as an innate quality that is possessed by some individuals and not others, but some theorists have argued that caring can also be learned (Finfgeld-Connett, 2007).
The abstract and ambiguous nature of caring means that it may not be fully understood or valued by nurses or the systems within which professional nursing practice takes place (Brilowski & Wendler, 2005; Finfgeld-Connet, 2007, Nelson & Gordon, 2006; Rolfe, 2009). Nurses themselves may not have the educational background to fully understand the theoretical underpinnings of caring theory. McCance, McKenna & Boore (1999) observed that many nursing theories of caring are based on abstract and complex ideas from drawn from philosophy, anthropology, theology, human science and the liberal arts. These bodies of knowledge may not be familiar to professional nurses. In addition, nurses who are more comfortable with a concrete or measurable world-view may not be able to understand the connections between caring theories, research findings based on these theories and nursing practice (McCance , McKenna & Boore, 1999). Caring may also be invisible or absent (Roach, 2002) within the healthcare system, particularly in instances where the focus is on measurable outcomes and benchmarking (Corbin, 2008; Mayben 2008).
Page | 110
Caring is a process, and mastery of that process occurs over time (Brown, 2011). Fundamental to the process is the nurse’s mastery of health, pathology, technology and psychomotor skills (knowledge and skill) so that it becomes possible to create the time and space necessary for caring relationships (Doane & Varcoe, 2007; Griffiths, 2007).
Caring involves antecedents and outcomes in addition to the actual caring encounter. The antecedents of caring are located within the care recipient, the nurse, and the work environment (Finfgeld-Connett, 2007). Many factors impinge on caring. Considerable emphasis has been placed on the nurse’s capacity to enter into a caring relationship, including knowing one-self as a caring person, the development of different ways of knowing the other, and possession of the capacity to appreciate the humanity of the other (Boykin & Schoenhofer, 2001; Brilowski & Wendler, 2005; Tarlier, 2005).
The most sustained discussion regarding factors that detract from the nurse’s capacity
to care centres around the challenge of creating caring work environments in the face of the increased workloads, patient acuity and other working conditions experienced by nurses (Clarke, Watson & Brewer; Corbin, 2008; Doane & Varcoe, 2007; Griffiths, 2008). Taking time to care within a system that does not consistently create the space within which to care becomes the challenge of every registered nurse and a particular challenge of nurses in leadership positions.
Finfgeld-Connett (2007) also asserts that the client’s need and openness to caring is also an important antecedent of the caring process. However, critical analysis of the range of health care needs to which nurses respond in the practice raises the question of whether caring is also possible in instances where the client is unable to perceive and/or reciprocate the caring encounter, including the unconscious patient, the profoundly cognitively impaired patient and even the care of the dead.
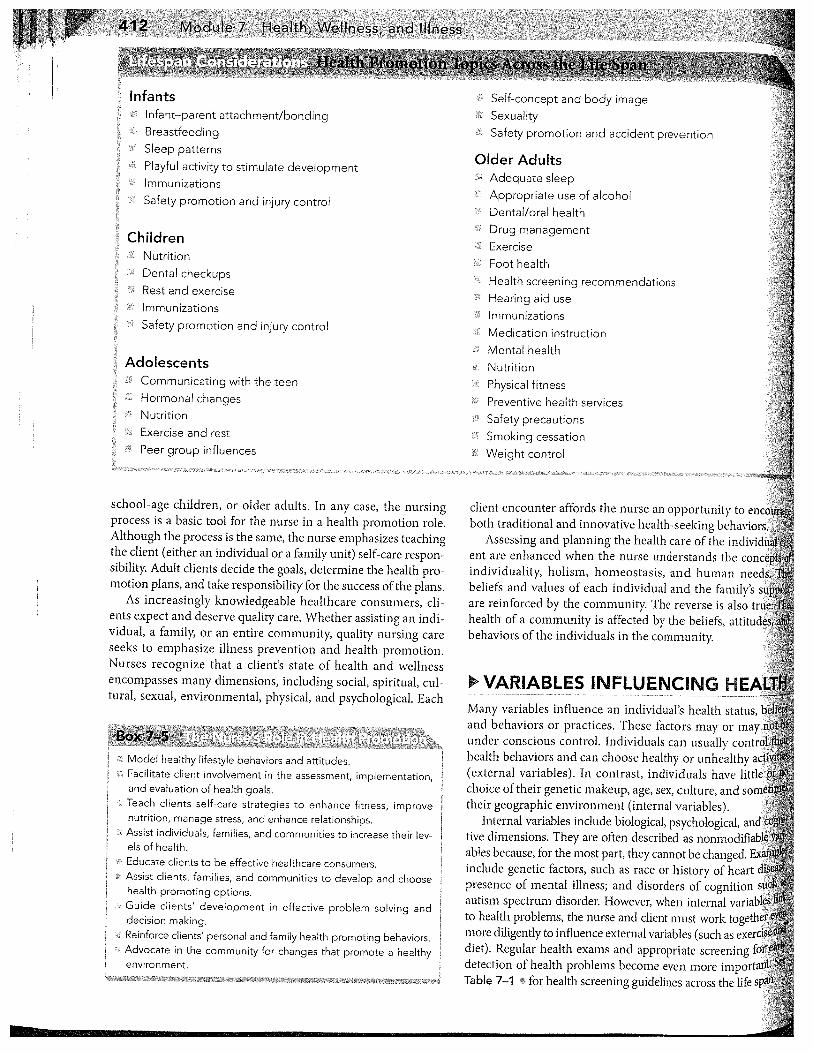
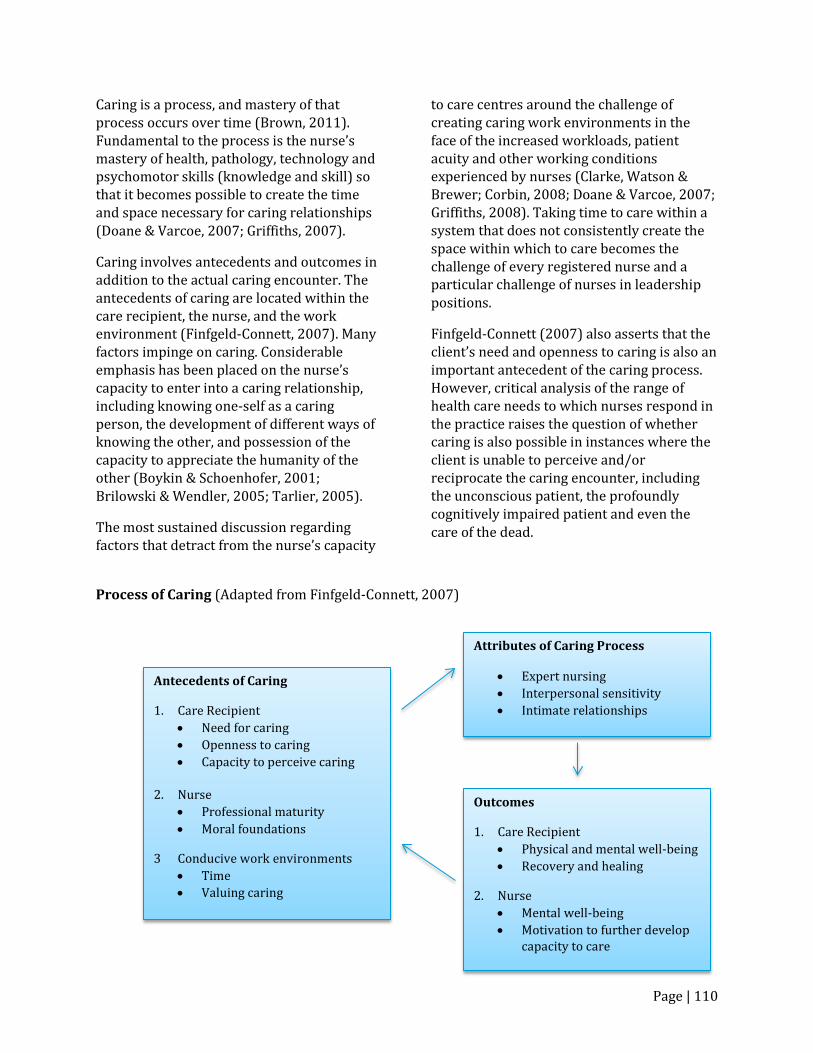
Process of Caring (Adapted from Finfgeld-Connett, 2007)
Antecedents of Caring
1. Care Recipient • Need for caring • Openness to caring • Capacity to perceive caring
2. Nurse
• Professional maturity • Moral foundations
3 Conducive work environments • Time • Valuing caring
Attributes of Caring Process
• Expert nursing • Interpersonal sensitivity • Intimate relationships
Outcomes
1. Care Recipient • Physical and mental well-being • Recovery and healing
2. Nurse • Mental well-being • Motivation to further develop
capacity to care
Page | 111
INTERRELATED CONCEPTS Client and Context Personhood Professional Foundations Clinical Judgment Communication
Critical Reflection Ethical Practice Evidence-informed Practice COMMON EXEMPLARS Client Centred Care Dignity Care Trauma Informed Care
REFERENCES Boykin, A., & Schoenhofer, S. (2001a). Nursing
as caring: A model for transforming practice. Sudbury, MA: Jones & Bartlett.
Boykin, A., & Schoenhofer, S. (2001b). The
role of nursing leadership in creating caring environments in health care delivery systems. Nursing Administration Quarterly, 25(3), 1-7.
Brilowski, G., & Cecilia Wendler, M. (2005).
An evolutionary concept analysis of caring. Journal of Advanced Nursing, 50(6), 641-650.
Brown, L. (2011). Revisiting our roots: Caring
in nursing curriculum design. Nurse Education in Practice, 11(6), 360-364.
Clarke, P, Watson, J., & Brewer, B. (2009).
From theory to practice; Caring Science according to Watson and Brewer, Nursing Science Quarterly, 22(4), 839-345.
Corbin, J. (2008). Is caring a lost art in
nursing? International Journal of Nursing Studies, 45(2), 163-165.
Doane, G. H., & Varcoe, C. (2007). Relational
practice and nursing obligations. Advances in Nursing Science, 30(3), 192-205.
Finfgeld-Connett, D. (2008). Meta-synthesis of
caring in nursing. Journal of Clinical Nursing, 17(2), 196-204.
Griffiths, P. (2008). The art of losing ….? A
response to the question ‘is caring a lost art?’. International Journal of Nursing Studies, 45(3), 329-332.
Maben, J. (2008). The art of caring: Invisible
and subordinated? International Journal of Nursing Studies, 45(3), 335-338.
McCance, T., McKenna, H., & Boore, J. (1999).
Caring: Theoretical perspectives of relevance to nursing. Journal of Advanced Nursing, 30(6), 1388-1395.
Myeroff, M. (1971). On Caring. New York, NY:
Harper-Collins. Nelson, S. & Gordon, S. (2006). The
complexities of care: Nursing reconsidered. Ithaca, NY: Cornell University Press.
Pavlish, C., & Ceronsky, L. (2009). Oncology
nurses' perceptions of nursing roles and professional attributes in palliative care. Clinical Journal of Oncology Nursing, 13(4), 404-12.
Reverby, S. (1987). Ordered to care: The
dilemma of American nursing, 1850 –
Page | 112
1945. Cambridge, UK: Cambridge University Press.
Roach, S. (2002). Caring, the human mode of
being, (2nd rev. ed.). Ottawa, ON: CHA Press.
Rolfe, G. (2009). Some further questions on
the nature of caring. International Journal of Nursing Studies, 46(1), 143-146.
Smith, M. (1999). Caring and the Science of
Unitary Human Beings. Advances in Nursing Science, 21(4), 14-28.
Smith, M. (2013). Caring and the discipline of
nursing. In Smith, M., Turkel, M., & Wolf, Z. (Eds). Caring in nursing classics: An essential resource. New York, NY: Springer Publishing, pp. 1-8.
Tarlier, D. (2005). Mediating the meaning of
evidence through epistemological diversity. Nursing Inquiry, 12(2), 126-134.
Watson, J. 2013). Nursing: The philosophy
and science of caring. In In Smith, M., Turkel, M., & Wolf, Z. (Eds). Caring in nursing classics: An essential resource. New York, NY: Springer Publishing, pp. 143-153.
Watson, J. (2012). Human Caring Science: A
theory of nursing, 2nd ed. Sudbury, MA: Jones & Bartlett Learning.
OTHER SOURCES Bath, H. (2008). The three pillars of trauma-
informed care. Reclaiming Children & Youth, 17(3), 17-20.
Bulfin, S. (2005). Nursing as Caring Theory: Living Caring in Practice. Nursing Science Quarterly : Theory, Research and Practice, 18(4), 313.
Courtois, C.A. (1999). Recollections of sexual
abuse: Treatment principles and guidelines. New York: W. W. Norton & Company.
Dyess, S., Boykin, A., & Rigg, C. (2010).
Integrating Caring Theory With Nursing Practice and Education: Connecting With What Matters. JONA: The Journal of Nursing Administration, 40(11), 498-503.
Dyess, S., Boykin, A., & Bulfin, M. (2013).
Hearing the Voice of Nurses in Caring Theory-Based Practice. Nursing Science Quarterly, 26(2), 167-173.
Dyess, S., Boykin, A., & Rigg, C. (2010).
Integrating Caring Theory With Nursing Practice and Education: Connecting With What Matters. JONA: The Journal of Nursing Administration, 40(11), 498-503
Harris, M., & Fallot, R. (2001). Using trauma
theory to design service systems. New Directions for Mental Health Services, 89. Jossey Bass.
Kapborg, I., & Berterö, C. (2003). The
phenomenon of caring from the novice student nurse's perspective: A qualitative content analysis. International Nursing Review, 50(3), 183-192.
Morrow, M. (2011). Caring and Nursing
Theory-Guided Practice. Nursing Science Quarterly : Theory, Research and Practice, 24(3), 287-289.

Page | 113
CRITICAL REFLECTION
MCKAY, M.
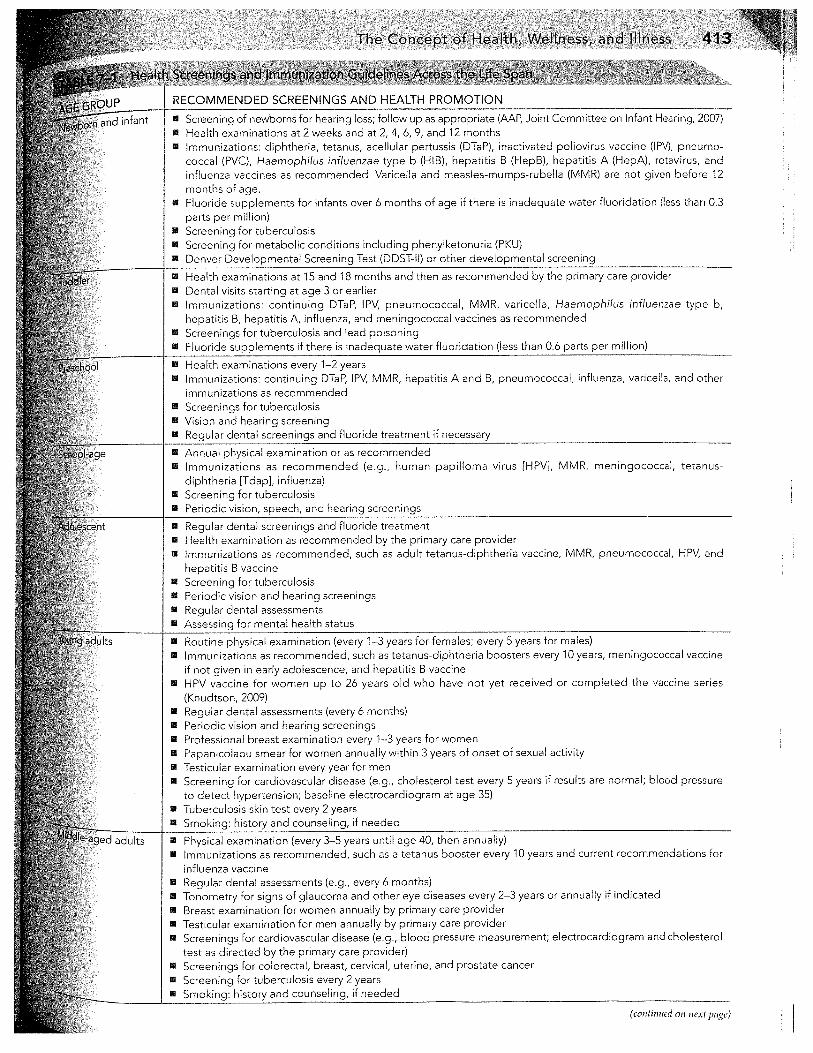
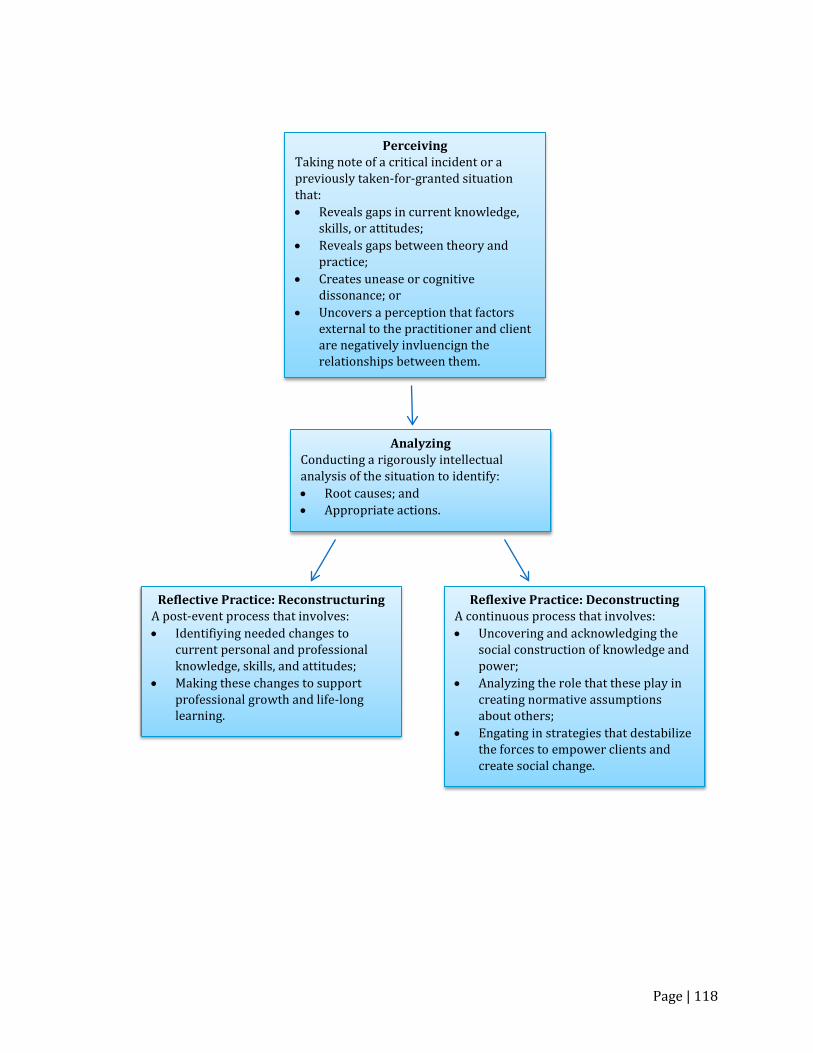
Professional nursing practice is characterized by practitioners who think deeply about their knowledge, skills and attitudes; about their clients and their circumstances; and about the organizational, social and political context within which they engage with their clients. A variety of terms have been used, often interchangeably, to describe this process. These include reflection (Bolton, 2010; Chambers, Brosnan, & Hassell, 2011; Kinsella, 2009), critical reflection (Josephson, 2014), reflexive practice (Bruno, Galuppo, & Gillardi, 2011; D’Cruz, Gillingham & Melendez, 2007; Lam, Wong & Leung, 2013), and critical reflection (Brookfield, 2009; Fook, White, & Gardner, 2006; Hibbert, 2013; Mackay & Tymon, 2013; Smith, 2011). DEFINITION Critical reflection is defined as “the process by which adults identify the assumptions governing their actions, locate the historical and cultural origins of these assumptions, question the meaning of these assumptions, and develop alternative ways of thinking” (Stein, 2000, p. 3). SCOPE, TYPE OR CATEGORY(IES) Critical reflection occurs at multiple levels, with different purposes and outcomes. Williams (2001) describes three levels of reflection, which, when the third level is achieved, can be conceptualized as critical reflection. 1. Content reflection This is the lowest level of reflection, which asks the question “what”? Practitioners enact content reflection when they encounter a new situation, procedure or piece of equipment, and need to understand the difference
between it and what they previously knew or understood. 2. Process reflection Process reflection occurs in instances where the practitioner perceives that their current knowledge, skills or abilities are not sufficient to guide decision-making and action in this situation. It asks the question “how”? Process reflection often motivates the practitioner to acquire new knowledge and skills, which is a fundamental component of life-long learning and professional growth. Content and process reflection are very similar in that both uncover attributes of the practitioner (knowledge, skills and attitudes) that require attention and further professional development. 3. Premise reflection (critical reflection) Premise or critical reflection asks the question “why”? This kind of analysis occurs when the practitioner deconstructs practice situations to uncover personal and social assumptions, particularly those where socially constructed knowledge and power-relations prevent both the practitioner and the client from achieving health outcomes desired by the client. ATTRIBUTES 1. Perception Taking note of a critical incident or a previously taken-for-granted situation that: • Reveals gaps in current knowledge, skills
or attitudes; • Reveals gaps between theory and
practice; • Creates unease or cognitive dissonance;
or
Page | 114
• Uncovers a perception that factors external to the practitioner and client are negatively influencing the relationship between them.
2. Analysis Conducting a rigorously intellectual analysis of the situation to identify: • Root causes; and • Appropriate actions. 3. Reconstruction (Content or Process
Reflection) A post-event process that involves: • Identifying needed changes to current
personal and professional knowledge, skills and attitudes; and
• Making these changes to support professional growth and life-long learning.
And/or 4. Deconstruction (Critical Reflection) A continuous process that involves: • Uncovering and acknowledging the social
construction of knowledge and power; • Analyzing the role that these play in
creating normative assumptions about others;
• Engaging in strategies that de-stabilize these forces to empower clients and create social change.
THEORY There are several problems with the current state of concept development for critical reflection. First, as previously noted, many terms are used interchangeably despite the fact that their theoretical foundations and intended outcomes are different (Lam et al., 2007; Ryan, 2012). Second, in instances where distinctive definitions and processes are identified, these are not always consistent with other definitions and processes described in the literature. Third, and perhaps most importantly, many theorists who seek to differentiate between the many
terms that characterize the process of intentionally analyzing troubling practice situations do not appear to recognize their similarities or that both the reconstruction and deconstruction components of critical reflection can occur simultaneously. The reconstructive component of critical reflection (frequently referred to as reflection or self-reflexivity) is most consistently described in the literature as a self-defining process that seeks to achieve professional growth and life-long learning through the purposive examination of the individual’s assumptions and experience, both personal and professional (Binding, Morck, & Moules, 2010; D’Cruz et al., 2007; Lam et al., 2013). This type of analysis is often triggered after a critical incident which alerts the practitioner to the reality that his/her current knowledge, skills and/or attitudes were not sufficient to deal successfully with a work-related situation (D’Cruz, 2007). Several sources (Bolton, 2010; D’Cruz, 2007) describe this process as reflection-on-action. The primary outcome of the reconstructive process is sustained change in the knowledge, skills and/or attitudes of the practitioner. In instances where reflection creates changes in the nurse’s capacity to engage effectively with clients, reflective practice may also change the nurse’s relationships with clients. The deconstructive component of critical reflection (frequently referred to as reflexivity) is described as the deliberate work on the part of the practitioner to uncover the socially constructed politics of knowledge and power that underlie relationships between the practitioner and clients. In particular, deconstruction is directed towards an analysis and challenge of the ‘taken for granted’, and the asymmetrical structures of power and knowledge (including professional knowledge) which underlie and shape relationships with clients (Ahmed, 2008; Binns, 2008; D’Cruz, 2007;
Page | 115
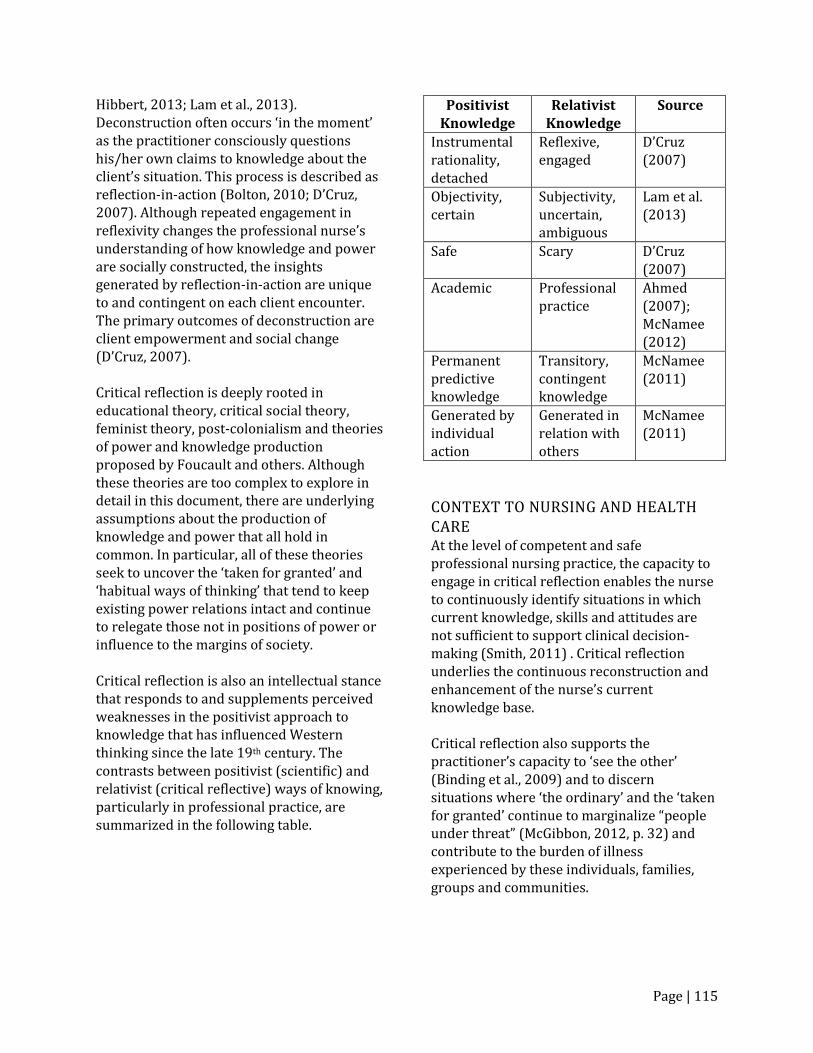
Hibbert, 2013; Lam et al., 2013). Deconstruction often occurs ‘in the moment’ as the practitioner consciously questions his/her own claims to knowledge about the client’s situation. This process is described as reflection-in-action (Bolton, 2010; D’Cruz, 2007). Although repeated engagement in reflexivity changes the professional nurse’s understanding of how knowledge and power are socially constructed, the insights generated by reflection-in-action are unique to and contingent on each client encounter. The primary outcomes of deconstruction are client empowerment and social change (D’Cruz, 2007). Critical reflection is deeply rooted in educational theory, critical social theory, feminist theory, post-colonialism and theories of power and knowledge production proposed by Foucault and others. Although these theories are too complex to explore in detail in this document, there are underlying assumptions about the production of knowledge and power that all hold in common. In particular, all of these theories seek to uncover the ‘taken for granted’ and ‘habitual ways of thinking’ that tend to keep existing power relations intact and continue to relegate those not in positions of power or influence to the margins of society. Critical reflection is also an intellectual stance that responds to and supplements perceived weaknesses in the positivist approach to knowledge that has influenced Western thinking since the late 19th century. The contrasts between positivist (scientific) and relativist (critical reflective) ways of knowing, particularly in professional practice, are summarized in the following table.
Positivist Knowledge
Relativist Knowledge
Source
Instrumental rationality, detached
Reflexive, engaged
D’Cruz (2007)
Objectivity, certain
Subjectivity, uncertain, ambiguous
Lam et al. (2013)
Safe Scary D’Cruz (2007)
Academic Professional practice
Ahmed (2007); McNamee (2012)
Permanent predictive knowledge
Transitory, contingent knowledge
McNamee (2011)
Generated by individual action
Generated in relation with others
McNamee (2011)
CONTEXT TO NURSING AND HEALTH CARE At the level of competent and safe professional nursing practice, the capacity to engage in critical reflection enables the nurse to continuously identify situations in which current knowledge, skills and attitudes are not sufficient to support clinical decision-making (Smith, 2011) . Critical reflection underlies the continuous reconstruction and enhancement of the nurse’s current knowledge base. Critical reflection also supports the practitioner’s capacity to ‘see the other’ (Binding et al., 2009) and to discern situations where ‘the ordinary’ and the ‘taken for granted’ continue to marginalize “people under threat” (McGibbon, 2012, p. 32) and contribute to the burden of illness experienced by these individuals, families, groups and communities.
Page | 116
INTERRELATED CONCEPTS Client Safety
Social Justice Cultural Safety
REFERENCES Ahmed, B. (2008). Teaching critical
psychology of ‘race’ issues: Problems in promoting anti-racist practice. Journal of Community and Applied Social Psychology, 1, 54-67.
Binding, L., Morck, A., & Moules, N. (2010).
Learning to see the other: A vehicle of reflection. Nurse Education Today, 30(6), 591-4.
Binns, J. (2008). The ethics of relational
leading: Gender matters. Gender, Work and Organization, 15(6), 600-620.
Bolton, G. (2010). Reflective practice: Writing
and professional development. Los Angeles, CA: Sage Publications.
Brookfield, S. (2009). The concept of critical
reflection: Promises and contradictions. European Journal of Social Work, 12(3), 293-304.
Bruno, A., Galupp, L, & Gilardi, S. (2011).
Evaluating the reflexive practices in a learning experience. European Journal of Psychological Education, 26, 527-543.
Chambers, S., Brosnan, C., & Hassell, A.
(2011). Introducing medical students to reflective practice. Education for Primary Care, 22, 100 – 105.
D’Cruz, H., Gillingham, P., & Melendez, S.
(2007). Reflexivity: A concept and its meanings for practitioners working with children and families. Critical Social Work, 8(1), no page numbers. Retrieved from:
http://www1.uwindsor.ca/criticalsocialwork/2007-volume-8-no-1
Fook, J., White, S., & Gardner, F. (2006).
Critical reflection: A review of contemporary literature and understandings. In S. White, J. Fook, & F. Gardner (Eds.), Critical Reflection in Health and Social Care (pp. 3-20). Berkshire, UK: Open University Press.
Hibbert, P. (2013). Approaching reflexivity
through reflection: Issues for critical management education. Journal of Management Education, 37(6), 803-827.
Josephsen, J. (2014). Critically reflexive
theory: A proposal for nursing education. Advances in Nursing. Retrieved from: http://dx.doi.org/10.1155/2014/594360
Kinsella, E.A. (2009). Professional knowledge
and the epistemology of reflective practice. Nursing Philosophy, 11, 3-14.
Lam, C.M., Wong, H., & Leung, T. (2007). An
unfinished reflexive journey: Social work students’ reflection on their placement experiences. British Journal of Social Work, 37, 91-105.
Mackay, M., & Tymon, A. (2013). Working
with uncertainty to support the teaching of critical reflection. Teaching in Higher Education, 18(6), 643-655.
McGibbon, E. (2012). People under threat:
Health outcomes and oppression. In E. McGibbon (Ed.) Oppression: A social
Page | 117
determinant of health (pp. 32-44). Winnipeg, MB: Fernwood Publishing.
McNamee, S. (2012). From social construction
to relational construction: Practices from the edge. Psychological Studies, 57(2), 150-156.
Ryan, M. (2012). The pedagogical balancing
act: Teaching reflection in higher education. Teaching in Higher Education, 18(2), 144-155.
Smith, E. (2011). Teaching critical reflection.
Teaching in Higher Education, 16(2), 211-223.
Stein, D. (2000). Teaching critical reflection.
Myths and Realities, 7. Retrieved from http://eric.ed.gov/?id=ED445256
Williams, B. (2001). Developing critical
reflection for professional practice through problem based learning. Journal of Advanced Nursing 34(1), 27-34.
OTHER SOURCES Alvesson, M., Hardy, C., & Harley, B. (2008).
Reflecting on reflexivity: Reflexive textual practices in organization and management theory. Journal of Management Studies, 45(3), 480-501.
Browne, A. (2000). The potential contributions of Critical Social Theory to nursing science. Canadian Journal of Nursing Research, 32(2), 35-55.
Carbó, P. (2008). Reflexive practice as ethics
and political position: Analysis in an ethnographic study of heroin use. Qualitative Social Work, 7, 466-483.
D’Cruz, H., Gillingham, P., & Melendez, S.
(2007). Reflexivity, its meanings and relevance for social work: A critical review of the literature. British Journal of Social Work, 7, 73-90.
Duffy, A. (2007). A concept analysis of
reflective practice: Determining its value to nurses. British Journal of Nursing, 16(22), 1400-1407.
Fook, J., & Gardner, F. (2013). Critical
reflection in context: Applications in health and social care. London, UK: Routledge.
Lacefield, S. (2011), Critical reflection as a
facilitator of palliative care in the neonatal intensive care unit. Journal of Hospice & Palliative Nursing, 14(6), 405-413.
Smith, R. (2005). Does reflexivity separate the
human sciences from the natural sciences? History of the Human Sciences, 18(1), 1-25.
Page | 118
Perceiving Taking note of a critical incident or a previously taken-for-granted situation that: • Reveals gaps in current knowledge,
skills, or attitudes; • Reveals gaps between theory and
practice; • Creates unease or cognitive
dissonance; or • Uncovers a perception that factors
external to the practitioner and client are negatively invluencign the relationships between them.
Analyzing Conducting a rigorously intellectual analysis of the situation to identify: • Root causes; and • Appropriate actions.
Reflective Practice: Reconstructuring A post-event process that involves: • Identifiying needed changes to
current personal and professional knowledge, skills, and attitudes;
• Making these changes to support professional growth and life-long learning.
Reflexive Practice: Deconstructing A continuous process that involves: • Uncovering and acknowledging the
social construction of knowledge and power;
• Analyzing the role that these play in creating normative assumptions about others;
• Engating in strategies that destabilize the forces to empower clients and create social change.